Embed Size (px)
Citation preview
Extracorporeal gas exchange for ARDS patients
Prof. Alain Combes Service de Réanimation iCAN, Institute of Cardiometabolism and Nutrition Hôpital Pitié-Salpêtrière, AP-HP, Paris Université Pierre et Marie Curie, Paris 6 www.reamedpitie.com [email protected]
Conflict of interest
¢ Principal Investigator: HEROICS trial l HVHF after complicated heart surgery l NCT01077349 l Sponsored by GAMBRO
¢ Principal Investigator: EOLIA trial l VV ECMO in ARDS l NCT01470703 l Sponsored by MAQUET, Getinge Group
¢ Received honoraria from MAQUET, Getinge Group, ALung
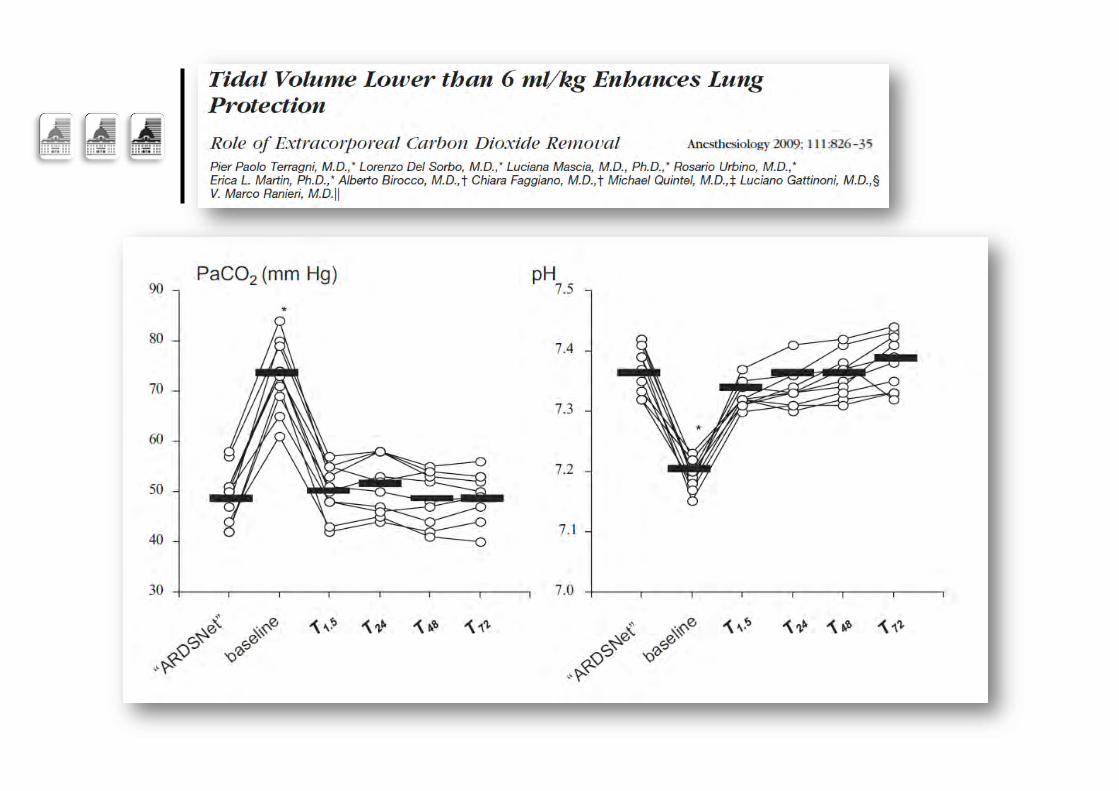
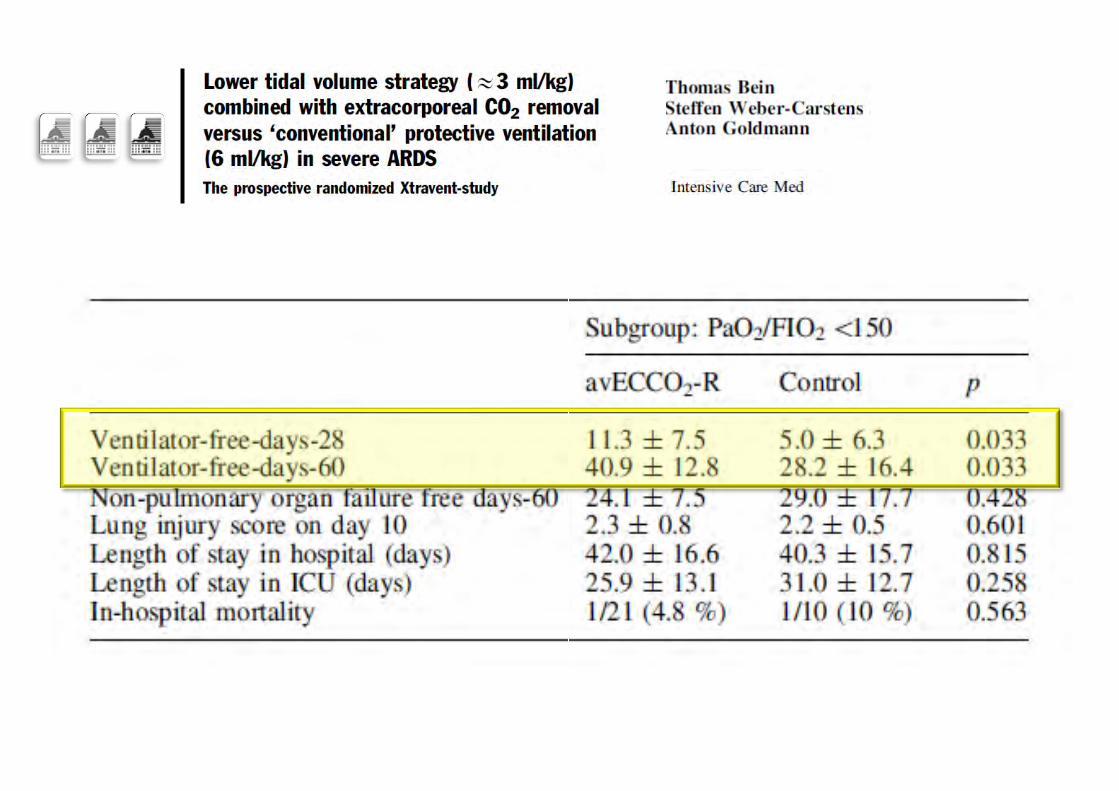
Lower Vt/Pplat + ECCO2R
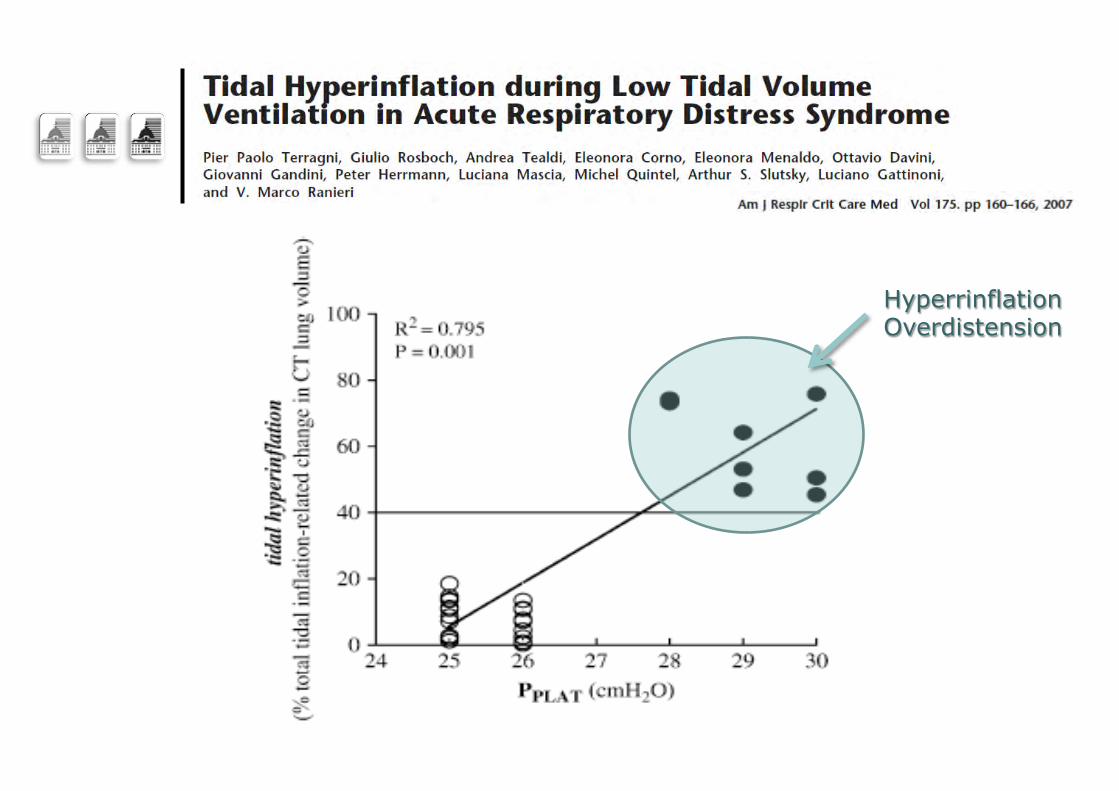
