Embed Size (px)
Citation preview

EXTRACORPOREAL CIRCULATION FOR CARDIOPULMONARY FAILURE
ROBERT H. BARTLETT, M.D. ALAN B. GAZZANIGA, M.D.
0011-3840/78/0005-0001505.00 �9 1978 Year Book Medical Publishers, Inc.

TABLE OF CONTENTS
SELF-ASSESSMENT QUESTIONS . . . . . . . . . . . . . . 3
HISTORY OF EXTRACORPOREAL CIRCULATION . . . . . . . . . 4
ARTIFICIAL ORGANS . . . . . . . . . . . . . . . . . 9
PHYSIOLOGY AND PATHOPHYSIOLOGY OF EXTRACORPOREAL
CIRCULATION . . . . . . . . . . . . . . . . . . . . 2~
TECHNIQUES OF CLINICAL ECMO . . . . . . . . . . . . . 46
CLINICAL E C M O IN ACUTE RESPIRATORY FAILURE . . . . . . 57
CLINICAL E C M O IN SHOCK . . . . . . . . . . . . . . . 75
OTHER APPLICATIONS OF ECMO . . . . . . . . . . . . . 81
EXTRACORPOREAL SUPPORT: ARTIFICIAL ORGANS AND REAL
PROBLEMS . . . . . . . . . . . . . . . . . . . . 81

SELF-ASSESSMENT QUESTIONS 1. What are the major differences between extracorpore~l cir-
cuits for cardiac surgery and those for prolonged support? 2. What is the major factor controlling oxygen transfer in mem-
brane lungs? 3. What is the "rated flow" of a membrane lung? 4. What is the l imited factor in CO 2 transfer in membrane
lungs? 5. What factors determine the maximum flow rate in extra-
corporeal circuits? 6. Why is venoarterial preferable to venovenous bypass for
prolonged cardiopulmonary support? 7. What causes the metabolic acidoses which some investigators
associate with nonpulsatile flow? 8. What are the common malfunctions of membrane lungs and
how is gas exchange affected? 9. What causes thrombocytopenia during extracorporeal mem-
brane oxygenator support (ECMO)? 10. What changes occur in fibrinogen and other clotting factors
during ECMO? 11. Which routes of vascular access are best for adults? For
children and infants? 12. What is the incidence of bleeding, septic, and mechanical
complications of E CMO? 13. What are the indications for ECMO in adult respiratory
failure? In newborn respiratory failure? In cardiac failure? 14. What are the results and the most common causes of failure
in ECMO treatment of adult respiratory fai lure? 15. What are the results and the most common causes of failure
during ECMO treatment of newborn respiratory failure? 16. What types of cardiac failure are appropriately treated with
ECMO?
Answers on Pages Shown Below
1. pp. 8 - 1 0 2. pp. 8 - 1 0 3. pp. 1 0 - 1 1 4. pp. 1 1 - 1 5 5. pp. 2 1 - 2 2 6. pp. 2 3 - 2 6
7. pp. 2 9 - 3 O 8. pp. 3 1 - 3 6 9. pp. 3 7 - 3 9
10. pp. 4 2 - 4 3 11. pp. 4 9 - 5 0 12. pp. 6 0 - 6 1
13. pp. 6 6 - 6 8 , 7 4 - 7 5 , 77
14. pp. 6 1 - 6 2 15. p. 72 16. pp. 7 5 - 7 8
3

is Professor of Surgery and Director of the University of California, Irvine, Burn Center. He received his M.D. from the University of Michigan Medical School and trained in general and thoracic surgery at Peter Bent Brigham Hospital and Children's Hospital, Boston. Dr! Bartlett practices and teaches general and thoracic sur- gery, with particular emphasis on trauma, pulmonary and metabolic disorders. His research activities include pulmonary physiology, artificial organs, metabolism and burns.
is Professor of Surgery and Director of the Intensive Care Unit at the University of California, Irvine. He received his M.D. from Harvard Medical School. He trained in general and thoracic surgery at Peter Bent Brigham Hospital and Children's Hospital, Boston. Dr. Gazzaniga practices and teaches general and thoracic surgery, with particular emphasis on congenital heart disease. His research activities include cardiovascular physiology, shock, nutrition and emergency and critical care.
In the 6 years since the first successful clinical application of prolonged extracorporeal circulation for cardiopulmonary sup- port, 14" the technique has been carried out in at least 290 other patients with 39 more survivors. The purpose of this monograph is to review the background and physiologic principles of ex- tracorporeal circulation, the modifications tha t have extended its use from a period of hours to weeks and the clinical applica- tion and potential future uses of this technique.
HISTORY OF EXTRACORPOREAL CIRCULATION
If necessity is the mother of invention, cardiac disease must be considered the mother of extracorporeal circulation (ECC). The father is John Gibbon, 11~ with the assistance of Gross, Harken, Murray and McLean before conception, and Kirklin, Lillehi, Sals- bury and many others during delivery. As cardiac surgery de-
4

veloped, it became apparent that Gibbon's heart-lung machine could sustain life during 1 - 2 hours for an intracardiac repair but f a i l e d - i n fact, became itself l e t h a l - b e y o n d that time. Lee et al. 's8 and Dobell et al., 77 among others, identified the gas ex- change device Coxygenator") as the cause of this limitation. It was postulated that if a gas-permeable membrane could~l~e sub- st i tuted for the blood-gas interface, the length of use of ECC could be extended to hours or days. Use of the biologic lung as the oxy- genator for ECC was reported by Lillehi, '93 using cross-circula- tion; Drew, using the in situ lung, and Mustard, 2'3 using excised animal lungs. The unwieldy circuitry and complications of these approaches st imulated artificial lung development.
OXYGENATOR DEVELOPMENT.--Kolff observed oxygenation of blood through the membrane of his early dialyzers, '7~ and report- ed gas exchange experiments with a modified artificial kidney in 1955. '7' In 1956, Clowes and co-authors 5s designed, built, tested and used clinically the first membrane oxygenator. This device used polyethylene and Teflon membranes, which had poor gas transfer efficiency and required large surface areas. The cumber- some nature of the device precluded general use, but the experi- ments did show that construction and use of a membrane oxygen- ator was feasible. At the same time successful application of filming oxygenators G3' ,~0, ,63 for cardiac surgery led to general acceptance and usage of those simpler devices. The bubble oxy- genator, a concept described in 1966 by DeWall, TM is now used al- most universally in the operating room.
In 1957, Kammermeyer '6~ reported the unique gas transfer characteristics of a polymer of dimethylsiloxane, which came to be known as silicone "rubber." Silicone polymer membranes were evaluated in blood-gas exchanges by Thomas 2s~ and Marx. 'gs In the 1960s Kolobow, 'n Crystal, 6" Bramson, 44 Peirce, 2"s Land6 '83 and others 6T, ,G._,,3o4 designed and built membrane oxygenators that utilized silicone rubber membrane. These devices had more efficient gas exchange than the oxygenator buil t by Clowes and permitted more extensive study of prolonged ECC. Oxygen diffu- sion through blood was the limiting factor in performance of these devices, in contrast to the Teflon device. Several investiga- tors tried improving performance "by flow-induced secondary flows,~2, 294 pulsing the membrane ~4 or externally induced second- ary flows, s6, ,54
HEMATOLOGY~ ANTICOAGULATION AND BLOOD-SURFACE INTER- ACTION.- While Gerbode, Hill, Osborn and Bramson ''6 undertook extensive clinical use of membrane oxygenators for cardiac sur- gery, Galletti, '~ Peircep "9 Kolobow '73 and others 9, 4s, ,84, 23., began extending the time limit of ECC from hours to days in the labora- tory. With the closed system made possible by membrane lungs, the hemodynamics were stable and easy to regulate. It soon be-
5

came apparent that normal animals could be maintained on ECC for more than 24 hours. The major problems were technical or mechanical, with oxygenators leaking and pumps breaking, or were related to coagulation, anticoagulation or platelet loss. Thus, research in hematology, coagulation and blood-syrface in- teraction became an essential part of ECC research. "
At the turn of the century, organ perfusion studies were being done with "whipped" or defibrinated blood. In 1916, anticoagu- lant activity was found in an extract of liver tissue by McLean, a medical student working in the laboratory of Howell. TM Since this material originated in the liver, it was named "heparin." This discovery of a biologic anticoagulant with dose-related activity, that could be reversed at will opened the door to the entire field of artificial organ development and all types of extracorporeal circu- lation. Heparin was used in the laboratory, in Gibbon's experi- ments, for example, but was first used clinically in 1938 in Toron- to by Gordon Murray 2~2 in the treatment of a patient with thromo bophlebitis and pulmonary embolism. Thus, both heparin anti- coagulation and extracorporeal circulation for cardiac surgery were ready for clinical trials in 1950.
Experience with ECC for cardiac surgery showed that total heparinization (infinitely long clotting time) could be carried out for 1 -2 hours and reversed with protamine. During this time, blood in the operative field could be aspirated and returned to the circuit ("coronary suction"). The procedure was always associated with thrombocytopenia, which became more pronounced with time. Ganz and Lillehi m, H2 reported the most definitive series of studies on coagulation and platelet loss during ECC in the early years of development. With membrane oxygenators, the effects of blood exposure to large foreign surfaces could be more carefully defined and quantitated. Fundamental studies-identifying the exact steps in blood-surface contact gained momentum in the ear- ly 70s, ~s7 and this is currently an area of intense research.
APPLIED PHYSIOLOGY. -- Much of the development and applica- tion of life-support systems has depended on advances in applied cardiac and pulmonary physiology. The simple experiments and perceptive observations of Starling in the 1890s have long been appreciated, but are only now reaching major clinical applica- tion.~O2, 277 Measurement of cardiac output, ventricular filling pressures, peripheral resistance and colloid osmotic pressure have only recently become commonplace bedside tools. Between Starling and Swan lie the important contributions of Forssmann; of Cournand and Richards in developing cardiac catheterization; of Dexter in demonstrating the concept of pulmonary wedge pressure; 75 of Gross, Crafoord, Gibbon, Lillehi and others of the first generation of cardiac surgeons who demonstrated that car- diac defects should be repaired, ~7 making precise diagnosis desir- able; of Stewart and Hamilton, '29 who developed dye curve analy-
6

sis for human blood flow measurement , and of Kirklin 16s and many others who brought laboratory cardiac physiology to the bedside. Basic demonstrations of the mechanism of gas transport in blood by Singer, Hastings, Roughton and others 273 depended on the methods for measuring gases in blood developed earlier by Van Slyke and Neill3 sG Widespread use of blood gas measure- ment was made possible by Clark, 5c' who developed the polaro- graphic electrode for oxygen and Severinghaus, 26~ who modified a pH electrode measurement of Pco.,. Measurement of gases in blood and an understanding of gas t ransport made development of gas exchange devices possible, and rational planning of new devices could be carried out on the understanding developed by these investigators.
Similarly, with these measurements, severe pulmonary insuffi- cieney could be quantitated, which led to identification, classifica- tion and intelligent management. Mechanical ventilation was conceived and used by Sauerbruch to carry out thoracic surgery in Germany in the early 1900s, but was not applied to manage- ment of respiratory failure until the design and construction of the Drinker "iron lung. ''ss The next logical step was positive- pressure ventilation for pulmonary insufficiency. This procedure had been used for anesthesia for several years, and the develop- ment of reliable ventilators by Engstrom, Emerson and others brought the ventilator to the intensive care unit. The major con- tributions of industry should be emphasized at this point. The general availability of reliable blood-gas machines, ventilators of several types and transducers, amplifiers, oscilloscopes and flow- directed catheters set the stage for a sophisticated level of inten- sive care that demanded education or re-education in basic phys- iology. In the decade of the 60s these measurements became available to every physician, and in the 70s it is considered mal- practice to ignore these advances.
With the use of ventilators, measurement of blood gases and reliable methods of t rea tment for renal failure, pulmonary insuf- ficiency was seen to be a major cause of morbidity and mortal i ty
250 in critically ill patients. " Premature infants were now success- fully delivered and resuscitated. Pulmonary insufficiency in these infants, whether from lung immaturi ty, pulmonary vascular abnormal!ty, pulmonary parenchymal abnormali ty or "hyaline membrane disease," came to be called the "respiratory distress syndrome" (RDS) of infancy. In the mid-60s infant RDS was lethal in 50% of cases, but considered curable if the patient could be sus- tained over a period of days. Infant RDS, therefore, was a major impetus to laboratory development of the membrane oxygenator and ECC support systems. Although prevention and t rea tment of RDS have improved survival results, 12,000 newborn infants still die of this lesion each year in the United States3 zG
Likewise, respiratory distress syndromes in adults were recog- nized and characterized. Unlike the infant syndrome, adult RDS
7

is characterized by pulmonary capillary leakage and atelectasis, resulting in poor compliance, high pulmonary vascular resistance and transpulmonary shunting. This syndrome has been called adult RDS, post-traumatic pulmonary insufficiency, congestive atelectasis, shock lung and a variety of other termsY ~4 Similar pathophysiology is seen in severe pneumonitis, drowning, smoke inhalation, aspiration and many other conditions causing lung failure. Recognition and treatment of these syndromes on a phys- iologic basis and attempts to define mortality specifically during the course of abnormal conditions represent the current state of the art. Approximately 40,000 adults die of acute pulmonary failure each year in the United States. 2~ Extracorporeal mem- brane oxygenation (ECMO) is the ultimate life-support systerh for patients with this syndrome.
With the measurement of cardiovascular function came the opportunity to study abnormal hemodynamics, notably the shock state. Rigorous experiments provided a model and a basic under- standing of hemorrhagic shock. Blalock demonstrated that shock after trauma was related to hypovolemia and not to a mysterious toxin. Lillehi's classic epinephrine-tolerant dog experiments demonstrated the importance of deleterious endogenous respons- es to shock and were the background for the current emphasis on end-organ response. 76 Pharmacologic assistance for cardiogenic shock had only minor effects on mortality from severe forms of this syndrome.
Mechanical assistance to the circulation originated .with the studies of Dennis, TM using left heart bypass. Ventricular assist devices have been studied extensively in the laboratory 33 but rarely used clinically. Venoarterial bypass with or without an oxygenator has only recently been studied in cardiog~enic shock. The concept of counterpulsation to assist the failing heart was originally described by Harken in 1958. T M The invasive nature of this technique precluded general usage until it was reintroduced in the form of intra-aortic balloon zounterpulsation by Kantrow- itz. ~6~ Counterpulsation is now widely practiced for management of cardiogenic shock. The use of extracorporeal circulation in shock, perhaps in combination with counterpulsation, is ready for laboratory and clinical study.
Galletti and Brecher's monograph on extracorporeal circula- tion (1962) is the classic reference2 ~ The subject has been re- viewed by Neville, 22~ Peirce 23' and Allen. 2 The current standard text edited by Ionescu and Wooler ~Ss emphasizes application of ECC in cardiac surgery. Devices and techniques for prolonged ECC were reviewed in symposia edited by Bartlett, Drinker and Galletti (1971) .0 and Peirce (1973). 23a The proceedings of a 1975 Copenhagen conference on membrane lung technology and appli- cation were recently published, edited by Zapol and Qvist (1976) 3~ and Dawids and Engell (1976). 6~
8

ARTIFICIAL ORGANS
Researchers in artificial organ development are fond of quoting Shakespeare 's observation: "Diseases desperate grown by desper- ate appliance are relieved, or not at all" (Hamlet). Tojremove venous blood from the body, render the blood incoag~lable, re- move CO s , add 0 2 and re turn it to the arterial system for days or weeks at a time may indeed seem not only desperate but unrea- sonable. Yet the technique is not only possible but successful. In this section we will examine the anatomy and physiology of the mechanical substi tutes for heart, lung, endothelium and other internal organs.
LUNGS
Devices that convert venous to arterial blood are generally re- ferred to as oxygenators, although "artificial lungs" or "respira- tors" would be bet ter descriptions. Oxygen is added, and carbon dioxide is removed in approximately equal quanti t ies by exposing the flowing blood to a gas (or liquid) with a high Po 2 and a low Pco 2. Prototype blood-liquid oxygenators have been developed that use silicone oil or fluorocarbon as the high oxygen equilibrat- ing material, 197, 538 but these devices are still in the developmen- tal phase. Consequently, the artificial lungs currently used in prolonged ECC are all membrane gas exchange devices. Al- though the artificial lung is only one component of the extracor- poreal circuit, it is probably the most important one; consequent- ly, the entire procedure has come to be known as membrane: lung support or extracorporeal membrane oxygenation, spawning the acronym ECMO.
Blood-Gas Interfaces The particulate elements of blood are certainly damaged, or at
least sensitized to mechanical damage, by direct gas exposure. Damage to serum proteins (denaturation, conversion to toxic pep- tides or both) was demonstrated by Lee 18s and Dobell. 77 Lung damage was demonstrated by Zotti et al. 3~ and others. Because of these studies, the blood-gas interface has been much maligned; the reason for these alterations may lie not so much in the nature of the interface as in the amount of exposure. In membrane artifi- cial lungs, the same 15 sq m of foreign surface is repeatedly ex- posed to blood flow. After the initial circulation, the blood ~'sees" no "new" surface as long as the procedure is carried out. With a bubble oxygenator, the blood sees approximately 15 sq m of solid foreign surface in the form of the casing, heat exchanger, filters and defoamers, and an additional 1 0 - 2 0 sq m/minute of raw gas interface. There is abundant evidence that even the most abnor- mal foreign surface becomes "pacified" after a brief exposure to blood. In this process, blood proteins are adsorbed on the foreign
9

surfaces so that subsequent blood sees a protein-liquid interface ra ther than the foreign material. The major changes in particu- late material and proteins occur with exposure to new (un- pacified) surfaces, a phenomenon that is found repeatedly only in the gas-interface devices. Fur ther evidence suppgrting this hypothesis comes from hematologic studies of prol~hged blood exposure to microporous membranes, where a direct gas interface exists but is not renewed continuously. Hematologic changes seen with microporous membrane devices are the same as those occurring in conventional membrane l u n g s - n o t gas-interface oxygenators.17, 2~
Membrane Oxygenators All membrane oxygenators have in common the characteristics
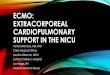
shown in Figure 1. Blood enters the device and is distributed through a header or manifold system to the gas exchange area. As blood flows past the membrane, 02 diffuses into the blood be- cause o f the pressure grad ien t (or driving force) between the 100% O., in the ventilating "gas and the O 2 pressure in venous blood (approximately 700 mm Hg). At the same time CO 2 diffuses
Fig 1 . - P r i n c i p l e s of gas t ransfer in a membrane oxygena to r . The expanded v iew shows in teract ions across the gas exchange membrane. Venous b lood enters f rom the left and becomes ar ter ia l ized as 02 d i f fuses th rough the mem- brane and the b lood f i lm, and CO 2 d i f fuses f rom the b lood f i lm across the mem- brane into the gas phase. In this examp le the ba romet r i c pressure is 765; Po 2 is 760 mm Hg in the vent i la t ing gas, and P c o 2 is 5 mm Hg, resul t ing f rom the passage of CO 2 f rom the b lood to the gas phase.
I I" T o t a l V o l u m e , I
I . Cos--- . - I I I Exchange I I I Volume I I
:::::: : : : : : : : : : : : : : : : :~:i:i:i:i;:.:h~ o o o o o q o o o o T o o o
~eno~ :::::: ? ~. .~. ~ I ~ L ~ ~ ~ ~ ~. L . B o : . - -: : . . . . : . . Blood I od ................ uxycjena,ea
::::::::::::::::~i! ti~i~i~:~:i:!:!:::l:::~-,, o c Blood �9 " ........ """"""i~!~ .......... '"""""."T::-~. o o c p 0 2 40 i : i : !pC02 4 5 ~:~:~!~.,~
10

out, responding to the pressure gradient between the Pco 2 of ve- nous blood and the ventilating gas (approximately 40 mm Hg). Although the pressure gradient for gas transfer is much greater for 02 than CO2, the rate of diffusion through the blood and the membrane per mm Hg gradient is much greater for CO 2. There- fore, the diffusion of both 02 and CO 2 through the membrffne and through the flowing blood film must be taken into consideration when studying membrane oxygenator performance.
OXYGEN TRANSFER.--The rate of 02 diffusion through a film of venous blood is the limiting factor in performance of almost all oxygenators. The rate of diffusion through the silicone polymer membrane used in most devices is 1,210 ml OJsq m of mem- brane/minute/mil membrane thickness (at a gradient of 760 mm Hg). Commercially used membranes are 3 - 6 mils* thick, so that most devices have a potential 02 transfer of 200-400 ml/sq m/minute. However, the rate of diffusion through a film of venous blood is approximately 100 ml OJsq m/minute/100 ~ thickness (at 72{J mm Hg gradient). It is difficult to build a device with blood film thickness less than 200 t~ across; hence the full potential of 02 transfer of the membrane is never reached.
These phenomena are shown in Figure 1. Oxygen diffuses read- ily through the membrane from point A to point B, then slowly through the blood film to the center. As blood enters the gas ex- change chamber, the red cells nearest the membrane become sat- urated with 02, the Po 2 in the surrounding plasma goes up and O., diffuses deeper into the blood film, saturating more red cells, with an advancing front of saturated blood that progresses further into the blood film with time. The longer the blood film is in the gas exchange area, the more complete the saturation of hemoglobin with 02. A definite period of time is required for full oxygenation. If the blood flows through faster than that t ime, incompletely saturated blood will leave the device. This situation is further complicated by the fact that the pattern of blood flow within the gas exchange film is laminar. Blood cells in the center of the film travel faster than those at the edges. This has the effect of mak- ing the exposure time for flowing blood relatively shorter than the exposure time of an equivalent amount of blood in a static film. Anything that can be done to interrupt the laminar flow pat- tern will improve the efficiency of 02 transfer performance.
Actual 02 delivery through the artificial lung (or the biologic lung, for that matter) is limited by the 02 carrying capacity of blood. Each gram of hemoglobin has the capability to bind 1.39 ml 02. (Some 02 is also dissolved in the plasma, but the amount is so small that it can be discounted for this discussion.) Oxygen is extracted from blood in the peripheral tissues, the actual amount ranging from 3 -7 ml O2/100 ml blood flow. Approximately one quarter of the 02 bound to hemoglobin is removed in this tissue
*1 m i l = . 0 0 1 i n . = 0 . 0 2 5 m m = 2 5 / 1 .
11

300. Z~ A - V . . , /
5 0 , ~ 3 v a " / ' / /
i ~, ~ ,~ ~, Blood flow L/ra in
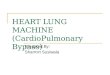
Fig 2.--The amount of 02 that can be delivered is directly related to the blood flow. Representative values are shown for fully saturated blood at temperature 37 C and pH 7.4. Values for a normal arterial-venous difference (5 vol %) are shown, along with high and low extremes of oxygen utilization. (Figs 2 -4 from Bartlett, R. H., and Gazzaniga, A. B.: In Ionescu, M., and Wooler, C. [eds.]: Current Techniques in Extracorporea/ Circulation [London: Butterworth & Co., Ltd., 1976]. Used by permission.)
respiration process, so that the hemoglobin in venous blood is approximately 75% saturated with 02. As this venous blood tray- els through the lung, the maximal amount of 02 it can pick up per minute is a product of the total hemoglobin times 25% (unsaturated fraction) times 1.39 (ml OJgm hemoglobin) times the flow rate. These relationships are shown in Figure 2, in which the maximal amount of 02 delivery is related to flow, carrying out the calculation outlined above for arteriovenous differences of 3, 5 and 7 vol %. The geometry and fluid'mechanics of any artificial lung determine how much venous blood can be saturated with 02 during the residence time in the device. When venous blood is perfused very slowly through the device, the out- let blood will be fully saturated, and the actual 02 delivery is de- termined by the flow rate, as shown in Figure 2. As the flow rate is increased, 02 transfer is proportionately increased, until the 02 transfer limitation imposed by blood thickness is reached for that specific device. From that point on, increased flow results in de- saturated blood leaving the arterial side of the oxygenator. This phenomenon is diagramed in Figure 3. The flow rate at which normal venous blood perfusate leaves the oxygenator at 95% ar- terial saturation has been referred to as the "rated flow" by Gal- letti, l~ The rated flow for any artificial lung can be specifically measured (Fig 4). This is an extremely valuable concept for de-
12

I00-
7s~
Hb 50 % satur-
ation
Outlet (arterial) saturation
Ihlet (venous) saturation
Flow L/rain
200 / Maximum 02 delivery---7/ for Z~ A-V 5vol.% /
/ /
150.
Oz I00' / / Ozdelivery
Delivery / cc/min
5@
Flow L/min
Rated Flow �9 3 L / r a i n
Fig 3.--The concept of rated flow. In the left graph the oxyhemoglobin sat- uration of blood leaving an oxygenator is shown during perfusion with venous blood (60% saturated). Outlet blood is fully saturated at lower flows, until a limitation caused by the device geometry is reached (3 L/minute at an arterio- venous [AV] difference of 5 vol % in this example). In the right graph the actual 02 delivery in this system is shown. Oxygen delivery increases in direct propor- tion to blood flow until the critical limitation is reached. The flow at which the outlet blood is 95% saturated is called, the rated f low--3 L/minute in this ex- ample.
sign and development of membrane oxygenators, for evaluat ing membrane oxygenator function with changes due to time, coagu- lation, etc. and in designing ECMO circuits for clinical use.
The complex interrelationship of the advancing front of satu- rated hemoglobin with laminar or turbulent flow patterns can be modeled and analyzed to assist in the design of devices with opti- mal characteristics2 ~ 2~4 Device testing can be done with blood, but prototypes are more easily tested by CO., diffusion into water,
Fig 4 . - Rated flow for some representative membrane oxygenators.
200- / Sci-Med. (Kolobow) 3.5 m 2
Bramson 5.6 m z membrane Oz 150-
Delivery cclmin
Peirce 2rn 2 membrane I00- / Lande' Edwards 3m z membrane /
/ / Travenol .75m z membrane 5O-
Blood flow L/min
13

Membrane Oxy.genators: Ty.pical Designs
~e
I. Norrow blood film, shorl channels
�9 IOmmHa ~ 20OOml 5Occ/m z Good
2. Wider spoces, longer chQnnel$
~'---~" I 0 0 I 0 0 0 60cc /m z Best
& Flow-induced rn~xing
50 IOOO 15OccJm 2 Good
4 E~ternolly- induced mixing
/ . ~ SO 5 0 0 50Occ/rnZ Fair
Fig &--Typical designs and characteristics of membrane lungs. Representa- tive values for large units at a flow of 5 L/minute are shown. Choice of a mem- brane lung type depends on the clinical application. For example, type 1 has the lowest perfusion pressure, type 4 has the lowest priming volume, and so on.
which has been shown to be" a reasonable analogy to blood/O 2 transfer2O, 25~
By means of a combination of theoretical analysis and simple experimentation, many types of membrane oxygenators have been constructed. A few types are available commercially. The limiting factor is 0 2 diffusion through plasma, as outlined above; much of oxygenator design has been aimed at minimizing this. The various approaches to this problem, and the relative advan- tages and disadvantages, are shown in Figure 5. Fo r example, the short, narrow channel design is the best to achieve a l o w perfu- sion pressure, but the worst in 0 2 transfer because the residence time of blood in the "capillaries" is short. A device with short, narrow gas exchange channels is the most analogous to the nor- mal lung. The membranes can be spaced as close as physically possible because the total cross-sectional area of the short mem- brane channels is greater than the inlet or outlet manifold. Con- sequently, the resistance to blood flow through such a device is minimal. The priming volume is quite high relative to other de- vices, and the 0 2 transfer/sq m of membrane is low. Safety and ease of use rate high. As with any membrane lung, part icularly careful attention must be paid to removing all the bubbles during priming. The Land~-Edwards oxygenator is an example of this type.
Considerably greater 0 2 transfer/unit of surface area can be achieved by making the blood channel longer and increasing the residence time, at the expense of a higher perfusion pressure.
14

