Embed Size (px)
Citation preview

F
Ma
b
c
a
ARRAA
KMKCL
1
r2pOttmcc
t
0d
Vaccine 28 (2010) 6723–6729
Contents lists available at ScienceDirect
Vaccine
journa l homepage: www.e lsev ier .com/ locate /vacc ine
actors affecting compliance with measles vaccination in Lao PDR
aniphet Phimmasanea, Somthana Douangmalab, Paulin Koffia, Daniel Reinharzc, Yves Buissona,∗
Institut de la Francophonie pour la Médecine Tropicale, Samsenthai Street, BP 9519, Vientiane, Lao People’s Democratic RepublicMinistry of Health, Vientiane, Lao People’s Democratic RepublicLaval University, Quebec City, Canada
r t i c l e i n f o
rticle history:eceived 3 March 2010eceived in revised form 22 July 2010ccepted 25 July 2010vailable online 6 August 2010
eywords:easles vaccine
APomplianceaos
a b s t r a c t
In line with WHO objectives, the Lao Government is committed to eliminate measles by 2012. Yet from1992 to 2007, the annual incidence of measles remained high while the vaccination coverage showed awide diversity across provinces. A descriptive study was performed to determine factors affecting com-pliance with vaccination against measles, which included qualitative and quantitative components. Thequalitative study used a convenience sample of 13 persons in charge of the vaccination program, consist-ing of officials from different levels of the health care structure and members of vaccination teams. Thequantitative study performed on the target population consisted of a matched, case-control survey con-ducted on a stratified random sample of parents of children aged 9–23 months. Overall, 584 individuals(292 cases and 292 controls) were interviewed in the three provinces selected because of low vacci-nation coverage. On the provision of services side (supply), the main problems identified were a lack ofvaccine supply and diluent, a difficulty in maintaining the cold chain, a lack of availability and competenceamong health workers, a lack of coordination and a limited capacity to assess needs and make coherentdecisions. In the side of the consumer (demand), major obstacles identified were poor knowledge aboutmeasles immunization and difficulties in accessing vaccination centers because of distance and cost. Inmultivariate analysis, a low education level of the father was a factor of non-immunization while the
factors of good compliance were high incomes, spacing of pregnancies, a feeling that children must bevaccinated, knowledge about immunization age, presenting oneself to the hospital rather than expectingthe mobile vaccination teams and last, immunization of other family members or friends’ children. Themain factors affecting the compliance with vaccination against measles in Laos involve both the supplyside and the demand side. Obtaining an effective coverage requires upgrading and training the ExpandedProgramme on Immunization (EPI) staff and a reinforcement of health education for target populations in all provinces.. Introduction
Vaccination programs implemented during the 1990s haveeduced measles deaths worldwide by 74% between 2000 and007. However, measles was still responsible for 197,000 vaccine-reventable deaths in 2007, nearly 540 deaths per day [1].utbreaks are reported each year on different continents, but more
han 95% of measles deaths occur in low-income countries. Failureo deliver at least one dose of measles vaccine to every infant is the
ain factor for this mortality. Maintaining a rate of immunization
overage of at least 90% would prevent the spread of the virus andontrol epidemics [2,3].Although measles has been eliminated in 24 of 37 countries anderritories in the Western Pacific Region (WPR), a large number of
∗ Corresponding author. Tel.: +856 21 250509; fax: +856 21 219347.E-mail address: [email protected] (Y. Buisson).
264-410X/$ – see front matter © 2010 Elsevier Ltd. All rights reserved.oi:10.1016/j.vaccine.2010.07.077
© 2010 Elsevier Ltd. All rights reserved.
cases have been reported in 2008, including 131,441 in China (98.4cases per million inhabitants) and 11,015 in Japan (86.1 cases permillion inhabitants), these two countries representing 82% of thepopulation of WPR and over 97% of confirmed cases of measles [4].
