Embed Size (px)
Citation preview
FACTORS AFFECTING THE ADOPTION OF mHEALTH
PRODUCTS AMONGST PATIENTS IN KENYA: A CASE
OF EMBU
BY
THOMAS O. KIRENGO
UNITED STATES INTERNATIONAL UNIVERSITY-
AFRICA
SPRING 2020
FACTORS AFFECTING THE ADOPTION OF mHEALTH
PRODUCTS AMONGST PATIENTS IN KENYA: A CASE
OF EMBU
BY
THOMAS O. KIRENGO
A Research Project Report Submitted to the School of Business
in Partial Fulfilment of the Requirement for the Degree of
Masters in Business Administration (MBA)
UNITED STATES INTERNATIONAL UNIVERSITY-
AFRICA
SPRING 2020
ii
STUDENT’S DECLARATION
I, the undersigned, declare that this is my original work and has not been submitted to any
other college, institution or university other than the United States International
University in Nairobi for academic credit.
Signed: ________________________ Date: _____________________
Thomas O. Kirengo (ID 655063)
This project has been presented for examination with my approval as the appointed
supervisor.
Signed: ________________________ Date: _____________________
Dr. Scott Bellows
Signed: _______________________ Date: ____________________
Dean, School of Business

iii
COPYRIGHT
All rights reserved; no part of this work may be reproduced, stored in a retrieval system
or transmitted in any form or by any means, electronic, mechanical, photocopying,
recording or otherwise without the express written authorization from the USIU-A or the
author.
©Copyright Thomas Onyango Kirengo, 2019
iv
ABSTRACT
The objective of the study was to determine the factors affecting the adoption mHealth
products amongst patients in Kenya, a case of Embu. This study aimed at determining the
social factors affecting adoption of mHealth products, examining the technical factors
affecting adoption of mHealth products and determining the individual factors affecting
adoption of mHealth products.
The study adopted a descriptive and correlational research method in gathering,
analyzing, interpretation, and presentation of information. The research design helped in
focusing at the strength and direction of relationship between factors influencing the
adoption of mHealth products. The study employed the use of questionnaires to obtain
relevant information from respondents. The study focused on 144, 347 adults living in
Embu town. Random sampling technique was used to determine the sample size of 277
respondents of which 207 respondents completed and returned back their questionnaires.
The study adopted a descriptive and inferential statistics in data analysis and presentation.
Correlation analysis and regression analysis was used in the study to determine the effect
of factors on adoption of mHealth products. Data was presented in tables and figures.
The study determined how social factors affect the adoption of mHealth products. The
study found that people who influence other people‟s behaviours think that they should
use mobile phone for healthcare. People who are important to others think that they
should use mobile phone for healthcare. The study reveals that people who are familiar to
others think that they should use mobile phone for healthcare. The findings of the study
showed that social factors positively and significantly correlated to adoption of mHealth
products. The study revealed that social factors are critical factors in enhancing or rather
influencing effective adoption of mHealth products.
The study revealed how technical factors influence the adoption of mHealth products.
The study found that majority of the population own or has access to smartphones hence
they have access to good mobile phone network service at home and at their work places.
People have good and high speed internet available at their homesteads and at their work
places. The study found that most people frequently use internet based applications like
whatsapp and email for communication. The study revealed that people frequently use
social media like facebook, instagram and twitter in their daily endeavours.

v
The study examined the influence of individual factors on adoption of mHeath products.
The study reveals that it is very useful to seek healthcare services using mobile phone.
The use of mobile phones enhances communication and helps in improving efficiency
thus improving the performance. The study found that in seeking healthcare using mobile
phone would save time hence majority of people seek healthcare using their mobile
regardless of their location. The study depicts that communication plays a critical role in
seeking healthcare services hence in enhancing access to healthcare services; open
communication environment should be encouraged.
In conclusion, due to the strong relationship between social factors and adoption of
technology, it is important for companies to carefully study the attitudes of the society to
their technology prior to rollout. It is seen that technical factors such as having access to
internet, smartphones, good mobile network coverage and high utilization of social
media, positively facilities the adoption of technology. Individual factors such as high
perceived benefit of use and ease of use of a technology increases the adoption of
technology.
The study recommends that organizations must actively plan how to break social barriers
when introducing mHealth products. They must carefully select influential individuals in
the society to launch and spread their products. Organizations need to focus on
technologies and products that can work well within the existing technological
infrastructure. Lastly, individual factors such as perceived ease of use, work in
complement with perceived benefit of use. mHealth products that will see the highest
levels of user adoption will have delivered products that are easy to use and provide a
very clear solution to existing users‟ problems.

vi
ACKNOWLEDGEMENT
I would like to thank God for the opportunity of life and giving me the capability to
undertake this research. My family and friends who supported me during this project. My
supervisor, Dr. Scott Bellows, who was always available to listen, advice and provide
assistance. I may not be able to appreciate everyone who contributed to my successful
completion of this project, however, please accept my deep gratitude for your patience,
kindness and wisdom. This project would not have been a success without your support.
vii
DEDICATION
I would like to dedicate this master‟s project to my loving parents, Henry and Caroline
Onyango. My four brothers, Chris, Mangosh, Steve and Evans. My one and only sister
Joyce. You have been there for me throughout my ups and downs; and have given me the
encouragement to successfully complete this project. Thank you
viii
TABLE OF CONTENTS
STUDENT’S DECLARATION .............................................................................................. ii
COPYRIGHT ......................................................................................................................... iii
ABSTRACT ............................................................................................................................. iv
ACKNOWLEDGEMENT ...................................................................................................... vi
DEDICATION........................................................................................................................ vii
TABLE OF CONTENTS .................................................................................................... viii
LIST OF TABLES .................................................................................................................. xi
LIST OF FIGURES ............................................................................................................... xii
LIST OF ABBREVIATIONS AND ACRONYMS ........................................................... xiii
CHAPTER ONE ...................................................................................................................... 1
1.0 INTRODUCTION......................................................................................................... 1
1.1 Background of the Study ............................................................................................. 1
1.2 Problem Statement ...................................................................................................... 5
1.3 General Objective ........................................................................................................ 7
1.4 Specific Objectives ...................................................................................................... 7
1.5 Significance of the Study ............................................................................................ 7
1.6 Scope of the Study....................................................................................................... 8
1.7 Definition of Terms ..................................................................................................... 8
1.8 Chapter Summery ........................................................................................................ 8
CHAPTER TWO ................................................................................................................... 10
2.0 LITERATURE REVIEW .......................................................................................... 10
2.1 Introduction ............................................................................................................... 10
2.2 Social Factors and Adoption of mHealth Products ................................................... 11
2.3 Technical Factors and Adoption of mHealth Products ............................................. 17
2.4 Individual Factors and Adoption of mHealth Products ............................................. 21
2.5 Chapter Summary ...................................................................................................... 26
ix
CHAPTER THREE ............................................................................................................... 28
3.0 METHODOLOGY ..................................................................................................... 28
3.1 Introduction ............................................................................................................... 28
3.2 Research Design ........................................................................................................ 28
3.3 Population and Sampling Design .............................................................................. 29
3.4 Data Collection Methods ........................................................................................... 31
3.5 Research Procedures ................................................................................................. 31
3.6 Data Analysis Methods ............................................................................................. 33
3.7 Chapter Summary ...................................................................................................... 33
CHAPTER FOUR .................................................................................................................. 34
4.0 RESULTS AND FINDINGS ...................................................................................... 34
4.1 Introduction ............................................................................................................... 34
4.2 Background Information ........................................................................................... 34
4.3 Social Factors and Adoption of mHealth Products ................................................... 36
4.4 Technical Factors and Adoption of mHealth Products ............................................. 41
4.5 Individual Factors and Adoption of mHealth Products ............................................. 46
4.6 Chapter Summary ...................................................................................................... 50
CHAPTER FIVE ................................................................................................................... 52
5.0 DISCUSSION, CONCLUSIONS AND RECOMMENDATIONS ......................... 52
5.1 Introduction ............................................................................................................... 52
5.2 Summary ................................................................................................................... 52
5.3 Discussion ................................................................................................................. 53
5.4 Conclusions ............................................................................................................... 61
5.5 Recommendations ..................................................................................................... 62
REFERENCES ....................................................................................................................... 65
APPENDICES ............................................................................................................................

x
Appendix I: Letter of introduction .......................................................................................
Appendix II: Research License .............................................................................................
Appendix III: Questionnaire .................................................................................................
xi
LIST OF TABLES
Table 3.1: Population Distribution ........................................................................................... 29
Table 3.2: Reliability Test Results ........................................................................................... 32
Table 4.1: Social Factors affecting Adoption of mHealth Products ........................................ 36
Table 4.2: Mean (M) and Standard Deviation (S.D) for Social Factors .................................. 37
Table 4.3: Correlation between Social Factors and mHealth Products ................................... 38
Table 4.4: Regression Model Summary for Social Factors and mHealth Products................. 39
Table 4.5: Regression ANOVA for Social Factors and mHealth Products ............................. 40
Table 4.6: Regression Coefficients for Social Factors and mHealth Products ........................ 40
Table 4.7: Technical Factors affecting Adoption of mHealth Products .................................. 42
Table 4.8: Mean (M) and Standard Deviation (S.D) for Technical Factors ............................. 43
Table 4.9: Correlation between Technical Factors and mHealth Products .............................. 44
Table 4.10: Regression Model Summary for Social Factors and mHealth Products ............... 45
Table 4.11: Regression ANOVA for Technical Factors and mHealth Products ..................... 45
Table 4.12: Regression Coefficients for Technical Factors and mHealth Products ................ 46
Table 4.13: Individual Factors affecting Adoption of mHealth Products ................................ 47
Table 4.14: Mean (M) and Standard Deviation (S.D) for Individual Factors .......................... 48
Table 4.15: Correlation between Individual Factors and mHealth Products ........................... 49
Table 4.16: Regression Model Summary for Individual Factors and mHealth Products ........ 49
Table 4.17: Regression ANOVA for Individual Factors and mHealth Products ..................... 50
Table 4.18: Regression Coefficients for Individual Factors and mHealth Products................ 50
xii
LIST OF FIGURES
Figure 2.1: Conceptual Framework ......................................................................................... 26
Figure 4.1: Age Bracket of Respondents ................................................................................. 34
Figure 4.2: Gender of the Respondents.................................................................................... 35
Figure 4.3: Level of Education of Respondents....................................................................... 35
xiii
LIST OF ABBREVIATIONS AND ACRONYMS
BI-Behavioural intentions
ICT-Information Communication Technology
IF-Individual Factors
GSMA - Groupe Spécial Mobile Association
KMPDB-Kenya Medical Practitioners and Dentist Board
mHealth- Mobile Health
PDAs-Personal digital assistants
SDG - Sustainable Developmental Goal
SF-Social Factors
SIM - Subscriber Identity Module
SMS-Short Message Service
SN- Subjective norm
SPSS - Statistical Package for Social Sciences
USSD - Unstructured Supplementary Service Data
TAM-Technology Acceptance Model
TF-Technical Factors
TRA - Theory of Reasoned Action
UHC-Universal Health Coverage
UN-United nations
UTAUT- Unified Theory of Acceptance and Use of Technology
WHO-World Health Organization
1
CHAPTER ONE
1.0 INTRODUCTION
1.1 Background of the Study
The economist Rifkin (2011) believes that the world is at the brink of a 3rd
industrial
revolution. The economic revolutions in history he says have occurred due to the
convergence of new communication technologies with new energy systems. In the 19th
century, this involved the evolution of print media communication, coal and steam
powered engines i.e. The 1st Industrial revolution. The 2
nd Industrial revolution, in the 20
th
century, arose due to the centralization of electricity and proliferation of telephone, radio
and television usage. Today, there is an exponential growth in internet communications
and this has been accompanied by an increase in renewable energy, creating an enabling
environment for what may become the 3rd
Industrial revolution. This would mark the
greatest change of the 21st century. Shifting from one economic revolution to the other
has been noted to be accompanied by alterations not only in the delivery of manufacturing
but also that of the service industry. Recently, digital technologies have been disrupting
businesses throughout every industry. Industries such as banking, retail and insurance
have experienced major changes through widespread implementation of digital systems.
The healthcare industry however, has seen no major change in how business is conducted.
Despite this, African countries are seen to be in a great position to develop and benefit
from healthcare technological advancements. These are seen as having the ability to help
the African healthcare industry leapfrog and overcome barriers such as the cost of
physical infrastructure (Stroetmann, 2018). In 2005 eHealth was established as a priority
by the World Health Organization (2005) at the World Health Assembly(WHA). The
WHO(2019) defines eHealth as the use of information and communication technologies
(ICT) in support of health and health related fields. African leaders, during the May 2017
World Health Assembly, committed to supporting e-health and establish a strong digital
health ecosystem. Digital health ecosystem was defined as the holistic application of
Information Communication Technology (ICT) to support and improve healthcare
delivery, coordination and integration amongst different healthcare providers at different
levels in the system from local to national (Stroetmann, 2018).According to WHO
(2016)It is increasingly becoming apparent that it is extremely difficult to achieve
Universal Health Coverage (UHC), without the support of eHealth.
2
In 2015, 191 Member States of the United Nations agreed to try and achieve 17
Sustainable development goals (SDG) by the year 2030(United Nations (UN), 2019).
SDG goal three is to ensure healthy lives and promoting well-being for all ages. Target
eight of this SDG is to achieve universal health coverage. However, the other sixteen
SDGs are related to or contribute to health. SDG goal nine is to build resilient
infrastructure, promote inclusive and sustainable industrialization and foster innovation.
This goal targets on increasing access to information and communication technology as
well as provide access to internet in developing countries. eHealth if or when successful,
has the potential of catalysing the achievement of the UN SDGs.
As the use of technology continues to grow, the health sector has embraced the use of
technology. A world health organization survey indicated that out of the total member
states 83% of the members have had at least one M-health initiative implemented in their
country (WHO, 2011). Prior research in healthcare provision in Kenya shows that the
country is faced with various challenges some of which are being affordability, access
and lack of enough health workers, the ratio being 15 health workers to 500 people
(GSMA, 2012) which includes community health workers, nurses and doctors.
Technology is seen to be a solution to the various issues faced in the provision of
healthcare in the country. Adoption of Mhealth in Kenya seeks to provide access to
healthcare for all, affordable access to medical practitioners and information via the
mobile phone, ability for a single medical practitioners to access many patients via the
mobile telephony network for example the use of Short Message Service (SMS) for
appointment reminders or reminding patients when to take their medicine and many
more. As a result, the M-health platform offers various exciting opportunities to improve
health care in Kenya.
The Government of Kenya developed an eHealth strategy 2011 - 2017 to guide reforms in
line with achieving universal health coverage (UHC). This is aligned to the Kenya Vision
2030, whose overall goal was to have equitable and affordable healthcare at the highest
achievable standard for the Kenyan citizen (Kenya Ministry of Medical Services, 2011).
The eHealth strategy was seen as having the ability to accelerate the access to health for
Kenyans living in rural areas. However, whether this has been achieved is debatable. The
key strategic areas of implementation that had been identified included: telemedicine,
health information systems, information for citizens, m-health and e-learning. The
3
Kenyan government prioritized health information systems as the first step in the
implementation of the ehealth strategy. Some of the strengths and opportunities
mentioned in the strategy include the strong political will of the government of Kenya to
progress healthcare reforms, high level of ICT awareness amongst the general population,
high awareness of existence of ehealth technologies amongst health practitioners, well
developed mobile telecommunications infrastructure, availability of alternative sources of
electrical power, availability of reliable, low cost internet access, GSM mobile
communications, high penetration of cellular phones, as well as the local availability of
technical experts in both ICT and Medical care to develop relevant e-health solutions.
Weaknesses and threats included immobility of current health records, inadequate ICT
infrastructure, low penetration of computer equipment, scarcity of funds, limited experts
in eHealth and medical informatics, low awareness of ehealth amongst general public,
data security threats, unreliable supply of electricity and government bureaucracy and
delays(Kenya Ministry of Medical Services, 2011).
mHealth (also known as mobile health) was defined as the use of mobile devices – such
as mobile phones, patient monitoring devices, personal digital assistants (PDAs) and
wireless devices – for medical and public health practice (WHO, 2016). Some examples
include short message service(SMS) appointment booking reminders, medical call
centres, mobile patient monitoring devices such as smart watches, electronic health
records and patient information available on mobile and mobile telehealth such as
hospital or clinic apps. mHealth is seen to have the capacity to increase access to health
services for those in remote and underserved locations. It is especially important in
regions with poor physical infrastructure that however have access to mobile
telecommunications. Mobile device use has increased remarkably in developing nations
from 1.2 billion to 5.5 billion in 2015. Mobile phones are currently the widespread form
of personal technology. As of 2014 60% of the global population, approximately 4.4
billion people, still had no access to internet. A negative bias to women has however been
observed, with women accounting for 53% of the non-internet users versus 41% of the
online population, with the gender gap rising up to 45% in certain parts of sub-Saharan
Africa.
Mobile internet is expected to fill this gap and catalyse the growth and impact of services.
The unconnected population are seen as the rural, low income earner with low literacy
levels in developing countries. It is estimated that there will be 3.8 billion mobile internet
4
users by 2020, up from 2.2 billion in 2013. This will be largely driven by increasing
coverage to the unconnected. This is seen as a growth opportunity for mHealth products
leveraging on the above. Developing countries now have mobile subscription rates
comparable to those in developed high-income countries. Despite this, access to
smartphones and mobile internet still remains challenging. Smartphones account for
nearly 50% of all mobile phones in developed countries, however, this is less than 10% in
developing countries (Groupe Spécial Mobile Association (GSMA), 2014).
