Embed Size (px)
Citation preview
ReceiveFrom th
of MediciAddress
Place, New
© Americ
AJNR Am J Neuroradiol 19:1849–1851, November 1998
Extranodal Non-Hodgkin Lymphoma Involving theMuscles of Mastication
June Chong, Peter M. Som, Adam R. Silvers, and Jack F. Dalton
Summary: Involvement of the skeletal muscle by non-Hodgkin lymphoma (NHL) is unusual. The most commonlyaffected muscles are those of the extremities, pelvis, andgluteal regions; rarely are the muscles in the head and neckinvolved. We report the clinical, CT, and MR imagingfindings in two patients with extranodal NHL in the headand neck region involving the muscles of mastication. Onepatient was immunocompetent and had lymphoma thatarose within the muscles; the other was a patient with AIDSwho had disseminated disease at diagnosis. In both pa-tients, the involved muscles were isodense with normalmuscles on CT scans. On MR images, the infiltrated mus-cles were isointense with normal muscles on the T1-weighted sequence and hyperintense on the fast spin-echoT2-weighted sequence, with variable enhancement after ad-ministration of intravenous contrast material.
Extranodal manifestations of lymphoma are wellrecognized and occur in 20% to 30% of patients (1).Skeletal muscle involvement is uncommon. The mostoften affected are the gluteal and pelvic muscles,occurring as a result of metastatic hematogenous orlymphatic spread, or contiguous spread from adjacentinvolved lymph nodes or bone; involvement from pri-mary disease is least common (2). Only three cases ofextranodal non-Hodgkin lymphoma (NHL) that ap-peared to arise from the muscles of mastication in thenon-AIDS patient have been reported (3–5).
We present the clinical, CT, and MR imaging find-ings in two cases of biopsy-proved extranodal NHL inthe head and neck region involving predominantly themuscles of mastication. One patient was immunocom-petent when diagnosed and the other had AIDS withdisseminated disease.
Case Reports
Case 1A 52-year-old woman presented with a painless, slowly growing
mass in the right cheek, which she first noticed a year earlier. Shewas otherwise healthy, with no significant medical history. Clinicalexamination revealed a painless fullness in the right cheek region.Intraoral examination showed a right submucosal tonsillar and
d October 27, 1997; accepted after revision February 11, 19e Departments of Radiology (J.C., P.M.S., A.R.S.), Otolaryng