In Laos, the elimination of measles by 2012 is part of the Mil-lennium Development Goals. It requires vaccinating at least 95%of the target population (i.e., more than 2.1 million children aged9 months to 15 years) [5,6]. Despite the introduction of measlesvaccine in the Expanded Programme on Immunization (EPI) in1982, the rates of vaccination coverage ranged from 40 to 70%in 2006–2007, revealing significant disparities between provinces,with the lowest rates being recorded in the provinces of Oudomxay(26%), Vientiane (46%) and Champasak (29%). The informationaimed at parents about the vaccination against measles, their access
to modern news media, and their social and cultural behavior havebeen cited as major determinants of vaccination compliance [7].In Lao PDR, two studies had been conducted among moth-ers of children targeted by the EPI. The first, conducted in 2004

6724 M. Phimmasane et al. / Vaccin
Table 1Immunization schedule in Lao PDR since 2007.
Vaccines Age immunization
BCG At birthMonovalent hepatitis B 24 h after childbirthDTP + HepB + OPV (dose 1) After 6 weeks
ilwctdstss
aN(
2
2amiEadg(CMttbt
3
3
pttTmf
3
coliph
DTP + HepB + OPV (dose 2) After 10 weeksDTP + HepB + OPV (dose 3) After 14 weeksMeasles 9–11 months and 12–23 months
n Sanakham district (Vientiane province), demonstrated that theevel of mothers’ education, occupation and number of children
ere factors of immunization services attendance [8]. The second,onducted in 2007 in Xaythany district (Vientiane Capital), showedhat knowledge and perception of mothers on vaccinations of chil-ren less than 3 years of age were strongly related to immunizationtatus of children [9]. Although they represent a cornerstone inhe success of measles elimination, factors associated with healthervices responsible for the EPI implementation have never beentudied.
The aim of this study was to identify factors of non-vaccinationgainst measles in Laos, related to the offer of services (from theational Immunization Program) and the consumption of services
by parents of children aged 9–23 months).
. Measles immunization in Laos
According to the Lao PDR immunization schedule updated in007, measles immunization, which is free of charge, should bedministered at 9–11 months of age and then repeated at 12–23onths [8] (Table 1). The National Center for Immunization located
n Vientiane Capital is responsible for the implementation of thePI. The National Center for Immunization supervises and evalu-tes all activities and program data at the provincial level, in theistricts, health centers and mobile teams. It includes five pro-ram areas: (1) planning and financing, (2) logistics and cold chain,3) administration, (4) statistics and research, and (5) Informationommunication Education (ICE). It is overseen by the Center forother and Child Health, which is itself placed under the control of
he Department of Hygiene and Prevention, under the authority ofhe Office of the Ministry of Health. Immunizations are carried outy primary care health center staff, who also participates in mobileeams [10].
. Patients and methods
.1. Study type
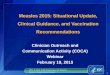
This is a descriptive and analytic study conducted in threerovinces selected for their low rates of vaccination coverage andheir geographical importance: Oudomxay in northern Laos, Vien-iane Capital in the center and Champasak in the south (Fig. 1).he study had two components: one qualitative, focused on theeasles vaccination program stakeholders, and one quantitative,
ocused on parents of children targeted for immunization.
.2. Study population
For the qualitative component, a representative sample wasonstituted involving actors at the different levels of responsibility
f the national immunization program, spreading from the centralevel down to the village health centers vaccination teams. Personsnterviewed at the central, provincial and districts levels were allublic health physicians. At the health center level, the interviewedealth workers were nurses most often inexperienced.e 28 (2010) 6723–6729
For the quantitative component, a case-control matched studyon a random sample of parents was performed. We used themethod of Quality Control Batch (CQL) recommended by the WHO[11]. For a degree of precision of ± 7% with a confidence intervalof 95%, the calculated total size of the sample was 600, esti-mated at 200 people per province. In each province, we randomlyselected one-third of districts, one-third of health centers per dis-trict and one-third of villages per health center. In each villagerandomly selected, we looked for cases (i.e., children aged 9–23months unvaccinated against measles) and controls (i.e., childrenvaccinated against measles living in the neighborhood), cases andcontrols were matched by age and sex.