Safety and ease of use a rebo th excellent. Examples of this type of oxygenator are the Kolobow/Sci-Med oxygenator, 172 the General Electric (Peirce) lung 229 and the Dow Corning capillary oxygena- tor.~G4
The induction of secondary flow by planned obstruction~ in the blood path (type 3 in Figure 5) improves 0 2 transfer by ~Hnging deoxygenated blood from the center of the blood film to the mem- brane surface, and vice versa. Laminar flow is inherently stable and difficult to disrupt, so that even major obstructions to blood flow (such as a screen in the blood path) yield only moderate im- provement of 0 2 transfer for a given surface area. Since the inten- sity of the secondary flow increases with the through-flow rate, mixing is greater at higher flow rates. This circumstance may be desirable in matching 0., transfer to blood flow rate, but may also result in inefficiency of oxygenation at low flow rates. Secondary flow can also be generated by modifying the blood path itself. For example, coiling capillaries in toa curved configuration generates secondary flows that can double 0 2 transfer/94 Most membrane oxygenators rely on some type of.flow-induced mixing to improve efficiency. The Travenol Silicone rubber ~s and Travenol micropo- rous membrane oxygenators:and the Bramson oxygenator 1~3 are examples of this type.
To approach complete mixin~ of the blood, some type of exter- nal mechanical force must be applied. Ear.Iy experiments on in- duced secondary flow by Illickal et al.l~ 4 and Drinker et al/~ dem- onstrated the feasibility of this approach and led to successful application in design of the toroidal membrane oxygenator of Drinker and Bart le t t / , J2. 203.2,0 and.the spinning disk membrane oxygenator studied by Hill et al. ~49, .,72 DorsonS2 and Bellhouse -~7, 21:J have used the mechanical force of pulsatile blood flow to gener- ate vortex shedding. Devices that rely on externally induced secondary flows have the highest 0 2 transfer and the lowest priming volume and residence time. These devices are easy to use, prime and debubble, but are larger and more cumbersome than the simpler designs and rely on an external power source.
The existing membrane oxygenators listed above can be and have been used successfully for prolonged cardiopulmonary sup- port. However, the ideal artificial lung has yet to be designed. The next generation of membrane oxygenators, currently in labo- ratory testing, will include wide blood channels for low flow re- sistance, flow-induced mixing for 0 2 efficiency and microporous membranes for improving CO~_ transfer. The interested reader is referred to excellent reviews of engineering and oxygenator de- sign by Drinker, s7 Colton 59 and Dorson. ~
CARBON DIOXIDE T R A N S F E R . - - C a r b o n dioxide is much more diffusible through plasma than oxygen, so CO 2 transfer is limited by the transfer rate through the membrane in most oxygenators. The rate of CO~ transfer through silicone polymer membrane is 6 t imes greater than that of O 2 for equivalent membrane thickness
15

and pressure gradient. However, the pressure gradient for CO 2 transfer can never be greater than the difference between the Pco,, of the venous blood and zero (usually 4 5 - 50 mm Hg). With this pressure gradient and the usual membrane thickness of 3 - 6 mils, CO 2 transfer limitation is approximately 200 ml/minute/sq m for most devices. This is much more than the 02 tran~'~er as out- lined above for all except the induced mixing type of gas ex- change devices. Hence, CO 2 transfer will always be more than 02 transfer for most devices. In fact, it is usual ly necessary to use a CO2-enriched mixture (2.5-5%) for ventilating the oxygenator to prevent hypocapnia and respiratory alkalosis. Total performance of highly efficient, thorough mixing oxygenators is limited by CO 2 . t ransfer when silicone membranes are used, or by 02 transfer if' microporous membranes are used.
Because CO~ transfer is relatively independent of blood flow rate but very dependent on surface area exposed, any malfunc- tion that diminishes overall surface area exposure will affect CO 2 transfer before other oxygenator functions. Therefore, CO 2 transfer (for a known value of blood Pco 2) is a very sensitive mea- sure of loss of functioning membrane surface area in the device. This is discussed in the section on physiology and pathophysiolo- gy of membrane lungs.
WATER VAPOR TRANSFER.--Water vapor at a temperature of 37 C passes through silicone polymer membranes at a rate corre- sponding to 5 - 7 ml liquid water/sq m of 4-mil membrane/hour. This water loss has two important consequences. (1) The patient on prolonged support may lose 2 - 3 L of sodium-free water/day through the oxygenator, resulting in progressive hypel:natre- mia with increased osmolarity. (2) The water vapor that leaves the blood at 37 C condenses and may fill compartments in the cooler gas phase, blocking ventilation and resulting in areas of decreased gas exchange. Water transfer is much greater with a microporous than a solid silicone polymer membrane; hence these probIems are compounded when microporous membranes are used.l~, x~7 The gradient for water transfer can be decreased by humidifying the venti lat ing gas, and the dew effect can be min- imized by warming the venti lat ing gas. Both of these methods are somewhat cumbersome and inefficient. The problem of water loss and clearance is most easily handled by using a high venti lat ing gas flow and designing the gas phase so that accumulated water will run out easily by gravity.
The theoretical concepts outlined above must be incorporated into designs that are practical and economical to build and safe to use. Some of these are shown in Figures 6 and 7.
PUMPS
Substi tut ing for the hear t has proved to be the easiest task in prolonged ECC. Simple roller pumps are almost universally used
16

~ E ~ R A . E | ~ t
A
C D Fig 6.-Representative membrane artificial lungs. The Land~-Edwards oxy-
genator (A and B) has short, wide blood channels. The Sci-Med-Kolobow oxy- genator (C and D) has long, narrow blood channels, as blood finds its way be- tween the wrappings of the gas-carrying envelope. Of the devices shown in Figures 6 and 7, only the Sci-Med unit is currently available commercially.
because of reliability, simplicity and ease of operation. In the roll- er pump, the blood-conducting tubing is held in a raceway and rollers compress the tubing, forcing the fluid forward and creat- ing suction upstream from the pump. The tubing in the pump can be the conduit tubing for the system or a specially designed pump chamber. The occlusiveness on the rollers on the tubing has been the subject of much investigation. Totally occlusive rollers may cause increased hemolysis if the red cells have been conditioned by air exposure. Elaborate methods have been established to
17

.I
A
("
, b '
,, . ~
D Fig 7.-Representative membrane artificial lungs. The Peirce-General Elec-
tric membrane lung (A and B) had small inlet blood manifolds and long, wide blood paths, which predispose to thrombosis. The Branson-Cutter (C and D) includes water mattresses to be used for heat exchange. Screens are used to create mixing in the blood phase in this device and in those manufactured by Travenol and Rhone-Poulenc.
make the pump almost occlusive (for example, a column of water 1 m high drops 10 cm/minute when held by the pump roller). This type of precision setting, requires that the tubing be exactly uniform throughout the raceway. Pumping chambers with rein- forced uniform walls have been described. For cardiac surgery these considerations may be important because of the extensive exposure of red cells to air. For prolonged ECMO support, hemo- lysis is not a significant problem, even with occlusive pumps.
Tubing subjected to continuous pumping will eventually crack, crumble or break. Polyvinyl chloride (PVC) tubing as used in most conventional bypass circuits will deform into an elliptic shape and crack along the edges after 2 4 - 72 hours of pumping in a roller pump. These cracks begin along the outside and are usu- ally visible. Therefore, PVC tubing in the raceway should be changed every 24 hours to avoid rupture. Silicone rubber tubing has a somewhat longer life in a roller pump. However, some types of this material tend to deteriorate by cracking and breaking off small particles on the inside of the tubing, which may form par-
18

t iculate emboli. Tubing deterioration is not obvious until rupture occurs. For this reason, we do not use silicone rubber tubing in the roller pu~np. A specially designed pump boot described by Kolobow and Zapol ~4 is made of polyurethane reinforced with fiberglass. This pumping chamber can be cleaned and reused and has an extremely long lifetime. Plain polyurethane tubing (Tygothane) has a similar life-span, showing no deformation dur- ing in vitro testing of up to 2 weeks.
During ECC for cardiac surgery, pump speed is controlled di- rectly by watching the level in the open reservoir and partially occluding the venous line to diminish flow. During prolonged ECC this type of minute-to-minute regulation is impractical. Some type of automatic pump regulation must be buil t into the circuit so that the flow can be maintained for weeks without con- tinuous technician attention. This may be accomplished in two ways: (1) by draining all the venous blood into a very small reser- voir or directly into the roller pump and limiting the ECC flow by the pump setting, or (2) by designing a Starling-type pump that pumps all the blood delivered to it and regulating the flow by par- tially clamping the venous line. Both types of systems are practi- cal and have been used in the laboratory and clinically.
In the simplest type of servoregulated roller pump, venous blood drains through a small compliant chamber that is distend- ed with venous blood. Whenever the pump speed exceeds the ve- nous return, the chamber collapses, opening a microswitch and turning off the pump. If the desired ECC flow cannot be main- rained because of venous catheter size, kinking or hypovolemia, the pump turns off and starts again when the chamber is distend- ed. An alarm is sounded when the pump turns off, and the techni- cian can rectify the problem. This system can be modified with modulating electronics so that the pump flow gradually speeds up as the chamber fills, reaching a maximum flow level and holding stable flow at that point. With this type of system, the desired ECC flow is set on the roller pump and maintained automatically. If hypovolemia or interruption to venous re turn occurs, the pump will deliver the maximum possible flow rate short of the desired level tha t has been preset. This lower flow is indicated by an alarm on the flowmeter, and appropriate steps are taken to cor- rect the problem. Most teams experienced with clinical ECMO use a roller pump with a reservoir and a level sensor similar to that described above.
In a t rue Starling-type pump the pumping chamber is normally collapsed and fills to a certain volume, dependent only on the in- flow. Hence, all the inflow blood will be pumped through the sys- tem, and a maximum flow rate is established e i ther by sett ing a ceiling on pump flow (assuming the pumping chamber to be com- pletely distended), or by partially occluding the venous re turn line. The pumping chamber may be squeezed intermit tently with flow regulation by valves, resulting in a pulsatile flow contour, 4, 49
19

or it may be continuously compressed as in a roller pump with a collapsible tubing pumping chamber. 5'-' Impeller Starling-princi- ple pumps have been described for extracorporeal circula- tion.3G, 243 A central rotor is driven by an external power source. Impeller pumps cause minimal damage to blood elements and cannot pump air. Starling-type pumps have the aff~antage of t ight servoregulation of the flow without complicated electronics. The only disadvantages are pulsatile flow in some ventricle pumps and tubing wear of the collapsible segment in roller pumps. Pulsatile flow is undesirable where a fairly high resis- tance occurs at the arterial inflow cannula, causing very high pressures in the circuit during the systolic pulse phase and possi.-
�9 �9 �9
ble je t effects at the end of the the perfuslon cannula. Thin proIJ- lem can be solved with use of a compliant depulsator in the cir- cuit. Ult imately most circuits will probably include a Starling- type roller or ventricle pump because of simplicity of prolonged use. Ei ther electromagnetic or ultrasonic flowmeters are suitable for prolonged ECC.
Some ECC circuit designs integrate the membrane oxygenator and pump into a single unit. For example, the original Bellhouse- Oxford oxygenator gained efficiency from secondary flows in- duced by a reciprocating through-flow pat tern with "two steps forward and one step back," hence requiring a double pump sys- tem for efficiency of blood oxygenation. 27 The Travenol Teflon microporous membrane oxygenator requires careful control of the blood outlet pressure for maximum efficiency so that both an ar- terial and venous reservoir and arterial and venous pumps are required for proper operation.'7, 2,,
Several investigators have combined the oxygenator and pump mechanism into a single unit. ~, ~5, ,o3, 192 The general principle involves valves in the blood flow lines and pulsed oxygen pressure against the membranes, squeezing the membranes together, oxy- genating the blood and expelling it from the device at the same time. This is a very attractive concept and may form the basis for pump oxygenator circuits of the future. At present, the system is limited; significant shunting of deoxygenated blood may occur during the diastolic phase, the efficiency of oxygenation is related to blood through-flow and, most important, the possibility of gas embolism exists when the gas pressure is higher than the blood pressure during the systolic phase.
The type of membrane oxygenator used will affect the choice of the pump, or at least the design of the circuit�9 The Land6-Ed- wards oxygenator '~3 is the only unit in which the blood-phase pressure drop is low enough to permit use on the venous side of the circuit. The oxygenator is designed to be used in this mode with venous blood draining directly through the oxygenators into a reservoir, and from there pumped back to the patient. This causes a minor limitation to achieving a high flow, and the device can also be used on the arterial side of the circuit. The Sci-Med
20

Kolobow*7~ spiral coil membrane oxygenator has a high blood flow resistance and must be used on the arterial side of the cir- cuit. Usual ly venous blood is perfused through the oxygenator and returned directly to the patient. The Bramson membrane oxygenator 4~ is used in the same fashion with a single pump.
HEAT EXCHANGERS
Because heat is lost in evaporation of water through the mem- brane oxygenator, it is essential to include a heat exchanger in the extracorporeal circuit. Under operating conditions for pro- longed support, this will always function as a blood warmer. The Bramson membrane oxygenator includes water blankets to main- tain temperature. This is the only membrane oxygenator tha t has this capability. Any commercially available heat exchanger is satisfactory for maintaining body temperature. The disposable Travenol "Miniprime" heat exchanger is safe, efficient and dura- ble under a variety of operating pressures and flows. This device is made of silicone rubber and siliconized metal. When mounted upright, it will serve as a t rap for major bubbles, although small bubbles will get through virtually any bubble trap. With the heat exchanger in the circuit, vir tually any temperature can be main- tained.
ARTIFICIAL BLOOD VESSELS AND ENDOTHELIUM
Intravascular catheters to gain access to the bloodstream and tubing to connect the pat ient to the artificial organs are usually made of some type of plastic. Polyvinyl chloride (PVC, Tygon) and silicone polymers (silicone "rubber," Silastic) are the most widely used materials. Polycarbonate, a rigid plastic, or metal are mate- rials commonly used for connectors.
The inner surfaces of the tubing and the surfaces in the pump, heat exchanger and oxygenator form an artificial endothelium. This is the weakest link in our chain of artificial organs and the subject of major research efforts. The state of understanding of blood surface interface effects and approaches to design of a bet ter artificial endothelium are discussed in detail elsewhere.
Even if an ideal prosthetic surface is devised, the anatomy and flow pat terns of prosthetic vessels must be improved. Right-angle turns and s tagnant zones must be eliminated. A simple Luer adaptor built into the side of a polycarbonate connector for blood sampling seems a small and innocuous space but provides ideal breeding ground for thrombus formation, even in heparinized blood. Even worse is a right-angle step-offgoing from a smaller to a larger orifice within the flow pattern. Such a step-offoccurs at both ends of every connector in the circuit. Although the connec- tors are designed to minimize this perpendicular joint, a stagna- tion zone is present wherever this variation in contour existsY G, 4o
21

Despite heparinization, these right-angle corners are gradually filled by fibrin-platelet complexes that are quite adherent and probably do not embolize. However, when blood-compatible sur- faces that do not require heparinization become available, these minor variations in flow pat tern will become the moss thrombo- genic portion of the extracorporeal circuit and will=~have to be eliminated.
The size of the tubing used in the circuit is determined by the flow requirements. Resistance to flow varies proportionate to the length of the tubing and the fourth power of the radius. Conse- quently, the internal diameter of the tubing is a more important consideration in circuit design than length of tubing. This is pa r- t icularly important in selection of venous access catheters, where resistance is the limiting factor for the flow rate. The outside diameter of the catheter is limited by the size of the vein used for blood access. Conventional venous catheters for open-heart sur- gery are thick walled. Thin-walled catheters for extrathoracic cannulation are custom made by each laboratory. They are usu- ally made of polyvinyl or polyurethane, reinforced by wire or fab- ric. Argyle PVC chest tubes have approximately 1 mm wall thick- ness and are suitable for jugular cannulation.
Flow resistance in the arterial access catheter determines the hydrostatic pressure in the extracorporeal circuit. Pressure in- creases with flow rate, so that high flow through long, narrow arterial catheters may lead to tubing or oxygenator rupture or to oxygenator malfunction. Flow rate i tself is limited by arterial line pressure when nonocclusive roller pumps or impeller pumps are used. Hemolysis will occur if the combination of high flow and pressure causes turbulence or jet effects. Consequently, arterial catheters should be of the shortest length and the largest bore possible. When femoral perfusion is used, the catheter should be long enough to reach the aortic arch, 94, 200. 27z hence the length of tubing is a determinant of flow resistance and a thin-walled cath- eter must be used. If carotid or axillary perfusion is used, a conven- tional thick-walled PVC arterial catheter is adequate. The diam- eter of conduit tubing in the circuit is larger than the access cath- eters, and becomes important because of the volume of prime required.
FILTERS--THE ARTIFICIAL RETICULOENDOTHELIAL SYSTEM
During ECC for cardiac surgery gross filtration (200-400 pore size) is always used to remove clots, debris and particles from the aspirated blood Ccoronary suction"). Gross filtration is usual ly used on the perfusion circuit itself; in fact, it is buil t into most oxygenators. Ultrafiltration (40 -50 ~) should be used for coronary suction blood to remove solid platelet-fibrin aggregates and fat particles. Ultrafiltration on the main perfusion line de- creases small particle '~counts" detected by ultrasound monitor-
22

ing, probably by serving as a microbubble trap. 22~ Some loose platelet aggregates (which would ordinarily break up and recir- culate) are also removed by ultrafiltration, resulting in accelerat- ed thrombocytopenia. '17 The trade-off between these effects re- quires further study.
Ultrasound microparticle counts are low or absent when no blood-gas interface is present. The loose platelet aggregates that form during ECMO seem to have no deleterious effects. There- fore, on-line ultrafiltration seems unnecessary and possibly harmful during prolonged ECC.
MONITORING AND SERVOREGULATION-- THE ARTIFICIAL NERVOUS SYSTEM
In taking over gas exchange and blood flow with artificial or- gans, we assume responsibility for regulation that is normally controlled by endogenous neuroendocrine mechanisms. The affer- ent limb of this system is provided by measurements from the patient and the extracorporeal circuit. The efferent limb may be built in (as in the Starling pump), but usually requires an active decision. The more automatic servoregulation that can be done safely, the better, but such systems must be completely reliable.
Monitors must include systemic arterial pressure, pulse con- tour, temperature and arterial and venous blood gas values from the patient and flow rate, temperature and oxygenator blood gas values from the extracorporeal circuit. For safety, it is wise to monitor arterial line pressure in the circuit, and pre- and postox- ygenator pressure if the device function is affected by perfusion pressure. Coagulation is monitored by whole blood activated clot- ting time (hourly), platelet count (daily) and measurement of other coagulation factors. Use of these monitors to regulate the ECMO system will be described in detail later.
PHYSIOLOGY AND PATHOPHYSIOLOGY OF EXTRACORPOREAL CIRCULATION
The term "physiology" was coined by the great Dutch physician Boerhaave to describe the interrelated function of organs under normal conditions. Hence, the physiology of extracorporeal circu- lation describes function of normal and prosthetic organs under conditions of uncomplicated prolonged ECC. This includes hepa- rinization, heart-lung circulatory bypass and the various prosthet- ic surfaces and organs outlined above, and is anything but nor- mal human biology. In mechanical substitution during cardiopul- monary support, alterations and simplifications are made that influence the physiologic response of nonsubstituted organs. For example, the systemic pulse contour is diminished or absent. Physiologic control of the substituted organs is removed, and re- lationship of this to other controls may need pharmacologic alter-
23

ation. For example, endogenous control of perfusion is lost so that dependent functions such as blood volume and systemic vascular resistance may require external regulation. Finally, some aspects of organ substitution impose mandatory abnormal conditions. For example, continuous anticoagulation is required ,with exist- ing devices.
Pathophysiology during extracorporeal circulation is a devia- tion in normal or artificial organs from the expected baseline. The line between physiology and pathophysiology during ECC varies with the type of organ substitution and the state of the art. For example, platelet aggregation and microembolization are consid- ered normal consequences of ECC at the present t ime but may be abnormal as technology improves.
Much of the clinical research on the physiology of ECC has been done by measuring variables during cardiac surgery. Al- though many important observations have been made in this set- ting, the uncontrolled variables of coronary suction, length of procedure, primary patient disease and the personal preferences of the surgeon and perfusionist should always be considered in interpreting these data. We will cite such references, with the caveat that physiologic findings during cardiac operations are similar but not identical to organ function during prolonged ex- tracorporeal support.
METHODS OF EXTRACORPOREAL CIRCULATION
There are four modes of blood drainage and return that might be followed: arteriovenous, venovenous, venoarterial or a combi- nation of these (Fig 8). Arteriovenous shunting through a mem- brane oxygenator is a convenient way to test small oxygenators in large animals and evaluate the effects of prolonged foreign sur- face exposure. No pump is required, and a prolonged stable prepa- ration for evaluating the effects of blood exposure to foreign sur- faces can be achieved. Although it has been used successfully, 6 the arteriovenous (AV) mode is not well suited for support of pa- tients with acute cardiac or pulmonary insufficiency 279 because: (1) the amount of 0 2 that can be delivered per ml of blood flow is considerably less than could be delivered to venous blood, even in patients with severe pulmonary insufficiency. (2) To achieve the blood flows of 3-5 L/minute that would be required to support an adult patient with pulmonary or cardiac insufficiency, at least twice the left ventricular output would be required to sustain sys- temic perfusion. Consequently, a low-resistance, high-flow AV shunt imposes a severe unnecessary strain on the left ventricle. (3) With this high flow, pulmonary artery (PA) pressure in- creases. Arteriovenous bypass with low flow is an effective way to remove CO 2, and has been evaluated as a means of treating hy- percapnia in chronic pulmonary failure. 233
Venovenous (VV) bypass is maintained by cannulating the 24

2 Veto- ~tnous
3 Veno-orleriol 4 M,led veno-~r vtno-orTeriol
Fig 8. -Four modes of extracorporeal circulation. 1, arteriovenous, used for hemodialysis but not suitable for cardiopulmonary support. 2, venovenous, providing extracorporeal gas exchange without affecting hemodynamics. 3, venoarterial, the conventional heart-lung bypass used for most life-support techniques. 4, mixed, which includes drainage of venous blood with arterialized return to both systemic arterial and venous sites.
superior vena cava through one major catheter and the inferior vena cava through another. Venous blood is drained from one catheter, oxygenated and returned to the other. This mode of per- fusion requires a pump but has no effect on overall cardiac output or PA pressure. The pulmonary capillary bed receives all the outflow blood. Hence, VV perfusion is a good laboratory model for s tudying the effects of prolonged surface exposure and arti- ficial oxygenation under conditions of undisturbed hemody- namics.73, 13~, 143, 275 This method also provides a single capillary bed for s tudy of the effects of embolization or short-acting vasoac- tive substances. Venovenous perfusion is not desirable for clinical use because short-circuiting begins to occur when the venous drainage exceeds half of the venous return. In this circumstance, oxygenated blood from one catheter is drained into the other cathe- ter without passing through the tricuspid valve and through the puImonary circulation. Hence, to oxygenate fully all the blood going through the right ventricle and pulmonary artery, VV flow rates at least equal to the cardiac output must be achieved, and excellent mixing must occur in the right a t r iumJ 3~ 131 This limi- tation can be avoided by venous drainage from the right a tr ium
25

and return directly to the right ventricle. Venovenous bypass does nothing to decrease PA pressure and provides no cardiac support. At low flow rates aortic root blood is desaturated, even at high FIo.,. The advantages are maintenance of full pulsatile flow in both pulmonary and systemic systems and a minimized possi- bility of systemic embolism. Venovenous bypass h~s been used successfully in clinical pulmonary failure. 'Ss, ,~7
In venoarterial (VA) bypass blood is drained from the right a tr ium through superior and/or inferior vena caval catheters, oxygenated and returned to the arterial system. Venoarterial bypass provides excellent support for both heart and lung. Maxiu mal benefit both in oxygenation and perfusion can be obtained from each milliliter ofextracorporeal flow. Pulmonary artery p~es- sure drops to normal or subnormal levels. Theoretically this should decrease the pulmonary capillary filtration pressure and favor the oncotic gradient, thereby diminishing extravascular pul- monary water, as demonstrated by Brandt et al. 45 Since heart and lungs are supported, VA bypass affords the opportunity to t reat the lungs via the trachea in ways that would not otherwise be possible. For example, it is possible to hold the lungs in static inflation, inflate and lavage the lungs with large amounts of sa- line, maintain the FIo., at 0.2 even in the face of no lung function, and so on. With aortic arch perfusion, the brain and coronary cir- culation are well oxygenated, even at low flowsY 3. 20o, 2To, 27, For all these reasons, VA bypass is the preferred mode for clinical ECC support. Disadvantages are: (1) The oxygenator outflow should be returned directly to the aortic arch and any particles, bubbles or emboli that arise from the circuit are perfused directly into the brain and coronary arteries. (2) At very high rates of flow the sys- temic arterial pulse contour is diminished, which may result in inadequate renal function. (3) Pulmonary artery flow and possi- ble parenchymal 0 2 delivery are diminished.
A combination of VA and VV perfusion (VVA) has been evalu- ated by Eberhart et al23 and Falke. 96 In this technique, ve- nous blood from the right a tr ium is oxygenated and returned to both the aorta and the right a tr ium or ventricle. This technique was developed on the theory that maintaining some degree of pulmonary blood flow with well-oxygenated blood would improve healing of the lung lesion and decrease the risk of pulmonary venous thrombosis. It gives the investigator total control over all aspects of the circulation and may prove to be a very worthwhile research tool. Falke found VVA perfusion preferable to VA or VV when flows of <50% of cardiac output were used. However, the complexity of the circuit and potential complications of the right ventricular catheter militate against general use of this mode until the value of maintaining PA flow is demonstrated. Unless otherwise specified, all subsequent references to ECC in this monograph refer to VA bypass.
26

HEMODYNAMICS
The hemodynamic effects 0fVA bypass (and the attendant neu- rohumoral responses) have.been thoroughly studied in animals and humans. ~4, ,s, 259 Most studies have served to corrOborate Or elaborate On the initial descriptions of SalsburyySg~'As flow through the extracorpereal circuit is increased, flow through the right ventricle and pulmonary artery decreases so that left ven: tricular filling pressure and left ventricular output fall. Although this dr.op in cardiac output is matched by arterial return from the extracorporeal circuit, the total flow is slightly less than the nor- mal cardiac output before bypass, and systemic hypotension usu- ally occurs transiently. The low-flow-low-pressure phenomenon early in ECC can be minimized by using whole blood for the prime; using a noncompliant, no-reservoir extracorporeal circuit; carefully controlling the temperature, pH, hemat.ocrit, Po 2 and Pco 2 in the prime to minimize vasodilation, effects, and transfus- ing the patient to a comfortably full level(central venous pres- sure [CVP] around 10 mm Hg) prior to initiating ECC. These ob: servations suggest that the'causes of the initial hypotension and low flow are decreased blood viscosity, peripheral vasodilation,
Fig 9. -Hemodynamic changes during VA bypass. Total f low and arterial blood pressure are shown during various levels of bypass. As blood is diverted from the right atrium to the extracorporeal circuit, pulmonary blood f low (and consequently left ventricular flow) decreases to the point where there is no flow during total bypass. Pulse amplitude decreases, reaching a nearly nonpul- satile state during total bypass. (From Bartlett, R. H., and Gazzaniga, A. B.: In Ionescu, M., and Wooler, C. [eds.]: Current Techniques in Extracorporeal Cir- culation [London: Butterworth & Co., Ltd., 1976]. Used by permission.)
ARTERIAL 1 5 0 ~ 1 ~ PRESSURE
mm Hg ~ 70 J - v ,
FLOW cc/mln.
1 I ,,=ECC
[ iil ,ooo ; ~ , o o o ~ ~ " " ~ f
t START PARTIAL BYPASS BYPASS
�9 .... :.....:......:..........
:::::::::::::::::::::::::::::::: . . : . . : . . i . i . : . . i . . : : . : . :::::::::::::::::::::::::::::::::::::: :::::::::::::::::::::::::::::::::::::::: . . . . . . . . . . . : : . : . i . . : * i v . ,
k .............. i f t
TOTAL OFF BYPASS BYPASS
.:::.....-.
i iiii!ii ii!i!!jiiii i iiiJi ili!ililiiii iiii!iiiii :-:.-:::.::::
27

uptake of fluid in reservoirs in the extracorporeal circuit and loss of blood volume by hemodilution and equilibration of extracellu- lar fluid. As the percentage of blood going through the extracor- poreal circuit increases, the systemic arterial pulse pressure de- creases, reaching a nonpulsatile characteristic when total cardio- pulmonary bypass is achieved. (The actual pulse contour is slightly pulsatile with a pulse amplitude of 5-10 mm Hg, due to the roller pump.) With the precautions mentioned above, mean arterial pressure remains normal throughout this transition from pulsatile to nonpulsatile flow. These interrelationships are dia- gramed in Figure 9.
Total bypass with essentially no PA flow and a nonpulsatile �9
systemic pulse contour is usually utilized only under operating room conditions for cardiac surgery. Total bypassis difficult to achieve without thoracotomy and occurs during prolonged sup- port only when extremely high pulr/mnary vascular resistance is encountered. Adequate 02 and CO 2 exchange to support life can be achieved with flow rates of 50-80% of the cardiac output. A convenient physiologic landmark is found when 80-85% of the venous return is bypassed into the extracorporeal circuit. At this point, pulmonary artery pressure contour becomes nonpulsatile during the inflation phase of mechanical ventilation and the sys- temic pulse pressure is markedly narrowed for a few beats follow- ing mechanical inflation. The overall systemic flow remains pul- satile, however�9 This relationship is diagramed in Figure 10,
Fig 10�9 and systemic arterial pressure tracings during VA bypass in a patient with acute pulmonary failure. Pulmonary hypertension.(60/35 ) is present, and right ventricular function is probably the limiting factor'regulating cardiac output. With progressively higher increments of VA bypass, pulmonary hydrostatic pressure decreases. Systemic perfusion improves because of im- proved oxygenation and the relief of right ventricular strain. (From Bartlett, R. H., et al.: J. Thorac. Cardiovasc. Surg. 68:918, 1974. Used by permission.)
PRESSURE (mrn/Hg)
Pulm. Art.ll Syst. I I
15 50 Y y~I ' \ / k , l ~ /
1V o / ,SL.m,n I .o.m,o 'w NI " 4 .O L / m i n
28 ECC FLOW

where systemic arterial pressure and abnormally elevated pul- monary arterial pressure tracings are shown at different ECMO flow rates in a patient with severe pulmonary insufficiency. The patient 's measured cardiac output was 5 L/minute. As bypass flow approached this level, PA pressure fell and meansys t emic pressure rose, although the pulse pressure decreased. At 4 L/minute flow, the pulmonary pulse contour became flattened during mechanical ventilation, as did the systemic pulse. It is interesting to note that mean systemic pressure gradually rose with improving perfusion and oxygenation, although the actual pulse pressure was becoming smaller.
PULSATILE FLOW.- The importance of pulse contour and ampli- tude during perfusion is controversial. There is universal agree- ment tha t the kidney "interprets" nonpulsatile flow as inade- quate flow, resulting i n renin production and antidiuresis. This phenomenon, first described over 25 years ago, h a s b e e n found by all investigators. '~6, 169, 196, 20T Several groups could find no other effects of nonpulsatile total body perfusion. 43, ,33, 257, 295 However, equally competent researchers have reported a syndrome of high systemic vascular resistance, high blood catecholamine levels and poor tissue perfusion, resulting in cerebral changes, renal failure and severe lactic acidosis. 9~ 2~, 262 Trinkle found this syn- drome during nonpulsatile perfusion in animals, 2s3 but found an equal incidence of the poor perfusion syndrome in both pulsatile and nonpulsatile flow during cardiac surgery in man. 2s~ These apparent contradictions can be resolved by careful examination of the experimental methods correlated with the classical studies of Harrison et al. 135, 136
Normally blood flow is approximately 110 ml/kg with a pulse amplitude of 2 0 - 4 0 mm Hg (with some species variations). The studies tha t demonstrated acidosis and organ failure during non- pulsatile flow were all conducted at flow rates ranging from 60 to 100 ml/kg2 ~ 249, 262, 267, 2s3 Those investigators who found no differ- ence between pulsatile and nonpulsatile flow used total perfusion rates of 130- 200 ml/kg. 43, ,33, 257, 29~ This relationship could have been predicted from the studies of Harrison and others, '35, ,36 who showed that adrenal catecholamine secretion is regulated in part by carotid sinus baroreceptors. Decreased pulse amplitude caused maximal catecholamine output when total flow was less than normal, but minimal catecholamine output during normal and supernormal flow rates. From Harrison's findings, one might expect no difference among normal flow, pulsatile perfusion and nonpulsatile perfusion at flow rates over 110 ml/kg; the high-re- s i s t a n c e - acidosis syndrome during nonpulsatile perfusion only at flow rates of 8 0 - 1 0 0 ml/kg, and the high-res is tance-acidosis syndrome during both pulsatile and nonpulsatile perfusion at flow rates less than 70 ml/kg. This corresponds almost exactly to the reports listed above. Harrison's studies and most of the com-
29

parative studies listed above were carried out at 37 C. The effects of hypothermia and its relationship on normal blood flow require- ment on the carotid sinus adrenal access have not been thorough- ly studied. This probably accounts for some of the variations seen during clinical cases. ~25. 28~
The implications of these studies for total cardiopulmonary bypass in cardiac surgery are" total perfusion is usually 70-100 ml/kg. At this abnormally low flow rate adrenal catecholamine secretion is increased by decreasing pulse amplitude, hence pul- satile flow or alpha blockade should be used to ameliorate the sys- temic effects of the altered flow pattern. During partial cardiopul~ monary bypass for life support, total flow should be maintaine d as near normal as possible, and should be regulated by whate~er means necessary to assure a pulse amplitude of 15 mm Hg or more.
PATHOPHY.qIOLOGY.- Hypovolemia during ECMO is manifested by decrease in extracorporeal flow rate and arterial pressure. It is treated by simple volume replacement, preferably with blood or colloidal solutions, If flow and pressure are not promptly restored with volume infusion, mechanical problems such as partial ve- nous catheter occlusion or pneumothorax should be suspected. (Tension pneumothorax is difficult to recognize during ECMO. Decreased flow and arterial pressure may be the only obvious manifestation. Pneumothorax should be vented with a needle until those experienced with placing chest tubes in heparinized thrombocytopenic ECMO patients are available.) Diminished arterial and pulmonary pulse amplitude and episodic emptying of the right or left ventricle are further signs of hypovolemia or ex- cessively high extracorporeal flows.
Hypervolemia can easily occur, particularly in small patients, when blood loss into dressings, etc., is overestimated. The find- ings in hypervolemia are widening pulse amplitude and decreas- ing systemic oxygenation at a fixed extracorporeal flow caused by larger amounts of blood passing through the malfunctioning lungs. It is easy to chase one's tail by going to higher extracorpo- real flows in hypervolemia. The syndrome is better treated by removing blood from the system.
Hypertension during ECMO is usually caused by an outpour- ing of catecholamines. If the patient becomes hypertensive with stable ECMO flow, one should suspect unusual pain or anxiety, gastric or bladder distention, CO 2 retention from a malfunction- ing oxygenator or increased intracranial pressure.
Failure of the mechanical pump can occur from loss of electric power or pump chamber distortion, wear or rupture. Whatever mechanical pump is used, it must have the capability of manual operation to deal with such emergencies. In addition we keep a fully charged 12-volt battery and AC converter on hand during all ECMO treatment.
3O