ne, City University of New York, NY.reprint requests to Peter M. Som, MD, Department of RadYork, NY 10029.
an Society of Neuroradiology
184
buccal mass that extended to the level of the third molar tooth onthe right. There was no palpable lymphadenopathy.
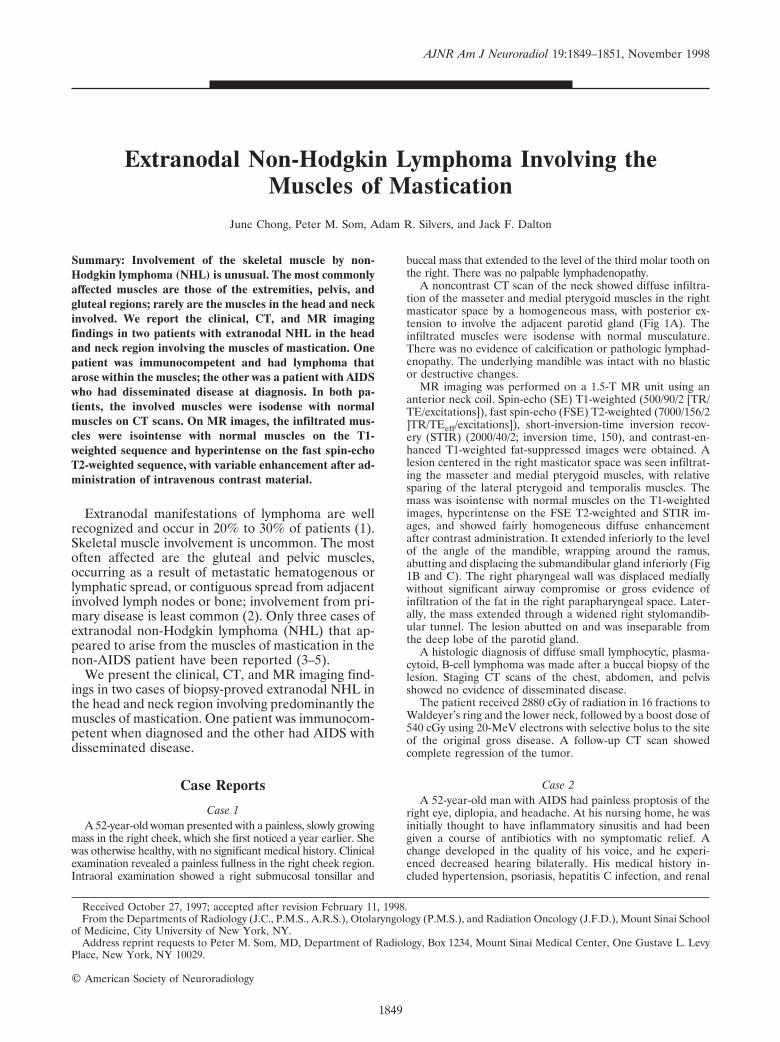
A noncontrast CT scan of the neck showed diffuse infiltra-tion of the masseter and medial pterygoid muscles in the rightmasticator space by a homogeneous mass, with posterior ex-tension to involve the adjacent parotid gland (Fig 1A). Theinfiltrated muscles were isodense with normal musculature.There was no evidence of calcification or pathologic lymphad-enopathy. The underlying mandible was intact with no blasticor destructive changes.
MR imaging was performed on a 1.5-T MR unit using ananterior neck coil. Spin-echo (SE) T1-weighted (500/90/2 [TR/TE/excitations]), fast spin-echo (FSE) T2-weighted (7000/156/2]TR/TEeff/excitations]), short-inversion-time inversion recov-ery (STIR) (2000/40/2; inversion time, 150), and contrast-en-hanced T1-weighted fat-suppressed images were obtained. Alesion centered in the right masticator space was seen infiltrat-ing the masseter and medial pterygoid muscles, with relativesparing of the lateral pterygoid and temporalis muscles. Themass was isointense with normal muscles on the T1-weightedimages, hyperintense on the FSE T2-weighted and STIR im-ages, and showed fairly homogeneous diffuse enhancementafter contrast administration. It extended inferiorly to the levelof the angle of the mandible, wrapping around the ramus,abutting and displacing the submandibular gland inferiorly (Fig1B and C). The right pharyngeal wall was displaced mediallywithout significant airway compromise or gross evidence ofinfiltration of the fat in the right parapharyngeal space. Later-ally, the mass extended through a widened right stylomandib-ular tunnel. The lesion abutted on and was inseparable fromthe deep lobe of the parotid gland.
A histologic diagnosis of diffuse small lymphocytic, plasma-cytoid, B-cell lymphoma was made after a buccal biopsy of thelesion. Staging CT scans of the chest, abdomen, and pelvisshowed no evidence of disseminated disease.
The patient received 2880 cGy of radiation in 16 fractions toWaldeyer’s ring and the lower neck, followed by a boost dose of540 cGy using 20-MeV electrons with selective bolus to the siteof the original gross disease. A follow-up CT scan showedcomplete regression of the tumor.
