Embed Size (px)
Citation preview

Dieses Heft wurde für die Fortbildung der Schweizer Dermatologen dank einer Hilfe die folgenden Firmen realisiert:
Ce numéro a été réalisé grâce à une aide pour la formation continue des
DHDERMATOLOGICA HELVETICASeptembre 2017 – Volume 29 – N° 7
Neuheit gegen Kalzinose
Du nouveau contre les calcinoses
Einen Patienten unter Isotretinoin
operieren ?
Opérer le patient sous isotrétinoïne ?
Orales Vitamin D gegen Sonnenbrand
Mutanom-Vakzine
Bräunung ohne UV
Vitamine D orale contre le coup de soleil
Vaccins mutanomiques
Bronzage sans UV
Klinische Fälle aus BernCas cliniques de Berne
Fokus AkneFocus acné
Jahresmagazin 2017/2018
IHRGRATIS- EXEMPLARHautratgeberAkne
Seite 14
Sonnenschutz
Seite 24
Haarausfall
Seite 34
Haut und Laser
Seite 46
* Signifikanter Unterschied zu Monosubstanzen (Adapalen, BPO) nach Woche 1.1, 3 ** Epiduo® hat sich in der Langzeitanwendung über 12 Monate als sicher erwiesen und kann als Erhaltungstherapie eingesetzt werden.1, 4, 5
Referenzen: 1. Fachinformation Epiduo®; www.swissmedicinfo.ch. 2. Gollnick H et al., Can we define Acne as a chronic disease? Am J Clin Dermatol. 9. (5). 2008; 279-284. 3. Gollnick HPM et al. Adapalene–BPO Study Group. Adapalene–benzoyl peroxide, a unique fixed-dose combination topical gel for the treatment of acne vulgaris: a transatlantic, randomized, double-blind, controlled study in 1670 patients. Br J Dermatol.; 161(5):1180-1189; 2009. 4. Pariser et. al., Longterm safety and efficacy of a unique fixed-dose combination gel of adapalene 0.1% and benzoyl peroxyde 2.5% for the treatment of acne vulgaris. J. Drugs Dermatol. 6. 9. 2007; 899-905. 5. Nast A. et. al., European Evidence-based (S3) Guideline for the Treatment of Acne (Update 2016); http://www.euroderm.org/edf/index.php/edf-guidelines/category/4-guidelines-acne; Zugriff 24.7.2017.
Epiduo® Gel. Z: Adapalenum 1 mg/g, Benzoylis Peroxidum 25 mg/g. Hilfsstoffe: Propylenglycolum, Excipiens ad gelatum. I: Behandlung der Haut bei Acne vulgaris, bei Vorliegen von Komedonen, Papeln und Pusteln. D: 1x / Tag, abends auf die gesamten von Akne befallenen Flächen auftragen, bei trockener und sauberer Haut. Die Sicherheit und Wirksamkeit bei Kindern unter 12 Jahren ist nicht gezeigt. KI: Überempfindlichkeit gegen einen Inhaltsstoff. VM: Nicht auf beschädigte und ekzematöse Haut auftragen. Bei irritativen Reaktionen die Medikationshäufigkeit reduzieren. Kontakt mit Augen-, Mund-, Nasen- und sonstigen Schleimhäuten vermeiden. Eine übermässige Aussetzung dem Sonnenlicht oder UV-Strahlen vermeiden. Kontakt mit farbigem Material (Haare und Textilien), Risiko der Bleichwirkung. IA: Andere Retinoide, Benzoylperoxid oder sonstige Arzneimittel mit ähnlicher Wirkung nicht gleichzeitig einsetzen. Kosmetika mit austrocknenden Eigenschaften. UAW: Häufig: Hautirritation, Trockene Haut, irritative Kontaktdermatitis, Hautabschuppung, Desquamation, Erythema, Hautbrennen. Anzeichen solcher lokalen Unverträglichkeiten bilden sich meistens nach 1 Woche zurück. SS/ST: Keine Anwendung in der Schwangerschaft und Stillzeit. Bei einer unerwartet eintretenden Schwangerschaft ist die Behandlung umgehend zu beenden. P: Tube zu 30 g und 60 g, Dispenser zu 45 g. Liste B, SL. Zulassungs- inhaberin: Galderma Schweiz AG, 4622 Egerkingen. Weiterführende Informationen unter www.swissmedicinfo.ch. Stand: April 2016. Code: 1708-Epi-I-01
Galderma Schweiz AG | Froschackerstrasse 6 | CH-4622 Egerkingen | T + 41 62 387 88 00 | F + 41 62 387 88 11 | [email protected]
• Epiduo® wirkt schnell gegen Akne.1, 3*
• Epiduo® ist langfristig anwendbar.1, 4 **
AKNEBEHANDLUNG OHNE ANTIBIOTIKA1
Akne benötigt eine schnell wirksame und langfristige Therapie.2
ANTIBIOTIKAFREI
ANTIB
IOTIKAFREI
1x
Authors instructions (peer reviews)
Size: Papers should comprise approximately 700-2000 words including fi gures, tables and references. Title page: The fi rst page of each paper should indicate the title, the authors’ names, the institute where the work was conducted, and a short title for use as running head.Full address: The exact postal address of the corresponding author complete with postal code must be given. Key words: For indexing purposes, a list of 3–5 key words in English is essential for all papers.Abstract: Normally each paper needs an abstract of not more than 150 words. It should contain the following information: purpose of the study, procedures, results, conclusions and message of the paper. Abstracts submitted for publication in the section Original Papers should be structured as follows:Background: What is the major problem that prompted the study• Objective: What is the purpose of the study?• Methods: How was the study performed?Results: Most important fi ndings?• Conclusion: Most important conclusion? Footnotes: Avoid footnotes. When essential, they are numbered consecutively and typed at the foot of the appropriate page.Formatting rules:• Do not use any special page layout. If you would like to see what your manuscript looks like with embedded tables and illustra-
tions, remember that we need text and illustrations as separate fi les! • Enter your text continuously fl ush left. Do not use hard returns ("enter") within a paragraph, only at its end. • Do not use footer and header functions. • Use boldface and italics as well as sub- and superscript where appropriate. • Use your word-processing program to insert Greek letters, mathematical symbols, etc. Legends: The legends to your fi gures are part of the text and should be listed at the end of your text fi le. Line Drawings Black and White Half-Tone Images, Color IllustrationsScans• For processing and retouching scanned half-tone images, Photoshop is recommended. Please save the original scan as well as
your processed version. • Export black and white half-tones and color illustrations as TIF or EPS format, as close as possible to their anticipated size in print. • Save them as separate fi les, not embedded in the text. • Scanned line drawings must be digitalized with a resolution of at least 800, better 1000 dpi (dots per inch) after scaling. • Scanned half-tone images should be digitalized with a fi nal resolution of 300 dpi, a 12 bit grayscale accuracy and a density range
of 2.8. Screen values must lie between 5% and 95%. • Scanned color illustrations must be digitalized in RGB mode with a resolution of at least 300 dpi, a 32 bit accuracy and a density
range of 2.8. • Summary.Make sure that your original has the resolution values in this table after scaling, otherwise the printing quality may be inadequate.
Detailled authors instruction will soon be avaible on our upcoming website.
Warnung / Avertissement
Für den Inhalt ausserhalb des redaktionellen Teils (insbesondere Anzeigen, Industrieinformationen, Pressezitate und Kongressinformationen) übernehmen Redaktion und Verlag keine Ge-währ. Eine Markenbezeichnung kann warenzeichenrechtlich geschützt sein, auch wenn bei ihrer Verwendung in dieser Zeitschrift das Zeichen® oder ein anderer Hinweis auf etwa bestehende Schutzrechte fehlen sollten.L’éditeur et la rédaction déclinent toute responsabilité concernant le contenu non rédactionel du périodique (en particulier les annonces, les informations émanant de l’industrie, les citations tirées de la presse et les informations issues de congrès). Une marque déposée peut jouir d’une protection légale même si elle est mentionée dans le périodique sans le symbole ® ou toute autre marque signalant, le cas échéant, une telle protection juridique.
Dosierungsangaben von Medikamenten: Autoren und Verlag haben alle Anstrengungen unternommen, um sicherzustellen, dass Auswahl und Dosierungsangaben von Medikamenten im vorliegenden Text mit den aktuellen Vor-schriften und der Praxis übereinstimmen. Trotzdem muss der Leser im Hinblick auf den Stand der Forschung, Änderungen staatlicher Gesetzgebungen und den unterbrochenen Fluss neuer Forschungsergeenisse bezüglich Medikamentenwirkung und -nebenwirkungen darauf aufmerksam gemacht werden, dass unbedingt bei jedem Medikament der Packungsprospekt konsul-tiert werden muss, um mögliche Änderungen im Hinblick auf Indikation und Dosis nicht zu übersehen. Gleiches gilt für spezielle Warnungen und Vorsichtsmassnahmen. Ganz besonders gilt dieser Hinweis für empfohlene neue und/oder nur selten gebrauchte Wirkstoff e. Alle Rechte vorbehalten. Ohne schriftliche Genehmigung des Verlags dürfen diese Publikation oder Teile daraus nicht in andere Sprachen übersetzt oder in irgendeiner Form mit mecha-nischen oder elektronischen Mitteln (einschliesslich Fotokopie, Tonaufnahme und Mikrokopie) reproduziert oder auf einem Datenträger oder einem Computersystem gespeichert werden.
Posologie des médicaments:Les auteurs et l’éditeur ont tout mis en œuvre pour s’assurer que le choix des médicaments et la posologie préconisés dans ce texte soient conformes aux recommandations et à la pratique au moment de la publication. Cependant, compte tenu des recherches en cours, des changements dans les législations et de l’affl ux constant de données nouvelles concernant la thérapie médicamenteuse et l’eff et des médicaments, il est vivement recommandé au lecteur de vérifi er sur la notice jointe à chaque emballage si aucune modifi cation n’est intervenue dans la poso-logie et si aucune nouvelle contre-indication ou précaution à prendre n’a été signalée. Cela est particulièrement important lorsque l’agent recommandé est nouveau ou peu employé. Tous droits de reproduction, même partielle, sous n’importe quelle forme, strictement réservés.
ANZEIGENREGIE / REGIE DES ANNONCES
Carine HERRERAS
Tél. +41 79 667 32 48
E-mail : [email protected]
EDITION
Dermatologica Helvetica
JH Saurat
22, rue de l’Athénée
CH-1206 Genève
DHDERMATOLOGICA HELVETICASeptembre 2017 – Volume 29 – N° 7
SOMMAIRE
4 Journal Club
10 Fokus - Focus
16 SGDV - SSDV
22,26 Reports
30 Portrait
31 Terminologie
32 Forum
33 Photo du mois
RUBRIKEN DER DERMATOLOGICA HELVETICA – RUBRIQUES DE DERMATOLOGICA HELVETICAWeiterbildung – Formation continue
Redaktionsbüro, Bureau éditorial:
JH Saurat: Chefredaktor, Editeur en chefM Harms: Chefredaktor StV, Editeur en chef adjointeA Navarini: Assoziierter Redaktor, Rédacteur associéC Hsu: Redaktor für die Social Media, Editeur sur les médias sociauxCarine Herreras ([email protected]): Redaktionsbüro, Bureau éditorialAtar Roto Presse SA, Genève: Druck, Impression
Sektionen, Sections :JH Saurat: Journal Club, FocusChefärzte, Médecins chef-de-service: Case reports, coups d’œil (Koordination: Redaktionsbüro, Coordination: Bureau rédactionel, C Herreras, [email protected])A Navarini: Peer-reviewed contributionsA Navarini: Weiterbildung der Assistenzärzte, Formation post-graduée des assistantsM Harms: Das diagnostische Photo, Photo du mois, terminologieJP Grillet: Humor, Billet d’humourJ Hafner, C Mainetti : Tribune des Präsidenten, Tribune du présidentM Tomasik: Neues aus dem Generalsekretariat, Nouvelles du secrétariat généralR Barbézat: Neue Mitglieder, Nouveaux membresNeues aus den kantonalen Dermatologengesellschaften, den Kommissionen und Arbeitsgruppen, Nouvelles des sociétés cantonales de dermatologie et vénéréologie, des commissions et des groupes de travail (Koordination: Redak-tionsbüro, Coordination: Bureau éditorial, C Herreras, [email protected])Neues aus der Industrie, Nouvelles de l’industrie (Koordination: Redaktionsbüro, Coordination: Bureau éditorial, C Herreras, [email protected])
Ständige Kommission für Kommunikation, Commission permanente pour la communication :AK Lapointe, AM Skaria: Redaktoren Westschweiz, Editeurs députés pour la Suisse romandeE Bianchi, F Pelloni: Redaktoren Tessin, Editeurs députés pour le TessinB. Schlagenhauff , J Hafner: Redaktoren deutsch-sprachige Schweiz, Editeurs députés pour la Suisse alémanique
e-mail : [email protected]
ISSN : 1420-2360
Dermatologica Helvetica – Volume 29(7) – Septembre 2017 3
JO
UR
NA
L C
LU
B S
ele
cte
d b
y J
H S
AU
RA
T
Vit D for treating sunburn
Oral vitamin D rapidly attenuates infl ammation from sunburn: an interventional study
J.F. Scott, et al.Department of Dermatology, University Hospi-tals Cleveland Medical Center, Cleveland,OH, USA
The diverse immunomodulatory eff ects of vita-min D are increasingly being recognized. Howe-ver, the ability of oral vitamin D to modulate acute infl ammation in vivo has not been esta-blished in humans. In a double-blinded, place-bo-controlled interventional trial, twenty heal-thy adults were randomized to receive either placebo or a high dose of vitamin D3 (cholecal-ciferol) one hour after experimental sunburn in-duced by an erythemogenic dose of ultraviolet radiation. Compared to placebo, participants receiving vitamin D3 (200,000 IU) demonstrated reduced expression of pro-infl ammatory me-diators TNF-α (p=0.04) and iNOS (p=0.02) in skin biopsy specimens 48 hours after experimental sunburn. A blinded, unsupervised hierarchical clustering of participants based on global gene expression profi les revealed that participants with signifi cantly higher serum vitamin D3 levels after treatment (p=0.007) demonstrated increased skin expression of the anti-infl am-matory mediator arginase-1 (p=0.005), and a sustained reduction in skin redness (p=0.02), correlating with signifi cant expression of genes related to skin barrier repair. In contrast, par-ticipants with lower serum vitamin D3 levels had signifi cant expression of pro-infl ammatory genes. Together the data may have broad impli-cations for the immunotherapeutic properties of vitamin D in skin homeostasis, and implicate arginase-1 up regulation as a previously unre-ported mechanism by which vitamin D exerts anti-infl ammatory eff ects in humans.
The Journal of Investigative Dermatology, 2017, doi: 10.1016/j.jid.2017.04.040.
A new tool against calcinosis
Ectopic calcifi cation in pseudoxanthoma elasti-cum responds to inhibition of tissue-nonspeci-fi c alkaline phosphatase
S.G. Ziegler, et al.Institute of Genetic Medicine, Johns Hop-kins University School of Medicine, Baltimore, MD21205, USA
Biallelic mutations in ABCC6 cause pseudoxan-thoma elasticum (PXE), a disease characterized by calcifi cation in the skin, eyes, and blood ves-sels. The function of ATP-binding cassette C6 (ABCC6) and the pathogenesis of PXE remain unclear. We used mouse models and patient fi broblasts to demonstrate genetic interaction and shared biochemical and cellular mecha-
nisms underlying ectopic calcifi cation in PXE and related disorders caused by defi ned per-turbations in extracellular adenosine 5'-triphos-phate catabolism. Under osteogenic culture conditions, ABCC6 mutant cells calcifi ed, sug-gesting a provoked cell-autonomous defect. Using a conditional Abcc6 knockout mouse model, we excluded the prevailing pathoge-nic hypothesis that singularly invokes failure of hepatic secretion of an endocrine inhibitor of calcifi cation. Instead, defi ciency of Abcc6 in both local and distant cells was necessary to achieve the early onset and penetrant ectopic calcifi cation observed upon constitutive gene targeting. ABCC6 mutant cells additionally had increased expression and activity of tissue-nonspecifi c alkaline phosphatase (TNAP), an enzyme that degrades pyrophosphate, a major inhibitor of calcifi cation. A selective and orally bioavailable TNAP inhibitor prevented calcifi ca-tion in ABCC6 mutant cells in vitro and attenua-ted both the development and progression of calcifi cation in Abcc6−/− mice in vivo, without the deleterious eff ects on bone associated with other proposed treatment strategies.
Science Translational Medicine, 2017, 9, eaal1669.
Innate immune pathways in cutaneous lupus
Immunostimulatory Endogenous Nucleic Acids Drive the Lesional Infl ammation in Cutaneous Lupus Erythematosus
B. Scholtissek, et al.Department of Dermatology and Allergy, Uni-versity Hospital Bonn, Bonn, Germany.
Cutaneous lupus erythematosus (CLE) is a pho-tosensitive autoimmune disease characterized by a strong type I IFN-associated infl amma-tion. Keratinocytes are known to determine the interface dermatitis pattern in CLE by pro-duction of proinfl ammatory cytokines in the lower epidermis. These cytokines drive a cyto-toxic antiepithelial immune response resul-ting in keratinocytic cell death and release of endogenous nucleic acids. We hypothesized that these endogenous nucleic acids (RNA and DNA motifs) have the capacity to activate innate immune pathways in keratinocytes via pathogen recognition receptors. Gene expres-sion analyses showed an excessive activation of innate immune response pathways with strong expression of IFN-regulated cytokines in CLE skin lesions. Cultured keratinocytes produce large amounts of these cytokines in response to stimulation of PRR with endogenous nucleic acids. UV stimulation enhances the immunoge-nicity of endogenous nucleic acids and induces CLE-like skin lesions in knockout mice lacking the cytosolic DNase TREX1. Our results provide evidence for a pathogenetic role of endoge-nous nucleic acids in CLE. They are released
4 Dermatologica Helvetica – Volume 29(7) – Septembre 2017

BEHANDLUNGMEDIKAMENT
HYGIENEKOSMETIK
NEU
3 wertvolle Inhaltsstoffe
Sehr trockene und zu Juckreiz neigende Haut
Reinigt, spendet Feuchtigkeit, schützt und beruhigt
Erhält die Hautbarriere und minimiert das Allergierisiko
TÄGLICHES PFLEGEPROGRAMM
SANFTE REINIGUNG, GESICHT UND KÖRPER
DEXERYL® ReinigungscremeDEXERYL® Creme
Kurzinformation DEXERYL® Creme:
Z: Glycerolum, Vaselinum album, Paraffi num liquidum. I: Trockene Haut bei gewissen Dermatosen,
z. B. Ichthyose. D: Zweimal täglich oder bei Bedarf öfter. KI: Überempfi ndlicheit gegen einen
der Inhaltsstoffe. VM: Nicht schlucken. Nicht auf infi zierten Wunden anwenden. Beim Stillen
wird empfohlen, die Brust auszulassen. IA: Es liegen keine Studien vor. UAW: Gelegentlich:
Urtikaria, Rötungen, Juckreiz. Vereinzelt Ekzeme. Liste D, SL. Ausführliche Informationen unter
www.swissmedicinfo.ch. Pierre Fabre (Suisse) SA, 4123 Allschwil. 07/2017. Dexe-CH-170713
· Glycerin· Vaseline· Paraffi nöl

JO
UR
NA
L C
LU
Bwithin the cytotoxic inflammation along the dermo-epidermal junction and have the capa-city to drive the CLE-typical inflammation. UV irradiation supports this inflammation by gene-ration of highly immunostimulatory DNA motifs (8-hydroxyguanosine). These findings explain the photosensitivity of patients with lupus and identify pathways of the innate immune system as targets for future therapies.