FLUIDS AND METABOLISM
The extracellular space is enlarged during ECC. Initially this is because of distribution ofcrystalloid solution in the prime, and the space is kept large by aldosterone and possibly antidiuretic hormone (ADH) effects. Generalized edema is the rule-f611owing cardiac operations with ECC, and also accompanies prolonged ECMO support. This extracellular fluid (ECF) expansion causes no deleterious effects except perhaps in the brain and certainly in the lung. During ECMO gross pulmonary edema disappears promptly, probably because of decreasing hydrostatic pressure in the pulmonary arterioles while normal oncotic pressure is main- tained. Therefore, until the weaning process begins, a moderate ! amount of ECF expansion is tolerated. This tendency to antidi- uresis can be overridden by diuretics such as furosemide if that is considered preferable because of brain or lung dysfunction. The blood volume itself is two to three times normal during ECMO, and this must be taken into account when calculating volume replacement and drug dosages. Because water antidiuresis usu- ally exceeds sodium retention, and because of the kaliuretic effect of aldosterone, generalized hyposmolarity with hyponatremia and hypokalemia usually accompanies short-term ECC. 224 Effects of ECMO on electrolyte concentration are minimal. The major importance of these changes is in the possibility of digitalis-in- duced arrhythmias exacerbated by hypokalemia.
Renal failure may occur if narrow pulse amplitude at high ECMO flow is superimposed on borderline renal function caused by the primary disease. Converting to pulsatile perfusion would seem a logical step, but the narrow gauge of arterial access cathe- ters limits the usefulness of this approach. Improving 'pulsation with an intra-aortic balloon would be a possible alternative. Usu- ally incipient renal failure is handled by allowing more blood to go through the lungs. This increases pulse amplitude, but re- quires increasing the FIo2 to 0.5 or 0.6.
Energy requirements as measured by O~ consumption and CO 2 production are often excessive, due to the primary disease. Once sepsis is controlled and peripheral perfusion and oxygenation are established, metabolic rate usually decreases to the high normal range. This phenomenon is frequently observed in the ECMO patient and has recently been reported by Freund, et al. '04
GAS EXCHANGE
Normal function of artificial lungs has been outlined in the preceding section. The maximal flow of normal venous blood that can be fully saturated for a given oxygenator can be measured (see Fig 3). Likewise, the amount of oxygen that can be delivered to flowing blood with a given device can be calculated (see Fig 4). The perfusion pressure of the oxygenator at a defined flow is also known.
31

PATHOPHYSIOLOGY OF MEMBRANE LUNGS
Like the biologic lung, the membrane lung is subject to pul- monary edema, ventilation perfusion imbalance, pulmonary embolism and several other abnormalities of function. Most of the malfunctions are illustrated in Figure 11, and can he~fliagnosed by measuring changes from the normal state in oxygen transfer, CO 2 transfer and vascular resistance.
Changes in membrane lung performance with time have been studied in detail by Ward et al. T M In the most exhaustive charac- terization of membrane lung performance yet reported, these authors defined gas exchange and hemodynamics over a wide range of flow and inlet blood characteristics. By means of t h e ~ data, the performance of similar membrane lungs could be evalu- ated at any set of running conditions, compared to the optimal performance data and expressed as a percentage of optimal per- formance. With this method, Ward and Hood 29~ studied the per- formance of 3 types of membrane lungs during 4 days ofextracor- poreal circulation. That study clearly identified and quantitated the problems of thrombosis and water accumulation, along with the specific design characteristics that led to those problems.
Abnormalities of perfusion in membrane lungs include throm-
Fig 11.-Areas of possible malfunction in a membrane lung. The numbers in the diagram identify the abnormal condit ions described in the key.
t Gas
oo:~:~ooooo~aa~ 3 o @ _ OOB'O"L.-
Blood I Water
32
BLOOD FLO~ 0~STRUCTIO~
~) Y,~OR INLET OR OUTLET T'RO~OSiS
(~) s THROf~OSI$ OF INDIVIDUAL CELLS
~) P~TIAL THRO~OSIS OF ]~DIVIDL~L CELLS
(~ BL~O CEAK (~Y r-AUSE ~ OR (~))
GJ~S FLOWer OBSTRUCTION
~) C(X'~LETE 0BSTRLCTION OF CELL (WATER OR ELOOD) VENTILATION
(~ PARTIAL (0~STROOTION OF CELL (WATER)
~o 2 ~e ~co 2
111 TTT 155
$ I J,,L
.L -- J l l
. . . . . . . I J .
0 ~s IEAK (~Y CAUSE ~)
VENTILATION ~ERFUS|ON |J'I.~aKUNCE
(~ POOR VENTILATION (~) , (~) IN AREA OF HIC,~4 I FLO. (DUE TO (~), (~), (~, (~) OR DESIGN ~ls

bosis of inlet headers and major distribution ports, minor throm- boses within the membrane cells, major thromboses of entire membrane units and blood leak into the gas phase.
Major inlet header thrombosis is unusual. It occurs in mem- brane oxygenators with very small distribution ports, such as the GE oxygenator. There is an abrupt rise in perfusion p~ssure, maldistribution of low flow to various cells in the unit follows and both 02 and CO 2 transfer decrease rapidly. Inlet header thrombo- sis is prevented by maintaining adequate heparinization and by avoiding those oxygenator designs that include abrupt right-an- gle turns, eddies in stagnant zones or channels less than 2 mm in the inlet header. Treatment requires discarding the involved unit and substituting a new one.
Minor thromboses occur in all membrane oxygenators wher- ever areas of slow flow are inherent in the design of the device. They probably represent more dehydration and drying of the in- volved areas than actual thrombosis. These minor thromboses have no significant effect on oxygenator function; hence they cannot be diagnosed. In fact, it is probably not important to diag- nose them during prolonged perfusion. They do not require treat- ment.
Major thrombosis of one or more of the units within the oxygen- ator occurs whenever minor variations in design of construction create units with uniquely slow flow. This may be due to inlet or outlet thrombosis in that particular cell or to the position of the cell relative to the major flow path. Figure 12 shows the outer- most cell of a Travenol microporous membrane oxygenator after prolonged perfusion. The entire cell is filled with gelatinous thrombus. When individual cells become coagulated, 02 and CO 2 transfer are equally affected. Since performance is limited by O~ transfer, the characteristic symptom is loss of oxygenation, and increase in perfusion pressure occurs, depending on the number of cells occluded. Coagulation of individual cells can be prevented by assuring a high flow of blood to all areas of the membrane oxy- genator both in the initial design and through the process of peri- odically directing excess flow through all the modules when sev- eral oxygenators are used in parallel. Pulsing the blood phase, pulsing the gas phase and varying shim pressure where appro- priate may be helpful in this regard. This lesion does not need treatment until it becomes quite extensive. When the oxygenat- ing capability has severely decreased due to cell thrombosis, the artificial lung module must be replaced.
Blood leakage into the gas phase is usually caused by actual defects in the membrane. Careful quality control by the manufac- turer will prevent this, although small pinholes may leak only at unusually high perfusion pressure. Small blood leaks (less than 5 ml/minute) often occur when Landd-Edwards oxygenators are used at high pressures and seal spontaneously with time. Major blood leaks are usually gross and require immediate oxygenator
33

I I
Fig 12. - Examples of minor thrombosis (A) and major thrombosis (B) in mem- brane lungs. Thrombi form in areas of low flow caused by device design. (From Bartlett, R. H., et al.: Trans. Am. Soc. Artif. Intern. Organs 21:250, 1975. Used by permission.)
replacement. If the membrane has a s t ructural defect tha t leads to a leak, this will be immediately noticeable. Once an oxygena- tor is successfully tested at normal perfusion pressures, it will remain intact for weeks at a time. The use of microporous mem- brane causes a different type of leakage problem: plasma can be
34

filtered through the pores at high pressure so that control of the perfusion pressure becomes of critical importance.
Ventilation of the membrane oxygenator can be impaired by accumulation of water droplets condensing in the gas phase, oc- clusion of entire cells by water in the gas phase or leakage of gas into the blood through mechanical defects in the oxyg~nator. Since water is converted from liquid water in the blood to water vapor passing through the membrane, cooling takes place. The gas side of the membrane is always somewhat cooler than the blood, so that a condensation of water is enhanced. Heat ing the gas does little to solve this problem, since gas has a low heat- carrying capacity. Heat ing and humidifying the gas minimizes the water vapor loss from blood by decreasing the gradient for water vapor pressure between the membrane surfaces and the gas phase. However, this does not improve the condensation prob- lem, since fully saturated gas is being supplied and any cooling will result in immediate condensation. Condensation can be min- imized by supplying heated humidified gas if the entire oxygena- tor is at 37 C. Hence water condensate collection is much less of a problem in a Bramson oxygenator (where the heat exchanger is built into the device) than it is with other oxygenators that do not include an integral heat exchanger. From a practical point of view we find the water loss helpful in management of the patient, as i t is an effective way of removing water in almost any desired amount without losing electrolytes.
The pathophysiologic characteristic of water accumulation in the gas phase is CO 2 retention (i.e., loss of CO 2 transfer). When water droplets occur on the membrane surface or when entire cells are closed from gas flow by water accumulation, the surface of the water is in equilibrium with flowing gas in adjacent pas- sages that have a very high Po 2. Consequently, the water Po 2 remains very high, and some oxygenation of blood on the opposite side of the membrane continues to occur. On the other hand, CO 2 diffusing from the blood dissolves in the water, raising the Pc% in the water. The CO 2 leaves the water wherever it comes in con- tact with ventilating gas, but as progressively larger amounts of membrane are covered with water, the barrier for CO 2 trans- fer becomes greater and greater and finally CO 2 transfer is lost. When many cells are occluded with water in the gas phase, 02 transfer falls as well. This problem can be prevented by careful design of the oxygenator, so that any accumulated water runs by gravity out of the device (as in the Sci-Med Kolobow oxygenator) and can be minimized by maintaining the temperature of the en- tire oxygenator at 37 C ( as in the Bramson device). If geometry or temperature of the device does not favor water excretion, very high gas flows with intermit tent pulsing of the gas flow ("coughing the oxygenator") must be carried out to avoid severe accumulation of condensed water. This is the case with the
35

Land~-Edwards oxygenator, in which water accumulation results in a severe drop in CO 2 transfer within 24 hours of ECC (at the manufacturer 's original recommended gas flow rates of 9 L/3 sq m module/minute). If this occurs, CO 2 transfer usually can be re- turned to normal by increasing gas flows to greater than 20 L/minute and intermittently occluding the gas outflow of the oxygenator to expel water droplets. The problem can be prevent- ed by running a continuous gas flow of 15 L/minute or greater.
Microporous membranes made of expanded Teflon or polypro- pylene, with or without additional coatings, will be used in the artificial lungs of the future. These membranes are stronger, more uniform and more reliable than silicone polymers, and are heat sealable. Even though membranes represent a microscopic continuous blood-gas interface, the hematologic effects of pro- longed exposure to this material are identical to the effects of sili- cone polymer exposure. 'n 2,~ Since CO~ and water vapor transfer are limited by membrane characteristics, their exchange through microporous membrane is much greater than that through solid membranes. Carbon dioxide must always be added to the venti- lating gas with such devices, and water accumulation in the gas phase precludes long-term use in currently available devices. ~7 Water loss can be controlled without losing oxygenating capabil- ity by coating the microporous substrate with a very thin layer of silicone polymer, polyalkylsulfone, etc. 121, ~6T
Gas leaks into the blood should never occur, and all devices are designed so that the gas phase pressure can not exceed the blood phase. If gas did leak into blood, gas embolism would occur.
Any or all of these malfunctions may occur singly or in combi- nation, leading to inequality of ventilation and perfusion. In an extreme example, all of the cells and inlet headers to one part of the membrane oxygenator may be occluded, so that there is no blood flow, while all the gas flow to the remaining cells may be occluded by water vapor, resulting in a totally nonfunctioning oxygenator. All variations between this example and normal ventilation and perfusion can occur. Despite the possibility of malfunctions, membrane oxygenators usually function well for weeks at a time when properly used. ~5, 17~. ~s~
PATH(~PHYSIOLOGY OF THE BIOLOGIC LUNG DURING ECMO
During the 1st decade of intracardiac surgery, severe pulmo- nary failure occurred frequently. This syndrome even had a n a m e - " p u m p l u n g " - a n d the pathophysiology and histologic appearance were described in detailY 4T, 28, Since 1970 this syn- drome has disappeared, so that changes in pulmonary function following cardiopulmonary bypass are only those related to a thoracotomy. Many factors may account for this abrulbt change. The patient population is different, perfusion techniques are bet- ter and the amount of transfused blood is less, but the most im-
36

portant factor (in the author's opinion) is conversion to single- use, disposable blood contact surfaces. Reuse of a small portion of the extracorporeal c i rcui t -even a few connectors that are thoroughly cleaned and sterilized-is commonly associated with pulmonary failure in laboratory animals. Reusing entire oxygen- ators, pumping chambers, connectors, reservoirs, etc., was common practice during the 1st decade of cardiac surgery. With the advent of the single-use, disposable oxygenator, most teams progressed to renewing the entire circuit for each patient.
The effect of days or weeks of ECMO on the biologic lung is difficult to determine because the technique has been used pri- marily in patients with pre-existing severe pulmonary failure. The fact that many of these patients eventually succumb to irre- versible lung damage inevitably leads to the suspicion that the ECMO system is oxygenating the blood but further damaging the lung. Spragg 275 and Bloom 4' have shown that platelets may be concentrated in the lung during ECMO, in VV or VA bypass. Rat- lift and Hill 245 have suggested that low flow through the pulmo- nary vasculature during ECMO may lead to thrombosis in pul- monary capillaries, venules or veins, with ultimate damage to lung tissue andsystemic embolization. On the other hand, many patients have survived and recovered normal lung function after long periods on ECMO support. Patients treated with ECMO for cardiac failure have been few in number, but lung function did not deteriorate in these patients. Finally, the most persuasive datum is the lack of lung damage in animals subjected to VA bypass for days or weeks. 9, 7:, 13,, :75
BLOOD-SURFACE INTERACTIONS
The use of prolonged ECC requires exposing most of the cardiac output to a large artificial surface each minute. Each red cell, white cell, platelet and protein molecule comes into contact with the foreign surface each hour. In addition to the abnormal sur- face, the flow patterns often include stagnant zones, eddy cur- rents, abrupt right-angle turns, rapid changes in velocity and the potential for jet and cavitation flow patterns. Although the poten- tial for damage to blood elements is great, in practice, hemoly- sis is negligible, 23. 34. 35. '3, ''~ white cell damage is probably minimal 26s and fibrinogen-to-fibrin conversion is held in abey- ance by heparin. Platelets show the greatest effect of prolonged foreign surface interaction, manifested by continuous platelet aggregate formation and decreasing blood platelet count.
The best evidence indicates that the sequence of events on blood-prosthetic surface exposure is as follows: 2s' (1) Within sec- onds of random exposure, a molecular layer of protein becomes adherent to the prosthetic surface. The more irregular the sur- face, the more dirt, grease or bacteria, the more silica filler in glass or silicone rubber, the more irregular interstices in cloth
37

materials, the more protein will adhere to the surface. 1~ (2) It has not been determined whether certain proteins have a preference for certain types of binding sites, but it appears that all proteins compete equally under most circumstancesY Hence some of the "binding sites" will have adherent fibrinogen whereas others may have albumin, alpha globulin, gamma globulin, etc. (3yOne of the proteins that changes characteristics with surface exposure is Hageman factor (factor XII). When this factor is activated, the coagulation cascade of enzymatic changes occurs, ul t imately re- sulting in the formation of thrombin, which converts the adher- ent fibrinogen to fibrin.
This final step of fibrin formation (as well as others) is inhibited by heparin. Without heparin, fibrin formation will trap platelet~, which further st imulate fibrin formation, ul t imately resulting in thrombosis at tha t site. In the presence of heparin the fibrinogen on the surface is not converted to fibrin, and thrombus formation, at least in the usual sense of a large red clot, does not occur. Once all the active sites on the prosthetic surface are covered by a pro- tein monolayer, the flowing blood "sees" a protein-water-electro- lyte molecular film ra ther than the plastic or metal surface itself. Fur ther adherence of protein does not occur, and this layer does not accumulate in size. The process occurs within seconds of expo- sure. Protein molecules in the flowing blood interchange with surface-adsorbed proteins, but the extent of this flux has not been completely studied/~ The majority of binding sites can be con- trolled by pre-exposure to a specific protein. For example, pre- exposure of plastic surfaces to albumin appears to minimize fibrinogen surface adherence and later platelet destruction2 ~ 2~
Repeated exposure of blood to such a "pacified" surface appears to have much less effect on blood constituents than repeated expo- sure to a fresh surface. This probably accounts for the major dif- ferences between gas-interface oxygenators and membrane oxy- genators.
The nature of the proteins that are adsorbed on the surface affects the other blood constituents, particularly platelets. Plate- lets adhere to the surface in specific locations, beginning minutes after exposure/37 They probably adhere to areas where fibrinogen molecules are adherent. The evidence for this is that pretreating a surface with albumin minimizes platelet adhesion to the sur- face, whereas pretreat ing a surface with pure fibrinogen maxi- mizes platelet adherenceY ~4, 255 A single platelet usually adheres first, at taching by a te ther or pseudopod. The surface of the plate- let distorts, depending on the blood flow conditions at tha t site. Distortion is accompanied by the release reaction in which the platelet discharges material from its granules into the adjacent blood. This material includes serotonin and adenosine diphos- phate (ADP). These and other factors induce .changes in other adjacent platelets that lead to adhesion to the surface and the formation of a platelet aggregate, or to adhesion of platelets to
38

other platelets, resulting in a flowing aggregate. In an extracor- poreal circuit the flowing aggregate is returned to the pat ient as a microembolus ofplatelets adherent to one another2 ~, o.,
White cells and red cells may also become enmeshed in the forming platelet aggregate, but in the presence of heparin the surface-attached aggregates usually consist primarily of~latelets with some white cells. The shape and growth of these aggregates depends on the flow pat tern at tha t point in the circuit. In areas where the flow path enlarges abrupt ly with a right-angle wall, such as the downstream side of a connector-to-tubing interface, eddy currents will form and a s tagnant zone of no flow will occur, which may be tens of microns in diameter. The platelet aggregate will grow in this no-flow zone until the area of active flow is reached. 26 Further aggregates forming at the surface presumably are washed off into the flow stream at that point. Fibrinogen is converted to fibrin in the midst of this platelet aggregate, wheth- er by thromboplastic factors released from platelets overcoming the heparin effect, or by metabolism of the heparin in the low-flow zone, or both. At any rate, the final product is a smooth fibrin- platelet white thrombus, which is firmly adherent to the surface and eventually results in smoothing the flow path of the blood. After days or weeks of ECC these white thrombi can be found in vir tually every microscopic low-flow zone, downstream from connectors, etc. The size of the right-angle step-off related to the flow rate of blood going past that point probably determines whether or not red cells are trapped in the midst of the growing aggregate. In areas of very low flow red cells are usually en- trapped in the aggregate, creating a red thrombus. In areas of high flow white thrombi form. Mechanical damage in. the pump probably enhances aggregation. If the pump is eliminated from a test, the ECMO circuit platelet count remains near normal.176.25c,
The platelet aggregates range from 2 to 200 ~ in size (Fig 13). These platelets do not ledge in the first capillary bed they encoun- ter, hence do not cause microembolic tissue damage. This is true if the oxygenator re turn is directed to the arterial or venous cir- culation2. 175, 27s If the platelets are labeled with radioactive iso- topes, radioactivity appears in the liver and spleen and to a lesser extent in the lung. Radioactivity can be found in the membrane lung during the 1st hour but decreases rapidly thereafter. The aggregated deformed platelets are probably bound or phagocy- tized by the reticuloendothelial cells, deLeval, TM Hicks '4~ and Dutton 9" reported data from 2- to 8-hour experiments suggesting that these platelets disaggregate and recirculate. Spragg 2;~ and Bloom 4~ could not demonstrate a re turn of radioactively labeled platelets to the circulation after 24 hours of ECMO, which sug- gests that most of the original cohort of tagged platelets (or at least the radioactive label) is removed from the circulation after 1 day of ECMO.
Since it has been shown that platelet aggregates are generated 39

f ' , ' ,
F~.cj 13,-Platelet microaggregates (iltered from an ECMO circuit. Each aggre- gate contains thousands of platelets. During ECMO these aggregates are con- tinuously formed, break down and reform. (From Dutton et al.: J. Thorac. Car- d[ovasc. Surg. 67:25~5, 1973. Used by permission.)
continuously and the number of aggregates is large, 9-" and assum- ing tha t aggregation occurs uniformly and randomly to all plate- leLs, it can be calculated that all the circulating platelets are in- corporated into aggregates every few hours. Even with maximal thrombopoiesis the platelet count would approach zero if the ag- gregated platelets did not recirculate. In animal and human studies the platelet count reaches a plateau at 30,000- 60,000/cu mm during ECMO, so recirculation must occur.
40

PHYSIOLOGIC CHANGES IN PLATELETS AND COAGULATION FACTORS DURING ECMO '6
The same pattern of response is seen in normal animals and in patients who have normal coagulation study results when started on ECMO 69, ,39 (Fig 14). Platelet count decreases to apprG'ximate- ly 50% of normal values in the first few hours, followed by a more gradual decrease and leveling off at approximately 30% of the ini- tial values after 1 - 2 days. '~176 '~, '~ Platelet count thereafter is a balance among (1) platelet aggregation, circulation and removal by the reticuloendothelial system, (2) platelet generation from bone marrow that is st imulated to maximal levels and (3) disag- gregation and recirculation of aggregated platelets. The amount of foreign surface exposure per unit of blood flow affects the amount of platelet aggregation, so that when the extracorporeal circuit is very large compared to the pat ient (as in the newborn), or when platelet generating capacity is small (also t rue of
Fig 14.-Change in platelet count during ECMO in normal sheep. Membrane lungs with minimal blood mixing (Land6) and maximal blood mixing (TMO) showed the same effects. Platelet count drops to 50% of initial value within the first few hours, then gradually decreases to approximately 30% of original value over the next 2 days. The rebound to twice normal levels following ECMO sug- gests that platelet generation from bone marrow is stimulated to maximal levels by blood surface contact, thrombocytopenia or both. (Figs 14 and 15 from Bart- lett, R. H., et al.: Trans. Am. Soc. Artif. Intern. Organs 21:250, 1975. Used by permission.)
Silicone Rubber Membrone Oxygenotors
c -
o )
o~
280
260
240
220
200
180
160
140
120
IO0
80
60
40
20
"E
8 0,) CD
0
,, . . . .
Lond~ } Av '~Range
I I I l t t I ' I I
Pre 6 12 18 24 36 48! 7 14 Byposs Hours of Bypass '. Doys
. . . . . . . . ; post-op
41

the newborn), thrombocytopenia is more pronounced. '~176 Large amounts of heparin can cause platelet aggregation in vitro, and thrombocytopenia caused by heparinization has been reported in man, so the possibility that heparin itself contributes to thrombo- cytopenia during ECMO must be considered. This seems,,unlikely for the following reason: chronic heparinization with Noses com- parable to those used for ECMO does not cause thromboeytopenia in animals '~ ,76 or man. 1~176 ,39 Patients who begin ECMO with pre-existing thrombocytopenia secondary to their basic disease usually experience an increase in platelet count that lasts for days, despite heparinization and aggregate formation. In animal studies low heparin dosage was associated with more severej thrombocytopenia,eg0, 291 and increasing heparin dosage during" ECMO was associated with a rise in platelet count. 17s Hence we conclude that heparin is not responsible for the thrombocytopenia during ECMO. On the contrary, heparin may improve platelet survival by inhibiting the formation of plasma cofactors that are necessary for the platelet release reaction and platelet aggrega- tion.293
Although thrombocytopenia uniformly appears during ECMO, investigators do not agree on the effects of ECMO on platelet function. Most of this apparent controversy arises from the fact that platelet function tests are difficult to interpret in heparin- ized thrombocytopenic blood. Heparin will block the conventional assay for platelet factor III, for example. The amount of adhesion or aggregation in response to standard stimuli decreases propor- tionately with decreasing platelet count, so that decreased activi- ty with these methods of testing may be related to decreased numbers of platelets, impaired function or both. Studies from our laboratory 1~176 and others 23~, ~78 show that platelets circulating dur- ing ECMO have a moderate decrease in function, even taking into account the thrombocytopenia. This is corroborated by ab- normal bleeding time, even after heparin effect has been re- versed. 6s These findings lend support to the hypothesis that the most active platelets aggregate easily, then recirculate with de- creased activity, perhaps repeating this cycle many times each day. Some insight into these interrelations can be gained from the study of patients who begin ECMO with pre-existing throm- bocytopenia secondary to consumption coagulopathy. In those patients the platelet count generally rises during ECMO, and platelet function usually improves (by direct measurement, or estimated from bleeding tendency or bleeding time). One expla- nation for this phenomenon is that fresh, healthy platelets are being generated rapidly from the bone marrow in response to thrombocytopenia, only to be rapidly consumed in the primary disease. Through heparinization, improved perfusion and im- proved gas exchange the stimuli to platelet consumption are re- versed during ECMO, so that new platelets circulate longer, im-
4 2