Case 2A 52-year-old man with AIDS had painless proptosis of the
right eye, diplopia, and headache. At his nursing home, he wasinitially thought to have inflammatory sinusitis and had beengiven a course of antibiotics with no symptomatic relief. Achange developed in the quality of his voice, and he experi-enced decreased hearing bilaterally. His medical history in-cluded hypertension, psoriasis, hepatitis C infection, and renal
98.ology (P.M.S.), and Radiation Oncology (J.F.D.), Mount Sinai School
iology, Box 1234, Mount Sinai Medical Center, One Gustave L. Levy
9
1850 CHONG AJNR: 19, November 1998
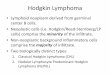
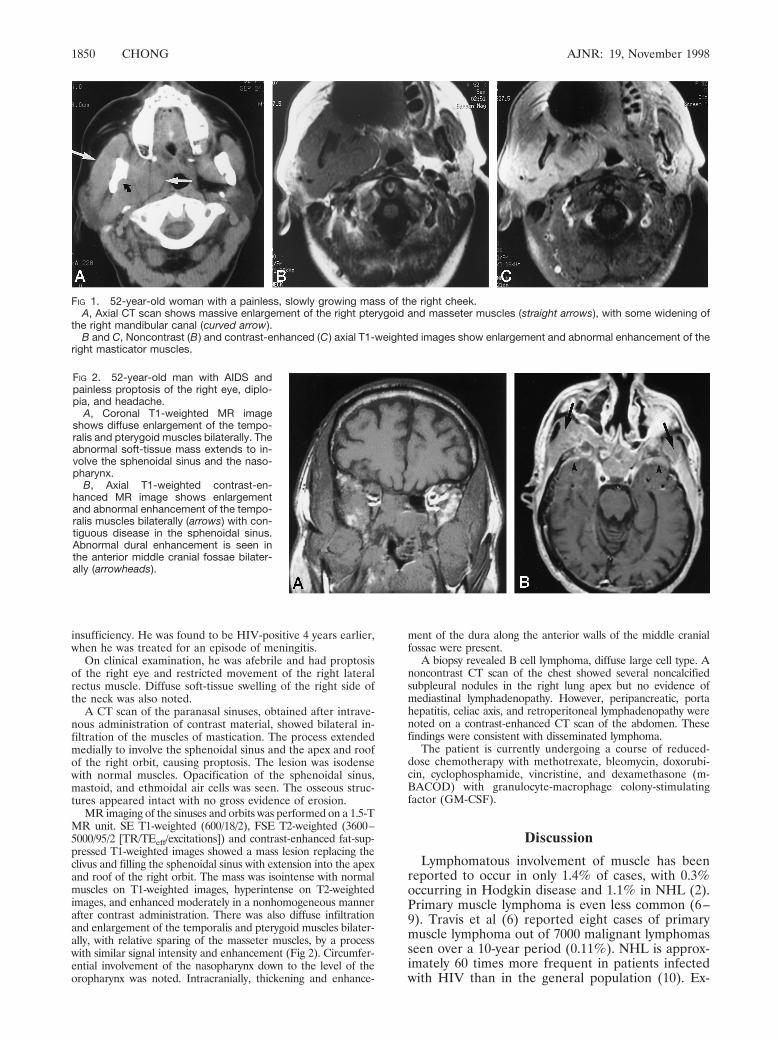
FIG 2. 52-year-old man with AIDS andpainless proptosis of the right eye, diplo-pia, and headache.
A, Coronal T1-weighted MR imageshows diffuse enlargement of the tempo-ralis and pterygoid muscles bilaterally. Theabnormal soft-tissue mass extends to in-volve the sphenoidal sinus and the naso-pharynx.
B, Axial T1-weighted contrast-en-hanced MR image shows enlargementand abnormal enhancement of the tempo-ralis muscles bilaterally (arrows) with con-tiguous disease in the sphenoidal sinus.Abnormal dural enhancement is seen inthe anterior middle cranial fossae bilater-ally (arrowheads).
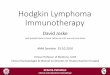
FIG 1. 52-year-old woman with a painless, slowly growing mass of the right cheek.A, Axial CT scan shows massive enlargement of the right pterygoid and masseter muscles (straight arrows), with some widening of
the right mandibular canal (curved arrow).B and C, Noncontrast (B ) and contrast-enhanced (C ) axial T1-weighted images show enlargement and abnormal enhancement of the
right masticator muscles.
insufficiency. He was found to be HIV-positive 4 years earlier,when he was treated for an episode of meningitis.
On clinical examination, he was afebrile and had proptosisof the right eye and restricted movement of the right lateralrectus muscle. Diffuse soft-tissue swelling of the right side ofthe neck was also noted.
A CT scan of the paranasal sinuses, obtained after intrave-nous administration of contrast material, showed bilateral in-filtration of the muscles of mastication. The process extendedmedially to involve the sphenoidal sinus and the apex and roofof the right orbit, causing proptosis. The lesion was isodensewith normal muscles. Opacification of the sphenoidal sinus,mastoid, and ethmoidal air cells was seen. The osseous struc-tures appeared intact with no gross evidence of erosion.
