Embed Size (px)
Citation preview
O R I G I N A L A R T I C L E
Factors affecting microbial contamination rate of cord bloodcollected for transplantation_3507 1..8
Pamela Clark, Annnette Trickett, Damien Stark, and Marcus Vowels
BACKGROUND: Collection and processing of cordblood (CB) is associated with significant risk of micro-bial contamination and hence relevant standardsmandate microbial screening of the final product. Thisstudy aimed to determine the contamination rate andassociated risk factors during 14 years of banking atthe Sydney Cord Blood Bank.STUDY DESIGN AND METHODS: CB was collectedand processed using a closed system and tested forcontamination using blood culture bottles (BacT/ALERT,bioMérieux) incubated for a minimum of 5 days. Fourmicrobial screening methods were used with differentcombinations of inoculated bottles (adult or pediatric)and associated sample volumes (10 or 1 mL).RESULTS: Of 13,344 CB units screened, 537 (4.0%)tested positive for contamination, with Bacteroides spp.(20.9%), Staphylococcus spp. (18.6%), and Propioni-bacterium spp. (13.7%) being the most common iso-lates. The contamination rate reduced from 10% in1997 to 1.1% in 2009. Multivariate analysis demon-strated the following variables were independently asso-ciated with higher contamination rates: vaginal delivery,collection by obstetric staff, and use of an anaerobicbottle in addition to an aerobic bottle (which facilitated alarger sample inoculation volume than pediatric bottles).CONCLUSIONS: This study demonstrates that con-tamination rates of CB collected for transplantation canbe substantially reduced by collection after cesareandelivery and utilizing trained CB collection staff. Thesedata also indicate that the common practice of testingusing a pediatric (aerobic) bottle with its attendant smallvolume of the final CB product may be suboptimal forsensitive detection of contaminating anaerobicmicrobes.
Regulatory requirements mandate that microbialscreening is performed on all cord blood (CB)banked for transplantation and that contami-nated products are excluded. Standards rel-
evant to CB banking require microbial cultures to beperformed on the final CB product using a system vali-dated for growth of anaerobic and aerobic bacteria andfungi.1,2 None of the standards applicable to cord bloodbanks (CBBs) prescribe how to perform the microbialscreening. Most CBBs test a small sample of the CB(�1 mL) that is substantially smaller than the manufac-turer’s recommendation (3-4 mL) for pediatric bottles inautomated blood culture systems.
Collection and/or processing of CB is associated witha significant risk of microbial contamination, as evi-denced by reported contamination rates of 0% to 48%.3-11
Factors that have been reported to be linked with higherrates of microbial contamination include CB collectionfrom vaginal deliveries with the placenta in utero.3
However, there has been no systematic evaluation of thecontribution of these factors.
Infusion of contaminated hematopoietic progenitorcell (HPC) products has not generally been associatedwith adverse clinical sequalae when given with prophylac-tic antibiotic therapy,10,12 although an increase in duration
ABBREVIATIONS: CB = cord blood; CBB(s) = cord blood
bank(s); CBU(s) = cord blood units; SCBB = Sydney Cord Blood
Bank.
From the Sydney Cord Blood Bank, Sydney Children’s Hospital,
Randwick, NSW; the University of New South Wales, Sydney,
NSW; the NSW Agency for Clinical Innovation BMT Network,
Darlinghurst, NSW; and the Division of Microbiology, SydPath,
St Vincent’s Hospital, Darlinghurst, NSW, Australia.
Address reprint requests to: Pamela Clark, Sydney Cord
Blood Bank, Level 3, Clinical Sciences Building, High Street,
Randwick, NSW 2031, Australia; e-mail: Pamela.Clark@
student.unsw.edu.au.
Received for publication August 9, 2011; revision received
October 17, 2011, and accepted November 11, 2011.
doi: 10.1111/j.1537-2995.2011.03507.x
TRANSFUSION **;**:**-**.
Volume **, ** ** TRANSFUSION 1
of hospitalization and patient death has been reported.12,13
Such risks emphasize the need for a CBB to reduce poten-tial contamination during collection and manufactureof CB.
There are three public CBBs in Australia that com-prise AusCord, the Australian network of CBB. AusCordincludes the Sydney Cord Blood Bank (SCBB); the BMDICBB, Melbourne; and the Queensland CBB at the Mater.The AusCord CBBs apply consistent quality parameters toCB banking in line with current FACT standards1 andTherapeutic Goods Administration (TGA) regulations14
and do not release CB known to contain microbial con-tamination. There is, however, a potential risk that screen-ing methods may be inadequate to detect all organisms,especially low-level and fastidious contaminants.
At the SCBB, microbial contamination rates have gen-erally decreased over time as quality improvements havebeen implemented. Changes include modifications tocord antiseptics used, microbial screening methodology,volume of CB tested, and stage of product sampling.Hence this study was undertaken to evaluate which ofthese factors affect the microbial contamination rate of CBbanked for transplantation.
MATERIALS AND METHODS
Data setThis retrospective study included all CB that met theinitial acceptance criteria for processing at the SCBB fromthe commencement of banking in 1995 until the time ofdata analysis in 2009. CB that did not have results formicrobial screening was excluded from the analysis.
