Embed Size (px)
Citation preview

Vol. 116 No. 5 November 2013
Facial trauma patients with a preexisting psychiatric illness:a 5-year studyGary R. Hoffman, MBBS, PhD, MMedSc, FRACDS, FACS, FRCS, andShofiq Islam, MBBCh(Hons), BDS, DOHNS (RCS), MFDSRCS, MRCS(Edin)
Objectives. The aim of this study was to identify and assess the demographics and presence of preexisting psychiatricdisorders in an adult patient cohort admitted for the management of a facial injury.Study Design. The analysis included demographics, type of facial injury, length of hospital stay, and psychiatric diagnosisaccording to criteria as set out in the DSM-IV-TR-2000.Results. We identified 71 patients who had confirmed psychiatric comorbidity. A range of intentional, unintentional, andrecidivist injuries were identified. We found a significant association between length of hospital stay and the number ofdiagnostic categories of preexisting psychopathology (P � .05).Conclusions. This study further confirms that there is a subgroup of facially injured patients with preexisting psychiatric illnesswhich often goes unrecognized and untreated. Early recognition, together with appropriate referral to and management byliaison psychiatry may play an important role in reducing the rate of facial trauma recidivism. (Oral Surg Oral Med Oral
Pathol Oral Radiol 2013;116:e368-e374)Events causing injury are generally thought to be ran-dom and unpredictable, often considered to be acci-dents beyond the control of the victim. However, aproportion of trauma patients may be victims of theirown impulsive, self-destructive, or high-risk behavior.These actions are often the result of impaired judgment,outbursts of anger or violence, and low appreciation ofthe consequences of their conduct. Such traits are alsocommon denominators of an underlying psychiatricdisorder.
There is a well defined subgroup of facially injuredpatients who present with a preexisting psychiatric dis-order.1 These mental health disorders remain an under-considered aspect in the assessment and management ofsuch patients.
We recently published the findings of our prelim-inary investigation into the presence of preexistingpsychologic comorbidity in a group of facially in-jured patients.1 Of the 300 patients included in that21-month study, 16 were identified as having a pre-existing psychiatric diagnosis. In view of the factthat only those facial trauma patients who receivedformal psychiatric input during their admission wereincluded in the study, the authors suspected that the
Presented in part (42-month interim data) at the British Association ofOral & Maxillofacial Surgeons (BAOMS), Annual Scientific Meet-ing, Nice, 2011.Department of Maxillofacial and Head and Neck Surgery, JohnHunter Hospital, Newcastle, New South Wales, Australia.Received for publication Nov 29, 2011; returned for revision Dec 19,2011; accepted for publication Jan 5, 2012.© 2013 Elsevier Inc. All rights reserved.2212-4403/$ - see front matter
http://dx.doi.org/10.1016/j.oooo.2012.01.043e368
figure of 16 patients was likely to underestimate thetrue prevalence of psychiatric illness in this patientgroup.
The early identification of psychologic symptomsin patients who present with a maxillofacial injuryallows for timely intervention and accordingly opti-mizes their recovery. Identifying and managing psy-chological symptoms would help to stabilize premor-bid (preinjury) psychiatric illness. It would alsopotentially help to improve patient compliance, de-crease the risk of reinjury, and decrease the likeli-hood of posttraumatic stress or maladaptive copingstrategies that may develop. That is, traumatic eventsand their psychosocial sequelae (e.g., anxiety, de-pression, dysfunction, deformity, chronic pain) mayfurther exacerbate mental illness. In addition, pre-trauma personality inadequacies may adversely af-fect patients’ coping mechanisms and, in turn, maycontribute to stress reactions and susceptibility tostress-related disorders.2
Regrettably, studies have shown that clinicianspoorly consider and document psychologic problems inpatients who have sustained a facial injury.3 Addition-ally, staff who work within various trauma fields would
Statement of Clinical Relevance
Preexisting psychiatric illness in facially injuredpatients often goes unrecognized. Oral and maxill-ofacial surgeons are ideally situated to recognizethis complex. Early recognition together with ap-propriate referral may play an important role inreducing the rate of facial trauma recidivism.