The four main barriers to increased mobile internet access adoption include reduced
network coverage infrastructure in rural areas, un-affordability due to taxation, lack of
local content and consumer barriers. Consumer barriers can be defined as illiteracy,
digital illiteracy and lack of internet awareness. However, this is often due to the fact that
a majority of online platforms prefer to use English as the primary language despite the
fact that English is not known by those whom the platforms consider as their intended
user. About 55% of webpages have been found to primarily use English as the preferred
language, this limits mobile phone use to largely voice calls. Majority of 774 million
illiterate globally, live in developing countries.
According to a survey conducted by McKinsey (2013), African individuals mentioned
lack of digital literacy as the top reason for low internet usage. Google (2014) conducted
a survey in six key nations in Africa with a sample size of 13,000 people living in urban
centres. The survey covered Senegal, Ghana, and Nigeria from West Africa, Uganda and
Kenya in East Africa, and South Africa. The study found that the top reason for low
internet use among non-adopters living in these regions was lack of knowledge on how to
use the internet as opposed to cost or coverage. GSMA notes that paradoxically, while
there has been a rise in mobile penetration, access to basic utilities such as financial
services, education and healthcare has not considerably improved. Mobile technology is
seen as an enabler as seen in the case of mobile banking providing access to financial
services to previously unbanked. Base of pyramid survey in Kenya, suggested in 2012 of
the 60% of Kenyan‟s with mobile phones, a limited number of users used mobile
technologies other than M-PESA, a mobile money banking platform, due to lack of
awareness of the alternative applications available thus causing confusion in the
users(Infodev, 2012). Additionally, most of the content available on mobile phones does
not contain local content. Majority of information (>50%) in the internet is in English,
while only 5% of the global population speaks English. In order to reach a wider
5
audience, content must be customized to fit the local context and language (GSMA,
2014).
Embu is a metropolitan town, east of Nairobi city. It is considered to have a diverse
population owing to the fact that it was the former headquarters of the Eastern province,
and its central location (Embu County Government, 2018). It is the headquarters of Embu
county, one of the 47 counties in Kenya. The 2009 Population and Housing Census
(2013) recorded a population of 516,212 persons for Embu County. The population was
additionally expected to increase at a rate of 1.4% per annum, which would put the total
population at 577,390 people. However, only 25% of the individuals are estimated to live
in the town/ urban area. At the time of the census however, the population consisted of
254,303 males and 261,909 females. Individuals living in the country have average
literacy levels with 60% individuals having only primary school education (KNBS,
2009). Due to its diversity, and central location, this town would be representative of such
areas where a majority of Kenyans currently live.
1.2 Problem Statement
In 2011 Safaricom PLC the largest Mobile Service provider in Kenya through a
partnership with „Call-a-Doc Limited‟, launched a new service dubbed „Daktari 1525‟.
The service was targeted at allowing sick persons to seek medical attention from expert
doctors available on phone 24 hours a day. The product despite addressing a very
apparent client need, having a fair pricing strategy, and endorsement by the Kenya
Medical Practitioners and Dentist Board (KMPDB) failed to gain traction. Prior to this
disappointment, the then CEO of KMPDB, DanielYumbya, mentioned that the product
had chances of failure. He expressed concerns saying that in medicine, touch, feel and see
are key vital signs that medics embrace in their practice, therefore he was sceptical that
patients would want to use technology that would not allow them to experience these
factors (Karongo, 2011) However, was this the real reason behind the failure of „Daktari
1525‟? This paper aims to examine this.
Developing countries face multiple challenges in delivering high quality healthcare to
their population. This is influenced by multiple factors such as poor funding and shortage
of healthcare human resource. According to the Kenya Demographic and Health Survey
2014, only 58% of women make it to the recommended 4 antenatal care visits before
6
child birth A meagre 53% of delivering mothers receive post-natal care within 2 days of
delivery. Only 1 in every 3 new-borns receives postnatal care from a doctor, nurse or
midwife. According to the survey, only 66% of children found to have respiratory illness
had been taken to a health facility while just 50% of those found with diarrheal disease
had been taken to a health provider (Government of Kenya (GOK), 2014). There is a need
to increase access to healthcare, improve the quality of care available and reduce the cost
of providing medical care.
Additionally, healthcare expenditure is noted to be on the rise globally (WHO, 2018).
Digitization of healthcare has shown viability as a solution to the healthcare issues
currently facing these countries. Example of a mobile phone system in Zanzibar that
enables mothers to contact their primary care provider, has led to a Wired Mothers
increased attendance of antenatal clinic visits. This led to a reduction in the prenatal
mortality rate of the wired mothers to 1.9% compared to that of non-wired mothers that
was high at 3.6%. However, current digital health solutions despite high benefit, have
little uptake and are not implemented to impactful scale (GSMA, 2017).
Kenya, through its ehealth strategy is dedicated to ensuring achievement of positive
healthcare outcomes through large scale implementation of eHealth. In order for ehealth
programs to become scalable the following need to be achieved. Higher government
involvement and investment in ehealth, increased collaboration and integration amongst
individual organizations in healthcare, Public-Private partnerships amongst other
stakeholders. mHealth is a component of e-health that involves provision of healthcare
services through mobile technologies such as mobile phones. The use of mobile phones in
Kenya and other developing countries is prolific. The mobile and internet penetration of
Kenya are among the highest in Africa at 83% and 58% of the 44.35 million population
(Communications Authority of Kenya (CCK), 2014). Smartphones accounted for 1.8
Million of 3.1 Million devices sold in Kenya in 2015 (Jumia Kenya, 2015). Mobile health
is noted to be key in implementing digital health in developing countries.
Digital health and mhealth initiatives in developing countries have been on the increase.
However scalability will depend on the ability of organizations to establish valuable
collaborations with all stakeholders. This involves the engagement and digitization of the
health professional, the health centre and the patient(GSMA, 2017).
7
A knowledge gap exists in the key factors influencing the adoption and usage of mHealth
products currently available in the market.
1.3 General Objective
The general objective of this study was to determine the factors affecting the adoption of
mhealth products amongst patients in Kenya: a case of Embu.
1.4 Specific Objectives
Specifically, the study aims to:
1.4.1 Determine the social factors affecting adoption of mHealth products
1.4.2 Determine the technical factors affecting adoption of mHealth products
1.4.3 Determine the individual factors affecting adoption of mHealth products
1.5 Significance of the Study
This study has relevance to the following potential beneficiaries.
1.5.1 Healthcare Companies
This study provides crucial insights for healthcare company managers that guides them
during strategic planning and consideration of launching mHealth Products.
1.5.2 Technology Companies
Technology companies borrow from this research when making decisions and strategies
for growing their companies in the African Health Market.
1.5.3 Hospitals
This study provides crucial insights for hospital managers that guide them during
restructuring or planning to adopt eHealth Strategies.
1.5.4 Health Sector Investors
Other domestic and foreign investors borrow from this research when making investment
decision and strategies for growing their companies in the African Health Market.
1.5.5 Government and Government Agencies
The policy makers borrow information and insights from this paper to guide in making
informed policy to help nature and develop the health sector.
8
1.5.6 The Academia
This study contributes to the bulk of knowledge and research on mHealth. It also provides
a base for scholars interested in furthering research on this aspect of mHealth.
1.6 Scope of the Study
The conceptual scope of the study is to identify the factors affecting the adoption of
mHealth products in Kenya. Social factors, technical factors and individual factors are
identified as the three main areas of focus. The study targeted adult individuals above the
age of 18 years, living and working in Embu town. The study was conducted between the
months of June – September 2019. This study was a case of factors influencing adoption
of mHealth products by patients in Kenya. It was based in Embu, Kenya. A total of 207
responses were received from the target group.
1.7 Definition of Terms
1.7.1 eHealth is defined as the use of information and communication technologies
(ICT) in support of health and health related fields (WHO, 2019).
1.7.2 mHealth(also known as mobile health) is defined as the use of mobile devices –
such as mobile phones, patient monitoring devices, personal digital assistants
(PDAs) and wireless devices – for medical and public health practice (WHO,
2016).
1.7.3 eBusiness(Also known as electronic business) is described as any kind of
business or commercial transaction that includes sharing information across the
internet (Gerstner, 2002).
1.7.4 eBusiness Modelis defined as the use of electronic business by a company or
organization to deliver value to its customers in order to generate revenues and
profitability (Osterwalder & Pigneur, 2002)
1.8 Chapter Summery
In chapter one, the study has presented the background information about factors
affecting the adoption of mHealth products. This section also outlines the research
objectives of the study, the significance of the study, importance and the scope of the
study as well as the definitions of specific terms used in the research. Chapter two
reviews literature which is guided by the research objectives identified in chapter one.
9
Chapter three identifies the research methodology that highlights the various procedures
and methods used by the researcher while conducting the research. Chapter four presents
the results and findings while chapter five provides a discussion on the findings of the
research guided by the specific research objectives then a conclusion and
recommendation of the study given.
10
CHAPTER TWO
2.0 LITERATURE REVIEW
2.1 Introduction
This chapter addresses the literature review on the factors affecting the adoption of
mhealth products amongst patients in Kenya. The study is divided into different sections.
The first section is to determine the social factors affecting adoption of mhealth products,
the second section is to determine the technical factors affecting adoption of mhealth
products and the third section is to determine the individual factors affecting adoption of
mhealth products. The last section of this chapter is a summary of the whole chapter.
The theories guiding the study are discussed herein. The Technology Acceptance Model
(TAM) is the mostly widely accepted and used theory to explain why individuals accept
new information technology and systems (Surendran, 2013). Conceptualized in 1989, by
Davis, it is based on principles of theory of reasoned action (Davis, 1989). According to
TAM two main factors, which can be considered individual factors, influence technology
use behaviour, this is, perceived usefulness and perceived ease of use. Many studies have
been conducted using modifications and extensions to the TAM model. Extended/
Modified TAM also referred to as TAM 2 model is one of the most frequently cited
modifications. Cognitive factors to the technology acceptance model. Social factors seen
to influence TAM are: subjective norms, voluntariness, and image (Venkatesh & David,
2000).
These theories have been further developed into Unified Theory of Acceptance and Use
of Technology (UTAUT). This theory identifies 4 key factors that influence acceptance of
information systems and four moderating factors that also predict if an individual will
adopt a technology. The four major indicators identified were: performance expectancy,
effort expectancy, social influence, and facilitating conditions. The four moderating
factors were also identified ie.: age, gender, experience and voluntariness(Venkatesh et
al. 2003).
This forms our primary theoretical framework on the study‟s approach to the factors
influencing adoption of mHealth. The factors highlighted are explored in further detail
throughout the chapter in relation to studies conducted in the recent past on adoption of
technology.
11
2.2 Social Factors and Adoption of mHealth Products
Mobile health which in most cases is referred to as mHealth integrates extensive series of
programs. WHO defines mHealth as a certain medical and public health practice that is
supported by a cell phone device like patient monitoring services, wireless devices and
personal digital services (PDAs) (WHO, 2011). According to Vital Wave Consulting
(2009), it is defined as the use of portable devices for with the capability of creating,
storing, retrieving and transmitting of data between the end-users to improve safety and
the quality of healthcare.
The accomplishments of mHealth have gained popularity globally according to a survey
conducted on 114 nations that were covered by the World Health Organizations that
initiated mHealth interventions (WHO, 2011). In their findings, they found out that
developed and underdeveloped nations vary when it comes to utilization of mHealth
products in healthcare. According to the study, Africa was at the bottom of the list when it
comes to adoption of mHealth services while North America, South Asia, and South
America that ranked in the top list when it comes to adoption levels. Informed activities
are underway with different analysts. They have predicted that the size of the worldwide
mobile health market is likely to rise to a tune of $23billion by the year 2017 (SNS
Telecom & IT, 2017). In addition to that Europe and Asia-Pacific are predicted to have
the largest market followed by North America. Lastly, Latin America and Africa were
anticipated to have the least marketplaces. In the USA, about 85% of the entire population
goes online at least once in a month. Of these users 16% are exclusively use smartphones
for conducting online activities. According to an eMarket study by McNair et al. (2018),
majority of the usage however is for digital media viewing and social media networking
at 82% & 72% respectively.
A survey that was conducted on US healthcare students, providers, administrators and
nurses in general with the help of a software company revealed in their findings that 83%
of this population uses smartphones when seeking for health services, 72% uses the same
smartphones in note-taking and memos, 50% uses smartphones for drug references, 28%
for accessing clinical decision support tool and 13% in viewing of medical images
(Krauskopf & Wyatt, 2012). Therefore, in their conclusion, it was true that mHealth is
highly used in the developed world for improving health awareness and education,
diagnosing of diseases and other support services like surveillance.
12
Although mHealth applications have more advantages than disadvantages, the adoption of
mHealth products has experienced several challenges due to being a relatively new and
emerging phenomenon. These challenges include low confidence by users of these
systems due to security fears such as the disclosure of their private information/data to a
third party. Patients may find it hard uncomfortable using the mHealth application unless
they are assured of confidentiality and security protection of their data. Lastly, not all
patients may understand the language used in the application unless translated into other
languages apart from English (Slobin, 1996).
Social factors are critical to consider as they have a great effect on the adoption of
technology within the health sector by the greater population (Alsaleh & Alshamari,
2016). Social factors have a higher influence on technology adoption especially in the
early stages of a new technology as majority of users have little experience and
knowledge of the technologies and its benefits (Hartwick & Barki, 1994). In developed
countries such as the US, Europe, and Canada, mHealth has been fully enhanced and
doctors can perform various tests on a patient and email the results to the patients directly.
Barriers to technology adoption have been reduced significantly. According to the World
Health Organization, Africa still lags in the adoption of the mHealth products and some
of the reasons for the delay include the poor technology in most countries, high poverty
levels, and poor health policies (Alsaleh & Alshamari, 2016). In Kenya, the health sector
has made major milestones since having efficient healthcare system is part of its Vision
2030 blueprint. However, Kenya still faces numerous challenges such as the low uptake
of technology particularly in the rural areas (Mwobobia, 2012). Social factors can be
conceptualized to influence innovation and technology adoption through the factors such
as compliance, subjective norms, group norms, social network configuration and
identification (social image and self-image) (Lorenz, Graf-Vlachy, & Buhtz, 2017)
2.2.1 Subjective Norms
Subjective norm is defined in several different ways depending on the nature in which the
words are used and the field of application. Subjective norm referred to as (SN) is known
as an individual‟s response when it comes to perceived expectations of the peer group and
the belief that one must comply with the set expectations even when not favourable
according to an individual‟s own perception. It can also be defined as an individual
observation concerning people that are of importance to the same individual (Avers &
13
Brown, 2009). Some factors guide the subjective norm in groups like family members,
colleagues, and activities that are related to work. The norms may have an influence on an
individual's acceptance through perceived usefulness in a positive way. The initial
technology acceptance model (TAM), ignored the subjective norm as one of the factors
that affect technology acceptance (Luborsky M. R., 1993). However, afterward, other
researchers incorporated the variable into their models such as TAM2 and TAM3, after
understanding the impacts of social occurrences on an individual‟s behaviour towards
technology acceptance (Vogelsang, Steinhuser, & Hoppe, 2013).
Other scholar‟s views concerning subjective norm is on the user's acceptance perspective
(Tseng, Hsia, & Chang, 2014). An individual‟s desire to maintain social status, high self-
image, prestige and avoid social stigma is a strong influencer of adoption of technology.
This reveals a sense of social consequence, resulting from the use of a technology
(Luborsky M. R., 1993). A study on patients who needed ventilator support showed low
acceptance of portable ventilators by users due to the perception that they would appear
impaired if seen to ambulating with a ventilator device. Despite the fact that these devices
offered high perceived usefulness, utility and flexibility for the patients. This was highly
influenced by the perceived outcome of social perception (Ainlay, Becker, & Coleman,
1986). The same has been observed with medication taking, whereby, patients are less
likely to take medication that will make them appear in a negative social stigma (Zola,
1982).
Vogelsang et al (2013), researched on risky effects that are normally considered when it
comes to ERP construction on examining the ERP success and system implementation in
the construction industry. The study realized the fact that subjective norm is significantly
related to perceived usefulness and perceived ease of use. On the other hand, perceived
ease of use is significantly related to the intention of use through usefulness thus
according to Schepers et al. (2008). In addition to that, a study was conducted by Guo et
al. (2015), on investigating determinants of acceptance when it comes to healthcare users.
The findings revealed that when it comes to integration of variables, they realized that
perceived ease of use, subjective norm, perceived usefulness, and trust have a positive
significant effect on expert's purpose to use the contrary occasion reporting system. Trust
and perceived usefulness had a direct impact on the perceived ease of use and subjective
norm. In a different study by Gupta (2008), exploring the adoption of ICT in enhancing
government to employee relationships, in a governmental organization in an
14
unindustrialized country, it was realized that subjective norm stands the highest
contributor in determining the use of the system.
Singletary et al (2002), conducted a study about social influences on technology
acceptance found within high school students using a new software application. The
results revealed that there was a strong positive significant relationship that existed
between image, social norms, innovative usage behaviour, and innovative usage. Su-pi et
al. (2013), explored the validity of the addition of social factors to TAM model, by
examining and predicting situations of telecare system usage. There results revealed that
social factors specifically social trust related to use positively predicted actual usage of
the system.