Journal of Investigative Dermatology, 2017, 137, 1484e1492; doi:10.1016/j.jid.2017.03.018.
Individual mutanome vaccines: a revolution in immunotherapy of melanoma
Personalized RNA mutanome vaccines mobilize poly-specific therapeutic immunity against can-cer
U. Sahin, et al.Biopharmaceutical New Technologies (BioN-Tech) Corporation, Mainz, Germany.
T cells directed against mutant neo-epitopes drive cancer immunity. However, spontaneous immune recognition of mutations is inefficient. We recently introduced the concept of indivi-dualized mutanome vaccines and implemented an RNA-based poly-neoepitope approach to mobilize immunity against a spectrum of can-cer mutations. Here we report the first-in-hu-man application of this concept in melanoma. We set up a process comprising comprehensive identification of individual mutations, compu-tational prediction of neo-epitopes, and design and manufacturing of a vaccine unique for each patient. All patients developed T cell responses against multiple vaccine neo-epitopes at up to high single-digit percentages. Vaccine-induced T cell infiltration and neo-epitope-specific kil-ling of autologous tumour cells were shown in post-vaccination resected metastases from two patients. The cumulative rate of metastatic events was highly significantly reduced after the start of vaccination, resulting in a sustained progression-free survival. Two of the five pa-tients with metastatic disease experienced vac-cine-related objective responses. One of these patients had a late relapse owing to outgrowth of β2-microglobulin-deficient melanoma cells as an acquired resistance mechanism. A third patient developed a complete response to vac-cination in combination with PD-1 blockade therapy. Our study demonstrates that indivi-dual mutations can be exploited, thereby ope-ning a path to personalized immunotherapy for patients with cancer.
Nature, 2017, doi:10.1038/nature23003.
Not all staph aureus equally bad in atopic dermatitis
Staphylococcus aureus and Staphylococcus epi-dermidis strain diversity underlying pediatric atopic dermatitis
A.L. Byrd, et al.Microbial Genomics Section, National Human Genome Research Institute, National Institutes of Health, Bethesda, USA
The heterogeneous course, severity, and treat-ment responses among patients with atopic dermatitis (AD; eczema) highlight the complexi-ty of thismultifactorial disease. Prior studies have used traditional typingmethods on culti-vated isolates or sequenced a bacterial marker gene to study the skin microbial communities of AD patients. Shotgunmetagenomic sequence analysis provides much greater resolution, elu-cidating multiple levels of microbial community assembly ranging from kingdom to species and strain-level diversification. We analyzedmicro-bial temporal dynamics from a cohort of pedia-tric AD patients sampled throughout the di-sease course. Species-level investigation of AD flares showed greater Staphylococcus aureus predominance in patients with more severe disease and Staphylococcus epidermidis pre-dominance in patients with less severe disease. At the strain level, metagenomic sequencing analyses demonstrated clonal S. aureus strains inmore severe patients and heterogeneous S. epidermidis strain communities in all patients. To investigate strain-level biological effects of S. aureus, we topically colonized mice with human strains isolated from AD patients and controls. This cutaneous colonization model demons-trated S. aureus strain–specific differences in eliciting skin inflammation and immune signa-tures characteristic of AD patients. Specifically, S. aureus isolates from AD patients with more severe flares induced epidermal thickening and expansion of cutaneous T helper 2 (TH2) and TH17 cells. Integrating high-resolution sequen-cing, culturing, and animal models demonstra-ted how functional differences of staphylococ-cal strains may contribute to the complexity of AD disease.
Science Translational Medicine, 2017, 9, eaal4651.
Sunbeds do induce vitD production
25-Hydroxyvitamin-D3 serum modulation after use of sunbeds compliant with European Union standards: A randomized open observational controlled trial
B. Weber, et al.Department of Dermatology, University Hospi-tal Zurich
6 Dermatologica Helvetica – Volume 29(7) – Septembre 2017
JO
UR
NA
L C
LU
B
Background: Regular use of sunbed exposure has been reported to increase 25-hydroxyvita-min-D3 [25(OH) D] serum levels. However, the influence of sunbeds compliant with the recent European Union standard EN-60335-2-27 on 25(OH)D serum levels is unknown.Objective: We investigated the impact of stan-dard sunbed use compliant with the European Union standard on 25(OH)D serum modulation and well-being.Methods: In a randomized controlled study, 25(OH)D serum levels were measured at enrol-lment, after 1 week, and after completion of the 12-week period of sunbed use with twice weekly exposure and compared with the control group without any sunbed exposure.Results: In the sunbed intervention group (N=31), a 27% increase of mean 25(OH)D levels was noted 1 week after starting sunbed use (P<.01). However, after 12 weeks, mean 25(OH)D levels had declined and were no longer dif-ferent from baseline (P = .06). After 12 weeks, 25(OH)D levels did not differ between the inter-vention and control group (P = .36). Also the 5-item World Health Organization Well-Being Index score did not differ between the sunbed and control groups (P = .19).Limitations: For ethical reasons recruitment was limited to persons actively seeking sunbed exposure.Conclusions: Standard use of sunbeds com-pliant with the European Union standard in-duced a transient increase of 25(OH)D levels, whereas no change in well-being was observed.
Journal of the American Academy of Dermato-logy, 2017;77: 48-54.
"You can always make your patient feel better even if you can't make him look better"
Shelley, Walter B. "Advanced Dermatologic Diagnosis" W.B. Saunders 1992
Dermatologica Helvetica – Volume 29(7) – Septembre 2017 7
JO
UR
NA
L C
LU
BTopical modulation of human skin pigmentation closer to the clinic
A UV-Independent Topical Small-Molecule Ap-proach for Melanin Production in Human Skin
N. Mujahid, et al.Department of Pathology and Laboratory Me-dicine, Boston University School of Medicine, Boston, USA.
The presence of dark melanin (eumelanin) wit-hin human epidermis represents one of the strongest predictors of low skin cancer risk. To-pical rescue of eumelanin synthesis, previously achieved in "redhaired" Mc1r-defi cient mice, demonstrated signifi cant protection against UV damage. However, application of a topical strategy for human skin pigmentation has not been achieved, largely due to the greater bar-
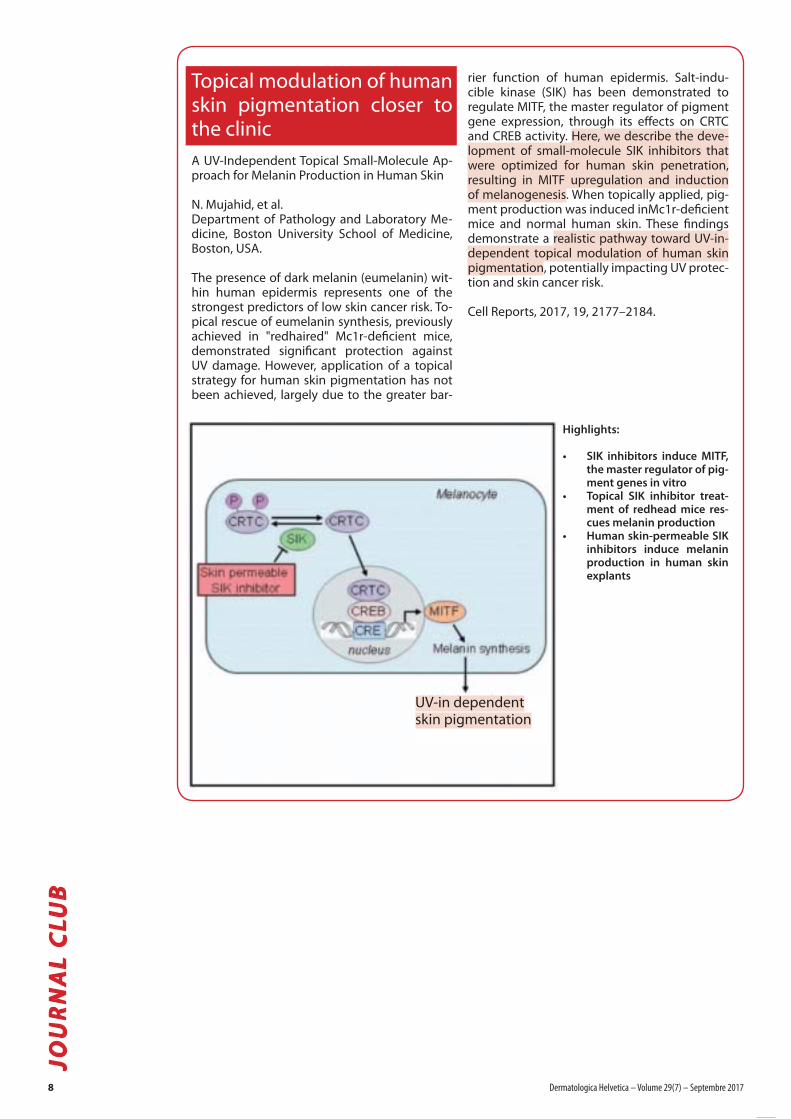
rier function of human epidermis. Salt-indu-cible kinase (SIK) has been demonstrated to regulate MITF, the master regulator of pigment gene expression, through its eff ects on CRTC and CREB activity. Here, we describe the deve-lopment of small-molecule SIK inhibitors that were optimized for human skin penetration, resulting in MITF upregulation and induction of melanogenesis. When topically applied, pig-ment production was induced inMc1r-defi cient mice and normal human skin. These fi ndings demonstrate a realistic pathway toward UV-in-dependent topical modulation of human skin pigmentation, potentially impacting UV protec-tion and skin cancer risk.
Cell Reports, 2017, 19, 2177–2184.
Highlights:
• SIK inhibitors induce MITF, the master regulator of pig-ment genes in vitro
• Topical SIK inhibitor treat-ment of redhead mice res-cues melanin production
• Human skin-permeable SIK inhibitors induce melanin production in human skin explants
UV-in dependentskin pigmentation
8 Dermatologica Helvetica – Volume 29(7) – Septembre 2017
ÜberzeugendeWirksamkeit
dank innovativerNano emulsion1–5
Wirksamerals Methylamino-levulinat bei AK2,4
Effektiv, selektivund nachhaltig1–5
Kassenzulässig*
Referenzen1 Maisch T et al. Fluorescence induction of protoporphyrin IX by a new 5-aminolevulinic acid nanoemulsion used for photodynamic therapy in a full-thickness ex vivo skin model.Experimental Dermatology 2010; 19: e302–e305. 2 Fachinformation AMELUZ®, www.swissmedicinfo.ch. 3 Schulten R et al. Comparison of the uptake of 5-aminolevulinic acidand its methyl ester in keratinocytes and skin. Naunyn-Schmiedeberg’s Arch Pharmacol 2012; 385:969–979. 4 Dirschka T et al. Photodynamic therapy with BF-200 ALA for thetreatment of actinic keratosis. Results of a multicentre, randomized, observer-blind phase III study in comparison with a registered methyl-5-aminolaevulinate cream and placebo.BJD 2012; 166: pp137–146. 5 Dirschka T et al. Long-term (6 and 12 months) followup of two prospective, randomized, controlled phase III trials of photodynamic therapy withBF-200 ALA and methyl aminolaevulinate for the treatment of actinic keratosis. BJD 2013; pp825–836.
Gekürzte Fachinformation AMELUZ®
Z: 1 g Gel enthält 100 mg Aminolävulinsäure HCL. I: Aktinische Keratosen leichter bis mittelschwerer Intensität im Gesicht und auf der Kopfhaut. D/A: Nur unter Aufsicht einesArztes oder einer Pflegekraft mit Erfahrung in der PDT. Die Läsion und ca. 5 mm des umgebenden Areals mit einem Film von etwa 1 mm Dicke bedecken und nach 3-stündigerInkubation mit einer Rotlichtquelle beleuchten. Rotlichtquelle von ca. 630 nm, Lichtdosis ca. 37 J/cm2, Lichtquelle im Bereich von 570–670 nm, Lichtdosis 75–200 J/cm2. KI:Überempfindlichkeit gegen den Wirkstoff, Porphyrine oder einen der Hilfsstoffe; Porphyrie; bekannte Photodermatose. VM: Keine Erfahrung bei Patienten mit Gerinnungsstörungenoder unter Immunsuppression. Keine Erfahrung mit der Behandlung des Basalzellkarzinoms, der Bowen-Krankheit und schweren aktinischen Keratosen oder pigmentierten oderstark infiltrierenden Läsionen. Nicht auf blutenden Läsionen anwenden. Keine Erfahrung bei Patienten mit Hauttyp V und VI. Keine gleichzeitige Anwendung von Arzneimitteln mitbekanntem phototoxischem oder photoallergischem Potenzial. Sonnenexposition der Läsion nach Behandlung für ca. 48 h vermeiden. Bei Patienten mitAllergie gegen Erdnüsse oder Soja nicht anwenden. IA: Keine Studien, keine bekannt. SS/SZ: Anwendung während der Schwangerschaft und beiFrauen im gebärfähigen Alter, die nicht verhüten, nicht empfohlen. Das Stillen nach Applikation von AMELUZ® für 12 h unterbrechen. UW: Sehrhäufig: lokale Hautreaktionen an der Applikationsstelle (Brennen, Erythem, Schmerzen, Ödem, Pruritus, Exfoliation, Schorfbildung, Induration).Häufig: Kopfschmerzen; an der Applikationsstelle: Haut straffung, Vesikel, Parästhesie, Hyperalgesie, Erosion, Wärme empfinden. Gelegentlich ander Appli kationsstelle: pustulöser Hautausschlag, trockene Haut, Petechien, Hyperkeratose, Blutung, Missempfinden, Absonderung, Verfärbung,Ulkus, Dysästhesie, Lidödem, Wundsekretion; nicht an der Appli kationsstelle: Nervosität, Schüttelfrost, Hitzegefühl, Pyrexie, Schmerzen. P: Tubemit 2 g Gel. Abgabekategorie: B. Ausführliche Informationen entnehmen Sie bitte der vollständigen Fachinformation: www.swissmedicinfo.ch.*Kassenzulässig für leichte aktinische Keratosen. Louis Widmer AG, Rietbachstrasse 5, 8952 Schlieren-Zürich.
AKTINISCHE KERATOSE
AMELUZ® IN DER PDT

Elective procedures in isotretinoin acne patients: (1) Wait or Do ?
A Systematic Review on Oral Isotretinoin The-rapy and Clinically Observable Wound Healing in Acne Patients.
The association between isotretinoin and aty-pical wound healing remains controversial. It is common practice to delay elective pro-cedures for 6 to 24 months after oral isotreti-noin therapy. The studies supporting common practices (SCP) recommend extending this pe-riod to include the 6 to 24 months preceding treatment. The opposing studies (challenging common practices; CCP) state that the rate of scarring in isotretinoin patients is low and that delaying elective procedures is unnecessary. These practices impact a large number of der-matology patients undergoing acne treatment. This systematic review compiled articles obtai-ned from online databases and examined data from both SCP and CCP studies. The inconsis-tencies in the reported data and the methodo-logical fl aws in the literature preclude any fi rm conclusions that can resolve the controversy. As such, this review demonstrates that there is insuffi cient evidence to either corroborate or refute delaying elective procedures in isotre-tinoin acne patients. Although the recent lite-rature trends toward removing the procedural delay, we advocate for clinicians to consider the research presented in this review in the context of their own clinical experience and each indi-vidual patient's situation. The possible negative procedural outcomes must be weighed against the severity of the patient's acne scarring and the psychosocial impact of this scarring on the patient.
Journal of Cutaneous Medicine and Surgery, 2017. Epub ahead of print.
Elective procedures in isotretinoin acne patients: (2) Have an evidence-based discussion with patients…
Isotretinoin and Timing of Procedural Inter-ventions A Systematic Review With Consensus Recommendations
Importance: The notion that systemic isotreti-noin taken within 6 to 12 months of cutaneous surgery contributes to abnormal scarring or delayed wound healing is widely taught and practiced; however, it is based on 3 small case series from the mid-1980s.Objective: To evaluate the body of literature to provide evidence-based recommendations re-garding the safety of procedural interventions performed either concurrently with, or imme-
diately following the cessation of systemic iso-tretinoin therapy.Evidence review: A panel of national experts in pediatric dermatology, procedural/cosme-tic dermatology, plastic surgery, scars, wound healing, acne, and isotretinoin was convened.A systematic PubMed review of English-language articles published from 1982 to 2017 was per-formed using the following search terms: iso-tretinoin, 13-cis-retinoic acid, Accutane, reti-noids, acitretin, surgery, surgical, laser, ablative laser, nonablative laser, laser hair removal, chemical peel, dermabrasion, wound healing, safety, scarring, hypertrophic scar, and keloid. Evidence was graded, and expert consensus was obtained.Findings: Thirty-two relevant publications re-ported 1485 procedures. There was insuffi cient evidence to support delaying manual derma-brasion, superfi cial chemical peels, cutaneous surgery, laser hair removal, and fractional ablative and nonablative laser procedures for patients currently receiving or having recently completed isotretinoin therapy. Based on the available literature, mechanical dermabrasion and fully ablative laser are not recommended in the setting of systemic isotretinoin treatment.Conclusions and relevance: Physicians and pa-tients may have an evidence-based discussion regarding the known risk of cutaneous surgical procedures in the setting of systemic isotre-tinoin therapy. For some patients and some conditions, an informed decision may lead to earlier and potentially more eff ective interven-tions.
JAMA Dermatology. doi:10.1001/jamaderma-tol.2017.2077.
How patients with acne decide if their treatment is working
Prioritizing treatment outcomes: How people with acne vulgaris decide if their treatment is working
Objective: To collect information about how-people with acne make day-to-day decisions concerning the eff ectiveness of their treatment.Methods: Between May and August 2013, an optional question was embedded in the James Lind Alliance Acne Priority Setting Partnership’s online survey to collect treatment uncertain-ties. The question asked people with acne to “Tell us in your own words how you decide if your treatment has been eff ective.”Results: A total of 742 respondents specifi ed at least one outcome or means of assessing change (outcome measure). Fewer spots were the most commonly cited outcome, identifi ed by 272 respondents (36.7%). Other frequently mentioned outcomes were in descending or-der: less redness (19.4%), reduction in spot size (12.1%), and less pain/discomfort (11.4%). Signs were much more commonly used than symp-toms and surrogate outcomes such as changes F
OC
US
– A
cn
é
Se
lec
ted
by
JH
SA
UR
AT
10 Dermatologica Helvetica – Volume 29(7) – Septembre 2017
Bonne tolérance grâce à une galénique innovante1,2
• ne contient pas de BPO• ne blanchit ni les poils ni les vêtements• application seulement 1 fois par jour• gel sans alcool
REMBOURSÉ PAR
LES CAISSES MALADIE
Références: 1. Del Rosso JQ, et al. Cutis 2008;81:405-8. 2. Goreshi R, et al. J Drugs Dermatol 2012;11:1422-6. Acnatac®/Gel (clindamycini phosphas et tretinoinum): I: traitement topique de l’acné vulgaire lorsque la trétinoïne topique en monothérapie ne paraît pas assez efficace. P:
CI: Hypersensibilité aux composants. Grossesse, Allaitement. Entérite régionale, colite ulcéreuse, colite associée aux antibiotiques. antécédents de cancer de la peau. eczéma aigu, rosacée, dermatite péri-orale, acné pustuleuse ou nodulokystique profonde. MP: IA: Administration concomitante de médicaments topiques,érythromycine, bloquants neuro-musculaires. EI: Acné, peau sèche, érythème, séborrhée, réactions de photosensibilité, prurit, éruption, éruption cutanée avec desquamation, exfoliation
cutanée, coup de soleil. Réactions au site d’application: sensation de brûlure, dermatite, sécheresse de (A) Admis par les caisses.
