Embed Size (px)
Citation preview

8/14/2019 Eyes Disorder
http://slidepdf.com/reader/full/eyes-disorder 1/14
Retinitis Pigmentosa
Retinitis pigmentosa (RP) is a group of
genetic eye conditions. In the progression of symptoms for RP, night blindness generally precedestunnel vision by years or even decades. Many people
with RP do not become legally blind until their 40s or
50s and retain some sight all their life. Others go
completely blind from RP, in some cases as early as
childhood. Progression of RP is different in each case.
RP is a type of hereditary retinal dystrophy, a group of
inherited disorders in which abnormalities of the
photoreceptors (rods and cones) or the retinal pigment
epithelium (RPE) of the retina lead to progressivevisual loss. Affected individuals first experiencedefective dark adaptation or nyctalopia (night
blindness), followed by reduction of the peripheral
visual field (known as tunnel vision) and, sometimes,
loss of central vision late in the course of the disease.
Signs
Mottling of the retinal pigment epithelium with black
bone-spicule pigmentation is typically indicative (or
pathognomonic) of retinitis pigmentosa. Other ocular
features include waxy pallor of the optic nerve head,
attenuation (thinning) of the retinal vessels, cellophane
maculopathy, cystic macular edema and posterior
subcapsular cataract.
Diagnosis
The diagnosis of retinitis pigmentosa relies upon documentation of progressive loss in photoreceptor function by electroretinography (ERG) and visual field testing. The mode
of inheritance of RP is determined by family history. At least 35 different genes or loci are known to cause "nonsyndromic RP" (RP that is not the result of another disease or
part of a wider syndrome).
Treatment
There is currently no medical treatment that can completely cure retinitis
pigmentosa, although the progression of the disease can be reduced by the daily intake of
15000 IU of vitamin A palmitate.[12]
Recent studies have shown that proper vitamin A supplementation can postpone blindness by up to 10 years. Scientists continue to
investigate possible treatments. Future treatments may involve retinal transplants,
artificial retinal implants, gene therapy, stem cells, nutritional supplements, and/or drug
therapies.
Scientists at the Osaka Bioscience Institute have identified a protein, named Pikachurin,
which they believe could lead to a treatment for retinitis pigmentosa.[15][16]
Normal vision. Courtesy NIH National
Eye Institute
The same view with tunnel vision fromretinitis pigmentosa. The blackness
surrounding the central image does not
indicate darkness, but rather a lack of
perceived visual information.

8/14/2019 Eyes Disorder
http://slidepdf.com/reader/full/eyes-disorder 2/14
AmblyopiaAmblyopia, otherwise known as lazy eye,[1] is a disorder of the visual system that is
characterized by poor or indistinct vision in an eye that is otherwise physically normal, or out of proportion to associated structural abnormalities. It has been estimated to affect 1–
5% of the population.[2]
The problem is caused by either no transmission or poor transmission of the visual imageto the brain for a sustained period of dysfunction or during early childhood. Amblyopia
normally only affects one eye, but it is possible to be amblyopic in both eyes if both are
similarly deprived of a good, clear visual image. Detecting the condition in early
childhood increases the chance of successful treatment.
While the colloquialism "lazy eye" is frequently used to refer to amblyopia, the term is
inaccurate because there is no "laziness" of either the eye or the amblyope involved in the
condition. This term is imprecise because "lazy eye" is also a layman's term for
strabismus, particularly exotropia
Symptoms
Many people with amblyopia, especially those who are only mildly so, are not even
aware they have the condition until tested at older ages, since the vision in their stronger
eye is normal. However, people who have severe amblyopia may experience associated
visual disorders, most notably poor depth perception. Amblyopes may suffer from poor spatial acuity, low sensitivity to contrast and some "higher-level" deficits to vision such
as reduced sensitivity to motion.[5] These deficits are usually specific to the amblyopic
eye. Amblyopes also suffer from problems of binocular vision such as limited
stereoscopic depth perception and usually have difficulty seeing the three-dimensional
images in hidden stereoscopic displays such as autostereograms.[6] However perception of
depth from monocular cues such as size, perspective, and motion parallax is normal.
Types
Amblyopia can be caused by deprivation of vision earlyin life by vision-obstructing disorders such as
congenital cataracts, by strabismus (misaligned eyes),
or by anisometropia (different degrees of myopia or
hyperopia in each eye). Ambylopia can also occur
physiologically after tobacco or alcohol consumption.