Vaccination against measles was confirmed by the presentationof an authenticated document (card of vaccination). The intervie-wee was the mother or father or, if not available, the person (e.g.,grandmother, grandfather, aunt, sister, etc.) who regularly tookcare of the child and who resided with him for more than 3 monthsat a time.
3.3. Variables studied and questionnaires
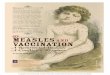
For the qualitative component, a questionnaire, constructedspecifically for the study, was designed to explore every dimen-sion of the conceptual framework, based on the literature aboutvaccination success factors (Fig. 2). This questionnaire was used insemi-structured interviews performed in the Lao language. For thequantitative survey, we developed a standardized questionnairefrom a WHO reference [11] and pre-tested it in the population toaddress the socio-demographics, immunization status of parentsand children, Knowledge Attitudes and Practices (KAP) of parentsabout measles and vaccination, including the influence of the envi-ronment and reasons for non-vaccination, availability, such as thelocation of vaccination services.
3.4. Ethics
The objectives and methods of the study were clearly explainedbefore starting interviews. Respondents had the choice to refuseto answer. All information collected was kept strictly confidential.The project was approved by the National Council of Ethics of theLao PDR.
3.5. Statistical analysis
The responses collected in the qualitative survey were analyzedto highlight the different dimensions of the conceptual framework.Validity of the analyses was based on a triangulation procedure(cross-checking of ideas from multiple sources), and a double cod-ing of information by two researchers. Data from the quantitativesurvey were treated on Epidata 3.1 and Stata 8.2. Comparisons weremade using Chi2 test for discrete variables and t test for continu-ous variables with a significance level of 5%. Multivariate analyseswere used to identify factors independently associated with non-vaccination.
4. Results
4.1. Qualitative survey of the vaccination program stakeholders
Each dimension of the conceptual framework was identifiedamong the reasons cited by interviewed persons to explain the
variance of measles vaccination in the country. On the provision ofservices side, key factors affecting the achievement of satisfactoryvaccine coverage were inadequate supplies of vaccine and diluents,difficulties in maintaining the cold chain (due to a lack of fridges,lack of ice for mobile teams, and frequent power cuts that affect
M. Phimmasane et al. / Vaccine 28 (2010) 6723–6729 6725
tion o
mhiaoatib
4m
tl(n
Fig. 1. Loca
any health care centers generally devoid of electric generators),ealth workers’ poor knowledge regarding their vaccination tasks
ncluding the importance of maintaining products at low temper-ture, lack of possibility to assume their responsibilities, lack ofrganization and coordination, and a weak capacity to assess needsnd make coherent decisions. On the consumer side, the main fac-ors were a lack of knowledge about measles immunization and itsmpact on health and the difficulties of access to vaccination sitesecause of distance or travel costs.
.2. Case-control survey among parents of children aged 9–23onths
Univariate analysis of sociodemographic data showed five fac-ors to be positively associated with vaccination of children: highevel of education of father (p = 0.001), good monthly incomep = 0.0006), large interval between pregnancies (p < 0.02), immu-ization status of mother (p = 0.001) and the practice of not giving
f the study.
birth at home (p < 0.0001) (Table 2). The KAP analysis revealed thatknowledge about measles and measles vaccination (i.e., number ofinjections, injection site, age, side effects and benefits of vaccina-tion) was significantly related to immunization of children.
The availability of health personnel at the vaccination cen-ter, as well as the quality of welcome and service, were similarlyappreciated by cases and controls. The only significant differenceconcerned the congratulations sometimes addressed by the physi-cian to the parents who came to immunize their child (p = 0.04);they seemed to encourage vaccination. The distance from the cen-ter of vaccination was a factor of non-vaccination (p = 0.01). Theopening hours of the vaccination center and the waiting time beforeinjection were not mentioned more often by cases than controls.