MEDA Pharma GmbH, a company of the Mylan group.
Start
contre l’acné
NOUVEAU
Fo
cu
sin aspects of life quality were infrequently mentioned. Visual inspection of the skin was the most widely adopted outcome measure (16.3%).Conclusions: Although the most frequently used methods map well onto the outcome measures adopted in the majority of acne trials, namely physician-assessed changes in lesion counts and global acne severity, people with acne often take into account several fac-tors that cannot be assessed by a third party at a single point in time. The minimal use of changes in psychosocial wellbeing and mood may reflect that these are regarded as secon-dary consequences of improvements in appea-rance. The robustness of these findings now requires independent evaluation. If confirmed, they could form the basis of a new patient-re-ported outcome measure.
Journal of Evidence-Based Medicine, 2017; 00: 1–8.
Revisiting isotretinoin for Hidradenitis Suppurativa
A New Perspective on Isotretinoin Treatment of Hidradenitis Suppurativa: A Retrospective Chart Review of Patient Outcomes.
Background: Hidradenitis suppurativa (HS) is a disease characterized by the development of painful, deep-seeded nodules and abscesses. Treatment guidelines include a combination of lifestyle, surgical, and medical interventions. Isotretinoin has not been included in the treat-ment guidelines due to the limited number of studies and conflicting reports of efficacy.Objectives: The purpose of this study is to eva-luate the clinical response to isotretinoin in HS patients and to determine whether there is a particular patient population that may benefit more from this treatment.Methods: A retrospective chart review was conducted on all HS patients treated with iso-tretinoin within the years of 2014-2016. Sex, age, weight, history of acne, Hurley stage, and treatment dose and duration were extracted from patient charts.Results: Of the 25 patients included in the study, 32% (8/25) had no response, 32% (8/26) showed partial response, and 36% (9/25) de-monstrated complete response to isotretinoin treatment. Complete response was seen only in Hurley stage I and II patients. Hurley III patients made up 50% of the non-responders. Those with any sort of treatment response were more likely to be female, younger, weigh less, and have a higher prevalence of acne compared to non-responders.Limitations: This is a retrospective chart review with a small sample size of 25 patients.Conclusions: Physicians should consider isotre-tinoin as a potential treatment for HS, as it may be beneficial in patients with mild and mode-rate disease and patients who are female, youn-
ger, weigh less, and have a personal history of acne.
Dermatology, 2017. Epub ahead of print.
Retinoids and the brain: a class effect, as a signal emerges for alitretinoin
Psychiatric disorders, acne and systemic reti-noids: comparison of risks
The link between isotretinoin, treatment of a se-vere form of acne, and psychiatric disorders re-mains controversial, as acne itself could explain the occurrence of psychiatric disorders. This study aims at assessing the disproportionality of psychiatric adverse events reported with iso-tretinoin in the French National PharmacoVigi-lance Database, compared with other systemic acne treatments and systemic retinoids.Materials and methods: Data were extracted from the French National PharmacoVigilance Database for systemic acne treatments, syste-mic retinoids and drugs used as comparators. Each report was subjected to double-blind ana-lysis by two psychiatric experts. A dispropor-tionality analysis was performed, calculating the number of psychiatric ADRs divided by the total number of notifications for each drug of interest.Results: Concerning acne systemic treatments: all 71 reports of severe psychiatric disorders involved isotretinoin, the highest proportion of mild/moderate psychiatric adverse events was reported with isotretinoin (14.1%). Among systemic retinoids, the highest proportion of severe and mild/moderate psychiatric events occurred with isotretinoin and alitretinoin.Conclusion: Our study raises the hypothesis that psychiatric disorders associated with iso-tretinoin are related to a class effect of retinoids, as a signal emerges for alitretinoin. Comple-mentary studies are necessary to estimate the risk and further determine at-risk populations.
Expert Opinion on Drug Safety, 2017, 12:1-7.
Light therapies for acne: do they really work ?
Light therapies for acne: abridged Cochrane systematic review including GRADE assess-ments
We undertook a Cochrane review of rando-mized controlled trials (RCTs) evaluating the effects of light-based interventions for acne vulgaris. We searched the Cochrane Skin Spe-cialised Register, CENTRAL, MEDLINE, Embase, LILACS, ISI Web of Science, and grey litera-
12 Dermatologica Helvetica – Volume 29(7) – Septembre 2017
ture sources (September 2015). We used the Grading of Recommendations Assessment, Development and Evaluation Working Group approach to assess the quality of evidence (QE). We included 71 RCTs (4211 participants, median sample size 31). Results from a single study (n = 266, low QE) showed little or no dif-ference in effectiveness on participants' assess-ment of improvement between 20% aminole-vulinic acid (ALA) photodynamic therapy (PDT), activated by blue light, versus vehicle plus blue light, whereas another study (n = 180) of a com-parison of ALA-PDT (red light) concentrations showed 20% ALA-PDT was no more effective than 15%, but better than 10% and 5% ALA-PDT. Pooled data from three studies, (n = 360, moderate QE) showed that methyl aminolevu-linate (MAL)-PDT, activated by red light, had a similar effect on changes in lesion counts, com-pared with placebo cream with red light. Seve-ral studies compared yellow light to placebo or no treatment, infrared light to no treatment, gold-microparticle suspension to vehicle, and clindamycin/benzoyl peroxide (C/BPO) com-bined with pulsed dye laser to C/BPO alone. None of these showed any clinically significant effects. Most studies reported adverse effects, but inadequately, with scarring reported as ab-sent, and blistering only in studies on intense pulsed light, infrared light and PDT (very low QE). Carefully planned studies, using standar-dised outcome measures, and common acne treatments as comparators are needed.
British Journal of Dermatology, 2017. Epub ahead of print.
The still-ongoing search for the acne-inducing Pacnes clone
A comparative study of Cutibacterium (Propio-nibacterium) acnes clones from acne patients and healthy controls
Background: Cutibacterium (Propionibacte-rium) acnes is assumed to play an important role in the pathogenesis of acneObjectives: To examine if clones with distinct virulence properties are associated with acne.Methods: Multiple C. acnes isolates from fol-licles and surface skin of patients with mode-rate to severe acne and healthy controls were characterized by multilocus sequence typing. To determine if CC18 isolates from acne patients differ from those of controls in the possession of virulence genes or lack of genes conducive to a harmonious coexistence the full genomes of dominating CC18 follicular clones from six patients and five controls were sequenced.Results: Individuals carried one to ten clones simultaneously. The dominating C. acnes clones in follicles from acne patients were ex-clusively from the phylogenetic clade I-1a and all belonged to clonal complex CC18 with the exception of one patient dominated by the worldwide-disseminated and often antibiotic
resistant clone ST3. The clonal composition of healthy follicles showed a more heterogeneous pattern with follicles dominated by clones re-presenting the phylogenetic clades I-1a, I-1b, I-2 and II.Comparison of follicular CC18 gene contents, allelic versions of putative virulence genes and their promoter regions, and 54 variable-length intragenic and inter-genic homopolymeric tracts showed extensive conservation and no difference associated with the clinical origin of isolates.Conclusions: The study supports that C. acnes strains from clonal complex CC18 and the often antibiotic resistant clone ST3 are associated with acne and suggests that susceptibility of the host rather than differences within these clones may determine the clinical outcome of colonization.
Anaerobe 47, 2017, 57-63.
The first study on skin microbiotas after acne treatment
Isotretinoin and lymecycline treatments modify the skin microbiota in acne
Oral retinoids and tetracyclines have a major role in acne treatment. Here, we report for the first time the effect of isotretinoin and lymecy-cline therapy on the skin microbiota in cheek, back and armpit swab samples of acne vulgaris patients using 16S ribosomal RNA (16S rRNA) gene amplicon sequencing. Propionibacterium acnes was the most common in sebaceous areas of healthy and untreated acne skin and more abundant in back than cheek samples. Five taxa, including a Streptococcus taxon, dif-fered significantly between the cheek samples of healthy controls and acne patients, and acne severity was positively correlated with the abundance of Propionibacterium. Both treatments reduced clinical acne grades and the abundance of Propionibacterium, while the abundance of several other taxa was signi-ficantly higher in treated cheek samples com-pared with untreated ones. Less variation was observed in back samples and none in armpit samples. There were no differences in alpha diversity between control and acnepatients in any of the sampled skin areas, but the diversity of the microbiota on the cheek and the back was significantly increased after acne treat-ments. This study provides insight into the skin microbiota in acne and how it is modulated by systemic acne treatment.
Experimental Dermatology, 2017. Epub ahead of print.
Fo
cu
s
Dermatologica Helvetica – Volume 29(7) – Septembre 2017 13
Fo
cu
sEvidence-based management of acne fulminans
Evidence-based recommendations for the ma-nagement of acne fulminans and its variants
Background: Acne fulminans (AF) is a severe variant of inflammatory acne. It typically mani-fests as an explosive worsening and ulceration of skin lesions, and can be associated with sys-temic symptoms. However, there is a paucity of evidence-based information and no clear gui-delines concerning the classification and treat-ment of AF.Objective: To better define the spectrum of AF and its variants, devise optimal therapeutic ap-proaches, and identify areas of future research.Methods: A panel of physicians with expertise in severe acne vulgaris was convened after a comprehensive literature review of severe acne variants. Priority topics were reviewed and pre-sented by each panelist at a 5-hour conference. Following review of the audiotape and scribed notes from the conference, surveys were uti-lized to address points of controversy and to clarify consensus recommendations.Results: Appropriate clinical case presentations and consensus survey questions were utilized to create final recommendations based on both the literature and the expert consensus.Limitations: Limited evidenced-based data and prospective studies in the literature concerning the treatment of AF is available.Conclusion: These guidelines better characte-rize AF and provide health care practitioners approaches to the classification, treatment, and prevention of AF and its variants.
Journal of the American Academy of Dermato-logy, 2017; 77: 109-17.
Vitamin B12 acne: a reminder
Acneiform eruptions caused by vitamin B12: A report of five cases and review of the literature
We describe five cases of acneiform eruption caused by vitamin B12 in five females aged 37, 32, 62, 29, and 21 years, respectively. The erup-tion appeared from 1 week to 5 months after the beginning of the therapy with i.m. or oral vitamin B12. Clinical picture was characterized by papules and pustules located on the face. In three patients, similar lesions were also present on the neck, shoulders, chest, and upper por-tion of the back. Comedones and cysts were ab-sent. In two patients, serum vitamin B12 levels were very high. Histopathologic examination in one patient revealed an eosinophilic follicu-litis. Spontaneous and complete remission was observed in all patients 3-6 weeks after vitamin B12 discontinuation.
Journal of Cosmetic Dermatology, 2017. Epub ahead of print.
14 Dermatologica Helvetica – Volume 29(7) – Septembre 2017
Plus de 60% des patients atteintes d’eczéma chronique sévère des mains qui consultent le dermatologue sont déjà
réfractaires aux corticostéroïdes topiques puissants.*,1
Instaurez le traitement à TOCTINO chez les patients qui n’ont pas répondu aux corticostéroïdes topiques puissants depuis au
moins 4 semaines.2,3
Limitatio: Le traitement avec TOCTINO ne peut être prescrit que par des dermatologues.4
UNE GUÉRISON PERCEPTIBLE
* Basé sur les données issues d’une étude transversale multicentrique auprès de 14 centres de dermatologie en Italie, chez 981 patients atteints d’un eczéma des mains, dont 163 souffraient d’un
eczéma chronique sévère des mains.1
Références: 1. Scalone L et al. Clinical epidemiology of hand eczema in patients accessing dermatological reference centres: results from Italy. Br J Dermatol 2015;172:187-95. 2. Information
professionnelle TOCTINO, www.swissmedicinfo.ch. 3. Diepgen T et al. Guidelines for diagnosis prevention and treatment of hand eczema. Journal of the German Society of Dermatology 2015;13:e1-22.
4. www.listedesspecialites.ch, 1.6.2017.
Trade marks are owned by or licensed to the GSK group of companies. ©2017 GSK group of companies or its licensor.
GlaxoSmithKline AG Talstrasse 3–5 CH-3053 Münchenbuchsee Tél. +41 (0)31 862 21 11 Fax +41 (0)31 862 22 00 www.glaxosmithkline.ch
CH/DERM/008/17(1)/19.7.17/7.17
TOCTINO. PA: Alitrétinoïne. I: Traitement de l’eczéma chronique sévère des mains, réfractaire au traitement, chez l’adulte qui a reçu un traitement local poussé (y c. le fait d’éviter tout contact avec les agents nocifs incriminés, protection de la peau et corticostéroïdes topiques puissants) pendant au moins 4 semaines et qui n’y a pas répondu. P: 10-30 mg 1×/jour au cours d’un repas principal. Durée du traitement: 12-24 semaines. Non recommandé chez les patients de moins de 18 ans ou chez les patients présentant une insuffisance rénale modérée. Prescription pour max. 30 jours, renouvelable à chaque fois pour max. 30 jours, délivrance enl‘espace de 7 jours après la date de l‘ordonnance. CI: Toctino est TÉRATOGÈNE et contre- indiqué chez les femmes enceintes. Toctino est contre-indiqué chez les femmes en âge de procréer, sauf si toutes les conditions du programme de prévention de la grossesse sont respectées (voir G/A). D’autres CI: allaitement, insuffisance hépatique, insuffisance rénale sévère, hypercholestérolémie incontrôlée, hypertriglycéridémie incon-trôlée, hypothyroïdie incontrôlée, hypervitaminose A; hypersensibilité à l’alitrétinoïne, à d’autres rétinoïdes ou à l’un des excipients (en particulier en cas d’allergie aux arachides ou au soja); intolérance héréditaire au fructose, en association aux tétracyclines ou au méthotrexate. M/P: Sous rétinoïdes systémiques, des cas de dépres-sion, d’aggravation d’une dépression existante, d’angoisse, d’agressi-vité, d’instabilité émotionnelle, de symptômes psychotiques et, rare-ment, de tentatives de suicide/suicide ont été rapportés; surveiller les patients afin de guetter les signes d’un trouble psychiatrique. Les patients ayant des antécédents de dépression ou de tendances suicidaires doivent être pris en charge psychologiquement psychiatri-quement avant et pendant le traitement. Renforcement de
l’action des rayons UV. Modifications osseuses (notamment fermeture épiphy-saire prématurée, calcification des tendons et ligaments). Sécheresse oculaire, diminution de la vision nocturne; les patients constatant un trouble de la vision doivent être adressés à un ophtalmologue. En cas d’augmentation bénigne de la pression intracrânienne (pseudotumor cerebri), le traitement doit être interrompu. Lors d’augmentation cliniquement significative des transaminases hépatiques, réduire la dose ou interrompre le traitement. Surveillance du taux plasmatique du cholestérol et de triglycérides. En cas d’hyperlipidémie non contrô-lable, de symptômes d’une pancréatite ou d’une maladie inflamma-toire intestinale, le traitement doit être interrompu. Lors de diabète, de surpoids important, de facteurs de risque cardio-vasculaire ou de troubles du métabolisme lipidique, des contrôles plus fréquents des taux de lipides sériques sont nécessaires. Interrompre le traitement en cas de réactions allergiques sévères, telle l’angéite allergique. Pas de dons de sang pendant et jusqu’à 1 mois après le traitement (risque potentiel pour le fœtus lors de transfusion pendant la G). IA: Un traitement concomitant par des inhibiteurs puissants du CYP3A4 ou de la PgP (p. ex. le kétoconazole) augmente le taux d’alitrétinoïne. Envisager une réduction de la dose de l’alitrétinoïne à 10 mg lors d’un traitement concomitant par des inhibiteurs puissants du CYP2C9 (p. ex. la diosmine, le miconazole, le fluconazole) ou du CYP2C8 (p. ex. le gemfibrozil). L‘alitrétinoïne peut augmenter l‘exposition aux substrats du CYP2C8 (p.ex. le paclitaxel, la rosiglitazone, le répagli-nide); traitement concomitant par amiodarone non recommandé. Simvastatine; tétracyclines; méthotrexate. G/A: Toctino est impé- rativement contre-indiqué chez les femmes enceintes. Si mal-gré les mesures de contraception prises une G survient pendant ou au cours
du mois qui suit la fin du traitement par Toctino, il existe un risque élevé de malformations graves du fœtus. En cas de G, le traitement doit être interrompu et la femme doit être orientée vers un médecin spécialisé en tératologie. Toctino est contre-indiqué chez les femmes en âge de procréer, sauf si toutes les conditions du programme de prévention de la grossesse sont respec-tées: information de la patiente, conseil de contraception, formulaire de confirmation; deux méthodes de contraception fiables et ininter-rompues à partir de min. 1 mois avant, pendant et jusqu’à min. 1 mois après le traitement; tests de grossesse (2 tests à intervalle de min. 3 semaines, tests mensuels pendant et jusqu’à 1 mois après le traite-ment). Toctino est contre-indiqué chez les femmes qui allaitent. EI: Très fréquents: maux de tête, augmentation du taux de triglycé-rides et de cholestérol, baisse des lipoprotéines (HDL). Fréquents: irritation oculaire, conjonctivite; sécheresse oculaire, de la peau et/ou des lèvres; rougeur du visage, eczéma, dermatite, érythème, chéilite, alopécie, arthralgie, myalgie, augmentation de la CPK et des transa-minases, anémie, augmentation de la capacité de fixation du fer, thrombocytose, monocytopénie, diminution de la TSH et de la T4 libre, hypertension, vertiges, fatigue, dépression, acouphène. Occasionnels: vue floue, cataracte, épistaxis, prurit, exfoliation cuta-née, eczéma astéatotique, exostose, hyperostose, spondylarthrite ankylosante. Rares: angéite, pseudotumor cerebri. Post-commerciali-sation: en autre hypersensibilité (y c. réactions anaphylactiques), fluctuation d’humeur, idées suicidaire, œdème périphérique. Pr: Cap-sules à 10 ou 30 mg, 30 pces. Admis par les caisses CR: A. Mise à jour de l’information: Octobre 2015. GlaxoSmithKline SA. Une infor-mation détaillée est disponible sur www.swissmedicinfo.ch. Veuillez annoncer tout effet indésirable à [email protected].