Strabismic amblyopia
Strabismus, sometimes erroneously also called
lazy eye, is a condition in which the eyes aremisaligned. Strabismus usually results in normal vision
in the preferred sighting (or "fellow") eye, but may
cause abnormal vision in the deviating or strabismiceye due to the discrepancy between the images
projecting to the brain from the two eyes.[7] Adult-onset
strabismus usually causes double vision (diplopia),
since the two eyes are not fixated on the same object.
Children's brains, however, are more neuroplastic, and therefore can more easily adapt by
suppressing images from one of the eyes, eliminating the double vision. This plastic
response of the brain, however, interrupts the brain's normal development, resulting in theamblyopia. Strabismic amblyopia is treated by clarifying the visual image with glasses,
A child wearing an adhesive
eyepatch to correct amblyopia

8/14/2019 Eyes Disorder
http://slidepdf.com/reader/full/eyes-disorder 3/14
and/or encouraging use of the amblyopic eye with an eyepatch over the dominant eye or
pharmacologic penalization of it. Penalization usually consists of applying atropine drops
to temporarily dilate the pupil, which leads to blurring of vision in the good eye. This
helps to prevent the bullying and teasing associated with wearing a patch, although
application of the eyedrops is more challenging. The ocular alignment itself may be
treated with surgical or non-surgical methods, depending on the type and severity of thestrabismus.[8]
Refractive or anisometropic amblyopia
Refractive amblyopia may result from anisometropia (unequal refractive error
between the two eyes). Anisometropia exists when there is a difference in the refraction between the two eyes. The eye which provides the brain with a clearer image (closer to
20/20) typically becomes the dominant eye. The image in the other eye is blurred, which
results in abnormal development of one half of the visual system. Refractive amblyopia is
usually less severe than strabismic amblyopia and is commonly missed by primary care
physicians because of its less dramatic appearance and lack of obvious physical
manifestation, such as with strabismus.[9] Frequently, amblyopia is associated with acombination of anisometropia and strabismus.
Pure refractive amblyopia is treated by correcting the refractive error early with
prescription lenses and patching or penalizing the good eye.
Meridional amblyopia is a mild condition in which lines are seen less clearly at someorientations than others after full refractive correction. An individual who had an
astigmatism at a young age that was not corrected by glasses will later have astigmatismthat cannot be optically corrected
Form-deprivation and occlusion amblyopia
Form-deprivation amblyopia ( Amblyopia exanopsia) results when the ocular media become
opaque, such as is the case with cataracts or corneal
scarring from forceps injuries during birth.[10] These
opacities prevent adequate visual input from
reaching the eye, and therefore disrupt development.If not treated in a timely fashion, amblyopia may
persist even after the cause of the opacity is
removed. Sometimes, drooping of the eyelid ( ptosis)
or some other problem causes the upper eyelid to
physically occlude a child's vision, which may cause
amblyopia quickly. Occlusion amblyopia may be a
complication of a hemangioma that blocks some or all of the eye.
Treatments
Treatment of strabismic or anisometropic amblyopia consists of correcting the
optical deficit and forcing use of the amblyopic eye, either by patching the good eye, or
by instilling topical atropine in the eye with better vision. One should also be wary of
over-patching or over-penalizing the good eye when treating for amblyopia, as this can
create so-called "reverse amblyopia" in the other eye.[8][11]
Form deprivation amblyopia is treated by removing the opacity as soon as possible
followed by patching or penalizing the good eye to encourage use of the amblyopic eye.[
A man with minor amblyopia

8/14/2019 Eyes Disorder
http://slidepdf.com/reader/full/eyes-disorder 4/14
Macular Degeneration
Macular degeneration is a medical condition usually of older adults which results in a
loss of vision in the center of the visual field (the macula) because of damage to the
retina. It occurs in “dry” and “wet” forms. It is a major cause of blindness in the elderly(>50 years)[citation needed
]. Macular degeneration can make it difficult or impossible to read or
recognize faces, although enough peripheral vision remains to allow other activities of
daily life.
The inner layer of the eye is the retina, which contains nerves that communicate sight,
and behind the retina is the choroid, which contains the blood supply to the retina. In the
dry (nonexudative) form, cellular debris called drusen accumulate between the retina andthe choroid, and the retina can become detached. In the wet (exudative) form, which is
more severe, blood vessels grow up from the choroid behind the retina, and the retina can
also become detached. It can be treated with laser coagulation, and with medication that
stops and sometimes reverses the growth of blood vessels.[1][2]
Although some macular dystrophies affecting younger individuals are sometimes referred
to as macular degeneration, the term generally refers to age-related macular
degeneration).