MR imaging of the sinuses and orbits was performed on a 1.5-TMR unit. SE T1-weighted (600/18/2), FSE T2-weighted (3600–5000/95/2 [TR/TEeff/excitations]) and contrast-enhanced fat-sup-pressed T1-weighted images showed a mass lesion replacing theclivus and filling the sphenoidal sinus with extension into the apexand roof of the right orbit. The mass was isointense with normalmuscles on T1-weighted images, hyperintense on T2-weightedimages, and enhanced moderately in a nonhomogeneous mannerafter contrast administration. There was also diffuse infiltrationand enlargement of the temporalis and pterygoid muscles bilater-ally, with relative sparing of the masseter muscles, by a processwith similar signal intensity and enhancement (Fig 2). Circumfer-ential involvement of the nasopharynx down to the level of theoropharynx was noted. Intracranially, thickening and enhance-
ment of the dura along the anterior walls of the middle cranialfossae were present.
A biopsy revealed B cell lymphoma, diffuse large cell type. Anoncontrast CT scan of the chest showed several noncalcifiedsubpleural nodules in the right lung apex but no evidence ofmediastinal lymphadenopathy. However, peripancreatic, portahepatitis, celiac axis, and retroperitoneal lymphadenopathy werenoted on a contrast-enhanced CT scan of the abdomen. Thesefindings were consistent with disseminated lymphoma.
The patient is currently undergoing a course of reduced-dose chemotherapy with methotrexate, bleomycin, doxorubi-cin, cyclophosphamide, vincristine, and dexamethasone (m-BACOD) with granulocyte-macrophage colony-stimulatingfactor (GM-CSF).
Discussion
Lymphomatous involvement of muscle has beenreported to occur in only 1.4% of cases, with 0.3%occurring in Hodgkin disease and 1.1% in NHL (2).Primary muscle lymphoma is even less common (6–9). Travis et al (6) reported eight cases of primarymuscle lymphoma out of 7000 malignant lymphomasseen over a 10-year period (0.11%). NHL is approx-imately 60 times more frequent in patients infectedwith HIV than in the general population (10). Ex-

AJNR: 19, November 1998 NON-HODGKIN LYMPHOMA 1851
tranodal presentation occurs in about 55% of AIDS-related NHL, with lymphomatous involvement of themuscle seen in 8.8%, of which 80% of cases developprimarily in the muscle (11), most commonly in theiliopsoas, paraspinal, pelvic, and extremity muscles.
Extranodal NHL arising from muscles of mastica-tion in the head and neck region has been reported inonly three cases. Harnsberger et al (3) described theCT findings in two patients who had extranodal NHLinvolving the muscles of mastication, but the diseaseappeared to be localized to the muscles in only one ofthe two cases. Set et al (4) described a 6-year-oldnon-AIDS patient with primary NHL of the acutelymphoblastic type involving the pterygomassetericmuscle complex unilaterally. Ceysens et al (5) alsodescribed a patient with extranodal NHL primarilyinvolving the masseter muscle. In all these cases, onlythe CT findings were reported, as no MR imaging wasperformed.
In our case 1, the affected muscles were isodensewith normal muscles on unenhanced CT scans, simi-lar to the CT characteristics seen in the patient re-ported by Harnsberger et al (3). In the case describedby Set et al (4), the involved muscles were hypodenserelative to normal muscles, probably because theirpatient received intravenous contrast materialwhereas our patient did not.
At MR imaging, NHL involving skeletal muscle hasbeen described as hyperintense or isointense relativeto normal muscle on the T1-weighted sequence andhyperintense on the T2-weighted sequence (12–14).In both our patients, the signal intensity of the lym-phomatous muscle was isointense with normal muscleon T1-weighted images and hyperintense on FSET2-weighted images, similar to the signal characteris-tics of muscle NHL outside the head and neck region.
The patient described by Set et al (4), with primarymuscle lymphoma (acute lymphoblastic type), re-sponded well to chemotherapy. Our patient in case 1,with presumed primary muscle lymphoma (diffusesmall lymphocytic B cell) extending to the adjacentparotid gland, received only local radiotherapy, andhad an excellent response, with complete regressionof the tumor.
The imaging characteristics of muscle NHL on CTand MR studies are nonspecific and can be seen in avariety of diseases. In the AIDS population, the dif-ferential diagnosis of multifocal bilateral masses in-volving masticator muscles includes bacterial myosi-tis, idiopathic polymyositis, Kaposi’s sarcoma, andrarely, metastases, all of which may have prolongedT2 relaxation times. It is particularly important toexclude bacterial myositis clinically as well as withtissue biopsy and culture. This entity is usually causedby Staphylococcus aureus and is potentially curablebut can be fatal if not treated immediately (15, 16).Pathologically, lymphoma can be confused with othersmall-cell malignancies, such as metastatic oat cell
carcinoma, neuroblastoma, plasmacytoma, and rhab-domyosarcoma.