SG
DV
– S
SD
V
Le GDG refuse l’adaptation du tarif annoncée par le Conseiller fédéral Alain Berset et tient à dénon-cer ses conséquences néfastes pour les raisons suivantes:
1. Le concept qui a prévalu à la diminution des valeurs de prestations, basé sur le fait que les avancées technologiques permettraient de diminuer les temps nécessaires à leur exécu-tion, est totalement erroné pour la dermato-logie. En effet, l’examen clinique (ou status dermatologique) prend toujours le même temps, voire plus, si l’on tient compte d’une part des lésions définies de plus en plus pré-cisément dans la littérature et qu’il faut re-chercher, et d’autre part du vieillissement de la population qui aboutit à une diminution de mobilité, qui rallonge d’autant l’examen. En ce qui concerne la chirurgie dermatolo-gique, les excisions sont pratiquées de la même manière depuis des décennies, donc sans diminution de temps objectivable.
2. Il est choquant de constater, avec les modi-fications envisagées, que plus une interven-tion technique ou chirurgicale est compli-quée et difficile (et donc nécessitant une for-mation longue et poussée), plus la réduction de sa valeur est importante. Ainsi, compte tenu des exigences de formation et d’infras-tructures pour pouvoir pratiquer une inter-vention en salle d’opération agréée, ces opé-rations complexes ne permettront plus de couvrir les frais d’installation et de fonction-nement et seront abandonnées. Les patients nécessitant ces gestes seront référés aux centres hospitaliers où les déficits inévitables engendrés par le tarif devront être couverts par les cantons, donc par les impôts. En effet, dans l’ambulatoire, les assurances assument les 100% des frais mais, dans le stationnaire, elles ne couvrent plus que les 45% des frais, les 55% restant étant pris en charge par le canton.
3. Les mesures annoncées correspondent à une attaque évidente de la qualité des soins aux patients atteints de maladies dermatolo-giques pour les raisons suivantes :
• La limitation de la position de status dermatologique (6 fois 5 minutes par 3 mois) ne permet plus de prendre en charge les patients atteints de mala-dies sévères ou chroniques (psoriasis, maladies bulleuses, érythrodermies, lymphomes, etc.) qui nécessitent des
contrôles biologiques rapprochés et un examen complet de la peau à chaque consultation.
• Avec 30 minutes de consultation par tri-mestre, il sera aussi impossible de suivre de manière rapprochée et optimale cer-tains patients à hauts risques de cancers cutanés. De plus, Il sera impossible d’exa-miner un patient entre deux contrôles, s’il présente une lésion suspecte de mé-lanome, tumeur agressive dont le déve-loppement peut être foudroyant. Ces patients seront dirigés dans un centre hospitalier avec des délais d’attente qui seront de plus en plus longs, souffriront d’une prise en charge retardée avec un risque de développer une maladie plus avancée ayant un impact évident sur la diminution d’espérance de vie du patient ainsi que des coûts de prise en charge évidemment bien plus impor-tants, ce qui va totalement à l’encontre du but visé.
• La limitation des positions de temps de consultation (00.0020) ne permet plus de prendre en charge les pathologies complexes qui nécessitent des anam-nèses très complètes et des enquêtes pour parvenir à déterminer les origines de réactions cutanées (patient avec polypathologies et polymédiqués, en-quêtes allergologiques, etc.).
• L’abaissement des valeurs des presta-tions pour les interventions chirurgi-cales complexes ne permet plus leur exécution en cabinet privé, car les va-leurs ne permettent plus la couverture des frais des infrastructures nécessaires et donc leur maintien à niveau. Il est to-talement erroné de penser que les actes chirurgicaux puissent être réalisés dans des temps plus courts qu’il y a 20 ou 30 ans. C’est exactement le contraire qui se produit, puisque les formations sont plus poussées et qu’elles permettent des interventions plus importantes chez des patients de plus en plus âgés. L’âge, net-tement plus avancé des patients opérés, pose des problèmes d’installation du pa-tient sur la table d’opération, nécessitant un personnel plus nombreux et expéri-menté. Par ailleurs, le nombre croissant de patients sous traitement anticoagu-lant occasionne des saignements per-opératoires nettement plus importants,
Prise de position du Groupe des Dermatologues Genevois
(GDG) sur la fixation et l’adaptation du tarif dans l’assurance
maladie (TarMed) annoncées le 22 mars 2017 par le Conseiller
fédéral Alain Berset
16 Dermatologica Helvetica – Volume 29(7) – Septembre 2017

Referenzen1. Gordon K et al. Long-term effi cacy and safety of adalimumab in patients with moderate to severe psoriasis treated continuously over 3 years: results from an open-label extension study for patients from REVEAL. J Am Acad Dermatol. 2012;66(2):241-251. 2. Menter A et al. Adalimumab therapy for moderate to severe psoriasis: a randomized, controlled phase III trial. J Am Acad Dermatol.2008;58(1):106-115. 3. Poulin Y et al. Effi cacy of adalimumab across subgroups of patients with moderate-to-severe chronic plaque psoriasis of the hands and/or feet: post hoc analysis of REACH. JEADV 2014;28:882-890. 4. Mease PJ et al. Adalimumab for long-term treatment of psoriatic arthritis: 2-year data from the Adalimumab Eff ectiveness in Psoriatic Arthritis Trial (ADEPT). Ann Rheum Dis. 2009;68(5):702-709. 5. Mease PJ et al. Eff ectiveness in Psoriatic Arthritis Trial Study Group. Adalimumab for the treatment of patients with moderately to severely active psoriatic arthritis: results of a double-blind, randomized, placebo-controlled trial. Arthritis Rheum. 2005;52(10):3279- 3289.
Humira® (Adalimumab): Z: Wirkstoff : Adalimumab. I: Erwachsene: mässig bis stark ausgeprägte aktive rheumatoide Arthritis (RA) mit unzureichendem Ansprechen auf krankheitsmodifi zierende Antirheumatika (DMARDs), in Monotherapie oder in Kombination mit Methotrexat (MTX) bzw. anderen DMARDs; kürzlich diagnostizierte (< 3 Jahre) MTX-naive Patienten mit mässig bis stark ausgeprägter RA, in Kombination mit MTX. Psoriasis-Arthritis (PsA) mit ungenügendem Ansprechen auf DMARDs, in Monotherapie oder Kombination mit DMARDs. Aktive ankylosierende Spondylitis (AS) mit unzureichendem Ansprechen auf herkömmliche Therapien. Morbus Crohn (MC) mit mässiger bis hoher Krankheitsaktivität mit unzureichendem Ansprechen auf herkömmliche Therapien, sowie ungenügendem Infl iximab Ansprechen/Unverträglichkeit. Mittelschwere bis schwere aktive Colitis Ulcerosa (UC) mit unzureichendem Ansprechen, Unverträglichkeit oder Kontraindikation von herkömmlichen Therapien. Mittelschwere bis schwere chronische Plaque Psoriasis (PsO) in Monotherapie, bei denen eine systemische Therapie oder eine PUVA-Therapie angezeigt ist. Aktive mittelschwere bis schwere Hidradenitis suppurativa (HS) mit unzureichendem Ansprechen auf systemische Antibiotikatherapie. Nicht-infektiöse intermediäre, posteriore oder Panuveitis (U) bei Kortikosteroid-Abhängigkeit oder unzureichendem Ansprechen auf Kortikosteroide oder Immunmodulatoren; nach anatomischem und funktionellem Verlauf in Kombination mit Kortikosteroiden oder Immunmodulatoren. Kinder und Jugendliche: Von 4 –17 Jahren, polyartikuläre juvenile idiopathische Arthritis (pJIA) mit ungenügendem Ansprechen/Intoleranz auf DMARDs, in Kombination mit MTX oder als Monotherapie (MTX Unverträglichkeit). Ab 6 Jahren mit schwerem aktivem MC, mit unzureichendem Ansprechen, Unverträglichkeit oder Kontraindikation auf konventionelle Therapien (Ernährungstherapie, Glukokortikoid und Immunsuppressivum). D: subkutane Injektion. Erwachsene: RA, AS, PsA: 40 mg alle zwei Wochen. MC, UC: 160 mg in Woche 0, 80 mg in Woche 2 und danach alle zwei Wochen 40 mg. Bei verminderter Wirkung in UC und RA, Dosisfrequenzerhöhung auf 40 mg wöchentlich möglich. PsO: 80 mg in Woche 0, 40 mg in Woche 1 und danach alle zwei Wochen 40 mg. HS: 160 mg in Woche 0, 80 mg in Woche 2 und 40 mg wöchentlich ab Woche 4. U: 80 mg in Woche 0, 40 mg in Woche 1 und danach alle zwei Wochen 40 mg. Kinder und Jugendliche: pJIA: 24 mg/m2 Körperoberfläche bis zu maximal 40 mg (Einzeldosis) alle zwei Wochen. MC: < 40 kg: 80 mg in Woche 0, 40 mg in Woche 2, gefolgt von 20 mg oder 10 mg alle zwei Wochen. ≥ 40 kg: 160 mg in Woche 0, 80 mg in Woche 2. Danach 40 mg oder 20 mg jede zweite Woche. KI: Überempfindlichkeit gegen Inhaltsstoffe, aktive Tuberkulose (TB), schwere Infektionen, mittelschwere bis schwere Herzinsuffizienz (NYHA Kl. III-IV). WH: Infektionen, einschliesslich opportunistische Infektionen, TB inkl. okulare TB, Syphilis und Hepatitis B Reaktivierung, neurologische Ereignisse einschliesslich demyelinisierende Störungen, allergische Reaktionen einschliesslich anaphylaktische Reaktionen, maligne Tumore inkl. intraokulare Lymphome, Immunsuppression, Impfungen, Lebendimpfungen, Lebendimpfungen bei Neugeborenen nach in utero Exposition, Herzinsuffi zienz, gleichzeitige Anwendung von biologischen DMARDs oder anderen TNF-Antagonisten, hämatologische Ereignisse, Auto-Antikörper, Anwendung in der Geriatrie. Interakt.: keine bekannt/nicht untersucht. SS: Empfängnisverhütung, Nutzen - Risiko Bewertung, Stillen für 5 Monate nach Behandlung nicht empfohlen. UAW: Reaktionen an der Injektionsstelle, Infektionen, Leukopenie, Kopfschmerz, Parästhesien, Benommenheit, Husten, Diarrhoe, Motilitätsstörungen, Abdominalschmerzen, entzündliche Darmerkrankung, oropharyngeale Schmerzen, Übelkeit, Erhöhung der Leberenzyme, Hautausschlag, Dermatitis, Pruritus, Arthritis, muskuloskelettale Schmerzen, Müdigkeit. P: 40 mg/0,4 ml: Eine Fertigspritze, ein vorgefüllter Injektor; 40 mg/0,8 ml: 2 Durchstechfl aschen mit Injektionslösung (pädiatrische Patienten) pro Packung. Abgabekategorie B. Kassenzulässig (exkl. U). Ausführliche Informationen siehe Arzneimittel-Fachinformation: www.swissmedicinfo.ch. (V6) Zulassungsinhaberin: AbbVie AG, Neuhofstrasse 23, 6341 Baar.
CHHUD170522 08/2017
HUMIRA® – Alltag möglich machen.4
Tun, was mir wichtig ist.
Starke Hautwirksamkeit
nutzen1,2,3
Umfassende Wirksamkeit
über die Haut hinaus
erleben4,5
HUMIRA® beim
1. Biologikum-Einsatz vertrauen
dont le traitement prend également plus de temps. Les interventions chez ces patients représentent un risque ac-cru d’accident et de complications pour les patients et les médecins. Finalement, les attentes des patients par rapport aux cicatrices ne cessent d’augmenter, ce qui demande au chirurgien d’utiliser des techniques chirurgicales de reconstruc-tion plus complexes et plus longues, qui nécessitent un suivi post opératoire et des soins plus importants.
• L’ensemble des patients cités ci-dessus devront être transférés dans des centres hospitaliers, où ils seront transférés dans les secteurs stationnaires, alors qu’ils au-raient pu être traités ambulatoirement, engendrant ainsi à terme des coûts to-taux bien supérieurs aux gains annon-cés par le Conseiller fédéral Alain Berset.
Ainsi, les mesures annoncées vont complète-ment à l’encontre du projet fédéral de Santé2020 qui prévoit de favoriser les soins ambulatoires par rapport aux soins stationnaires. On comprend aisément que le transfert des charges – inévi-tables pour les raisons ci-dessus – va décharger en partie les assurances mais qu’il va considéra-blement alourdir la facture des cantons et donc des impôts ; on saisit donc pourquoi le lobby des assureurs soutient l’ordonnance du Conseiller fédéral Alain Berset.
En résumé, les mesures en préparation sont ina-déquates car:
1. on peut prédire avec une grande certitude qu’elles n’auront aucune répercussion sur les primes d’assurance. En effet, on ne peut attendre d’une diminution de 0.1% des coûts de la maladie, qu’elle ait une influence quel-conque sur les primes;
2. elles auront un impact direct et important sur la qualité de la prise en charge des pa-tients et sur la qualité des soins, pourtant si chère au Conseiller fédéral Berset;
3. elles sont en contradiction avec la volonté de « Santé2020 » qui prévoit « l’ambulatoire avant le stationnaire »;
4. elles vont entraîner un bouleversement complet du système, un retour en arrière, avec des implications très sérieuses sur l’or-ganisation des services hospitaliers et un alourdissement des charges des cantons. Ces mesures vont naturellement peser très lourd sur l’organisation administrative et financière des cabinets de dermatologie, essentiellement pour les dermatologues qui ont orienté leur pratique sur la dermato-chirurgie ou sur les pathologies complexes;
5. elles représentent, dans leur présentation, une marque de mépris du Conseiller fédéral Alain Berset à l’égard du corps médical dans son ensemble;
6. elles sont basées sur un postulat inaccep-table qui considère les médecins comme seuls responsables de l’augmentation des coûts de la santé. Les médecins ne sauraient supporter les coûts engendrés par le vieil-lissement de la population, les progrès de
la médecine, qui ont permis, entre autres, durant les deux dernières décennies, le transfert des prestations du stationnaire vers l’ambulatoire, progrès que le Conseiller fédé-ral Berset voudrait maintenant annuler par la révision du tarif !
Dr Alexandre CampanelliPrésident du GDG
Dre Konstantine Buxtorf-FriedliMembre du comité
Dr Thomas GaudinMembre du comité
Dr Jean-Pierre GrilletMembre du comité
Dr Joachim KrischerMembre du comité
SG
DV
– S
SD
V
18 Dermatologica Helvetica – Volume 29(7) – Septembre 2017

myHEALTH und SGDV:
Ein starkes Team für den Hautratgeber
myHEALTH et la SSDV:
une équipe forte pour le Guide de la peau
SG
DV
– S
SD
V
Vor drei Jahren begann die partnerschaftliche Zusammenarbeit zwischen dem SGDV und myHEALTH. Heute ist das Magazin und Online-Medium Hautratgeber auf dem Schweizer Markt das führende Publikumsmagazin im Bereich Der-matologie. Der Hautratgeber bietet dem breiten Schweizer Publikum sowohl im jährlich erschei-nenden Magazin als auch online unter www.hautratgeber.ch aktuelle Informationen aus dem gesamten Fachgebiet der Dermatologie und Venerologie. Seine Inhalte entstehen in enger Kooperation mit Experten der Schweizerischen Gesellschaft für Dermatologie und Venerologie (SGDV) sowie weiteren Partnern aus angrenzen-den Disziplinen. Versierte Journalisten bereiten die Texte verständlich und anschaulich auf, um eine große Zielgruppe ansprechen zu können. Wir sprachen mit Prof. Dr. med. Hafner, dem Past President der SGDV, und Sabine Swigulski, die das Projekt seitens myHEALTH leitet.
Kai Kaufmann: Welche Bedeutung hat für Sie die Kooperation von SGDV und myHEALTH?Prof. Hafner: Für uns als Fachgesellschaft ist das eine hervorragende Chance, unsere fachlichen Informationen auf einem seriösen medialen Ka-nal einem Laien-Publikum zugänglich zu ma-chen. S. Swigulski: Die Zusammenarbeit mit dem SGDV bildet das starke Fundament des Hautratgebers. Es ermöglich zum einen den Zugang zu füh-renden Experten aus der Praxis und Forschung, zudem versendet der Verband die Magazine an all seine Mitglieder und bietet an, diese auch ko-stenfrei nachzubestellen. Somit sind wir direkt beim Leser in den Wartezimmern.
Kai Kaufmann: Die Artikel des Hautratgebers ba-sieren auf Interviews mit Experten der SGDV. Die-se Form der Zusammenarbeit stellt für myHEALTH die fachliche Qualität und Aktualität der Inhalte des Magazins und der Online-Plattformen sicher. Prof. Hafner: Richtig, unsere anerkannt qualifi-zierten Spezialisten lesen die myHEALTH-Texte gegen und autorisieren schliesslich die Inhalte. Insgesamt ist es für die SGDV und myHEALTH also eine Win-Win-Situation.S. Swigulski: Durch die Experten an unserer Seite haben wir immer die Gewissheit, dass im Haut-ratgeber dem Leser absolut valide Inhalte ange-boten werden. In Zeiten von "Dr. Google" ist es für Nutzer schwer zu filtern, welche Informatio-nen fachlich wirklich verlässlich sind. Es war von Beginn an unser Ziel, sowohl auf der Website als
La collaboration entre la SSDV et myHEALTH a débuté il y a trois ans. Aujourd'hui, le Guide de la peau est le premier magazine de derma-tologie destiné au grand public. Le Guide de la peau fournit au public suisse les dernières informations en dermatologie et en vénéréolo-gie, en version papier annuelle ou en ligne, à l'adresse www.guide-de-la-peau.ch. Ses conte-nus sont rédigés en étroite collaboration avec des experts de la Société Suisse de Dermatolo-gie et Vénéréologie (SSDV) et des partenaires d’autres disciplines. Des journalistes spéciali-sés rédigent les textes de manière compréhen-sible et synthétique pour atteindre un vaste public. Nous nous sommes entretenus avec le Prof Dr med. Hafner, ancien président de la SSDV, et avec Sabine Swigulski, responsable du projet pour myHEALTH.
Kai Kaufmann: Quelle est pour vous l'impor-tance de la coopération entre la SSDV et myHEALTH ?Prof Hafner: Pour notre société spécialisée, c'est une opportunité formidable de mettre nos informations spécialisées à disposition du grand public, à travers un canal sérieux. S. Swigulski: La collaboration avec la SSDV est la clé de voûte du Guide de la peau. Elle nous permet d'accéder à des spécialistes re-nommés dans les domaines cliniques et de la recherche et elle transmet le magazine à tous ses membres, en leur permettant de se réap-provisionner gratuitement. Nous sommes ainsi directement à disposition des lecteurs, dans les salles d'attente.