The influence of family or friends and the immunization status ofchildren in the family or friends were factors related to vaccination.Among the reasons for non-vaccination given by parents, fear ofinjections or side effects, lack of parents’ availability, remoteness ofthe place of vaccination, perception of ineffectiveness of the vaccine

6726 M. Phimmasane et al. / Vaccine 28 (2010) 6723–6729
ptual
ohvs
TS
Fig. 2. Conce
r benignity of measles, requirement to wait for the mobile team,
ealth condition of the child (i.e., to not perceive the advantage ofaccinating a child who seemed to be healthy) and poverty wereignificantly more cited by cases than controls (Table 3).able 2ociodemographic characteristics of the study population.
Variables Total (%)N = 584
IntervieweesAverage age 30.99CI 95% (30.09–31.88)Mothers 473 (80.99)Other relatives 111 (19.01)Age: <30 years 337 (57.71)30–40 years 158 (27.05)>40 years 89 (15.24)ChildrenAverage age 16.27CI 95% (15.81–16.74)IlliteracyFather 173 (30.78)Mother 285 (48.89)Mean number of people in the household 5.98CI 95% (5.79–6.17)Average income (USD) 89.59CI 95% (82.58–96.60)Average number of children 2.09CI 95% (1.98–2.21)Average interval between pregnancies 3.97CI 95% (3.67–4.27)UnvaccinatedFathers 309 (52.91)Mothers 145 (24.83)ChildbirthAt home 226 (38.70)In hospital 358 (61.30)
a No significant.
framework.
In multivariate analyses, low education level of father was
a factor of non-vaccination (OR = 1.67, p = 0.003). Factors inde-pendently associated with vaccination against measles werehigh income level (OR = 0.99, p = 0.008), spacing of pregnancies(OR = 0.88, p = 0.03), the belief that children must be vaccinatedCases (%) Controls (%) pN =292 N = 292
31.13 30.84(29.80–32.47) 29.64–32.04 NSa
234 (80.14) 239 (81.85)58 (19.86) 53 (18.15) NS165 (56.51) 172 (58.90)
77 (26.37)43 (14.73)
}NS81 (27.74)
46 (15.75)
16.18 16.37 NS(15.52–16.84) (15.71–17.03)
102 (36.56) 71 (25.09) 0.001151 (51.89) 134 (45.87) NS6.09 5.86(5.82–6.37) (5.59–6.13) NS77.46 101.72(69.62–85.31) (90.22–113.2) <0.0002.20 1.99(2.02–2.37) (1.85–2.13) NS3.63 4.30(3.21–4.06) (3.88–4.71) 0.02
165 (56.51) 144 (49.32) 0.00188 (30.14) 57 (19.52) NS
139 (47.60) 87 (29.79)153 (52.40) 205 (70.21) <0.000

M. Phimmasane et al. / Vaccine 28 (2010) 6723–6729 6727
Table 3Univariate analysis of non-vaccination reasons advanced by parents.
Variables Cases (%) Controls (%) OR CI 95% p
Fear of side effects 182 (62.33) 104 (35.62) 4.39 2.79–6.90 <0.0001Fear of injections 154 (52.74) 92 (31.51) 2.77 1.88–4.07 <0.0001Parents too busy 59 (20.21) 21 (7.19) 5.22 2.55–10.65 <0.0001Travel difficulties 5 (1.71) 2 (0.68) 4 0.44–35.78 NSDistance to vaccination center 21 (7.19) 8 (2.74) 3.16 1.26–7.92 0.007Non-effectiveness of the vaccine 8 (2.74) 2 (0.68) 7 0.86–56.89 0.02Traditional belief 6 (2.05) 4 (1.37) 1.5 0.42–5.31 NSIgnorance– Need for vaccination 44 (15.07) 27 (9.25) 1.94 1.10–3.43 0.01– Seriousness of measles 7 (2.40) 1 (0.34) 7 0.86–56.89 0.02– Benefits of vaccination 15 (5.14) 8 (2.74) 2.4 0.84–6.81 NSNeed to wait for the mobile team 10 (3.42) 4 (1.37) 7 0.86–56.89 0.02Poverty 23 (7.88) 7 (2.40) 17 2.26–127.74 <0.0001Health condition of children 40 (13.70) 19 (6.51) 2.4 1.31–4.38 0.002
Table 4Multivariate analysis of factors affecting vaccination.