Relevant data were extracted from the SCBB elec-tronic database into a computer spreadsheet (Excel,Microsoft Corp., Redmond, WA). All extracted data from asample of 1000 CB records was verified by checkingagainst the hard copy files. Since some sets of electronicdata were found to have entry errors in variables such ascollection and processing dates, such data was reenteredmanually (for all CB data sets identified with errors) intothe spreadsheet before analysis, and these fields were thenchecked and, if necessary, corrected on the whole data set.
Variables in the analysis included year of CB collec-tion, collector details (SCBB or obstetric unit staff), deliv-ery mode (cesarean or vaginal), type of cord antisepticused (70% isopropanol or chlorhexidine-cetrimide), dura-tion of storage between collection and processing (0-2days), and microbial screening method.
The files for the 537 CB units (CBUs) known to becontaminated were manually reviewed and the bottle typepositive for contamination was recorded. The detectionrate of each bottle type (aerobic, anaerobic, or pediatric)was calculated according to the organism type detected(all, aerobe, or obligate anaerobe). Early records did not
specify the bottle type in which growth was detected, andhence these were excluded from this analysis.
CB collection, processing, and cryopreservationInformed consent was obtained before collection of all CBunder an ethics committee approved protocol. CB wasobtained at fixed collection centers, by dedicated SCBBstaff, and trained or (in early years of banking) nontrainedobstetric staff at the participating hospital, after the birth ofthe baby by either vaginal delivery or cesarean section. CBwas collected using standard protocols. Briefly, after cordantisepsis with 70% isopropanol or chlorhexidine glucon-ate (0.015%)-cetrimide (0.15%) solution, blood was drainedinto the collection bag by gravity with the placenta in situ(in utero) or after the placenta was delivered (ex utero).
Initially, in 1995, CBUs were frozen without under-going volume reduction processing. The New York(Pentaspan/Hespan) method was introduced in February1996 and then changed to the current Optipress method15
in September 1997. The CBUs were maintained in aclosed-bag system apart from the removal of samples andthe addition of the cryopreservation agent (10% dimethylsulfoxide/1% Dextran 40). The final products were cryo-preservered in a volume between 35 and 60 mL and thenmaintained at or below -150°C.
CB microbial samplingAfter inoculation of culture bottles (BacT/ALERT,bioMérieux, Marcy l’Etoile, France) as described for thefour methods below, bottles were forwarded to a diagnos-tic laboratory (SEALS Microbiology, Kogarah, NSW, Aus-tralia) and incubated in a microbial detection system(BacT/ALERT 3D, bioMérieux) as per the manufacturer’sinstructions. If a positive culture was detected, the labo-ratory identified the organism.
• Method 1 utilized a 20-mL sample taken from thediscard plasma bag split equally and inoculated intoBacT/ALERT FA (FAN aerobic) and BacT/ALERT FN(FAN anaerobic) “adult” culture bottles.
• Method 2 utilized a 1-mL sample taken from the finalproduct immediately before freezing, inoculated intoa single BacT/ALERT PF (FAN, low volume) “pediat-ric” bottle.
• Method 3 utilized a 10-mL sample taken from theplasma discard inoculated into an anaerobic adultbottle and a 1-mL sample taken from the finalproduct inoculated into a pediatric bottle.
• Method 4 utilized a 20-mL sample taken from thediscard plasma bag split equally and inoculated intoan aerobic and an anaerobic adult culture bottle. Inaddition, a 1-mL sample was taken from the finalproduct immediately before freezing, inoculated intoa single pediatric bottle.
CLARK ET AL.
2 TRANSFUSION Volume **, ** **
Statistical analysisWith the use of univariate analysis, theincidence of contamination in CB wascross-tabulated by a number of factors(cleaning antiseptic, mode of delivery,collector type, time to inoculation, earlyyears of banking, and type of culturebottle used for testing), and significanteffects were assessed by a chi-squaredtest.
Based on the results of univariateanalysis, a multivariate logistic regres-sion was performed on data from 2000forward (excluding the early years ofbanking) to find factors with indepen-dent significant effects on the contami-nation rate. CB collected from 1995 to1999 was excluded from the multivari-ate analysis due to substantially highercontamination rates before 2000, whichcorrespond to published reports of highcontamination associated with thestart-up years of a CBB. Statistical testswere carried out in a software package(Statistical Package for the Social Sciences [SPSS], Version19.0, SPSS, Inc., Chicago, IL). Values of p less than 0.05were considered significant.