Furthermore, social influences have been shown to effects on subjective norms like the
acceptance of new technology. Giving a very close example to a study which was
conducted by Haderi & Aziz (2015), in examining the relationship of social norms in
adoption of information systems found that a positive effect exists between the two
variables. A separate study found that a negative relationship may exist between social
norms and adoption of technology when examining adoption of an electronic police
management system (POLNET) expected to improve police effectiveness in Turkey. The
reason was later revealed that this negative relationship was because the police force
promoted the use of the technology when arresting and dealing with the public in the
country. Therefore, the individuals in the public ended up forming negative associations
with the system (Yalcinkaya, 2007). Individual adoption and technology use were also
looked into by Tseng et al (2014), regarding workplace resistance to technology adoption
that had resulted secondary to poor social attitudes about the technology. The study
revealed that the social norm did not influence men that used the system as significantly
as it influenced the women using the same system. This showed the existence of a
relationship between social influence and gender of the users intended to adopt a new
system. This relationship is highlighted in the framework of the UTAUT theory
(Venkatesh et al. 2003).
2.2.2 Diffusion of Innovation (DOT)
ICT adoption in healthcare has received much attention in the recent times. In the current
technological environment, most manual systems have rapidly been converted into
automated systems that are quickly turning institutions into paperless workspaces where

15
the flow of documents is through removable media, emails, optical discs and computer
networks. Rogers (2003) described five stages through which an individual goes through
prior to adoption of a new innovation. Today, products and services, events and other
notices can be placed in an online platform and the users allowed accessing the
information through creation of user accounts and subscriptions. According to Davenport
(2001), banks and financial institutions, as well as other large enterprises, have adopted
feedback appliances that uses a touch screen to effectively capture the satisfaction level of
each attended customer in a manner that can be easily understood and reacted upon. This
should also be the case when it comes to notices and customer feedback mechanisms.
Most people have adopted the use of smartphones and are becoming increasingly adept in
their usage.
Diffusion of innovation is largely influenced by the social context of the population
observed. Hofstede‟s theoretical model (2001) demonstrates how natural cultural context
influences the diffusion of innovation. Five socio-cultural contexts are noted that is power
distance which discusses the extent to which less powerful individuals in the society
accept that power is unevenly distributed. African countries have a high-power distance
compared to developed countries such as the United States of America and the United
Kingdom (Chinweike & Ona, 2014). Power distance reduces the rates of technology
adoption and innovation. Secondly, individualism and collectivism defined as the extent
to which individuals act as part of a group or alternatively looks after themselves as
individuals. Collectivists are more likely to conform to the wants and needs of a group
rather than their own individual choices and preferences. This lack of individualism is
seen to curtail innovation. African countries are generally more collectivist than
individualistic. Thirdly, masculinity and femininity which talks about the degree to which
a society is dominated by masculine or feminine views and values. High masculinity is
seen to positively influence innovation and technology adoption. This is due to the fact
that societies high in masculinity value individualism and incentivize individual
performance. African societies are seen to have high masculinity. However, uncertainty
avoidance, the level at which members of the society feel comfortable or uncomfortable
with situations of uncertainty is seen to oppose risk taking and thus curtails innovation.
African societies are seen to more likely be risk adverse. Long-term vs short term
orientation the degree to which a society is seen to be future oriented. Societies with a
long-term orientation are more likely to invest in technologies and innovations that will
16
offer advantages in the future. African societies generally have been found to lack in long
term orientation. However, studies done in Kenya have found significantly different
levels of the four cultural dimensions mentioned by Hofstede, depending on the tribe
analysed and the location ie. city or rural (Ketter & Arfsten, 2015). Therefore,
generalization of the cultural dimensions may not be appropriate as various factors may
cause this to vary amongst the different African countries.
There is a close relationship between social cultural norms and the diffusion of
technology and innovation. As such it is seen necessary to achieve societal level changes
in order to have sustainable technological and innovation adoption (William & Dennis,
2011). In Kenya it is also seen that people exhibit positive attitudes to already proven
beneficial technologies and innovations. Companies and competitors tend to adopt/ copy
new innovations seen to give their competitors a competitive advantage (Muchiri, 2015).
In another study, it was noted that the main group that influences an individual‟s
decisions is their family, friends and colleagues (Ajzen & Fishbein, 1980).
2.2.3 Social Risk
There is always the general perception towards the use of the mHealth products which
both users experience. In such instances, others may find it difficult to interact with the
different mHealth products and develop a negative attitude towards the devices. Whereas
others may find the products useful in the management of their health, others would still
prefer the traditional face-to-face interactions where they can explain their health issues in
details (Slovensky & Malvey, 2017). Such setbacks have continued to challenge the
effectiveness and usefulness of mHealth products.
Also, the feeling among the healthcare providers that the products are not effective in
capturing critical data from the patients have made it difficult for the healthcare systems
to adopt the technologies. One of the major problems that affect the perceived usefulness
of technology is a social risk. According to Featherman & Hajli (2015), they describe
social risk as the belief of the consumers that they will look foolish to others. In this
context, they stop using certain mHealth products for the fear of looking foolish if they
are unable to use them effectively. The ease of use is also another major factor which
stems from its reasons from perceived usefulness. In this context, consumers will readily
adopt an application, technology or device that seems to be useful in improving
performance in healthcare as long as they do not appear imprudent in society. In the same

17
way, they may adopt an application which seems to be complex to operate if it makes
them appear intelligent in society. Others end up not using such technologies at all and
prefer using traditional methods such as booking an appointment with the doctors.
2.3 Technical Factors and Adoption of mHealth Products
The technical factors are those which concern the technology itself. These are factors
associated with the operation and the management of the mHealth products. With the
developed countries, the technical factors are no longer a major problem since technology
is highly enhanced and any technical problems can be resolved almost immediately.
Other countries have developed more complex devices that have troubleshooting features
and can detect and correct any problem within the devices in case of any breakdown or
malfunctioning. In developing countries, such technologies are not yet fully implemented
and breakdowns are common. Kenya has been partnering with global health organizations
such as the World Health Organization to fund different healthcare technologies which
always come as a huge expense to the health sector. Screening and diagnosis machines
have been installed in numerous country referral hospitals to improve detecting and
diagnosis of various ailments and such data can be sent directly to centres abroad for
further analysis. There are numerous technical factors which impact on the adoption of
mHealth products such as infrastructure, complexity, reliability, cost, and connectivity.
The European Fifth Framework Project entitled, E-factors a thematic network of e-
business models, presents a holistic approach in analysis of technology adoption. It
suggests taking into consideration 5 broad thematic areas referred to as e-factors:
technology, individual, organization, industry and society (Athanasia, Xenia, &
Konstantina, 2003). These technical and technological factors are considered as usually
externally controlled variables. They include factors such as infrastructure and the level
of technological advancement, user needs and benefits, and the competitive landscape.
These however, are also largely influenced by the technical factors influencing e-business
ie. compatibility with existing technology, customizability, integration, system
performance, reliability, support and serviceability
2.3.1 Relative Advantage
Globally cell phones have become a necessity and almost everyone owns a cell phone.
The cell phones have made communication very easy and they keep families in-touch
18
irrespective of the distance. It also helps in accessing business emails, group
communications and sharing of files as well (Mwobobia, 2012). In developing countries
such as Sub-Saharan Africa, mobile technologies have evolved into a service delivery
tool (Aker & Mbiti, 2010). For instance, the abrupt advancement cell phone use or
smartphone technology is having in the 21st century, is so impactful that any business or
service offered through the use of cell phones covers a bigger area than anything seen in
the past. Countries like Bangladesh, with a population of 156 million and beyond, the
government guarantees that all cell phone users are capable of getting phone network
signal irrespective of their geographic location. A study by Bangladesh Telecom
Regulatory Commission (BTRC) (2015) found that by January 2015, Bangladesh citizens
had 121.860 million cell phone users. Taking note that cell phones were introduced in
Bangladesh in the year 1993.
Technological advancement varies from one region to another. Most urban areas have
witnessed major milestones in technological advancement while in the rural areas;
technology penetration is still at the lower levels. At times, it is easy to introduce a
technology product, however, it might become more difficult to gain acceptance not only
from the healthcare professionals but also the patients and other users (Aker & Mbiti,
2010). In this context, it becomes extremely difficult to adopt any technology within the
healthcare system. In most instances, health care practitioners often believe that
technology is meant to take over the roles they play; however, some technologies help in
simplifying work and making it easier for them to discharge their duties effectively.
According to Lorenz (2017), the most appropriate way to ensure that change is effected in
health behaviour is by understanding the motivation behind the change itself. It is,
therefore, the role of policymakers to ensure that everyone understands the motivation
behind any mHealth product for effective transition and acceptance of the said change.
Also, the other challenge is the task of acceptance from the patients. Due to issues of
privacy and trust, most patients might choose not to adopt certain mHealth products such
as communication through mobile devices. In such cases, it becomes hard to scale the
adoption mHealth products.
An added advantage of mHealth is its ability to minimize the operational costs in health.
This is seen as one of the top priorities for managers and the Government. Costs,
however, must be balanced with the quality of service. This brings out the difference
19
between the services provided in both the private and the public healthcare sectors. Costs
are an integral part of the mHealth programs and cannot be overlooked. Technology in
healthcare can be one of the most expensive ventures. The implementation of mHealth
products is costly and requires careful consideration of the viability and reliability of such
products before carrying any implementation program. The adoption of mHealth products
should be proportional to their cost. Expensive and complex products will get a cold
reception from the healthcare providers. People prefer products that are easy to use and
affordable while meeting healthcare objectives. Cost, is, therefore, a significant factor
which requires a critical feasibility evaluation to avoid making wrong decisions.
Healthcare centres are more receptive to affordable but quality mHealth products with the
ability to improve healthcare services and enhance customer satisfaction.
2.3.2 Communication, Sending and Receiving Information
Most of the mHealth products utilize the advanced communication channels which are
not common to many people, especially in the rural regions. In this context, individuals
with limited technological background experience difficulties using mHealth
technologies. Sophisticated mHealth products might deter customers and providers from
using them and thus affecting their adoption. Even though the technology is expected to
make health care systems more effective, it becomes difficult to achieve the objective if
the players do not have the required skills to operate the different mHealth products thus
making them look complex to the users.
Mobile phone penetration, connectivity and coverage are seen as major factors
influencing communication. There has been a rapid increase in all three of these factors in
the past few decades in Kenya and other countries. Kenyan mobile phone penetration was
seen as 80% as of 2013 (Oteri, 2015). However according to GSMA (2014) less than 10%
of these phones in developing countries are smart phones. Kenya has also seen a rapid
increase in network coverage, mostly fuelled by competition within the telecoms industry.
However, a large part of the country still remains unserved according to the study by
Oteri (2015), which showed that only 38% mobile geographic network coverage by 2015.
Additionally, this is challenged by a low access to internet via high speed wireless local
area networks or fibre optics. However, technology such as 3G and 4G has enabled
mobile access to internet through mobile telephone service providers. Mobile internet
20
coverage and utilization has rapidly been on the rise in Kenya and other parts of Africa
thus providing internet access to people who previously lacked it.
Social networking technologies are applications that enable people to connect based on
their social bonds and ties. These include social networking websites such as Facebook
and Instagram that have enabled this to occur through the internet. Use of social
networking platforms have been on the rise throughout the world, African countries
included. Majority of these users in Africa, access the internet using mobile devices such
as smartphones only. In their study on Cultural Influence on the diffusion and adoption of
social media technologies by entrepreneurs in rural South Africa, Lekhanya (2013) found
that, proper use of social media positively influenced diffusion and adoption of new
technologies by individual living in rural areas in South Africa.
2.3.3 Compatibility
Compatibility implies the ability of the technology to work with and improve the current
requirement of the user of the new technology or innovation. Tan and Teo (2000) found
that technologies with a high compatibility are more likely to be adopted than those which
lack it. This is challenging in healthcare as devices are produced by multiple
manufactures and are difficult to integrate. Additionally, medical equipment usually have
a high purchase cost, and older machinery may not be compatible with new innovations
such as mobile connectivity. The cost of upgrading machinery may introduce an
additional variable in adoption of technologies in healthcare. One must also consider
compatibility of all these devices with the multiple different electronic health record
software that different hospitals and different service providers are using.
2.3.4 Perceived Security
There is a perception among new users that mHealth products impact negatively on their
privacy. Patients often believe that if the devices are not regulated, individual data could
be at a greater risk of being exposed to third parties even without the knowledge of the
patient. Technologies have different privacy terms and levels and it becomes an issue
when the safety of the data is at risk. mHealth devices with free access are always under
threat, cyber-attacks have been rampant in recent years and even big technology and
communication firms have not been spared (Alsaleh & Alshamari, 2016). With big
companies such as Facebook facing such threats, there is no guarantee that data is safe
with mHealth devices. The fear of data being exposed to external users is one of the
21
major reasons why some healthcare systems have been slow in adopting mHealth
technologies.
Patients' privacy and security of their data are of high importance, especially when using
mHealth products. Access of patients' data by third parties as even led to numerous
lawsuits as the victims launch court cases with healthcare centres (Alsaleh & Alshamari,
2016). In such instances, it becomes extremely expensive for healthcare providers to
prove that they can provide maximum data security through mHealth products. There are
applications used by healthcare institutions which collect data about patient details,
gender, and location and if such data lands in the hands of criminals, patients become an
easy target. In such instances, patients could be reluctant to install such applications on
their mobile devices for fear of data exposure to unknown individuals. According to
Alsaleh & Alshamari(2016), there are six different types of risks. These include
performance risk, privacy risk, time risk, psychological risk, financial risk, and social
risk. Privacy risk is of greatest importance when it comes to health-related e-services.
With such risks, face-to-face communications become the only option for patients who
feel such devices would impact negatively on their privacy. Furthermore, other than
privacy, patients find it easier to explain their conditions to a doctor physically rather than
having to send information through the various mHealth platforms.
Security concerning the mHealth products implies the ability of the products to ensure
information is relayed from one party to another without any breakdown. Such
information could be from one department to another, from the healthcare provider to the
patient or from one institution to another within the health sector. Any mHealth product
that achieves this primary goal is highly adopted as it makes communication more
efficient. Also, security between the user and the consumer is critical in health care.
Patients are always anxious about their health status and if a technology product could
relay results more effectively, patients will be willing to spend any amount to get such
products. Getting real-time information and real-time updates about a condition are
beneficial for the patients as they can track their health progress.
2.4 Individual Factors and Adoption of mHealth Products
This examines the individual at the micro-level, seeking to provide insight as to the
psychological influences that affect an individual‟s decision-making process. This
concerns both the customer and the providers (employees). Factors here include
22
demographics, level of education, age, gender, cultural background, attitude and
behaviour as well as psychological mind state. Technology Adoption Model is the mostly
widely accepted and used theory to explain why individuals accept new information
technology and systems (Surendran, 2013). Conceptualized by Davis (1989), it is based
on principles of theory of reasoned action. According to TAM two main factors, which
can be considered individual factors, influence technology use behaviour, this is,
perceived usefulness and perceived ease of use.
People have varied views about different technologies depending on their perceptions and
attitude. The adoption of mHealth products by an individual depends on the ability of
such products to meet their needs and expectations. Any shortcoming with the products
could result in an unwillingness to adopt the technologies (Mwobobia, 2012). In regions
such as Europe, individuals have been enlightened by technology and they find nearly all
forms of innovation beneficial. Hence, they readily adopt a new development in
technology with little resistance.
Exposure to different mHealth products plays a critical role in making it easy to penetrate
the market with new products. Advanced countries take new products as new
developments meant to improve their healthcare experience. However, people with little
experience in new technology would otherwise have a negative view of the new
developments, and are likely to resist such developments (McNair et al., 2018). For better
penetration of mHealth products in developing countries, there is a need for more
awareness on their importance to dispel the fears among people who believe that
technology in the health sector has a higher risk of exposing them to harm such as private
data leakage, as compared to its perceived benefits.
2.4.1 Perceived Benefits of Technology Use
Perceived benefit of use of technology is a major individual influencer for adoption of
technology. People are assumed to adopt technology if it is believed to offer or contribute
additionally benefit to the current or existing system of doing things (Akter et al, 2019).
Due to advanced technology, the difficulty of using cell phones has drastically dropped,
call quality has increased over time due to improved satellite and wireless use. Other
services like messaging (SMS), voice communication and wireless communication
services have as well improved with advancement in technology. In addition to that,
developing countries, such as Bangladesh have developed different platforms of offering
23
services via cell phones. Examples include Obopay for bank services, Manoshi-healthcare
services and Janala-used in education. The entire healthcare delivery in Bangladesh today
is transformed and the accessibility of the services is enhanced through mobile
technology. In Kenya mobile technology use has been popularized by innovations in
mobile financial services such as using MPESA which was reported to have 20.5 million
active daily users in a country with a population of 40 million people (Alushula, 2019).
On a study on MPESA adoption, perceived usefulness was found to be one of the major
contributing factors to its wide acceptance and use (Morawczynski & Pickens, 2009).
The health sector has continued to experience massive changes in operations as a result of
technological advancement. The integration of technology into the different sections of
health care systems in Kenya has made service delivery not only accessible but also
affordable. The roll-out of Mobile Health products has been received overwhelmingly
well by most of the health care practitioners as it has made their work easier(McNair et
al., 2018). The implementation of these technologies has been affected by numerous
factors which occur at the technical, social, and even individual levels. In the current
review, the focus goes for the set of individual factors which have impacted on the
adoption of mHealth products.