Variables OR CI 95% p
Low level of education of father 3.74 1.55–9.02 0.003High income level 0.99 0.98–0.99 0.008Interval between pregnancies >4.3 years 0.88 0.78–0.99 0.03Belief that children must be vaccinated 0.09 0.01–0.45 0.003Knowing the age of vaccination 0.27 0.09–0.79 0.01
00
(pto(
5
vctfitTr
Vaccination at the hospital rather than by the mobile teamVaccinal status of other children in the family
OR = 0.09, p = 0.003), knowing the age of vaccination (OR = 0.27,= 0.01), presenting oneself to the hospital rather than expecting
he mobile vaccination teams (OR = 0.20, p = 0.03) and the fact thatther children in the family were vaccinated (OR = 0.36, p = 0.02)Table 4).
. Discussion
In order to identify comprehensively the factors involved in non-accination of Lao children against measles, this study included twoomponents, a qualitative one and a quantitative one. The qualita-
ive approach was chosen to explore unknown or poorly exploredelds: it consisted of interviews with professionals involved inhe implementation and functioning of the vaccination program.he quantitative approach aimed at confirming and clarifying theesults of the qualitative survey and at identifying additional infor-Fig. 3. Sample of pop
.20 0.05–0.86 0.03
.36 0.15–0.86 0.02
mation: it focused on parents of children aged 9–23 months, whoare the targets of measles vaccination. This is the first time that suchinvestigation is conducted in Laos to identify the main obstacles toobtaining adequate vaccine coverage.
The representativeness of the results is satisfactory; the samplesize calculated by the method of Quality Control Batch has beenachieved in the three provinces. Only 16 people refused to respondto the questionnaire, claiming lack of time or because of difficul-ties in understanding the Lao language in ethnic minorities (Fig. 3).The survey was conducted on only 3 of the 18 provinces of Lao PDR,deliberately chosen for their low immunization coverage in order to
better identify key factors of non-vaccination. Possible informationbias must be considered, associated with poor recall of vaccinationand medical history or with a lack of sincerity, as some respon-dents may have been possibly ashamed to give an answer not inaccordance with the expected response.ulation studied.

6 accin
fi
spaicptarbnkbarihtevcatr
oivcev[
aetrtllacattf
ior
ecdthassris
[
[
[
[
[
728 M. Phimmasane et al. / V
What did we learn from the qualitative component? First, theactors associated with poor vaccination coverage most often citedn the literature are also found in Lao PDR.
The main factors affecting the provision of care are inadequateupply of vaccines and diluents, discontinuity of the cold chain,oor training of health workers regarding their vaccination tasksnd inability to perform them. The maintenance of the cold chains particularly difficult under the current conditions: some healthare centers have no fridge or no working fridge, there are frequentower cuts and health care centers usually do not have elec-ric generators. Moreover, some villages are at hours-motorbikend walking distance from health care centers, making the use ofefrigerated box irrelevant. There is also insufficient coordinationetween relevant organizations to assess the needs and make ratio-al decisions. The main factors affecting the demand are lack ofnowledge about the prevention of measles, not only in familiesut also among health workers and village chiefs. These personsre generally uninformed about the benefits of vaccination. Nurseseceive little training in vaccination. Most knowledge is acquiredn the field. However, experienced nurses seldom remain at theealth center level. As soon as better paid job opportunities arise,hey leave, being replaced by young ones with little or no knowl-dge about vaccines. Families did not perceive the advantage ofaccinating a child who seemed to be healthy. They have miscon-eptions about the risks. Moreover, poverty and lack of parents’vailability, who often have several children and cannot leaveheir work, reduce ability to access vaccination centers that areemote.