Kai Kaufmann: Les articles du Guide de la peau se fondent sur des entretiens avec des experts de la SSDV. Cette forme de collaboration per-met à myHEALTH d'assurer la qualité profes-sionnelle des contenus du magazine et de la plateforme en ligne. Prof Hafner: C'est vrai, nos spécialistes quali-fiés reconnus relisent et approuvent les textes de myHealth. Dans l'ensemble, c'est une situa-tion win-win pour la SSDV et myHEALTH.S. Swigulski: La présence de spécialistes à nos côtés nous permet de toujours offrir à nos lec-teurs des contenus valides. En cette époque de "Dr Google", les utilisateurs ont du mal à filtrer les informations réellement fiables du point de vue médical. Dès le début, notre objectif était de travailler avec des partenaires disposant de connaissances approfondies et se portant
Dermatologica Helvetica – Volume 29(7) – Septembre 2017 19
SG
DV
– S
SD
Vauch später im Magazin, mit Partnern zu arbei-ten, die ein äußerst fundiertes Wissen haben und mit Ihrem Namen für die Inhalte einstehen.
Kai Kaufmann: Herr Prof. Hafner, die Website der SGDV richtet sich primär an Fachärzte für Derma-tologie. Gibt es dort auch Informationen für Pa-tienten?Prof. Hafner: Es gibt eine ganze Patienten-Rubrik. Patienten erfahren hier zum Beispiel, wo sie in ih-rer Region einen Dermatologen finden. Künftig wird es auch einen Link zum myHEALTH-Portal geben. Auf diesem Weg können wir den Nutzern unserer Website fachlich wertvolle Infos anbie-ten.
Kai Kaufmann: Frau Swigulski, dank der Zusam-menarbeit zwischen myHEALTH und dem SGDV hat sich ein großes Netzwerk bilden können. S. Swigulski: Es macht wirklich Freude zu sehen, wie viele Partner über die Jahre dazugekommen sind. Dazu zählen nicht allein die medinform HAUTapotheken, welche die Magazine gezielt mitverteilen, sondern auch weitere Verbände und Organisationen wie der SPVG, aha! Schweiz, die Rheumaliga, der SPV, die SGML, die SSP, der Verein für Hautkrebsforschung oder auch gynea. Es zeigt, welches Netz wir heute mit dem Hautrat-geber spannen können – es vereint die Leser bzw. Betroffenen, Disziplinen und Experten. Wir alle arbeiten Seite an Seite für ein gemeinsames Ziel. Nur so konnten wir es schaffen, das bedeutend-ste Publikumsmagazin im Bereich Dermatologie im Schweizer Markt zu werden.
Infobox Hautratgeber:• Schweizweites Publikumsmagazin zum The-
ma Dermatologie• Dreisprachig• Auflage: 145‘000 Stück• Spannende Mischung der Verteilung (von
der Schalterabgabe in der Post bis zum War-tezimmer sowie an verschiedenen Veranstal-tungen)
• Kooperation mit vielen Verbänden und Or-ganisationen – Hauptpartner SGDV
Links im Internet:www.derma.chwww.hautratgeber.ch
garants des contenus par leur signature, tant sur le site Web que, par la suite, dans le maga-zine.
Kai Kaufmann : Professeur Hafner, le site Web de la SSDV est principalement destiné aux der-matologues. Contient-il également des infor-mations pour les patients ?Prof Hafner: Une partie du site est destinée aux patients. Ils peuvent par exemple recher-cher un dermatologue dans leur région. Le site contiendra également un lien au portail myHEALTH. Ceci nous permettra d'offrir à nos visiteurs des informations spécialisées de qua-lité.
Kai Kaufmann: Madame Swigulski, grâce à la collaboration entre myHEALTH et la SSDV, un réseau étendu a été mis en place. S. Swigulski: C'est très gratifiant de voir le nombre de partenaires nous ayant rejoint au fil des ans. Non seulement les medinform HAUTapotheken, qui distribuent le magazine de manière ciblée, mais aussi d'autres associa-tions dont la SSPV, aha ! Suisse, la Ligue suisse contre le rhumatisme, la Société suisse des podologues, la SGML, la Société Suisse de Phlébologie, la Verein für Hautkrebsforschung ou gynea. Nous savons que nous pouvons aujourd'hui atteindre un vaste réseau avec le Guide de la peau, qui réunit les lecteurs et les personnes concernées, les disciplines et les experts. Nous travaillons côte à côte pour un objectif commun. C'est ainsi que nous sommes devenus le magazine de dermatologie grand public le plus important en Suisse.
Infobox Guide de la peau :• Magazine de dermatologie grand public
diffusé dans toute la Suisse• Trilingue• Publié à 145'000 exemplaires• Un mélange réussi des modes de distribu-
tion (de la remise au guichet à la poste aux salles d'attentes et lors de différents évé-nements)
• Coopération avec de nombreuses associa-tions – Partenaire principal: SSDV
Liens Internet:www.derma.chwww.guide-de-la-peau.ch
20 Dermatologica Helvetica – Volume 29(7) – Septembre 2017
Jahresmagazin 2017/2018
IHRGRATIS- EXEMPLARHautratgeberAkne
Seite 14
Sonnenschutz
Seite 24
Haarausfall
Seite 34
Haut und Laser
Seite 46
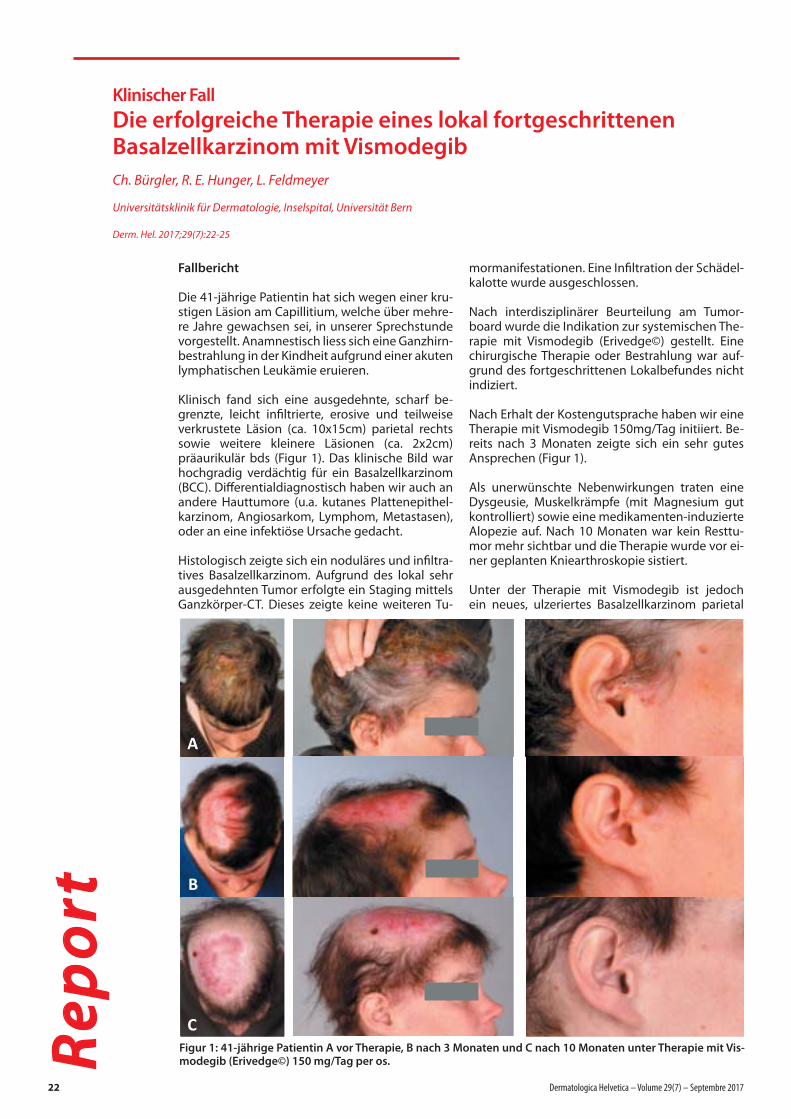
Klinischer Fall
Die erfolgreiche Therapie eines lokal fortgeschrittenen Basalzellkarzinom mit Vismodegib
Ch. Bürgler, R. E. Hunger, L. Feldmeyer
Universitätsklinik für Dermatologie, Inselspital, Universität Bern
Derm. Hel. 2017;29(7):22-25
Re
po
rt
Fallbericht Die 41-jährige Patientin hat sich wegen einer kru-stigen Läsion am Capillitium, welche über mehre-re Jahre gewachsen sei, in unserer Sprechstunde vorgestellt. Anamnestisch liess sich eine Ganzhirn-bestrahlung in der Kindheit aufgrund einer akuten lymphatischen Leukämie eruieren.
Klinisch fand sich eine ausgedehnte, scharf be-grenzte, leicht infi ltrierte, erosive und teilweise verkrustete Läsion (ca. 10x15cm) parietal rechts sowie weitere kleinere Läsionen (ca. 2x2cm) präaurikulär bds (Figur 1). Das klinische Bild war hochgradig verdächtig für ein Basalzellkarzinom (BCC). Diff erentialdiagnostisch haben wir auch an andere Hauttumore (u.a. kutanes Plattenepithel-karzinom, Angiosarkom, Lymphom, Metastasen), oder an eine infektiöse Ursache gedacht.
Histologisch zeigte sich ein noduläres und infi ltra-tives Basalzellkarzinom. Aufgrund des lokal sehr ausgedehnten Tumor erfolgte ein Staging mittels Ganzkörper-CT. Dieses zeigte keine weiteren Tu-
mormanifestationen. Eine Infi ltration der Schädel-kalotte wurde ausgeschlossen.
Nach interdisziplinärer Beurteilung am Tumor-board wurde die Indikation zur systemischen The-rapie mit Vismodegib (Erivedge©) gestellt. Eine chirurgische Therapie oder Bestrahlung war auf-grund des fortgeschrittenen Lokalbefundes nicht indiziert.
Nach Erhalt der Kostengutsprache haben wir eine Therapie mit Vismodegib 150mg/Tag initiiert. Be-reits nach 3 Monaten zeigte sich ein sehr gutes Ansprechen (Figur 1).
Als unerwünschte Nebenwirkungen traten eine Dysgeusie, Muskelkrämpfe (mit Magnesium gut kontrolliert) sowie eine medikamenten-induzierte Alopezie auf. Nach 10 Monaten war kein Resttu-mor mehr sichtbar und die Therapie wurde vor ei-ner geplanten Kniearthroskopie sistiert.
Unter der Therapie mit Vismodegib ist jedoch ein neues, ulzeriertes Basalzellkarzinom parietal
Figur 1: 41-jährige Patientin A vor Therapie, B nach 3 Monaten und C nach 10 Monaten unter Therapie mit Vis-modegib (Erivedge©) 150 mg/Tag per os.
22 Dermatologica Helvetica – Volume 29(7) – Septembre 2017
Gekürzte Fachinformation Stelara®: Stelara® (Ustekinumab, humaner monoklonaler IgG1 -Antikörper) I:Plaque-Psoriasis: Behandlung erwachsener Patienten mit mittelschwerer bis schwerer Plaque-Psoriasis, bei denen andere system-
ische Therapien einschliesslich Ciclosporin, Methotrexat oder PUVA nicht angesprochen haben, kontraindiziert sind oder nicht vertragen wurden. Psoriasis-Arthritis: Behandlung erwachsener Patienten mit aktiver Psoriasis Arthritis, als
Monotherapie oder in Kombination mit MTX, wenn das Ansprechen auf eine vorhergehende Therapie mit DMARDs unzureichend gewesen ist. Stelara® verbessert die körperliche Funktionsfähigkeit bei Patienten mit Psoriasis-Arthritis.
D: Die Anw. sollte unter Anleitung und Aufsicht eines in Diag. und Beh. der Psoriasis erfahrenen Arztes erfolgen. PsO: Erw. ab 18 Jahren: 45 mg als s.c. Injektion Woche 0, 4, anschliessend alle 12 Wochen. Pat > 100 kg: 90 mg.
PsA: Erw. 45 mg als s.c. Injektion Woche 0, 4, anschliessend alle 12 Wochen. Bei ungenügendem Ansprechen kann die Dosis auf 90 mg gesteigert werden. Kein Ansprechen nach 28 Wochen: Therapie absetzen. KI: Schwerwieg-
ende Überempfindlichkeit gegenüber dem Wirkstoff oder einem der Hilfsstoffe. VM: Vor Verabreichung von Stelara® soll der behandelnde Arzt die ärztespez. Firmeninformation zum Produkt, insbesondere zu den pot. Risiken, gelesen
haben. Zudem soll er sicherstellen, dass der Pat. die pot. Risiken, die in der Patbroschüre und der Patientenkarte aufgeführt sind, verstanden hat. Infektionen: Stelara® darf Patienten mit einer klinisch bedeutsamen, aktiven Infek-
tion nicht verabreicht werden. TB: Abklärung auf TB-Infektion vor Therapiestart. Einleitung antituberkulöse Therapie bei latenter TB vor Therapiestart. Reversibles posteriores Leukoenzephalopathie Syndrom. Maligne Tumoren. Über-
empfindlichkeitsreaktionen (einschliesslich Anaphylaxie und Angioödem). Immunisierungen: Keine Verabreichung von Lebendimpfstoffen während der Behandlung mit Stelara®. Kombination mit immunsuppressiver Begleittherapie,
Phototherapie, intensive Sonnenbestrahlung vermeiden. Immuntherapie. Schwerwiegende Hautreaktionen: Im Rahmen der Psoriasis-Kontrolluntersuchungen auf Symptome einer erythrodermischen Psoriasis bzw. exfoliativen Derma-
titis achten, bei Verdacht auf Arzneimittelreaktion Stelara® Therapie absetzen. UAW: Infektion der oberen Atemwege, Nasopharyngitis, Dentalinfektionen, Schwindel, Kopfschmerzen, Schmerzen im Mundrachenraum, Diarrhoe, Erbre-
chen, Juckreiz, Rückenschmerzen, Muskelschmerzen, Arthralgie, Erschöpfung, Erythem und/oder Schmerzen an der Injektionsstelle. IA: Es wurden keine Wechselwirkungsstudien durchgeführt. Sicherheit und Wirksamkeit von Stelara® in Kombination mit immunsuppressiven Wirkstoffen oder Phototherapie wurden nicht untersucht. SS: Stelara® darf in der Schwangerschaft nur angewendet werden, wenn klar notwendig. Bei der Entscheidung über eine Beendigung des
Stillens oder ein Absetzen der Stelara® Therapie, sollte der Nutzen des Stillens für das Kind und der Nutzen der Stelara® -Therapie für die Mutter berücksichtigt werden. - Packungen: Stelara® Injektionslösung in Fertigspritze, 45 mg
(0,5 ml) bzw. 90 mg (1 ml). Kassenzulässig. Abgabekat.: B. Ausführliche Informationen: www.swissmedic.ch oder www.swissmedicinfo.ch; Zulassungsinhaberin: Janssen-Cilag AG, Gubelstrasse 34, 6300 Zug (PHCH/MDMK/0915/0002)
ZEIG DICH!1
ain der Erhaltungstherapie
1. Leonardi C.L. et al., Efficacy and safety of ustekinumab, a human interleukin-12/23 monoclonal antibody, in patients with
psoriasis: 76-week results from a randomized, double-blind, placebo-controlled trial (PHOENIX 1), Lancet 2008; 371: 1665-74.
2. Fachinformation STELARA® (Mai 2015) unter www.swissmedicinfo.ch (aufgerufen am 09.11.2016).
3. Menter A. et al., Drug survival of biologic therapy in a large, disease-based registry of patients with psoriasis: results from the
Psoriasis Longitudinal Assessment and Registry (PSOLAR), Eur Acad Dermatol Venerol 2016; 30: 1148-58.
Langfristige Erfolge in der Therapie von Plaque-Psoriasie mit nur 4 Injektionen pro Jahr a,2,3
PHALP/STE/1216/0001

Re
po
rt
rechts aufgetreten. Dieses wurde in Lokalanästhe-sie exzidiert. Seither ist die Patientin trotz zahlrei-cher Auff orderungen nicht mehr zur Verlaufskon-trolle erschienen.
Diskussion
Der Goldstandard zur Therapie des unkomplizier-ten Basalzellkarzinom ist die chirurgische Exzision. Alternative Therapieoptionen sind die Kryothe-rapie, Radiotherapie, Photodynamische Therapie oder Behandlung mittels Imiquimod oder 5-FU [1]. Bei lokal fortgeschrittenem oder metastasieren-dem Basalzellkarzinom ist unter Umständen eine chirurgische Behandlung oder Strahlentherapie nicht möglich. In diesem Fall ist eine Therapie mit einem Hedgehog Signalweg Inhibitor indiziert.
Der Hedgehog Signalweg ist essentiell für das Zell-wachstum und die Diff erenzierung in der embryo-logischen Entwicklung. Im adulten Gewebe ist der Hedgehog Signalweg weitgehend inaktiviert. BCC sind assoziiert mit pathogenetisch relevanten Mutationen im Hedgehog Signalweg welche zu einer Reaktivierung und so zum ungebremsten Zellwachstum führen (Figur 2) [2]. Zurzeit sind 2 verschiedene Hedgehog Signalweg Inhibitoren (HPI) auf dem Markt, Vismodegib (Erivedge©) und Sonidegib (Odomzo©), wobei in der Schweiz bis-her nur Vismodegib zur Behandlung von erwach-senen Patienten mit fortgeschrittenem BCC zuge-lassen ist.
Vismodegib und Sonidegib sind kompetitive Ant-agonisten vom smoothened Rezeptor (SMO). Die Hemmung des SMO führt zu einer Inaktivität der Transkriptionsfaktoren GLI1 und GLI2 und hemmt so die Expression von Genen des Hedgehog Si-gnalwegs, welche Proliferation und Diff erenzie-rung beeinfl ussen [3].
Bisherige Studien haben Ansprechraten (partiel-les und komplettes Ansprechen) von 43 - 64% für lokal fortgeschrittene BCC resp. 30 - 48% für meta-
stasierte BCC gezeigt [4-6]. Etwa 20% der Patien-ten entwickeln eine Therapieresistenz gegenüber Vismodegib im ersten Behandlungsjahr, welche hauptsächlich durch eine Mutation der Zielstruk-tur am SMO zustande kommt [7]. Der bei unserer Patientin während der Therapie neu aufgetretene Tumorknoten ist mit hoher Wahrscheinlichkeit auf die Entwicklung einer Resistenz zurückzuführen. Die Kosten einer Therapie mit 150mg Vismodegib p.o. pro Tag belaufen sich auf rund CHF 8000.-/Monat. In den Zulassungsstudien wurden die Pati-enten über 12 Monate behandelt. Ob kürzere The-rapiezeiten oder auch Interwalltherapien möglich sind, kann zur Zeit nicht abschliessend beurteilt werden, hierfür sind weitere Studien notwen-dig. Die häufi gsten Nebenwirkungen (NW) einer Therapie mit Vismodegib sind Muskelkrämpfe, Dysgeusie (frühe NW) und eine Alopezie (spä-te NW) [8]. Daneben können Diarrhoe, Übelkeit, Müdigkeit und Gewichtsverlust auftreten, zuletzt wurden zudem Amenorrhoe und ein erhöhtes Ri-siko für Plattenepithelkarzinom beschrieben [6,9]. Alle Nebenwirkungen sind nach Therapiestopp reversibel. Die Muskelkrämpfe lassen bereits we-nige Tage nach Absetzen des Medikaments nach, bis zur Erholung des Geschmackssinn dauert es in der Regel 1-2 Monate [10]. Aufgrund der wichti-gen Bedeutung des Hedgehog Signalweg in der Embryogenese ist eine Therapie mit Vismode-gib oder Sonidegib teratogen und bedingt eine doppelte Kontrazeption bis 24 Monate nach The-rapieschluss für Frauen resp. eine Verhütung mit Kondom bis 2 Monate nach Therapieschluss bei Männern.