2.4.2 Perceived Ease of Use
Perceived ease of use is seen as the extent to which a user of a technology believes the
using the technology will require minimum effort to achieve required output (Davis,
1989). It has been shown to be directly and positively correlated to adoption on new
technology and information systems (Venkatesh & David, 2000). mHealth can be shown
to reduce the effort needed in several aspects of healthcare such as health record because
these can be stored in the cloud servers for easy access on phones for example in
accessing all patients‟ history electronically. According to records management procedure
manual for public service (McNair et al., 2018), electronic records management system is
an electronic system that manages the capture, storage, location and retrieval of records
electronically. It is important to note that technology is changing so fast such that
organizations are sometimes unable to adopt the new technology in time and are forced to
use traditional methods of production and delivery. Government departments for example
are also slow to adapt to these changes. According to McGaughey, Gunasekaran, & Ngai
(2008), electronic records management is one of the recent and fast-growing applications
24
of e-commerce having been embraced with organizations, governments and personal
investors who are seeking great business transactions and, or activities. Its utilization in
various organizations has been enabled by its fast evolution, value saving ability, ease of
information entry and high potency. Most developing and developed countries, for
example, are in the run to implementing electronic records management technologies to
enhance transparency while at the same time minimize losses in their operations.
The fundamental principle of any government is to put together its document in good
state, in order for efficiency and effectiveness. The method though which this is achieved
should, however, be objective-oriented, open and clear. However, the lack of political
goodwill, auditing, public participation, and corruption poses serious drawbacks to
achieving openness and responsiveness. For example, in Kenya is structured into national
and county governments. This is according to the primary Schedule of the Constitution of
Kenya (COK) which outlines the institutions of the forty-seven county governments
within the Republic of Kenya (GOK, 2010). The introduction of mHealth stands a better
chance to reduce corruption cases in health services, which can be now be accessed and
paid via phone directly to health institutions without having to pay cash to corrupt
individuals. This is seen as a major incentive to facilitate the adoption of technology by
Government and its partners.
Current measures have been initiated to boost public service delivery, through ehealth
initiatives such as the utilization of electronic records. It is on this that the government
when signing performance contracts with the ministries has outlined electronic records as
one of the requirements to be met by the ministries. This demonstrates the Ministry of
health commitment to the implementation of the constitutional and legislative provisions
geared towards streamlining healthcare service delivery. Nath & Angeles(2007),
specifically explored the challenges to mHealth management and determined vital
problems such as lack of system integration and standardization and immatureness of
mHealth management market services with different systems. The adoption of mHealth
management could have a round-faced variety of challenges in its adoption.
According to Reem(2017),the advantages of distributing mHealth are very clear. As a
base, information makers ought to append mHealth to every one of the information that
they distribute, and the Web Best Practices gives a decent beginning stage. To get the
most extreme advantage from distributing this mHealth however, information makers
25
ought to go above and beyond. This is achievable by ensuring they distribute mHealth to
a similar standard or, at any rate, should look for operable answers for guarantee that the
information they are distributing turns out to be effortlessly discoverable to any potential
information clients crosswise over stages.
With the above in place, ease of use should focus on the design of systems that will be
used by the patients and health service providers. A human centred design approach
should be employed in developing mHealth technologies to guarantee easy to use
innovations. mHealth technologies have in the past focused on features and productivity
rather than on the user experience. As such, poorly designed products are difficult to use
and end up having low user adoption or retention. MPESA a widely adopted mobile
financial services application in Kenya was found to also have a high adoption rate due to
its high perceived ease of use and access (Morawczynski & Pickens, 2009).In a study of
factors affecting the adoption of technology in Kenya Revenue Authority (KRA) by
Mwambia(2015), she found that the use of a complicated interface, discouraged
individuals from interacting with the system. A complete user centred redesign of the
system in use was recommended, in order to reduce resistance and increase utilization of
the system. Kariuki (2016) found that barriers such as use of English language rather than
local language, compatibility challenges with using the same mobile application on
different platform mobile phones, and poorly designed graphic user interfaces. This,
points out the challenge with poorly designed products, that ultimately result in low user
engagement and poor adoption rates.
2.4.3 Adoption of mHealth
According to Lorenz (2017), the most appropriate way to ensure that change is effected in
health behaviour is by understanding the motivation behind the change itself. The factors
described previously in the chapter highlight the motivators behind adoption of mHealth.
Additionally, adoption of technology, can be measured by determining either the
intention to use of the technology or the actual usage of the technology (Venkatesh et al.,
2003).
Behaviour has a lot of doing with personal feelings towards mHealth products. It can be
influenced by the level of education as those individuals who are not good in technology
would readily develop a negative attitude towards technology products. Nath & Angeles
(2007) found that with a pre-existing negative attitude towards technology, it becomes
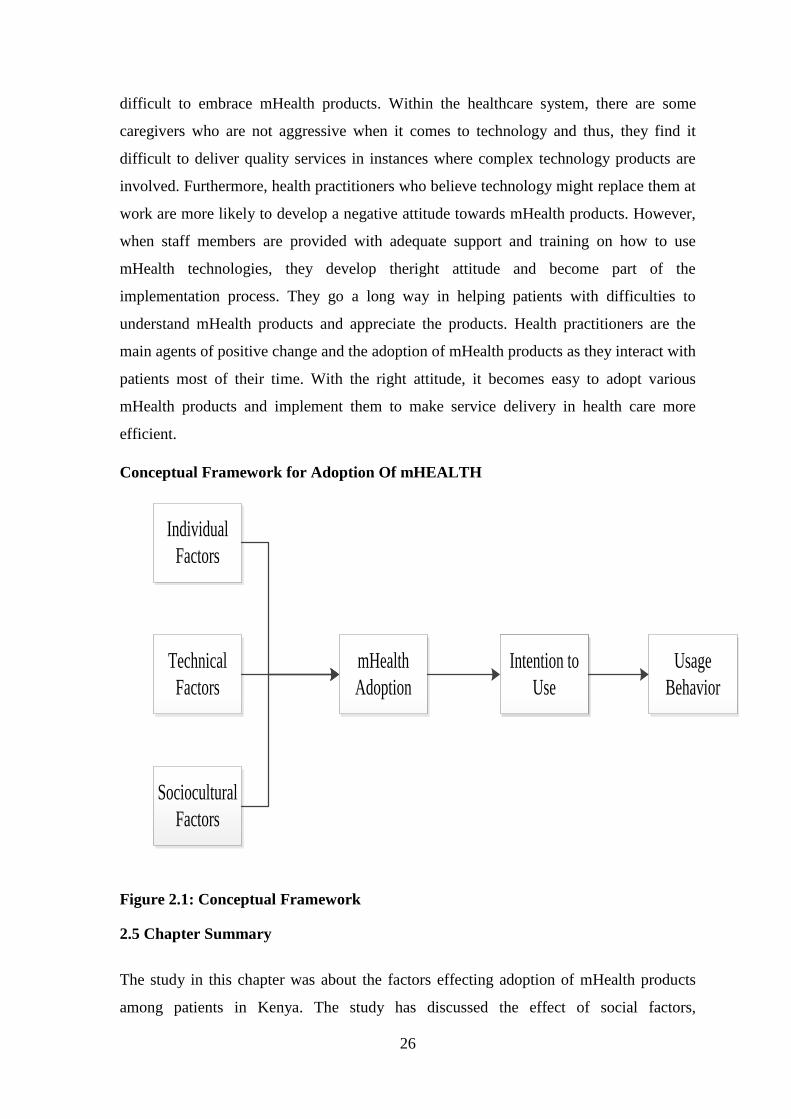
26
difficult to embrace mHealth products. Within the healthcare system, there are some
caregivers who are not aggressive when it comes to technology and thus, they find it
difficult to deliver quality services in instances where complex technology products are
involved. Furthermore, health practitioners who believe technology might replace them at
work are more likely to develop a negative attitude towards mHealth products. However,
when staff members are provided with adequate support and training on how to use
mHealth technologies, they develop theright attitude and become part of the
implementation process. They go a long way in helping patients with difficulties to
understand mHealth products and appreciate the products. Health practitioners are the
main agents of positive change and the adoption of mHealth products as they interact with
patients most of their time. With the right attitude, it becomes easy to adopt various
mHealth products and implement them to make service delivery in health care more
efficient.
Conceptual Framework for Adoption Of mHEALTH
Individual
Factors
Technical
Factors
Sociocultural
Factors
mHealth
Adoption
Intention to
Use
Intention to
Use
Usage
Behavior
Figure 2.1: Conceptual Framework
2.5 Chapter Summary
The study in this chapter was about the factors effecting adoption of mHealth products
among patients in Kenya. The study has discussed the effect of social factors,
27
technological factors, and individual factors on adoption of mHealth products. The next
chapter, research methodology, explores the best methodology the research adopted to
reach the solution of the research problem.
28
CHAPTER THREE
3.0 METHODOLOGY
3.1 Introduction
This section entails the study methodology applied in conducting this research.
Specifically, it outlines the research design of the study with a justification on the criteria
used, why and how each item was determined and chosen. It shall discuss the study
population and sampling design. It describes the data collection methods used in the
study. The research procedures used are presented. Finally, it presents the data analysis
methods and a summary of the chapter. It takes into consideration understandings
borrowed from similar studies of different literatures.
3.2 Research Design
This study employed descriptive research type of design due to the nature of study. This
design was chosen due to its capability of establishing bivariate relationships between the
variables observed. However, it is noted that these relationships are only correlative and
not causative. The objective of this research design is to present descriptions of
characteristics or phenomena linked with respondent‟s population, approximations of the
magnitudes of a population with the identified features and innovation of relations
amongst the diverse variables (Cooper & Schindler, 2014). The results are described in
words, pictures, chart or tables. This design is justified as it enables the researcher to
make inferences as to the factors influencing adoption of mHealth products in users in
Kenya.
The study used analytical models to infer relationships concerning the study variables.
The dependent variable in this study was intention to use mHealth products, while the
independent variables were technical factors, social factors and individual influences that
affect the adoption of mHealth products.
Quantitative research design was selected for this study. Data collection was done with
the help of questionnaires. To ensure validity, questions were adopted from
aforementioned studies, reviewed and reworded to fit the framework of this study. The
reworded questionnaire received an expert academic review from the professor
supervising the project. Additionally, a 10 person pilot/ pre-test was conducted to ensure
the questions were clearly understood and properly structured. The collected data out of
29
the questionnaires was also scrubbed for errors in biases, responses, omission, and
exaggeration.
3.3 Population and Sampling Design
3.3.1 Population
The population of a study is well-defined as the entire group of objects or events that have
common or similar characteristics which are observable (Mbwesa, 2006). For this study,
the population was recognized as any individual above the age of 18 years living or
working within Embu County, central business district with an estimate population of
144,347 (KNBS, 2009). The researcher chose Embu Town centre due to its central
location and the diversity of people found in this area. This study therefore focused on
144, 347 people living in Embu town.
Table 3.1: Population Distribution
Category Population
Embu Town 144, 347
Source: (KNBS, 2009)
3.3.2 Sampling Design
This is the methodology through which a trial is drawn from a certain populace (Cooper
& Schindler, 2014). This describes how the researcher systematically selected their study
sample. This includes all the activities carried out in gathering the research study. The
study used a structured close-ended questionnaire that was distributed to the entire study
population. The decision to use the close-ended questionnaires was driven by the
capability of the technique to collect an extensive variety of information within a time
convenient manner. Besides, questionnaires were easy and quick to answer conclusive
questions and facilitate fast data analysis. For clarity and for detailed information the
researcher also used interview schedules in order to get more detailed information when it
comes to gathering of information from the respondents without disclosing their details.
3.3.2.1 Sampling Frame
This institutes all the study essentials available to the investigator at that time in which
the study is carried out. This is usually a segment of the population from which the

30
researcher draws their sample (Cooper & Schindler, 2014). In this study the sampling
frame was adult persons above the age of 18 years in Embu Central Business District.
3.3.2.2 Sampling Technique
The tactic which the researcher uses in selecting a fraction out of the entire population is
the sampling technique. It includes choosing a group of individuals, procedures or
behaviour with the aim of carrying out a study(Cooper & Schindler, 2014). This process
involves the study of a select portion of the population and the use of those findings to
make generalizations about the characteristics of the rest of the population.
This study used random sampling, where the questionnaire survey was conducted in a
natural setting in Embu central business district while the participants in the sampling
frame continued to undertake their daily routines. The participants were approached and
requested to respond to the questionnaire.
3.3.2.3 Sampling Size
This is well-defined as the number of essentials chosen by the research to be included in a
statistical sample. Due to the limited time and resources, choosing the correct sampling
size enables research to be feasible (Cooper & Schindler, 2014).
Yamane„s formula of 2001 was used to determine the sample size from the population. In
the sampling of people living in Embu town, a standard error of 5% was considered in
this sampling calculation. On a population of 144347, gives a sample of 277 respondents
a figure that will be adopted in this study. It provides a 95 percent level of confidence and
a maximum variability (p) =.05.
n = ___N___
1+N (e) 2
Where n is the sample size, N is the population size and e is the level of precision
n=___ 144347__ = 277 respondents
1+ 144347(0.05x0.05)
The Yamane (2001) formula was considered appropriate for use in this study, first,
because it is easy to use, and second, because empirical data shows this formula is widely
accepted for determining sample sizes in different contexts. It is evident that in any
31
sampling situation, complete accuracy cannot be guaranteed and conventional precision
errors which are widely accepted include precision errors of 0.01, 0.05 and 0.1. The
precision error for this study was 0.05.
3.4 Data Collection Methods
Survey instruments are tools used to collect data in research. These include
questionnaires, interviews, observation, and documentation. Instruments are useful as
they help researchers save resources such as time and money, required to collect large
volumes of data. The following activities were conducted: adoption and designing of the
questionnaire, pilot testing, redesigning and filling of the questionnaire by the
respondents.
The researcher adopted the questionnaire from previous studies conducted by skilled
experts in order to reduce cost and time for the research. The questionnaire collected
demographic data, technical factors, social factors, individual factors and behavioural
intention to use mHealth products.
To enhance response to the questionnaire, the following structure was used in its design.
The questionnaire starts with a small overview to the research project. Its first section
includes simple demographic questions. The second section includes simple questions on
the variables, structured on a table for easy response. This section included closed ended
questions in the form of a 7-point Likert scale. The responses recorded the level of
agreement to the questionnaire statements. The scale was as follows, (1) Disagree
strongly; (2) Disagree; (3) Somewhat disagree; (4) Neither agree or disagree; (5)
Somewhat agree; (6) Agree; (7) Agree strongly.
3.5 Research Procedures
The procedures involved pilot testing where the questionnaires were randomly given to
ten respondents in order to find out if in any case there is ambiguity in the questionnaires
and if there is any form of bias when it comes to questions. Therefore, the questionnaires
were tested on a rural setup in order to achieve the objective of using a group with similar
characteristics to those in the intended study in order to improve the prediction of study
outcome results. A 10-respondent pilot study was piloted prior to the main survey. This
created room for correcting questionnaires that may have been unclear for the study
respondents. The researcher aimed at classifying the reliability and validity of the test.
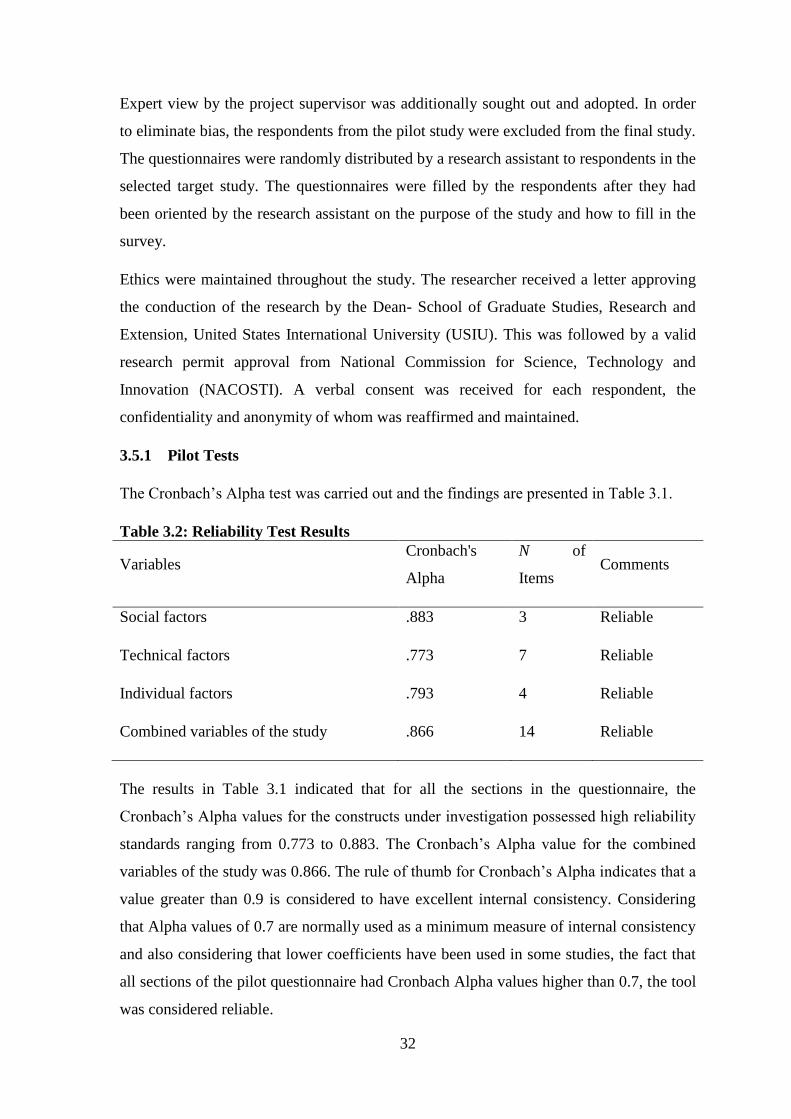
32
Expert view by the project supervisor was additionally sought out and adopted. In order
to eliminate bias, the respondents from the pilot study were excluded from the final study.
The questionnaires were randomly distributed by a research assistant to respondents in the
selected target study. The questionnaires were filled by the respondents after they had
been oriented by the research assistant on the purpose of the study and how to fill in the
survey.