Hyperrinflation Overdistension
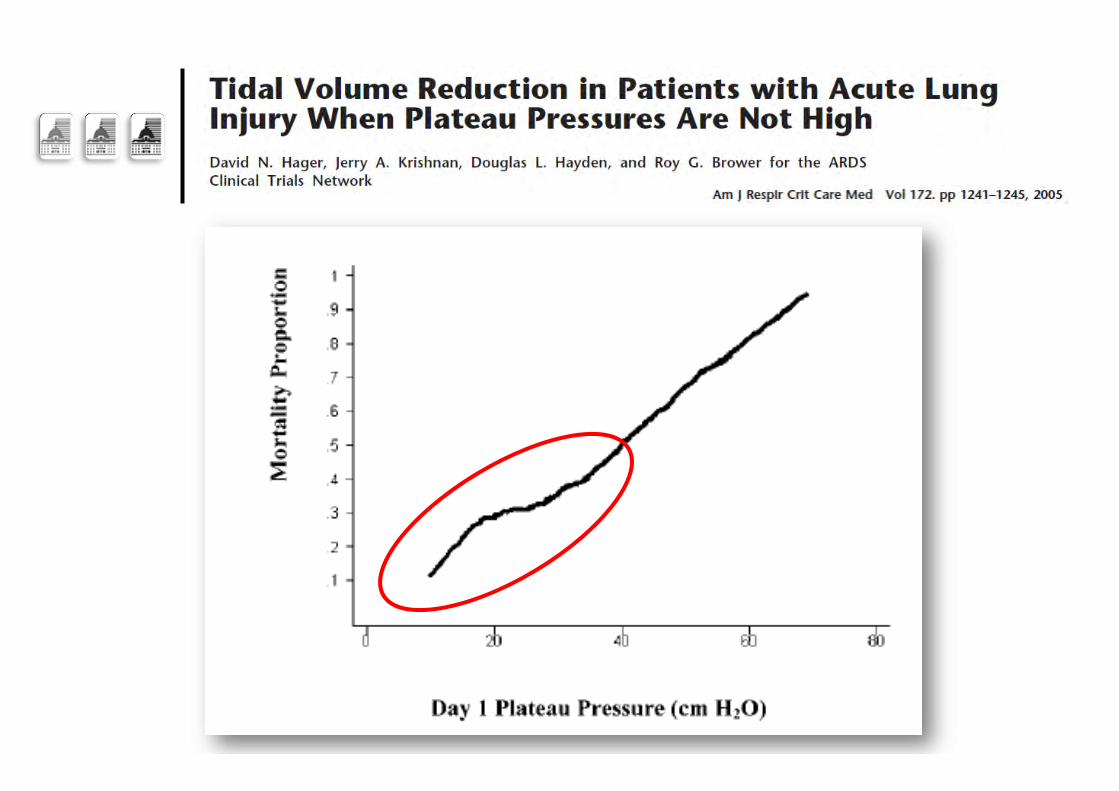
Hager AJRCCM 2005
The evolving paradigm…
¢ ARDSnet strategy might not protect against tidal hyperinflation when Pplat remains >28-30 cm H2O
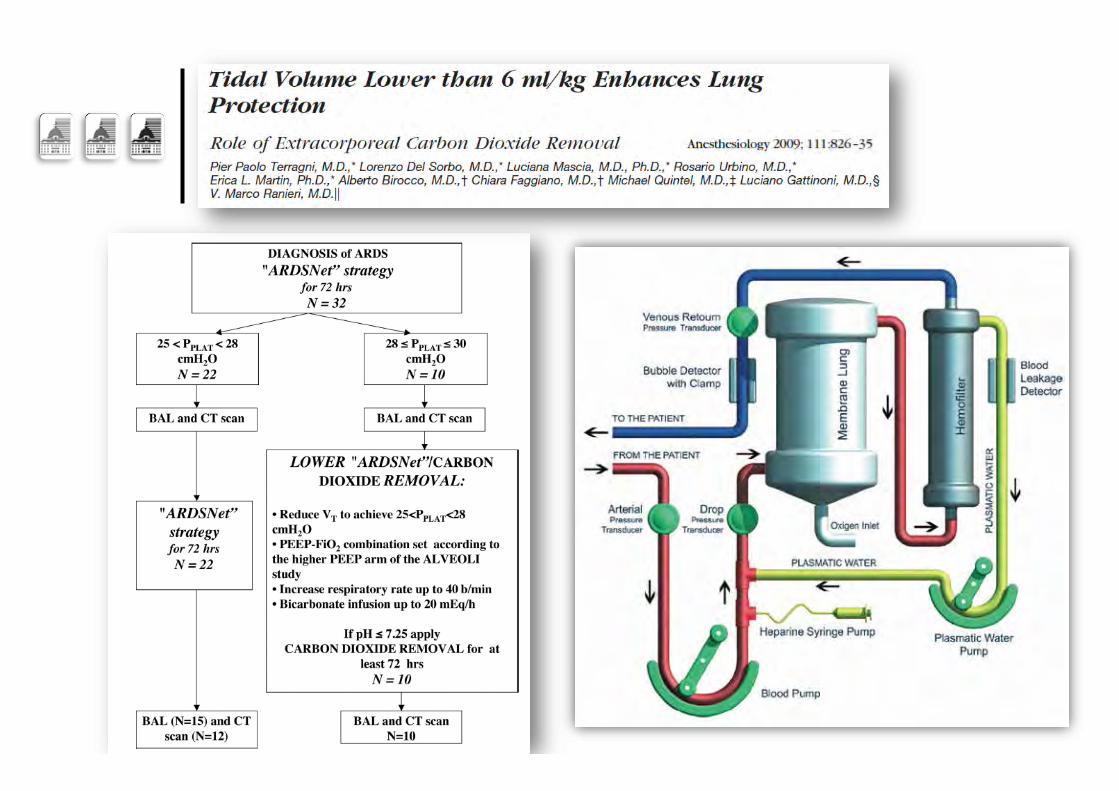
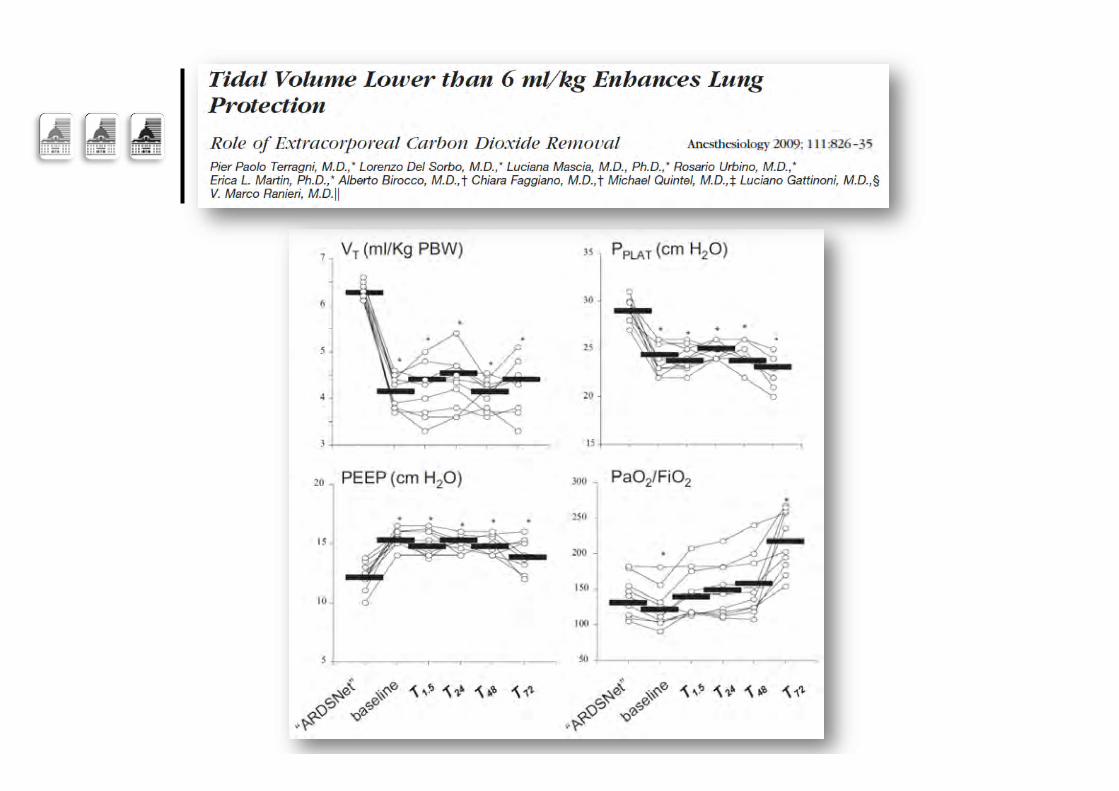
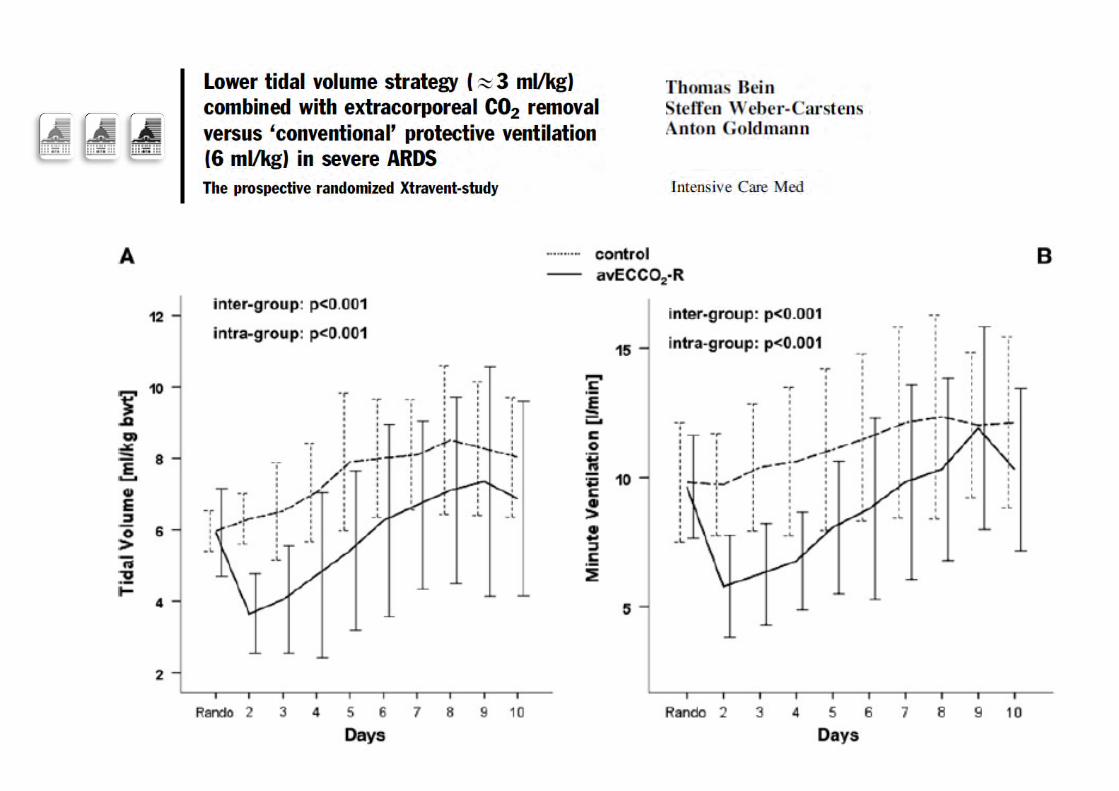
¢ Further decrease of Vt l From 6 to 5, 4 or 3 ml/kg IBW l To decrease Pplat <25 cm H2O l To further reduce VILI l With sufficient PEEP to prevent lung derecruitment
¢ Induced Hypercapnia controlled by extracorporeal CO2 removal l “CO2 dialysis” l Low-flow devices
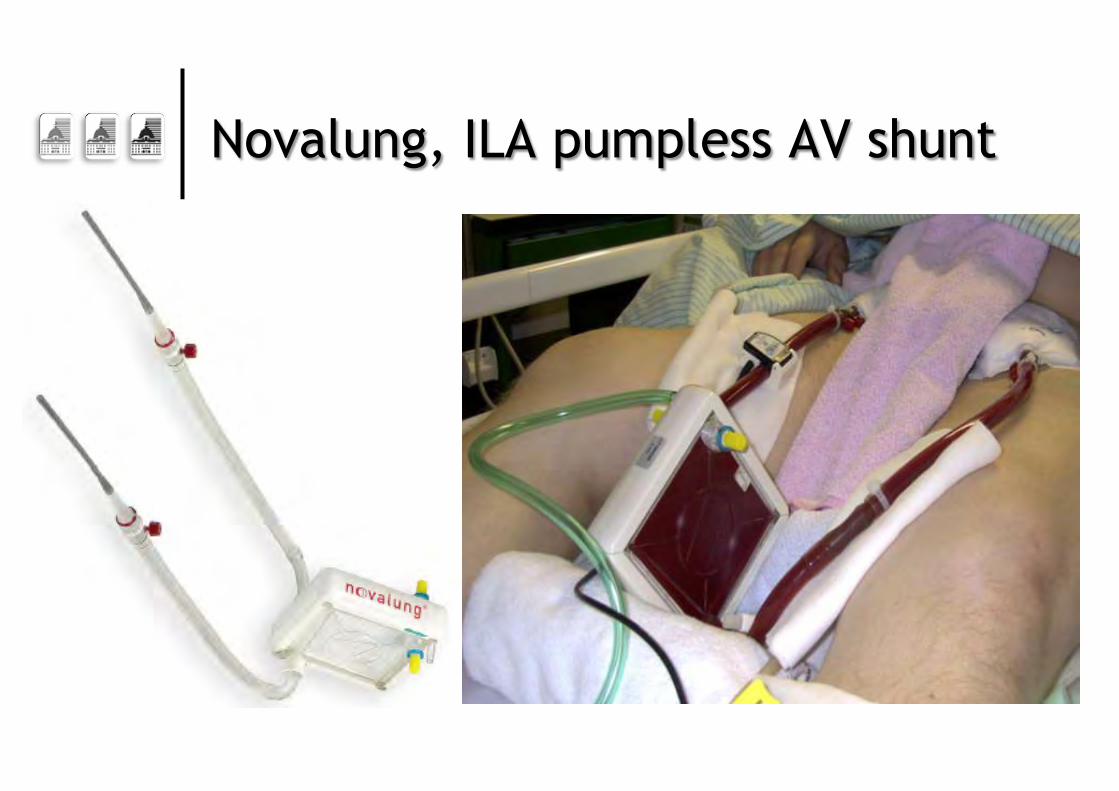
Novalung, ILA pumpless AV shunt
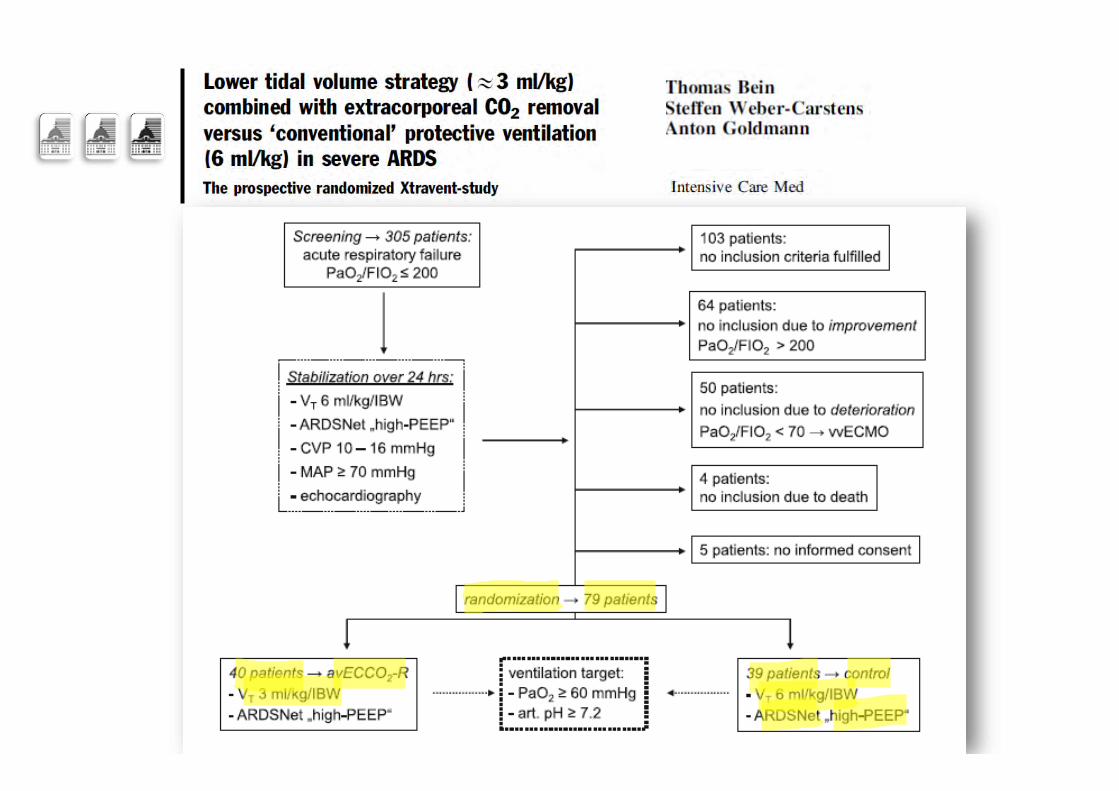