Zusammenfassung
Wir berichten über die erfolgreiche Behandlung einer Patientin mit einem lokal fortgeschrittenen Basalzellkarzinom mit dem Hedgehog Signalweg Inhibitor Vismodegib. • HPI sind indiziert zur Behandlung von er-
wachsenen Patienten mit lokal fortgeschritte-nem oder metastasiertem Basalzellkarzinom,
Figur 2: Schematische Darstellung des Hedgehog-Signalweg (aus [3]). Im normalen Gewebe ist der Hedgehog-Signalweg durch die hemmende Wirkung des patched Rezeptor (PTCH1) auf den smoothened Rezeptor (SMO) inhibiert. Die Bindung eines Liganden am PTCH1 führt über eine fehlende Hemmung des SMO zur Aktivierung des Hedgehog-Signalweg. Eine Mutation des PTCH1 (wie bei den meisten BCC oder dem Gorlin-Goltz-Syndrom der Fall) oder SMO führt durch die wegfallende Hemmung zu einer Ligand-unabhängigen Aktivierung des SMO, zur Aktivierung des Transkriptionsfaktors GLI und über die Transkription multipler Zielgene zum unkon-trollierten Zellwachstum. Die Hedgehog-Signalweg Inhbitoren Vismodegib und Sonidegib wirken als kompe-titive Antagonisten am SMO.
24 Dermatologica Helvetica – Volume 29(7) – Septembre 2017
Re
po
rt
für die eine chirurgische Behandlung oder Strahlentherapie nicht in Betracht kommt. Multiple BCC im Rahmen von Erbkrankheiten, insb. beim Gorlin-Goltz-Syndrom, werden ebenfalls erfolgreich mit Vismodegib behan-delt [11].
• Alle Nebenwirkungen, wovon Muskelkrämp-fe, Dysgeusie und Alopezie am häufigsten auftreten, sind reversibel. Sie können die Le-bensqualität des Patienten jedoch stark be-einträchtigen und sind deshalb oft der Grund für einen Therapieabbruch.
• Aufgrund der Teratogenität ist auf eine kon-sequente Antikonzeption zu achten. Unter Therapie sind regelmässige klinische und la-borchemische Kontrollen indiziert [10].
• Die Therapiedauer ist noch nicht abschlies-send definiert, hierfür sind weitere Studien notwendig.
• Vor Therapiebeginn muss eine Kostengut-sprache eingeholt werden.
References
1. Trakatelli M, Morton C, Nagore E et al. Update of the European guidelines for basal cell carcinoma management. Eur J Dermatol 2014; 24: 312-329
2. Scales SJ, de Sauvage FJ. Mechanisms of Hedgehog pathway activation in cancer and implications for therapy. Trends Pharmacol Sci 2009; 30: 303-312
3. Dlugosz A, Agrawal S, Kirkpatrick P. Vismodegib. Nat Rev Drug Discov 2012; 11: 437-438
4. Von Hoff DD, LoRusso PM, Rudin CM et al. Inhibiti-on of the hedgehog pathway in advanced basal-cell carcinoma. N Engl J Med 2009; 361: 1164-1172
5. Sekulic A, Migden MR, Lewis K et al. Pivotal ERI-VANCE basal cell carcinoma (BCC) study: 12-month update of efficacy and safety of vismodegib in ad-vanced BCC. J Am Acad Dermatol 2015; 72: 1021-1026 e1028
6. Jacobsen AA, Aldahan AS, Hughes OB et al. Hedge-hog Pathway Inhibitor Therapy for Locally Advan-ced and Metastatic Basal Cell Carcinoma: A Syste-matic Review and Pooled Analysis of Interventional Studies. JAMA Dermatol 2016; 152: 816-824
7. Sharpe HJ, Pau G, Dijkgraaf GJ et al. Genomic analy-sis of smoothened inhibitor resistance in basal cell carcinoma. Cancer Cell 2015; 27: 327-341
8. Chang AL, Solomon JA, Hainsworth JD et al. Expan-ded access study of patients with advanced basal cell carcinoma treated with the Hedgehog pa-thway inhibitor, vismodegib. J Am Acad Dermatol 2014; 70: 60-69
9. Mohan SV, Chang J, Li S et al. Increased Risk of Cuta-neous Squamous Cell Carcinoma After Vismodegib Therapy for Basal Cell Carcinoma. JAMA Dermatol 2016; 152: 527-532
10. Nägeli MC DR. Vismodegib (Erivedge©). Schweiz Med Forum 2014; 14: 284-286
11. Tang JY, Ally MS, Chanana AM et al. Inhibition of the hedgehog pathway in patients with basal-cell nevus syndrome: final results from the multicen-tre, randomised, double-blind, placebo-controlled, phase 2 trial. Lancet Oncol 2016; 17: 1720-1731.
Dermatologica Helvetica – Volume 29(7) – Septembre 2017 25
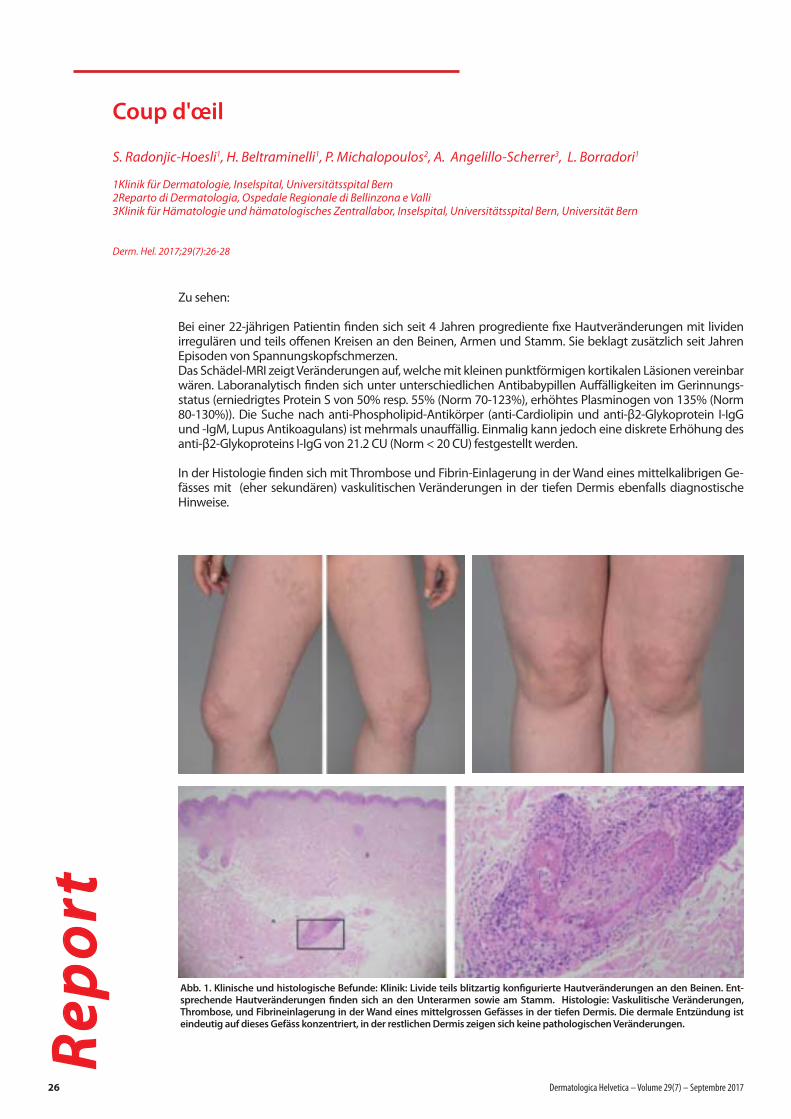
Coup d'œil
S. Radonjic-Hoesli1, H. Beltraminelli1, P. Michalopoulos2, A. Angelillo-Scherrer3, L. Borradori1
1Klinik für Dermatologie, Inselspital, Universitätsspital Bern2Reparto di Dermatologia, Ospedale Regionale di Bellinzona e Valli3Klinik für Hämatologie und hämatologisches Zentrallabor, Inselspital, Universitätsspital Bern, Universität Bern
Derm. Hel. 2017;29(7):26-28
Re
po
rt
Zu sehen:
Bei einer 22-jährigen Patientin fi nden sich seit 4 Jahren progrediente fi xe Hautveränderungen mit lividen irregulären und teils off enen Kreisen an den Beinen, Armen und Stamm. Sie beklagt zusätzlich seit Jahren Episoden von Spannungskopfschmerzen.Das Schädel-MRI zeigt Veränderungen auf, welche mit kleinen punktförmigen kortikalen Läsionen vereinbar wären. Laboranalytisch fi nden sich unter unterschiedlichen Antibabypillen Auff älligkeiten im Gerinnungs-status (erniedrigtes Protein S von 50% resp. 55% (Norm 70-123%), erhöhtes Plasminogen von 135% (Norm 80-130%)). Die Suche nach anti-Phospholipid-Antikörper (anti-Cardiolipin und anti-β2-Glykoprotein I-IgG und -IgM, Lupus Antikoagulans) ist mehrmals unauff ällig. Einmalig kann jedoch eine diskrete Erhöhung des anti-β2-Glykoproteins I-IgG von 21.2 CU (Norm < 20 CU) festgestellt werden.
In der Histologie fi nden sich mit Thrombose und Fibrin-Einlagerung in der Wand eines mittelkalibrigen Ge-fässes mit (eher sekundären) vaskulitischen Veränderungen in der tiefen Dermis ebenfalls diagnostische Hinweise.
Abb. 1. Klinische und histologische Befunde: Klinik: Livide teils blitzartig konfi gurierte Hautveränderungen an den Beinen. Ent-sprechende Hautveränderungen fi nden sich an den Unterarmen sowie am Stamm. Histologie: Vaskulitische Veränderungen, Thrombose, und Fibrineinlagerung in der Wand eines mittelgrossen Gefässes in der tiefen Dermis. Die dermale Entzündung ist eindeutig auf dieses Gefäss konzentriert, in der restlichen Dermis zeigen sich keine pathologischen Veränderungen.
26 Dermatologica Helvetica – Volume 29(7) – Septembre 2017
Psoriasis am Körper Psoriasis du corps
Ich möchte / Je souhaite
Mehr Informationen per E-Mail* erhalten / recevoir plus d’informations par e-mail*
E-Mail*:
von einem LEO Aussendienstmitarbeiter kontaktiert werden / être contacté par un délégué médical de LEO
Tel:
Bitte ausgefüllt mit Unterschrift zurückschicken /à renvoyer SVP signé: Fax 043 343 75 70 /E-Mail [email protected]
* J’autorise LEO Pharma à me faire parvenir à cette adresse e-mail du matériel d’information sur le thème dermatologie, des invitations à des formations en dermatologie, des informations sur les produits et services de LEO Pharma. Il est possible à tout moment et avec un effet immédiat, d’éliminer cette adresse e-mail de la liste de distribution par une simple demande informelle adressée à [email protected].
* Ich berechtige LEO Pharma, mir Informationsmaterial zum Thema Dermatologie, Einladungen zu Dermatologie-Fortbildungen und Informationen über Produkte und Dienstleistungen von LEO Pharma an diese E-Mail-Adresse zuzustellen. Eine Entfernung aus diesem E-Mail-Verteiler ist jederzeit mit sofortiger Wirkung durch ein formloses E-Mail an [email protected] möglich.
Innovation:
Schaumspray für den Körper
Spray mousse pour le corps
Stempel / UnterschriftTampon / Signature
www.enstilar.ch
Gekürzte Fachinformation ENSTILAR® SCHAUMZusammensetzung: 1 g Schaum enthält 0.05 mg Calcipotriol und 0.5 mg Betamethason in Form von Betamethasondipropionat. Indikationen: Psoriasis vulgaris bei Erwachsenen. Dosierung: 1x täglich, max. 100 g/Woche bzw. 15 g/Tag. Empfohlene Behandlungsdauer: Nicht länger als 4 Wochen. Anwendung: Dose vor Gebrauch schütteln, mindestens 3cm entfernt von der Haut sprühen und sanft in die betroffenen Hautregionen einreiben. Kontraindikationen: Überempfindlichkeit gegen Inhaltsstoffe. Anwendung im Gesicht, insbesondere auf augennahen Hautarealen (Kataraktgefahr). Anwendung mit Okklusiv-Verbänden. Psoriasis guttata, erythrodermische, exfoliative und pustulöse Psoriasis. Bekannte Störungen des Calciumstoffwechsels. Infektionen mit Viren, Pilzen, Bakterien und Parasiten, Hautmanifestationen von Tuberkulose oder Syphilis, periorale Dermatitis, atrophische Haut, Dehnungsstreifen, erhöhte Fragilität der Hautvenen, Ichthyose, Akne vulgaris, Akne rosacea, Rosacea, Hautulzera, Wunden, perianaler und genitaler Pruritus. Schwere Niereninsuffizienz und schwere Leberfunktionsstörungen. Keine Anwendung bei Kindern, da noch keine Erfahrungen. Vorsichtsmassnahmen: Druckbehälter mit hochentzündlichem Inhalt. Explosionsgefahr bei Erhitzung. Von Funken/offenen Flammen fernhalten. Übertragen auf Gesicht, Mund oder Augen vermeiden, Hände nach Anwendung waschen. Behandlung von >30% der Körperoberfläche vermeiden. Bei einer Dosis von mehr als 100 g/Woche können Hypercalcämien nicht ausgeschlossen werden. Bei Dosisüberschreitung Kontrolle des Serumcalcium. Während der Therapie mit Enstilar® wird empfohlen, exzessive Bestrahlung mit natürlichem oder künstlichem Sonnenlicht zu begrenzen oder zu meiden. Eine gleichzeitige Behandlung mit anderen Kortikosteroiden sowie eine grossflächige oder okklusive Anwendung sollten vermieden werden (Suppression endogener Cortisolproduktion). Sorgfältige Therapieüberwachung empfohlen, da die Psoriasistherapie mit Kortikosteroiden ein gewisses Risiko eines Reboundeffektes, einer Toleranzentwicklung und einer Auslösung einer generalisierten Psoriasis pustulosa birgt. Unerwünschte Wirkungen: Gelegentlich: Follikulitis, Überempfindlichkeitsreaktionen (Urtikaria, Ödeme, Lippen- und Zungenschwellung oder Atembeschwerden), Hyperkalzämie, Hyperkalziurie, Hypopigmentierung der Haut, Exazerbation der Psoriasis, Rebound-Effekt, Hautschmerzen, Pruritus und Irritationen. Interaktionen: Nicht mit salicylsäurehaltigen Zubereitungen mischen, die Salicylsäure inaktiviert Calcipotriol. Salicylsäure bleibt auf der Hautoberfläche, so dass auch eine zeitlich versetzte Calcipotriol-Anwendung in der Wirkung vermindert sein kann. Packungen: Enstilar®: 1 Sprühdose (60* g) (Liste B); Stand der Information: April 2016. *Kassenzulässig.Ausführliche Informationen entnehmen Sie bitte der aktuellen Fachinformation auf www.swissmedicinfo.ch
LEO Pharmaceutical Products Sarath Ltd., Eichwatt 5, 8105 Regensdorf, Tel: 043 343 75 75 LEO® © LEO 03 2017 D/F - ALL LEO TRADEMARKS BELONG TO THE LEO GROUP - MAT-05596
Ref: 1. Fachinformation / Information professionnelle Enstilar®, www.swissmedicinfo.ch, 2. Koo J. et al., Superior efficacy of calcipotriene and betamethasone dipropionate aerosol foam versus ointment in patients with psoriasis vulgaris – A randomized phase II study. J Dermatolog Treat, 2016; 27(2): 120–1127. 3. Lebwohl M. et al., Fixed combination aerosol foam calcipotriene 0.005 % (Cal) plus betamethasone dipropionate 0.064 % (BD) is more efficacious than Cal or BD aerosol foam alone for psoriasis vulgaris. A randomized, doubleblind, multicenter, three-arm, phase 2 study. J Clin Aesthet Dermatol. 2016;9(2):34–41. 4. Leonardi C et al. Efficacy and Safety of Calcipotriene Plus Betamethasone Dipropionate Aerosol Foam in Patients With Psoriasis Vulgaris – a Randomized Phase III Study (PSO-FAST) J Drugs Dermatol 2015; 14: 1468–1477.
Enstilar®: nur 1x täglich für 4 Wochen1
Wirkt stark1, 2 – Wirkt schnell2, 3 – Wirkt spürbar4
Enstilar®: seulement 1x par jour pendant 4 semaines 1
Efficace1, 2 – Rapide2, 3 – Perceptible4

Re
po
rtEntzündliche Livedo reticualris bzw. Livedo race-mosa
Das vorliegende klinische Bild entspricht einer Live-do racemosa. Klinisch lässt sie sich von der Livedo reticularis (im deutschen Sprachraum) darin unter-scheiden, dass es sich bei der Livedo racemosa um eher fi xe netzförmigen Hautveränderungen mit ty-pischerweise irregulären und nicht geschlossenen Kreisen (siehe hierzu untenstehende Abbildungen) handelt. Diese zyanotische Hautzeichungen befal-len typischerweise auch die obere Körperpartien (Flanken, Rücken, Gesäss) und sind nicht (vollstän-dig) temperaturabängig.
In Anbetracht der Klinik und der Auff älligkeiten in der Hautbiopsie besteht der Verdacht, dass die neurologischen Beschwerden gemeinsam mit den sehr diskreten Veränderungen im Schädel-MRI in Zusammenhang mit einer gefässthrombosierenden Erkrankung stehen. Die Konstellation Livedo race-mosa mit zerebrovaskulären Veränderungen ist ver-einbar mit einem Sneddon Syndrom[1]. Eine retrospektive Datenanalyse von Patienten mit Sneddon Syndrom ohne positiven Antiphospholi-pid-Antikörpernachweis und Schlaganfall zeigte in den meisten Fällen das Auftreten der Livedo vor dem ersten zerebrovaskulären Ereignis auf[1]. Die Hälfte der Patienten gaben Kopfschmerzen und 25% Spannungskopfschmerzen an[1], wie bei vorliegen-der Patientin. Es ist gut möglich, dass die Seronegativität in vielen Fällen des seronegativen Antiphosholipidsyndroms die jetztigen technischen Limitationen bei fehlen-den adäquaten Suchtests und Kenntnis der Zielan-tigene wiederspiegelt. Die Präsenz von isolierten IgA anti-Phospholipidantikörpern[2], von Antikörpern gegen Domäne I des β2-Glykoprotein I[2], Phospha-tidylethanolamine[3,5], Prothrombin[4], Lyso(bis)phosphatidic Säure[5], und Annexin II[5], werden in Patienten mit seronegativem Antiphospholipidsyn-
drom zunehmend beschrieben. Ihre pathogeneti-sche Relevanz bleibt noch unklar. Die Therapie zielt auf eine Prävention thrombotischer Ereignisse ab. Die Zugabe von einer niedrigdosierten Warfarintherapie zu Aspirin hat bisher keinen Bene-fi t zur Thromboseprophylaxe in Patienten mit Anti-phospholipidsydrom gezeigt[6]. Die Zugabe von Hy-droxychloroquin kann ebenfalls evaluiert werden. In Antiphospholipid-Tiermodellen wurde bspw. aufge-zeigt, dass Hydroxychloroquin die Thrombusgrösse nach experimentell induzierter Gefässverletzung re-duzieren kann[7]. Oestrogen-haltige Kontrazeptiva sind bei Patientinnen mit Antiphospholipidsyndrom prinzipiell kontraindiziert[8]. Entsprechend der Indi-kation der Oestrogen-haltigen Kontrazeptiva, muss die Verabreichung im Gesamtkontext interdiziplinär mit Experten evaluiert werden.