Ethics were maintained throughout the study. The researcher received a letter approving
the conduction of the research by the Dean- School of Graduate Studies, Research and
Extension, United States International University (USIU). This was followed by a valid
research permit approval from National Commission for Science, Technology and
Innovation (NACOSTI). A verbal consent was received for each respondent, the
confidentiality and anonymity of whom was reaffirmed and maintained.
3.5.1 Pilot Tests
The Cronbach‟s Alpha test was carried out and the findings are presented in Table 3.1.
Table 3.2: Reliability Test Results
Variables Cronbach's
Alpha
N of
Items Comments
Social factors .883 3 Reliable
Technical factors .773 7 Reliable
Individual factors .793 4 Reliable
Combined variables of the study .866 14 Reliable
The results in Table 3.1 indicated that for all the sections in the questionnaire, the
Cronbach‟s Alpha values for the constructs under investigation possessed high reliability
standards ranging from 0.773 to 0.883. The Cronbach‟s Alpha value for the combined
variables of the study was 0.866. The rule of thumb for Cronbach‟s Alpha indicates that a
value greater than 0.9 is considered to have excellent internal consistency. Considering
that Alpha values of 0.7 are normally used as a minimum measure of internal consistency
and also considering that lower coefficients have been used in some studies, the fact that
all sections of the pilot questionnaire had Cronbach Alpha values higher than 0.7, the tool
was considered reliable.
33
3.6 Data Analysis Methods
Data analysis was done by use of the computer software Statistical Package for Social
Scientist (SPSS) on a Windows computer. The data was collected electronically using
Microsoft Excel. All the data was then coded and verified at point of data entry. Data
collected was 100% quantitative.
In both descriptive and inferential analysis was conducted. Descriptive analysis used
frequencies, percentages, means and other central tendencies. Relationships between the
dependent and independent variables were established by using correlations and
regression analysis. Statistical significance was considered prior to making any
interpretations from the data collected. The findings from the study were presented in
graphs, charts and tables.
3.7 Chapter Summary
This chapter brought into light the methodological way through which this study was
conducted. It starts with a short introduction. This is followed by a description of the
research design, the population and study design, and data collection methods used,
procedures used in research and the methods of data analysis methods used in the study.
The subsequent chapter presents the results and findings of the study on factors affected
the adoption of mHealth products in Kenya.
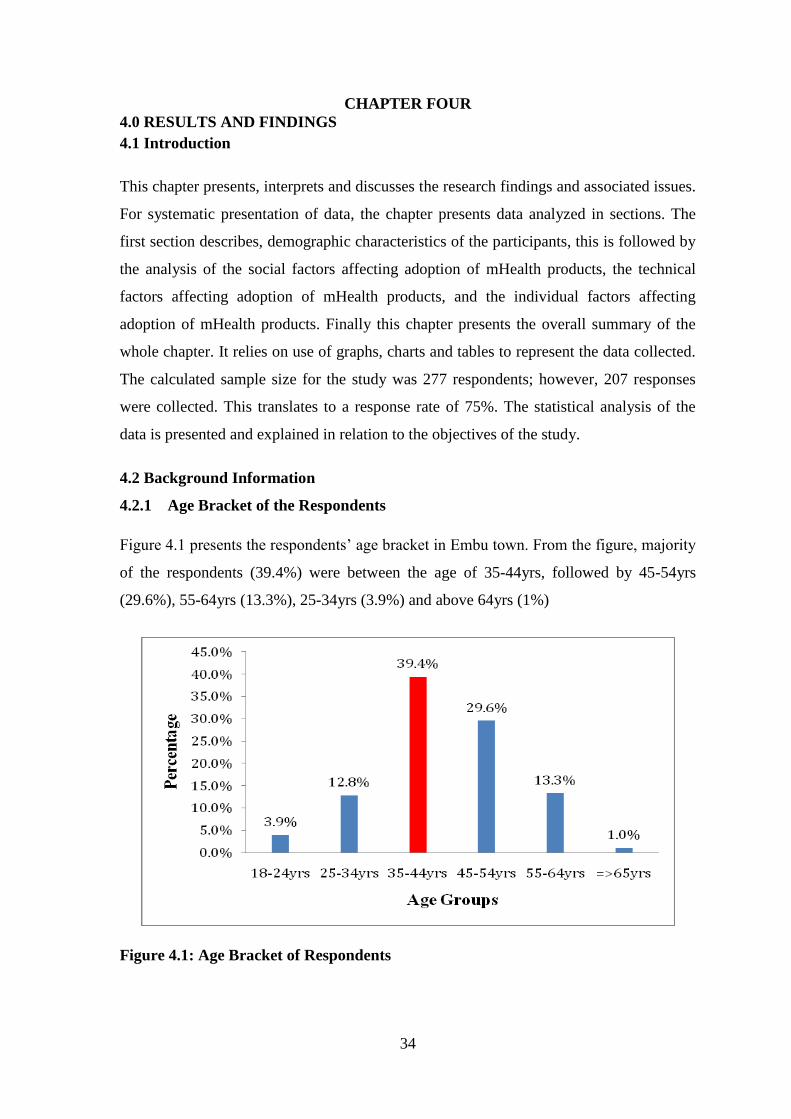
34
CHAPTER FOUR
4.0 RESULTS AND FINDINGS
4.1 Introduction
This chapter presents, interprets and discusses the research findings and associated issues.
For systematic presentation of data, the chapter presents data analyzed in sections. The
first section describes, demographic characteristics of the participants, this is followed by
the analysis of the social factors affecting adoption of mHealth products, the technical
factors affecting adoption of mHealth products, and the individual factors affecting
adoption of mHealth products. Finally this chapter presents the overall summary of the
whole chapter. It relies on use of graphs, charts and tables to represent the data collected.
The calculated sample size for the study was 277 respondents; however, 207 responses
were collected. This translates to a response rate of 75%. The statistical analysis of the
data is presented and explained in relation to the objectives of the study.
4.2 Background Information
4.2.1 Age Bracket of the Respondents
Figure 4.1 presents the respondents‟ age bracket in Embu town. From the figure, majority
of the respondents (39.4%) were between the age of 35-44yrs, followed by 45-54yrs
(29.6%), 55-64yrs (13.3%), 25-34yrs (3.9%) and above 64yrs (1%)
Figure 4.1: Age Bracket of Respondents
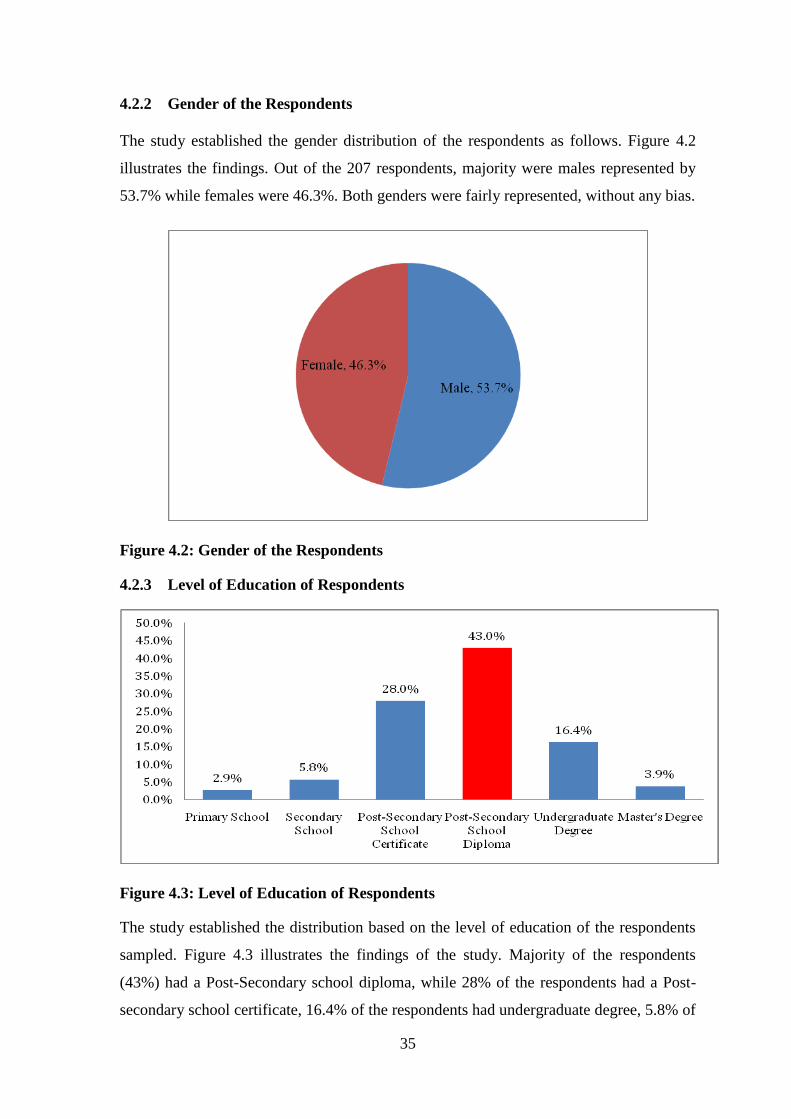
35
4.2.2 Gender of the Respondents
The study established the gender distribution of the respondents as follows. Figure 4.2
illustrates the findings. Out of the 207 respondents, majority were males represented by
53.7% while females were 46.3%. Both genders were fairly represented, without any bias.
Figure 4.2: Gender of the Respondents
4.2.3 Level of Education of Respondents
Figure 4.3: Level of Education of Respondents
The study established the distribution based on the level of education of the respondents
sampled. Figure 4.3 illustrates the findings of the study. Majority of the respondents
(43%) had a Post-Secondary school diploma, while 28% of the respondents had a Post-
secondary school certificate, 16.4% of the respondents had undergraduate degree, 5.8% of
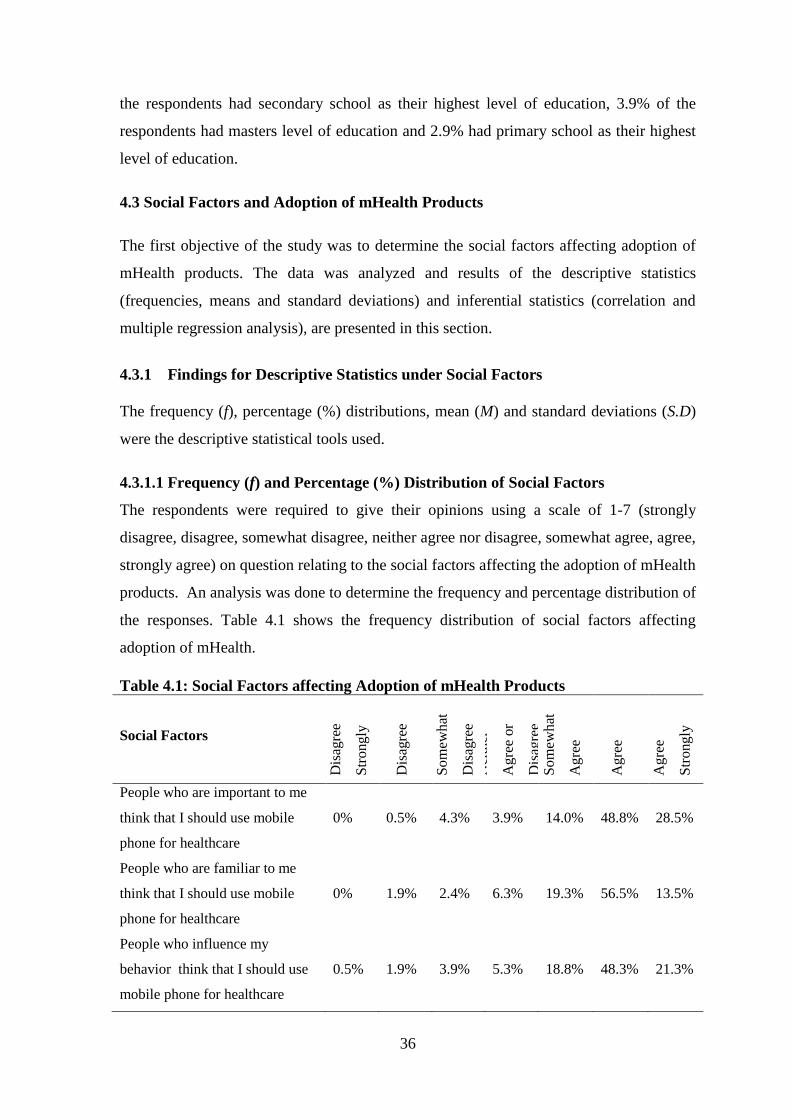
36
the respondents had secondary school as their highest level of education, 3.9% of the
respondents had masters level of education and 2.9% had primary school as their highest
level of education.
4.3 Social Factors and Adoption of mHealth Products
The first objective of the study was to determine the social factors affecting adoption of
mHealth products. The data was analyzed and results of the descriptive statistics
(frequencies, means and standard deviations) and inferential statistics (correlation and
multiple regression analysis), are presented in this section.
4.3.1 Findings for Descriptive Statistics under Social Factors
The frequency (f), percentage (%) distributions, mean (M) and standard deviations (S.D)
were the descriptive statistical tools used.
4.3.1.1 Frequency (f) and Percentage (%) Distribution of Social Factors
The respondents were required to give their opinions using a scale of 1-7 (strongly
disagree, disagree, somewhat disagree, neither agree nor disagree, somewhat agree, agree,
strongly agree) on question relating to the social factors affecting the adoption of mHealth
products. An analysis was done to determine the frequency and percentage distribution of
the responses. Table 4.1 shows the frequency distribution of social factors affecting
adoption of mHealth.
Table 4.1: Social Factors affecting Adoption of mHealth Products
Social Factors
Dis
agre
e
Str
ongly
Dis
agre
e
Som
ewhat
Dis
agre
e N
eith
er
Agre
e or
Dis
agre
e S
om
ewhat
Agre
e
Agre
e
Agre
e
Str
ongly
People who are important to me
think that I should use mobile
phone for healthcare
0% 0.5% 4.3% 3.9% 14.0% 48.8% 28.5%
People who are familiar to me
think that I should use mobile
phone for healthcare
0% 1.9% 2.4% 6.3% 19.3% 56.5% 13.5%
People who influence my
behavior think that I should use
mobile phone for healthcare
0.5% 1.9% 3.9% 5.3% 18.8% 48.3% 21.3%
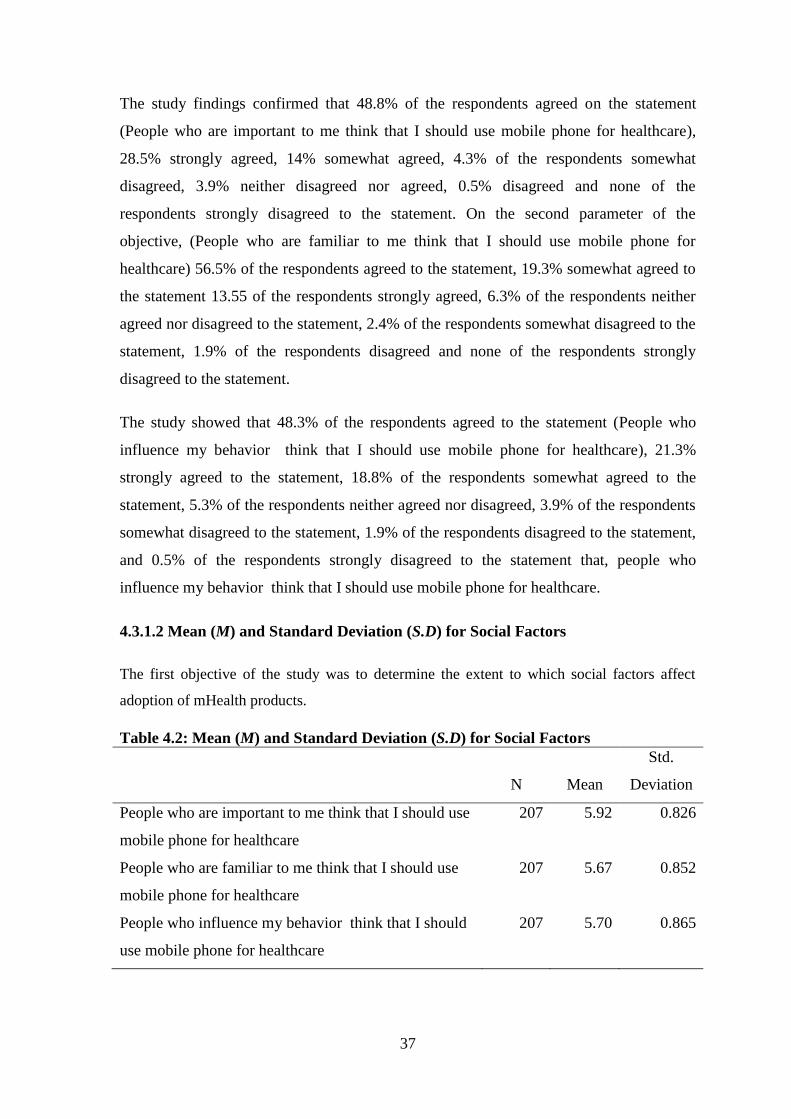
37
The study findings confirmed that 48.8% of the respondents agreed on the statement
(People who are important to me think that I should use mobile phone for healthcare),
28.5% strongly agreed, 14% somewhat agreed, 4.3% of the respondents somewhat
disagreed, 3.9% neither disagreed nor agreed, 0.5% disagreed and none of the
respondents strongly disagreed to the statement. On the second parameter of the
objective, (People who are familiar to me think that I should use mobile phone for
healthcare) 56.5% of the respondents agreed to the statement, 19.3% somewhat agreed to
the statement 13.55 of the respondents strongly agreed, 6.3% of the respondents neither
agreed nor disagreed to the statement, 2.4% of the respondents somewhat disagreed to the
statement, 1.9% of the respondents disagreed and none of the respondents strongly
disagreed to the statement.