Silicone Rubber Membron~ Oxygenofors
soo ,, . . . . :
2oor " T T ! I - ' " *~ : . . . . . . . . . .
Z00
O - ' , , , , i i i i i
2 8 0
240
200
'160;
120
80
4 0
0 ~ , H o u r s o f B y p o ~ O~yS
, . . . . . . . . . post- o~
Fig 15.-Changes in representative clotting factors during 48 hours of ECMO in sheep. Normal values are maintained after the initial dilution, with abrupt increase following ECMO. (Values for factors are expressed as percent of nor- mal human control.)
proving overall platelet function in spite of the .inevitable sur- face-induced adhesion and microaggregate formation.
Fibrinogen and other coagulation factors decrease abruptly with the onset of ECMO, partly due to dilutional effects and part- ly due to adherence to the prosthetic surface (Fig 15). This occurs even if the prosthetic surface has been exposed to albumin or whole blood prior to ECMO. Plasma concentration of clotting fac- tors is usually back to normal by 6 hours and remains normal or at moderately elevated levels throughout ECMO. 1~176 Some of this may be due to the heparinization itself, since heparin interrupts the gradual normal conversion of fibrinogen to fibrin. Fibrin deg- radation products (FDP) are usually not detectable during ECMO. However, if the heparin dose is titrated to very low levels, or if some stimulus to coagulation such as endotoxemia occurs, the typical pattern of consumption coagulopathy is seen with fall- ing fibrinogen, rising FDP and falling platelet count.
When the stimulus to platelet and coagulation factor loss is removed at the time of decannulation, the accelerated generation
43

rates continue unopposed, so that a rebound effect occurs, with platelet and fibrinogen levels reaching twice the original baseline 2 -7 days after ECMO 1~176 ~5 (see Fig 14). All values return to normal by 2 weeks after ECMO.
PREVENTION OF THROMBOCYTOPENIA AND BLEEDING DURING ECMO
Although we can characterize and understand the platelet and coagulation changes with ECMO as outlined above, bleeding is still the major complication of the procedure. There are three approaches to solving this problem: (1) modifying or eliminating~ anticoagulant requirement, (2) improving platelet life-span by" modifying platelet function and (3) modifying prosthetic surfaces to decrease platelet aggregate and fibrin formation.
Several researchers have approached the problem of develop- ing a nonanticoagulant system. Since the introduction of continu- ous low heparin titration, 9 investigators have modified the circuit to carry the heparin dose as low as possible. Fletcher and asso- ciates reported 24-hour ECMO in dogs 98 and baboons 99 using no heparin at all. They could maintain extracorporeal flow and oxy- genator function during this time, although clotting occurred throughout the system and there was a blood picture of extensive consumption coagulopathy. High levels of FDP combined with thrombocytopenia to produce an autoanticoagulation in these animals. Similar observations were reported by Ward and asso- ciates, T M using a heparin dose (in calves) of approximately half the usual required level. In Ward's study, carried out for longer periods of time at high bypass flow rates, severe oxygenator mal- function occurred. Defibrination using an agent such as Arvin was studied in ECMO by Bfiky et al. 5~ They found adequate anti- coagulation, easily monitored by thrombin time and reversed by fibrinogen. Platelet counts in Bfiky's experiments showed de- creases similar to those found with heparin anticoagulation. The hazards of defibrination anticoagulation are: a controlled con- sumption coagulopathy must be induced to achieve the desired effect; reversing the effect with fibrinogen requires inducing even more consumption coagulopathy with potential problems, and fibrinogen infusion always carries the risk of hepatitis.
Inhibition of platelet release reaction and aggregation with drugs should decrease microaggregate formation and increase platelet count during ECMO. Many agents inhibit platelet func- tion, but most do not improve platelet economy when used in con- junction with ECMO. 42 Dipyridamole and sulfinpyrazone have been shown to improve platelet quantity in short-term experi- mentsY. 204 Dextran2GO and prostaglandin EI2GI may have similar effects. Of course, larger numbers of the circulating platelets whose function has been impaired by drugs may make bleeding complications worse rather than better.
44

Design of a biocompatible surface may involve: (1) eliminating irregularities or protein binding sites on the surface, 95, ~52, ,76 (2) accepting surface binding sites and precoating them with specifi- cally selected proteins, ~.~4 (3) inhibiting fibrinogen conversion to fibrin with surface-bound anticoagulants2 TM 2~s (4) elinlinating fibrin as it forms with surface-bound fibrinolysis, '8~ (5) completely eliminating stagnant zones in the flow path and/or (6) inhibiting platelet adhesion to the surface with surface-bound agents.
Coating the entire extracorporeal circuit with a thromboresis- tant material has been evaluated in other types ofextracorporeal shunts but has presented problems in ECMO because of the possi- bility of inhibiting transmembrane gas exchange by surface coat- ing. Hagler et al. '2s approached this problem by modifying TDMAC surface coating to one that was compatible with mem- brane oxygenator function. Using this approach, they reported 5 days of ECC in dogs with no heparin and no oxygenator dysfunc- tion. Platelet count was not measured in these experiments. These results encourage intensive study of this approach.
Theorizing that thrombocytopenia was in part related to sur- face irregularities in the circuit and silica filler used for adding strength to silicone polymers, Kolobow coated the entire circuit with a very thin layer of silica-free pure siloxane polymer. Using a very high initial heparin dose followed by conventional titra- tion, his group reported 0% platelet loss during 24-hour AV by- pass (without a pump), '76 and 30% platelet loss during VV bypass with a pump. ~Ts These results have been corroborated by Zapol. 3~176 Richardson 2~2 suggested that the improvement may be due to the uniform smooth coating rather than a property unique to silicone polymer. These studies serve to bring us one step closer to the nonanticoagulated system.
ORGAN EFFECTS OF ECMO
Effects on the heart and lung have been discussed. Follow-up studies on ECMO survivors (both animal and human) show no effects on growth and development or on brain, heart, hepatic, reticuloendothelial, gastrointestinal or renal function. We evalu- ated parenchymal organ damage during 48 hours of ECMO in sheep by measuring serum levels of tissue-specific enzymes. Only slightly elevated levels of enzymes specific to heart, liver and muscle were found.~4
Disordered brain function, including memory loss, can be de- tected in 10-20% of patients following open-heart surgery. '26, ,s9 These findings are usually transient and disappear within a peri- od of weeks. These minor changes occur with bubble oxygenators and are correlated with ultrasonically detected particles (probably microbubbles) in the perfusion line. The microbubbles (and presumably the brain dysfunction) can be prevented by on- line 40-~ filtration using the filter primarily as a microbubble
45

trap. Carlson et al. ~3 corroborated this phenomenon and showed that the use of membrane oxygenators eliminates the microparti- cles and the brain dysfunction. Brain function during ECMO is grossly normal for periods up to 3 weeks. Detailed studies have not been done, primarily because moderate sedation is usually administered and the patient cannot talk because of airway ac- cess. Although liver function usually remains normal by conven- tional serum tests during ECMO, hepatosplenomegaly usually occurs, becoming more and more prominent with t ime on ECMO. We relate this to the continuous load on the reticuloendothelial components of those organs. Hepatosplenomegaly resolves promptly after bypass.
TECHNIQUES OF CLINICAL ECMO
Each research group studying ECMO develops techniques that fit its needs. This "how-to-do-it" section is included to give the reader some insight into how the basic principles outlined earlier are applied to clinical cases. Alternative methods are discussed, but our own techniques are emphasized2 5. ,9. 23 The interested reader should review the methods of Hill. '39, ,44, ,4s, ,s, Zapol,29s, 299 Drinker, '32 and others m, ,ss, ,77, ,sT, 242, 264, 270 listed in the following sections.
'~THE MACHINE" - - DESIGNING THE CIRCUIT
Visitors to the ECMO laboratory often wish to see "the ma- chine." From the preceding sections it is obvious that the equip- ment used for ECMO is not a specific device but a combination of devices, which is custom-made for each application. Circuit com- ponents are selected according to pat ient size, vascular access and preference of the ECMO team. Typical component diagrams and an assembled circuit are shown in Figure 16.
The "machine" should be capable of total cardiopulmonary support, even though that may never be required. The combina- tion of venous catheter, conduit tubing and pump must be capable of achieving a flow rate equivalent to the normal cardiac output (3.2 L/sq m/minute in adults, 120 ml/kg in the newborn). The gas exchange capability must be adequate to saturate venous blood fully at that flow rate. That is, the "rated flow" of the oxygena- tor(s) must be greater than the cardiac output. In modular systems (such as the Land~-Edwards or Travenol oxygenators) modules are added in parallel until the sum of the rated flow for each unit is greater than the total cardiac output. The gas exchange re- quirements of hypermetabolic patients may be as high as twice normal, and this should be taken into account when planning the circuit.
The next consideration after flow and gas exchange is perfusion 46

A
C
ARTERIAL (J,N NUL& " ~
M E M B R A N E OXYGENATOR
"..VENOUS ¢.~NNUL,A
\ Jll HERARIN ~ ~ ~ I I E- ,..us,o. y . ~ .~o.,.o.s
• - - ~ L ~ h II I F ' ° W - r ~
s..~o.:oo~.,.oT I~1 I l l sAT~"'C PUMP~-'..'..'='-I,--[I I I I I POz-i'~II~J . . . . . . . . . . . "~o ot II I ° " - ~
I I
Fig 16.-ECMO circuit. A, typical per- ,~0,- = .t,T fusion circuit for infants; B, an adult I ." R
~ i i circuit diagram. (From Bartlett, R. H., et al.: J. Thorac. Cardiovasc. Surg. 73:375, 1977.) C, an infant circuit
o~ooo" diagram. (From Bartlett, R. H., et al.: Trans. Am. Soc. Artif. Intern. Organs 22:80, 1976. Used by permission.)
MEPA~]N INFI~I$10N
Pu~IP
pressure. The major determinant of line pressure is the size of the arterial return catheter. The hydrostatic pressure within the membrane oxygenator and heat exchanger are minimized by mounting them at or above the level of the patient. The diameter and length of conduit tubing should be as small as possible to minimize priming volume and slow-flow areas. In general 3/1G in. tubing is used in the newborn, 1/4 in. in infants and a/s or 1/2 in. tubing in adults. Connections and access sites should be as few as possible. These are usually combined by using connectors with
47

Luer-Lok access sites built into the side. One withdrawal and two infusion sites should be included on the venous (preoxygenator) side of the circuit, and one withdrawal and one infusion site should be buil t into the arterial side. A short bridge between the arterial and venous line should be included close to the pat ient to permit recirculation when the patient catheters are clamped. Transducers for on-line monitoring are included, and the circuit is ready for priming.
PRIMING
Priming the artificial organ circuit for ECMO requires a dif- ferent procedure than that usually used for cardiac surgery. The patient has acute cardiac or pulmonary insufficiency and may have renal failure as well. A large amount of crystalloid solution with resul tant hemodilution will lower the hematocrit and over- load the extracellular space, as well as depending on good renal function for normal clearance. Hence, a blood prime is advisable, and the constituents of the prime should be as close as possible to normal blood. Removal of microbubbles from all corners of the membrane lung is an essential step. This is done by ventilating the entire circuit with CO 2 prior to adding the first fluid 292 (making the bubbles more soluble) or by recirculating initial prime and agitating the tubing until all small air bubbles have been removed. Kolobow advocates priming the circuit under vac- uum, utilizing degassed solutionsJ TM Whatever method is used, it is best to arrive at a total filling of the system with a crystaIIoid solution of balanced electrolyte components such as Hartman's solution. This solution is recirculated until all bubbles have been cleared from the system. At that point, we add albumin (12.5 gm/L of prlme) and continue recirculation. The purpose of the al- bumin is to adhere to any irregular or active binding sites on the prosthetic surfaces, inhibiting subsequent adherence of fibrino- gen, thereby decreasing platelet adhesion and aggregation. After the albumin solution is circulated for several minutes, it is dis- placed from the circuit by whole blood. Blood should be the fresh- est available to preserve coagulation factors and platelets. If fresh blood is not available, packed red cells and fresh frozen plas- ma are used for the prime. Blood is recirculated until the temper- a ture of the prime is 37 C, the Pco~, Po 2 and pH are within an ac- ceptable range and bypass is begun. In children and infants it is mandatory to measure and regulate the sodium, chloride, potas- sium and calcium levels and the osmolarity before beginning per- fusion.
Ninety-five percent 02, 5% CO 2 is used to ventilate the mem- brane oxygenator during priming. This will maintain the Pco 2 between 40 and 50. The pH is then brought to normal range by means of bicarbonate solution or TRIS buffer, preferably the lat- ter. Water bath temperature must be carefully checked to avoid
48

overheating the recirculating blood. If citrate-anticoagulated blood is used to prime, heparin (2,000 units/L of prime) is added to prevent clotting, then calcium is added (1 gm/500 ml prime). Sodium and chloride are adjusted by adding appropriate amounts of 5% glucose or sodium chloride solutions. If potassium is over 10 mEq/L, bypass must be started very slowly to avoid cardiac arrest. The final hematocrit of the prime should be between 20 and 30%.
During priming, or any time there is fluid in the blood path of the oxygenator, it is essential to maintain adequate gas flow to prevent water accumulation in the gas phase. This can occur quite rapidly and will severely affect oxygenator function, as out- lined elsewhere. Where multiple oxygenator modules are used, a separate gas flow regulator should be used for each.
In some emergency situations it may be necessary to begin: ECMO with a nonblood prime. Some investigators even prefer this method of initiating bypass. When this is done, significant hypovolemia should be anticipated as the prime equilibrates into the extracellular space, and packed red cells will be required as that occurs.
VASCULAR ACCESS
When the artery and vein are exposed, a loading dose ofhepa- rin is given (200 units/kg) and the vessels are cannulated proxi- mally, and distally if necessary. The position of the catheters must be verified by x-ray. It is helpful, but not necessary, to pass the catheters under direct fluoroscopic control. Connections are then made to the circuit and extracorporeal circulation begun. The incisions are closed in one or two layers. No specific drains are left, as the presence of the large catheters permits free drain- age of any blood or fluid. If oozing occurs, small suction catheters are helpful to keep the wound clean and quantitate blood loss. In our experience these wounds heal primarily, and can be kept free of infection by daily changes of Betadine-soaked dressings around the catheter-cutaneous junction. If bleeding from a cannulation site occurs during the course of ECMO, the wound is opened and thoroughly explored. Often small vessels can be identified and can be successfully controlled by cautery or ligation.
Venoarterial perfusion is the technique of choice. Venous drainage is achieved by cannulation of the right atrium. The ve- nous drainage is the limiting factor in flow rate. The right inter- nal jugular vein will accept the largest-bore, shortest catheter and can be ligated distally. Others favor the iliac or femoral ap- proach; this vein must be cannulated both proximally and distal- ly. Usually a 36 F (12-mm diameter) thin-wall tube can be intro- duced into the right internal jugular vein in adults. When this is combined with a 100-150-cm siphon, flow rates of 6 L/minute can be achieved. The position of the catheter in the right atrium
49

is very important. It is easy to enter the right ventricle or the cor- onary sinus. Both of these positions have been associated with endocardial hemorrhage in laboratory preparations. For this rea- son, the tip of the catheter is passed through the right a tr ium into the inferior vena cava. The distal third of the catheter has multi- ple side holes so that all blood coming through the superior vena cava and inferior vena cava drains freely. The possibility of air embolism during venous cannulation is eliminated by phar- macologic paralysis with succinylcholine or pancuronium and positive-pressure ventilation. This precaution must be followed whenever the venous catheter is repositioned or removed. Blood. leakage from the side holes during cannulation is preventedjby an obturator.
The arterial return must be directed into the aortic arch if well- oxygenated blood is to be delivered to the brain and coronary ar- teries over the full range of flow. ~~ Blood perfused from the extra- corporeal circuit mixes with blood pumped from the left ventricle so that oxygenation of the resulting peripheral arterial blood is the average of the oxygen content multiplied by the flow for the extracorporeal and the normal cardiac system. We find right axil- lary ar tery perfusion to be the simplest, most effective means of arterial return in adults and children. Usual ly a 22 or 24 F (8- mm) catheter, which does not pose a significant pressure drop at high flow rates, can be used in an adult. Unless there is a large collateral artery distal to the cannulation site, the axillary ar tery must be perfused both proximally and distally with a small side- arm catheter. An alternative solution is to pass a long catheter from the femoral ar tery to the aortic arch. G~ The only advantage offered by this approach is tha t a single groin incision can occa- sionally be used for both venous and arterial cannulation. In our experience, venous drainage from a single femoral cannulation is often inadequate and a jugular catheter must be added. There- fore, since two incisions are to be used, neck and axillary inci- sions are considered preferable to neck and groin incisions, the la t ter being more subject to local contamination.
Cannulation technique is not difficult but does require practice in the laboratory. Catheter dislodgment is a fatal complication, so fixation must be very secure. Double l igatures are placed on the vessels (with "bumpers" included to facilitate decannulation) and tied to a ligature on the catheter. Since the patient will be hepa- rinized, absolute hemostasis is mandatory. This is achieved with liberal use of suture l igatures and cautery prior to heparinization and cannulation. Both arteries and veins respond to manipula- tion with intense spasm, so that dissection must be done care- fully, avoiding traction on the vessels until the actual t ime of cannulation. Any procedures that require skin incision and dissection should be done before heparinization. These include placement of a tracheostomy, arterial monitoring lines, central venous or pulmonary ar tery catheters, insertion of chest tubes if
5O

indicated and even placement of bladder catheters and nasogas- tric tubes, if this has not already been done.
CONDUCT OF BYPASS
After cannulation, bypass flow is instituted at a slow rate and continued until the prime is thoroughly mixed in with the pa- tient's blood. The flow rate is then increased to a level represent- ing approximately 80% of the patient's normal cardiac output. This will be approximately 2.5 L/sq m/minute. At this level of flow both systemic and pulmonary artery pulse contour will nar- row. The pulmonary artery pulse contour may disappear during the inflation phase of the ventilator. Pulmonary artery pressure will drop to normal or subnormal levels. Systemic mean pressure will usually remain normal or increase slightly in the patient whose hypoxia is improved by the procedure (see Fig 11). If the desired blood flow cannot be reached, the venous catheter is prob- ably poorly positioned or too small. The bed is raised to increase the siphon suction, and the venous reservoir is placed as near the floor as possible. With a single superior vena cava catheter it is usually necessary to raise the patient approximately 3 - 4 feet off the floor. The catheter may be repositioned for better drainage. If the systemic pulse contour disappears or the systemic arterial pressure drops before the desired flow rate is reached, the patient is probably hypovolemic. Moderate hypovolemia usually occurs during the 1st half hour of perfusion secondary to equilibration of some of the crystalloid prime solution into the extracellular space; slight loss of volume due to bleeding and complianc e of the extracorporeal circuit, and vasodilation, or more properly a relax- ation of the vasoconstriction associated with the hypoxic, hyper- dynamic state that existed prior to ECC. Blood is infused until the desired ECC flow is reached with a pulsatile systemic pulse contour, or until a limitation clearly due to the venous catheter is reached (i.e., good left ventricular stroke volume despite maxi- mum venous drainage). When the bypass flow is limited by the venous catheter and higher flows are desired, another venous access site must be added. This may be difficult in the heparinized patient but is essential if adequate support is to be obtained.
There are two schools of thought in maintaining ECC flow. The first is to maintain the flow rates as high as possible, unloading the pulmonary artery hydrostatic pressure and taking over al- most all the work of the heart and lungs. The other is to take only enough ECC flow to sustain adequate gas exchange at ventilator settings of FIo., 0.5, high tidal volume and high pressure; with this method pulmonary blood flow is higher. We incline to the former view, feeling that high ventilator pressures and elevated FIo2 m a y cause further damage to the lung. However, data sup- porting either point of view do not exist at present. Decreasing pulmonary artery blood flow to the point of total ligation does not
51

cause lung tissue necrosis. Bronchial supply in normal lungs is adequate to maintain viability. In damaged lungs slow pulmo- nary venous flow combined with thromboplastic factors may com- bine to create thrombosis; this favors the high pulmonary flow approachY, ~G
Once the desired flow rate is attained, the pa~ient no longer requires his own lung function for gas exchange. Ventilation can be managed to promote maximal lung inflation and healing with- out particular regard to gas exchange. Continuous positive pres- sure on the airway is well tolerated; in fact, it enhances flow to the extracorporeal circuit. Our practice is to reduce the Fro,, to 0,4 or less, and put 15-20 cm H20 pressure on the airway. The pa- tient often stops breathing, and is mechamcally venhlated with a low tidal volume to a peak inspiratory pressure of 30 cm of water, 6 -10 times/minute. Chest physical therapy, tracheal irrigation and suctioning and periodic flexible bronchoscopy are carried out as usual. Since the patient is totally supported by the extracorpo- real circuit, bronchoscopy and irrigation can be carried out for indefinite periods of time without risking hypoxia. If the patient has bacterial pneumonia or other processes that may respond to a specific drug, Ringer's solution containing the drug is instilled directly into the bronchus of the lobe or lung involved and al- lowed to remain in place for periods of up to an hour. Thick puru- lent sputum can be eliminated completely with this process. The use of different fluids and chemical compounds and actual venti- lation with liquid will probably play an increasing .role in pul- monary therapy, facilitated by the use of ECMO.
Oxygen requirement of patients with high metabolic rates from post-traumatic catabolism or sepsis may exceed the capacity of the circuit. In this circumstance flows over 3 L/sq m/minute are obtained, but the venous saturation progressively falls and even- tually arterial desaturation occurs. When this happens, the first tendency is to suspect malfunction of the membrane oxygenators. This can be readily checked by measuring exhaust CO 2 or calcu- lating 02 delivery from each unit. If the oxygenators are function- ing properly and inadequate oxygenation exists, then more mem- brane oxygenator units must be added to the circuit until the oxygen consumption needs are met. An alternative approach is to decrease the metabolic demand by cooling and paralyzing the patient. Usually the hypermetabolic state returns to normal after 6-12 hours of ECMO. Temperature is easily regulated by the heat exchanger in the extracorporeal circuit.
Lung function is evaluated daily by taking the patient off by- pass at Fio2 1.0 for 30 minutes (or whatever interval is tolerated) and measuring arterial and venous blood gases. Whenever the patient is taken off bypass by clamping the access catheters (for testing lung function or modifying and repairing the extracorpo- real circuit), heparin infusion is turned off, the heat exchanger is
52

turned down to 37 C to avoid overheating the blood and the oxy- genator is ventilated with 95% 02, 5% CO z to avoid respiratory alkalosis.
MONITORING THE PATIENT AND ECC
Systemic and pulmonary artery pressure are displayed contin- uously, and flow is regulated to maintain the pulmonary artery pressure at a low normal level. Pulmonary artery diastolic pres- sure and the pulmonary capillary wedge pressure will be nearly the same as the intrathoracic pressure. Measurement of central venous or right atrial pressure may not be helpful during ECC because the central venous catheter is often distorted or mis- placed by the right atrial bypass catheter, giving fictitious read- ings. Central venous pressure or pulmonary artery pressure mea- surement is mandatory for managing pulmonary or cardiac fail- ure patients before ECMO and during weaning. The extra- corporeal flow rate is monitored by an on-line flowmeter or a well- calibrated pump. When using membrane oxygenators with a high blood phase pressure drop (Sci-Med, General Electric, Travenol), it is important to monitor pressure before and after the oxygena- for. The pressure downstream from the oxygenator will represent the pressure gradient across the arterial cannula at that particu- lar flow rate. An abrupt increase in pressure drop across the oxy- genator is a sign of thrombosis. Oxygenators with a low blood phase pressure drop (Land6-Edwards) do not require careful mon- itoring, as an increase in perfusion pressure will not occur even with extensive thrombosis. Temperature in the water bath for the heat exchanger and the blood or patient should be monitored con- tinuously. Oxygenator function is evaluated by sampling mixed venous blood and blood leaving the oxygenators; 02 content and 02 delivery are calculated. When several units are used in paral- lel, the function of each unit can be evaluated by measuring COo in the exhaust gas without diverting all the blood flow througl~ each unit individually.
The most important aspect of monitoring the patient on ECC is frequent and careful measurement of coagulation status and heparin dose. It is important to use a whole blood activated clot- ting time (ACT) rather than plasma partial thromboplastin time because the interrelationship of platelet count, heparin dose and heparin activity must be included in the management. Conven- tional Lee-White whole blood clotting time takes too long to be useful as a guide to frequent changes in heparin dose. Heparin dose is regulated to maintain the whole blood ACT between two and three times normal; ACT is measured every hour, and more frequently where heparin requirement appears to be changing. Automatic clot-timing devices are used for these measure- ments.,~,, 208 The heparin requirement is approximately 50-100
53

units/kg/hour. Heparin is readily excreted in the urine, so hepa- rin requirement will increase during diuresis and decrease in renal failure; it also varies directly with platelet count.
Individuals familiar with hemedialysis often suggest the possi- bility of regional heparinization for coagulation control during ECC. In this technique a heparin antagonist, suc~'as protamine sulfate, is infused continuously into the blood return line. This technique is not applicable to major ECC because the flow rates are so fast that exact matching of heparin and protamine effects is difficult, systemic anticoagulation is required because of the large intravascular catheters and any minor error on the side of allowing thrombosis in the oxygenator may be lethal to th~ pa- tient, whereas such is not the case with dialysis.
Mechanical integrity of the circuit must be checked at frequent intervals. All connectors must be checked to be certain they are remaining tight. The fixation of the catheters to the patient should be checked every 8 hours and every time the patient is turned or moved. The function of the pump and the condition of the tubing in the pump (if it is a roller pump) should he checked every 8 hours and the tubing in the roller pump moved every 24 hours if PVC or silicone rubber tubing is used. Replacement parts for all components of the extracorporeal circuit should be easily available.
The most important factor in maintaining ECMO for days or weeks is the team. Running the procedure without mistakes re- quires continuous concentration. Human fatigue is the greatest threat to successful perfusion. At all times there should be at least one nurse caring for the patient and at least one technician or physician monitoring and regulating ECMO. Duty shifts should last no longer than 8 hours. The entire team should be repeatedly drilled in the laboratory to the point where healthy animals can be started on ECMO, maintained by the technical team for at least 48 hours and taken off routinely without mor- tality.
WEANING OFF
When lung function begins to improve, we set FIo., at 0.4, con- tinuous positive-pressure breathing (CPPB) at 20 cm H20 or tidal volume at 10-15 ml/kg, positive end-expiratory pressure (PEEP) at 5 -10 cm H~O and decrease the extracorporeal flow by slowing the roller pump (or gradually occluding the venous line when Starling pumps are used). The lowest ECMO flow is used that will maintain mixed arterial saturation over 95% (Pao2 around 60 mm Hg). When the flow rate is down to one tenth of the normal car- diac output at these settings, the patient is ready to be weaned off support. The limiting factor at this point is usually right ventric- ular function, as the pulmonary vascular resistance is often ele- vated and the right ventricle has been "at rest" for several days.
54

Ten percent cardiac output flow rate is maintained for 12-24 hours until cardiac performance has adjusted to normal function and sustained lung improvement is documented (i.e., normal gas exchange at the ventilator settings listed above). If the patient has not already received digitalis, a congener of that drug is, often helpful during the weaning process. Before decannulatV(~n, the access catheters are clamped and the circuit slowly recirculated to prevent stagnation. If the patient remains stable after 4 - 6 hours without support, the catheters are removed. The artery is repaired and the vein is ligated. The heparin is metabolized in a few hours; heparin reversal is not required.
PATIENT CARE
The patient is alert and awake with mild analgesia and seda- tion during ECMO. The anxiety of the critical care unit becomes even more intense because of the apparatus and personnel re- quired for the ECMO procedure. The attending nurse has an es- sential role in calmly and pleasantly reassuring the patient while constantly guarding against position or movements that might dislodge or kink the access lines. Keeping the patient clean, dry and comfortable, keeping the room orderly, clean and free of traf- fic and helping distraught family members adjust to the unfamil- iar and frightening scene are important considerations.
Despite the many vascular intrusions, systemic sepsis is usu- ally successfully avoided by cleaning catheter access sitesdaily with Betadine and cleaning and replacing stopcocks and infusion tubing at regular intervals. We require clean scrub suits or gowns over street clothing (primarily to discourage frequent visi- tors), but do not wear masks, favoring the psychologic Value of a friendly face over the possibility of contamination by fomites.
Except for the newborn (or the intubated patient), the patient is allowed to eat and drink. Usually, appetite will be poor and the full requirement of calories and protein is supplied by hypertonic glucose and amino acid solutions, infused directly into the extra- corporeal circuit. Serum electrolytes are measured daily; one must watch for desiccation dehydration that may occur with wa- ter loss through the membrane oxygenator.
Because of heparinization no intramuscular injections should be given, and traumatic procedures like tracheal suction must be done very carefully.
PROCEDURES DURING ECMO
Since the patient is no longer dependent on the ventilator, endotracheal tubes can be removed and changed at will, bron- choscopy can be safely done for indefinite periods of time and en- dotracheal-bronchial lavage can be done without limitation2, "' Extensive air leaks can be diminished by lowering ventilator
55

pressure. A novel approach to this problem has been reported by RatliffY 46 The segmental bronchus leading to the pleural tear is identified by sequentially occluding bronchi with a flexible bron- choscope. A radiopaque occlusive plug is introduced into the bron- chus, allowing segmental collapse until the air leak seals.
Cardiac catheterization and angiography is facilitated by ECMO support, particularly in the newborn. With dye injected through bypass catheters, congenital anomalies can be identified and the size and patency of the ductus arteriosus can be seen. Hemodialysis is easily added to ECMO, even in the newborn, by attaching the dialyzer to withdrawal and infusion sites on the extracorporeal circuit.
Any surgical procedure will lead to extensive hemorrhage in the ECMO patient unless precautions are followed. However, with extensive use of electrocoagulation, suture ligatures and platelet infusion during operation, even major operations can be done safely. This procedure should be followed for cutdowns, chest tube placement, thoracotomy, etc. If the question of intra- abdominal bleeding or viscus rupture arises, we find laparoscopy under local anesthesia a useful alternative to exploratory lapa- rotomy for diagnosis.
RESPIRATORY MANAGEMENT
The principles and practice of respiratory care are described in detail elsewhere, '3s, 24o and have not been discussed in this mono- graph. As a rule, ECMO is used when the patient fails to respond to "optimal management," which may have slight variations in different hospitals. The principles we follow 'I. ,3 are summarized briefly here.
Airway access is preferably by nasotracheal intubation, pro- gressing to tracheostomy in 3-5 days. Soft, low-pressure cuffed plastic tubes are used. Controlled mechanical ventilation is used with large tidal volumes (10-15 units/kg) at a rate that keeps the Paco2 around 40 mm Hg; FIo2 is set at the minimum level that maintains arterial saturation over 95% (Pao2 around 60 mm Hg). An intra-arterial catheter is placed for frequent blood gas sam- pling; usually a pulmonary artery catheter is placed for pressure and cardiac output measurements. Chest physical therapy, change of position and airway cleaning are done at regular inter- vals.
The results of t reatment are monitored by measurement of ar- terial and venous blood gases, cardiac output and effective com- pliance (tidal volume/unit airway pressure). Transpulmonary shunt is measured or estimated by blood sampling during 100% 02 breathing and calculation of effective alveoloarterial gradient for oxygen. Functional residual capacity (FRC) is estimated by effective compliance, transpulmonary shunt and changes in those parameters with increasing airway pressure.
56