RESULTS
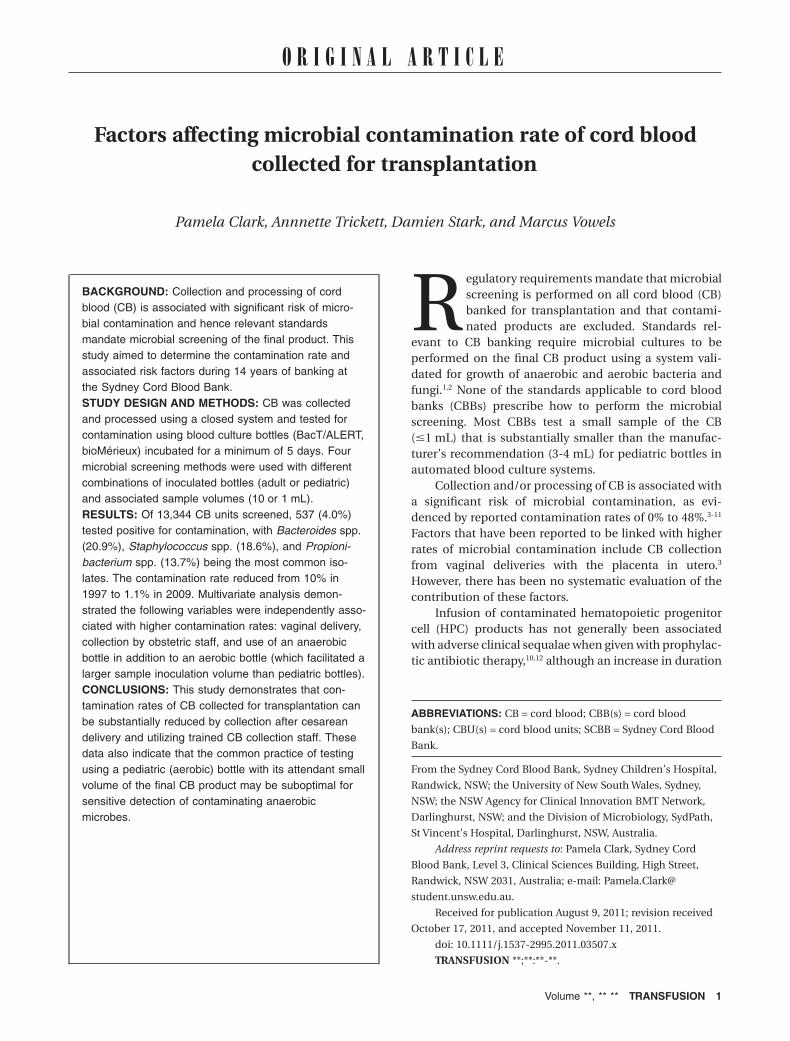
Contamination rate and microbes identifiedA total of 13,344 CBUs were collected, processed, andtested for microbial contamination at the SCBB between1995 and 2009. Of these, 537 tested positive for microbialcontamination resulting in a total contamination rate of4.0%. Over the 14-year period, 9040 CB collections wereobtained from vaginal deliveries with 489 resulting inpositive microbial cultures, a contamination rate of 5.4%.An additional 4228 CB collections were obtained fromcesarean deliveries, with 46 positive microbial cultures, acontamination rate of 1.1%. The contamination rates overtime are summarized in Fig. 1.
A wide variety of microbes have been isolated fromthe CB samples, with skin (38.4%) and gastrointestinalflora (33.9%) being the most frequent organisms. Environ-mental contaminants (6.5%) and vaginal flora (1.8%) werealso detected. The more common microbes detected arelisted in Table 1.
The majority of the cultures were reported asmonomicrobial, although 4.8% were polymicrobial. Theroutine procedure for microbial screening of CB in thisstudy involved unloading bottles from the BacT/ALERTsystem as soon as they signaled positive for subsequentsubculture and identification. Due to this practice, it ispossible that more contaminant organisms were present
in samples but undetected because they had not reacheddetectable levels at the time the bottle was unloaded forthe profuse organism.
Effect of microbial screening methodContamination rates observed with the four sequentialsampling methods are summarized in Table 2 and Fig. 1.The detection rate for all four methods has rangedbetween 1.5 and 5.6% over the 14-year period. The lowestdetection rate was for Method 2 (inoculation of finalproduct into a pediatric bottle only), which used thelowest total inoculation volume of 1 mL.
Fig. 1. SCBB contamination rates per financial year from 1996 to present. Data from
1995 to 1996 were excluded from the analysis since fewer than 50 CB products were
processed during that period. Methods 1 to 4 refer to the usage periods for microbial
screening as per Table 2.
TABLE 1. Frequency of microbial organismsisolated
Potential contamination source Frequency (%)
Skin flora 38.4Staphylococcus spp., coagulase negative (17.5)Propionibacterium spp. (13.7)Diphtheroids (Coryneforms) (4.5)Micrococcus spp. (1.6)Staphylococcus aureus (1.1)
Gastrointestinal tract flora 33.9Anaerobes (26.5)Enterobacteriaceae (7.4)
Environmental contaminants 6.5Bacillus spp. (4.0)Pseudomonads (2.5)
Vaginal flora 1.8Group B streptococci (S. agalacticae) (1.4)Lactobacillus spp. (0.2)Candida albicans (0.2)
CONTAMINATION FACTORS OF CORD BLOOD
Volume **, ** ** TRANSFUSION 3
Microbial screening using a sample from the plasmadiscard fraction into aerobic and anaerobic cultures(Method 1) yielded a contamination rate of 5.6%. Uponchanging the screening method to a 1-mL sample of thefinal product (Method 2), the contamination rate droppedto the lowest level detected of 1.5% (p < 0.001). After rein-troduction of an adult anaerobic bottle inoculated withplasma discard in addition to the final product screen(Method 3), a contamination rate of 3.6% was observed.More recent modification of the microbial screeningmethod, to include the original method of testing plasmadiscard in aerobic and anaerobic cultures as well as testingthe final product (Method 4), yielded a contamination rateof 2.2%.