The study showed that 48.3% of the respondents agreed to the statement (People who
influence my behavior think that I should use mobile phone for healthcare), 21.3%
strongly agreed to the statement, 18.8% of the respondents somewhat agreed to the
statement, 5.3% of the respondents neither agreed nor disagreed, 3.9% of the respondents
somewhat disagreed to the statement, 1.9% of the respondents disagreed to the statement,
and 0.5% of the respondents strongly disagreed to the statement that, people who
influence my behavior think that I should use mobile phone for healthcare.
4.3.1.2 Mean (M) and Standard Deviation (S.D) for Social Factors
The first objective of the study was to determine the extent to which social factors affect
adoption of mHealth products.
Table 4.2: Mean (M) and Standard Deviation (S.D) for Social Factors
N Mean
Std.
Deviation
People who are important to me think that I should use
mobile phone for healthcare
207 5.92 0.826
People who are familiar to me think that I should use
mobile phone for healthcare
207 5.67 0.852
People who influence my behavior think that I should
use mobile phone for healthcare
207 5.70 0.865
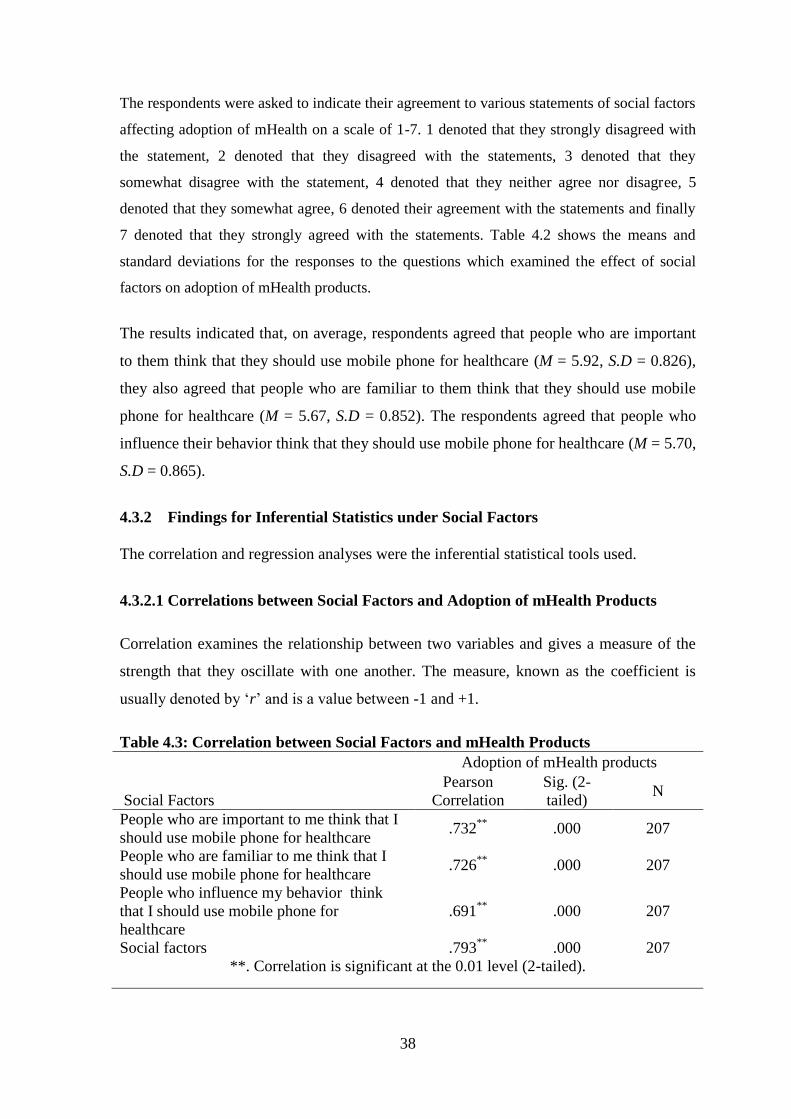
38
The respondents were asked to indicate their agreement to various statements of social factors
affecting adoption of mHealth on a scale of 1-7. 1 denoted that they strongly disagreed with
the statement, 2 denoted that they disagreed with the statements, 3 denoted that they
somewhat disagree with the statement, 4 denoted that they neither agree nor disagree, 5
denoted that they somewhat agree, 6 denoted their agreement with the statements and finally
7 denoted that they strongly agreed with the statements. Table 4.2 shows the means and
standard deviations for the responses to the questions which examined the effect of social
factors on adoption of mHealth products.
The results indicated that, on average, respondents agreed that people who are important
to them think that they should use mobile phone for healthcare (M = 5.92, S.D = 0.826),
they also agreed that people who are familiar to them think that they should use mobile
phone for healthcare (M = 5.67, S.D = 0.852). The respondents agreed that people who
influence their behavior think that they should use mobile phone for healthcare (M = 5.70,
S.D = 0.865).
4.3.2 Findings for Inferential Statistics under Social Factors
The correlation and regression analyses were the inferential statistical tools used.
4.3.2.1 Correlations between Social Factors and Adoption of mHealth Products
Correlation examines the relationship between two variables and gives a measure of the
strength that they oscillate with one another. The measure, known as the coefficient is
usually denoted by „r‟ and is a value between -1 and +1.
Table 4.3: Correlation between Social Factors and mHealth Products
Social Factors
Adoption of mHealth products
Pearson
Correlation
Sig. (2-
tailed) N
People who are important to me think that I
should use mobile phone for healthcare .732
** .000 207
People who are familiar to me think that I
should use mobile phone for healthcare .726
** .000 207
People who influence my behavior think
that I should use mobile phone for
healthcare
.691**
.000 207
Social factors .793**
.000 207
**. Correlation is significant at the 0.01 level (2-tailed).
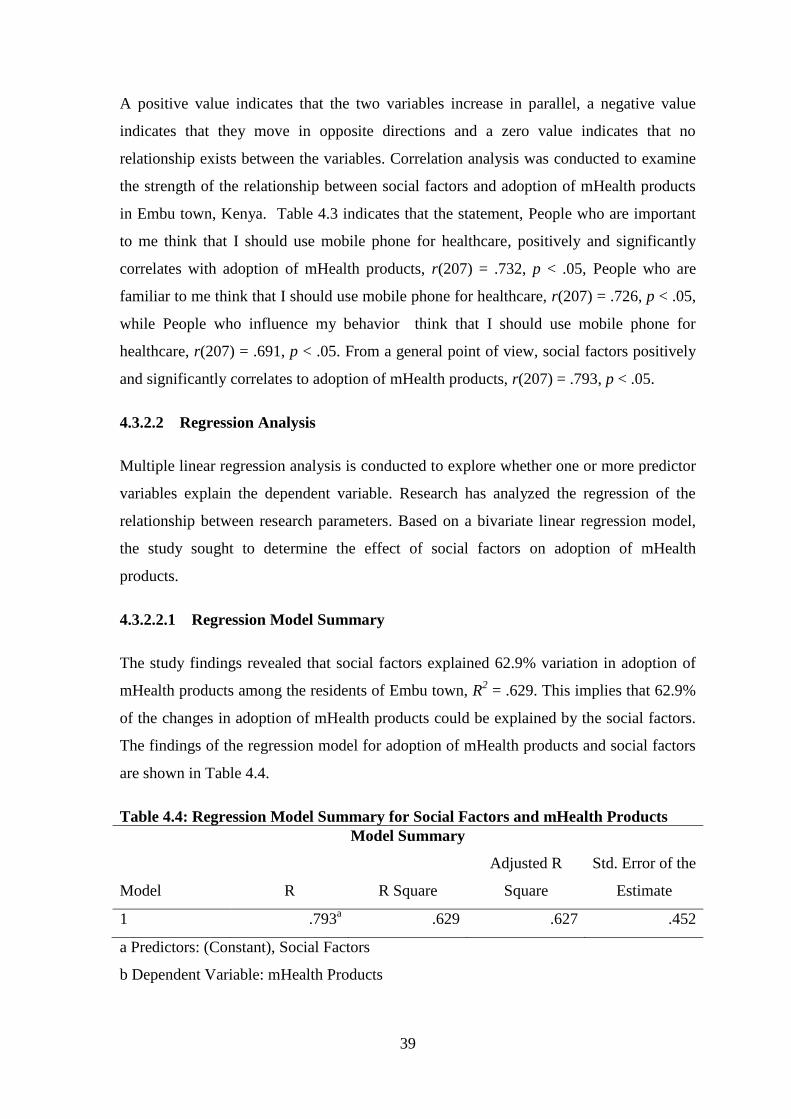
39
A positive value indicates that the two variables increase in parallel, a negative value
indicates that they move in opposite directions and a zero value indicates that no
relationship exists between the variables. Correlation analysis was conducted to examine
the strength of the relationship between social factors and adoption of mHealth products
in Embu town, Kenya. Table 4.3 indicates that the statement, People who are important
to me think that I should use mobile phone for healthcare, positively and significantly
correlates with adoption of mHealth products, r(207) = .732, p < .05, People who are
familiar to me think that I should use mobile phone for healthcare, r(207) = .726, p < .05,
while People who influence my behavior think that I should use mobile phone for
healthcare, r(207) = .691, p < .05. From a general point of view, social factors positively
and significantly correlates to adoption of mHealth products, r(207) = .793, p < .05.
4.3.2.2 Regression Analysis
Multiple linear regression analysis is conducted to explore whether one or more predictor
variables explain the dependent variable. Research has analyzed the regression of the
relationship between research parameters. Based on a bivariate linear regression model,
the study sought to determine the effect of social factors on adoption of mHealth
products.
4.3.2.2.1 Regression Model Summary
The study findings revealed that social factors explained 62.9% variation in adoption of
mHealth products among the residents of Embu town, R2 = .629. This implies that 62.9%
of the changes in adoption of mHealth products could be explained by the social factors.
The findings of the regression model for adoption of mHealth products and social factors
are shown in Table 4.4.
Table 4.4: Regression Model Summary for Social Factors and mHealth Products
Model Summary
Model R R Square
Adjusted R
Square
Std. Error of the
Estimate
1 .793a .629 .627 .452
a Predictors: (Constant), Social Factors
b Dependent Variable: mHealth Products
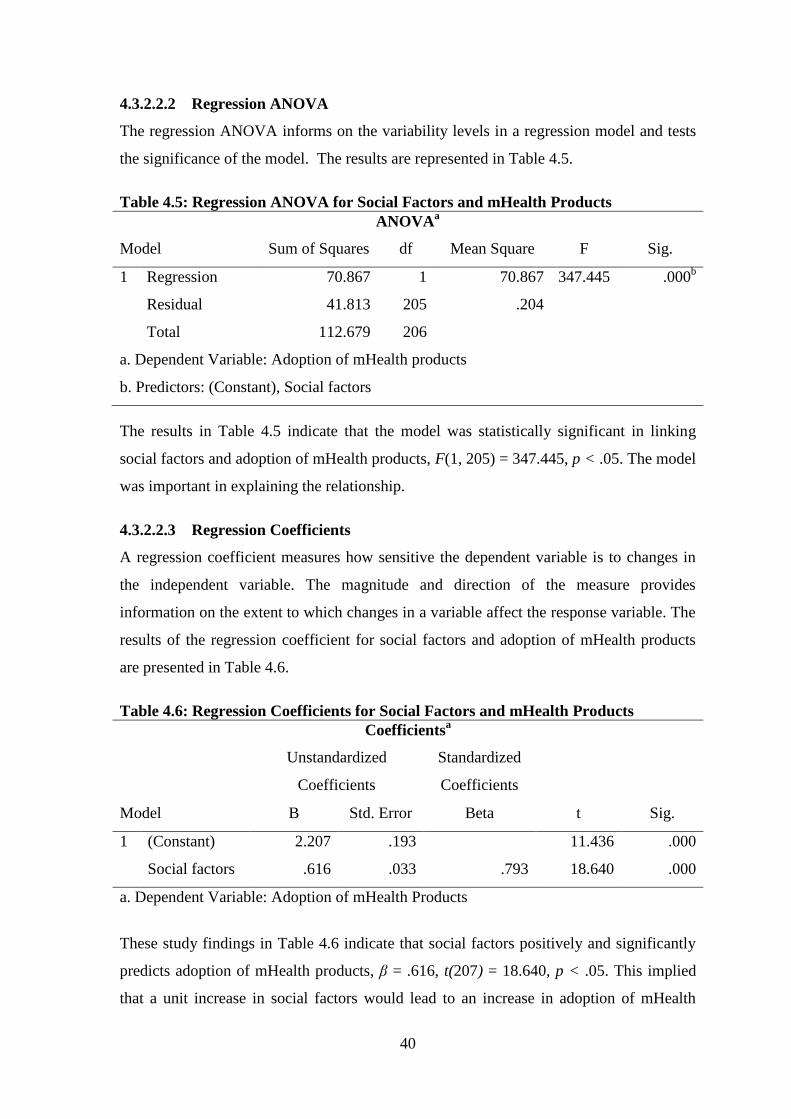
40
4.3.2.2.2 Regression ANOVA
The regression ANOVA informs on the variability levels in a regression model and tests
the significance of the model. The results are represented in Table 4.5.
Table 4.5: Regression ANOVA for Social Factors and mHealth Products
ANOVAa
Model Sum of Squares df Mean Square F Sig.
1 Regression 70.867 1 70.867 347.445 .000b
Residual 41.813 205 .204
Total 112.679 206
a. Dependent Variable: Adoption of mHealth products
b. Predictors: (Constant), Social factors
The results in Table 4.5 indicate that the model was statistically significant in linking
social factors and adoption of mHealth products, F(1, 205) = 347.445, p < .05. The model
was important in explaining the relationship.
4.3.2.2.3 Regression Coefficients
A regression coefficient measures how sensitive the dependent variable is to changes in
the independent variable. The magnitude and direction of the measure provides
information on the extent to which changes in a variable affect the response variable. The
results of the regression coefficient for social factors and adoption of mHealth products
are presented in Table 4.6.
Table 4.6: Regression Coefficients for Social Factors and mHealth Products
Coefficientsa
Model
Unstandardized
Coefficients
Standardized
Coefficients
t Sig. B Std. Error Beta
1 (Constant) 2.207 .193 11.436 .000
Social factors .616 .033 .793 18.640 .000
a. Dependent Variable: Adoption of mHealth Products
These study findings in Table 4.6 indicate that social factors positively and significantly
predicts adoption of mHealth products, β = .616, t(207) = 18.640, p < .05. This implied
that a unit increase in social factors would lead to an increase in adoption of mHealth
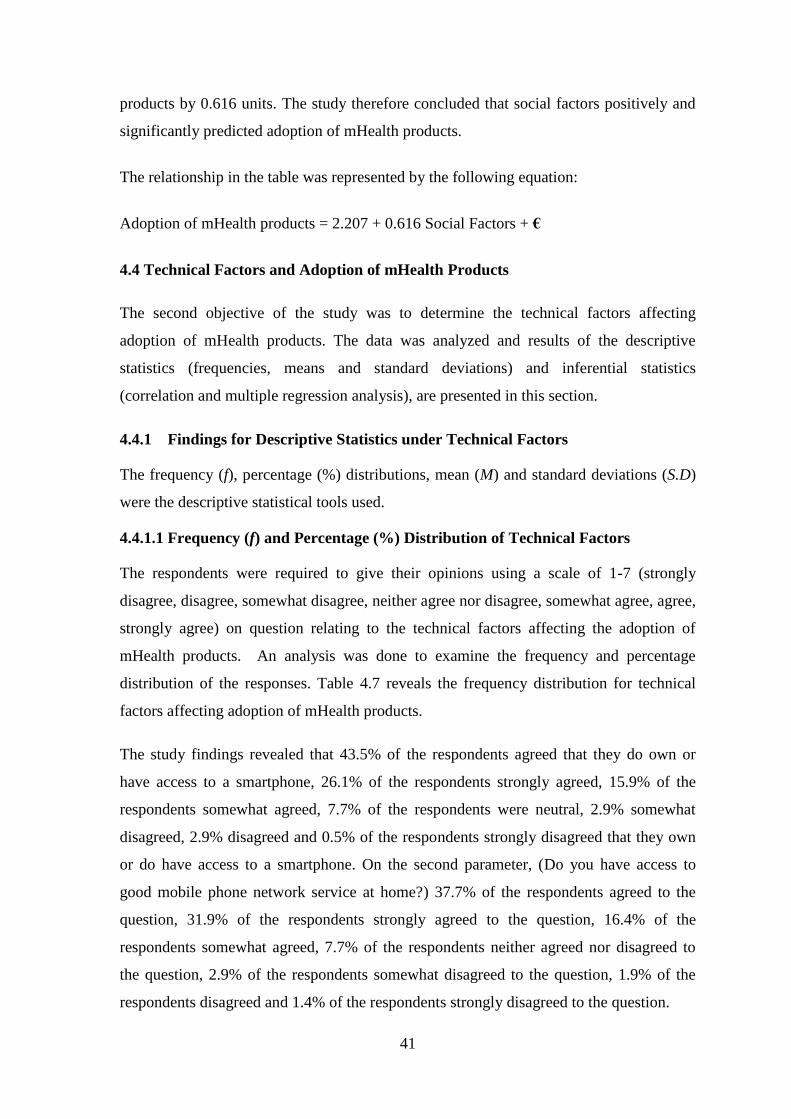
41
products by 0.616 units. The study therefore concluded that social factors positively and
significantly predicted adoption of mHealth products.