Normal vision (B&W). Courtesy The same view with age-related
NIH National Eye Institute macular degeneration (B&W).
Risk factors
• Aging: Approximately 10% of patients 66 to 74 years of age will have findings of
macular degeneration. The prevalence increases to 30% in patients 75 to 85 years
of age.[4]
• Family history: The lifetime risk of developing late-stage macular degeneration is
50% for people who have a relative with macular degeneration, versus 12% for people who do not have relatives with macular degeneration, a fourfold higher
risk.[
• Macular degeneration gene: The genes for the complement system proteins
factor H (CFH) and factor B (CFB) and factor 3 (C3) have been determined to be
strongly associated with a person's risk for developing macular degeneration. CFH
is involved in inhibiting the inflammatory response mediated via C3b (and theAlternative Pathway of complement) both by acting as a cofactor for cleavage of
C3b to its inactive form, C3bi, and by weakening the activecomplex that forms
between C3b and factor B. C-reactive protein and polyanionic surface markers
such as glycosaminoglycans normally enhance the ability of factor H to inhibit
complement
• Mutation of the ATP synthase gene: Retinitis Pigmentosa (RP) is a geneticallylinked dysfunction of the retina and is related to mutation of the Adenosine Tri-
Phosphate (ATP) Synthase Gene 615.1617
• Hypertension: Also known as high blood pressure.

8/14/2019 Eyes Disorder
http://slidepdf.com/reader/full/eyes-disorder 5/14
• Cardiovascular status — high cholesterol, obesity. Race Macular degeneration is
more likely to be found in Caucasians than in people of African descent.[13][14]
• Exposure to sunlight especially blue light. There is conflicting evidence as to
whether exposure to sunlight contributes to the development of macular
degeneration
Signs
• Drusen
• Pigmentary alterations
• Exudative changes: hemorrhages in the eye, hard exudates, subretinal/sub-
RPE/intraretinal fluid
• Atrophy: incipient and geographic
• Visual acuity drastically decreasing ((two levels or more) ex: 20/20 to 20/80)
Symptoms
• Blurred vision: Those with nonexudative macular degeneration may be
asymptomatic or notice a gradual loss of central vision, whereas those with
exudative macular degeneration often notice a rapid onset of vision loss.
• Central scotomas (shadows or missing areas of vision)
• Distorted vision (i.e. metamorphopsia) - A grid of straight lines appears wavy and
parts of the grid may appear blank. Patients often first notice this when looking atmini-blinds in their home.
• Trouble discerning colors; specifically dark ones from dark ones and light ones
from light ones.
• Slow recovery of visual function after exposure to bright light
• A loss in contrast sensitivity.
Diagnosis
Fluorescein angiography allows for the identification and localization of abnormal
vascular processes. Optical coherence tomography is now used by most ophthalmologists
in the diagnosis and the followup evaluation of the response to treatment by using either Avastin or Lucentis which are injected into the vitreous of the eye at various intervals.
Prevention
The Age-Related Eye Disease Study showed that a combination of high-dose beta-
carotene, vitamin C, vitamin E, and zinc can reduce the risk of progressing from early to
advanced AMD by about 25 percent.[21] A followup study, Age-Related Eye Disease
Study 2, to study the potential benefits of lutein, zeaxanthine, and fish oil, is underway.[22]
Studies are underway at Harvard, with the goal of reducing lipofuscin accumulation. [12]
In 2007, a study at the National Eye Institute, Maryland found that Lutein and zeaxanthin
(nutrients in eggs and green vegetables) protect against macular degeneration. [23]
Studies found that antioxidants disrupt the link of two processes that cause macular
degeneration and extend the lifetime of irreplaceable photoreceptors and other retinal
cells

8/14/2019 Eyes Disorder
http://slidepdf.com/reader/full/eyes-disorder 6/14
CataractA cataract is a clouding that develops in the crystalline lens
of the eye or in its envelope, varying in degree from slight tocomplete opacity and obstructing the passage of light. Early
in the development of age-related cataract the power of the
lens may be increased, causing near-sightedness (myopia),
and the gradual yellowing and opacification of the lens may
reduce the perception of blue colours. Cataracts typically
progress slowly to cause vision loss and are potentially
blinding if untreated. The condition usually affects both the
eyes, but almost always one eye is affected earlier than the
other.[1]
A senile cataract, occurring in the aged, is characterized by an initial opacity in the lens,
subsequent swelling of the lens and final shrinkage with complete loss of transparency.[2]
Moreover, with time the cataract cortex liquefies to form a milky white fluid in a
Morgagnian cataract, which can cause severe inflammation if the lens capsule ruptures
and leaks. Untreated, the cataract can cause phacomorphic glaucoma. Very advanced
cataracts with weak zonules are liable to dislocation anteriorly or posteriorly. Such
spontaneous posterior dislocations (akin to the historical surgical procedure of couching)
in ancient times were regarded as a blessing from the heavens, because some perceptionof light was restored in the cataractous patients.