Type of organism identified by type of culturebottle usedTable 3 summarizes the detection rate of organisms ineach bottle type. Aerobic and facultative anaerobic organ-isms were detected in all three bottle types. However, forobligate anaerobic organisms, a detection rate of 98% wasobserved in the adult anaerobic bottle compared to 8% inthe pediatric bottle and 2% in the adult aerobic bottle(p < 0.001).
Since Method 4 utilized all culture bottle types, thisdata set was further analyzed for patterns of positivity. Allobligate anaerobes were only detected in a single bottlefor each CBU. Of the 33 obligate anaerobes detected, 94%were only detected in the adult anaerobic bottle, 3% only
in the adult aerobic bottle, and 3% onlyin the pediatric bottle. Of the 48 aerobicand facultative organisms observed,85% were detected in a single bottle(69% in the pediatric bottle, 4% in theadult aerobic, and 12% in the anaerobicbottle). Four percent of organisms weredetected by both the pediatric and theaerobic bottles, another 4% by the pairof adult bottles, and 6% were detected inall three bottles.
Other factors influencing contamination rateThe effect of cleaning antiseptic, mode of delivery, collec-tor type, time to inoculation, early years of banking, andtype of culture bottle used for testing in relation to the rateof bacterial contamination at the SCBB are summarized inTable 4. On univariate analysis, cesarean deliveries (1.1%)gave a lower contamination rate than vaginal births (5.4%;p < 0.001) and CB collected by SCBB staff resulted in asignificantly lower contamination rate of 3.5% than whencollected by obstetric staff (4.8%; p < 0.001). Further,cleaning of the umbilical cord with 70% isopropanolwas associated with 4.4% contamination whereaschlorhexidine-cetrimide yielded 1.3% (p < 0.001). CB thatwas processed 2 days after collection resulted in a highercontamination rate of 8.5% compared to cords processedon the same or next day from collection (5.0 and 3.9%,respectively; p = 0.003). Additionally, CB banked in theearly years before established standard protocols andquality enhancements resulted in a higher contaminationrate (7.9%) than CB banked from 2000 onward (3.1%;p < 0.001).
Since many of the factors assessed in the univariateanalysis are potentially interrelated, a multivariate logisticregression model was used to further evaluate the findings(Table 5). CBUs collected during the initial years of banking(1995-1999) were excluded from this latter analysis. Inde-pendent significant risk factors for higher contaminationrates were CB collected from vaginal delivery, collection byobstetric staff, and screening with an adult anaerobic
TABLE 2. Summary of microbiologic screening methods at the SCBB including contamination ratesMethod Date in use Bottle Sample Volume (mL) Contaminated/total Contamination rate (%)
1 Jun 1995-Oct 2002 Adult aerobic Plasma discard 10 345/6,213 5.6Adult anaerobic Plasma discard 10
2 Oct 2002-Feb 2003 Pediatric Final product 1 6/410 1.53 Feb 2003-Jan 2005 Adult anaerobic Plasma discard 10 103/2,871 3.6
Pediatric Final product 14 Jan 2005-Jun 2009 Adult aerobic Plasma discard 10 83/3,850 2.2
Adult anaerobic Plasma discard 10Pediatric Final product 1
Total 537/13,344 4.0
TABLE 3. Breakdown of organism detection per bottle type*
Organism type detected
Detection rate per bottle type: contaminated/sample,size n/N (%)
Aerobic Pediatric Anaerobic
All organisms 32/124 (26) 76/190 (40) 158/223 (71)Aerobes/facultative
anaerobes31/76 (41) 69/98 (70) 56/119 (47)
Obligate anaerobes 1/48 (2) 7/92 (8) 102/104 (98)
* Data before May 3, 2002, were excluded from the analysis since the first 305 positiveculture reports did not specify which bottle type was positive for contamination.
CLARK ET AL.