The relationship in the table was represented by the following equation:
Adoption of mHealth products = 2.207 + 0.616 Social Factors + €
4.4 Technical Factors and Adoption of mHealth Products
The second objective of the study was to determine the technical factors affecting
adoption of mHealth products. The data was analyzed and results of the descriptive
statistics (frequencies, means and standard deviations) and inferential statistics
(correlation and multiple regression analysis), are presented in this section.
4.4.1 Findings for Descriptive Statistics under Technical Factors
The frequency (f), percentage (%) distributions, mean (M) and standard deviations (S.D)
were the descriptive statistical tools used.
4.4.1.1 Frequency (f) and Percentage (%) Distribution of Technical Factors
The respondents were required to give their opinions using a scale of 1-7 (strongly
disagree, disagree, somewhat disagree, neither agree nor disagree, somewhat agree, agree,
strongly agree) on question relating to the technical factors affecting the adoption of
mHealth products. An analysis was done to examine the frequency and percentage
distribution of the responses. Table 4.7 reveals the frequency distribution for technical
factors affecting adoption of mHealth products.
The study findings revealed that 43.5% of the respondents agreed that they do own or
have access to a smartphone, 26.1% of the respondents strongly agreed, 15.9% of the
respondents somewhat agreed, 7.7% of the respondents were neutral, 2.9% somewhat
disagreed, 2.9% disagreed and 0.5% of the respondents strongly disagreed that they own
or do have access to a smartphone. On the second parameter, (Do you have access to
good mobile phone network service at home?) 37.7% of the respondents agreed to the
question, 31.9% of the respondents strongly agreed to the question, 16.4% of the
respondents somewhat agreed, 7.7% of the respondents neither agreed nor disagreed to
the question, 2.9% of the respondents somewhat disagreed to the question, 1.9% of the
respondents disagreed and 1.4% of the respondents strongly disagreed to the question.
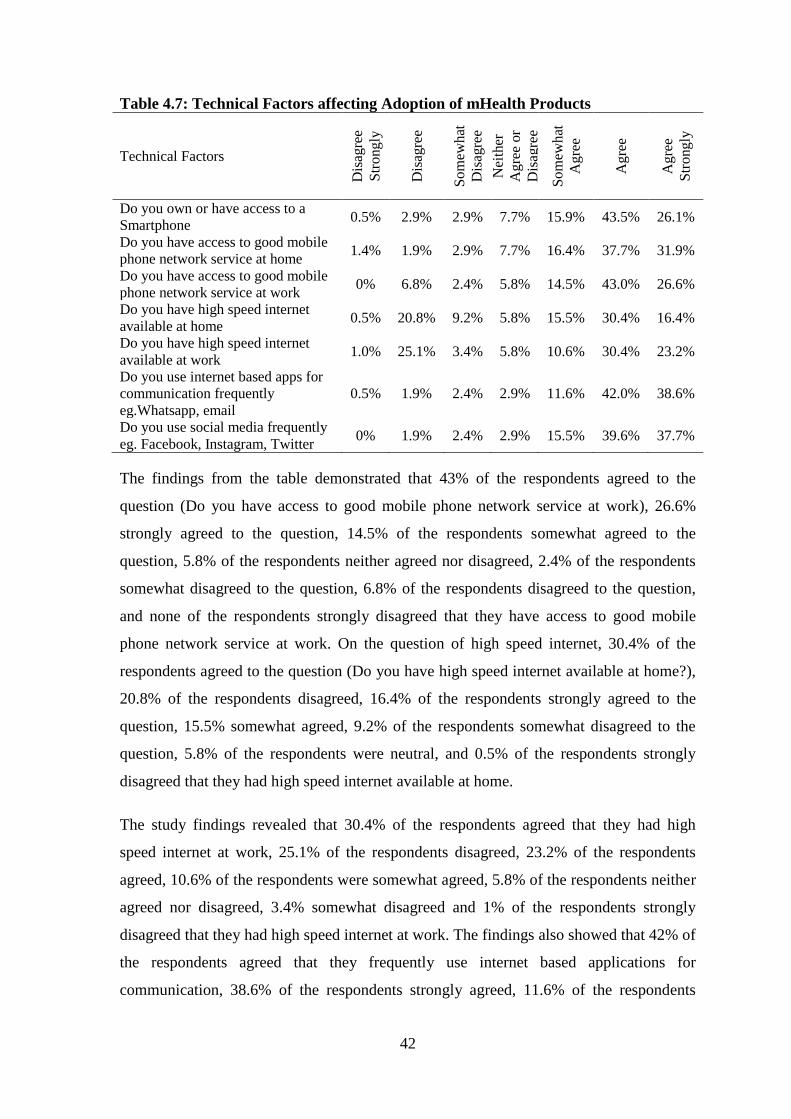
42
Table 4.7: Technical Factors affecting Adoption of mHealth Products
Technical Factors
Dis
agre
e
Str
ong
ly
Dis
agre
e
So
mew
hat
Dis
agre
e
Nei
ther
Ag
ree
or
Dis
agre
e
So
mew
hat
Ag
ree
Ag
ree
Ag
ree
Str
ong
ly
Do you own or have access to a
Smartphone 0.5% 2.9% 2.9% 7.7% 15.9% 43.5% 26.1%
Do you have access to good mobile
phone network service at home 1.4% 1.9% 2.9% 7.7% 16.4% 37.7% 31.9%
Do you have access to good mobile
phone network service at work 0% 6.8% 2.4% 5.8% 14.5% 43.0% 26.6%
Do you have high speed internet
available at home 0.5% 20.8% 9.2% 5.8% 15.5% 30.4% 16.4%
Do you have high speed internet
available at work 1.0% 25.1% 3.4% 5.8% 10.6% 30.4% 23.2%
Do you use internet based apps for
communication frequently
eg.Whatsapp, email
0.5% 1.9% 2.4% 2.9% 11.6% 42.0% 38.6%
Do you use social media frequently
eg. Facebook, Instagram, Twitter 0% 1.9% 2.4% 2.9% 15.5% 39.6% 37.7%
The findings from the table demonstrated that 43% of the respondents agreed to the
question (Do you have access to good mobile phone network service at work), 26.6%
strongly agreed to the question, 14.5% of the respondents somewhat agreed to the
question, 5.8% of the respondents neither agreed nor disagreed, 2.4% of the respondents
somewhat disagreed to the question, 6.8% of the respondents disagreed to the question,
and none of the respondents strongly disagreed that they have access to good mobile
phone network service at work. On the question of high speed internet, 30.4% of the
respondents agreed to the question (Do you have high speed internet available at home?),
20.8% of the respondents disagreed, 16.4% of the respondents strongly agreed to the
question, 15.5% somewhat agreed, 9.2% of the respondents somewhat disagreed to the
question, 5.8% of the respondents were neutral, and 0.5% of the respondents strongly
disagreed that they had high speed internet available at home.
The study findings revealed that 30.4% of the respondents agreed that they had high
speed internet at work, 25.1% of the respondents disagreed, 23.2% of the respondents
agreed, 10.6% of the respondents were somewhat agreed, 5.8% of the respondents neither
agreed nor disagreed, 3.4% somewhat disagreed and 1% of the respondents strongly
disagreed that they had high speed internet at work. The findings also showed that 42% of
the respondents agreed that they frequently use internet based applications for
communication, 38.6% of the respondents strongly agreed, 11.6% of the respondents
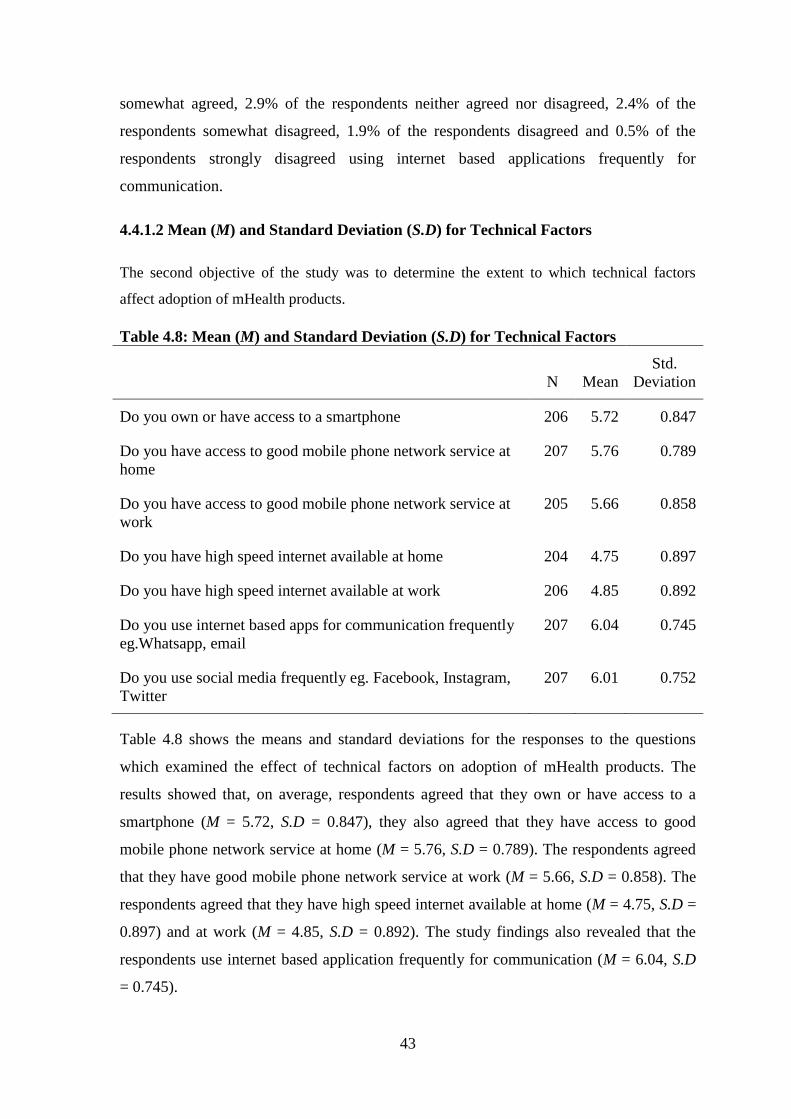
43
somewhat agreed, 2.9% of the respondents neither agreed nor disagreed, 2.4% of the
respondents somewhat disagreed, 1.9% of the respondents disagreed and 0.5% of the
respondents strongly disagreed using internet based applications frequently for
communication.
4.4.1.2 Mean (M) and Standard Deviation (S.D) for Technical Factors
The second objective of the study was to determine the extent to which technical factors
affect adoption of mHealth products.
Table 4.8: Mean (M) and Standard Deviation (S.D) for Technical Factors
N Mean
Std.
Deviation
Do you own or have access to a smartphone 206 5.72 0.847
Do you have access to good mobile phone network service at
home
207 5.76 0.789
Do you have access to good mobile phone network service at
work
205 5.66 0.858
Do you have high speed internet available at home 204 4.75 0.897
Do you have high speed internet available at work 206 4.85 0.892
Do you use internet based apps for communication frequently
eg.Whatsapp, email
207 6.04 0.745
Do you use social media frequently eg. Facebook, Instagram,
207 6.01 0.752
Table 4.8 shows the means and standard deviations for the responses to the questions
which examined the effect of technical factors on adoption of mHealth products. The
results showed that, on average, respondents agreed that they own or have access to a
smartphone (M = 5.72, S.D = 0.847), they also agreed that they have access to good
mobile phone network service at home (M = 5.76, S.D = 0.789). The respondents agreed
that they have good mobile phone network service at work (M = 5.66, S.D = 0.858). The
respondents agreed that they have high speed internet available at home (M = 4.75, S.D =
0.897) and at work (M = 4.85, S.D = 0.892). The study findings also revealed that the
respondents use internet based application frequently for communication (M = 6.04, S.D
= 0.745).
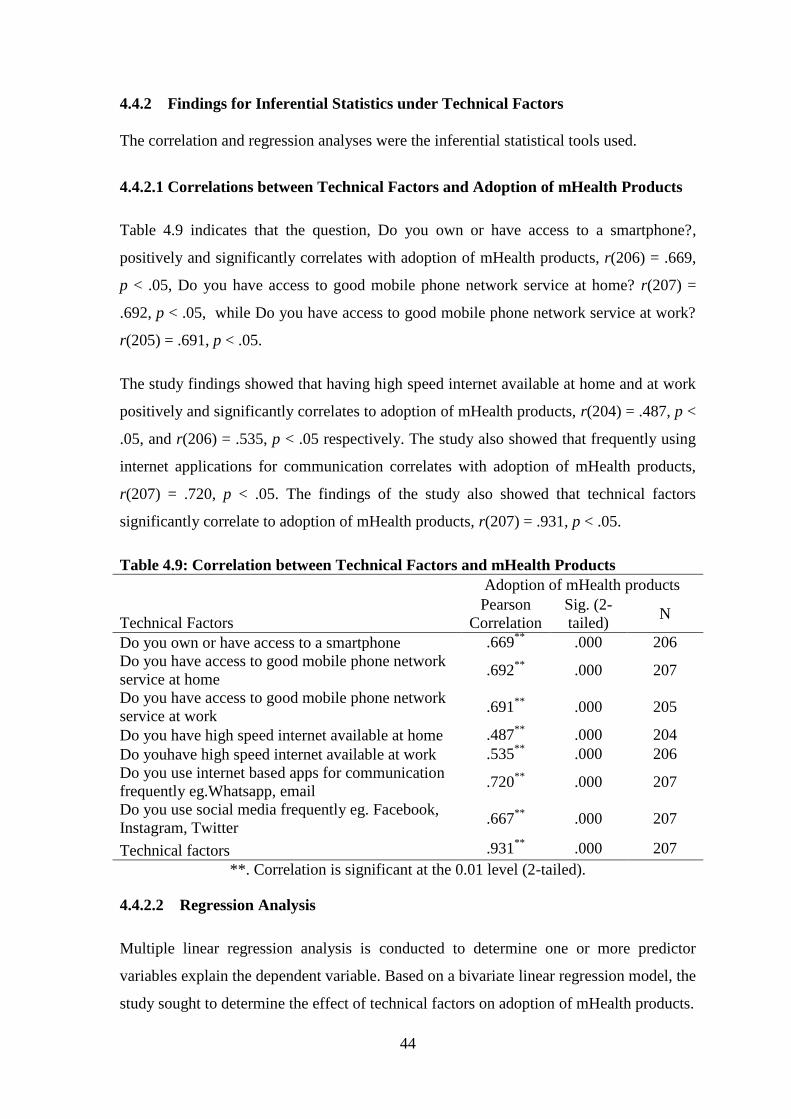
44
4.4.2 Findings for Inferential Statistics under Technical Factors
The correlation and regression analyses were the inferential statistical tools used.
4.4.2.1 Correlations between Technical Factors and Adoption of mHealth Products
Table 4.9 indicates that the question, Do you own or have access to a smartphone?,
positively and significantly correlates with adoption of mHealth products, r(206) = .669,
p < .05, Do you have access to good mobile phone network service at home? r(207) =
.692, p < .05, while Do you have access to good mobile phone network service at work?
r(205) = .691, p < .05.
The study findings showed that having high speed internet available at home and at work
positively and significantly correlates to adoption of mHealth products, r(204) = .487, p <
.05, and r(206) = .535, p < .05 respectively. The study also showed that frequently using
internet applications for communication correlates with adoption of mHealth products,
r(207) = .720, p < .05. The findings of the study also showed that technical factors
significantly correlate to adoption of mHealth products, r(207) = .931, p < .05.
Table 4.9: Correlation between Technical Factors and mHealth Products
Technical Factors
Adoption of mHealth products
Pearson
Correlation
Sig. (2-
tailed) N
Do you own or have access to a smartphone .669**
.000 206
Do you have access to good mobile phone network
service at home .692
** .000 207
Do you have access to good mobile phone network
service at work .691
** .000 205
Do you have high speed internet available at home .487**
.000 204
Do youhave high speed internet available at work .535**
.000 206
Do you use internet based apps for communication
frequently eg.Whatsapp, email .720
** .000 207
Do you use social media frequently eg. Facebook,
Instagram, Twitter .667
** .000 207
Technical factors .931**
.000 207
**. Correlation is significant at the 0.01 level (2-tailed).
4.4.2.2 Regression Analysis
Multiple linear regression analysis is conducted to determine one or more predictor
variables explain the dependent variable. Based on a bivariate linear regression model, the
study sought to determine the effect of technical factors on adoption of mHealth products.