Cataract derives from the Latin cataracta meaning "waterfall" and the Greek kataraktes
and katarrhaktes, from katarassein meaning "to dash down" (kata-, "down"; arassein, "to
strike, dash"[3]). As rapidly running water turns white, the term may later have been usedmetaphorically to describe the similar appearance of mature ocular opacities. In Latin,
cataracta had the alternate meaning " portcullis",[4] so it is also possible that the name
came about through the sense of "obstruction". Early Persian physicians called the term
nazul-i-ah, or 'descent of the water' - vulgarised into waterfall disease or cataract -
believing such blindness to be caused by an outpouring of corrupt humour into the eye.[5]
In dialect English a cataract is called a pearl , as in "pearl eye" and "pearl-eyed"
Causes
Cataracts develop from a variety of reasons, including long-term exposure to ultraviolet
light, exposure to radiation, secondary effects of diseases such as diabetes, hypertensionand advanced age, or trauma (possibly much earlier); they are usually a result of
denaturation of lens protein. Genetic factors are often a cause of congenital cataracts and
positive family history may also play a role in predisposing someone to cataracts at an
earlier age, a phenomenon of "anticipation" in pre-senile cataracts. Cataracts may also be
produced by eye injury or physical trauma. A study among Icelandair pilots showed
commercial airline pilots are three times more likely to develop cataracts than peoplewith non-flying jobs. This is thought to be caused by excessive exposure to radiation
coming from outer space.[7] Cataracts are also unusually common in persons exposed to
infrared radiation, such as glassblowers who suffer from "exfoliation syndrome".
Exposure to microwave radiation can cause cataracts. Atopic or allergic conditions are
also known to quicken the progression of cataracts, especially in children.[8]
Cataracts may be partial or complete, stationary or progressive, hard or soft.
Some drugs can induce cataract development, such as corticosteroids[9] and Ezetimibeand
Seroquel.
8/14/2019 Eyes Disorder
http://slidepdf.com/reader/full/eyes-disorder 7/14
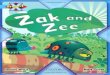
There are various types of cataracts, e.g. nuclear, cortical, mature, and hypermature.
Cataracts are also classified by their location, e.g. posterior (classically due to steroid use)
and anterior (common (senile) cataract related to aging).
SymptomsAs a cataract becomes more opaque, clear vision is compromised. A loss of visual acuity
is noted. Contrast sensitivity is also lost, so that contours, shadows and color vision are
less vivid. Veiling glare can be a problem as light is scattered by the cataract into the eye.
A contrast sensitivity test should be performed and if a loss in contrast sensitivity is
demonstrated an eye specialist consultation is recommended.
In the developed world, particularly in high-risk groups such as diabetics, it may be
advisable to seek medical opinion if a 'halo' is observed around street lights at night,
especially if this phenomenon appears to be confined to one eye only.
Epidemiology
Age-related cataract is responsible for 48% of world blindness, which represents about 18
million people, according to the World Health Organization (WHO).[11] In many countries
surgical services are inadequate, and cataracts remain the leading cause of blindness. As
populations age, the number of people with cataracts is growing. Cataracts are also animportant cause of low vision in both developed and developing countries. Even where
surgical services are available, low vision associated with cataracts may still be prevalent,
as a result of long waits for operations and barriers to surgical uptake, such as cost, lack of information and transportation problems.