4 TRANSFUSION Volume **, ** **
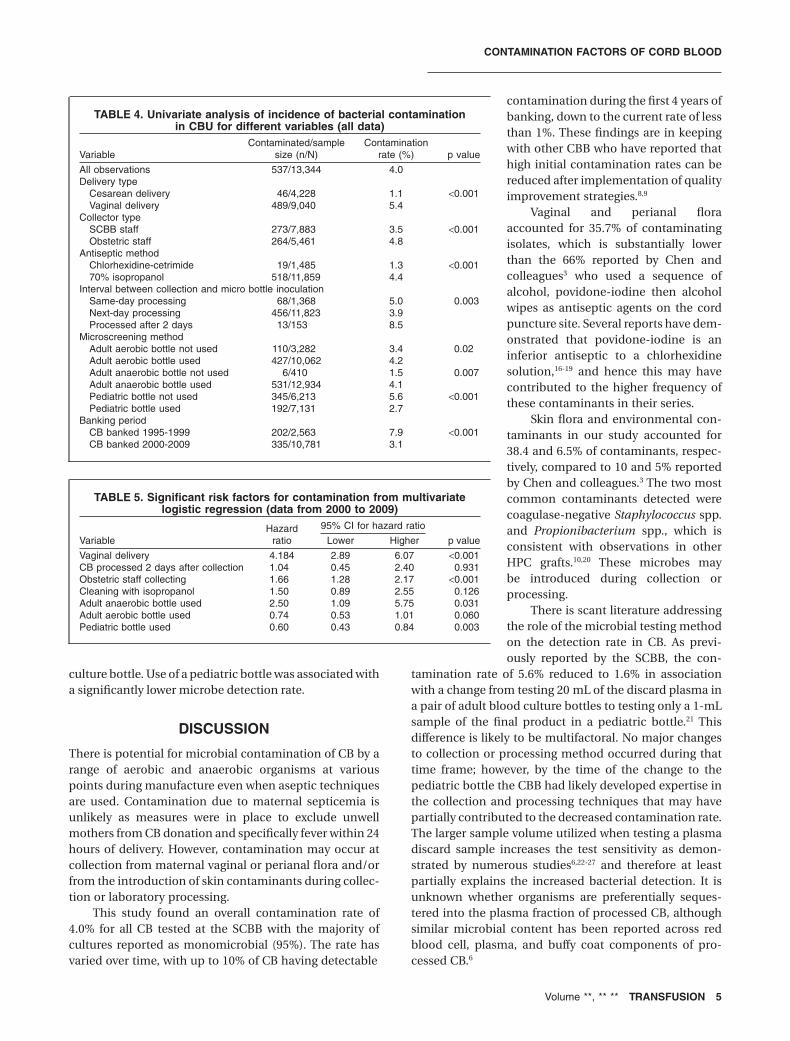
culture bottle. Use of a pediatric bottle was associated witha significantly lower microbe detection rate.
DISCUSSION
There is potential for microbial contamination of CB by arange of aerobic and anaerobic organisms at variouspoints during manufacture even when aseptic techniquesare used. Contamination due to maternal septicemia isunlikely as measures were in place to exclude unwellmothers from CB donation and specifically fever within 24hours of delivery. However, contamination may occur atcollection from maternal vaginal or perianal flora and/orfrom the introduction of skin contaminants during collec-tion or laboratory processing.
This study found an overall contamination rate of4.0% for all CB tested at the SCBB with the majority ofcultures reported as monomicrobial (95%). The rate hasvaried over time, with up to 10% of CB having detectable
contamination during the first 4 years ofbanking, down to the current rate of lessthan 1%. These findings are in keepingwith other CBB who have reported thathigh initial contamination rates can bereduced after implementation of qualityimprovement strategies.8,9
Vaginal and perianal floraaccounted for 35.7% of contaminatingisolates, which is substantially lowerthan the 66% reported by Chen andcolleagues3 who used a sequence ofalcohol, povidone-iodine then alcoholwipes as antiseptic agents on the cordpuncture site. Several reports have dem-onstrated that povidone-iodine is aninferior antiseptic to a chlorhexidinesolution,16-19 and hence this may havecontributed to the higher frequency ofthese contaminants in their series.
Skin flora and environmental con-taminants in our study accounted for38.4 and 6.5% of contaminants, respec-tively, compared to 10 and 5% reportedby Chen and colleagues.3 The two mostcommon contaminants detected werecoagulase-negative Staphylococcus spp.and Propionibacterium spp., which isconsistent with observations in otherHPC grafts.10,20 These microbes maybe introduced during collection orprocessing.
There is scant literature addressingthe role of the microbial testing methodon the detection rate in CB. As previ-ously reported by the SCBB, the con-
tamination rate of 5.6% reduced to 1.6% in associationwith a change from testing 20 mL of the discard plasma ina pair of adult blood culture bottles to testing only a 1-mLsample of the final product in a pediatric bottle.21 Thisdifference is likely to be multifactoral. No major changesto collection or processing method occurred during thattime frame; however, by the time of the change to thepediatric bottle the CBB had likely developed expertise inthe collection and processing techniques that may havepartially contributed to the decreased contamination rate.The larger sample volume utilized when testing a plasmadiscard sample increases the test sensitivity as demon-strated by numerous studies6,22-27 and therefore at leastpartially explains the increased bacterial detection. It isunknown whether organisms are preferentially seques-tered into the plasma fraction of processed CB, althoughsimilar microbial content has been reported across redblood cell, plasma, and buffy coat components of pro-cessed CB.6
TABLE 4. Univariate analysis of incidence of bacterial contaminationin CBU for different variables (all data)
VariableContaminated/sample
size (n/N)Contamination
rate (%) p value
All observations 537/13,344 4.0Delivery type
Cesarean delivery 46/4,228 1.1 <0.001Vaginal delivery 489/9,040 5.4
Collector typeSCBB staff 273/7,883 3.5 <0.001Obstetric staff 264/5,461 4.8
Antiseptic methodChlorhexidine-cetrimide 19/1,485 1.3 <0.00170% isopropanol 518/11,859 4.4
Interval between collection and micro bottle inoculationSame-day processing 68/1,368 5.0 0.003Next-day processing 456/11,823 3.9Processed after 2 days 13/153 8.5
Microscreening methodAdult aerobic bottle not used 110/3,282 3.4 0.02Adult aerobic bottle used 427/10,062 4.2Adult anaerobic bottle not used 6/410 1.5 0.007Adult anaerobic bottle used 531/12,934 4.1Pediatric bottle not used 345/6,213 5.6 <0.001Pediatric bottle used 192/7,131 2.7
Banking periodCB banked 1995-1999 202/2,563 7.9 <0.001CB banked 2000-2009 335/10,781 3.1
TABLE 5. Significant risk factors for contamination from multivariatelogistic regression (data from 2000 to 2009)
VariableHazard
ratio
95% CI for hazard ratio
p valueLower Higher
Vaginal delivery 4.184 2.89 6.07 <0.001CB processed 2 days after collection 1.04 0.45 2.40 0.931Obstetric staff collecting 1.66 1.28 2.17 <0.001Cleaning with isopropanol 1.50 0.89 2.55 0.126Adult anaerobic bottle used 2.50 1.09 5.75 0.031Adult aerobic bottle used 0.74 0.53 1.01 0.060Pediatric bottle used 0.60 0.43 0.84 0.003