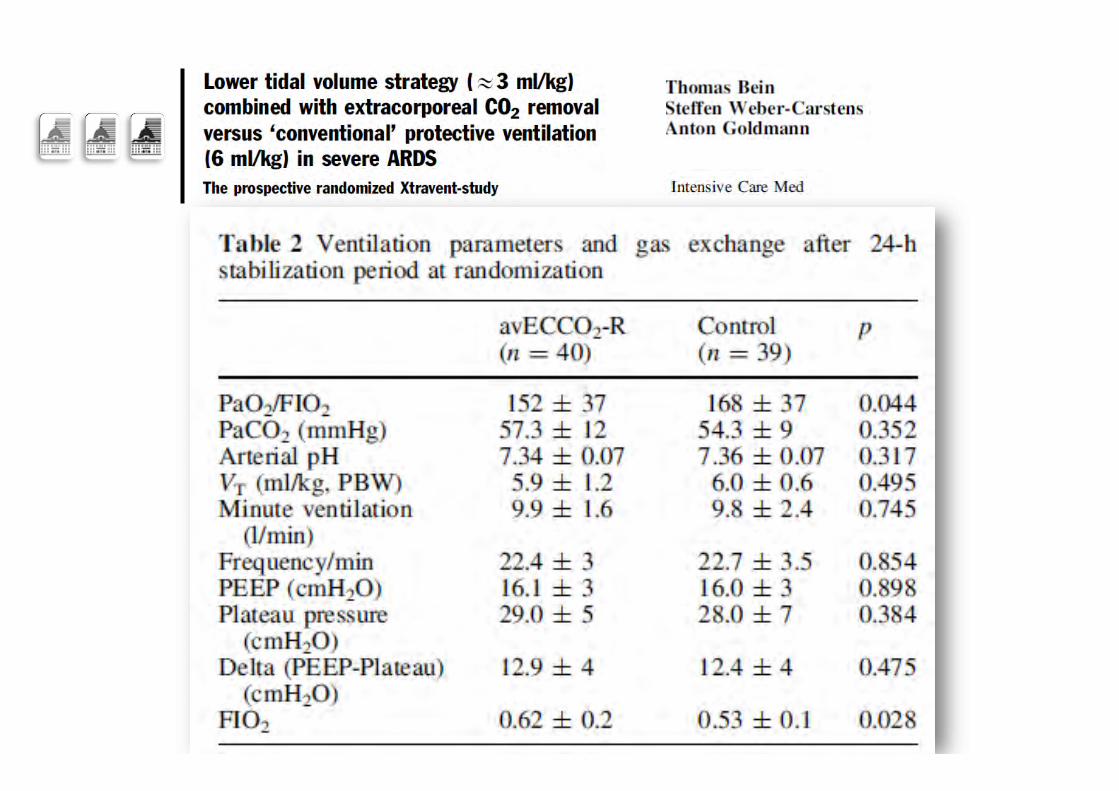
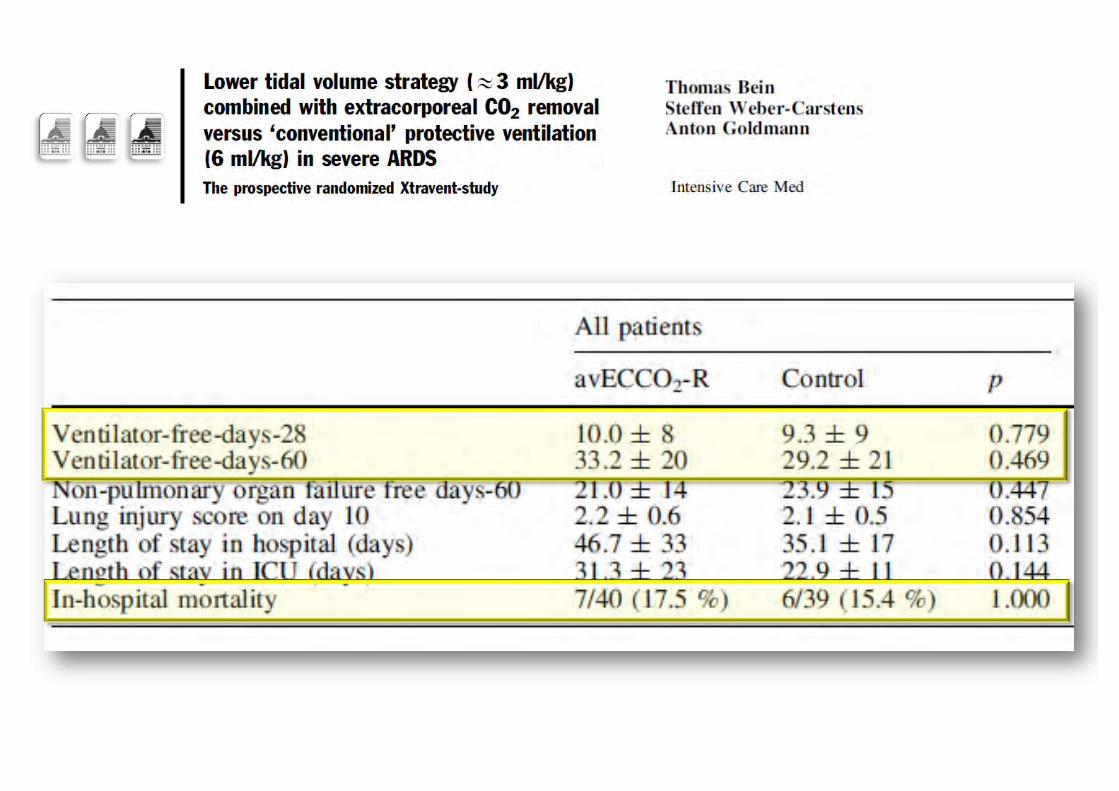
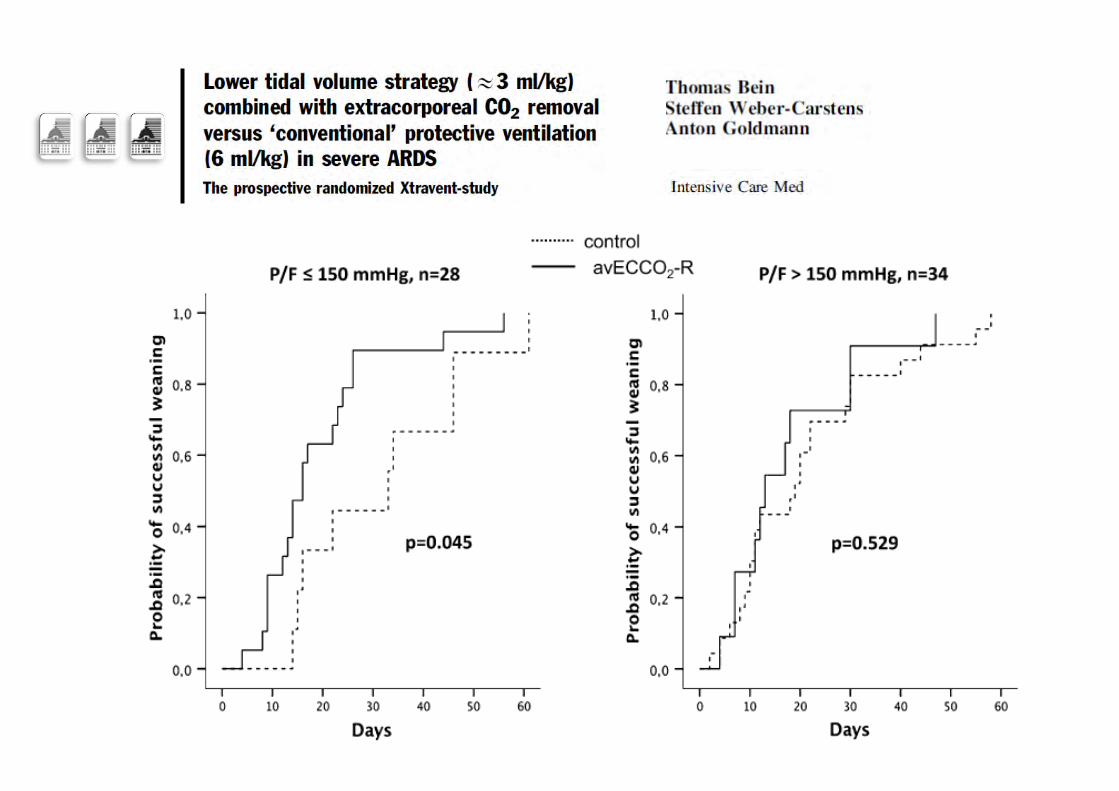
The Xtravent trial
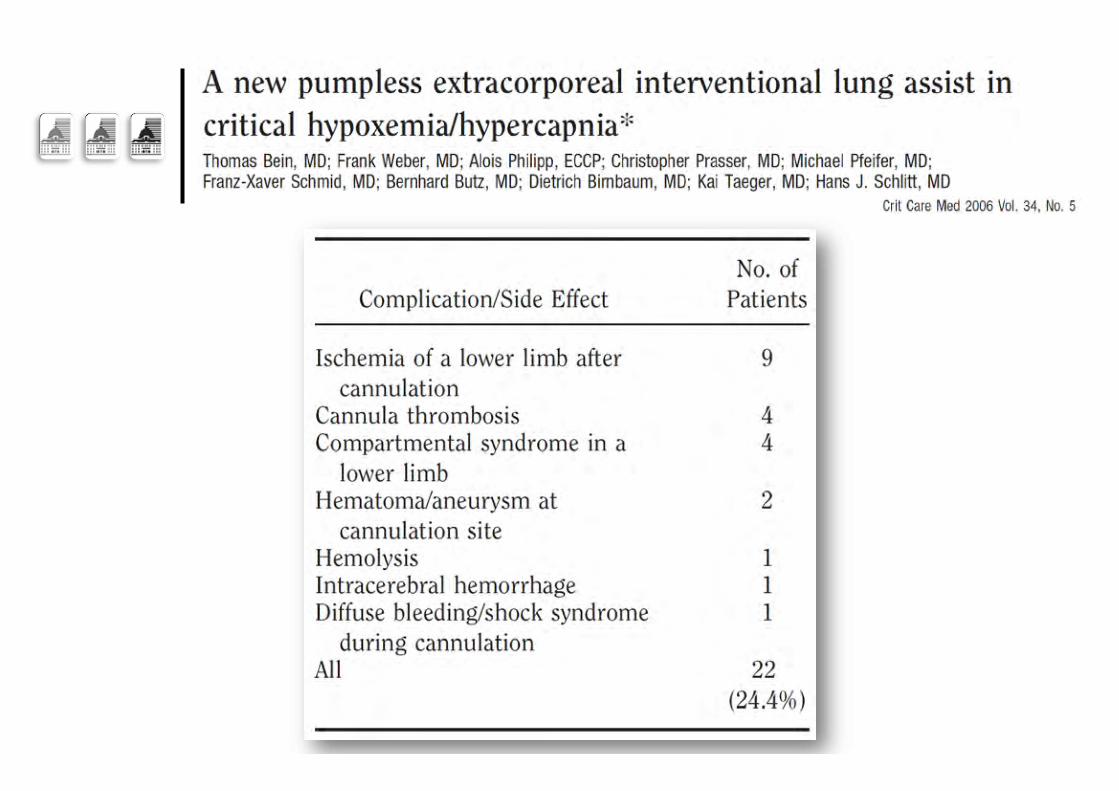
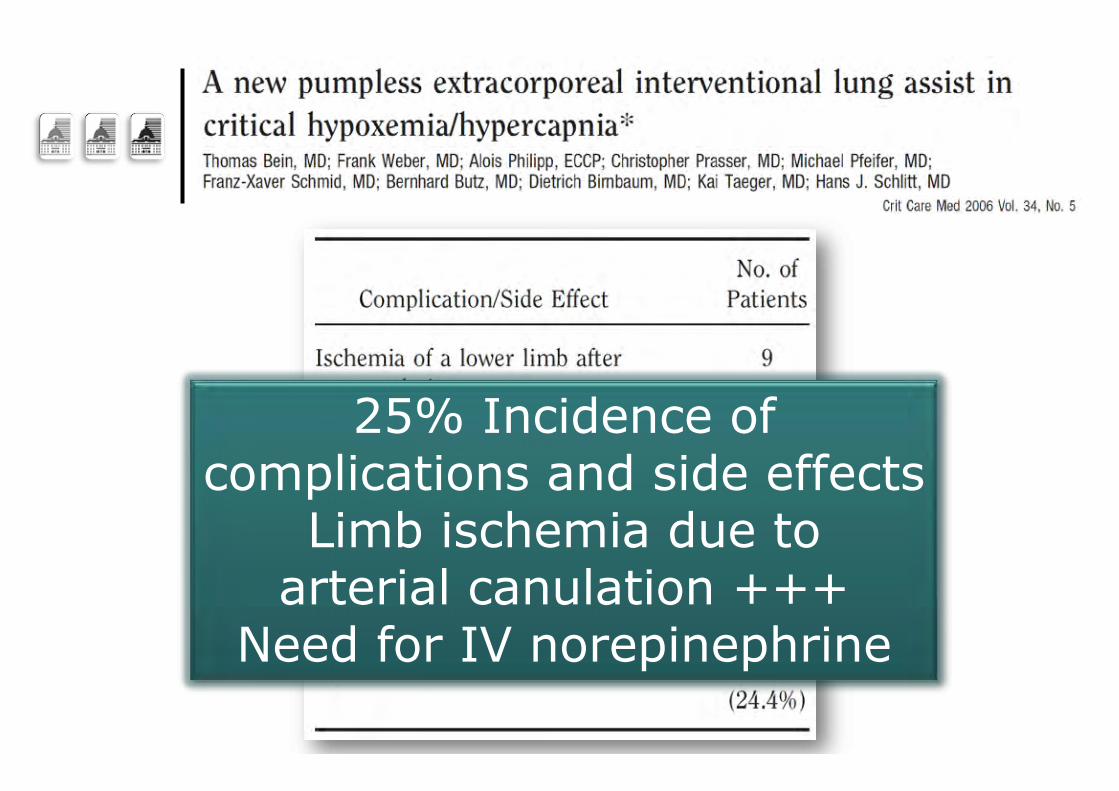
25% Incidence of complications and side effects
Limb ischemia due to arterial canulation +++
Need for IV norepinephrine
Techniques of the 2010’s…
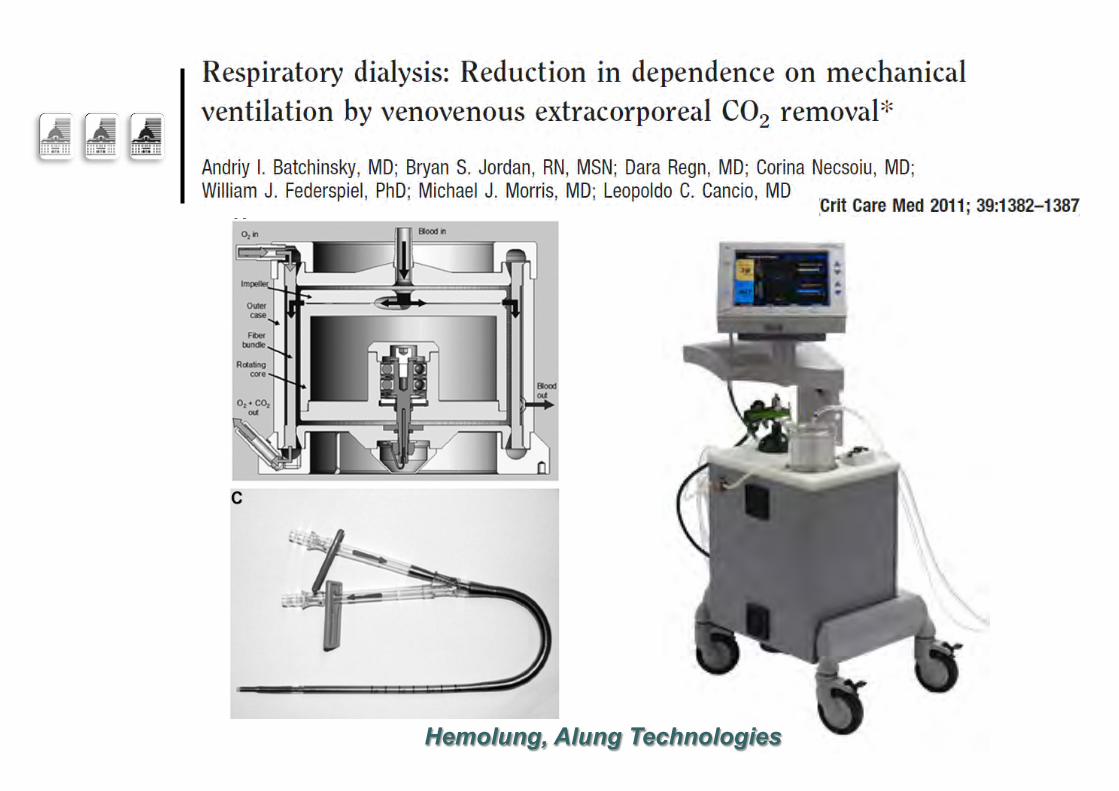
Hemolung, Alung Technologies

PALP, MAQUET®
PrismaLung, Amplya…
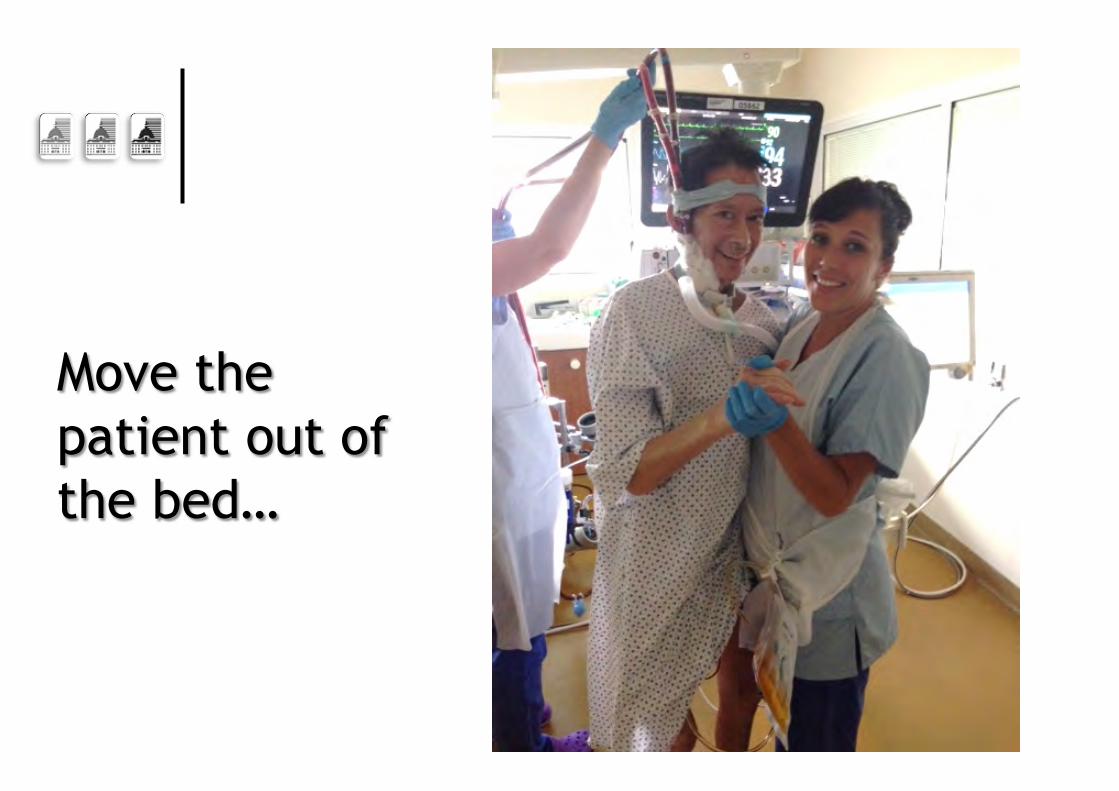
Move the patient out of the bed…
More to come…
“In God we trust; all others must bring data…” W. Edwards Deming (1900-1993)
A Strategy of UltraProtective lung ventilation With Extracorporeal CO2 Removal for
New-Onset moderate to seVere ARDS