In the United States, age-related lenticular changes have been reported in 42% of those
between the ages of 52 to 64, [12] 60% of those between the ages 65 and 74,[13] and 91% of
those between the ages of 75 and 85

8/14/2019 Eyes Disorder
http://slidepdf.com/reader/full/eyes-disorder 8/14
ConjunctivitisConjunctivitis (commonly called "pink eye" or "Madras
eye"[1]) is an inflammation of the conjunctiva (the outermostlayer of the eye and the inner surface of the eyelids), most
commonly due to an allergic reaction or an infection (usually
viral, but sometimes bacterial
Symptoms
Redness (Hyperaemia), irritation (Chemosis) and watering(Epiphora) of the eyes are symptoms common to all forms of
conjunctivitis.
Acute allergic conjunctivitis is typically itchy,
sometimes distressingly so, and often involves some lid
swelling. Chronic allergy often causes just itch or
irritation.
Viral conjunctivitis is often associated with an
infection of the upper respiratory tract, a common cold,
and/or a sore throat. Its symptoms include watery discharge and variable itch. The
infection usually begins with one eye, but may spread easily to the other.
Bacterial conjunctivitis due to the common pyogenic (pus-producing) bacteria causes
marked grittiness/irritation and a stringy, opaque, grey or yellowish mucopurulent
discharge ( gowl , goop, "gunk", "eye crust", or other regional names, officially known as
'gound') that may cause the lids to stick together (matting ), especially after sleeping.Another symptom that could be caused by bacterial conjunctivitis is severe crusting of
the infected eye and the surrounding skin. However discharge is not essential to the
diagnosis, contrary to popular belief. Bacteria such as Chlamydia trachomatis or
Moraxella can cause a non-exudative but persistent conjunctivitis without much redness.
The gritty and/or scratchy feeling is sometimes localised enough for patients to insist they
must have a foreign body in the eye. The more acute pyogenic infections can be painful.Like viral conjunctivitis, it usually affects only one eye but may spread easily to the other
eye. However, it is dormant in the eye for three days before the patient shows signs of
symptoms.
Irritant or toxic conjunctivitis is irritable or painful when the infected eye is pointed far
down or far up. Discharge and itch are usually absent. This is the only group in which
severe pain may occur.
Inclusion conjunctivitis of the newborn (ICN) is a conjunctivitis that may be caused by
the bacteria Chlamydia trachomatis, and may lead to acute, purulent conjunctivitis.[4]
However, it is usually self-healing.[4]
An eye with viral conjunctivitis.
Eyes with conjunctivitis

8/14/2019 Eyes Disorder
http://slidepdf.com/reader/full/eyes-disorder 9/14
Signs
Injection (redness) of the conjunctiva on one or both eyes should be apparent, but may be
quite mild. Except in obvious pyogenic or
toxic/chemical conjunctivitis, a slit lamp (biomicroscope) is needed to have any
confidence in the diagnosis. Examination of the
tarsal conjunctiva is usually more diagnostic
than the bulbar conjunctiva.
Allergic conjunctivitis shows pale watery
swelling or edema of the conjunctiva andsometimes the whole eyelid, often with a ropy,
non-purulent mucoid discharge. There is
variable redness.
Viral conjunctivitis, commonly known as "pink
eye", shows a fine diffuse pinkness of the
conjunctiva which is easily mistaken for the
'ciliary injection' of iritis, but there are usually
corroborative signs on bio microscopy,
particularly numerous lymphoid follicles on the
tarsal conjunctiva, and sometimes a punctatekeratitis.
Pyogenic bacterial conjunctivitis shows anopaque purulent discharge, a very red eye, and
on bio microscopy there are numerous white cells and desquamated epithelial cells seen
in the 'tear gutter' along the lid margin. The tarsal conjunctiva is a velvety red and not
particularly follicular. Non-pyogenic infections can show just mild infection and bedifficult to diagnose. Scarring of the tarsal conjunctiva is occasionally seen in chronic
infections, especially in trachoma.
Irritant or toxic conjunctivitis show primarily marked redness. If due to splash injury, it is
often present only in the lower conjunctival sac. With some chemicals—above all with
caustic alkalis such as sodium hydroxide —there may be necrosis of the conjunctiva witha deceptively white eye due to vascular closure, followed by sloughing of the dead
epithelium. This is likely to be associated with slit-lamp evidence of anterior uveitis.