CONTAMINATION FACTORS OF CORD BLOOD
Volume **, ** ** TRANSFUSION 5

A known limitation of the pediatric bottle is subopti-mal detection of obligate anaerobic organisms and hencethe manufacturer recommends this bottle be used todetect aerobic and facultative anaerobic bacteria only. Thisfact and inoculation of the pediatric bottle at the lowerthreshold of the recommended volume are likely reasonsfor the lower detection rate. Due to the pediatric bottlelimitations, the adult anaerobic bottle was reintroducedin 2002. Although this partially restored detection of con-tamination, the rate was still below that previously seen inMethod 1, and hence testing of the discard plasma in anadult aerobic bottle was reintroduced in 2005. It is likelythat the contamination rates did not increase to the origi-nal levels due to improvements in other variables such ascollection staff training and cord cleaning technique. Sub-stantially higher contamination rates were observedbefore 2000, which corresponded to published reportsassociating high contamination rates with the start-upyears of a CBB.5,9 To assess other contributing risk factorsfor high contamination, CB collected between 1995 and1999 was excluded from the multivariate analysis.
Findings show that the use of a pediatric bottle wasassociated with a significantly lower contamination rate,which may be due to the decreased detection capacity forstrict anaerobes and a sample volume at the lower thresh-old of that recommended by the manufacturer. Use of ananaerobic culture bottle was associated with a significantlyhigher detection rate, specifically of obligate anaerobes,which were rarely detected in the aerobic and pediatricbottle. All obligate anaerobes were only detected in a singlebottle for each CBU, with the majority (94%) only detectedin the adult anaerobic bottle. This finding highlights theinability to detect anaerobes present in the final product ifonly a pediatric bottle is used. The anaerobic organismsidentified in this study included a large proportion ofBacteroides spp., although Prevotella spp. and Clostridiumspp. were also identified. Since a 2005 study in Japanreported a post–bone marrow transplant death attributedto a blood stream infection with Clostridium innocum28
and the most widely recommended prophylactic antibiot-ics (fluoroquinolones) are active against aerobic but notanaerobic organisms, the identification of anaerobic con-taminants would appear to be of high importance.29
Factors reported in the literature to reduce contami-nation are using a closed processing system, use of trainedcollection staff, antisepsis of the umbilical cord beforecollection, and collection from cesarean deliveries.3,5,8,9
Our data demonstrate a significantly higher contamina-tion rate after vaginal delivery compared to cesareansection, which is consistent with the findings of Chen andcolleagues.3
In 2007, after a formal validation study, the SCBBchanged the antiseptic used to clean the cord from 70%isopropanol to a chlorhexidine-cetrimide solution. Onunivariate analysis, the latter antiseptic was found to yield
a significantly lower contamination rate, which is inkeeping with a recent report that demonstrated thebenefit of a chlorhexidine-based antiseptic procedure forskin cleaning before collection of blood for transfusion.16
Although alcohol is a very effective agent in inactivation ofbacteria, it evaporates quickly and does not have thelasting antimicrobial effect that can be improved by com-bination with other agents such as chlorhexidine, whichhas a strong affinity for skin and can be effective forhours.30
At the commencement of a CBB, and when personnelwith limited training are utilized, contamination rates of28% have been reported,5,9 and after specific training ofmaternity staff or use of CBB-trained personnel contami-nation rates can be reduced to 0% to 5%.5,8,9 Our finding ofsignificantly higher contamination in CB collected byobstetric staff is likely related to training, expertise, andfrequency of performing the procedure. SCBB collectionstaff undergo a much more extensive training and compe-tency program than obstetricians and midwives andperform the procedure with more frequency. The highervaginal and/or perianal contaminants reported by Chenand colleagues may in part relate to their use of obstetricstaff who have only received CB collection instructionsfrom an educational DVD.3 In 2007, a more comprehen-sive training program with an accreditation process forthe obstetric collectors was introduced by the SCBB,which has reduced the difference in contamination ratesbetween the obstetric staff and SCBB staff.