Airway pressure is regulated to produce a normal FRC without decreasing cardiac output or O~ delivery. As PEEP is increased to achieve this goal, the tidal volume can be decreased to avoid high peak inspiratory pressure and high mean airway pressure. These ventilator adjustments are carried out during controlled or assist- ed mechanical ventilation. Patients with normal diaphragm function can be managed by high airway pressure (20-40 cm H20) and spontaneous breathing (intermittent manual ventila- tion [IMV] or CPPB). This technique has theoretical and practical advantages, and excellent results have been reported. 85
Excess extravascular lung water is always present in respira- tory failure patients, usually as a result of abnormal capillary permeability. This is minimized by (1) restricting fluid intake and giving diuretics to decrease the entire extracellular fluid space; (2) using inotropic drugs to allow maximal left ventricular function at the lowest possible filling pressure, and (3) increasing plasma oncotic pressure with concentrated albumin (when abnor- mal leakage has stopped, as judged by a test dose).
CLINICAL ECMO IN ACUTE RESPIRATORY FAILURE
To date, ECMO support for acute respiratory failure has been used in approximately 225 patients (including 35 newborn in- fants) of whom 35 ultimately survived. One quarter of this expe- rience has been accumulated by tworesearchgroups. 19, 23, 139, 1~2, ~sl Most of these patients were in a moribund condition with no chance of survival despite maximal ventilatory and pharmacolog- ic therapy. This is appropriate for the first clinical trials of a new life-support system with inherent risks, and the low salvage rate is expected.
ADULTS AND CHILDREN
The best results have been obtained in patients with acute capillary leak syndromes without infection, such as "shock lung," fat embolism and Goodpasture's syndrome. Fair results have been obtained in patients with viral or protozoan lung in- fection. The worst results have been in patients with aspiration and/or bacterial pneumonitis. As might be expected, successful cases have been those in which something could be actively done to treat the lung during ECMO, and in self-limiting diseases that required only time in healing. Most of the worldwide experience has been collected and reported by J. P. Gille of France. 122"124 No improvement in blood gas values occurred during ECMO in 40% of the cases he collected. Since adequate gas exchange can always be achieved when ECMO is properly conducted, this sug- gests that many of the unsuccessful cases were treated by in- experienced investigators who exposed patients to all the compli- cations but none of the benefits of ECMO. The worldwide ex-
57

TABLE 1 . - U S E OF ECMO FOR PULMONARY FAILURE-WORLDWIDE EXPERIENCE
AS OF J U N E 1977
DIAGNOSIS CASES SURVIVED
Pneumoni t i s (viral, bacterial , aspiration) 98 10
Capillary leak and pulmonary edema 58 13
Thromboembolism 7 1
Chest t r auma 9 0
Pneumocystis carinii 7 2
Goodpasture's syndrome 7 3
Burns 4 0
Newborn 35 6
Total 225 35
perience listed in Table 1 and the successful cases listed in Table 2 have been compiled from Gille's publications-and personal communication, n~ other publications, (references: 29, 79, 110, 114, 115, 132, 139, 141, 177, 242, 253, 264, 265, 270, 299) the NIH ECMO collaborative study 2'5, 2,s and personal experience and communication of the authors. It is the most complete pic- ture we can draw of clinical experience to date, but may contain some inaccuracies. For example, the definition of survival was 30 days after ECMO in some reports, hospital discharge in others.
Forty-three of these ECMO-treated patients constituted half of a controlled-randomized study sponsored in 1974-77 by the Lung Division of the National Heart, Lung, and Blood Institute, Nation- al Institutes of Health. ~ls This study (henceforth referred to as the "NIH-ECMO study") included nine collaborating centers follow- ing a common protocol in which optimal ventilator therapy was compared to ECMO support. Selection criteria (based on high Aa gradient despite optimal therapy) defined a group of patients with 91.5% mortality risk (4 survivors out of 47 patients treated with optimal therapy). The mortality rate was similar in those treated with ECMO (4 survivors out of 43 patients, 90.7% mortal- ity). The majority of patients in this study had viral and/or bacte- rial pneumonitis (59 out of 90), so the final results are influenced by the natural history of those disorders. However, many impor- tant observations were made on the techniques, course and com- plications of ECMO, the natural history of acute respiratory failo
58

TABLE 2 . - U S E OF ECMO FOR RESPIRATORY FAILURE*-SUCCESSFUL CASES
CASE AGE/SEX DIAGNOSIS ~IODE DURATION, LUN(~ REFERENCE) YEAR DAYS
1 24 M Shock, t rauma VA 3 Bram. HilP '6 1971 (fern.)
2 19 M Fat embolism VA 5 Brain. H~I ''~ 1971 (fern.)
3 10 F Post-AVcanal VA 3 Bram. Schulte ~G~ 1971 repair (il.)
4t 36 hi Pneumocystis VV 4 GE Geelhoed ~" 1972 pneumonia
5 I1 hi P,~eumocystis VV 10 Sci-Med Kolobow "~ 1972 pneumonia
6 46 M Viral pneumonia VA 3~/2 L-E Gannon "~ 1972 (ax.)
7 26 F Post VA 4 L-E Robertson 2~ 1973 appendectomy (fern.)
8 20 F Goodpasture's VA 3 L-E Benedict ~ 1972 9 4V2 Cystic fibrosis AV 4~/z Tray. Awad '2' 1973
pneumonia (fem.) 10 33 F Goodpasture's VA 3Y~ L-E Hanson '32 1974
(fern.) 11 37 hi Trauma, pneumonia VA 41 t~ Sci-Med Zapol ~ 1973
(arch) 12 4 F Post-tetralogy repair VA 2 Tray. Soeter 27o 1973
(ax.) 13 55 hl Viral pneumonia VA 1 RP Goulon '~2 1974
(fem.) 14 35 hi Inhalation VA 1 u RP Goulon t2~ 1974
intoxication (fem.) 15 19 M Shock, t rauma VA 5 Brain. Heiden ~ 1973
(fem.) 16 28 hi Shock, t rauma VVA 3 Bram. Heiden t~ 1973 17 20 hi Shock, t rauma VV 3 Sci-Med Pyle 2'2 1974 18 27 hi Trauma, pneumonia VA 4V2 Sci-Med McEnany ~ 1974
(arch) 19 5 hl Varicella VA 4 Sci-Med tlicks m 1974
pneumonia (ax.) 20 16 hl Myocarditis VA 3 RP Beaufils ~ 1974
(fem.) 21 22 F Post-tetralogy repair 4Yz RP Ohressor "2 1975 22 17 F Goodpasture's VA 4 L-E Bartlett z3 1975
(ax.) 23 19 F Pulmonary emboli VA 5 Sci-Med Cooper 6~ 1975
(arch) 24 36 hi Viral pneumonia VA 2 Sci-Med Zapol ~ 1975
(arch) 25 26 F Aspiration pneumonia VA 1 I rE Proctor =~ 1975
(fern.) 26 23 F Post-sepsis VA 4 Sci-Med Morris ~'" 1976
(aorta) 27 1 F Aspiration pneumonia VA 3u L-E Bartlett ~ 1976
(car.) 28 18 hi Sal twater VA 3 Tray. McNamara ~2 1976
drowning (ax.) 29 24 F Fatembolism VA 5u Tray. McNamara :~2 1977
(ax.)
*Excluding newborn infants. ?Died 6 weeks later.
ure and the advantages and limitations of ECMO life support. Our center was one of the collaborators in this study, and some of the information in this section is derived from that experience.
TECHNIQUES.- A study of the successful ECMO cases shown in Table 2 provides some insight to correct clinical application.
59

Twenty-three patients were treated with VA bypass, 3 with VV and 2 with other methods. Arterial re turn was directly to the aor- tic arch in many but not all cases. Six different membrane oxy- genators are represented. A wide variety of vascular access cathe- ters, connectors, occlusive and nonocclusive pumps a n d monitor- ing equipment were used. Anticoagulation was acl~ieved by con- t inuous heparin infusion in almost all cases. Time on ECMO ranged from 1 to 10 days. Several patients have been perfused for more than 2 weeks. The longest perfusion on record is 19 days. ~39 However, the average t ime of successful ECMO cases is 4 days of perfusion, indicating that lung function usually improved rapidly on ECMO, if it improved at all. Venti lator management was not discussed in detail in all the case reports, but FIo2 was n~ain- rained below 0.5, and ventilator pressures as low as possible in the successful cases where that information could be obtained.
PATIENTS. -- The pat ient population in successful cases is pri- mari ly made up of those with capillary leak syndromes and other self-limiting or treatable disorders. Three had Goodpasture's syndrome. This rare disorder causes severe pulmonary failure very rapidly so that patients are seen and treated early. It re: sponds to immunosuppressive therapy and/or nephrectomy, is self-limiting with a short natural history and usual ly resolves to healing rather than fibrosis. Hence patients with Goodpasture's syndrome are ideally suited for ECMO support. Pat ients with acute respiratory failure related to immunologic suppression have many of the same characteristics. Successfully" treated pa- t ients were usually started on ECMO early in the disease. Fifty- five percent of the survivors were men. The age range of survivors extended from 1 year to 55 years.
COMPLICATIONS. - - T h e NIH-ECMO study~provides the first measurement of complications in a large consecutive series of patients. The results were similar to those reported in other se- ries and in anecdotal communications. Abnormal bleeding occurs in virtually all ECMO-treated patients secondary to hepariniza- tion and thrombocytopenia. Bleeding was considered a significant complication in 16% of the NIH-ECMO study patients, 2~s in 7% of our series, ~9, 23 in 19% of Hill 's series '39 and in 34% of the cases collected by Gille. TM
Bleeding complications range from oozing at cannulation and operative sites to fatal gastrointestinal, nasopharyngeal or intra- cranial hemorrhage. Intracranial bleeding is the most feared of all complications. It rarely occurs spontaneously, but often occurs in patients who have sustained head t rauma as part of their ini- tial injury. For example, intracranial bleeding occurred in all four of the head t rauma patients we treated with ECMO. 23 With careful hemostasis during operations, frequent measurement and control of heparin anticoagulation and judicious use of platelet
60

transfusions, blood requirement can and should average less than 1 unit/day.
Mechanical complications occur, but are usually successfully managed by changing the component part. Oxygenator blood leaks or malfunction due to water in the gas phase have, become unusual as manufacturing and user techniques have improved. Tubing leak or rupture, oxygenator thrombosis, electric or me- chanical pump failure and so on, occurred in 35% of the NIH- ECMO study patients, 2~s but none of these technical complica- tions was fatal.
Considering the opportunity for infection, the actual incidence of sepsis is quite low (20% positive blood cultures for both ECMO patients and '~controls" in the NIH-ECMO study). Septicemia occurred in three of our first six patients. Following that experi- ence, we adopted the protocol of daily Betadine washing of cannu- lation sites with application of Betadine ointment, limiting blood access ports to infusion or withdrawal only and cleaning all stop- cocks with alcohol after each use. Major broad-spectrum antibiot- ics are rotated every 5 days. Positive blood cultures occurred in 1 of the next 33 patients in our series. When septicemia does occur, it is almost always related to invasive sepsis in the lung or else- where, ra ther than contamination through the extracorporeal circuit or cannulation.
RESOLUTION OF ACUTE PULMONARY FAILURE.-- Only a few years ago it was a s s u m e d - or at least h o p e d - that in most cases, acute pulmonary failure would resolve to normal lung function if t ime and lung rest could be provided by ECMO support. Unfortu- nately, the experience to date has shown that in most cases, by the time the patient has reached a moribund condition the lung is irreversibly damaged, and resolution proceeds to acute fibrosis rather than normal architecture. This phenomenon has been ob- served in all types of patients, whether life support is provided by ECMO or by ventilator techniques. 15~ Irreversibility, secondary to fibrosis and/or bacterial infection, is the major cause of failure in ECMO-treated patients. For this reason, the pres- ence of fibrosis is now considered a contraindication to ECMO support. Fibrosis is suggested by a high pulmonary vascular re- sistance unresponsive to local vasodilators and by extremely low lung compliance. It is confirmed by direct lung biopsy.
The cause of acute pulmonary fibrosis following interstitial edema is not known. Fibrosis does not occur following episodes of high-pressure low-protein pulmonary edema from cardiac failure. This suggests that fibrosis is s t imulated by some large-molecular- weight compound or particle that enters the lung interstitial fluid following pulmonary capillary damage. Hill and Ratliff et al. studied lung histology in 42 patients with acute respiratory fail- ure, many of whom were treated with ECMO. ~s~ Early reversible
61

disease was characterized by interstit ial edema and round cell infiltration. Irreversible disease was associated with fibroblasts, destruction of architecture and collagen formation. Fibrin or fibrinogen were identified by immunofluorescent staining tech- niques in 85% of cases of Hill et al. The study of the pathogenesis and prevention of acute fibrosis is the next phase rg~luired in ad- vancing the t rea tment of acute respiratory failure. Such study depends on development of a reproducible animal model of this syndrome.
FOLLOW-UP STUD~Es. -- Patients Who recover from acute pul- monary failure generally return to normal lung function within 1 year. Decreased lung volume, decreased compliance and mod~er- ate abnormalities of gas exchange characterize the early period of recovery and may represent some areas of fibrosis that ul t imately disappear or convert to small amounts of innocuous scar tissue. The most complete late follow-up study of these patients has been reported by Fal la tY
CASE EXAMPLEs. -- Typical applications of ECMO in adult res- piratory failure are shown in Cases I and 2.
CASE 1.-P.G. was a woman, 29, whose pregnancy had reached term, at which time the fetus died. Following induction of labor, she had era- bolism of amniotic fluid to the lung plus disseminated intravascular co- agulation (DIC) with hemorrhage and shock. After appropriate treat- ment with fresh blood and fibrinogen, all organ systems recovered except
Fig 17. - Case 1. Pulmonaryfunction improved (decreasing Aa gradient) during the first 3 days of ECMO support, and ECMO was discontinued. However, lung function deteriorated and did not recover (high fixed Aa gradient) during a second prolonged perfusion. (Figs 17 and 18 from Fong, S. W., et al.: Trans. Am. Soc. Artif. Intern. Organs 20:239, 1974. Used by permission.)
EFFECTIVE A /o GRADIENT 600
(OFF BYPASS)
OzCONT[NT A,FUePA~rs 20 OaPI"ART[RIAL =,VENOUS
BYPASS PLOW L/fn,n
* , C~01AC 0UT~JT IL/mm
(OFF ~FASS)
62
BYPASS - -
s 6 r e 9 o i~ ~ 13 ~ i~ .~ IT ,e m zO El - -OFF BYPAss~T ON BYPASS E;(
DAYS

the lungs. After maximal respiratory assistance for 3 days, the pulmo- nary insufficiency index (PII) was 9.0, and ECMO was instituted.
For this patient, who weighed 71 kg, five Land~-Edwards 3 sq m units in parallel were used for VA bypass; bypass was established through the internal jugular vein and axillary artery. A flow of 4 - 5 L/minute was obtained.
The course is illustrated in Figure 17. Near total bypass and oxygen delivery were maintained for 4 days while the lungs improved, as shown by a decreasing Aa gradient. When an arterial Po 2 greater than 60 mm Hg could be maintained at an F1o., of 0.6, bypass was discontinued. Lung function deteriorated over a 3~day period, and ECMO was reinstituted for 12 days. Pulmonary function did not improve, as shown by the fixed Aa gradient. Pneumonia with gram-negative organisms supervened, associated with septicemia on the 12th day. Septicemia cleared on appro- priate antibiotic therapy despite continuing ECMO. Postmortem exami- nation revealed irreversible lung damage characterized by fibrosis and necrotizing pneumonitis. No evidence of DIC, emboli or other potential complication of ECMO was found.
Review of the coagulation status prior to ECMO showed prolongation of the prothrombin time and thrombin time, which may be explained by the high level of FDP present (Fig 18). During the first period of bypass, the most remarkable change was a decrease in FDP and continued rise
Fig 18.-Case 1. Coagulation studies during ECMO. The pattern of consump- tion coagulopathy treated with fresh plasma was present before ECMO. Im- provement occurred during ECMO (rising platelet count, falling FDP and throm- bin time). (ACT = activated clotting time; PTT = partial thromboplastin time, prothrombin time; TT = thrombin time; FDP = fibrin degradation products.)
P.G
AC"
OAYS
63

in coagulation factors. During the second period of ECMO, there was persistent prolongation of the prothrombin time, without liver enzyme elevation, and an increase in thrombin time without elevation of FDP.
Heparinization inhibited platelet adhesiveness and platelet factor III availability to a greater degree than aggregation ofplatelets by ADP. On day 12, the platelet count dropped to 75,000/cu mm with the develop- ment of septicemia. Subsequent deterioration in platelet function may be related to decreasing platelet concentration or septicemia.
This case demonstrates the use of physiologic measurements to provide indication for ECMO, and prompt reversal of pulmonary capillary leak with VA bypass. Abnormal coagulation status caused by the basic disease improved during ECMO. In retro'- spect, ECMO was discontinued before the capillary leak had "healed," and interst i t ial edema recurred, which led to infection and fibrosis despite ECMO support. If the initial period of ECMO had been continued until lung function was almost normal (as we would now do), the outcome might have been different.
CAS~ 2.--L.M., a 17-year-old girl, was hospitalized in March 1975 in Albuquerque, New Mexico, with typical acute nephritis complicated by hemoptysis. Goodpasture's syndrome was documented by immunoflu- orescent studies of renal and lung biopsy specimens; high titers of anti- basement membrane antibody were found in the circulating plasma. She was treated with prednisone, heparin, Imuran and Persantine without improvement. Finally, gross hemoptysis occurred, and the trachea rapid- ly filled with blood and clots. Despite intubation, mechanical ventilation with ventilator pressure at 80/15 cm H~O and an FIo~ of 1.0, the Pao., was 45 mm Hg. Chest x-ray films are shown in Figure 19. Our team was con- sulted and arrived in Albuquerque with the ECMO appm:atus 8 hours later; ECMO was instituted by insertion ofcannulas through the jugular vein and axillary artery. Three 3 sq m Land~-Edwards oxygenators were used. Gas exchange and perfusion improved dramatically, but a fourth oxygenator had to be added for total cardiopulmonary bypass. Data during the ECMO period are shown in Figure 20. During total by- pass, the endotracheal tube could be removed, and bronchoscopy was per- formed twice to remove blood from the trachea and to examine the smaller bronchi. Further bleeding into the lung was minimal despite heparinization for ECMO. The patient became alert and responsive. The
Fig 19.-Chest x-rays in Case 2. Intrapulmonary hemorrhage secondary to Goodpasture's syndrome seen on day 1. ECMO cannulas in place on day 5. Clear lung fields just before discharge on day 15. (Figs 19-21 from Bartlett, R. H., et al.: J. Thorac. Cardiovasc. Surg. 73:375, 1977. Used by permission.)
64

FIOz
|.0-
,5-
O-
150-
PRESSURE I00-
~ o SYSTEMIC ,50 X" PULMONARY
O"
POz ~.- PUMP ART. O-PT ART.
D-VENOUS i ( /
il- 4
ECMO FLOW RATE L/" ra in
0 PRE 0
30 60 90 I10 HOURS OF BYPASS
Fig 20.-Case 2. Data during ECMO support. The FIo2 was kept at low levels except during transport on the 2d day, and the patient was weaned from ECMO between hours 60 and 110. During this time Pao 2 was maintained around 100 mm Hg, and PA pressure was normal with gradually decreasing ECMO support.
following day we transported the patient, supported by near-total car- diopulmonary bypass, to University of California at Irvine Medical Cen- ter with the aid of the United States Air Force. Pulmonary function im- proved, as shown by daily testing with the patient off ECMO (Fig 21). Bypass flow was gradually lessened and finally terminated after 4 days. Four days later the patient no longer required the ventilator, and she was discharged 2 weeks later on hemodialysis.
We had planned to do a bilateral nephrectomy as soon as the patient's condition was stable on ECMO; however, the hemoptysis had ceased de- spite heparinization, and pulmonary function was improving. Therefore, we elected to manage the immunologic syndrome with prednisone, 1 mg/kg, and Cytoxan, 0.5 mg/kg. Pulmonary function continued to im- prove, although the patient became anuric. Total renal failure was anti- cipated, and a program of long-term hemodialysis was begun. Several months later renal function began to return, and 1 year after the illness the patient was off hemodialysis with normal pulmonary and renal func- tion.
Typical positioning of VA bypass catheters is shown in Figure 19. Five liter/minute flow was maintained during the first 2 days when lung func- tion was minimal. This permitted the use of low FIo., (except during air transport), so that total 100% 02 exposure was less than 36 hours during the entire course of management.
INDICATIONS.--To p a r a p h r a s e Dwigh t H a r k e n ' s axiom regard- ing medical devices: ECMO should be used in acute revers ib le
65

AIo OOa
~00M l/~IR
6O
PCOz pH O �9
40-
20
ECMO FLOW RATE L / r a i n
0 4 8 12 16 DAYS
Fig 21.-Case 2. Blood gases during extracorporeal support (shaded area) were measured after short test periods off ECMO at FIo2 1.0. Lung improvement, signified by decreasing Aa/Do 2, occurred on the 2d ECMO day.
lung disease when the risk of the procedure is less than the risk of the disease. The incidence of serious complications of ECMO, in- cluding mechanical failure and infection, is less than 20%. Conse- quently, the use of ECMO is certainly justified in treatment of patients with 90% mortality risk, perhaps in patients with 75% or 60% mortality risk. To define an exact figure as indication for ECMO implies that a method exists to measure pulmonary fail- ure and predict mortality risk. This will be discussed subsequent- ly. Patients with severe fibrosis demonstrated by biopsy, indicat- ed by high fixed pulmonary vascular resistance or suggested by extremely poor compliance after treatment of interstitial edema have irreversible disease and in general would not be helped by ECMO support. Most patients with acute lung disease of more than 10 days' duration are in this category; consequently, 7-10 days of intubation and ventilation is currently considered a rela- tive contraindication to ECMO support. If fibrosis could be pre-
66

vented or reversed by pharmacologic therapy, l~n 30., then ECMO would provide the time required for drugs such as penicillamine ~2T to act. Other contraindications include those conditions that severely limit the quality of life: incurable malignancy, severe brain damage and other chronic incurable disorders. Other ma- jor acute organ failure, such as renal failure, is not a contram- dication, nor is coagulopathy or intravascular coagulation.
Acute respiratory failure may be caused by pneumonitis, aspi- ration or inhalation capillary leak syndromes, chest trauma, car- diac i'ailure, fluid overload, thromboembolism or primary lung disease. Overall mortality risk for patientswho require intuba- tion and mechanical ventilation ranges fron~ 20% "to 60%. In a multicenter study of 490 patients (age 12-65) who required intu- bation and whose FIo2 was greater than .05, the mortality was 61%. Three hundred thirty-seven of these patients had multiple organ system failure (of which 71% died). However, the mortality risk of 153 patients with respiratory failure only was 41%, de- spite optimal ventilator management/17
The severity of acute pulmonary failure can be measured through a technique described as a pulmonary insufficiency index (Pii).ls, 21. ls~ This index is based on a graph of effective alveolo- arterial gradient for oxygen versus time, starting with intuba- tion. Mortality risk for those on mechanical ventilation with PII over 3 is well over 50%. Mortality risk at PII 6 is approximate- ly 90%, and only 3 survivors had PII greater than 10 in our ex- perience with 306 cases.
Another method of detecting the high-risk patient with revers- ible lung disease is to establish contraindications based on prior unsuccessful experiences. This approach has been taken by Hill, Ratliff, Fallat 1s2 and their group. By sequential measurement of alveoloarterial gradient at different levels of FIo2 and PEEP, they were able to define a group of patients with a high fixed shunt who had a uniformly poor prognosis. This physiologic change correlat- ed with the presence of fibrosis on lung biopsy or autopsy, and in general was associated with a long initial illness (more than 7 days). Hypercapnia and consumption coagulopathy were also bad prognostic factors. Conversely when physiologic testing shows a variable shunt that improves with higher PEEP levels, the lung lesion is probably still reversible.
Detection of irreversible lung damage based on pulmonary vas- cular resistance was recently reported by Zapol and Snider/~ They measured pulmonary vascular resistance and right ventric- ular function in 30 patients with acute respiratory failure. Revers- ible lung damage was associated with decreasing pulmonary vascular resistance, whereas increasing pulmonary vascular re- sistance was associated with pulmonary fibrosis and death. We have reported similar findings/5 with progression to total pul- monary vascular occlusion in one patient maintained alive with ECMO.
67

All of these methods were developed to determine the revers- ibility of lung damage (i.e., the extent of architectural disruption and fibrosis) without actual lung biopsy. Histologic evidence of destroyed lung architecture and fibrosis, described by Ratliff and Hill '5~ and others '~, 2,s is the definitive evidence ofjrreversibil i ty and a contraindication to ECMO in the current sts of the art.
Based on all these considerations, the indications for ECMO in children and adults are: acute reversible lung disease (no physio- logic or histologic evidence of fibrosis), lack of response to optimal therapy and high mortal i ty risk (PII over 3 and rising). Contrain- dications are: irreversible lung damage, PII over 12, duration over 10 days, CNS disorders, incurable chronic disease and active bleeding.
SUMMARY. -- From the worldwide experience with ECMO in children and adults the following conclusions can be drawn: (1) when done properly, ECMO can provide near total pulmonary support for 2 - 3 weeks; (2) if lung function improves during or because of ECMO, this usually occurs during the first 5 days; (3) ECMO is most useful in diseases that are self-limiting, or that can be treated definitively; (4) the major cause of failure is irre- versible lung damage, not technical complications; (5) acute pul- monary fibrosis can occur quickly and seems to be related to the durat ion and nature of interstit ial edema fluid. This makes it particularly important to measure pulmonary failure and there- by to identify the high mortal i ty risk patient early in the course of the disease; (6) ECMO support is a futile exercise in end-stage acute pulmonary failure (until lung transplantat ion or prosthesis implantation is clinically feasible).
NEWBORN RESPIRATORY FAILURE
Throughout the 1960s, respiratory distress syndrome (RDS) of the newborn was a major stimulus to ECMO research and de- velopment. It seemed an ideal disease for ECMO support-a high-mortality (50%) disorder, easily diagnosed, apparently to- tally reversible with time, occurring in patients small enough to be totally supported by the small prototype oxygenators of that decade. Rashkind et a]. TM attempted extracorporeal gas ex- change, using a femoral arteriovenous shunt through a small bubble oxygenator. For reasons outlined earlier, any low-resis- tance arteriovenous mode of ECC will inevitably be unsuccessful for pulmonary support. Dorson and colleagues s~ 8, (1969) first evaluated ECMO support in the newborn, using a capillary membrane oxygenator and umbilical vascular access. These ex- periments were unsuccessful, although the protocol was designed to test the feasibility of the technique in moribund infants rather than to achieve patient survival. White and others 296, 29, (1970) used ECMO support for 2, 3 and I0 days in three infants with
68

TABLE 3.-RESULTS OF ECMO IN NEWBORN RESPIRATORY FAILURE (AUTHORS' SERIES)
NUI*,IBER IMPROVED* SURVIVED
Respiratory distress syndrome (RDS) 4 2 1
Meconium aspiration syndrome (MAS) 8 4 3
Persistent fetal circulation syndrome (PFC) 4 3 2
Total 16 9 6
*"Improved"=satisfactory lung function at FIaz of 0.5 offECMO.
RDS. They used umbilical vessels for vascular access and evalu- ated several modes of bypass. None of the infants survived, but the feasibility of ECMO in the newborn was demonstrated. In 1970 the mortality rate from RDS dropped dramatically with improved perinatal and ventilator management techniques. At the same time adult-sized oxygenators and circuits became avail- able for clinical testing, so attention shifted away from newborn RDS. Pyle et al/42 and others attempted newborn cases without success. The problemsidentified in these early studies were: inad- equate flow through the long, narrow umbilical catheters; renal failure; coagulopathy, and intracranial bleeding.
With laboratory studies and the early clinical experience de- scribed above as a base, the authors with neonatologist Robert Huxtable, surgeon John German and many other collaborators have used ECMO in 16 newborn cases. Nine infants improved and 6 ultimately survived. 24 Since this is the only successful ex- perience with ECMO in the newborn to date, we will refer only to this series in the discussion that follows (Table 3).
Pulmonary parenchymal dysfunction in the newborn is caused by respiratory distress syndrome (RDS, hyaline membrane dis- ease), meconium aspiration syndrome (MAS), persistent fetal cir- culation syndrome (PFC, with or without congenital diaphrag- matic hernia) or streptococcal pneumonitis. All of these syn- dromes are treatable and reversible with time. With improved techniques of care the survival rate has been greatly improved in the last few years, but respiratory failure still remains the most common cause of death in the newborn period. 2~6 Management is complicated by the fact that the treatment itself (high FIo~ and high airway pressure) is damaging to the lung, and may lead to a chronic lung disease known as bronchopulmonary dysplasia/2~ Coagulopathy is common. 51 Intracranial bleeding occurs in at least 60% of fatalities from newborn RDS. 13T
Our patients were selected by neonatologists when there ap- peared to be no chance of survival with continuing maximal
69

therapy. This clinical judgment was corroborated by uniformly greater than 90% mortality risk when pulmonary failure was measured by the newborn PII. The best results were obtained in MAS, followed by RDS and PFC. Intracranial bleeding occurred in 43% of the patients, less than the expected 60%
TECHNIQUES.--The extracorporeal volume is approximately 500 ml, which may be more than twice the patient's blood vol- ume. Therefore, it is particularly important that the prime be as close to normal blood as possible. When citrate anticoagulated blood is used for the prime, serious problems are hypocalcemia, acidosis and hyperglycemia. It is much safer to use freshly drawn heparinized blood for priming the extracorporeal circuit.
Vascular access via the umbilical vessels is obviously the first consideration. After all, the patient has been sustained by arte- riovenous shunting through the placenta for the past several months. The newborn infant is no longer a fetus, however, and gas exchange through an artificial placenta does not provide ade- quate support in newborn RDS. The extracorporeal circuit must be capable of total cardiac and pulmonary support, since total pulmonary failure or right ventricular failure may occur in any patient. The right internal jugular vein is the largest extrathorac- ic vein in the newborn and can be ligated with impunity. The carotid arteries are the largest extrathoracic arteries in the new- born, in fact, the only vessels with access to the aortic arch large enough for arterial return. Collateral circulation to the brain is evaluated by temporarily clamping the common Carotid under local anesthesia and verifying normal neurologic function. Col- lateral circulation through the external carotid an~d vertebral systems has always been adequate. We have not repaired the ves- Sels after ECMO, since the risk of thrombus formation and distal embolization from the abraded intima seems greater than the risk of late complications.
Even though the extracorporeal blood volume is much larger than that of the infant, hemodynamics and fluid balance remain stable because the extracorporeal volume remains constant. Elaborate systems have been devised for continuously weighing the patient and adding and subtracting blood from reservoirs, 2s5 but these have not been necessary in our experience. Arterial pressure is monitored continuously via an umbilical artery cathe- ter, and blood volume adjusted to maintain normal newborn per- fusion pressure. Blood sampling is done from the same catheter. In premature infants it is important to keep the arterial Po 2 be- low 70 mm Hg to avoid retrolental fibroplasia. The arterial Po 2 is the result of mixing hyperoxygenated perfusion blood with deoxy- genated blood shunting through the lungs and out the left ventri- cle. If a right-to-left ductus arteriosus shunt is present (in PFC syndrome), Po 2 must be monitored in an artery above the ductus (such as the superficial temporal) to avoid high 02 exposure to the eyes.
70