The SUPERNOVA trial
VV-ExtraCorporeal Membrane Oxygenation
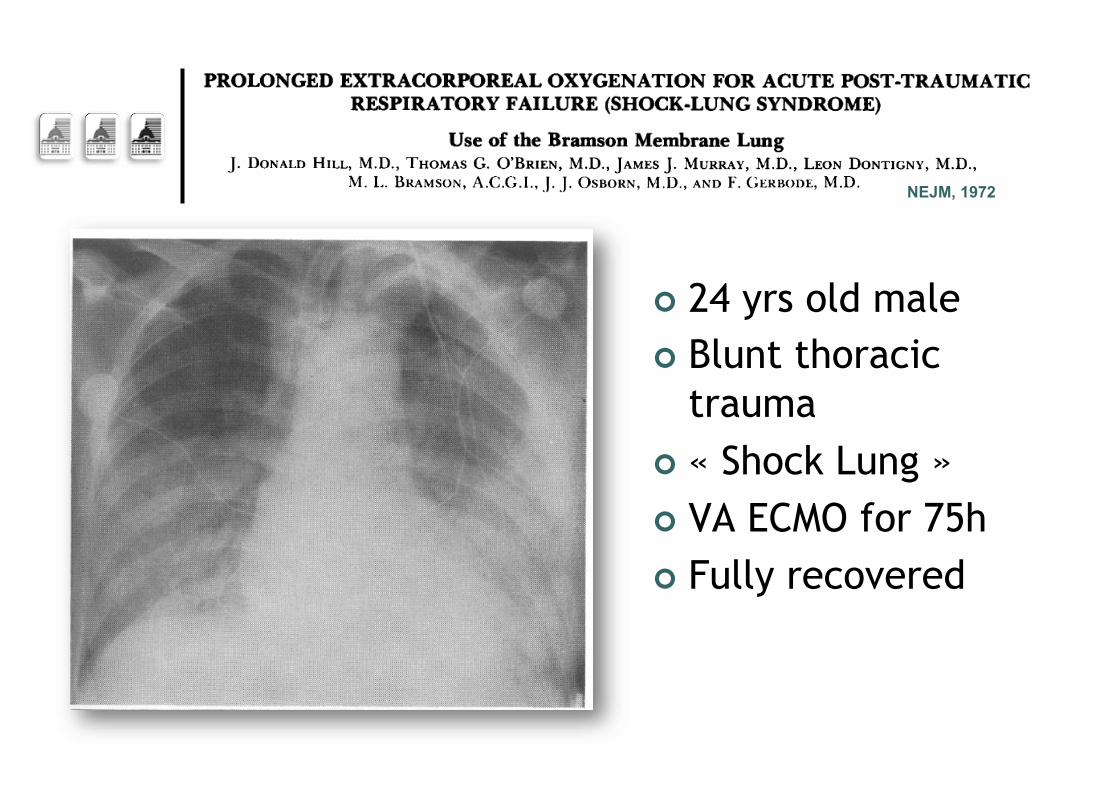
NEJM, 1972
¢ 24 yrs old male ¢ Blunt thoracic
trauma ¢ « Shock Lung » ¢ VA ECMO for 75h ¢ Fully recovered
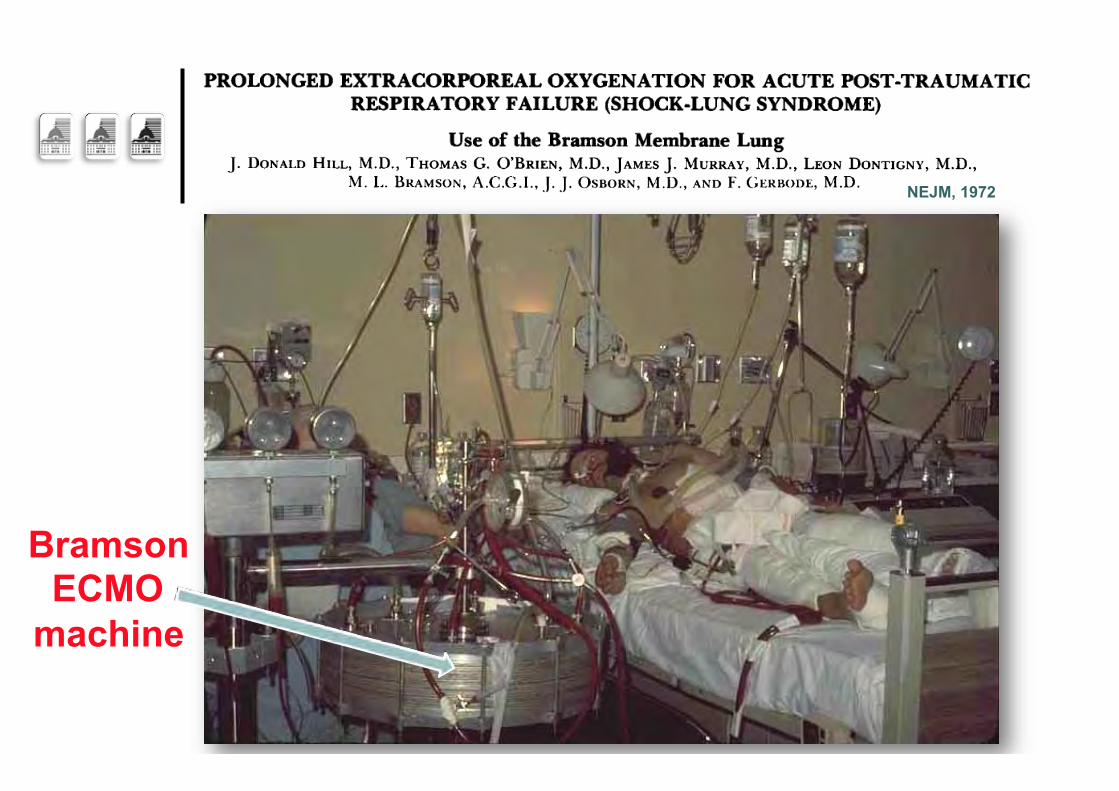
NEJM, 1972
Bramson ECMO
machine
NEJM, 1972
Did he survive despite ECMO????
2009… ECMO strikes back!
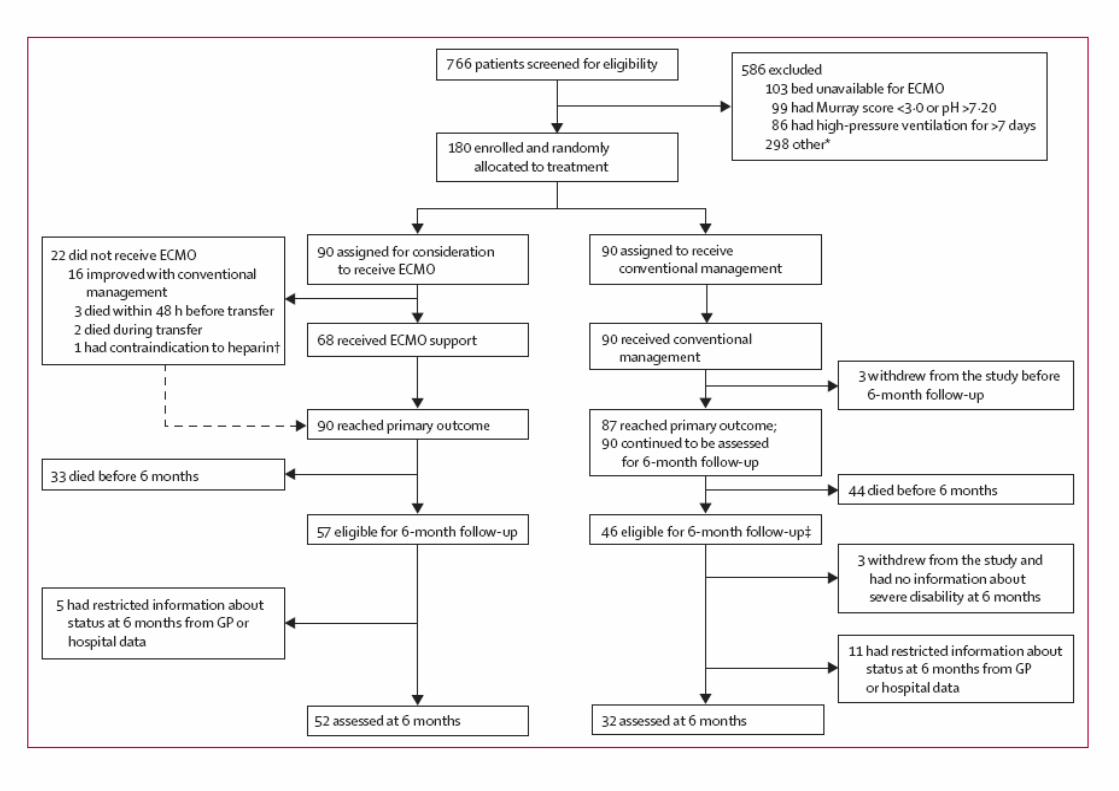
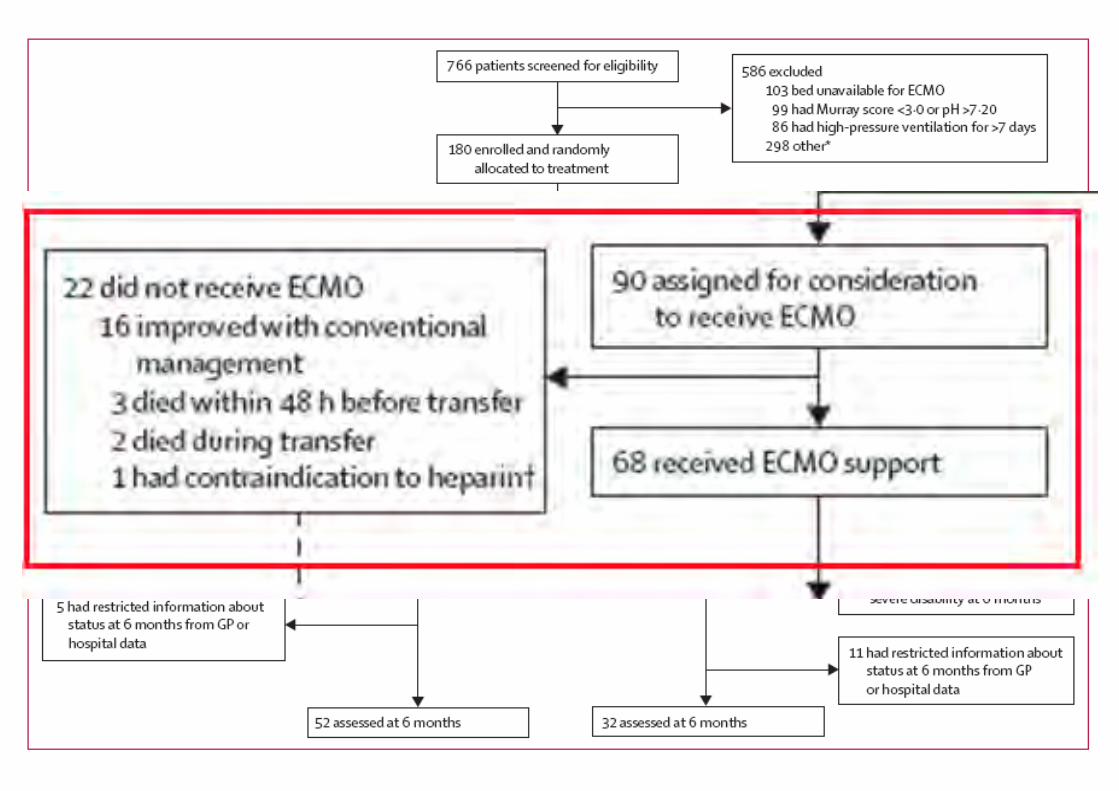
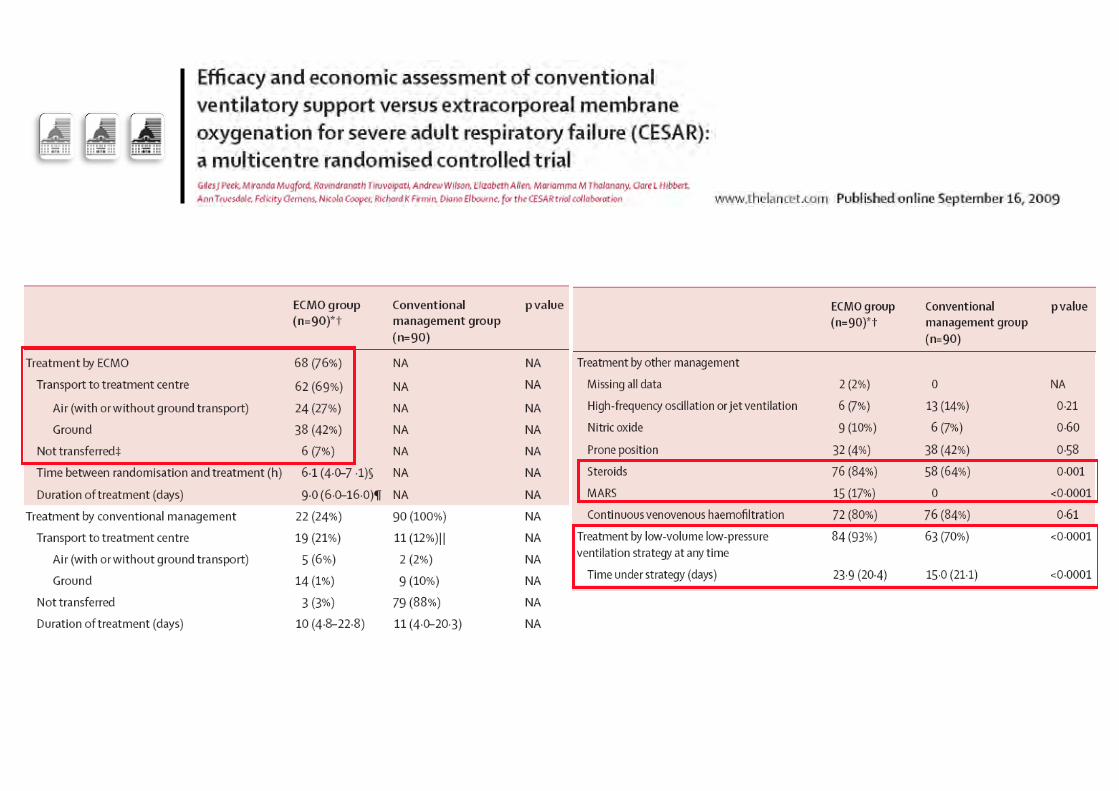
The CESAR trial
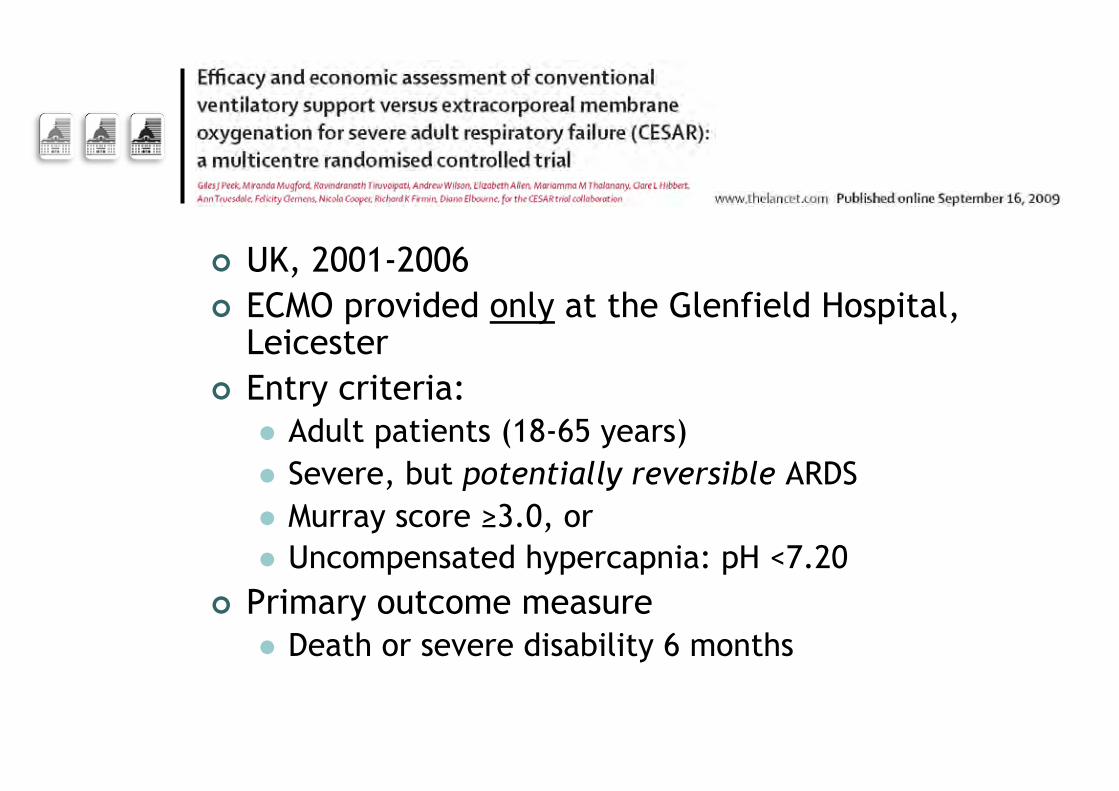
¢ UK, 2001-2006 ¢ ECMO provided only at the Glenfield Hospital,
Leicester ¢ Entry criteria:
l Adult patients (18-65 years) l Severe, but potentially reversible ARDS l Murray score ≥3.0, or l Uncompensated hypercapnia: pH <7.20