OOOO ORIGINAL ARTICLEVolume 116, Number 5 Hoffman et al. e369
appear to have a limited knowledge of the possiblepsychologic sequelae that may result after an episode oftrauma.4
The psychiatric classification used in the presentstudy is the system of the American Psychiatric Asso-ciation Diagnostic and Statistical Manual of MentalDisorders, 4th edition (DSM-IV). The DSM-IV is amultiaxial system that organizes each psychiatric diag-nosis into 5 dimensions (axes) relating to differentaspects of the disorder. The 5 axes of DSM-IV are I)clinical disorders (all major mental disorders); II) un-derlying pervasive personality disorders and mentalretardation; III) somatic (nonmental) medical condi-tions; IV) psychosocial and environmental; and V)global assessment of functioning.
The aim of the present study was to further identifyand assess the demographics and presence of preexist-ing psychiatric disorders in an adult patient cohort whowere admitted to a tertiary referral hospital for themanagement of a facial injury.
STUDY DESIGNThe findings of a previously published retrospectivechart audit (21-month period) were combined with aprospective audit (39-month period) to further investi-gate the evidence of preexisting psychiatric comorbid-ity in consecutive adult public admissions to the Max-illofacial Surgery Department, John Hunter Hospital(JHH). JHH is the tertiary referral center for HunterNew England Area Health and serves a population of840,000 people.
This region is characterized by both an urban-met-ropolitan population (n � 500,000) and a rural-remotepopulation (n � 340,000). JHH functions as a tertiaryreferral center, a trauma center, and a university teach-ing hospital.
Psychiatric diagnosis was defined according to crite-ria as set out in the DSM-IV text revision of 2000(DSM-IV-TR2000). Psychiatric diagnosis was assessedat admission. Subjects recruited into the study wereidentified as having a pretraumatic psychiatric diagno-sis as formally established by psychiatry-trained staff.At our institution, trauma patients who did not fulfillthe criteria for hospital admission also did not meet thecriteria for assessment by the liaison psychiatry team.As such, facial trauma patients with “minor injuries”who were discharged directly from the emergency de-partment were not included in this study. Similarly,polytrauma patients not admitted directly under care ofthe maxillofacial team, i.e., those admitted to intensivecare unit who were intubated and ventilated with con-comitant injuries (head injury and multisystem failure);
their general condition precluded mental state assess-ment, and as such they could not be included in thestudy.
Data collected and analyzed included demographics,injury type, length of hospital stay, and psychiatricdiagnosis. Student t test was used to compare meanlength of hospital stay between patients who met thecriteria for a single DSM-IV psychopathology andthose patients who met the criteria for �2 preexistingpsychiatric disorders.
All patients recruited in this study were identifiedas having either features suggestive of psychologicdisturbance, a documented past history of mentalillness, a self-harm facial wound, or a positive toxi-cology screen for substances of abuse or currentlytaking prescribed psychiatric medication (mood sta-bilizers, antidepressants, antipsychotics). In thosepatients without a documented history of mentalillness, with features suggestive of a mental illness,pretraumatic psychopathology was confirmed afterfull in-house psychiatric consultation.
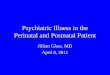
RESULTSThe clinical details of all 71 patients are summarized inTable I. The cohort was predominantly adult male (n �58) with an overall median age of 31 and a bimodaldistribution of 20 and 37 years (range 17-83). A broadspectrum of both soft and hard tissue facial injurieswere represented within the patient cohort. A range ofintentional, unintentional, and recidivist injuries wereidentified. In the context of adult facial injury admis-sions, this study revealed that there is �1 premorbidpsychiatric presentation per month that would require aconsultation liaison psychiatry referral.