ConclusionAwareness of NHL as a differential diagnosis in
patients with and without AIDS, who present withunilateral or bilateral muscle enlargement in the headand neck region, allows appropriate handling of thetissue at biopsy. Special techniques, like electron mi-croscopy and immunohistochemical cell marker stud-ies, can then be used to differentiate these lesions,thus ensuring proper diagnosis and optimizing patientmanagement (17–19).
References1. Freeman C, Berg JW, Cutler SJ. Occurrence and prognosis of
extranodal lymphomas. Cancer 1972;29:252–2602. Komatsuda M, Nagao T, Arimori S. An autopsy case of malignant
lymphoma associated with remarkable infiltration in skeletal mus-cles. Rinsho Ketsueki 1981;22:891–895
3. Harnsberger RH, Bragg DG, Osborn AG, et al. Non-Hodgkin’slymphoma of the head and neck: CT evaluation of nodal andextranodal sites. AJR Am J Roentgenol 1987;149:785–791
4. Set PAK, Somers JM, Britton PD, Freer CEL. Pictorial review:benign and malignant enlargement of the pterygo-masseteric mus-cle complex. Clin Radiol 1993;48:57–60
5. Ceysens C, Horvath M, Termote JL, Lemahieu SF. Extranodalnon-Hodgkin lymphoma of the head and neck presenting as amandibular swelling: report of two cases. J Belge Radiol 1992;75:37–39
6. Travis WD, Banks PM, Reiman HM. Primary extranodal softtissue lymphoma of the extremities. Am J Pathol 1987;11:359–366
7. Beggs I. Primary muscle lymphoma. Clin Radiol 1997;52:203–2128. Eustace S, Winalski CS, McGowen A, Lan H, Dorfman D. Skeletal
muscle lymphoma: observations at MR imaging. Skeletal Radiol1996;25:425–430
9. Lee VS, Martinez S, Coleman RE. Primary muscle lymphoma:clinical and imaging findings. Radiology 1997;203:237–244
10. Beral V, Peterman T, Berkelman R, Jaffe H. AIDS-associatednon-Hodgkin lymphoma. Lancet 1991;337:806–809
11. Raphael M, Gentilhomme O, Tulliez M, Byron PA, Diebold J, theFrench Study Group of Pathology for Human ImmunodeficiencyVirus-associated Tumors. Histologic features of high grade non-Hodgkin’s lymphoma in immunodeficiency syndrome. Arch PatholLab Med 1991;115:15–20
12. Hosono M, Kobayashi H, Kotoura Y, Tsuboyama T, Tsutsui K,Konishi J. Involvement of muscle by malignant lymphoma: MR andCT appearances. J Comput Assist Tomogr 1995;19:455–459
13. Negendank WG, Al-Katib AM, Karanes C, Smith MR. Lympho-mas: MR imaging contrast characteristics with clinical-pathologiccorrelations. Radiology 1990;177:209–216
14. Metzler JP, Fleckenstein JL, Vuitch F, Frenkel EP. Skeletal musclelymphoma: MRI evaluation. Magn Reson Imaging 1992;10:491–494
15. Steinbach LS, Tehranzadeh J, Fleckenstein JL, Vanarthos WJ, PaisMJ. Human immunodeficiency virus infection: musculoskeletalmanifestations. Radiology 1993;186:833–838
16. Fleckenstein JL, Burns DK, Murphy FK, Jayson HT, Bonte FJ.Differential diagnosis of bacterial myositis in AIDS: evaluationwith MR imaging. Radiology 1991;179:653–658
17. Kandel RA, Bedard YC, Pritzker PH, Luk SC. Lymphoma present-ing as an intramuscular small cell malignant tumor. Cancer 1984;53:1586–1589
18. Pizzolo G, Sloane J, Beverly P, et al. Differential diagnosis ofmalignant lymphoma and nonlymphoid tumors using monoclonalantileukocyte antibody. Cancer 1980;46:2640–2647
19. Berg AR, Linder J, Anderson RW, Tempero MA, Edney JA,Armitage JO. The undifferentiated malignant neoplasm. JAMA1985;254:2625–2626
Please see the Editorial on page 1808 in this issue.