Literatur 1. Bottin L, Francès C, de Zuttere D, Boëlle PY, Muresan
IP, Alamowitch S. Strokes in Sneddon Syndrome wit-hout Antiphospholipid antibodies. Ann Neurol 2015; 77: 817-29. doi: 10.1002/ana.24382.
2. Cousins L, Pericleous C, Khamashta M, Bertolaccini ML, Ioannou Y, Giles I, Rahman A. Antibodies to do-main I of beta-2-glycoprotein I and IgA antiphos-pholipid antibodies in patients with “seronegative” antiphospholipid syndrome. Ann Rheum Dis 2015; 74:317–19. doi: 10.1136/annrheumdis-2014-206483.
3. Narazaki H, Kaizu K, Kuwabara K, Fujino O, Itoh Y. Seronegative Antiphospholipid Syndrome with Anti-phosphatidylethanolamine Antibody in a Boy. J Nippon Med Sch 2015; 82:117-20. doi 10.1272/jnms.82.117.
4. Bertolaccini ML, Gomez S, Pareja JF, Theodoridou A, Sanna G, Hughes GR, Khamashta MA. Antiphospholi-pid antibody tests: spreading the net. Ann Rheum Dis 2005;64:1639-43. doi: 10.1136/ard.2005.035824.
5. Conti F, Alessandri C, Sorice M, Capozzi A, Longo A, Garofalo T, Misasi R, Bompane D, Hughes GR, Kha-mashta MA, Valesini G. Thin-layer chromatography immunostaining in detecting anti-phospholipid antibodies in seronegative anti-phospholipid syn-drome. Clin Exp Immunol 2012; 167:429-37. doi: 10.1111/j.1365-2249.2011.04532.x.
6. Cuadrado MJ, Bertolaccini ML, Seed PT, Tektonidou MG, Aguirre A, Mico L, Gordon C, Ruiz-Irastorza G, Egurbide MV, Gil A, Espinosa G, Houssiau F, Rahman A, Martin H, McHugh N, Galindo M, Akil M, Amigo MC, Murru V, Khamashta MA. Low-dose aspirin vs low-dose aspirin plus low-intensity warfarin in thrombo-prophylaxis: a prospective, multicentre, randomized, open, controlled trial in patients positive for antiphos-pholipid antibodies (ALIWAPAS). Rheumatology (Ox-ford) 2014; 53: 275-84. doi: 10.1093/rheumatology/ket313.
7. Scascia S, Branch DW, Levy RA, Middeldorp S, Pavord S, Roccatello D, Ruiz-Irastorza G, Tincani A, Khamashta M, Schreiber K, Hunt BJ. The effi cacy of hydroxychlo-roquine in altering pregnancy outcome in women with antiphospholipid antibodies. Evidence and cli-nical judgment. Thromb Haemost 2016; 115: 285–90. doi: 10.1160/TH15-06-0491.
8. Sammaritano LR. Lupus. Contraception in pati-ents with systemic lupus erythematosus and an-tiphospholipid syndrome. 2014; 23:1242-5. doi: 10.1177/0961203314528062.
28 Dermatologica Helvetica – Volume 29(7) – Septembre 2017
Abb. 2. Bildvergleich einer Livedo reticularis und der Livedo racemosa bei unserer Patientin. A. Das Bild zeigt mit geschlossenen lividen Kreise den klinischen Befund einer nicht entzündlichen Livedo reticularis auf. Typischerweise sind die Veränderungen nach Wärmeapplikation vollständig regredient. B. Die Nahaufnahme der Hautveränderungen am linken Oberschenkel bei unserer Patientin zeigt im Bildvergleich einen deutlichen Unterschied der Hautveränderun-gen in deren Verteilung und Regularität auf. Bildarchiv, Klinik für Dermatologie, Inselspiral, Universitätsspital Bern.
A B

SOOLANTRA®
. ULTRA-EFFICACE CONTRE LA ROSACÉE!1,2,3
NOUVEAU
Références : 1. Information professionnelle SOOLANTRA®, www.swissmedicinfo.ch. 2. Taieb A. et al.; Superiority of ivermectin 1 % cream over metronidazole 0.75 % cream in treating inflammatory lesions of rosacea: a randomized, investigator-blinded trial; Br J Dermatol., 172:1103–1110; 2015. 3. Stein Gold L. et al; Efficacy and Safety of Ivermectin 1 % Cream in Treatment of Papulopustular Rosacea: Results of Two Randomized, Double-Blind, Vehicle- Controlled Pivotal Studies; Journal of Drugs in Dermatology, 13(3):316–323; 2014. Information professionnelle abrégée: Soolantra® Crème: C: ivermectine 10 mg/g. Excipients: E216, E218, phénoxyéthanol; propylèneglycol; alcool cétylique; alcool stéarylique; excipiens ad unguentum. I: traitement externe des lésions inflammatoires en cas de rosacée papulopustuleuse moyennement sévère à sévère chez l’adulte. P: une fois par jour, habituellement jusqu’à 3 mois, répétition après évaluation du rapport bénéfice/risque individuel. Maximum 1 g/jour. CI: hypersensibilité à l’un des excipients. PC: Soolantra n’a pas été étudié chez les patients présentant une insuffisance rénale ou hépatique. Contient de l’alcool cétylique, de l’alcool stéarylique, du propylèneglycol qui peuvent provoquer des réactions cutanées locales ainsi que du parahydroxybenzoate de méthyle (E218), du parahydroxybenzoate de propyle (E216) qui peuvent provoquer des réactions allergiques éventuellement retardées. Soolantra ne doit pas être administré avec de puissants inhibiteurs de la P-gp et de CYP3A4 (p. ex. kétoconazole, itraconazole) ainsi qu’avec des substances à fenêtre thérapeutique étroite dont l’excrétion dépend largement de la P-gp (p. ex. digoxine, ciclosporine). La prudence est de mise en cas d’administration avec des inhibiteurs modérés de la P-gp et de CYP3A4. EI: Fréquents: sensation de brûlure cutanée. Occasionnels: irritation cutanée, prurit, sécheresse cutanée. G/A: éviter l’utilisation pendant la grossesse. Ne pas utiliser durant l’allaitement. E: tube de 30 g. Liste B, LS. Titulaire de l’autorisation: Galderma Suisse SA, 4622 Egerkingen. Plus d’informations sur www.swissmedicinfo.ch. Mise à jour: septembre 2016 (v001). Galderma Suisse SA, Froschackerstrasse 6, 4622 Egerkingen; Tél.: +41 62 387 88 00, Code: 1702-Soo-I-01, www.galderma.ch, www.rosacea-info.ch
SOOLANTRA®
Appliqué 1 x par jour, agit rapidement et efficacement
contre papules et pustules1,2,3
• Efficacité supérieure – vs 2 x par jour pour métronidazole 0.75 %1,2
• Anti-inflammatoire et anti-parasitaire – la double action d’ivermectine2,3
• Meilleure tolérance locale – qu’avec l’application 2 x / j de métronidazole 0.75 %2
(ivermectine) 10 mg/g crème
ADMIS PAR
LES CAISSES

Po
rtra
itPortrait Carolina Gouveia
Klinik für Dermatologie, Inselspital, Universitätsspital Bern
Derm. Hel. 2017;29(7):30
Nach einer glücklichen Kindheit und Jugend auf Madeira zog ich 1993 aufs Portugiesische Festland, nach Lissabon, um Medizin zu studieren. Mein Interesse für den Menschen mit seinen bio-psycho-sozialen Aspekten überwog weite-ren, wie Meeresbiologie, Literatur, Musik und Theater. Manchmal fra-ge ich mich wie alles gekommen wäre, wenn meine Wahl eine ande-re gewesen wäre… Aber ich habe meinen Weg, den ich damals ein-geschlagen habe, nie bereut. So-wohl die täglichen medizinischen Anforderungen, als auch die Mög-lichkeiten von und mit anderen KollegInnen zu lernen, in verschie-denen medizinischen und kulturellen Umfeldern, sind für mich nach wie vor eine grosse Bereicherung.
Nach Abschluss des Medizinstudiums folgte das obli-gatorische zweijährige Ausbildungsprogramm in All-gemeinmedizin. Einige Monate davon absolvierte ich auf den kapverdischen Inseln, wo ich versucht habe Medizin zu lernen und zu praktizieren in einem Land mit stark limitierten medizinischen Ressourcen. Wäh-rend dieser Zeit wuchs mein Interesse für die Derma-tologie. 2002 trat ich meine dermatologische Ausbil-dungsstelle in Portugals grösster Universitätsklinik an, dem Hospital de Santa Maria. Mein Tutor war damals auch gleichzeitig zuständig für die Sprechstunde für pädiatrische Dermatologie, meinem Hauptinteresse von Anfang an. So hatte ich zusätzlich zum obligato-rischen Dermatologie-Ausbildungsprogramm einen privilegierten Kontakt zur Kinderdermatologie. Ein Fellowship-Aufenthalt an der Klinik für pädiatrische Dermatologie in Milano bei Prof. Carlo Gelmetti berei-cherte diese Zeit zusätzlich.
Nach Abschluss des Facharztes für Dermatologie 2008 wurde mir die Verantwortung für die pädiatrische Dermatologie an der Universitätsklinik Santa Maria übertragen. Damals gab es in Portugal noch keine Spezialsprechstunde für Genodermatosen. Inspiriert durch Professor Louis Dubertret, Präsident der Fon-dation René Tourain sowie des Projektes "Genoder-matoses et Mediterranée", gründete ich damals die multidisziplinäre Sprechstunde primär für Menschen mit Epidermolysis bullosa (EB), als auch Ichthyosis. Dazu gehörte die Mitgründung der portugiesischen Patientenvereinigung für EB und die Zusammenar-beit mit der damals neuen Ichthyosis-Delegation des nationalen Parlaments, mit der Zielsetzung, dass diese Erkrankungen endlich durch das Gesundheits-wesen anerkannt und finanziell unterstützt werden. Weitere Genodermatose-Projekte wurden von der Eu-ropäischen Union finanziell unterstützt. Aus dieser in-tensiven Phase des Austausches mit anderen europä-
ischen Genodermatose-Zentren, reich an Informationskampagnen, medizinischen Kongressen und Pressekonferenzen, Kontakten mit Entscheidungsträgern im Gesund-heitswesen, mit Politikern, Patien-ten und deren Familien, sehe ich zurück auf grosszügige Begegnun-gen mit den meisten Menschen die ich in diesem Zusammenhang getroffen habe.
Ende 2013, nach unserem Ent-schluss als Familie mit zwei Kindern nach Schweden zu ziehen, begann ich als "Senior Consultant in Der-matology" an der Universitätsklinik in Linköping zu arbeiten. In ent-
spannter und nicht-hierarchisch geregelter Zusam-menarbeit, wie sie für Nordische Spitäler typisch ist, wurde ich bekannt mit einem sehr gut organisierten Klinikalltag, in welchem Fallbesprechungen, klinische und therapeutische Guidelines und Algorithmen, als auch politische Aspekte teils sehr umfassend in Teams diskutiert wurden. Nebst meiner Verantwortung für die pädiatrische Dermatologie war ich Teil eines mul-tidisziplinären Teams am Allergie-Zentrum der Uni-versitätsklinik, sowie der Sprechstunde für Hauttumo-ren – einem der Hauptgründe für dermatologische Konsultationen in Schweden. Wir haben das Leben in diesem Land, welches mit Rahmenbedingungen das Familienleben unterstützt und eine gute Work-Life-Balance gewährt, sehr genossen. Dennoch konnte ich, ohne ein Wort Deutsch sprechen zu können, das Angebot der Dermatologischen Universitätsklinik in Bern nicht widerstehen, um mich wieder vermehrt der pädiatrischen Dermatologie und insbesondere den Fragen rund um EB zu widmen. Im Dezember 2015 habe ich meine Arbeit in Bern begonnen. Hier, in einer familiären Umgebung, habe ich ein profession-nelles, vielseitiges, kosmopolitisches, vielsprachiges, unterstützendes und dynamisches Team gefunden. Dank der grossen Unterstützung durch Professor Bor-radori war es möglich die multidisziplinäre, Patienten-zentrierte medizinische Betreuung von Menschen mit EB zu erhalten und weiter auszubauen. Diese her-ausfordernde Arbeit erfolgt in Zusammenarbeit mit anderen Schweizer Kliniken, internationalen EB-Re-ferenz- und Forschungszentren, als auch Patientenor-ganisationen sowie privaten Institutionen, welche un-sere Arbeit grosszügig unterstützen. Mit dem Gefühlt endlich mein "professionelles Zuhause" gefunden zu haben freue ich mich auf die kommenden Jahre …
30 Dermatologica Helvetica – Volume 29(7) – Septembre 2017

Naevus de Spitz
Das Eponym geht auf Sophie Spitz (1910-1956) zurück. Sie wurde in Tennessee geboren und ent-stammt jüdischer Immigrantenfamilien aus Euro-pa. Ihr Spezialgebiet war die Pathologie und da vor allem die Tropenpathologie über die sie auch ein Buch veröffentlichte. Ein weiteres Interesse galt der orthopädischen Pathologie. Sie setzte sich sehr für die Anwendung des cervicalen PAP-Abstriches zur Diagnose des Cervix-Karzinoms ein. Die Dermato-logie betreffend publizierte sie 1948 "melanoms of childhood". Dabei handelt es sich um gutartig verlaufende Läsionen, die bei Kindern in Form von einzelnen rötlichen Knötchen meist im Gesicht auf-treten. Die histologischen zytologischen Merkmale stellen bei stärker pigmentierten Läsionen Schwie-rigkeiten zur Unterscheidung von Melanomen dar was den Titel der Publikation erklärt. Diese Form ist auch unter dem Namen "Naevus de Reed" oder pigmentierter Naevus de Spitz bekannt.
Naevus de Spitz
L’éponyme se relate à Sophie Spitz (1910-1956). Elle est née à Tennessee et est d’origine des familles juives immigrées de l’Europe. Sa spécialité était la pathologie en particularité la pathologie tropicale, qui a été également le sujet d’un livre. Un autre intérêt spécialisé concernait la pathologie orthopé-dique. Elle s’est très engagée à l’utilisation du PAP cervical pour le diagnostic du carcinome cervical. Concernant la dermatologie, elle a publié en 1948 "melanoms of childhood". Il s’agit d’une lésion rosée bénigne chez les enfants se localisant surtout au visage. Les structures histologiques peuvent poser des difficultés de diagnostic différentiel lorsque les lésions sont plus pigmentées, ce qui explique la dé-nomination de la dermatose. Cette forme s’appelle aussi "naevus de Reed" ou naevus de Spitz pigmen-té.
Te
rmin
olo
gie
Dermatologica Helvetica – Volume 29(7) – Septembre 2017 31
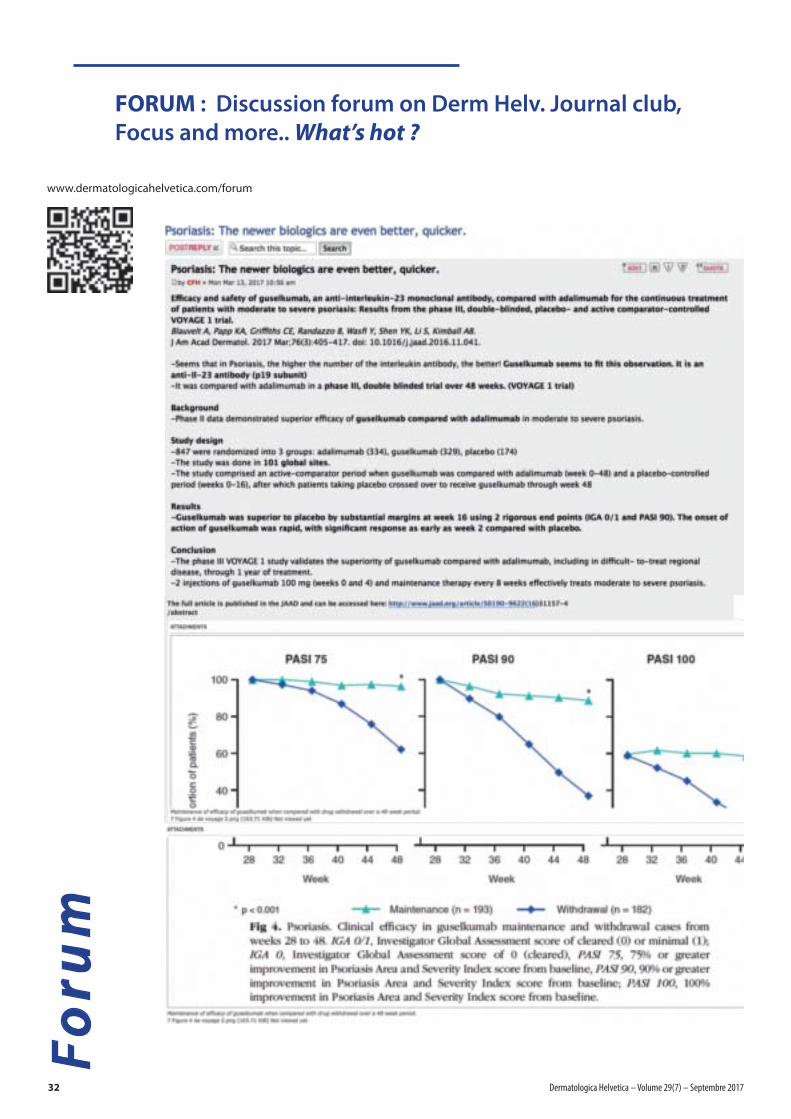
FORUM : Discussion forum on Derm Helv. Journal club,
Focus and more.. What’s hot ?