The most common axis I diagnosis identified wasmood disorder (n � 47), followed by substance abuse/dependence (n � 23) and schizophrenia (n � 17). Ofthe axis II diagnoses identified, there were 5 patientspresenting with borderline personality disorder, 5 pa-tients presenting with antisocial personality disorder,and 1 patient with a diagnosis of narcissistic personalitydisorder. Intentional injuries accounted for 57 presen-tations (assault 51, self-harm 4, suicide attempt 2), andthere were 14 unintentional injury presentations.Within the 71 patients, 7 were recidivist injuries re-presenting after successful surgical management anddischarge, 2 of which had multiple readmissions andunderwent multiple surgical interventions during thestudy period.
We found high rates of alcohol or other drug abuseproblems among this subgroup of 45 patients. In thisstudy, patients with substance abuse comorbidity alsohad a relatively high percentage of intentional facial
injuries. Of the 23 patients admitted with facial injury
ORAL AND MAXILLOFACIAL SURGERY OOOOe370 Hoffman et al. November 2013
Table I. Summary of facially injured patients referred to liaison psychiatry for formal interventionCase no. Etiology Sex Age (y) Pretrauma psychiatric diagnosis Maxillofacial injury
1 MVA M 23 Substance abuse Le Fort I fractureMandible fracture
2 Assault M 28 SchizophreniaAlcohol abuse
Mandible fracture
3 Assault M 46 Polysubstance abuse Orbit floor fractureZMC fracture
4 Assault M 23 Schizophrenia Zygoma fractureMandible fracture
5 Suicide attempt M 41 Major depressionAlcohol abuse
Deliberate gunshot facial injury
6 Assault M 37 Major depressionAnxiety
Mandible fracture
7 Self-harm F 22 DysthymiaBorderline PD
Deliberate facial laceration
8 Assault M 52 Substance abuseAntisocial PDMajor depression
Orbital fractures
9 Assault M 37 Major depressionPolysubstance abuse: alcohol, nicotine, cannabis
Nasal fracture
10 MVA F 20 Major depression Le Fort III fracture (blindness)11 Assault F 27 Borderline PD
Polysubstance abuseOrbital fractures
12 Self-harm M 56 SchizophreniaSubstance abuse
Deliberate facial burns
13 Assault M 20 Schizophrenia Mandible fracture14 Assault M 38 Major depression Orbital nasal fracture15 Accident F 19 Substance abuse Degloving scalp laceration16 Assault M 28 Antisocial PD
Borderline PDPolysubstance abuse
Stab laceration
17 Assault M 62 Major depressionSubstance abuseEtOH induced amnesic disorder
Mandible fracture
18 Assault M 37 DepressionAnxiety disorder
Mandible fracture
19 Assault M 29 Bipolar disorderSubstance abuse
Mandible fracture
20 Assault M 24 Major depressionSchizophrenia
Mandible fracture
21 Assault M 37 SchizophreniaSubstance abuse
Orbital floor fractureNasal bone fracture
22 Assault M 27 Bipolar disorder Zygomatic arch fracture23 Assault M 37 Major depression Mandible fracture24 Assault M 20 Major depression
Polysubstance abuseZygomatic complexFacial laceration
25 Suicide attempt/MVA M 53 Major depressionNarcisistic PD
Facial laceration
26 MVA M 23 OCD Orbital floor fractureComminution of maxillary sinus wall
27 Assault M 21 Polysubstance abuse Mandible fracture28 Assault M 28 Major depression Le Fort II fracture
Zygomatic arch fracture29 Self-harm M 25 Major depression Facial laceration30 Assault M 39 Anxiety
Major depressionOrbital floor fracture
31 MVA M 61 Major depression Le Fort II fracture32 Fall F 33 Bipolar disorder
Polysubstance abuseMandible fracture
33 MVA M 33 Paranoid schizophrenia Mandible fractureOrbital floor fractureZMC fractureHard palate fracture
34 Assault M 35 Bipolar disorder Orbital floor fracture
35 Assault M 20 Antisocial PD Mandible fracture
matic c
OOOO ORIGINAL ARTICLEVolume 116, Number 5 Hoffman et al. e371
and substance abuse comorbidity, 70% of injuries (16/23) were caused by assault.