Lung recovery usually occurs during the first few days on ECMO, and the average perfusion time is 4 days. In two success- ful cases of PFC, the infants were on bypass for 7 days and 11 days, however.
Measurement and control of anticoagulation is even more im- portant in the infant than in the adult. Consumption coagtilopa- thy from pre-existing hypoxia, acidosis and poor perfusion is the rule. This is compounded by the inability of the premature infant to synthesize some coagulation factors. The heparin requirement is greater than that in the adult (approximately 80 units/kg), possibly because the ratio of foreign surface to blood volume is much greater in infant ECMO. Thrombocytopenia is more pro- nounced in the newborn, probably for the same reason. Plasma clotting factors are assessed frequently by neutralizing heparin with Polybrene (50 ~g/ml of blood) and measuring thrombin time, prothrombin time and partial thromboplastin time. Fresh frozen plasma is given periodically to maintain these screening test values near the normal range. A single unit platelet trans- fusion will raise the platelet count for 18- 24 hours. Spontaneous bleeding can occur with platelet counts less than 20,000/cu mm. Our arbitrary policy is to infuse platelets whenever the platelet count falls below 50,000/cu mm. One or two units of platelets per day are usually required to maintain this level.
PATIENT CARE. - - Once ECMO is established, FIo., is decreased to 0.4 or less and'peak inspiratory pressure is decreased to 20 cm of water or less. End-expiratory pressure can be set at any level without interfering with hemodynamics. We use no PEEP in MAS and high PEEP (5-10 cm water) in RDS and PFC. Exten- sive lavage can be carried out in MAS. The endotracheal tube can be changed without urgency. After 6-12 hours of ECMO the pa- tient stablizes at the desired flow rate, the ACT returns to low levels (following metabolism of the heparin given for cannulation) and a patent ductus arteriosus may close in response to adequate oxygenation in the aortic arch. At this point blood sampling, pres- sure and arteriographic studies should be done if there is reason to suspect congenital heart lesions or patent ductus arteriosus. If a patent ductus arteriosus with either right or left shunting is present, thoracotomy and ductus ligation will almost certainly be required and should be done without delay.
Ductus ligation (or any other operation) can be done successful- ly during heparinization and ECMO as long as the principles out- lined earlier are followed. Renal failure is usually related to de- creased pulse pressure caused by ECMO and compounded by the damping effect of a large patent ductus. In our experience ductus ligation usually leads to resumption of renal function. Renal fail- ure can be treated with dialysis, simply by attaching the dialyzer to the extracorporeal circuit. Fu l l intravenous alimentation is begun when ECMO is stablized. No feedings are given into the gastrointestinal tract for the first 2 weeks of life, with the hope of
71

preventing necrotizing enterocolitis. Insensible water loss will be increased by evaporative losses from the oxygenator, so that ap- propriate fluid replacement must be planned.
COMPLICATIONS.--Intracranial bleeding occurred in 43% of our patients. One patient with PFC was suecessfull:~..off ECMO and improving when intracranial bleeding occurred, associated with a platelet count of 12,000. This 43% incidence was lower than a 58% incidence in a comparison group of patients with pulmonary failure not treated with ECMO. This implies tha t the cause of intracranial bleeding in newborn respiratory failure is related more to poor perfusion and oxygenation, acidosis and high venti- lator pressure than it is to bleeding tendency. Major ble~ding from other sites did not occur, nor did infection.
FOLLOW-UP. -- Five of the 6 newborn survivors have had normal growth, development and psychomotor test results. One infant who originally had PFC associated with a right-sided diaphrag- matic hernia and a small left lung has barely enough pulmonary function to sustain life. He is still hospitalized at 12 months of age.
CASE EXAMPLES.--Typical applications of ECMO in newborn respiratory failure are shown in Cases 3 and 4.
CAsE 3.--This full-term newborn male sustained massive meconium aspiration at birth. He required intubation, mechanical ventilation and high FIo2 but remained hypoxemic and acidotic. This combination carries an extremely high mortality, and ECMO support was instituted, using jugular and carotid access. The lungs were lavaged during VA support. Lung function improved gradually over a 3-day period, and ECMO was discontinued. The patient was extubated shortly thereafter and survived with no sequelae. The clinical course is shown in Figure 22.
Meconium aspiration syndrome is best managed by prevention or early lavage in the delivery room. Even when it occurs, mortal- i ty and morbidity is low. However, when it is followed by severe respiratory failure, mortal i ty risk is nearly 100%. The lesion is mechanical and easily reversible; hence ECMO support is an appropriate means of treatment.
CASE 4.--H.L. was born at 34 weeks of gestation; the birth weight was 1,840 gin. Typical findings of RDS were noted shortly after birth, and the child was transferred to the neonatal intensive care unit at University of California at Irvine Medical Center. Despite supplemental oxygen, CPPB, endotracheal intubation and eventually mechanical ventilation, hypoxia and hypercarbia persisted. At 13 hours of life, arterial blood gas values were: Po 2 45 mm Hg, Pco 2 44 mm Hg, and pH 7.33 at an Fro,, of 1.0 and a ventilator pressure of 32/4 mm Hg. The clinical course is shown in Figure 23. Interstitial emphysema and bilateral pneumothorax required placement of chest tubes. Pulmonary function did not improve despite maximal management at 60 hours of life. Neurologic function was nor- mal. The neonatologists considered a trial of ECMO support indicated, and ECMO was instituted through cannulas in the jugular vein and carotid artery at flow rates of 120-140 ml/minute; FIo~ and ventilator pressure were turned down, and the air leak diminished. Lung function
72

d J / r
, , , . . . . . . |
FI02 I I
FlOW 150 r
75
:30 60 90 f20 150 l~t0 HOURS OF LIFE HOURS OF ECMO
j / \ MECOmUM
�9 \ + .
HOURS OF LIFt 0 3o eo 9o I~ ~so wo HOURS OF ECMO I~t 2'4 3~ 4'~ e~o
Fig 22.-Case 3, newborn, MAS. This infant was failing despite mechanical ventilation with high pressure and 100% oxygen. Ventilator pressure and FIo 2 could be decreased during ECMO support, and the baby was weaned off ECMO during the 3d day. Blood gas data were taken during brief test periods off ECMO.
improved during the 2d day of ECMO; ECMO was continued at lower flow rates, and the baby was weaned offECMO after 70 hours. Heparini- zation titer was based on whole blood ACT. Thrombocytopenia occurred, but there was no bleeding. The baby was extubated 6 days later and dis- charged at age 44 days. Growth, development and psychomotor function are normal at age 1 year.
73

A .
1 2 3 4 5 6 7 8 9 10 11 12 DAYS
Fig 23.-Case 4, newborn, RDS. Bilateral air leaks occurred during high- pressure 100% 02 ventilation. These sealed when airway pressure was de- creased during ECMO. Lung function improved promptly, as shown by Aa/Do 2 measured off ECMO. (From Bartlett, R. H., et al.: J. Thorac. Cardi0vasc. Surg. 73:375, 1977. Used by permission.)
For infants with RDS who weigh more than 1,500 gm at birth, the prognosis generally is good (10-20% mortali ty rate). How- ever, extensive bilateral air leaks may preclude adequate venti- lation, as was the case in this baby; ECMO support permits lowering of airway pressure and FIo2, so that air leaks can seal and late onset of bronchopulmonary dysplasia may be prevented. A patent ductus arteriosus was probably present in this child, al though the echocardiogram indicated it was not hemodynami- cally significant. The ductus appeared to close in response to the oxygenation produced by ECMO.
INDICATIONS. -- In our hospital, ECMO is indicated in the new- born infant at greater than 90% mortal i ty risk with maximal venti lator therapy, provided no contraindications exist. Mortali ty risk can be measured by methods described by Stahlman ~76 and SilvermanY 69 However, these methods were described before the use of CPPB. O'Connor ~22 from our laboratory devised a method for measuring newborn respiratory failure (and thereby defining mortal i ty risk), using as a base the same analytic principles as for
74

the adult PII. The method (NPII) is simple, applicable retrospec- tively or prospectively and provides a single-number cumulat ive index of oxygen requirement, acidosis and time.
All of the 16 newborn ECMO patients were started on ECMO at a NPII level that indicated mortal i ty risk greater than 90%; 10 of these were above 100%. Hence the 37% survival rate can be compared to the survival ra te (less than 10%) in a large group of patients with similar severity of disease.
SUMMARY. -- Early results with ECMO in newborn respiratory failure are encouraging. The survival rate is iDcreased and the incidence of intracranial bleeding decreased compared to a simi- lar group of patients. Important factors in the success of this tech- nique are: (1) high-mortality-risk infants were detected soon af- ter birth and started on ECMO when high mortal i ty risk was ob- vious; (2) VA bypass with perfusion of the aortic root even during low bypass flow rates was achieved by jugular and carotid cannu- lation; (3) the disorders causing newborn respiratory failure are reversible in a short period of t ime or t reatable by lavage and ductus ligation; (4) FIo,, and airway pressure were maintained at nondamaging levels during ECMO; (5) the disorders causing re- spiratory failure in the newborn generally do not include capillary leak syndrome and do not progress to fibrosis. The implications of these observations for lung disease and ECMO support in the old- er child and adult are obvious.
Respiratory distress syndrome and MAS account for at least 90% of respiratory failure patients. Both of these syndromes are preventable with careful prenatal and intranatal care; hence the incidence of newborn respiratory failure should decrease dramat- ically in the next decade. The technique will be most often used in cyanotic hear t disease and PFC.
CLINICAL ECMO IN SHOCK
CARDIAC FAILURE
Part ial or total VA bypass provides excellent support for the failing heart. In fact, partial cardiopulmonary bypass is used dai- ly in the operating room for temporary support after cardiac oper- ations and is maintained while the hear t re turns to normal tem- perature and contractility. With borderline cardiac reserve, this may be continued for an hour or more. Following the same princi- ple, VA bypass may be established under local anesthesia be- fore general anesthesia and thoracotomy in high-risk cardiac patients,65,,s5 or in patients with massive pulmonary embo- lism.32, ,86 Cardiopulmonary bypass has also been used to support the circulation during other surgical procedures in patients with cardiac disease.~6~
75

LEFT VENTRICIJLAR suPPOXT.--Counterpulsation, or systolic pressure unloading with diastolic augmentation, was originally proposed as a type of arterioarterial extracorporeal circulation by Harken and associates. TM Intra-aortic balloon pumping TM is a simplification of counterpulsation that is now widely applied2 6 Counterpulsation by external body compression ~r~d decompres- sion achieves similar results without vascular invasionY 9 Coun- terpulsation is effective in resting the left ventricle and simulta- neously improving systemic perfusion. In conjunction with phar- macologic therapy, it has become the method of choice for tempo- rary treatment of severe left ventricular failure. As with ECMO for pulmonary support, aortic balloon pumping is most uw when active therapeutic intervention (such as a coronary byi~ass graft or replacement of a damaged valve) is possible. 2~
Cardiac support by extracorporeal left ventricular bypass was originally described by Dennis, TM with subsequent modifications by Geddes, H3, 263 Zwart,30~ Litwak~94 and others. The Dennis tech- nique would be the ideal approach to left ventricular failure, were it not for vascular access and anticoagulation problems. In the original description, the left atrium was cannulated with a large tube, which was passed through the right internal jugular vein, punctured through the atrial septum and positioned in the left atrium under fluoroscopy. Oxygenated blood from the left atrium was pumped back into a systemic artery, bypassing and resting the left ventricle. Heparinization was required. Several patients in cardiogenic shock were treated by the Dennis technique.
Geddes, 263 Wakabayashi, 28s Zwart 3~ and others have proposed left ventricular bypass with blood takeoff directly from the left atrium or ventricle. These and other methods of left ventricular support are discussed in detail in a recent monograph in this se- ries. 47 Litwak et al2 94 simplified the vascular access problems of left ventricular bypass by attaching flexible conduits to the right superior pulmonary vein and aorta. These channels can be used to cannulate for left ventricular bypass, and plugged with silicone rubber obturators while testing off bypass. This technique has been used in 14 postoperative patients who could not be support- ed with intra-aortic balloon pumping alone. It was successful in 9 patients weaned off bypass support, of whom 6 ultimately sur- vived.
Any type of left ventricular support system will be unsuccessful if pulmonary failure or right ventricular failure occurs. An alter- native approach that unloads both the right and left ventricle has been proposed by Connolly and Wakabayashi. 289 Venoarterial bypass without an oxygenator is established via the femoral ves- sels at low flow (less than 1 L/minute). The legs and pelvic viscera are perfused with venous blood, but this does not cause significant metabolic acidosis. With venous return decreased, adequate sys- temic perfusion to the rest of the body can be maintained by the left ventricle, which has been failing when required to carry the
76

whole load. This approach has the advantages of simple cannula- tion and circuitry. It may be used with coated tubing to avoid sys- temic heparinization. One major disadvantage is lack of ability to proceed to total support if the ventricle fails further, or if pulmo- nary failure supervenes.
PROLONGED VENOARTERIAL BYPASS (ECMO). -This is the ulti- mate in mechanical support systems for the failing heart. It has the advantages of total support capability, biventricular and pulmonary support and easy adaptabili ty to total bypass for car- diac surgery. The indications for this technique in cardiac failure are, therefore, acute reversible r ight or biventricular failure not suitable for (or unresponsive to) counterpulsation or left ventricu- lar bypass. Such conditions exist in acute pulmonary embolism, myocarditis, cardiac contusion, postoperative low cardiac output in children with congenital hear t disease and cardiac disorders and low cardiac output in unstable cyanotic newborn infants.
Techniques for cardiac support with ECMO are basically the same as those described for pulmonary support. Weaning is based on adequacy of systemic perfusion and filling pressure of the criti- cal ventricle as ECMO flow is gradually decreased. If the pat ient has already been on a bubble oxygenator for several hours, severe thrombocytopenia and coagulopathy will exist. Heparin may not be required for the 1st day of cardiac support in such a case.
Results.-Sixty-nine cases of prolonged ECC support for car- diac failure have been reported. These are summarized in Table 4. The most successful application has been in young children, following cardiac operations that leave the right ventricle as the dominant factor controlling cardiac output. 15, 27o Acute massive pulmonary embolism has been successfully treated b y C o o p e r 62 and others. Once cardiopulmonary bypass is established in the
TABLE 4.-ECMO FOR CARDIAC FAILURE, COMBINED CARDIOPULMONARY FAILURE OR
SHOCK-WORLDWIDE EXPERIENCE AS OF JUNE 1977
D I A G N O S I S C A S E S S U R V I V E D
Cardiac failure, shock, myocardial infarction 47 3
Postoperative Adults 9 1" Children 12 3*
Myocarditis 1 1"
Total 69 8 *4 combined cardiopulmonary failure, listed
in Tables 1 and 2.
77

p u l m o n a r y embol i sm pa t ien t , the diagnosis can be prec ise ly de- fined by ang iography in a l e i sure ly fashion. Th o raco to m y wi th r emova l of emboli or wa i t ing for clots to lyse in the hepar in ized ECMO pa t i en t a re bo th sa t i s fac tory a l te rna t ives .
Beaufils and associates ~5 from France reportect the use of ECMO suppor t for 4 days in a young pa t i en t wi th severe viral myocardi t is . Card iac funct ion improved du r ing ECMO support ; the pa t i en t u l t i m a t e l y survived. Th is is the only case r epor t of the use of ECMO in severe myocardi t i s , bu t the resu l t s a re ve ry en- couraging. Final ly , the t echn iques used for ECMO in newborn r e sp i r a to ry fa i lure have been appl ied to p reopera t ive cardiac support , bypass for the opera t ive t echn ique i t se l f and postopera- t ive suppor t in a smal l group of pat ientsY 4 The diagnost ic stfidies and opera t ive procedure can be done wi thou t r i sk or u rgency , and b leeding is m in ima l despi te hepar in iza t ion .
Case examples.-A typical appl ica t ion of ECMO in Cardiac fail- u re is shown in Case 5.
CASE 5.--E. A., a 2-year-old boy, underwent correction of transposition of the great vessels. The operation was complicated by bleeding, and re- operation was necessary. Six hours postoperatively hypotension and oli- guria developed, and he required isoproterenol to maintain a mean ar- terial pressure of 75 mm Hg. Peritoneal dialysis was begun 20 hours af- ter operation. Blood pressure gradually fell despite increasing doses of isoproterenol, digoxin and calcium. Thirty hours postoperatively blood pressure was 35/20 mm Hg on maximal inotropic therapy. Study of the arterial blood showed Po 2 110 mm Hg, pH 7.31 and Pco., 30 mm Hg on mechanical ventilation with an FIo., of 0.3. Because of poor perfusion and metabolic acidosis, ECMO was instituted (Fig 24). The right axillary artery was cannulated with a no. 10 catheter. A no. 16 argyle chest tube was placed down the right internal jugular vein into' the new venous atrium. Flow rates were initially maintained between 500 and 600 ml/min. With these flow rates the systemic artery mean pressure in- creased to 60 mm Hg, and isoproterenol concentration could be reduced to half. Over the next 24 hours the flow rate was gradually decreased as systemic pressure increased. Peritoneal exchanges were continued through the entire period that he was on partial cardiopulmonary sup- port. Thirty-four hours after the start of bypass, systemic blood pressure was 110180 mm Hg. The cannulas were kept in place and the blood was allowed to perfuse through a bridge in the circuit for 2 hours, during which time he maintained good systemic pressure, was alert and tolerat- ed the ventilator well. The arterial cannula was removed and the artery repaired. The internal jugular vein was ligated. Isoproterenol require- ment increased slightly, then gradually diminished over the next 4 days. Ventilator support was continued for 3 weeks because of low tidal vol- ume. Hypoxia was never a problem. During the next 21/2 weeks, renal function improved and peritoneal dialysis was discontinued. He was dis- charged after 6 weeks of hospitalization and is doing well 4 years later, with normal brain, cardiac, pulmonary and renal function.
Case 5 demons t r a t e s the va lue of VA bypass in b iven t r i cu l a r or r i gh t ven t r i cu la r fai lure. I f the myocard ia l d am ag e is t r an s i en t and reversible , ECMO suppor t can be ve ry useful. A combina t ion
78

7.60
7.55
7.50-
pH 7.45- (~ = Priming
Solution 7.40.
7.55-
7.50-
7.25.
t50
125.
I00
ARTERIAL 75 PRESSURE
(mean) 50
25
0
600
5OO
4OO
BYPASS FLOW 300 cc/min
200-
I00-
E.A. VA Bypass Jugular- Axillary
Pte ~' " ~'.""lb" ,~,' ,~ ' ~2' 2'6' 3 ' o ' ~ Hours on Byposs
Fig 2 4 . - C a s e 5, ECMO for cardiogenic shock fol lowing a Mustard procedure. Hypotension, acidosis and renal failure occurred despite maximal inotropic therapy. Perfusion and pressure improved during VA bypass, and ventr icular function recovered, permitt ing weaning from ECMO. Arterial PCO 2 remained between 30 and 35 before and dur ing ECMO. (From Bartlett, R. H., et al.: J. Thorac. Cardiovasc. Surg. 68:918, 1974. Used by permission.)
of counterpulsation and ECMO has been found to be part icularly effective and will probably be used more widely in the future. =~
HEMORRHAGIC SHOCK
Appropriate t reatment of hemorrhagic shock is blood replace- ment by transfusion. However, ECC offers several advantages as adjunctive t reatment for the exsanguinating patient in the oper- ating room. Autotransfusion systems in which shed blood from the operative field is aspirated, anticoagulated, filtered and rein- fused into the patient constitute a mini-extracorporeal circula- tion.Sg, =5o Blood flow in this procedure may be as high as 500 ml/minute, the rate being limited by the size of the intravenous re turn catheter in most situations. The use of a very large venous catheter can turn the autotransfusion system into a type of VV
79

bypass, and permits maintenance of normal blood volume even in massively bleeding patients. If cardiac arrest occurs in the course of hemorrhagic shock, autotransfusion (with v e n o u s return) may be inadequate to return blood fast enough to resuscitate the pa- tient. In addition, if bank blood or large amountso~eroom-temper- ature solutions have been used, the patient's body temperature may be decreased to the point where acidosis and cardiac cooling interfere with resuscitation. In this circumstance, rapidly estab- lished VA bypass with oxygenation and a heat exchanger may provide the required mechanical assistance while the vascular damage is repaired. We have utilized cardiopulmonary bypass several times in trauma patients in this dire position, with~occa- sional success. One patient sustained hypovolemia and sbvere hypothermia (20 C) following an automobile accident in the snow. Blood was warmed and transfused with VA bypass during 2 hours of direct cardiac massage. The heart was eventually resus- citated, and the patient recovered with normal brain function. Pulmonary function is usually normal during hemorrhagic shock, so that arch perfusion is not necessary. Femoral catheters provide the necessary access to institute VA bypass. Investiga- tion of hemorrhagic shock treatment with ECC in the laboratory has been reported by BergentzY ~
SEPTIC SHOCK
The use of ECC in septic shock has been investigated by Lefem- ine et al. is~ Since endotoxemia is characterized by systemic vaso- dilation and abnormally high cardiac output, it is not surprising that VA bypass adds little to this hyperdynamic state. Our clini- cal experience corroborates these findings. We have used ECMO for pulmonary failure in 3 patients who were also in endotoxic shock. ~3 Although excellent extracorporeal flow could be achieved, systemic perfusion, blood pressure and oxygen delivery never improved sufficiently to clear metabolic acidosis and reverse the moribund condition.
CAPILLARY LEAK SYNDROMES
Shock that accompanies diffuse systemic capillary leakage will probably not be effectively treated with artificial organs, with the possible exception of hemodialysis or filtration to remove mi- croemboli and vasoactive polypeptides. Cardiac output in acute pancreatitis, massive burns and hepatorenal syndrome is already high, and oxygenation is generally adequate. The problem lies at the capillary level, and mechanically pumping the blood around will probably not further alter the course of events. Our clinical experience with ECMO support in one patient with hepatorenal syndrome and pulmonary failure resulted in pulmonary and renal improvement but ultimate death from liver failure.
80

SUMMARY
1. Left ventricular assistance is best provided by counterpulsa- tion. Ifcounterpulsation is inadequate, VA bypass may be consid- ered.
2. Full VA bypass (ECMO) is indicated for isolated rigbt, ven- tricular or biventricular failure, or cardiac failure associated with severe pulmonary failure. In that setting, ECMO has been used infrequently but has been successful in selected cases.
3. Extracorporeal circulation is helpful as an adjunct to cardiac resuscitation, particularly in trauma patients in the operating room. Except for this unusual circumstance, ECMO has not been beneficial in management of shock.
OTHER APPLICATIONS OF ECMO
Extracorporeal circulation has been applied to several other clinical problems that are outside the scope of this monograph, but should be mentioned. Total body washout, an extreme of ex- change transfusion, has been used to remove toxins, particularly in liver failure, with some success. 1, 57 This technique is facilitat- ed by ECC, which sustains perfusion and permits controlled cool- ing. 25s Limb and organ perfiLsion with oxygenated blood has been used in isolated cancer chemotherapy for many years. 199 Similar apparatus has been used to perfuse amputated limbs prior to reimplantation, and to perfuse isolated organs for physiologic study ~36 or transplantation. 2s2 Cadaver perfusion (after brain death and cardiac arrest) has been investigated as a method to preserve several organs for subsequent transplantation, allowing time for tissue typing. 2s
Multiple organ failure, including heart, lung and kidney, may be treated with extracorporeal support before failure of any one organ system becomes predominant. The mortality in multiple organ failure is very high, and such a radical step may prove to be the safest course. The possibility of inducing bleeding complica- tions makes such an approach impractical at present, but if non- coagulable circuits become available, early use of ECMO in mul- tiple organ failure could be evaluated. Finally, ECC has been reported in the successful treatment ofpriapism, 84 a rare but dev- astating disorder.
EXTRACORPOREAL SUPPORT: ARTIFICIAL ORGANS AND REAL PROBLEMS
In the last decade ECMO has progressed from a laboratory cu- riosity to a well-defined clinical entity. Through improvements in artificial organ design, understanding of pathophysiology, control of anticoagulation and simplification of the procedure, ECMO can support life in severe cardiac and pulmonary failure for weeks at
81

a time. Complications and deleterious effects are significant and primarily related to bleeding and blood-surface interface prob- lems. However, these effects are detectable, controllable and ac- ceptable when compared to the mortality risk of the primary dis- ease.
For cardiac failure, ECMO has found its greatest application in postoperative low cardiac output syndrome in children, where a few hours or days of perfusion allow ventricular function to im- prove.
In pulmonary failure, the limiting factor has been irreversibili- ty of end-stage acute lung disease. The technique has been most successful when applied early, where something can be actively done to treat (or avoid mistreating) the lung. For these redsons, the most successful applications have been in acute pulmonary capillary leak syndromes and newborn respiratory failure.
The successful application of ECMO (or any life-support tech- nique) inevitably leads to profound clinical and moral dilemmas. The alert patient with no functional lung who is totally depen- dent on ECMO poses unique problems in med'ical care. In the future lung transplantation or implantable prostheses may be possible in this situation. At present the physician and his team must decide when the fine line between therapy and palliation is crossed. The exciting advances in technology that salvage lives from "diseases desperate grown" also raise the spectre of sus- taining existence by impersonal machines. Compassionate care of a terminal patient is the responsibility of the physician (not the courts), whether the patient suffers from cancer, brain dam- age or acute respiratory failure.
Prolonged ECMO is at a stage of development comparable to that of the artificial kidney in 1955. '09 At that tinie hemodialysis was being applied only in acute renal failure, and then only in end-stage disease. Mortality for dialyzed patient's was approxi- mately 90%. The technique was being studied in only a few spe- cialized centers, and its future was uncertain. A majsr advance in simplification was required to make the technique generally useful. For hemodialysis this breakthrough was chronic vascu- lar access. If such an advance is forthcoming in ECMO research, it will probably be in eliminating bleeding complications.
The next decade will bring a "third generation" of vastly im- proved artificial lungs, general application of thromboresistant surfaces and improved methods of measuring acute cardiac and pulmonary failure. These advances will make it feasible to eval- uate: very early application in acute pulmonary failure, chronic vascular access, ECMO as an adjunct to lung transplantation or lung prosthesis and combination of ECMO with other left ven- tricular support measures as an adjunct to heart transplantation or prosthesis.
82