These results were confirmed in the quantitative componentf the study. The level of parents’ knowledge about measles andts prevention is indeed a major determinant in the decision toaccinate their child [12]. Conversely, distance to the vaccinationenters or inadequate supplies of vaccine might discourage par-nts to return if they could not vaccinate their child during the firstisit. Similar results were reported in studies conducted in Africa13–16].
Some determinants are highlighted by the quantitative survey,s the expectation of visits by the mobile team and the low level ofducation of the father. The distance to the center of vaccination,he lack of public transport and poor road conditions affect manyural families. Parents prefer to wait for the possible tour of a mobileeam to avoid costs and delays. As these teams cannot visit every vil-age for logistical reasons, children waiting for their arrival are moreikely not to be vaccinated. This factor of incomplete vaccination haslso been reported in Turkey and Pakistan [17,18]. The factor “edu-ation of the father” seems related to the traditional Lao culture:s chief of family, the father makes all decisions, including vaccina-ion of children. Other studies have emphasized the importance ofhe educational level of the mother, but these investigations wereocused on mothers of children targeted for vaccination [8,19,20].
How can these results help to achieve and maintain a highmmunization coverage against measles in Laos? Two main linesf action emerge: information on measles and its prevention, andeorganization of the immunization services.
This study emphasizes the need to adapt and maintain healthducation to target sub-groups of the population (i.e., villagers,hiefs of village and health workers). In a cross-sectional study con-ucted in the Lasbela district in southern Pakistan, it appeared thathe discussions about vaccines and knowledge about the vaccinead a positive impact on immunization against measles in urbannd rural areas, regardless of the negative effect of determinants
uch as access, maternal education and household socio-economictatus [21]. Similarly, Laos is a multi-ethnic country. The literacyate is still low. Sub-groups specific messages are desirable tak-ng into account the cultural characteristics. The rural population,teeped in traditional culture, is not accessible to messages using[
[
e 28 (2010) 6723–6729
Western-style arguments. The demographic diversity justifies non-standard approaches, adapted to the cultural specificities of eachethnic group. Involvement of anthropologists in the design of publichealth programs would make health messages more understand-able, leading to a better appropriation by the population.
On the offer of services side, these results show that the currentsystem does not adequately meet the needs of the population. Diffi-cult access to health centers justifies the implementation of mobileteams, provided they can operate at night, when families in villagesare together and available. This also requires the cooperation of thechiefs of village who will provide the exact number of children tar-geted for measles vaccination. Moreover, the population should beinformed about the fact that vaccination is free of charge, contraryto consultations for illness. Also, some simple solutions to the main-tenance of the cold chain should be considered, as providing eachhealth care centers with a working fridge and an electric generator.Finally, measles vaccine being one of the most heat-sensitive vac-cines, the use of vaccine vial monitors (VVM) should be encouragedin order to pinpoint the cold chain problems and reduce vaccinewasting [22].
Taking into account the factors of non-vaccination againstmeasles in Laos is a prerequisite to achieve optimal immunizationcoverage to reach the elimination target set for 2012 by WHO.
Acknowledgments
This study was funded by the Agence Universitaire de la Franco-phonie (AUF) and the Institut de la Francophonie pour la MédecineTropicale (IFMT).
We express our gratitude to the provincial and district healthauthorities of Lao PDR as well as personal of health centers for theirhelp in our work.
We thank Mark A. Fletcher for critical reading of the manuscript.
References
[1] WHO. Measles mortality reduction: a successful initiative; 2008,http://www.who.int/entity/immunization/newsroom/measles/en/.