We analyzed the hospital discharge rates to examine
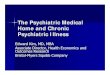
Table I. Continued
Case no. Etiology Sex Age (y)
36 Assault M 2437 Assault M 2038 Assault M 2339 Assault M 25
40 Assault M 3541 Assault M 2042 Assault F 2443 Assault M 2044 Assault M 2345 Assault M 25
46 Fall F 3247 Assault M 2348 Fall M 25
49 Self-harm M 4750 Assault M 35
51 MVA M 43
52 Assault M 2653 Assault M 55
54 Assault M 45
55 Assault M 51
56 Fall F 83
57 Assault M 5558 Assault M 2959 Assault M 47
60 Assault M 2461 Assault M 50
62 Assault M 58
63 Assault M 61
64 Assault M 27
65 Assault M 2266 Assault M 2167 Assault F 3768 Fall M 3669 Assault M 23
70 Assault M 34
71 Fall M 17
MVA, Motor vehicle accident; PD, personality disorder; ZMC, zygo
the effect of preexisting mental illness on the length of
hospital stay after admission with facial trauma. Weexcluded patients eventually needing inpatient psychi-atric care after definitive surgical treatment as well as
Pretrauma psychiatricdiagnosis Maxillofacial injury
Schizophrenia Mandible fractureMajor depression Mandible fractureSchizophrenia ZMC fractureSchizophrenia Orbital floor fracture
ZMC fractureBipolar disorder Orbital floor fractureAntisocial PD Mandibular fractureSchizophrenia Mandibular fractureMajor depression Mandibular fractureSchizophrenia ZMC fractureSchizophrenia Orbital floor fracture
ZMC fractureMajor depression Mandible fractureMajor depression Orbital rim fractureMajor depression Orbital floor fracture
ZMC fractureMajor depression Stab wound to tongueMajor depressionSubstance abuse
Mandible fracture
Major depression Mandible fractureFacial laceration
Major depression Mandible fractureSchizophreniaDepression
ZMC fracture
Major depression Orbital wall fractureZygomatic arch fractureNasal fracture
AnxietyDepression
ZMC fractureMandible fracture
Major depression Nasal fractureFacial laceration
Major depression ZMC fractureBorderline PD Facial lacerationAnxietyDepression
ZMC fracture
Major depression Orbital floor fractureSchizophreniaDepression
Mandible fracture
Major depressionSubstance abuse
Mandible fracture
Major depressionSubstance abuse
ZMC fracture
AnxietyDepression
Mandible fracture
Major depression ZMC fractureMajor depression Mandible fractureMajor depression Nasal fracturePolysubstance abuse ZMC fractureDepressionPolysubstance abuseBorderline personality disorder
Mandible fracture
Bipolar disorderSchizophreniaPolysubstance abuseAntisocial personality disorder
Mandible fracture
Bipolar disorderSchizophrenia
Mandible fracture
omplex.
those who had nonpsychiatric comorbid disorders

ORAL AND MAXILLOFACIAL SURGERY OOOOe372 Hoffman et al. November 2013
which may have influenced duration of hospital admis-sion from the analysis. An interesting finding in ourstudy was that those patients who met the criteria for�2 preexisting DSM-IV psychopathologies stayed sig-nificantly longer than those who had fulfilled the crite-ria for 1 [6.91 days (SD 4.56) vs. 2.89 days (SD 1.71),95% CI 1.42-7.01; P � .014].
We did not identify any statistically significant cor-relation between sociodemographic variables and clin-ical characteristics or association between specific pre-morbid psychologic diagnoses in those patients whoexhibit a pattern of multiple readmissions with facialinjuries.