¢ Primary outcome measure l Death or severe disability 6 months
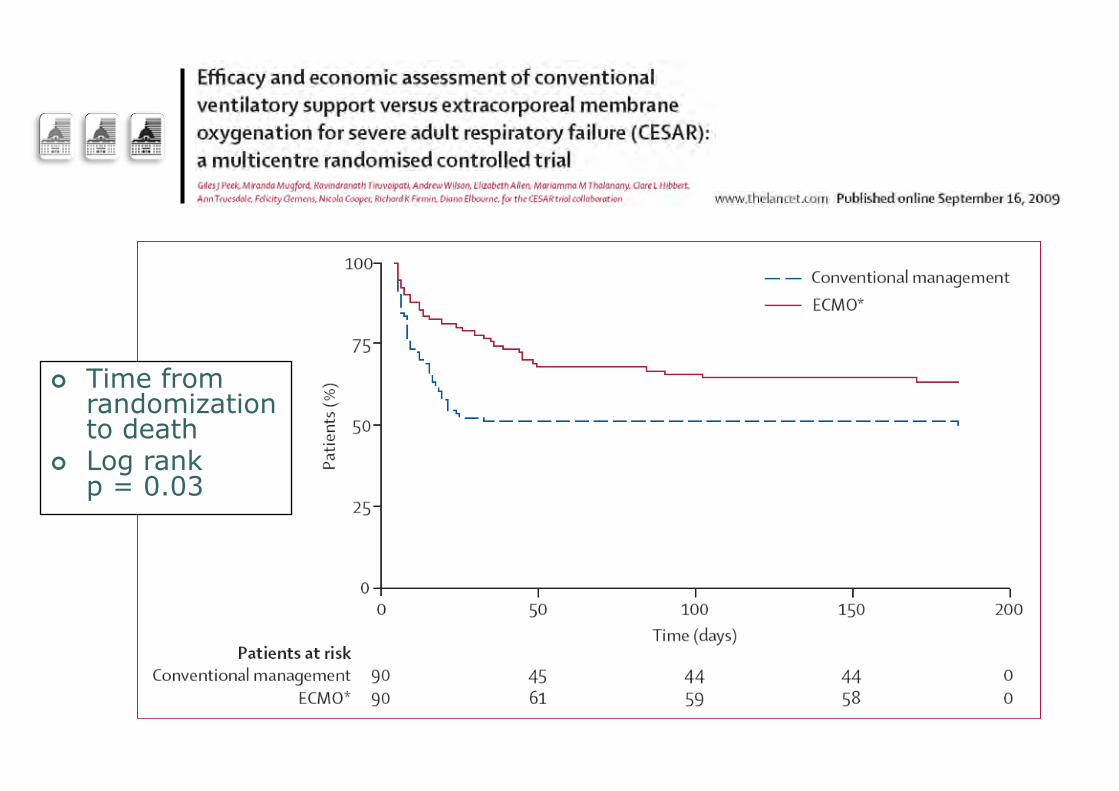
¢ Time from randomization to death
¢ Log rank p = 0.03
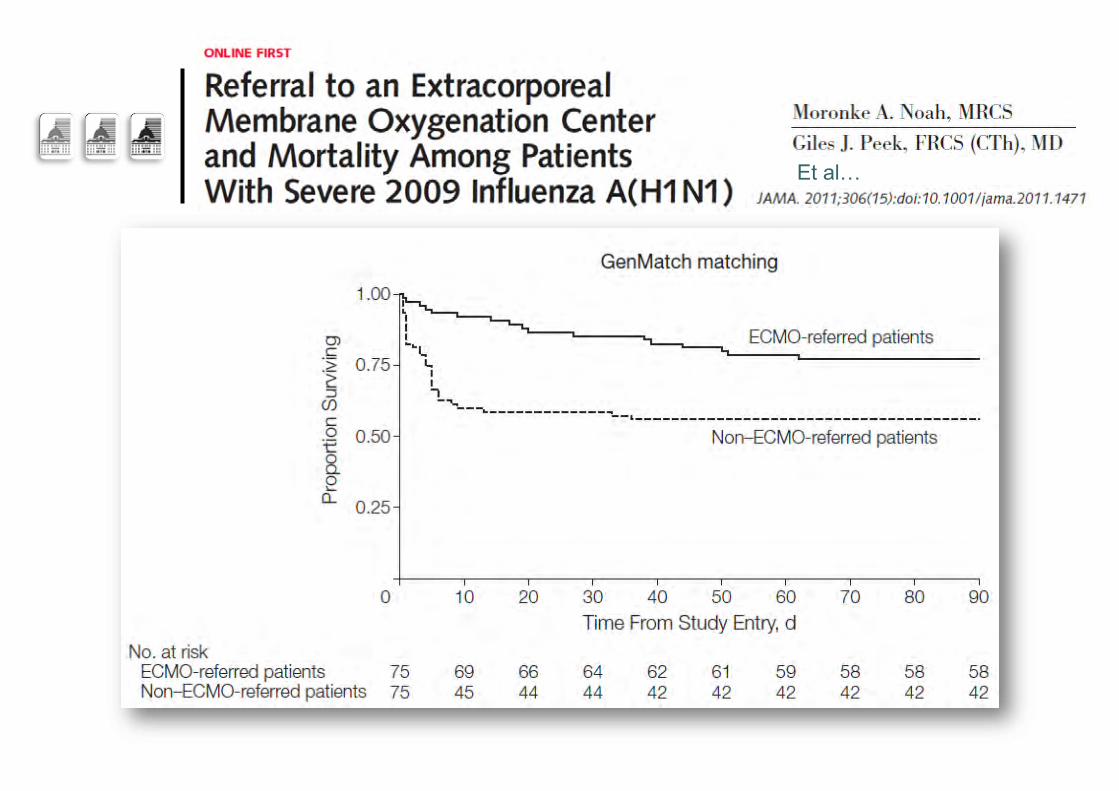
Influenza A (H1N1)v09 …
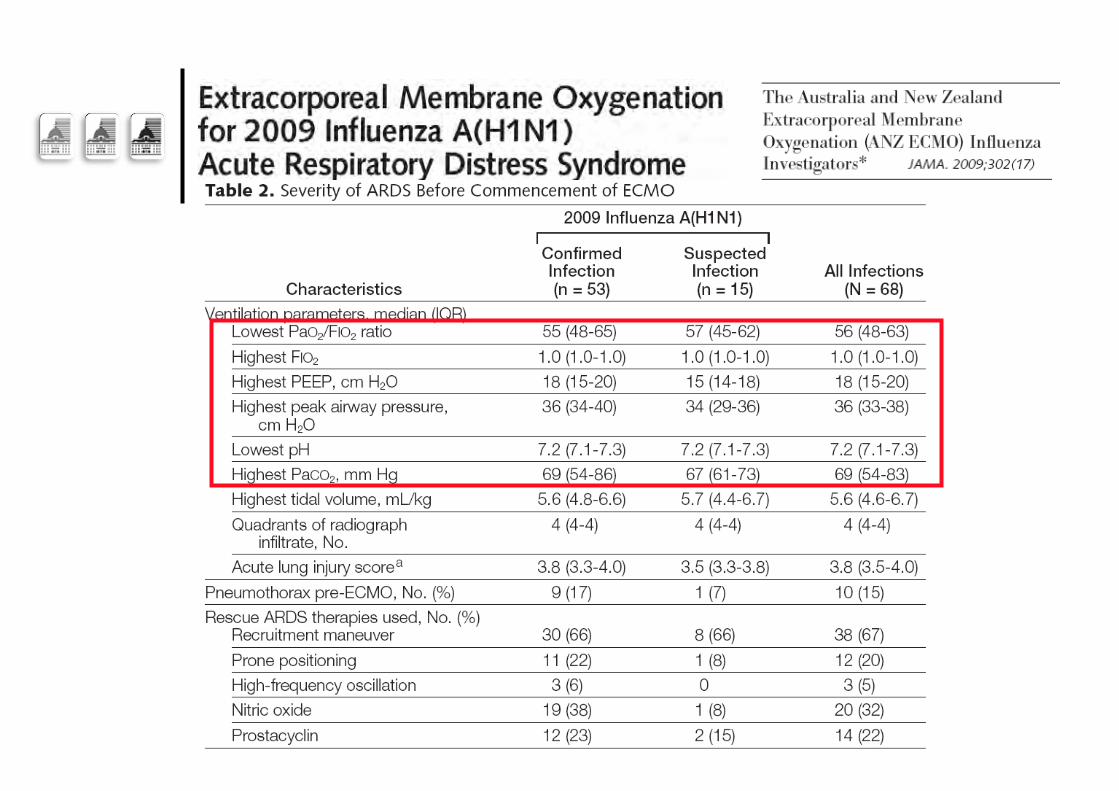
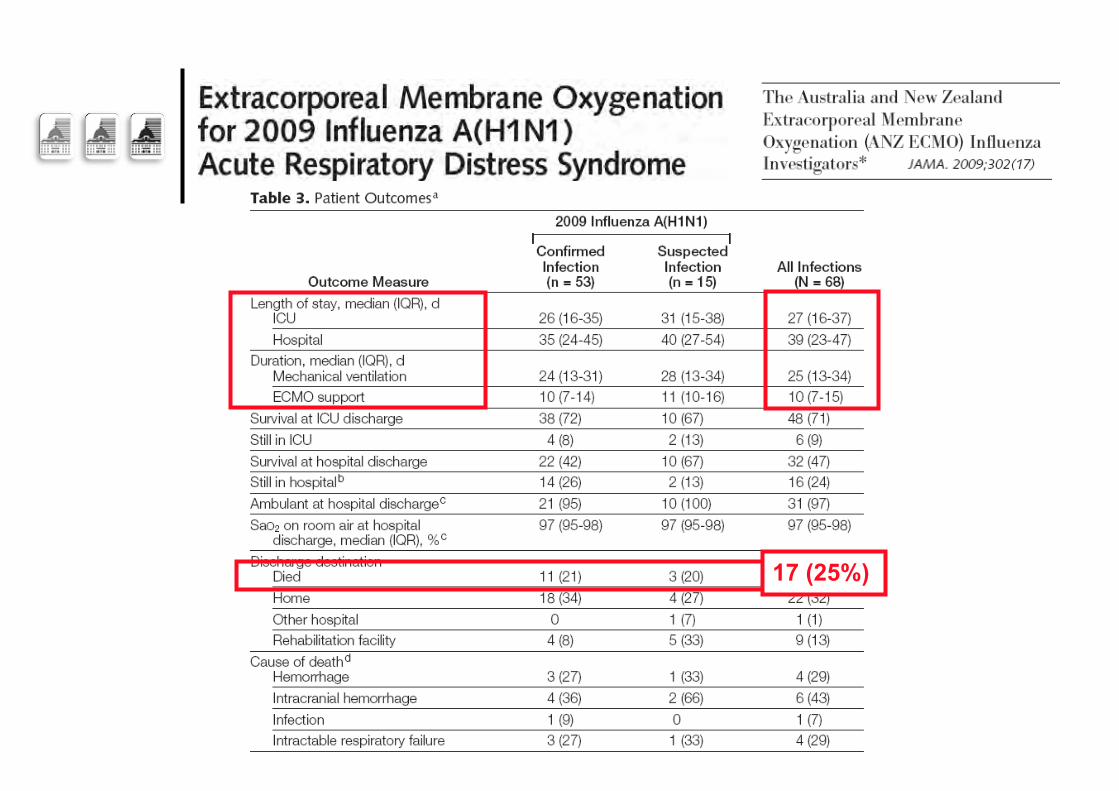
17 (25%)
Et al…
Et al…
Et al…
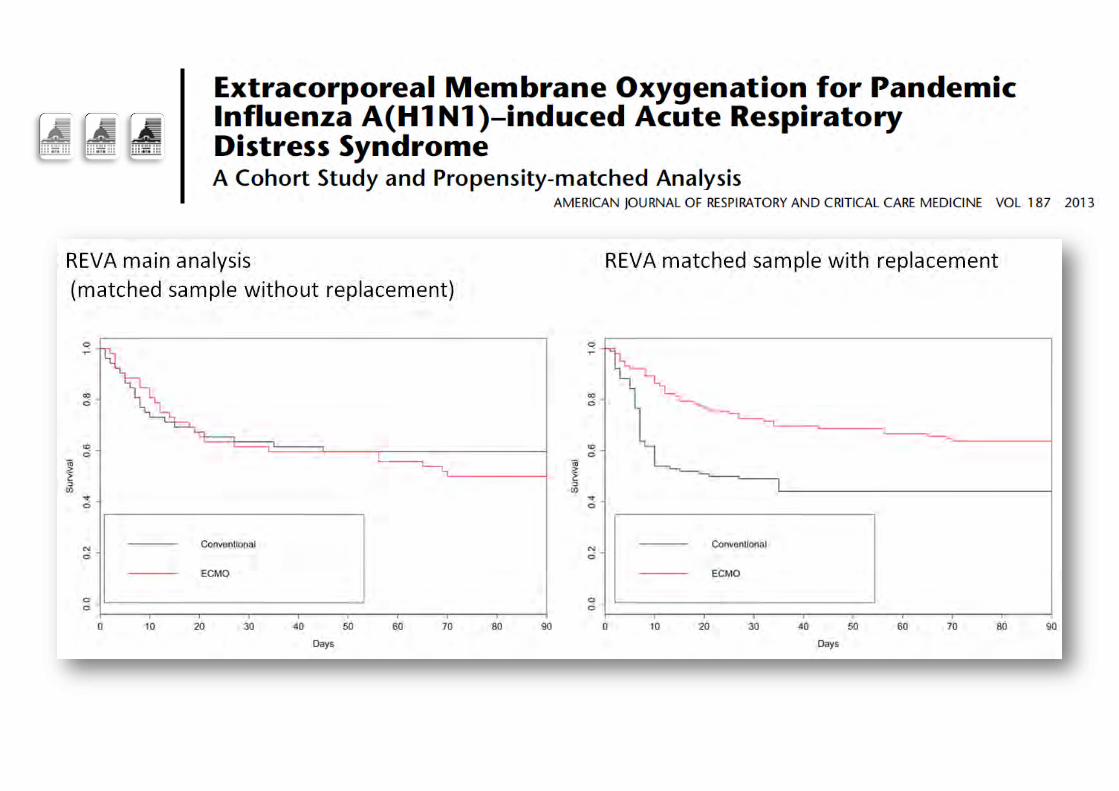
The French REVA H1N1 ECMO cohort
¢ The French REVA Registry collected data of patients hospitalized in ICUs for H1N1-associated ARDS
¢ Analysis of factors associated with death among 123 patients who received ECMO
¢ Case-control study with matching on a propensity score to receive ECMO
When to decide on the initiation of ECMO?