Although not confirmed in the multivariate analysisthat excluded the early data when a higher proportion ofCB was stored for longer periods before processing, ourunivariate analysis demonstrated an increased contami-nation rate in CB stored for 2 days before processing. Thisfinding may indicate that low-level bacterial or fungalcontamination or slow-growing organisms, such as Propi-onibacterium acnes, may be present that are undetectableby current methods but may reach detectable levels after2 days of storage at room temperature.
It is unknown whether contaminant organismsalways survive cryopreservation and the subsequentthawing process before infusion, although preliminarystudies in our laboratory indicate that many organisms dosurvive and could thus be infused into a recipient ifpresent in a CB product. Although microbial contamina-tion of infused CB and marrow has generally not beenassociated with adverse clinical outcome when given withprophylactic antibiotic therapy,10,12 rare adverse eventsand prolonged hospital stays have been reported afterinfusion of contaminated HPC products.12,13 Hence, aCB-associated infection could be detrimental to therecipient, particularly if the contamination was unknownbefore transplant and the patient was not on appropriateantibiotic therapy. Clinical programs may not considerposttransplant infections to be acquired from the CB if
CLARK ET AL.
6 TRANSFUSION Volume **, ** **

indicated by the CBB to be free of microbes. Since theclinical programs rely on the reported microbial status of aCB product before transplantation and rarely performtheir own cultures postthaw, it is imperative that thereported microbial status be as accurate as possible. Thisaccuracy can be increased by testing larger samplevolumes in media permissive for all contaminating organ-isms including anaerobes and fungi.
It is therefore concluded that the sole use of a pediat-ric bottle may not detect all contaminating organisms. Inan effort to provide the safest possible CB product, as wellas undertaking appropriate measures to minimize con-tamination during the collection and processing, the uti-lization of adequate screening procedures should beundertaken by a CBB. We suggest that the most conserva-tive approach of testing a discard fraction to achieve anacceptable inoculation volume in addition to the smallvolume of the final product is appropriate. Recommenda-tions from this study include the use of trained collectors,cleaning the umbilical cord with an effective antiseptic,testing a suitable volume of the CB by performing a test ona discard fraction in addition to the final product, andusing a detection system appropriate for both aerobic andanaerobic bacteria as well as fungi. This will help to ensurethat microbial contamination of CB is detected beforerelease and distribution of products for transplant.
ACKNOWLEDGMENT
The author thanks Ian Nivison-Smith, Senior Analyst/Statistician
at the Australian Bone Marrow Transplant Recipient Registry
(ABMTRR), for assisting with the logistic regression.
CONFLICT OF INTEREST
The authors declare that they have no conflicts of interest rel-
evant to the manuscript submitted to TRANSFUSION.
REFERENCES
1. Netcord and the Foundation for the Accreditation of Cellu-
lar Therapy (FACT). Netcord-FACT international standards
for cord blood collection, banking, and release for admin-
istration, 4th ed. Netcord-FACT; 2010.
2. American Association of Blood Banks. Standards for cellu-
lar therapy product services. 4th ed. Bethesda (MD):
American Association of Blood Banks; 2010.
3. Chen S, Zheng Y, Yang S, Yang K, Shyr M, Ho Y. Microbial
contamination of the Tzu-Chi Cord Blood Bank from 2005
to 2006. Acta Paediatr Taiwan 2008;49:9-13.
4. Bertolini F, Lazzari L, Lauri E, Corsini C, Castelli C, Gorini
F, Sirchia G. Comparative study of different procedures for
the collection and banking of umbilical cord blood.
J Hematother 1995;4:29-36.
5. Elchalal U, Fasouliotis S, Shtockheim D, Brautbar C,
Schenker JG, Weinstein D, Nagler A. Postpartum umbilical
cord blood collection for transplantation: a comparison of
three methods. Am J Obstet Gynecol 2000;182(1 Pt 1): 227-
32.
6. Honohan Á, Olthuis H, Bernards AT, van Beckhoven JM,
Brand A. Microbial contamination of cord blood stem cells.
Vox Sang 2002;82:32-8.
7. Meyer TPH, Hoffman B, Zaisserer J, Jacobs VR, Fuchs B,
Rapp S, Weinauer F, Burkhart J. Analysis and cryopreserva-
tion of hematopoietic stem and progenitor cells from
umbilical cord blood. Cytotherapy 2006;8:265-76.
8. Reboredo M, Diaz A, Castro A, Villaescusa RG. Collection,
processing and cryopreservation of umbilical cord blood
for unrelated transplantation. Bone Marrow Transplant
2000;26:1263-70.
9. Armitage S, Warwick R, Fehily D, Navarrete C, Contreras M.
Cord blood banking in London: the first 1000 collections.
Bone Marrow Transplant 1999;24:139-45.
10. Kamble R, Pant S, Selby GB, Kharfan-Dabaja MA, Sethi S,
Kratochvil K, Kohrt N, Ozer H. Microbial contamination of
hematopoietic progenitor cell grafts-incidence, clinical
outcome, and cost-effectiveness: an analysis of 735 grafts.
Transfusion 2005;45:874-8.
11. Lasky LC, Lane TA, Miller JP, Lindgren B, Patterson HA,
Haley NR, Ballen K. In utero or ex utero cord blood
collection: which is better? Transfusion 2002;42:
1261-7.