DISCUSSIONIt has been stated that 12% of the U.S. population arediagnosed and treated for mental illness annually.5 Therelationship between mental illness and intentional in-jury (assault, self-harm, suicide), unintentional injury(motor vehicle accident [MVA], pedestrian accidents,falls) and injury recidivism, have been reported in theliterature.5 Six out of 10 people with a substance usedisorder also suffer from another form of mental ill-ness.6 Alcohol and substance abuse is also a contribut-ing factor to injury.6 A significant proportion of thepatients in the present study (23/71) were identified ashaving a substance abuse disorder.
In 1985, Silverman et al.7 reported that 19 of 56patients (34%) in their study of trauma admissions metthe criteria for �1 psychiatric disorders (alcohol abuseand dependence, affective and antisocial personalitydisorder). A similar study was undertaken by Whetsellet al.,2 who interviewed 100 patients admitted to a level1 trauma center. They used the Hanger scale to docu-ment the incidence of preinjury psychopathology traits,subdividing 22 neurovegetative symptoms into eitherneurotic or somatic categories. They found that 56% ofpatients displayed symptoms consistent with psychopa-thology. Seventy-four percent of their cohorts weremale, with an overall mean age of 33 years. Forty-ninepercent of patients were intoxicated at the time of theiradmission. Eight percent of injuries were self-inflicted.
In 1997, Poole et al.8 investigated a cohort of 183patients (intentional trauma, nonintentional trauma orelective surgical) to assess the importance of personalpsychologic factors in traumatic injury. They docu-mented sociodemographic variables, psychologic-intel-lectual status, and evidence supportive of a formalpsychiatric disorder. They found that 63% of patients(29/46) presenting with intentional injuries met thecriteria for �1 category of psychopathology. Signifi-cantly, of these 29, 16 patients further met the criteria
for �3 categories of psychopathology.The present study was an ongoing investigation offacially injured patients who presented with a preexist-ing mental illness. It further identified that male pa-tients (n � 58) were more likely to have psychologiccomorbidity than their female patient counterparts (n �13) (estimated odds ratio 12.3, 95% CI 6.4-23.8; P �.001). The mean age of presentation was 31 years.However, the majority of patients were actually underthe age of 30 years (n � 41).
Axis I diagnoses (mental disorder syndromes) dom-inated the range of psychopathology identified withinthis cohort of facially injured adults. As previouslystated, it was not always entirely clear as to whatspecific role the patient’s premorbid mental illness hadplayed in the cause of the injury. That is, aggression,deliberate self-harm, intoxication, risk taking, and ac-cident are all variably known to be associated with theoccurrence of trauma. Axis II diagnoses (pervasive-personality disorders) are considered to be inflexible,maladaptive, or dysfunctional behaviors that are evi-dent across a broad range of personal and social situa-tions. Axis II diagnosis represented 15% of the group(n � 11). Patients were equally represented by eithercluster A (antisocial—a pervasive disregard for therights of others), or cluster B (borderline—rigid, unsta-ble in relationships, self-identity, and behavior).
The effect of preexisting mental illness on the lengthof hospital stay after admission with facial trauma alsohas significant economic implications. Analysis of ourinstitution’s discharge data indicated that those patientswho met the diagnostic criteria for �2 categories ofpreexisting DSM-IV psychopathology had a signifi-cantly extended length of hospital stay compared withpatients who met the category for only 1. According toPoole et al.’s8 case-control study, 63% of patients ad-mitted with intentional trauma met the diagnostic cri-teria for �1 and 32% for �3 categories of mentalillness. These findings suggest that there may be highereconomic cost with the clinical management of thesepatients. The limitations in our analysis are that we didnot control for facial injury severity, as well as otherpotential confounders, e.g., delay in obtaining theatertime. However, other studies that have looked at thecharacteristics of trauma patients with psychiatric mor-bidity have also demonstrated prolonged hospital staysand greater use of resources.9,10 Posel and Moss9 dem-onstrated that patients referred for psychiatric assess-ment admitted under general trauma services had, onaverage, twice the length of hospital stay.