Can we rely on guidelines???…
SDRA lié à la grippe H1N1
Recommandations pour la ventilation
A. Mercat, J-C.M. Richard, A. Combes, J. Chastre, J.D. Ricard, D. Dreyfuss, L. Brochard
Réseau de Recherche en Ventilation Artificielle
(REVA)
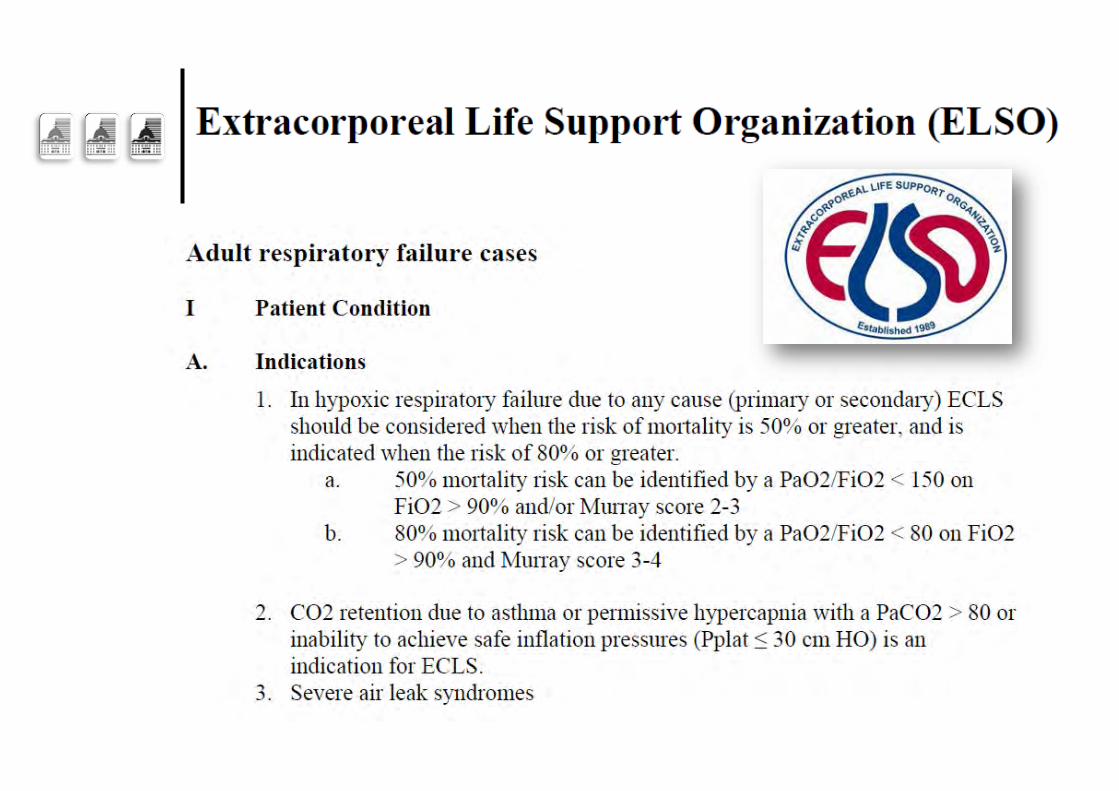
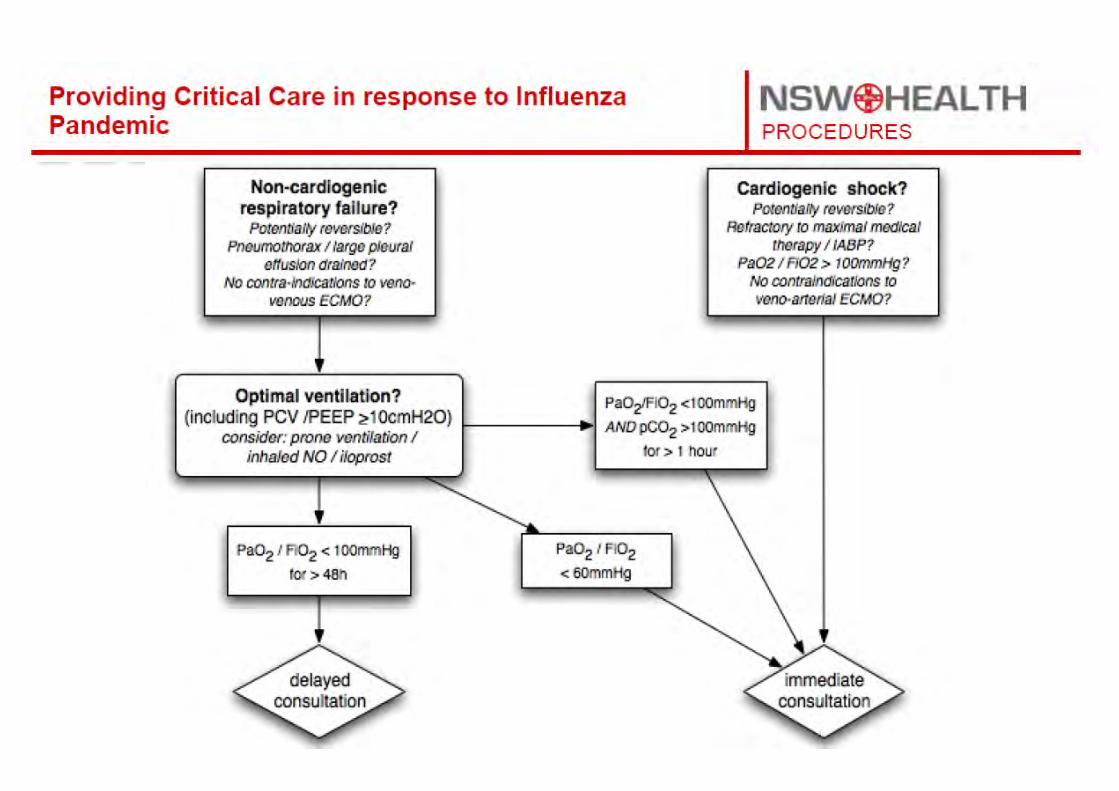
ECMO : potential indications
• Refractory hypoxemia: PaO2/FiO2 < 50, persistent *
Despite: FiO2 > 80 %, PEEP (≤ 20 cmH2O)
Targeting Pplat = 32 cmH2O, prone position +/- NOi
• Plateau Pressure ≥ 35 cmH2O
despite reducing PEEP to 5 cmH2O
AND Vt to 4 ml/kg with pH remaining ≥ 7,15 * : Should also account for disease’s type and evolution
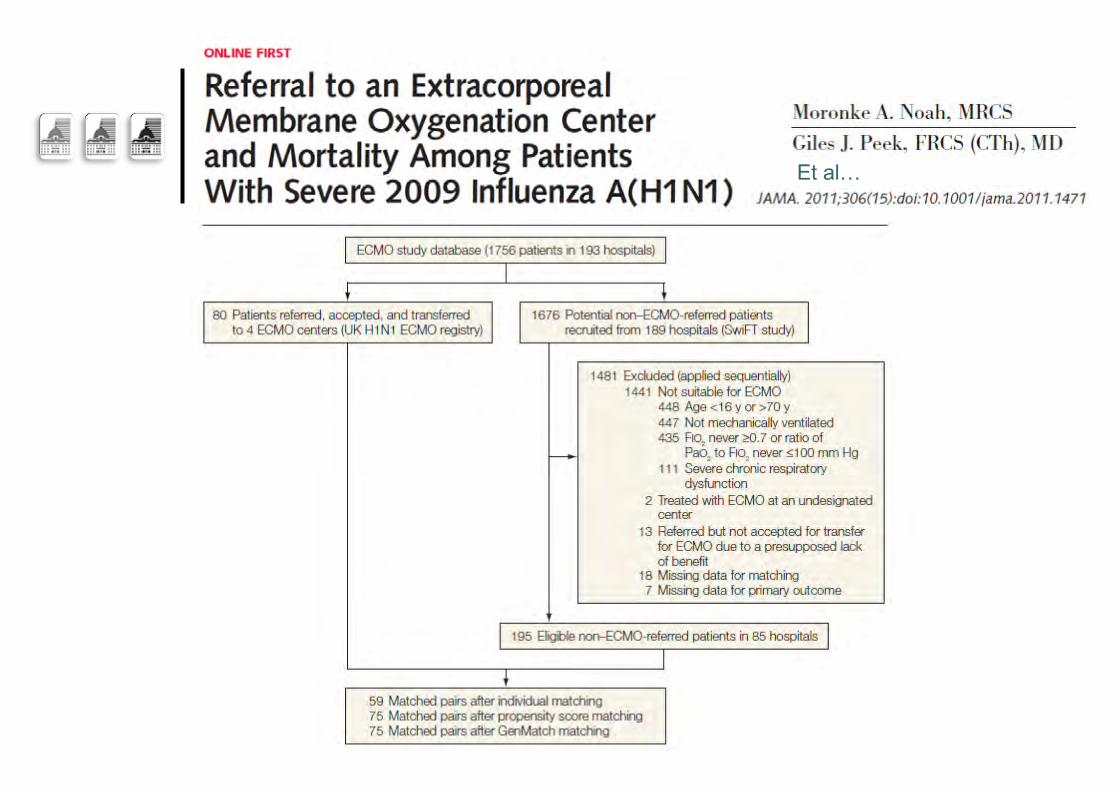
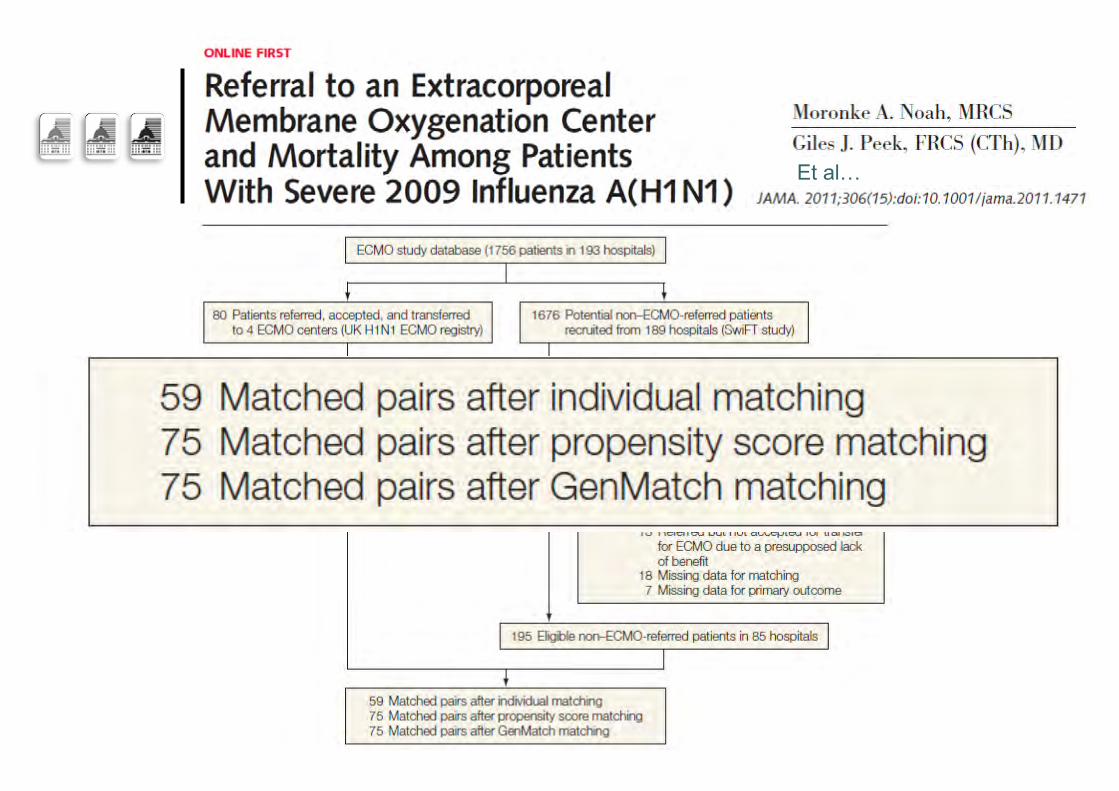
How to improve outcomes?