Causes
The leading cause of a red, inflamed eye is a bacterial infection. A number of different
bacteria can be responsible for the infection. Bacterial symptoms are usually associated
with more of a discharge that is green or yellow in color. Often, bacterial "cold-like"
symptoms, such as sinus congestion and runny nose, are also present. The eyelids may be
swollen. Sometimes looking at bright lights is painful. While bacterial conjunctivitis maynot require an antibiotic, those affected should see a doctor, as occasionally this form of
conjunctivitis can be associated with infection of the cornea (the clear portion of the front
of the eyeball). This infection must be correctly detected and treated. Bacterial
conjunctivitis is highly contagious and airborne, but usually resolves in seven to 10 days
after symptoms appear.
An eye red due to acute conjunctivitis.
An eye with bacterial conjunctivitis.

8/14/2019 Eyes Disorder
http://slidepdf.com/reader/full/eyes-disorder 10/14
Differential diagnosis
Formally known as the Ian Wood Virus, Conjunctivitis symptoms and signs are relatively
non-specific. Even after bio microscopy, laboratory tests are often necessary if proof of
etiology is needed.
A purulent discharge (a whitish-yellow, yellow or yellow-brown substance more
commonly known as pus) strongly suggests bacterial cause, unless there is known
exposure to toxins. Pink eye can also be caused by bacteria from feces, pet hair, or smoke
or other fumes. Infection with Neisseria gonorrhoeae should be suspected if the
discharge is particularly thick and copious.
Itching (rubbing eyes) is the hallmark symptom of allergic conjunctivitis. Other
symptoms include past history of eczema, or asthma.
A diffuse, less "injected" conjunctivitis (looking pink rather than red) suggests a viralcause, especially if numerous follicles are present on the lower tarsal conjunctiva on bio
microscopy.
Scarring of the tarsal conjunctiva suggests trachoma, especially if seen in endemic areas,
if the scarring is linear (von Arlt's line), or if there is also corneal vascularisation.
Clinical tests for lagophthalmos, dry eye (Schirmer test) and unstable tear film may help
distinguish the various types of pink eye.
Other symptoms including pain, blurring of vision and photophobia should not be prominent in conjunctivitis. Fluctuating blurring is common, due to tearing and mucoid
discharge. Mild photophobia is common. However, if any of these symptoms are
prominent, it is important to exclude other diseases such as glaucoma, uveitis, keratitis and even meningitis or caroticocavernous fistula.
Many people who have conjunctivitis have trouble opening their eyes in the morning
because of the dried mucus on their eyelids. There is often excess mucus over the eye
after sleeping for an extended period.
Treatment and managementConjunctivitis sometimes requires medical attention. The appropriate treatment depends
on the cause of the problem. For the allergic type, cool water poured over the face with
the head inclined downward constricts capillaries, and artificial tears sometimes relieve
discomfort in mild cases. In more severe cases, non-steroidal anti-inflammatory
medications and antihistamines may be prescribed. Some patients with persistent allergic
conjunctivitis may also require topical steroid drops.

8/14/2019 Eyes Disorder
http://slidepdf.com/reader/full/eyes-disorder 11/14
Diabetic RetinopathyDiabetic retinopathy is retinopathy (damage to the retina) caused by
complications of diabetes mellitus, which caneventually lead to blindness. It is an ocular
manifestation of systemic disease which affects
up to 80% of all patients who have had
diabetes for 10 years or more[1]. Despite these
intimidating statistics, research indicates that at
least 90% of these new cases could be reduced
if there was proper and vigilant treatment and
monitoring of the eyes
Signs and symptoms
Diabetic retinopathy often has no earlywarning signs. Even macular edema, which
may cause vision loss more rapidly, may not
have any warning signs for some time. In
general, however, a person with macular
edema is likely to have blurred vision, making
it hard to do things like read or drive. In somecases, the vision will get better or worse during
the day.
As new blood vessels form at the back of the
eye as a part of proliferative diabetic
retinopathy (PDR), they can bleed
(hemorrhage) and blur vision. The first time
this happens, it may not be very severe. In
most cases, it will leave just a few specks of
blood, or spots, floating in a person's visual field, though the spots often go away after a
few hours.
These spots are often followed within a few days or weeks by a much greater leakage of
blood, which blurs vision. In extreme cases, a person will only be able to tell light from
dark in that eye. It may take the blood anywhere from a few days to months or even years
to clear from the inside of the eye, and in some cases the blood will not clear. These types
of large hemorrhages tend to happen more than once, often during sleep.
On fundoscopic exam, a doctor will see cotton wool spots, flame hemorrhages, and dot-
blot hemorrhages.