The co-occurence of mental health disorders andsubstance (ab)use is common.1,6 Illicit drug takingcould result in mental health problems, and those withmental health problems are potentially more likely to
resort to illicit drug taking. These drugs are used to
OOOO ORIGINAL ARTICLEVolume 116, Number 5 Hoffman et al. e373
decrease anxiety, decrease social inhibition, or increasewell-being. Regrettably, however, they are also respon-sible for inducing deleterious delusional, paranoid-psy-chotic, depressional, or euphoric states.
An association appears to exist between mental ill-ness and the likelihood of being involved in violentincidents. The dual diagnosis of mental health disorderand substance abuse probably dramatically increasesthe risk of violence.11 Indeed, several studies havedemonstrated that substance abuse, psychotic symp-toms, and lack of contact with mental health services inthe community are associated with a greater risk oflifetime violence among people with mental illness.
A significant proportion of adults who required hos-pital admission for the surgical management of a trau-matic injury displayed harmful substance (alcohol andillicit drug)–abusive behavior.12 Up to 40% of patientsmay have a positive blood alcohol concentration onadmission.12 This figure has been shown to rise signif-icantly in patients who are subjected to urine toxicology(e.g., cocaine/opiate screening).13
As with general trauma, there are substantial associ-ations between substance abuse and the occurrence offacial injury.14 It is reasonable to conclude that there isa strong association between psychiatric illness, sub-stance abuse, incidents of interpersonal violence, andresultant maxillofacial injury. Furthermore, substanceabuse can compromise wound repair and levels ofpostsurgical outpatient compliance as well as predis-pose to trauma recidivism. Shetty et al.15 found thatrecalcitrant trauma patients (compared with sociode-mographically matched cohorts) are more likely to re-port habitual use of alcohol and drugs. Twenty-threepatients in the present study were identified as habitualsubstance abusers. Thirteen had a comorbid mentalhealth disorder (17 axis I; 3 axis II), and 5 were sub-stance abusers in the absence of such disorder.
Routine screening and counseling for alcohol andother substance abuse problems may play a role in thereduction of maxillofacial trauma. Gentilello et al.16
conducted a randomized prospective controlled trial ina level 1 trauma center and demonstrated that alcoholintervention reduced trauma recurrences by as much as47% over a 3-year follow-up period. That study lendssupport to the argument that screening for alcohol/substance abuse should be a routine component of thework-up of all trauma patients. A U.S. survey, how-ever, showed that only 40% of level 1 and level 2trauma centers and only 26% of level 3 centers werefound to perform routine toxicology screens.17
There are several reasons cited for failure to rou-tinely screen for substance abuse and failure of theadmitting clinician’s inclination to pursue psychosocial
factors that may have precipitated the episode oftrauma. Cost related to screening is undoubtedly animportant factor. Many hospitals do not have 24-hourpsychiatric coverage, and the availability of communitybased psychiatric and addiction services may be lim-ited. It is reasonable to assume that ready access to suchcare will influence a clinician’s decision. However, webelieve the limiting factor for the generation of suchrequests, in the context of tertiary-care institutions, islack of time, as well as the clinician’s intuitive recog-nition and understanding of the impact of mental dis-orders associated with (or complicating) a medicalproblem. Oral and maxillofacial surgeons are uniquelypositioned to maintain vigilance and, where appropri-ate, screen for such conditions.
We think that the present study underestimates thetrue prevalence of mental illness in victims of facialinjury, because the survey was restricted to inpatientsonly. There may have been patients with psychiatricdisorder who we inadvertently missed because they didnot have documented history of psychiatric illness ormanifest abnormal behaviors. As mentioned previ-ously, facial trauma patients who met the criteria for apreexisting psychopathology who were discharged di-rectly from the emergency department were not in-cluded in this study. Similarly, polytrauma patients notadmitted directly under care of the maxillofacial teamwere not included in our survey.