Increase adherence to ARDS treatment protocols
Including early prone positioning…
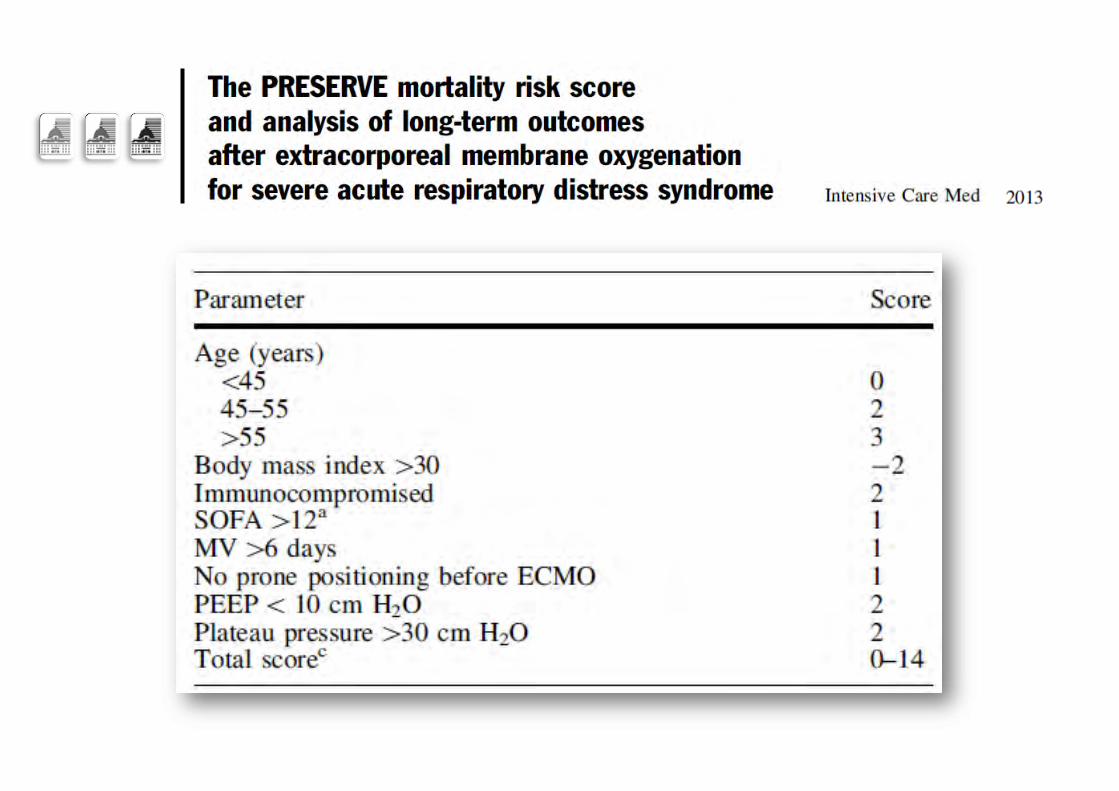
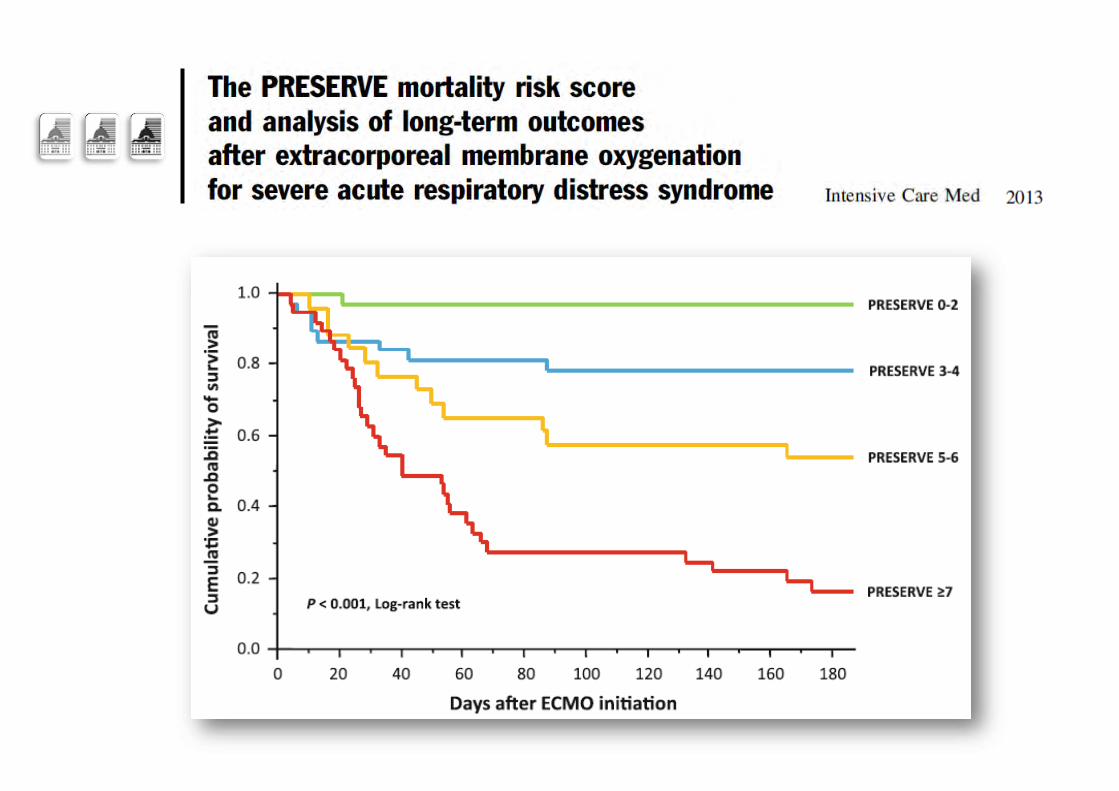
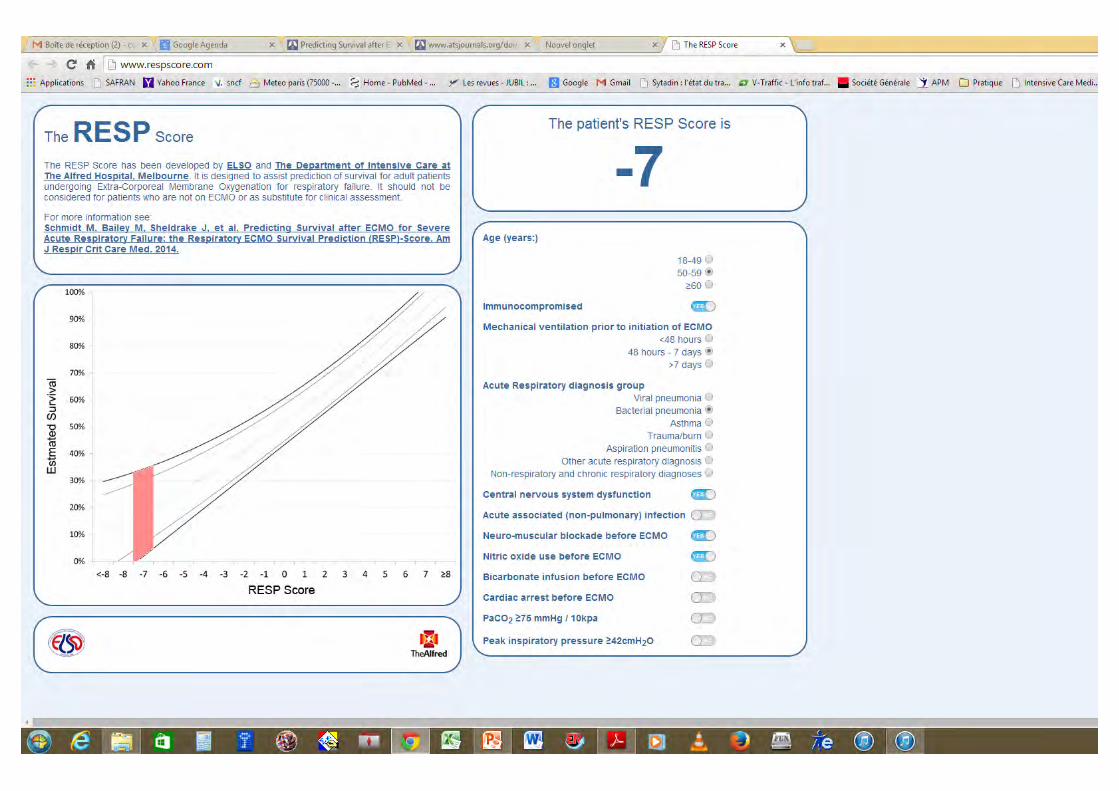
Better selection of severe ARDS patients for ECMO treatment…

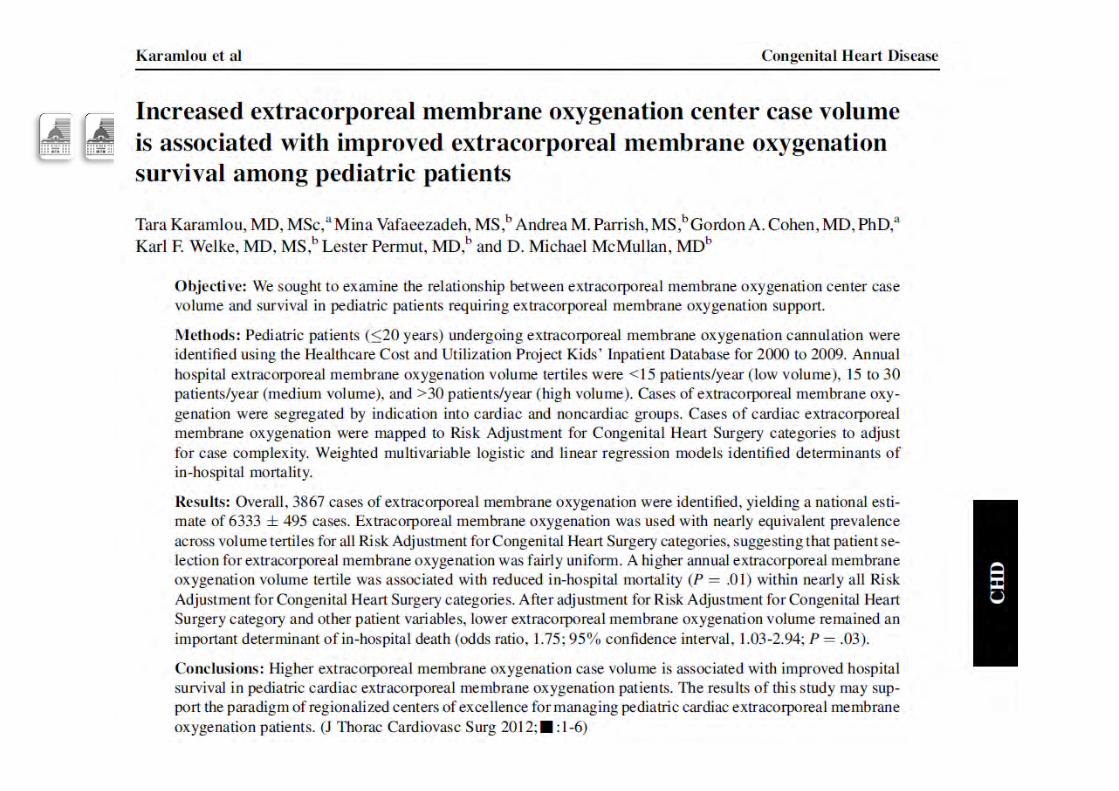
Limitation of the number of ECMO centers
Is associated with better outcomes…
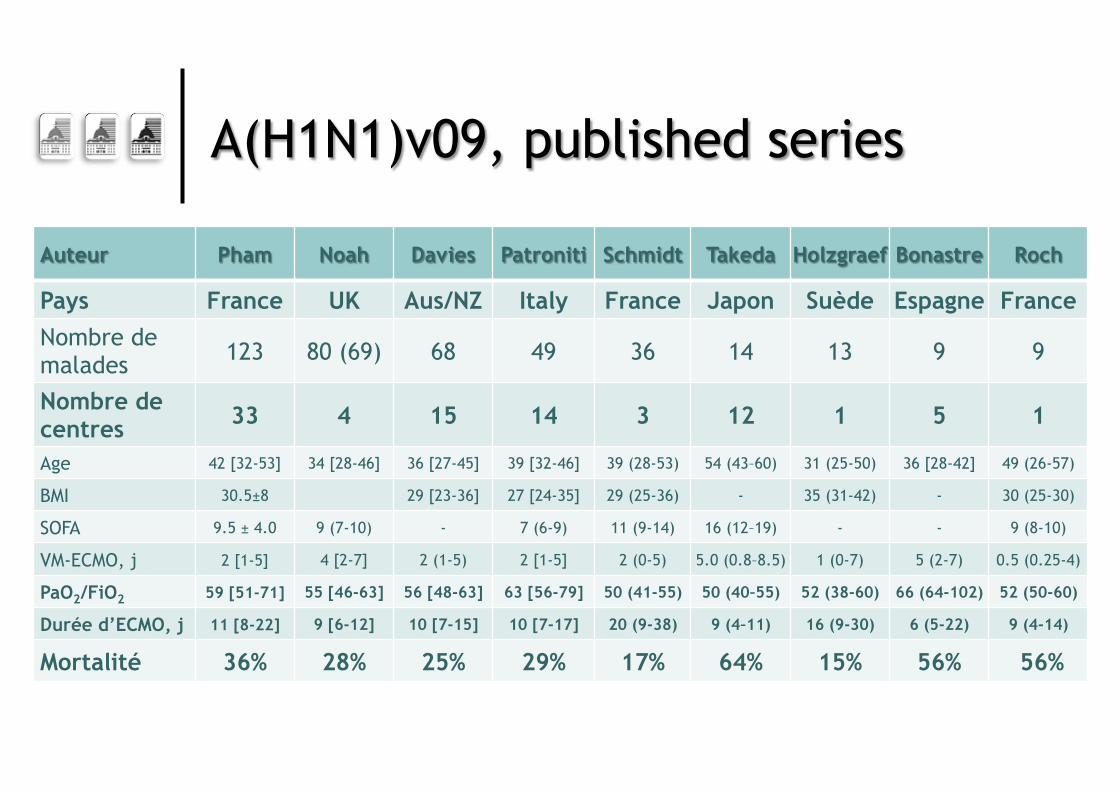
Auteur Pham Noah Davies Patroniti Schmidt Takeda Holzgraef Bonastre Roch
Pays France UK Aus/NZ Italy France Japon Suède Espagne France Nombre de malades 123 80 (69) 68 49 36 14 13 9 9
Nombre de centres 33 4 15 14 3 12 1 5 1
Age 42 [32-53] 34 [28-46] 36 [27-45] 39 [32-46] 39 (28-53) 54 (43–60) 31 (25-50) 36 [28-42] 49 (26-57)
BMI 30.5±8 29 [23-36] 27 [24-35] 29 (25-36) - 35 (31-42) - 30 (25-30)
SOFA 9.5 ± 4.0 9 (7-10) - 7 (6-9) 11 (9-14) 16 (12–19) - - 9 (8-10)
VM-ECMO, j 2 [1-5] 4 [2-7] 2 (1-5) 2 [1-5] 2 (0-5) 5.0 (0.8–8.5) 1 (0-7) 5 (2-7) 0.5 (0.25-4)
PaO2/FiO2 59 [51-71] 55 [46-63] 56 [48-63] 63 [56-79] 50 (41-55) 50 (40–55) 52 (38-60) 66 (64-102) 52 (50-60)
Durée d’ECMO, j 11 [8-22] 9 [6-12] 10 [7-15] 10 [7-17] 20 (9-38) 9 (4–11) 16 (9-30) 6 (5-22) 9 (4-14)
Mortalité 36% 28% 25% 29% 17% 64% 15% 56% 56%
A(H1N1)v09, published series
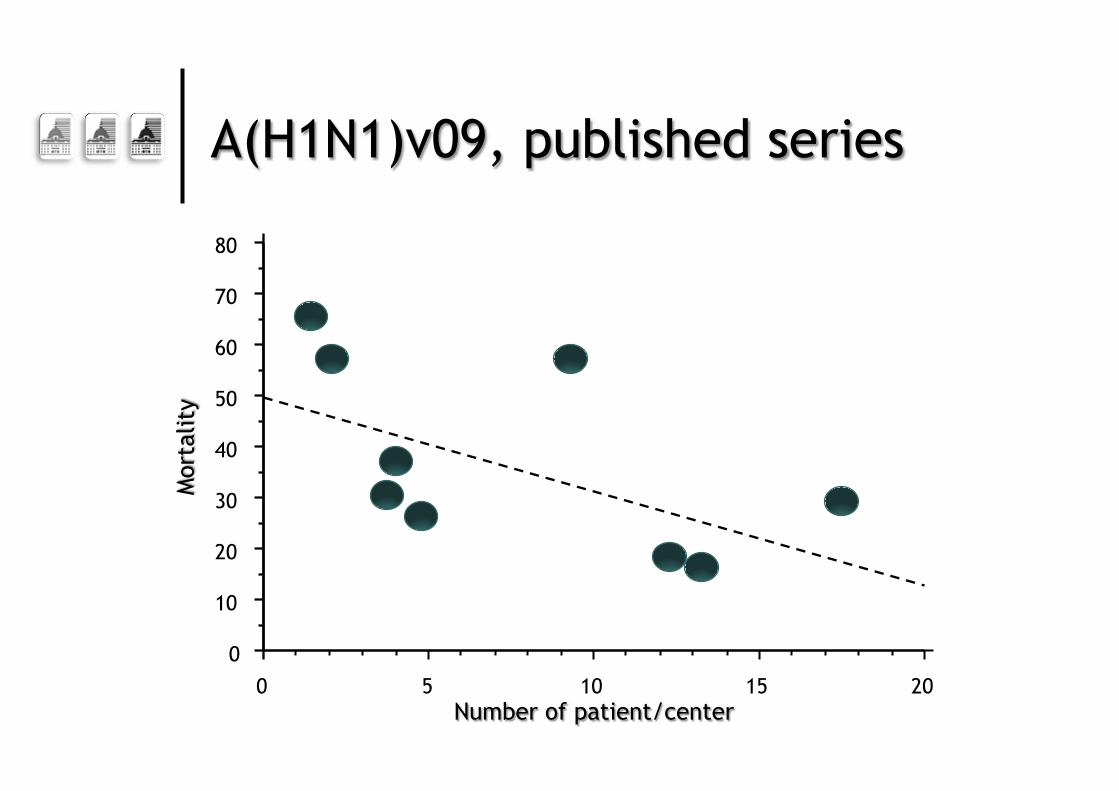
A(H1N1)v09, published series
0 10 20 30 40 50 60 70 80
0 5 10 15 20 Number of patient/center
Mor
talit
y
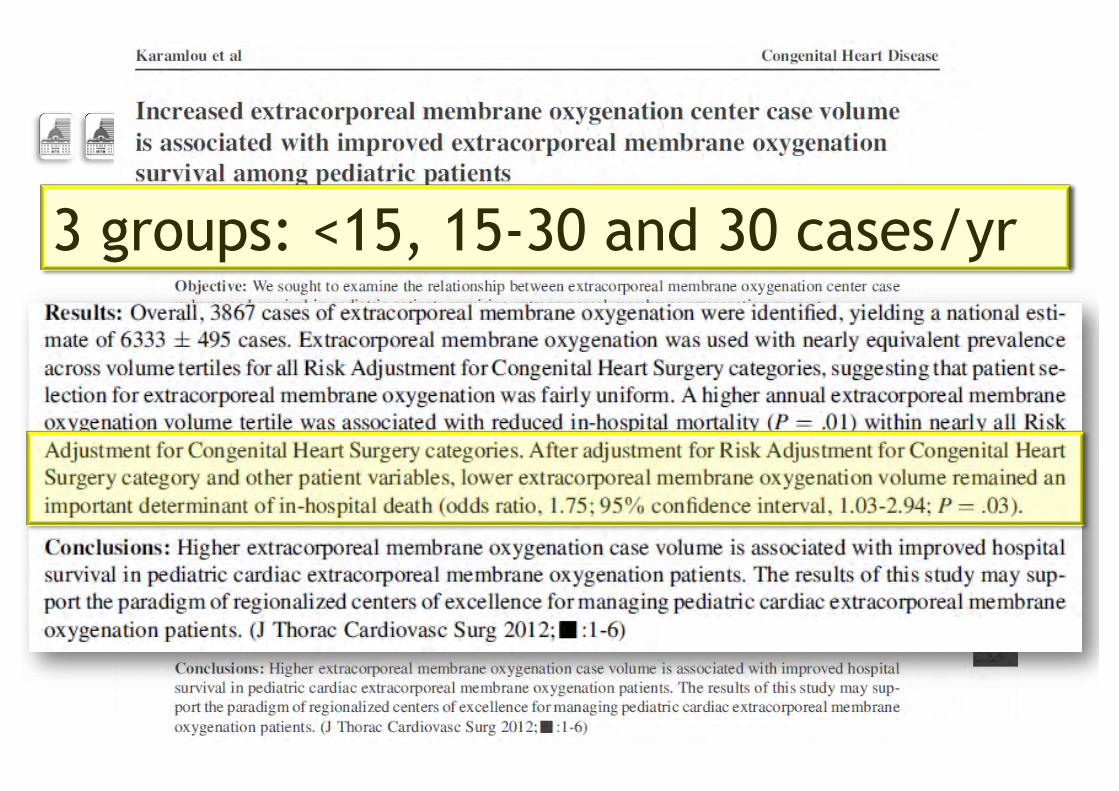
3 groups: <15, 15-30 and 30 cases/yr
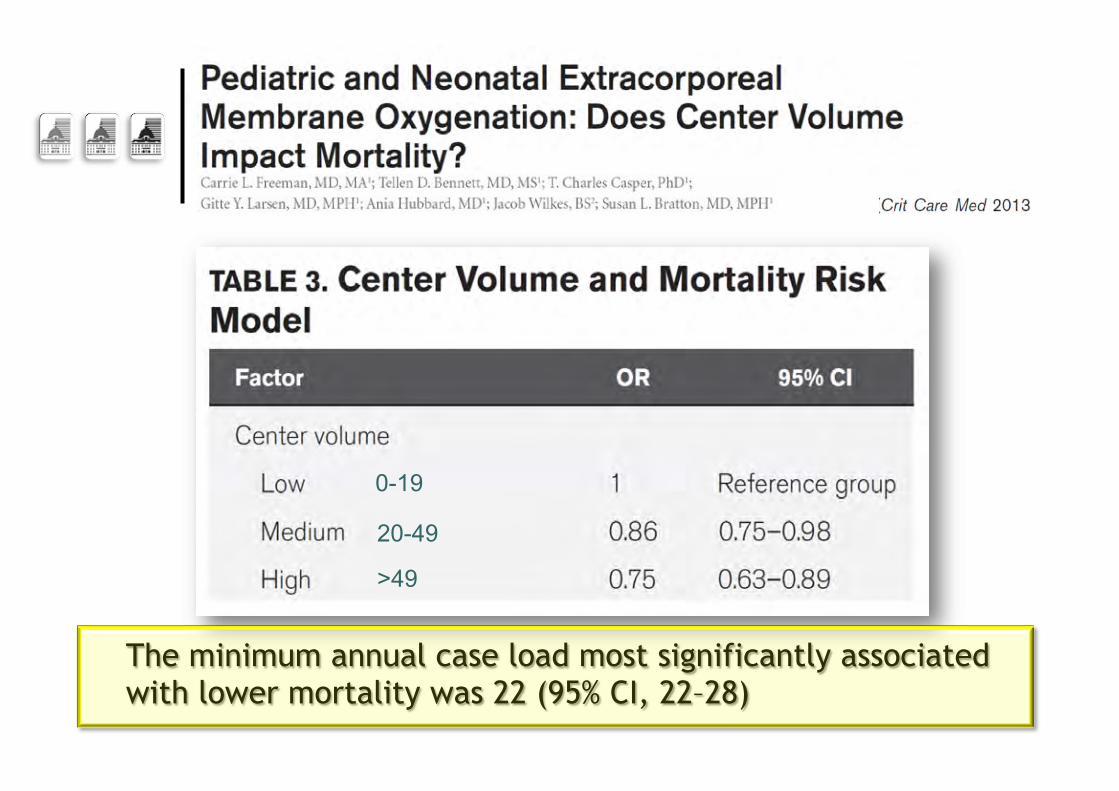
The minimum annual case load most significantly associated with lower mortality was 22 (95% CI, 22–28)
0-19
20-49
>49
Number of potential indications per year…
5-10 per million population/year
Where to perform VV-ECMO?
¢ Experienced centers in both ARDS and ECMO ¢ Better if cardiac and respiratory ECMO combined
on the same site l With experienced intensivists, heart surgeons,
perfusionists, nurses…. l Minimum of 20 total ECMO runs per year