ACKNOWLEDGMENTS
The research on which this monograph is based was supported by the National Institutes of Health (Lung Division of the Na- tional Heart, Lung, and Blood Institute), the Orange County Heart Association, the California Lung Association and th~Don- ald E. Baxter Foundation. The UCI-ECMO team included over 60 individuals, organized around the nucleus of Nick Haiduc, C.C.P., Nancy Wetmore, R.N., H. Vernon Roohk, Ph.D., Paul Mullin, B.A. and Eleanor Hung, B.A. We wish to thank our col- leagues for contributing data and comments, and the physicians and nurses of University of California at Irvine Medical Center and other hospitals for their support and excellent patient care. Our special thanks to Nancy Hoffman, who nursed this manu- script through many revisions into its final form.
REFERENCES
1. Agostini, J., Ramirez, R., Albert, S., et al.: Successful reversal of lethal car- bon monoxide intoxication by total body asanguineous hypothermic perfu- sion, Surgery 75:213, 1973.
2. Allen, J. G. (ed.): Extracorporeal Circulation {Springfield, Ill.: Charles C Thomas, Publisher, 1958).
3. Altose, M. D., Hicks, R. E., and Edwards, M. W.: Extracorporeal membrane oxygenation during bronchopulmonary lavage, Arch. Surg. 111:1148, 1976.
4. Anderson, R. M., O'Hare, J. E., and Fritz, J. M: Automatic-demand pump for cardiopulmonary bypass, Ann. Thorac. Surg. 10:424, 1970.
5. Ashbaugh, D. G., and Petty, T. L.: Sepsis complicating the acute respiratory distress syndrome, Surg. Gynecol. Obstet. 135:865, 1972.
6. Awad, J. A., Matte, J., and Brassard, A.: Prolonged extracorporeal respira- tion with a membrane gas exchanger, J. Thorac. Cardiovasc. Surg. 66(1):40, 1973.
7. Baler, R. E.: Organization of blood components near interfaces, Ann. NY Acad. Sci. 283:17, 1977.
8. Bartlett, R. H., Kittredge, D., Noyes, B. S., Jr., et al.: Development of a membrane oxygenator: Overcoming blood diffusion limitation, J. Thorac. Cardiovasc. Surg. 58:795, 1969.
9. Bartlett, R. H., Isherwood, J., Moss, R. A., et al.: A toroidal flow membrane oxygenator: Four day partial bypass in dogs, Surg. Forum 20:152, 1969.
10. Bartlett, R. H., Drinker, P. A., and Galletti, P. M. (eds3: Mechanical Devices for Cardiopulmonary Assistance, in Advances in Cardiology, Vol. 6 {Basel: S. Karger AG, 1971).
11. Bartlett, R. H.: Post-traumatic Pulmonary Insufficiency, in Cooper and Nyhus (eds.): Surgery Annual, 1971 (New York: Appleton-Century Crofts, Inc., 1971).
12. Bartlett, R. H., Drinker, P. A., Burns, N. E., et al.: The toroidal membrane oxygenator: Design, performance and bypass testing of a clinical model, Trans. Am. Soc. Artif. Intern. Organs 18:369, 1972.
13. Bartlett, R. H., Gazzaniga, A. B., Brennan, M., et al.: Studies in pathogenesis and prevention of postoperative pulmonary complications, Surg. Gynecol. Obstet. 137:925, 1973.
14. Bartlett, R. H., Fong, S. W., and Burns, N. E.: Prolonged partial venoarterial bypass: Physiologic, biochemical, and hematologic responses, Ann. Surg. 180:850, 1974.
15. Bartlett, R. H., Gazzaniga, A. B., Fong, S. W., et al.: Prolonged extracorpo- real cardiopulmonary support in man, J. Thorac. Cardiovasc. Surg. 68:918, 1974.
83

16. Bartlett, R. H. (chairman): Hematological Analysis of Extra-corporeal Mem- brane Oxygenation. Report of NHLI Workshop, Sept. 1974. DHEW Publica- tion no. 75-865 (NIH) (Washington, D.C.: Department of Health, Education, and Welfare, 1974).
17. Bartlett, R. H., Fong, S. W., Woldanski, C., et al.: Hematologic responses to prolonged extracorporeal circulation (ECC) with microporous membrane devices, Trans. Am. Soc. Artif. Intern. Organs 21:250, 197~ z.
18. Bartlett, R. H., Gazzaniga, A. B., Wilson, A. F., et al.: Mortality prediction in adult respiratory insufficiency, Chest 67:680, 1975.
19. Bartlett, R. H., Gazzaniga, A. B., Jefferies, R., et al.: Extracorporeal mem- brane oxygenation (ECMO) cardiopulmonary support in infancy, Trans. Am. Soc. Artif. Intern. Organs 22:80, 1976.
20. Bartlett, R. H., and Rucker, R.: Pneumonitis and foreign body aspiration treated with ECMO, personal communication, 1976.
21. Bartlett, R. H., Drinker, P. A., Hill, J. D., et al.: Indications for ECMO~ Sup- port: Quantitating Pulmonary Insufficiency, in Zapol, W. M., and Qvist, J. (eds.): Artificial Lungs for Acute Respiratory Failure (New York: Academic Press, Inc., 1976).
22. Bartlett, R. H., and Gazzaniga, A. B.: The Physiology and Pathophysiology of Extracorporeal Circulation, in Ionescu, M., and Wooler, C. (Eds.): Current Techniques in Extracorporeal Circulation (London: Butterworth & Co., Ltd., 1976).
23. Bartlett, R. H., Gazzaniga, A. B., Fong, S. W., et al.: Extracorporeal mem- brane oxygenator (ECMO) support for cardiopulmonary failure: Experience in twenty-eight cases, J. Thorac. Cardiovasc. Surg. 73(3):375, 1977.
24. Bartlett, R. H., Gazzaniga, A. B., Ituxtable, R. F., et al.: Extracorporeal cir- culation (ECMO) in neonatal respiratory failure, J. Thorac. Cardiovasc. Surg., 1977. (In press.)
25. Beaufils, P., Piwnica, A., Eisemann, B., et al.: Insuffisance cardiaque subai- gu5 chez un sujet jeune et assistance cardiocirculatoire m~canique tempo- raire, Nouv. Presse Med. 3:2108, 1974.
26. Begent, N. A., and Bonn, G. V. R.: Growth rate in vivo ofplatelet thrombi produced by iontophoresis of ADP, as a function of mean blood flow velocity, Nature 227:926, 1970.
27. Bellhouse, B. J., Bellhouse, F. H., Curl, C. M., et al.: A high efficiency mem- brane oxygenator and pulsatile pumping system, and its application to ani- mal trials, Trans. Am. Soc. Artif. Intern. Organs 19:72, 1973.
28. Belzer, F. O., and Kountz, S. L.: Preservation and transplantation of human cadaver kidneys: A two-year experience, Ann. Surg. 172:394, 1970.
29. Benedict, J. S.: Personal communication, 1977. 30. Benn, J. A., Drinker, P. A., Mikic, B., et al.: Predictive correlation of oxygen
and carbon dioxide transfer in a blood oxygenator with induced secondary flows, Trans. Am. Soc. Artif. Intern. Organs 17:317, 1971.
31. Bergentz, S. E., and Brief, D. F.: Assisted circulation in hemorrhagic shock: Effects ofpulsatile partial venoarterial bypass with an oxygenator, J. Surg. Res. 4:322, 1964.
32. Berger, R. L.: Pulmonary embolectomy with pre-operative circulatory sup- port, Ann. Thorac. Surg. 16:217, 1973.
33. Bernhard, W. F., Husain, M., Robinson, T., et al.: An appraisal of blood trau- ma and the blood-material interface following prolonged assisted circula- tion, J. Thorac. Cardiovasc. Surg. 58:801, 1969.
34. Bernstein, E. F., Blackshear, P. L., Jr., and Keller, K. H.: Factors influencing erythrocyte destruction in artificial organs, Am. J. Surg. 114:126, 1967.
35. Bernstein, E. F., and Gleason, L. R.: Factors influencing hemolysis with roll- er pumps, Surgery 61:432, 1967.
36. Bernstein, E. F., Cosentino, L. C., Reich, S., et al.: A compact low hemolysis non-thrombogenic system for nonthoracotomy prolonged left ventricular bypass, Trans. Am. Soc. Artif. Intern. Organs 20:643, 1974.
37. Birek, A., Duffin, J., Glynn, M. F. X., et al.: The effect of sulfinpyrazone On
84

platelet and pulmonary responses to onset of membrane oxygenator perfu- sion, Trans. Am. Soc. Artif. Intern. Organs 22:94, 1976.
38. Birabaum, D., and Eiseman, B.: Laboratory evaluation of a new silicone membrane oxygenator, J. Thorac. Cardiovasc. Surg. 64:441, 1972.
39. Birtwell, W. C., Giron, F., Ruiz, V., et al.: The regional hemodynamic re- sponse to synchronous external pressure assist, Trans. Am. Soc. Artif. Intern. Organs 16:462, 1970.
40. Blackshear, P. L., Jr." Summation: Flow-related surface phenomena, Fed. Proc. 30:1709, 1971.
41. Bloom, S., Zapol, W., Wonders, T., et al.: Platelet destruction during 24-hour membrane lung perfusion, Trans. Am. Soc. Artif. Intern. Organs 20:299, 1974.
42. Bloom, S. R., Snider, M. T., Peterson, R., et al.: Platelet life-span and gas exchange during perfusion with spiral coil membrane lungs coated with ethylcellulose perfluorobutyrate, Trans. Am. Soc. Artif. Intern. Organs 22: 119, 1976.
43. Boucher, J. K., Rudy, L. W., and Edmunds, L. H.: Organ blood flow during pulsatile cardiopulmonary bypass, J. Appl. Physiol. 36:86, 1974.
44. Bramson, M. L., Osborn, J. J., Main, F. B., et al.: A new disposable mem- brane oxygenator with integral heat exchanger, J. Thorac. Cardiovasc. Surg. 50:391, 1965.
45. Brandt, B., Doyle, B., Weintraub, H., et al.: Pulmonary artery pressure and lung water during extracorporeal circulation in experimental pulmonary insufficiency, Ann. Thorac. Surg. 20(3):308, 1975.
46. Bregman, D.: Assessment of intra-aortic balloon counterpulsation in cardi- ogenic shock, Crit. Care Med. 3:90, 1975. "
47. Bregman, D.: Mechanical Support of the Failing heart, Current Problems in Surgery (Chicago: Year Book Medical Publishers, Inc., Dec. 1976).
48. Brinsfield, D. E., Hopf, M. A., Geering, R. B., et al.: Hematological changes in long-term perfusion, J. Appl. Physiol. 17:531, 1962.
49. Bruner, J. D., Schuhmann, R. E., Geddes, L. A., et al.: Des!gn and perfor- mance of a vacuum reservoir blood pump, J. Assoc. Advancement Med. In- strum. 4:182, 1970.
50. Buckles, R. G., Merrill, E. W., and Gilliland, E. R.: An analysis of oxygen absorption in a tubular membrane oxygenator, Am. Inst. Chem. Eng. J. 14: 703, 1968.
51. Btiky, B., Bell, W., Matthews, P., et al.: Arvin anticoagulation for prolonged extracorporeal membrane oxygenation, Trans. Am. Soc. Artif. Intern. Or- gans 19:56, 1973.
52. Butruille, Y., Chevallet, J., Granger, A., et al.: Rhone-Poulenc Oxygenator and Associated Pumping System, in Zapol, W. M., and Qvist, J. (eds.): Artifi- cial Lungs for Acute Respiratory Failure (New York: Academic Press, Inc., 1976}, p. 223.
53. Carlson, R. G., Land~, A. J., Landis, B., et al.: The Land6-Edwards mem- brane oxygenator during heart surgery, J. Thorac. Cardiovasc. Surg. 66:894, 1973.
54. Chadd, M. A., Elwood, D. C., Gray, O. P., et al.: Coagulation defects in hypox- ic full-term newborn infants, Br. Med. J. 4:516, 1971.
55. Claff, C. L., Crescenzi, A. A., and Ippolito, P. F.: Pulsatile Membrane Oxygen- atorApparatus. United States Letters Patent no. 3,332,746, July 25, 1967.
56. Clark, L. C.: Monitor and control of blood and tissue oxygen tensions, Trans. Am. Soc. Artif. Intern. Organs 2:41, 1956.
57. Cline, R. E., Klebanoff, G., Armstrong, R. G., et al.: Extracorporeal circula- tion in hypothermia as used for total body wash-out in stage 4 hepatic coma, Ann. Thorac. Surg. 16:44, 1973.
58. Clowes, G. H. A., Jr., Hopkins, A. L., and Neville, W. E.: An artificial lung dependent upon diffusion of oxygen and carbon dioxide through plastic membranes, J. Thorac. Surg. 32:630, 1956.
59. Colton, C. K.: Fundamentals of Gas Transport in Blood, in Zapol, W. M., and
85

Qvist, J. (eds.): Artificial Lungs for Acute Respiratory Failure (New York: Academic Press, Inc., 1976), p. 1.
60. Cooper, J. D., Duffin, J., and Zapol, W. M.: Cannulation of ascending aorta for long-term membrane oxygenator support, J. Thorac. Cardiovasc. Surg. 69:905, 1975.
61. Cooper, J. D., Duffin, J., Glynn, hi. F. X., et al.: Combination of membrane oxygenator support and pulmonary lavage for acute r2~iratory failure, J. Thorac. Cardiovasc. Surg. 71:304, 1976.
62. Cooper, J. D., Teasdale, S., Nelems, J. M., et al.: Cardiorespiratory failure secondary to peripheral pulmonary emboli." Survival following a combina- tion of prolonged extracorporeal membrane oxygenator support and pulmo- nary embolectomy, J. Thorac. Cardiovasc. Surg. 71(6):872, 1976.
63. Crafoord, C., Norberg, B., and Senning, A.: Clinical studies in extracorporeal circulation with a heart-lung machine, Acta Chir. Seand. 112:220, 1957.
64. Crescenzi, A. A., Hofstra, P. C., Szek, C., et al.: Development ofa si~aplified disposable membrane oxygenator, Surg. Forum 10:610, 1959.
65. Dawids, S. G., and Engell, H. C. (eds.): Physiological and Clinical Aspects of Oxygenator Design, Proceedings of the Seminar on Advances in Oxygenator Design, Copenhagen, 1975 (New York: Elsevier Scientific Publishing Com- pany, 1976).
66. Day, S. W., Crystal, D. K., Wagner, C. L., et al.: Properties of synthetic membranes in extracorporeal circuits, Am. J. Surg. 114:214, 1967.
67. de Filippi, R. P., Tompkins, F. C., Jr., Porter, J. H., et al.: The capillary membrane blood oxygenator: In vitro and in vivo gas exchange measure- ments, Trans. Am. Soc. Artif. Intern. Organs 14:236, 1968.
68. deJong, J. C. F., Smit Sibinga, CTh., and Wildeveur, Ch. R. H.: Thrombocy- topenia in extracorporeal circulation (ECC} II: Bubble oxygenator versus artificial kidney, Trans. Am. Soc. Artif. Intern. Organs 21:40, 1975.
69. deLeval, M., Hill, J. D., Mielke, H., et al.: Platelet kinetics during extracor- poreal circulation, Trans. Am. Soc. Artif. Int. Organs 28:355, 1972.
70. deLeval, M. R., Hill, J. D., Mielke, C. H., et al.: Blood platelets and extra'cor- poreal circulation, J. Thorac. Cardiovasc. Surg. 69:144, 1975.
71. Demling, R. H., Hicks, R. E., and Edmunds, L. H.: Changes in extravascular lung water during veno-venous perfusion, J. Thorac. Cardiovasc. Surg. 71" 291, 1976.
72. Dennis, C.: Certain methods for artificial support of the circulation during intracardiac surgery, Surg. Clin. North Am. 36:423, 1956.
73. Depp, D. A., and Hughes, R. K.: Veno-venous perfusion with a membrane oxygenator, J. Thorac. Cardievasc. Surg. 62:658,1971.
74. DeWall, R., Bentley, D. J., Hirose, M., et al.: A temperature controlling (omnithermic) disposable bubble oxygenator for total body perfusion, Dis. Chest 49:207, 1966.
75. Dexter, L., Haynes, F. W., Burwell, C. S., et al.: Studies of congenital heart disease. I. Technique ofvenous catheterization as a diagnostic procedure, J. Clin. Invest. 26:547, 1947.
76. Dietzman, R. H., Bloch, J. H., Lyons, G. W., et al.: Prevention of lethal cardi- ogenic shock in epinephrine-tolerant dogs, Surgery 65:623, 1969.
77. Dobell, A. R. C., Mitri, M., Galva, R., et al.: Biologic evaluation of blood after prolonged recirculation through film and membrane oxygenators, Ann. Surg. 161:617, 1965.
78. Dedrill, F. D., Hill, E., Gerisd, R. A., et al.: Pulmonary valvuloplasty under direct vision using a mechanical heart for complete bypass of the right heart in a patient with congenital pulmonary stenosis, J. Thorac. Surg. 26:584, 1953.
79. Dorson, W. J., Baker, E., Hull, H., et al.: A long-term partial bypass oxygen- ation system, Ann. Thorae. Surg. 8(4):297, 1969.
80. Dorson, W. J., Baker, E., Cohen, M. L., et al.: A perfusion system for infants, Tr. Amer. Soc. Artif. Intern. Organs 15:155, 1969.
81. Dorson, W. J., Jr., Meyer, B., Baker, E., et al.: Response ofdistressed infants
86

to partial bypass lung assist, Trans. Am. Soc. Artif. Intern. Organs 16:345, 1970.
82. Dorson, W. J., and Larsen, K. G.: Secondary flows in membrane oxygenators, Adv. Cardioh 6:17, 1971.
83. Dorson, W. J., and Voorhees, M. E.: Analysis of Oxygen and Carbon Dioxide Transfer in Membrane Lungs, in Zapol, W. hi., and Qvist, J. (eds.): Artificial Lungs for Acute Respiratory Failure (New York: Academic Pre~s, Inc., 1976), p. 43.
84. Douglas, L. L.: Extracorporeal circulatory management ofpriapism, Urolo- gy 7:198, 1976.
85. Douglas, hi. E., and Downs, J. B.: Pulmonary function following severe acute respiratory failure and high levels of positive end expiratory pressure, Chest 71(1):18, 1977.
86. Drinker, P. A., Bartlett, R. H., Bialer, R., et al.: Augmentation of membrane gas transfer by oscillation of a coiled tube, Surgery 66:775, 1969.
87. Drinker, P. A.: Progress in membrane oxygenator design, Anesthesiology 37: 242, 1972.
88. Drinker, P., and McKahn, C.: The use of a new apparatus for the prolonged administration of artificial respiration. I: A fatal case of poliomyelitis, J.A.M.A. 92:1658, 1929.
89. Duncan, S. E., Klebanoff, G., and Rogers, W.: A clinical experience with intra-operative autotransfusion, Ann. Surg. 180:296, 1974.
90. Dunn, J., Kirsch, hi., Harness, J., et al.: Hemodynamic, metabolic and hema- tologic effects of pulsatile cardiopulmonary bypass, J. Thorac. Cardiovasc. Surg. 68:138, 1974.
91. Dutton, R. C., and Edmunds, L. H., Jr.: Measurement of emboli in extracor- poreal perfusion systems, J. Thorac. Cardiovasc. Surg. 65:523, 1973.
92. Dutton, R. C., Edmunds, L. H., Jr., Hutchinson, J. C., et al.: Platelet aggre- gate emboli in patients during cardiopulmonary bypass with membrane and bubble oxygenators and blood filters, J. Thorac. Cardiovasc. Surg. 67:258, 1973.
93. Eberhart, R. C., Lamy, hi., Dietrich, H. P., et al.: Hemodynamic aspects of prolonged extracorporeal oxygenation, Trans. Am. Soc. Artif. Intern. Organs 21:491, 1975.
94. Esato, K., Richards, R., and Eiseman, B.: Distribution of oxygenated blood in experimental perfusion via the femoral and carotid arteries, J. Thorac. Car- diovasc. Surg. 69:467, 1975.
95. Falb, R. D., Leiniger, R. I., and Crowley, J. P.: Materials with chemically ac- tive substituants, Ann. NY Acad. Sci. 283:396, 1977.
96. Falke, K. J., Herzer, A., Krian, A., et al.: Extrac0rporeal Membrane Oxygen- ation in Experimental Pulmonary Insufficiency: Effect of Perfusion Route on Regional Blood Gas Tension and Oxygen Delivery, in Zapol, W. hi., and Qvist, J. (eds.): Artificial Lungs for Acute Respiratory Failure (New York: Academic Press, Inc., 1976).
97. Fallat, R. J., Tucker, H. J., and Sigcova, L." Lung function in long-term sur- vivors from severe respiratory distress syndrome (RDS). Presented at Amer- ican Thoracic Society, 1977. Submitted to Am. Rev. Respir. Dis.
98. Fletcher, J. R., McKee, A. E., Mills, hi., et al.: 24 hour membrane oxygena- tion in dogs without anticoagulants, Surgery 80:214, 1976.
99. Fletcher, J. R., McKee, A. E., and Herman, C. M.: Membrane oxygenation in baboons without anticoagulants, J. Surg. Res. 22:273, 1977.
100. Fong, S. W., Burns, N. E., Williams, G., et al.: Changes in coagulation and platelet function during prolonged extracorporeal circulation (ECC) in sheep and man, Trans. Am. Soc. Artif. Intern. Organs 20:239, 1974.
101. Fong, S. W., Woldanski, C., Hung, E., et al.: Coagulation and platelet values in normal and heparinized sheep. (In preparation.)
102. Forrester,J. S., Ganz, W., Diamond, G., et al.: Thermodilution cardiac out- put determination with a single fiow-directed catheter, Am. Heart J. 83:306, 1972.
87

103. Frantz, S. L., Chopra, P., Goldenberg, A. L., et al.: A membrane combined oxygenator and pump-principles, Trans. Am. Soc. Artif. Intern. Organs 14: 233, 1968.
104. Freund, U., Carlson, R. W., Schaffer, R. C., et al.: Oxygen transport during extracorporeal oxygenation for the treatment of adult respiratory distress syndrome, Surg. Gynecol. Obstet. 143:709, 1976.
105. Friedman, L. I., and Leonard, E. F.: Platelet adhesion t~'~rtificial surfaces: Consequences of flow, exposure time, blood condition, and surface nature, Fed. Proc. 30:1641, 1971.
106. Galletti, P. M., Hopf, M. A., and Brecher, G. A.: Problems associated with long-lasting heart-lung bypass, Trans. Am. Soc. Artif. Intern. Organs 6:180, 1960.
107. Galletti, P. M., and Brecher, G. A.: Heart-LungBypass {New York: Grune & Stratton, Inc., 1962).
108. Galletti, P. M., Richardson, P. D., and Snider, M. T.: A standardized method for defining the overall gas transfer performance of artificial lungs, Trans. Am. Soc. Artif. Intern. Organs 18:359, 1972.
109. Galletti, P. M.: Lessons from the Past and Projections for the Future, in Zapol, W. M., and Qvist, J. (eds.): Artificial Lungs for Acute Respiratory Failure (New York: Academic Press, Inc., 1976).
110. Gannon, P. G.: Viral pneumonia with anoxic convulsions and treatment with membrane oxygenator, Mt. Sinai J. Meal. 40:244, 1973.
111. Ganz, H., Subramanian, V. A., Lillehi, C. W., et al.: Problems in hemostasis during open heart surgery. VIII. On the in vivo turnover rate ofplasminogen activator after cardiopulmonary bypass, Surgery 62:292, 1967.
112. Ganz, H., Castaneda, A. R., Subramanian, V. A., et al.: Problems in hemosta- sis daring open heart surgery. IX. Changes observed in the plasminogen- plasma system and their significance for therapy, Ann. Surg. 166:980, 1967.
113. Geddes, L. A., Schuhmann, R. E., Hoff, H. E., et al.: Total maintenance ofcir- culation in the closed-chest animal with ventricular fibrillation, Cardiovasc. Res. Cent. Bull. 6:33, 1967.
114. Geelhoed, G. W., Corso, P., and Joseph, W. L.: The role of membrane lung support in transient acute respiratory insufficiency of Pneumocystis carinii pneumonia, J. Thorac. Cardiovasc. Surg. 68:802, 1974.
115. Geelhoed, G. W., Adkins, P. C., Corso, P. J., and Joseph, W. L.: Clinical ef- fects of membrane lung support for acute respiratory failure. Ann. Thorac. Surg. 20(2):177, 1975.
116. Gerbode, F., Osborn, J. J., and Bramson, M. L.: Experiences in the develop- ment of a membrane heart-lung machine, Am. J. Surg. 114:16, 1967.
117. Gervin, A. S., McNear, J. F., Wolfe, W. G., et al.: Ultrapore hemofiltration during extracorporeal circulation, J. Thorac. Cardiovasc. Surg. 67:237, 1974.
118. Giannelli, S., Ayres, S. M., Fleming, P., et al.: Peripheral vascular volumes and whole body hematocrit during human heart lung bypass, Circulation 41: 629, 1970.
119. Gibbon, J. H., Jr.: Artificial maintenance ofcirculation during experimental occlusion of pulmonary artery, Arch. Surg. 34:1105, 1937.
120. Gibbon, J. H., Jr.: Application of a mechanical heart and lung apparatus to cardiac surgery, Minn. Med. 37:171, 1954.
121. Gille, J. P., Trudell, L., Snider, M. T., et al.: Capability of the microporous, membrane-lined, capillary oxygenator in hypercapnic dogs, Trans. Am. Soc. Artif. Intern. Organs 16:365, 1970.
122. Gille, J. P.: L'assistance respiratoire par circulation extracorporeal avec poumon artificiel h membrane, Bull. Physiopath. Respir. 10:373, 1974.
123. Gille, J. P.: World Census of Long Term Perfusions for Respiratory Support, in Zapol, W. M., and Qvist, J. (eds.): Artificial Lungs for Acute Respiratory Failure (New York: Academic Press, Inc., 1976).
124. Gille, J. P., and Bagniewski, A. M.: Ten years of use of extracorporeal mem- brane oxygenation (ECMO) in the treatment of acute respiratory insufficien- cy (ARI), Trans. Amer. Soc. Artif. Intern. Organs 22:102, 1976.
88

125. Gille, J. P.: Personal communication, 1976. 126. Gilman, S.: Cerebral disorders after open-heart operations, N. Engl. J. Med.
272:489, 1965. 127. Gross, K.: Therapeutic influencing of the connective tissue proliferation in
lung fibrosis using D-penicillamine, MOd. Klin. 67:1034, 1972. 128. Hagler, H. K., Powell, W. M., Eberle, J. W., et al.: Five-day partial bypass
using a membrane oxygenator without systemic heparinization, Trar/'s. Am. Soc. Artif. Intern. Organs 21:178, 1975.
129. Hamilton, W. F., Riley, R. L., Attyah, A. M., et al.: Comparison of the Fick and Dye injection methods of measuring the cardiac output in man, Am. J. Physiol. 153:309, 1948.
130. Hammond, G. L., and Poulain, H.: Pulmonary support using venovenous bypass and a biological oxygenator, Thorax 29:121, 1974.
131. Hanson, E. L., Bartlett, R. H., Burns, N. E., et al.: The use of a membrane oxygenator in air breathing and hypoxic lambs: Veno-venous bypass, Sur- gery 73:284, 1973.
132. Hanson, E. L., Drinker, P. A., Don, H. F., et al.: Venoarterial bypass with a membrane oxygenator: Successful respiratory support in a woman following pulmonary hemorrhage secondary to renal failure, Surgery 75:557, 1974.
133. Harken, A. H.: The influence of pulsatile perfusion on oxygen uptake by the isolated canine hind limb, J. Thorac. Cardiovaso. Surg. 70:237, 1975.
134. Harken, D. E.: Presentation at the International College of Cardiology Meet- ing, Brussels, Belgium, 1958.
135. Harrison, T. S., Chawla, R. C., Seton, J. F., et al.: Carotid sinus origin of ad- renergic response comprising the effectiveness of artificial circulatory sup- port, Surgery 68:20, 1970.
136. Harrison, T. S., and Seton, J. F.: An analysis of pulse frequency as an adren- ergic excitant in pulsative circulatory support, Surgery 73:868, 1973.
137. Harrison, V. C., deVHesse, H., and Klein, M.: Intracranial hemorrhage asso- ciated with hyaline membrane disease, Arch. Dis. Child. 43:116, 1968.
138. Hedley-Whyte, J., Burgess, G. E., Feeley, T. W., et al.: Applied Physiology of Respiratory Care (New York: Little, Brown & Company, 1976).
139. Heiden, D., Mielke, C. H., Rodvien, R., et al.: Platelets, hemostasis, and thromboembolism during treatment of acute respiratory insufficiency with extracorporeal membrane oxygenation, J. Thorac. Cardiovasc. Surg. 70:644, 1975.
140. Hicks, R. E., Dutton, R. C., Ries, C. A., et al.: Production and fate ofplatelet aggregate emboli during venovenous perfusion, Surg. Forum 24:250, 1973.
141. Hicks, R. E., Kinney, T. R., Raphaely, R. C., et al.: Successful treatment of varicella pneumonia in a leukemic child with prolonged extracorporeal membrane oxygenation, J. Thorac. Cardiovasc. Surg. 73:297, 1977.
142. Hill, J. D., Bramson, M. L., Rapaport, E., et al.: Experimental and clinical experiences with prolonged oxygenation and assisted circulation, Ann. Surg. 170:448, 1969.
143. Hill, J. D., Bramson, M. L., Osborn, J. J., et al.: Observations and manage- ment during clinical veno-venous bypass for respiratory insufficiency, Adv. Cardiol. 6:133, 1971.
144. Hill, J. D., de Leval, M. R., Fallat, R. J., et al.: Acute respiratory insufficien- cy: Treatment with prolonged extracorporeal oxygenation, J. Thorac. Car- diovasc. Surg. 64:551, 1972.
145. Hill, J. D., de Leval, M. R., Mielke, C. H., et al.: Clinical prolonged extracor- poreal circulation for respiratory insufficiency: Hematological effects, Trans. Am. Soc. Artif. Intern. Organs 18:546, 1972.
146. Hill, J. D., O'Brien, T. G., Murray, J. J., et al.: Prolonged extracorporeal oxy- genation for acute post-traumatic respiratory failure (shock lung syndrome), N. Engl. J. Med. 286:139, 1972.
147. Hill, J. D., Dontigny, L., de Leval, M., and Mielke, C. H.: A simple method of heparin management during prolonged extracorporeal circulation, Ann. Thorac. Surg. 17:129, 1974.
89