CONCLUSIONThere are remarkably consistent findings from numer-ous studies that have investigated the psychosocial fac-tors associated with patients who sustain a facial injuryand who require treatment at a large urban hospital.These patients are typically young, male, and socioeco-nomically disadvantaged. Most injuries are intentional(assault) and many involve alcohol and/or substanceabuse. Patients often have high rates of life-time andcontemporary social and mental health needs. The pres-ent study further identifies that there is also a small butnonetheless well recognized patient cohort who presentwith a demonstrated pretraumatic psychiatric comor-bidity. They would seem to benefit from early recog-nition together with subsequent referral to and manage-ment by liaison psychiatry.
REFERENCES1. Islam S, Hooi H, Hoffman GR. Presence of pre-existing
psychological comorbidity in a group of facially injured pa-tients: a preliminary investigation. J Oral Maxillofac Surg2009;67:1889-94.
2. Whetsell LA, Patterson CM, Young DH, Schiller WR. Preinjurypsychopathology in trauma patients. J Trauma 1989;29:1158-61.
3. Shepherd JP, Qureshi R, Preston MS, Levers BG. Psychologicaldistress after assaults and accidents. BMJ 1990;13:849-50.
4. Alexander DA, Atcheson SF. Psychiatric aspects of trauma care:
a survey of nurses and doctors. Psychol Bull 1998;22:132-6.
ORAL AND MAXILLOFACIAL SURGERY OOOOe374 Hoffman et al. November 2013
5. Wan JJ, Morabito DJ, Khaw L, Knudson MM, Dicker RA.Mental illness as an independent risk factor for unintentionalinjury and injury recidivism. J Trauma 2006;61:1299-304.
6. National Institute of Drug Abuse. Topics in brief. ComorbidDrugs Abus Ment Illn 2004.
7. Silverman JJ, Peed SF, Goldberg S, Hamer RM, Stockman SJ.Surgical staff recognition of psychopathology in trauma patients.J Trauma 1985;25:544-6.
8. Poole GV, Lewis JL, Devidas M, Hauser CJ, Martin RW,Thomae KR. Psychopathologic risk factors for intentional andnonintentional injury. J Trauma 1997;42:711-5.
9. Posel C, Moss J. Psychiatric morbidity in a series of patientsreferred from a trauma service. Gen Hosp Psychiatry1998;20:198-201.
10. Saravay SM, Lavin M. Psychiatric comorbidity and length ofstay in the general hospital. A critical review of outcome studies.Psychosomatics 1994;35:233-52.
11. Mulvey EP. Assessing the evidence of a link between mentalillness and violence. Hosp Community Psychiatry 1994;45:663-8.
12. Murphy DA. Substance use and facial injury. Oral MaxillofacSurg Clin North Am 2010;22:231-8.
13. Cornwell EE third, Belzberg H, Velmahos G, Chan LS, Dem-
etriades D, Stewart BM, et al. The prevalence and effect ofalcohol and drug abuse on cohort-matched critically injuredpatients. Am Surg 1998;64:461-5.
14. Mathog RH, Toma V, Clayman L, Wolf S. Nonunion of themandible: an analysis of contributing factors. J Oral MaxillofacSurg 2000;58:746-52; Discussion: 752-3.
15. Shetty V, Dent DM, Glynn S, Brown KE. Psychosocial sequelaeand correlates of orofacial injury. Dent Clin North Am2003;47:141-57.
16. Gentilello LM, Rivara FP, Donovan DM, Jurkovich GJ, Daran-ciang E, Dunn CW, et al. Alcohol interventions in a traumacenter as a means of reducing the risk of injury recurrence. AnnSurg 1999;230:473-80.
17. Soderstrom CA, Dailey JT, Kerns TJ. Alcohol and other drugs:an assessment of testing and clinical practices in U.S. traumacenters. J Trauma 1994;36:68-73.
Reprint requests:
Dr. Shofiq IslamSenior House OfficerBirmingham Children’s HospitalSteel House LaneWest Midlands, B1United Kingdom
[email protected]