12. Patah PA, Parmar S, McMannis J, Sadeghi T, Karandish S,
Rondon G, Tarrand J, Champlin R, de Lima M, Shpall EJ.
Microbial contamination of hematopoietic progenitor cell
products: clinical outcome. Bone Marrow Transplant 2007;
40:365-8.
13. Majado MJ, Hernandez AG, Morales A, Gonzalez C,
Martınez-Sanchez V, Menasalvas A, Rosique P, Rubio A,
Sanz-Imedio E. Influence of harvest bacterial contamina-
tion on autologous peripheral blood progenitor cells post-
transplant. Bone Marrow Transplant 2007;39:121-5.
14. TGA. Australian code of good manufacturing practice—
human blood and tissue. Canberra: Therapeutic Goods
Administration; 2000.
15. Armitage S, Fehily D, Dickinson A, Chapman C, Navarrete
C, Contreras M. Cord blood banking: volume reduction of
cord blood units using a semi-automated closed system.
Bone Marrow Transplant 1999;23:505-9.
16. Marlowe L, Mistry RD, Coffin S, Leckerman KH, McGowan
KL, Dai D, Bell LM, Zaoutis T. Blood culture contamination
rates after skin antisepsis with chlorhexidine gluconate
versus povidone-iodine in a pediatric emergency depart-
ment. Infect Control Hosp Epidemiol 2010;31:171-6.
17. Mimoz O, Karim A, Mercat A, Cosseron M, Falissard B,
Parker F, Richard C, Samii K, Nordmann P. Chlorhexidine
compared with povidone-iodine as skin preparation before
blood culture. A randomized, controlled trial. Ann Intern
Med 1999;131:834-7.
CONTAMINATION FACTORS OF CORD BLOOD
Volume **, ** ** TRANSFUSION 7

18. Darouiche RO, Wall M, Itani KMF, Otterson M, Webb AL,
Carrick MM, Miller HJ, Awad SS, Crosby CT, Mosier MC,
Alsharif A, Berger DH. Chlorhexidine–alcohol versus
povidone–iodine for surgical-site antisepsis. N Engl J Med
2010;362:18-26.
19. Ramirez-Arcos S, Goldman M. Skin disinfection methods:
prospective evaluation and postimplementation results.
Transfusion 2010;50:59-64.
20. Klein MA, Kadidlo D, McCullough J, McKenna DH, Burns
LJ. Microbial contamination of hematopoietic stem cell
products: incidence and clinical sequelae. Biol Blood
Marrow Transplant 2006;12:1142-9.
21. Mison L, Stillianou J, Goodear A, Vowels M. Microbial con-
tamination in cord blood: an analysis of three test-
protocols. ISCT Vancouver, 2005. Abstract: 05-A-83-ISCT.
22. Mermel LA, Maki DG. Detection of bacteremia in adults:
consequences of culturing an inadequate volume of blood.
Ann Intern Med 1993;119:270-2.
23. Bouza E, Sousa D, Rodriguez-Creixems M, Lechuz JG,
Munoz P. Is the volume of blood cultured still a significant
factor in the diagnosis of bloodstream infections? J Clin
Microbiol 2007;45:2765-9.
24. Hall MM, Ilstrup DM, Washington JA. Effect of volume of
blood cultured on detection of bacteremia. J Clin Micro-
biol 1976;3:643-5.
25. Gonsalves WI, Cornish N, Moore M, Chen A, Varman M.
Effects of volume and site of blood draw on blood culture
results. J Clin Microbiol 2009;47:3482-5.
26. Connell TG, Rele M, Cowley D, Buttery JP, Curtis N. How
reliable is a negative blood culture result? Volume of blood
submitted for culture in routine practice in a children’s
hospital. Pediatrics 2007;119:891-6.
27. Arpi M, Bentzon M, Jensen J, Frederiksen W. Importance of
blood volume cultured in the detection of bacteremia. Eur
J Clin Microbiol Infect Dis 1989;8:838-42.
28. Chizuka A, Kami M, Kanda Y, Murashige N, Kishi Y, Hamaki
T, Kim SW, Hori A, Kojima R, Mori SI, Tanosaki R, Gomi H,
Takaue Y. Value of surveillance blood culture for early diag-
nosis of occult bacteremia in patients on corticosteroid
therapy following allogeneic hematopoietic stem cell trans-
plantation. Bone Marrow Transplant 2005;35:577-82.
29. Engelhard D, Akova M, Boeckh MJ, Freifeld A, Sepkowitz K,
Viscoli C, Wade J, Raad I. Bacterial infection prevention
after hematopoietic cell transplantation. Bone Marrow
Transplant 2009; 44: 467-70.
30. Segers P, Speekenbrink RGH, Ubbink DT, van Ogtrop ML,
de Mol BA. Prevention of nosocomial infection in cardiac
surgery by decontamination of the nasopharynx and
oropharynx with chlorhexidine gluconate. JAMA 2006;
296:2460-6.
CLARK ET AL.
8 TRANSFUSION Volume **, ** **



