[2] WHO/UNICEF. Global plan for the mortality reduction due to measles2006–2010. WHO/IVB/05.11. 2006.
[3] WHO. Progress in global measles control and mortality reduction, 2000–2007.WER 2008;83:441–8.
[4] CDC. Progress toward the 2012 measles elimination goal—Western PacificRegion, 1999–2008. MMWR 2009;58(24):669–73.
[5] National Immunization Center. Report the successful organization of thenational day of the vaccination against measles in November 2007 in Lao PDR.2008:1–24.
[6] UNICEF. Nationwide push in Lao PDR to eliminate measles. 16 November 2007.http://www.unicef.org/infobycountry/laopdr 41824.html.
[7] Jheeta M, Newell J. Childhood vaccination in Africa and Asia: the effect of par-ents’ knowledge and attitudes. Bull WHO 2008;86(6):419.
[8] Shiyalap K, Siharath D, Chamroonsawasdi K. Maternal utilization of immuniza-tion services for their children aged 2–5 years in Sanakham District, VientianeProvince, Lao PDR. J Public Health Dev 2004;2(3):37–49.
[9] Phouphenghack K, Khamsrichan W, Vorakitpokatorn S. Knowledge and per-ception of mothers about immunization of children under 3 years of age in theXaythany District, Vientiane, Lao P.D.R. J Public Health Dev 2007;5(3):107–16.
10] National Immunization Center. Plan of action measles catch up campaign SIA2007 in Lao PDR. 2007:7–8.
11] WHO. The survey method by Quality Control Batch. Global programfor vaccines and immunization. Research-development on vaccines.WHO/VRD/TRAM/96.1. 1997:7–16.
12] Alfredsson R, Svensson E, Trollfors B, Borres MP. Why do parents hesitate tovaccinate their children against measles, mumps and rubella? Acta Paediatr2004;93(9):1232–7.
13] Ndiaye NM, Ndiaye P, Diedhiou A, et al. Factors related to failure to com-plete immunization of children aged 10–23 months in Ndoulo (Senegal). Sante2009;19(1):9–13.
14] Jani JV, Schacht CD, Jani IV, Bjune G. Risk factors for incomplete vaccination
and missed opportunity for immunization in rural Mozambique. BMC PublicHealth 2008;8:161.15] Makoutode M, Mohamed S, Paraiso NM, et al. Impact of parental attitudes oninfant vaccinal coverage in Benin. Med Trop 2009;69:267–71.
16] Odusanya OO, Alufohai EF, Meurice FP, Ahonkhai VI. Determinants of vaccina-tion coverage in rural Nigeria. BMC Public Health 2008;8:381.

accin
[
[
[
[Indian J Pediatr 2007;74(2):131–4.
[21] Mitchell S, Andersson N, Ansari NM, et al. Equity and vaccine uptake: a cross-
M. Phimmasane et al. / V
17] Harmancı H, Gürbüz Y, Torun SD, et al. Reasons for non-vaccination duringnational immunization days: a case study in Istanbul, Turkey. Public Health2003;117(1):54–61.
18] Cockcroft A, Andersson N, Omer K, et al. One size does not fit all: local determi-nants of measles vaccination in four districts of Pakistan. BMC Int Health HumRights 2009;9(Suppl. 1):S4.
19] Elliott C, Farmer K. Immunization status of children under 7 years in theVikas Negar area, North India. Child Care Health Dev 2006;32(4):415–21.
[
e 28 (2010) 6723–6729 6729
20] Chhabra P, Nair P, Gupta A, et al. Immunization in urbanized villages of Delhi.
sectional study of measles vaccination in Lasbela District, Pakistan. BMC IntHealth Hum Rights 2009;9(Suppl. 1):S7.
22] WHO. Getting started with vaccine vial monitors; 2002 http://whqlibdoc.who.int/hq/2002/WHO V&B 02.35.pdf.