Diagnosis
Diabetic retinopathy is detected during an eye examination that includes:
• Visual acuity test : This test uses an eye chart to measure how well a person sees at
various distances (i.e., visual acuity).
• Pupil dilation: The eye care professional places drops into the eye to widen the
pupil. This allows him or her to see more of the retina and look for signs of
Normal vision. Courtesy NIH NationalEye Institute
The same view with diabetic retinopathy.
8/14/2019 Eyes Disorder
http://slidepdf.com/reader/full/eyes-disorder 12/14
diabetic retinopathy. After the examination, close-up vision may remain blurred
for several hours.
• Ophthalmoscopy: This is an examination of the retina in which the eye care
professional: (1) looks through a device with a special magnifying lens that
provides a narrow view of the retina, or (2) wearing a headset with a bright light,
looks through a special magnifying glass and gains a wide view of the retina. Notethat hand-held ophthalmoscopy is insufficient to rule out significant and treatablediabetic retinopathy.
• Optical coherence tomography (OCT): This is an optical imaging modality based
upon interference, and analogous to ultrasound. It produces cross-sectional images
of the retina (B-scans) which can be used to measure the thickness of the retina
and to resolve its major layers, allowing the observation of swelling and or
leakage.
• Digital Retinal Screening Programs: Systematic programs for the early detection
of eye disease including diabetic retinopathy are becoming more common, such as
in the UK, where all people with diabetes mellitus are offered retinal screening atleast annually. This involves digital image capture and transmission of the images
to a digital reading center for evaluation and treatment referral. See Vanderbilt
Ophthalmic Imaging Center [1] and the English National Screening Programmefor Diabetic Retinopathy [2]
• Slit Lamp Biomicroscopy Retinal Screening Programs: Systematic programs for
the early detection of diabetic retinopathy using slit-lamp biomicroscopy. These
exist either as a standalone scheme or as part of the Digital program (above) where
the digital photograph was considered to lack enough clarity for detection and/or
diagnosis of any retinal abnormality.
Treatments
Laser photocoagulation
Laser photocoagulation can be used in two scenarios for the treatment of diabetic
retinopathy.It is widely used for early stages of proliferative retinopathy.
Panretinal photocoagulation
Panretinal photocoagulation, or PRP (also called scatter laser treatment), is used to treat proliferative diabetic retinopathy (PDR).The goal is to create 1,000 - 2,000 burns in the
retina with the hope of reducing the retina's oxygen demand, and hence the possibility of
ischemia. In treating advanced diabetic retinopathy, the burns are used to destroy the
abnormal blood vessels that form in the retina. This has been shown to reduce the risk of
severe vision loss for eyes at risk by 50%.
Intravitreal Triamcinolone acetonide
Triamcinolone is a long acting steroid preparation. When injected in the vitreous cavity,
it results in a decrease in the macular edema (thickening of the retina at the macula)caused due to diabetic maculopathy, along with an increase in the visual acuity. The
effect of triamcinolone is transient, lasting up to three months, and necessitating repeated
injections for maintaining the beneficial effect. Complications of intravitreal injection of
triamcinolone include cataract, steroid induced glaucoma and endophthalmitis.
Vitrectomy
Instead of laser surgery, some people need an eye operation called a vitrectomy to restore
vision. A vitrectomy is performed when there is a lot of blood in the vitreous. It involves
removing the cloudy vitreous and replacing it with a saline solution.

8/14/2019 Eyes Disorder
http://slidepdf.com/reader/full/eyes-disorder 13/14
Studies show that people who have a vitrectomy soon after a large hemorrhage are more
likely to protect their vision than someone who waits to have the operation. Early
vitrectomy is especially effective in people with insulin-dependent diabetes, who may be
at greater risk of blindness from a hemorrhage into the eye.
Vitrectomy is often done under local anesthesia. The doctor makes a tiny incision in thesclera, or white of the eye. Next, a small instrument is placed into the eye to remove the
vitreous and insert the saline solution into the eye.
Patients may be able to return home soon after the vitrectomy, or may be asked to stay in
the hospital overnight. After the operation, the eye will be red and sensitive, and patients
usually need to wear an eyepatch for a few days or weeks to protect the eye. Medicated
eye drops are also prescribed to protect against infection.

8/14/2019 Eyes Disorder
http://slidepdf.com/reader/full/eyes-disorder 14/14