148. Hill; J. D., Ratliff, J. L., Fallat, R. J., et al.: Prognostic factors in the treat- ment of acute respiratory insufficiency with long-term extracorporeal oxy- genation, J. Thorac. Cardiovasc. Surg. 68:905, 1974.
149. Hill, J. D., Iatridis, A., O'Keefe,:R., et al.: Technique for achieving high gas exchange rates in membrane oxygenation, Trans. Am. Soc. Artif. Intern. Organs 20:249, 1974.
150. Hill, J. D., Ratliff, J. L., Parrott, J. C., et al.: Pulmonary.pdthology in acute respiratory insufficiency: Lung biopsy as a diagnostic tool, J. Thorac. Car- diovasc. Surg. 71(1):64, 1976.
151. Hill, R. N., Shibel, E. M., Spragg, R. G., et al.: Adult respiratory distress syndrome: Early predictors of mortality, Trans. Am. Soc. Artif. Intern. Or- gans 21:199, 1975.
152. Hoffman, A. S., Horbett, T. A., and Ratner, B. D.: Interactions of blood and blood components at hydrogel interfaces, Ann. NY Acad. Sci. 283:372, 197"h
153. Holdefer, W. F., Dowling, E. A., and Kirklin, J. W.: Hemodynamic, metabol- ic, and organ function studies in animals subjected to prolonged .veno- arterial bypass with the Bramson membrane lung, J. Thorac. Cardiovasc. Surg. 61:217, 1971.
154. Illickal, M. hi., Brown, G. E., Van de Water, J. hi., et al.: Boundary layer phenomena in membrane oxygenators, Surg. Forum 18:134, 1967.
155. Ionescu, hi. I., and Wooler, G. H. (eds.): Current Techniques in Extracorpo- real Circulation (London: Butterworth & Co., Ltd., 1976).
156. Jacobs, L. A., Klopp, E. H., Seamone, W., et al.: Improved organ function during cardiac bypass with a roller pump modified to deliver pulsatile flow, J. Thorac. Cardiovasc. Surg. 58:703, 1969.
157. Johnson, S. L.: The History of Cardiac Surgery 1896-1958 (Baltimore: Johns Hopkins Press, 1970).
158. Joseph, W. J., Giordano, J. hl., and Goelhoed, G. W.: Clinical use of the membrane oxygenator for acute respiratory insufficiency, Mt. Sinai J. Med. 40:1973.
159. Kahn, D.: Personal communication, 1977. 160. Kammermeyer, K.: Silicone rubber as a selective barrier, Ind. Eng. Chem.
49:1685, 1957. 161. Kantrowitz, A., Tj0nneland, S., Freed, P: S., et al.: Initial clinical experience
with intra-aortic balloon pumping in eardiogenic shock, J.A.M.A. 203:135, 1968.
162. Katsuharff, K., Yokosuka, T., and Sakakibara, S.: The swing-type mem- brane oxygenator: Gas exchange performance of the Swing motion system, J. Surg. Res. 8:245, 1968.
163. Kay, E. B., and Cross, F. S.: Direct vision and repair of intracardiac defects utilizing a rotating disc reservoir oxygenator, Surg. Gynecol. Obstet. 104: 701, 1957.
164. Kaye, M. P., Pace, J. B., Blatt, S. J., et al.: Use of a capillary membrane oxy- genator for total cardiopulmonary bypass in calves, J. Surg. Res. 14:58, 1973.
165. Kennedy, J. H., Bailas, N., Barnard, P. M., et al.: Use of a pump oxygenator in clinical cardiac failure, J.A.M.A. 195(2):105, 1966.
166. Kennedy, J. H.: Assisted circulation: An extended concept of cardiopulmo- nary resuscitation in man, J. Assoc. Advancement Med. Instrum. 4(6):237, 1970.
167. Ketteringham, J., Zapol, W., Birkett, J., et al.: A high permeability, nonpo- rous, blood compatible membrane for membrane lungs: In vivo and in vitro performance, Trans. Am. Soc. Artif. Intern. Organs 21:224, 1975.
168. Kirklin, J. W., and Rastelli, G. C.: Low cardiac output after open-heart intra- cardiac operations, Prog. Cardiovasc. Dis. 10:117, 1967.
169. Kohlstaedt, K. G., and Page, I. H.: The liberation of renin by perfusion of kidneys following reduction of pulse pressure, J. Exp. Med. 72:201, 1940.
170. Kolff, W. J., and Berk, H. T., Jr.: Artificial kidney: A dialyser with a great area, Acta Meal. Scand. 117:121, 1944.
9O

171. Kolff, W. J., and Balzer, R. R.: Artificial coil lung, Trans. Am. Soc. Artif. In- tern. Organs 1:39, 1955.
172. Kolobow, T., and Bowman, R. L.: Construction and evaluation of an alveolar membrane artificial heart lung, Trans. Am. Soc. Artif. Intern. Organs 9:238, 1963.
173. Kolobow, T., Zapol, W., Pierce, J. E., et al.: Partial extracorporeal.~gas ex- change in alert newborn lambs with a membrane artificial lung pert'used via an A-V shunt for periods up to 96 hours, Trans. Am. Soc. Artif. Intern. Or- gans 14:328, 1968.
174. Kolobow, T., Zapol, W., and Pierce, J.: High survival and minimal blood damage in lambs exposed to long term (1 week) veno-venous pumping with a polyurethane chamber roller pump with and without a membrane blood oxygenator, Trans. Am. Soc. Artif. Intern. Organs 15:172, 1969.
175. Kolobow, T., Spragg, R. G., Pierce, J. E., et al.: Extended term (to 16 days) partial extracorporeal blood gas exchange with the spiral membrane lung in unanesthetized lambs, Trans. Am. Soc. Artif. Intern. Organs 17:350, 1971.
176. Kolobow, T., Stool, E. W., Weathersby, P. K., et al.: Superior blood compati- bility of silicone rubber free of silica fller in the membrane lung, Trans. Am. Soc. Artif. Int. Organs 20:269, 1974.
177. Kolobow, T., Stool, E., Sacks, K., et al.: Acute respiratory failure: Survival following ten days support with membrane lung, J. Thorac. Cardiovasc. Surg. 69(6):947, 1975.
178. Kolobow, T., Stool, E. W., and Pierce, J.: Long Term Perfusion with the Membrane Lung in Lambs, in Zapol, W. M., and Qvist, J. (eds.): Artifi- cial Lungs for Acute Respiratory Failure (New York: Academic Press, Inc., 1976), p. 234.
179. Kumar, A., Falke, K. J., and Geffin, B.: Continuous positive pressure venti- lation in acute respiratory failure, N. Engl. J. Med. 283:1430, 1970.
180. Kusserow, B. K., Larrow, R., and Nichols, J.: The urokinase-heparin bonded synthetic surface, Trans. Am. Soc. Artif. Intern. Organs 17:1, 1971.
181. Lamy, M., Eberhart, R. C., Fallat, R. J., et al.: Effects of extracorporeal membrane oxygenation (ECMO) on pulmonary hemodynamics, gas ex- change, and prognosis, Trans. Am. Soc. Artif. Intern. Organs 21:188, 1975.
182. Lamy, M. R., Fallat, R. J., Coeniger, E., et al.: Pathologic features and mech- anisms of hypoxemia in adult respiratory distress syndrome, Am. Rev. Res- pir. Dis. 114:267, 1976.
183. Land~, A. J., Dos, S. J., Carlson, R. G., et al.: A new membrane oxygenator- dialyzer, Surg. Clin. North Am. 47:1461, 1967.
184. Land~, A. J., Fillmore, S. J., Subramanian, V., et al.: 24 hour veno-arterial perfusions of awake dogs with a simple membrane oxygenator, Trans. Am. Soc. Artif. Intern. Organs 15:181, 1969.
185. Land~, A. J., Edwards, L., Bloch, J. H., et al.: Clinical experience with emer- gency use of prolonged cardiopulmonary bypass with a membrane pump- oxygenator, Ann. Thorac. Surg. 10:409, 1970.
186. Land~, A. J.: Treatment of massive pulmonary embolism with ECMO. Pre- sented at International Conference on Artificial Lungs for Acute Respiratory Failure, Copenhagen, 1975.
187. Lautier, A., Bonnet, A., Volter, F., et al.: Studies on oxygenator membrane surface in long term extracorporeal assistance, Trans. Am. Soc. Artif. Intern. Organs 20:307, 1974.
188. Lee, W. H., Jr., Krumhaar, D., Fonkalsrud, E. W., et al.: Denaturation of plasma proteins as a cause of morbidity and death after intracardiac opera- tions, Surgery 50:29, 1961.
189. Lee, W. H., Jr., Brady, M. P., Rowe, J. M., et al.: Effects ofextracorporeal cir- culation upon behavior, personality, and brain function. Part II. Hemody- namic, metabolic, and psychometric correlations, Ann. Surg. 173:1013, 1970.
190. Lefemine, A. A., and Harken, D. E.: Extracorporeal support of the circula- tion by means of venoarterial bypass with an oxygenator, J. Thorac. Car- diovasc. Surg. 62:769, 1971.
91

191. Lefrak, E. A., Stevens, P. M., Noon, G. P., et al.: Current status of prolonged extracorporeal membrane oxygenation for acute respiratory failure, Chest 63(5), 1973.
192. Lewis, F. R., Tylke, J. A., and Winchell, H. S.: A combined membrane pump~ oxygenater: Design and testing, Trans. Am. Soc. Artif. Intern. Organs 20: 253, 1974.
193. Lillehi, C. W., Cohen, M., Warden, H. C., et al.: The re,u-It of direct vision closure of ventricular septal defects in 8 patients by means of controlled cross circulation, Surg. Gynecol. Obstet. 101:447, 1955.
194. Litwak, R. S., Koffsky, R. M., Lukban, S. B., et al.: Implanted heart assist device after intracardiac surgery, N. Engl. J. Med. 291:1341, 1975.
195. Madras, P. N., Morton, W. A., and Petschek, H. E.: Dynamics of thrombus formation, Fed. Proc. 30:1665, 1971.
196. Many, hl., Giron, F., Birtwell, W. C., et al.: Effects of depulsation of renal blood flow upon renal function and renin secretion, Surgery 66:242, 1960.
197. Marx, G. H.: A capillary membrane-oxygenator utilizing gas dispersed ~n oil, Trans. Am. Soc. Artif. Intern. Organs 16:381, 1970.
198. Marx, T. I., Snyder, W. E., St. John, A. D., et al.: Diffusion of oxygen into a film of whole blood, J. Appl. Physiol. 15:1123, 1960.
199. McBride, C. M., Sugarbaker, E. V., and Hicky, R. C.: Prophylactic isolation- perfusion as the primary therapy for invasive malignant melanoma of the limbs, Ann. Surg. 182:316, 1975.
200. McEnany, M. T., Zapol, W. M., Seebacher, J., et al.: Cannulation of the proxi- mal aorta during long-term membrane lung perfusion, J. Thorac. Cardio- vasc. Surg. 70:631, 1975.
201. McLean, J.:Thediscoveryofheparin, Circulation 19:75, 1959. 202. McNamara, J.: Personal communication, 1977. 203. Melrose, D. G., and Singh, M. P.: Prolonged circulatory assistance in awake
neonatal lambs, J. Thorac. Cardiovasc. Surg. 67:584, 1974. 204. Mielke, C. H., Jr., de Leval, M., Hill, J. D., et al.: Drug influence on platelet
loss during extracorporeal circulation, J. Thorac. Cardiovasc. Surg. 290:144, 1973.
205. Moore, F. D., Lyons, J. H., Jr., Peirce, E. C., et al.'Post-traumatic Pulmonary Insufficiency (Philadelphia: W. B. Saunders Co., 1969).
206. Morrissey, V. W.: The adsorbtion and conformation of plasma proteins: A physical approach, Ann. NY Acad. Sci. 283:50, 1977.
207. Mukherjee, N. D., Berran, A. V., Hirai, J., et al.: In vivo determination of renal tissue oxygenation during pulsatile and nonpulsatile left heart bypass, Ann. Thorac. Surg. 15:345, 1973.
208. Mullin, P., Lee, S., Burd, S., et al.: A new device for the rapid automated de- termination of the activated clotting time of whole blood, Amsect Proceed- ings, 1976.
209. Mundth, E. D., Yurchak, P. M., Buckley, M. J., et al.: Circulatory assistance and emergency direct coronary-artery surgery for shock complicating acute myocardial infarction, N. Engl. J. Med. 283:1382, 1970.
210. Murphy, D. A., Norris, K., and Martin, M.: The in vivo characteristics of a toroidal flow membrane oxygenator, Trans. Am. Soc. Artif. Intern. Organs 17:337, 1971.
211. Murphy, W., Trudell, L. A., Freidman, L. I., et al.: Laboratory and clinical experience with a microporous membrane oxygenator, Trans. Am. Soc. Artif. Intern. Organs 20:278, 1974.
212. Murray, G.: Surgery in the Making (London; Johnson Publishers, Ltd., 1964). 213. Mustard, W. T.: Clinical and experimental experience with hemalogous and
heterologous lung perfusion, Trans. Am. Soc. Artif. Intern. Organs 1:94, 1955.
214. NHLI Respiratory Diseases Task Force Report on Problems, Research, Ap- proaches and Needs: Lung Program of National Heart and Lung Institute, DHEW Publication no. NIH73-432 (Washington, D.C.: Department of Health, Education, and Welfare, 1972).
215. NHLI Extracorporeal Support for Respiratory Insufficiency-Collaborative 92

Program. Division of Lung Diseases, National Heart and Lung Institute, 1974.
216. NHLI Respiratory Diseases: Task Force Report on Prevention, Control, Edu- cation, DHEW Publication no. NIH771248 (Washington, D.C., Department of Health, Education, and Welfare, 1977).
217. NHLI.ECMO Study: Extracorporeal Support for Respiratory Insufficiency; DHEW Publication. (In preparation.)
218. NHLI-ECMO Study: Extracorporeal support for respiratory insufficiency: Final Report, DHEW Publication. (In preparation.)
219. Nelems, J. M., Bellhouse, B. J., Curl, C. M., et al.: Prolonged pulmonary sup- port of newborn lambs with the Oxford membrane oxygenator, Trans. Am. Soc. Artif. Intern. Organs 20:293, 1974.
220. Neville, W. C.: Extracorporeal Circulation, Current Problems in Surgery (Chicago: Year Book Medical Publishers, Inc., July 1967).
221. Northway, W. H., Rosan, R. C., and Porter, D. Y.: Pulmonary disease follow- ing respiratory therapy of hyaline-membrane disease: Bronchopulmonary dysplasia, N. Engl. J. Med. 7:355, 1967.
222. O'Connor, M. J., Huxtable, R. F., Bartlett, R. H., et al.: Neonatal pulmonary insufficiency index: A method of newborn mortality prediction. {Submitted for publication.)
223. Orell, S. R.: Lung pathology in respiratory disease following shock in the adult, Acta Pathol. Microbiol. Scan& 79A:65, 1971.
224. Pacifieo, A. D., Digerness, S., and Kirklin, J. W.: Acute alterations of body composition after open intracardiac operations, Circulation 41:331, 1970.
225. Pappas, G., Winter, S., Kopriva, C. J., et al.: Improvement of myocardial and other vital organ functions and metabolism with a simple method of pulsa- tile flow (IABP) during clinical cardiopulmonary bypass, Surgery 77:34, 1975.
226. Patterson, R. H., Kessler, J., and Burglund, R. M.: A filter to prevent cere- bral damage during experimental eardiopulmonary bypass, Surg. Gynecol. Obstet. 132:71, 1971.
227. Peacock, E. E., and VanWinkle, W.: Surgery and Biology of Wound Repair (Philadelphia: W. B. Saunders Company, 1970).
228. Peirce, E. C., II: Modification of the Clowes membrane lung, J. Thorae. Car- diovasc. Surg. 39:438, 1960.
229. Peirce, E. C.: The membrane lung: Its excuse, present status, and promise, J. hit. Sinai Hosp. 34:437, 1967.
230. Peirce, E. C., Corrigan, J. J., Kent, B. B., et al.: Comparative trauma to blood in the disc oxygenator and membrane lung, Trans. Am. Soc. Artif. Intern. Organs, 15:33, 1969.
231. Peirce, E. C.: Extracorporeal Circulation for Open.heart Surgery (Springfield, Ill.: Charles C Thomas, Publisher, 1969).
232. Peirce, E. C., II, Thebaut, A. L., Kent, B. B., et al.: Techniques of extended perfusion using a membrane lung, Ann. Thorac. Surg. 12:451, 1971.
233. Peirce, E. C., Tamari, Y., and Geron, F.: Auxiliary Lung: State of the Art, in Rapaport and Merrill (eds.): Artificial Organs and Cardiopulmonary Support Systems (New York: Grune & Stratton, Inc., 1971), p. 29.
234. Peirce, E. C. (ed.): Clinical use of membrane lungs, hit. Sinai J. Med. 40 (No. 2): 1973.
235. Peirce, E. C.: The theory and function of the membrane lung, hit. Sinai J. Med. 40:119, 1973.
236. Perma, H. S., Caldini, P., Masai, A., et al.: Recruitment vs. Distensibility in the Pulmonary Vascular Bed, in Fishman, A. P., and Hedt, H. T. (eds.): Pul- monary Circulation and Interstitial Space (Chicago: University of Chicago Press, 1969).
237. Petschek, H. E., Adamis, D., and Kantrowitz, A. R.: Stagnation flow throm- bus formation, Trans. Am. Soc. Artif. Intern. Organs 14:256, 1968.
238. Pitzele, S., Sze, S., Hagemann, A., et al.: A liquid-liquid oxygenator utilizing oxygen-saturated inert fluorocarbon for organ perfusion-preservation, Sur- gery 68:1079, 1970.
93

239. Pois, A. J., Katzman, L., Weston, C. B., et al.: Longterm support with a membrane lung, Chest 62(6):690, 1972.
240. Pontoppidan, H., Geffen, B., and Lowenstein, E.: Acute respiratory failure in the adult, N. Engl. J. Med. 287:690- 98,743 -52,799-806, 1972.
241. Pratt, P.: Report of the Pathology Center. NHLI-ECMO Study, 2d Annual Report, 1976.
242. Pyle, R. B., Helten, W. C., Johnson, F. W., et al.: Clinical use of the mem- brane oxygenator, Ann. Surg. 110:966, 1975.
243. Rafferty, E. H., Kletschka, H. D., and Olsen, D. A.: A nonpulsatile artificial heart, J. Extracorporeal Tech. 5:30, 1973.
244. Rashkind, W. J., Freeman, A., Klein, D., et al.: Evaluation of a disposable plastic low volume, pumpless oxygenator as a lung substitute, J. Pediatr. 66: 94, 1965.
245. Ratliff, J. L., Hill, J. D., Fallat, R. J., et al.: Complications associated with membrane lung support by venoarterial perfusion, Ann. Thorac. Surg. t9(5): 537, 1975.
246. Ratliff, J. L., Hill, J. D., Tucker, H, et al.: Endobronchial control of broncho- pleural fistulae, Chest 71:98, 1977.
247. Ratliff, N. B., Young, W. G., Hackel, D.B., et al.: Pulmonary injury second- ary to extracorporeal circulation, J. Thorac. Cardiovasc. Surg. 65:425, 1973.
248. Rea, W. J., Whitley, D., and Eberle, J. W.: Long-term membrane oxygena- tion without systemic heparinization, Trans. Am. Soc. Artif. Intern. Organs 28:316, 1972.
249. Replogle, R., Levy, M., DeWall, R. A., et al.: Catecholamine and serotonin response to cardiopulmonary bypass, J. Thorac. Cardiovasc. Surg. 44:638, 1962.
250. Reul, G. J., Jr., Solis, R. T., Greeuberg, S. D., et al.: Experience with auto- transfusion in the surgical management of trauma, Surgery 76:546, 1974.
251. Richardson, P. D., Snider, hi. T., and Galletti, P. M.: Oxygen transfer to blood in membrane lungs: Correlation with and prediction from in vivo mea- surements, Trans. Am. Soe. Artif. Intern. Organs 17:323, 1971.
252. Richardson, P. D.: Design Factors Affecting Thrombus duringExtracorporeal Membrane Oxygenation, in Zapol, W. M., and Qvist, J. (eds.): Artificial Lungs for Acute Respiratory Failure (New York: Academic Press, Inc., 1976), p. 141.
253. Robertson, M., and Stacey, R. B.: Prolonged extracorporeal circulation for respiratory support, J. Extracorporeal Technol. Fall 1973, p. 34.
254. Roohk, H. V., Pick, J., Hill, R., et al.: Kinetics offibrinogen and platelet ad- herence to biomaterials, Trans. Am. Soc. Artif. Intern. Organs 22:1, 1976.
255. Roohk, H. V., Nakamura, M., Hill, R. L., et al.: A thrombogenic index for blood contact materials, Trans. Am. Soc. Artif. Intern. Organs 23:152, 1977.
256. Ross, J. N., Brown, C. H., Harness, M. K., et al.: Role ofplatelet aggregation in prolonged extraeorporeal respiratory support, Circulation 49 and 50:219, (supp. 11), 1974.
257. Rudy, L. W., Heyman, M. A., and Edmunds, L. H.: Distribution of systemic blood flow during cardiopulmonary bypass, J. Appl. Physiol. 34:194, 1973.
258. Ryan, J. F., Donlon, J. V., Molt, R. A., et al.: Cardiopulmonary bypass in the treatment of malignant hyperthermia, N. Engl. J. Med. 290:1121, 1974.
259. Salsbury, P. F., Morgenstein, L., Hyman, M. M., et al.: Physiologic factors in the use of the pump oxygenator, Trans. Am. Soe. Artif. Intern. Organs 1:68, 1955.
260. Salzman, E. W.: Blood Platelets: Their Behavior with Respect to Extracorpo- real Membrane Oxygenation, in Zapol, W. M., and Qvist, J. (eds.): Artificial Lungs for Acute Respiratory Failure (New York: Academic Press, Inc., 1976), p. 105.
261. Salzman, E. W., Lindon, J., Brier, D., et al.: Surface induced platelet adhe- sion aggregation and release, Ann. NY Acad. Sci. 283:114, 1977.
262. Sanderson, J. M., Wright, G., and Simms, F. W.: Brain damage in dogs im- mediately following pulsatile and nonpulsatile blood flows in extracorporeal circulation, Thorax 27:275, 1972.
94

263. Schuhmann, R. E., Geddes, L. A., and Hoff, H. E.: Prolonged left ventricular bypass by transvalvular aortic catheterization, Surgery 67:957, 1970.
264. Schulte, H. D., Bircks, W., and Dudziak, R.: Erste Erfahrungen mit der Bramson-Membran-Lunge, Thoraxchirurgie 20:54, 1972.
265. Schulte, H. D.: Membrane oxygenators in prolonged assisted extracorporeal circulation, Dtsch. Med. Wochenschr. 98:508, 1973.
266. Severinghaus, J. W., and Bradley, A. F.: Electrodes for blood pO 2 and pCO 2 determination, J. Appl. Physiol. 13:515, 1958.
267. Shepard, R. B., and Kirklin, J. W.: Relation ofpulsatile flow to oxygen con- sumption and other variables during cardiopulmonary bypass, J. Thorac. Cardiovasc. Surg. 58:694, 1969.
268. Silva, J., Hoeksema, H., and Fekety, F. R.: Transient defects in phagocytic functions during cardiopulmonary bypass, J. Thorac. Cardiovasc. Surg. 67: 175, 1974.
269. Silverman, W. A., and Anderson, D. A.: A controlled clinical trial of effects of water mist on obstructive respiratory signs, death rate, and necropsy find- ings among premature infants, Pediatrics 17(1):1, 1956.
270. Soeter, J. R., Mamiya, R. T., Spragne, A. Y., et al.: Prolonged extracorporeal oxygenation for cardiorespiratory failure after tetralogy correction, J. Tho- rac. Cardiovasc. Surg. 66:214, 1973.
271. Soeter, J. R., Smith, G. T., Anema, R. J., et al.: Distribution of oxygenated blood in femoral and brachial artery perfusion during venoarterial bypass in primates, J. Thorac. Cardiovasc. Surg. 65:825, 1973.
272. Spaan, J. A. E., Oomens, J., and Garred, L. J.: A high shear stress annular membrane oxygenator with tangential flow. (Tenth International Confer-
. ence on Medical and Biological Engineering, Dresden, 1973.) 273. Spaeth, E. E., and Friedlander, S. K.: The diffusion of oxygen, carbon diox-
ide, and inert gas in flowing blood, Biophys. J. 7:827, 1967. 274. Spaeth, E. E.: "The Oxygenation of Blood in Artificial Membrane Devices,"
in D. Hershey (ed.): Blood Oxygenation (New York: Plenum Press, 1970), p. 276.
275. Spragg, R. G., Hill, R. N., Wedel, M. K., et al.: Platelet kinetics in veno- venous membrane oxygenation, Trans. Am. Soc. Artif. Intern. Organs 21" 171, 1975.
276. Stahlman, M. T., Battersby, E. J., Shepard, F. M., et al.: Prognosis in hyaline membrane disease-use of a linear discriminant, N. Engl. J. Med. 276(6): 303, 1967.
277. Starling, E. H.: The Law of the Heart, Linnacke Lecture(1918). Cited in Evans, C. L.: Starling's Human Physiology (Philadelphia: Lea & Febiger, 1956).
278. Tamari, Y., Aledort, L., Puszkin, E., et al.: Functional changes in platelets during extracorporeal circulation, Ann. Thorac. Surg. 19(6):639, 1975.
279. Tessler, I., Li, W., Siassi, B., et al.: Prolonged use of membrane oxygenator to treat pulmonary insufficiency, Am. Surg. 38(6):299, 1972.
280. Thomas, J. A.: Coeur-poumon h membrane pulmonaire artificielle, C. R. Acad. Sci. [D] (Paris) 246:1084, 1958.
281. Tilney, N. L., and Hester, W. J.: Physiologic and histologic changes in the lungs of patients dying after prolonged cardiopulmonary bypass, Ann. Surg. 166:759, 1967.
282. Toledo-Pereyra, L. H., Simmons, R. L., and Najeren, J. S.: Two to three day intestinal preservation utilizing hypothermic pulsatile perfusion, Ann. Surg. 179:454, 1974.
283. Trinkle, J. K., Helton, N. E., Wood, R. E., et al.: Metabolic comparison of a new pulsatile pump and a roller pump for cardiopulmonry bypass, J. Thorac. Cardiovasc. Surg. 58:562, 1969.
284. Trinkle, J. K., Helton, N. E., Bryant, L. R., et al.: Pulsatile cardiopulmonary bypass: Clinical evaluation, Surgery 68:1074, 1970.
285. Turina, M., Litchford, B., Babotai, I., et al.: Servo-controlled extended car- diopulmonary bypass, Trans. Am. Soc. Artif. Intern. Organs 19:504, 1973.
286. Van Slyke, D. D., and Neill, J. A.: The determination of gas in blood and 95

other solutions by vacuum extraction and manometric measurements, J. Biol. Chem. 61:523, 1924.
287. Varco, R. L. (conference chairman): Conference on mechanical surface and gas layer effects on moving blood (San Diego, California, Jan. 1971), Fed. Proc. 30:1485, 1971.
288. Wakabayashi, A., Dietrick, W., and Connolly, J. E.: Closed chest left heart bypass without anticoagulation, J. Thorac. Cardiovasc. Su-~. 58:811, 1969.
289. Wakabayashi, A., Connolly, J. E., Stemmer, E. A., et al.: Clinical experience with heparinless venoarterial bypass without oxygenation for the treatment of acute cardiogenic shock, J. Thorac. Cardiovasc. Surg. 68:687, 1974.
290. Ward, B. D., and Hood, A. G.: Comparative performance of clinical mem- brane lungs, J. Thorac. Cardiovasc. Surg. 68:830, 1974.
291. Ward, B. D., Hood, A. G., and Hershgold, E. J.: Pathophysiology and me- chanics of membrane lung performance deterioration, Trans. Am. Soc. A~r - tif. Intern. Organs 21:206, 1975.
292. Ward, C. A., Ruegsegger, B., Stanga, D., et al.: Reduction in platelet adhe- sion to biomaterials by removal of gas nuclei, Trans. Am. Soc. Artif. Intern. Organs 20:77, 1974.
293. Weiss, H. J., Rogers, J., and Brand, H.: Properties of the platelet retention (yon Willebrand) factor and its similarity to the antihemophilic factor (AHF) Blood 41:809, 1973.
294. Weissman, M. H., and Mockros, L. F.: Oxygen transfer to blood flowing in round tubes, J. Eng. Mech. Div. ASCE 93: No. EM6, Proc. paper 5696, Dec. 1967, pp 225- 244.
295. Wesoloski, S. A., Sauvage, L. R., and Pinc, R. D.: Extracorporeal circulation: The role of the pulse in maintenance of the systemic circulation during heart-lung bypass, Surgery 37:663, 1954.
296. White, J. J., Leenders, E., Andrews, H. G., et al.: Studies of a membrane oxy- genator for prolonged respiratory support, J. Pediatr. Surg. 5:610, 1970.
297. White, J. J., Andrews, H. G., Risemberg, H., et al.: Prolonged respiratory support in newborn infants with a membrane oxygenator, Surgery 70(2): 288, 1971.
298. Zapol, W., Pontoppidan, H., McCullough, N., et al.: Clinical membrane lung support for acute respiratory insufficiency, Trans. Am. Soc..Artif. Intern. Organs 18:553, 1972.
299. Zapol, W, M., Qvist, J., Pontoppidan, H., et al.: Extracorporeal perfusion for acute respiratory failure, J. Thorac. Cardiovasc. Surg. 69:439, 1975.
300. Zapol, W. M., Bloom, S., Carvalho, A., et al.: Improved platelet economy us- ing filler-free silicone rubber in long-term membrane lung perfusion, Trans. Am. Soc. Artif. Intern. Organs 21:587, 1975.
301. Zapol, W. M., and Qvist, J.: Artificial Lungs for Acute Respiratory Failure (New York: Academic Press, Inc., 1976).
302. Zapol, W. M.: Post-traumatic pulmonary failure: Case records of the Massa- chusetts General Hospital, N. Engl. J. MOd. 296:1279, 1977.
303. Zapol, W. M., and Snider, M. T.: Pulmonary hypertension in severe acute respiratory failure, N. Engl. J. Med. 296:476, 1977.
304. Zingg, W.: Membrane oxygenator for infants, Trans. Am. Soc. Artif. Intern. Organs 13:334, 1967.
305. Zotti, E. F., Ikeda, S., Lesage, A. M., et al.: Prolonged venovenous perfusion with a membrane oxygenator for respiratory failure, J. Thorac. Cardiovasc. Surg. 51(3):383, 1966.
306. Zwart, H. H. J., Kralios, A. C., Kwan-Gett, C. S., et al.: Transarterial closed chest left ventricular bypass for desperate heart failure, J. Assoc. Advance- ment Med. Instrum. 5:44, 1971.
96