¢ ECMO programs should include a mobile ECMO referral team l Available 24H/7D l Nationwide or regional EMCO networks necessary
International ECMOnet To promote research on ECMO
Designing a new trial…
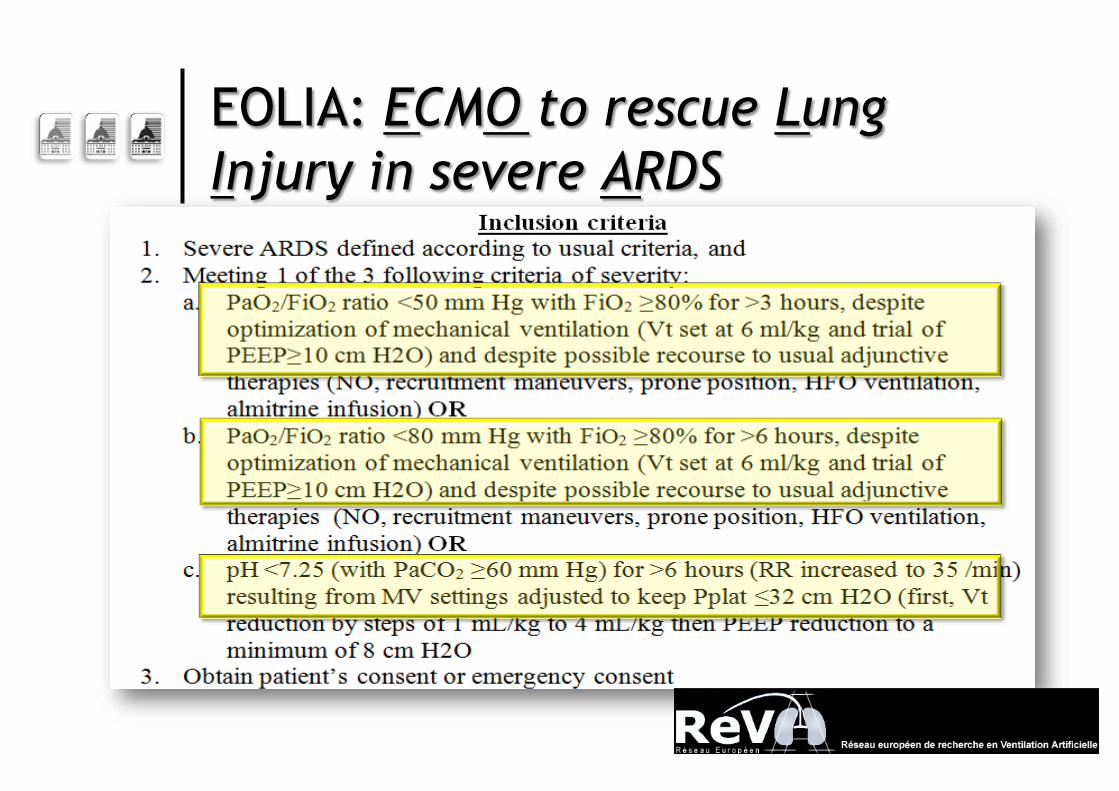
EOLIA: ECMO to rescue Lung Injury in severe ARDS
EOLIA: ECMO to rescue Lung Injury in severe ARDS
¢ Multicenter international randomized controlled trial ¢ Best care possible in the ECMO arm
l ECMO initiated asap for every patient randomized • Using the most recent ECMO technology
l Transport of randomized patients to the referral center UNDER ECMO
l ECMO managed only in highly experienced centers l “Highly protective” MV
• Plateau pressure limited to ≤ 24 cm H2O
EOLIA: ECMO to rescue Lung Injury in severe ARDS
¢ Best care possible in the control arm l MV protocolized using the
“high PEEP – high recruitment” strategy of the EXPRESS trial
l To limit plateau pressure <28-30 cm H2O • Vt limited to 6 ml/kg IBW
l Including Prone positioning l “Ethical” cross-over option to ECMO if the patient
develops refractory hypoxemia
EOLIA: ECMO to rescue Lung Injury in severe ARDS
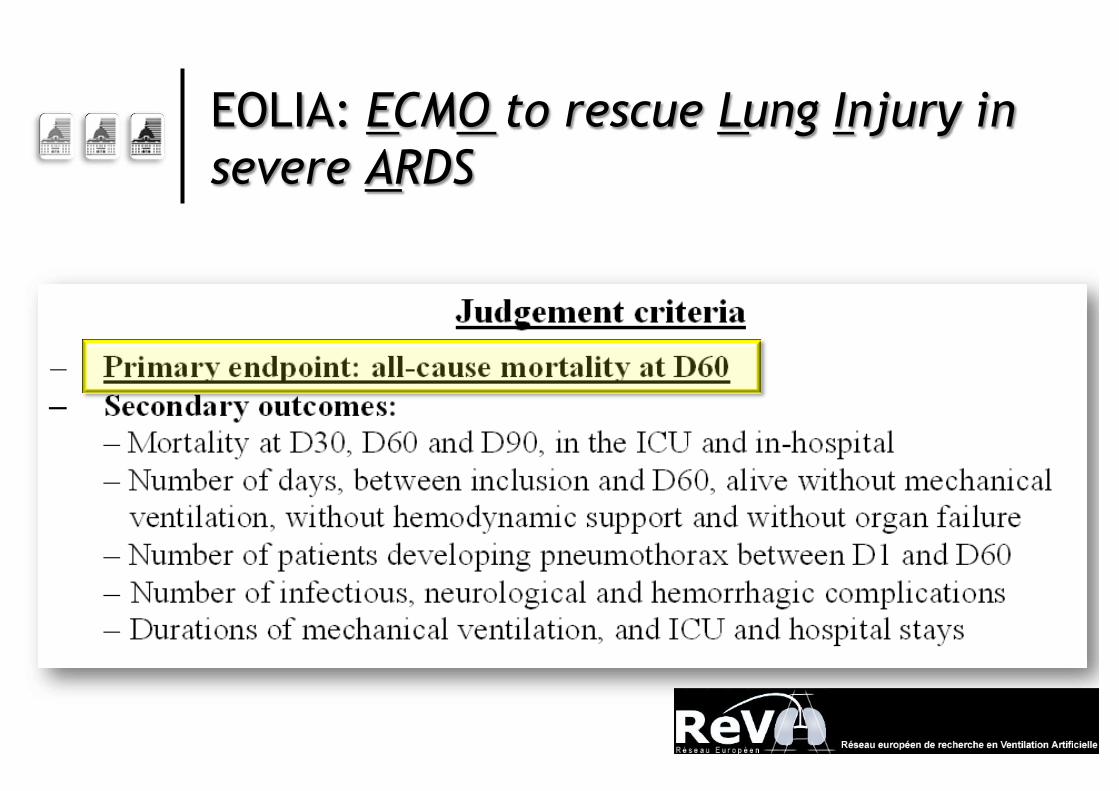
EOLIA: ECMO to rescue Lung Injury in severe ARDS
We need EOLIA… A new trial of ECMO for severe pneumonia/ARDS
153 patients randomized so far…
YES WE CAN
YES WE CAN




![COVID19 ARDS (CARDS) · 2020. 11. 7. · ARDS, requiring positive pressure oxygen therapy and intensive care therapy [18] in 17–19.6% of symptomatic patients. Age more commonly](https://img.pdfslide.net/doc/110x75/60ad87ed240c1a4ebc4fd16d/covid19-ards-cards-2020-11-7-ards-requiring-positive-pressure-oxygen-therapy.jpg)

![Impact of statin therapy on mortality in patients with sepsis ......respiratory distress syndrome (ARDS), mortality among patients with sepsis-associated ARDS remains high [1]. The](https://img.pdfslide.net/doc/110x75/60a4c7629b40e8516b28d227/impact-of-statin-therapy-on-mortality-in-patients-with-sepsis-respiratory.jpg)






