www.dermatologicahelvetica.com/forum
Fo
rum
32 Dermatologica Helvetica – Volume 29(7) – Septembre 2017
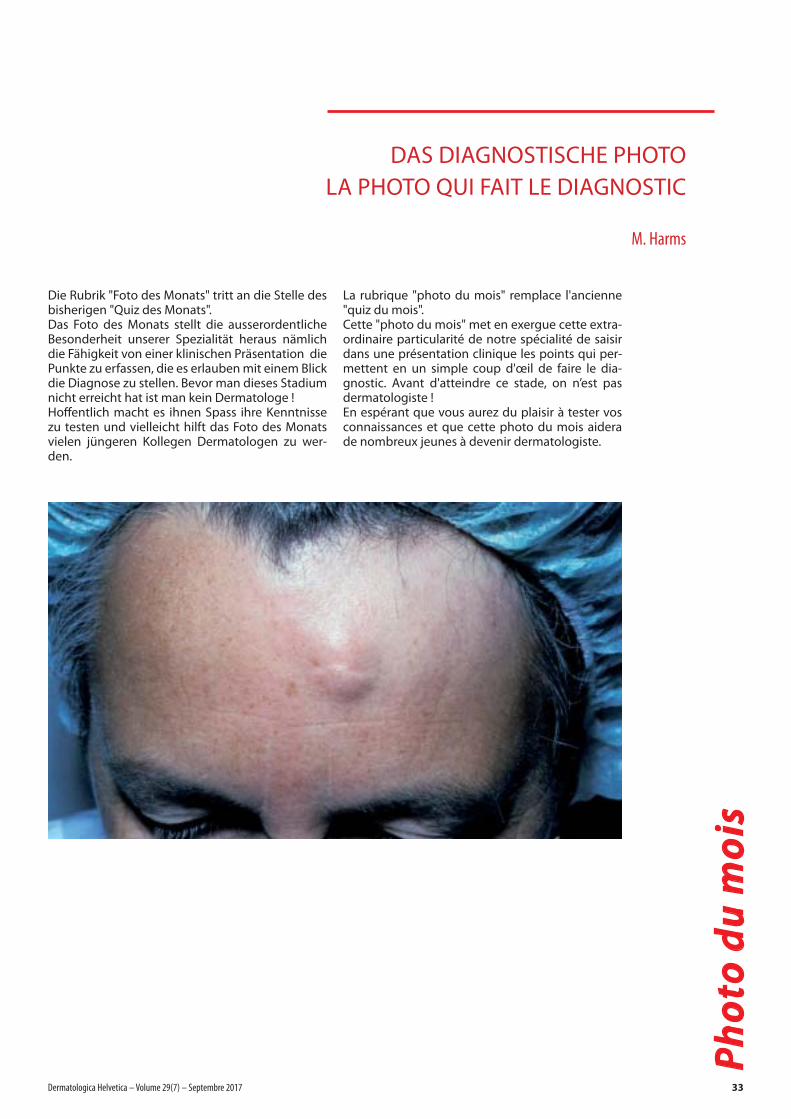
DAS DIAGNOSTISCHE PHOTO
LA PHOTO QUI FAIT LE DIAGNOSTIC
M. Harms
Die Rubrik "Foto des Monats" tritt an die Stelle des bisherigen "Quiz des Monats". Das Foto des Monats stellt die ausserordentliche Besonderheit unserer Spezialität heraus nämlich die Fähigkeit von einer klinischen Präsentation die Punkte zu erfassen, die es erlauben mit einem Blick die Diagnose zu stellen. Bevor man dieses Stadium nicht erreicht hat ist man kein Dermatologe ! Hoffentlich macht es ihnen Spass ihre Kenntnisse zu testen und vielleicht hilft das Foto des Monats vielen jüngeren Kollegen Dermatologen zu wer-den.
La rubrique "photo du mois" remplace l'ancienne "quiz du mois". Cette "photo du mois" met en exergue cette extra-ordinaire particularité de notre spécialité de saisir dans une présentation clinique les points qui per-mettent en un simple coup d'œil de faire le dia-gnostic. Avant d'atteindre ce stade, on n’est pas dermatologiste ! En espérant que vous aurez du plaisir à tester vos connaissances et que cette photo du mois aidera de nombreux jeunes à devenir dermatologiste.
Ph
oto
du
mo
is
Dermatologica Helvetica – Volume 29(7) – Septembre 2017 33
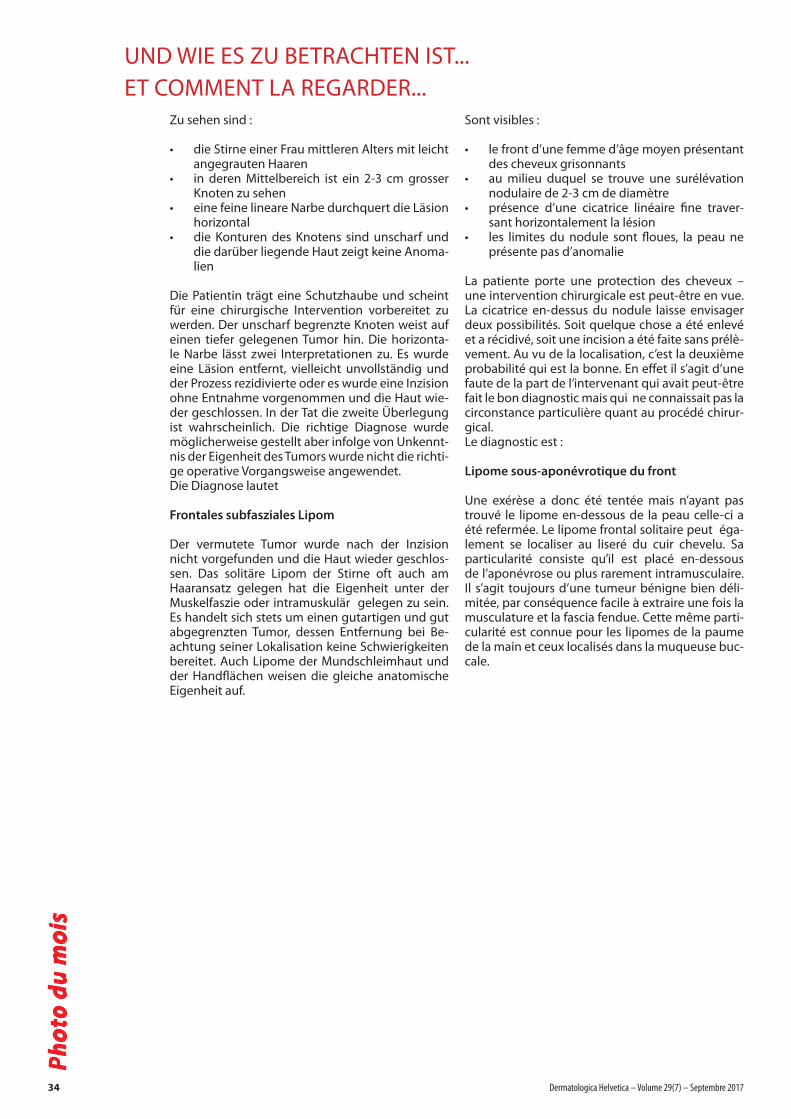
UND WIE ES ZU BETRACHTEN IST...
ET COMMENT LA REGARDER...
Ph
oto
du
mo
is
Zu sehen sind :
• die Stirne einer Frau mittleren Alters mit leicht angegrauten Haaren
• in deren Mittelbereich ist ein 2-3 cm grosser Knoten zu sehen
• eine feine lineare Narbe durchquert die Läsion horizontal
• die Konturen des Knotens sind unscharf und die darüber liegende Haut zeigt keine Anoma-lien
Die Patientin trägt eine Schutzhaube und scheint für eine chirurgische Intervention vorbereitet zu werden. Der unscharf begrenzte Knoten weist auf einen tiefer gelegenen Tumor hin. Die horizonta-le Narbe lässt zwei Interpretationen zu. Es wurde eine Läsion entfernt, vielleicht unvollständig und der Prozess rezidivierte oder es wurde eine Inzision ohne Entnahme vorgenommen und die Haut wie-der geschlossen. In der Tat die zweite Überlegung ist wahrscheinlich. Die richtige Diagnose wurde möglicherweise gestellt aber infolge von Unkennt-nis der Eigenheit des Tumors wurde nicht die richti-ge operative Vorgangsweise angewendet. Die Diagnose lautet
Frontales subfasziales Lipom
Der vermutete Tumor wurde nach der Inzision nicht vorgefunden und die Haut wieder geschlos-sen. Das solitäre Lipom der Stirne oft auch am Haaransatz gelegen hat die Eigenheit unter der Muskelfaszie oder intramuskulär gelegen zu sein. Es handelt sich stets um einen gutartigen und gut abgegrenzten Tumor, dessen Entfernung bei Be-achtung seiner Lokalisation keine Schwierigkeiten bereitet. Auch Lipome der Mundschleimhaut und der Handflächen weisen die gleiche anatomische Eigenheit auf.
Sont visibles :
• le front d’une femme d’âge moyen présentant des cheveux grisonnants
• au milieu duquel se trouve une surélévation nodulaire de 2-3 cm de diamètre
• présence d’une cicatrice linéaire fine traver-sant horizontalement la lésion
• les limites du nodule sont floues, la peau ne présente pas d’anomalie
La patiente porte une protection des cheveux – une intervention chirurgicale est peut-être en vue. La cicatrice en-dessus du nodule laisse envisager deux possibilités. Soit quelque chose a été enlevé et a récidivé, soit une incision a été faite sans prélè-vement. Au vu de la localisation, c’est la deuxième probabilité qui est la bonne. En effet il s’agit d’une faute de la part de l’intervenant qui avait peut-être fait le bon diagnostic mais qui ne connaissait pas la circonstance particulière quant au procédé chirur-gical.Le diagnostic est :
Lipome sous-aponévrotique du front
Une exérèse a donc été tentée mais n’ayant pas trouvé le lipome en-dessous de la peau celle-ci a été refermée. Le lipome frontal solitaire peut éga-lement se localiser au liseré du cuir chevelu. Sa particularité consiste qu’il est placé en-dessous de l’aponévrose ou plus rarement intramusculaire. Il s’agit toujours d’une tumeur bénigne bien déli-mitée, par conséquence facile à extraire une fois la musculature et la fascia fendue. Cette même parti-cularité est connue pour les lipomes de la paume de la main et ceux localisés dans la muqueuse buc-cale.
34 Dermatologica Helvetica – Volume 29(7) – Septembre 2017

le don d‘apaiser
UNE AMÉLIORATION SIGNIFICATIVE DES SIGNES CLINIQUES
AMÉLIORATION DES SIGNES CLINIQUES DANS LE CADRE DES TRAITEMENTS ANTI-ACNÉ ORAUX
Favorisez l’observance de vos traitements avec
HYDRA
• Cleanance HYDRA est destiné aux patients qui souffrentdes effets secondaires des traitements anti-acnéiques (oraux ou locaux)
• La crème lavante Cleanance HYDRA nettoie l’épidermedes peaux fragilisées et restaure le confort cutané
• La crème hydratante Cleanance HYDRA assure unemeilleure hydratation et une meilleure nutrition (glycé-rine et huiles végétales)
• Effet apaisant grâce au bisabolol et à l’Eau Thermaled’Avène
La diminution des signes d’irritation favorise une bonneobservance des traitements médicamenteux.
1) 44 patients acnéiques traités par isotrétinoïne orale (n =10) ou traitement anti-acnéique topique (n = 34).2 applications par jour/28 jours.
-63,2 %1,9
0,5
1,0
1,5
2,0
Scor
es c
liniq
ues
Rougeurs Sécheresse Sensation de brûlure
Inconfort0
J0 J28
0,7 0,7
0,3 0,3
1,6
1,8-61,1 %
-81,3 % -81,3 %1,6
LES SIGNES D’IRRITATION SONT VISIBLEMENT DIMINUÉS(1)
* In Woche 16 mit Cosentyx® 300 mg; der primäre Endpunkt PASI 75 in Woche 12 / § Cosentyx® 300 mg (Fertigspritze)/Cosentyx® 300 mg SensoReady® (Fertigpen) ist zur Behandlung erwachsener Patienten mit mittelschwerer
bis schwerer Plaque-Psoriasis indiziert.1
Referenzen: 1 Fachinformation Cosentyx®, Stand der Information: Oktober 2016, www.swissmedicinfo.ch. 2 Bissonette R et al. Secukinumab demonstrates sustained high effi cacy and a favorable safety profi le in moderate to
severe psoriasis patients through 4 years of treatment (extension of SCULPTURE study). Seminars in Cutaneous Medicine and Surgery (Supplement 7). 2016 Dec (35) DOI: 10.12788/j.sder.2016.062 3 Novartis Q2 and H1 2017
Condensed Interim Financial Report – Supplementary Data, 17. Juli 2017, verfügbar unter: https://www.novartis.com/sites/www.novartis.com/fi les/2017-07-interim-fi nancial-report-en.pdf, zuletzt eingesehen: 9. August 2017.
4 Novartis International AG: Das Medikament Cosentyx® (Secukinumab) gegen Schuppenfl echte gewinnt den Innovationspreis Prix Galien Suisse 2016, Medienmitteilung Novartis, verfügbar unter: https://www.novartis.ch/de/news/
media-releases/novartis-international-ag-das-medikament-cosentyxr-secukinumab-gegen, zuletzt eingesehen: 5. Mai 2017.
Cosentyx® (Secukinumab) gekürzte Fachinformation: Z: Pulver zur Herstellung einer Injektionslösung: Jede Durchstechflasche enthält nach Rekonstitution mit 1 ml Wasser für Injektionszwecke 150 mg Secukinumab.
Injektionslösung (Fertigspritze und Fertigpen): Jede Fertigspritze bzw. jeder Fertigpen enthält 150 mg Secukinumab. I: Plaque-Psoriasis: Cosentyx/-SensoReady ist zur Behandlung erwachsener Patienten mit mittelschwerer
bis schwerer Plaque-Psoriasis indiziert, die auf andere systemische Therapien einschliesslich Ciclosporin, Methotrexat oder PUVA nicht angesprochen haben, bei denen diese Therapien kontraindiziert sind oder die diese
Therapien nicht tolerieren. Psoriasis-Arthritis: Cosentyx/-SensoReady, alleine oder in Kombination mit Methotrexat, ist zur Behandlung erwachsener Patienten mit aktiver Psoriasis-Arthritis indiziert, die unzureichend auf
eine vorhergehende Therapie mit krankheitsmodifizierenden Antirheumatika (disease-modifying anti-rheumatic drugs, DMARD) angesprochen haben. Ankylosierende Spondylitis (Morbus Bechterew): Cosentyx/-SensoReady
ist für die Behandlung erwachsener Patienten mit schwerer, aktiver ankylosierender Spondylitis indiziert, die unzureichend auf konventionelle Therapie (beispielsweise NSAIDs) angesprochen haben. D: Plaque-Psoriasis: Die empfohlene Dosis beträgt 300 mg als subkutane Injektion mit Startdosen in den Wochen 0, 1, 2 und 3, gefolgt von monatlichen Erhaltungsdosen beginnend in Woche 4. Jede 300-mg-Dosis wird in Form von zwei
subkutanen Injektionen zu je 150 mg verabreicht. Bei schwerwiegenden unerwünschten Wirkungen soll eine temporäre Unterbrechung der Therapie erwogen werden. Seltene mukokutane Kandida-Infekte traten häufiger
unter 300 mg auf, in schwerwiegenden Fällen eine Dosisreduktion auf 150 mg erwägen. Psoriasis-Arthritis: Die empfohlene Dosis liegt bei 150 mg als subkutane Injektion mit Startdosen in den Wochen 0, 1, 2 und 3, gefolgt
von monatlichen Erhaltungsdosen beginnend in Woche 4. Bei Patienten, die ungenügend auf Anti-TNF ansprechen liegt die empfohlene Dosis bei 300 mg. Für Patienten mit begleitender mittelschwerer bis schwerer
Plaque-Psoriasis siehe Dosierungs- und Anwendungsempfehlungen für Plaque-Psoriasis. Ankylosierende Spondylitis (Morbus Bechterew): Die empfohlene Dosis liegt bei 150 mg als subkutane Injektion mit Startdosen in
den Wochen 0, 1, 2 und 3, gefolgt von monatlichen Erhaltungsdosen beginnend in Woche 4. Einzelheiten und spezielle Patientengruppen s. www.swissmedicinfo.ch. KI: Schwere Überempfindlichkeitsreaktionen gegenüber
dem Wirkstoff oder einem der Hilfsstoffe. Schwere aktive Infektionen. VM: Vorsicht bei Patienten mit einer chronischen Infektion oder rezidivierenden Infektionen in der Vorgeschichte. Vorsicht bei chronisch-entzündlichen
Darmerkrankungen. Bei Auftreten einer anaphylaktischen oder einer anderen schwerwiegenden allergischen Reaktion die Gabe unverzüglich abbrechen und geeignete Therapiemassnahmen einleiten. Risiko bezüglich
Aufflammen der Psoriasis bei Absetzen der Therapie («Rebound») berücksichtigen. Vorsicht bei Impfungen. Die gleichzeitige Verabreichung mit anderen Biologika wurde nicht untersucht und wird nicht empfohlen.
Die Nadelkappe kann Trockenkautschuk (Latex) enthalten. Nur während einer Schwangerschaft anwenden, wenn der Nutzen die möglichen Risiken eindeutig überwiegt. Entscheidung, entweder mit dem Stillen aufzuhören
oder Cosentyx/-SensoReady bei der Mutter abzusetzen soll unter Berücksichtigung der Vorteile des Stillens für das Kind und der Vorteile der Therapie für die Mutter, gefällt werden. Einzelheiten s. www.swissmedicinfo.
ch. IA: Lebendvakzinen sollten nicht gleichzeitig verabreicht werden. Patienten, die Arzneimittel einnehmen, deren Dosis individuell eingestellt wird und die durch CYP450 3A4, 1A2 oder 2C9 metabolisiert werden, sollten
zu Beginn und Ende einer Therapie mit Secukinumab kontrolliert werden und die Dosis dieser Substanzen bei Bedarf angepasst werden. Einzelheiten s. www.swissmedicinfo.ch. UW: Sehr häufig: Infektionen der oberen
Atemwege (17.5%); Häufig: Oraler Herpes, Rhinorrhö, Diarrhö; Gelegentlich: Orale Candidose, Tinea pedis, Candidose des Oesophagus, Neutropenie, Bindehautentzündung, Leberenzyme erhöht, Bilirubin erhöht, Urtikaria.
Einzelheiten s. www.swissmedicinfo.ch. P: Fertigspritze zu 150 mg: Packungen zu 1 und 2 / Fertigpen zu 150 mg: Packungen zu 1 und 2 / Pulver zur Herstellung einer Injektionslösung in Durchstechflasche zu 150 mg:
Packung zu 1 / Verkaufskategorie: B. Weitere Informationen finden Sie unter www.swissmedicinfo.ch. V2 Novartis Pharma Schweiz AG, Risch; Adresse: Suurstoffi 14, 6343 Rotkreuz, Tel. 041 763 71 11.
30
53
5 0
8/2
017
Gewinner Prix Galien Suisse
20164
Für einen spürbar besseren Therapieerfolg bei Psoriasis1*§
Anhaltend und weitgehend erscheinungsfreies Hautbild über 4 Jahre.2
Bestätigte Wirksamkeit für Patienten mit Psoriasis Arthritis.1
Etablierte Erfahrung bei über 90’0003 weltweit behandelten Patienten.
EEtablierrte Er
BBestätigtte W
Hauutbbild