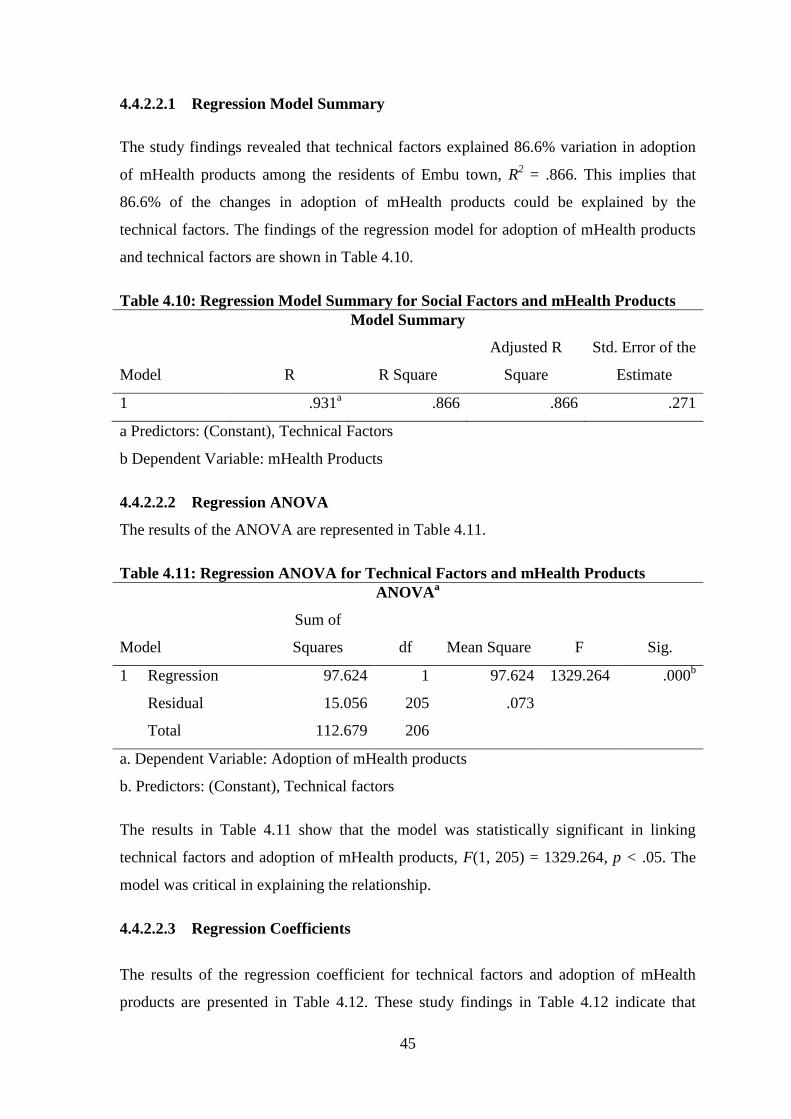
45
4.4.2.2.1 Regression Model Summary
The study findings revealed that technical factors explained 86.6% variation in adoption
of mHealth products among the residents of Embu town, R2 = .866. This implies that
86.6% of the changes in adoption of mHealth products could be explained by the
technical factors. The findings of the regression model for adoption of mHealth products
and technical factors are shown in Table 4.10.
Table 4.10: Regression Model Summary for Social Factors and mHealth Products
Model Summary
Model R R Square
Adjusted R
Square
Std. Error of the
Estimate
1 .931a .866 .866 .271
a Predictors: (Constant), Technical Factors
b Dependent Variable: mHealth Products
4.4.2.2.2 Regression ANOVA
The results of the ANOVA are represented in Table 4.11.
Table 4.11: Regression ANOVA for Technical Factors and mHealth Products
ANOVAa
Model
Sum of
Squares df Mean Square F Sig.
1 Regression 97.624 1 97.624 1329.264 .000b
Residual 15.056 205 .073
Total 112.679 206
a. Dependent Variable: Adoption of mHealth products
b. Predictors: (Constant), Technical factors
The results in Table 4.11 show that the model was statistically significant in linking
technical factors and adoption of mHealth products, F(1, 205) = 1329.264, p < .05. The
model was critical in explaining the relationship.
4.4.2.2.3 Regression Coefficients
The results of the regression coefficient for technical factors and adoption of mHealth
products are presented in Table 4.12. These study findings in Table 4.12 indicate that
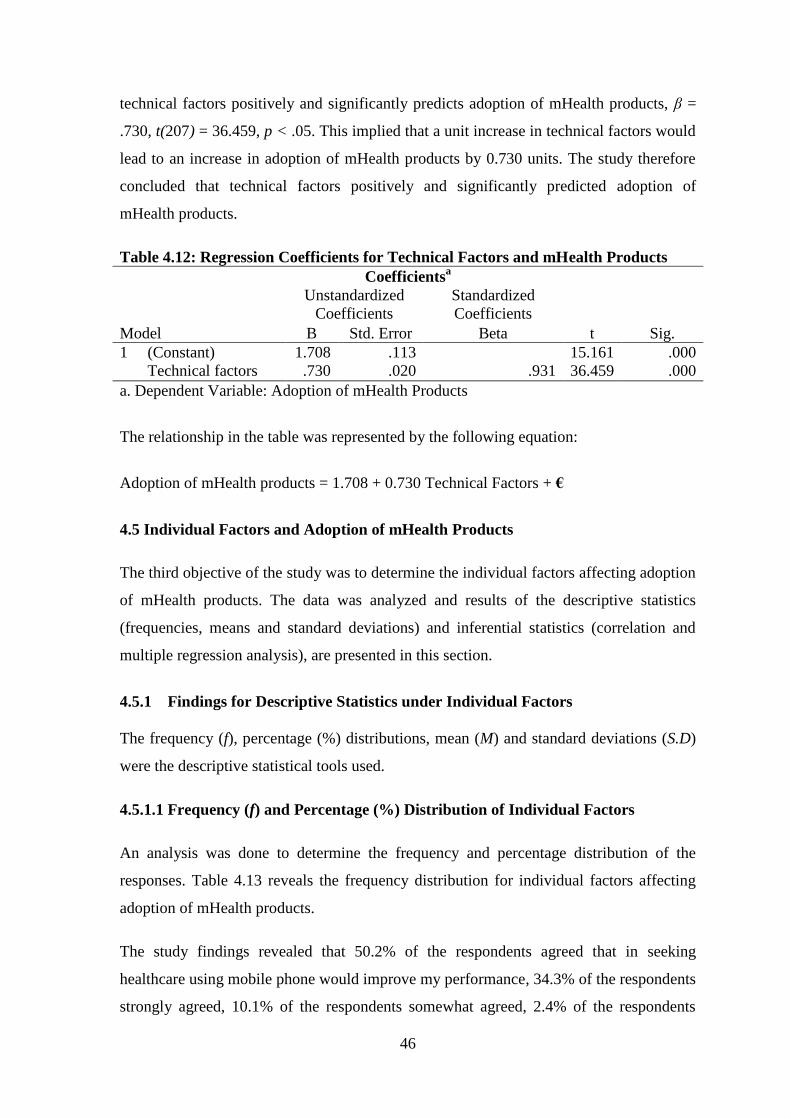
46
technical factors positively and significantly predicts adoption of mHealth products, β =
.730, t(207) = 36.459, p < .05. This implied that a unit increase in technical factors would
lead to an increase in adoption of mHealth products by 0.730 units. The study therefore
concluded that technical factors positively and significantly predicted adoption of
mHealth products.
Table 4.12: Regression Coefficients for Technical Factors and mHealth Products
Coefficientsa
Model
Unstandardized
Coefficients
Standardized
Coefficients
t Sig. B Std. Error Beta
1 (Constant) 1.708 .113 15.161 .000
Technical factors .730 .020 .931 36.459 .000
a. Dependent Variable: Adoption of mHealth Products
The relationship in the table was represented by the following equation:
Adoption of mHealth products = 1.708 + 0.730 Technical Factors + €
4.5 Individual Factors and Adoption of mHealth Products
The third objective of the study was to determine the individual factors affecting adoption
of mHealth products. The data was analyzed and results of the descriptive statistics
(frequencies, means and standard deviations) and inferential statistics (correlation and
multiple regression analysis), are presented in this section.
4.5.1 Findings for Descriptive Statistics under Individual Factors
The frequency (f), percentage (%) distributions, mean (M) and standard deviations (S.D)
were the descriptive statistical tools used.
4.5.1.1 Frequency (f) and Percentage (%) Distribution of Individual Factors
An analysis was done to determine the frequency and percentage distribution of the
responses. Table 4.13 reveals the frequency distribution for individual factors affecting
adoption of mHealth products.
The study findings revealed that 50.2% of the respondents agreed that in seeking
healthcare using mobile phone would improve my performance, 34.3% of the respondents
strongly agreed, 10.1% of the respondents somewhat agreed, 2.4% of the respondents
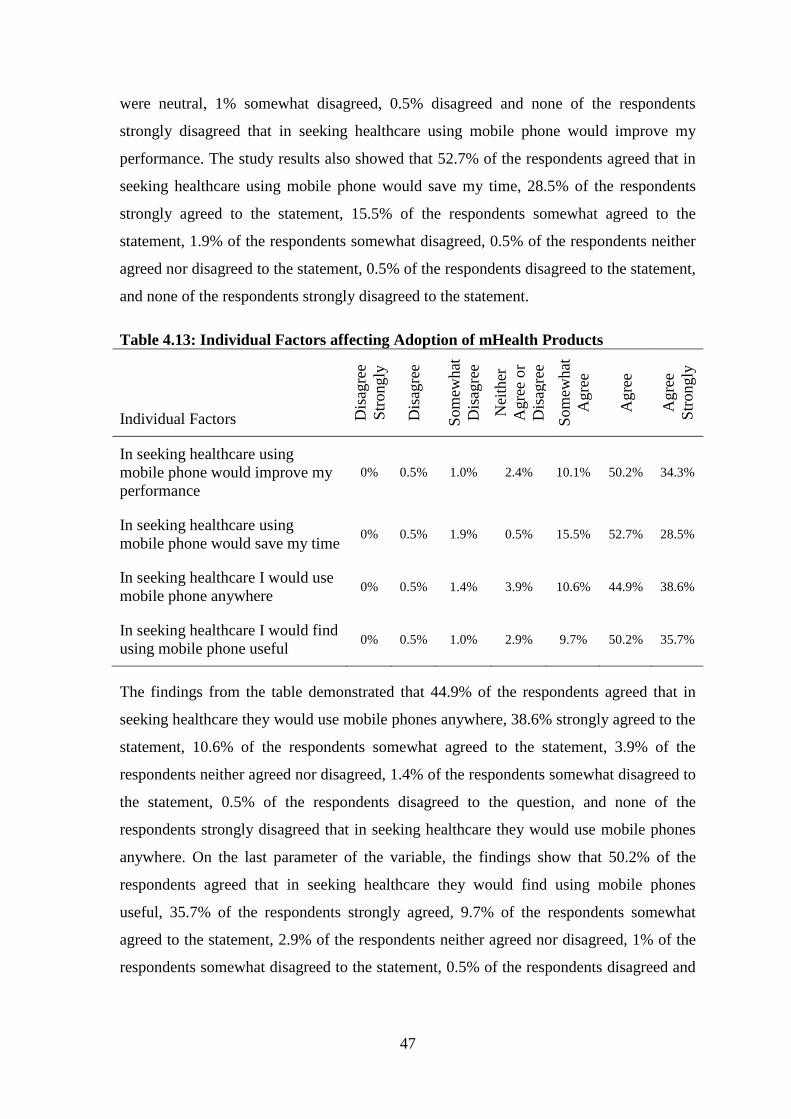
47
were neutral, 1% somewhat disagreed, 0.5% disagreed and none of the respondents
strongly disagreed that in seeking healthcare using mobile phone would improve my
performance. The study results also showed that 52.7% of the respondents agreed that in
seeking healthcare using mobile phone would save my time, 28.5% of the respondents
strongly agreed to the statement, 15.5% of the respondents somewhat agreed to the
statement, 1.9% of the respondents somewhat disagreed, 0.5% of the respondents neither
agreed nor disagreed to the statement, 0.5% of the respondents disagreed to the statement,
and none of the respondents strongly disagreed to the statement.
Table 4.13: Individual Factors affecting Adoption of mHealth Products
Individual Factors Dis
agre
e
Str
ongly
Dis
agre
e
Som
ewhat
Dis
agre
e
Nei
ther
Agre
e o
r
Dis
agre
e
Som
ewhat
Agre
e
Agre
e
Agre
e
Str
ongly
In seeking healthcare using
mobile phone would improve my
performance
0% 0.5% 1.0% 2.4% 10.1% 50.2% 34.3%
In seeking healthcare using
mobile phone would save my time 0% 0.5% 1.9% 0.5% 15.5% 52.7% 28.5%
In seeking healthcare I would use
mobile phone anywhere 0% 0.5% 1.4% 3.9% 10.6% 44.9% 38.6%
In seeking healthcare I would find
using mobile phone useful 0% 0.5% 1.0% 2.9% 9.7% 50.2% 35.7%
The findings from the table demonstrated that 44.9% of the respondents agreed that in
seeking healthcare they would use mobile phones anywhere, 38.6% strongly agreed to the
statement, 10.6% of the respondents somewhat agreed to the statement, 3.9% of the
respondents neither agreed nor disagreed, 1.4% of the respondents somewhat disagreed to
the statement, 0.5% of the respondents disagreed to the question, and none of the
respondents strongly disagreed that in seeking healthcare they would use mobile phones
anywhere. On the last parameter of the variable, the findings show that 50.2% of the
respondents agreed that in seeking healthcare they would find using mobile phones
useful, 35.7% of the respondents strongly agreed, 9.7% of the respondents somewhat
agreed to the statement, 2.9% of the respondents neither agreed nor disagreed, 1% of the
respondents somewhat disagreed to the statement, 0.5% of the respondents disagreed and
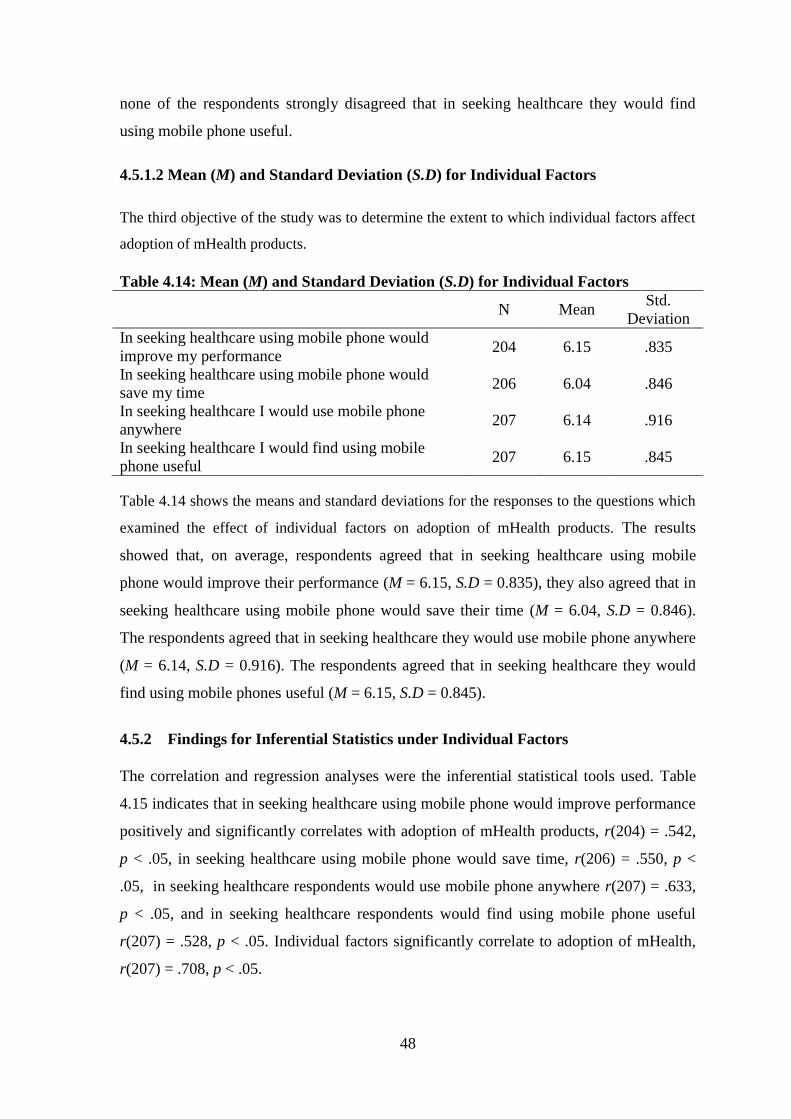
48
none of the respondents strongly disagreed that in seeking healthcare they would find
using mobile phone useful.
4.5.1.2 Mean (M) and Standard Deviation (S.D) for Individual Factors
The third objective of the study was to determine the extent to which individual factors affect
adoption of mHealth products.
Table 4.14: Mean (M) and Standard Deviation (S.D) for Individual Factors
N Mean
Std.
Deviation
In seeking healthcare using mobile phone would
improve my performance 204 6.15 .835
In seeking healthcare using mobile phone would
save my time 206 6.04 .846
In seeking healthcare I would use mobile phone
anywhere 207 6.14 .916
In seeking healthcare I would find using mobile
phone useful 207 6.15 .845
Table 4.14 shows the means and standard deviations for the responses to the questions which
examined the effect of individual factors on adoption of mHealth products. The results
showed that, on average, respondents agreed that in seeking healthcare using mobile
phone would improve their performance (M = 6.15, S.D = 0.835), they also agreed that in
seeking healthcare using mobile phone would save their time (M = 6.04, S.D = 0.846).
The respondents agreed that in seeking healthcare they would use mobile phone anywhere
(M = 6.14, S.D = 0.916). The respondents agreed that in seeking healthcare they would
find using mobile phones useful (M = 6.15, S.D = 0.845).
4.5.2 Findings for Inferential Statistics under Individual Factors
The correlation and regression analyses were the inferential statistical tools used. Table
4.15 indicates that in seeking healthcare using mobile phone would improve performance
positively and significantly correlates with adoption of mHealth products, r(204) = .542,
p < .05, in seeking healthcare using mobile phone would save time, r(206) = .550, p <
.05, in seeking healthcare respondents would use mobile phone anywhere r(207) = .633,
p < .05, and in seeking healthcare respondents would find using mobile phone useful
r(207) = .528, p < .05. Individual factors significantly correlate to adoption of mHealth,
r(207) = .708, p < .05.
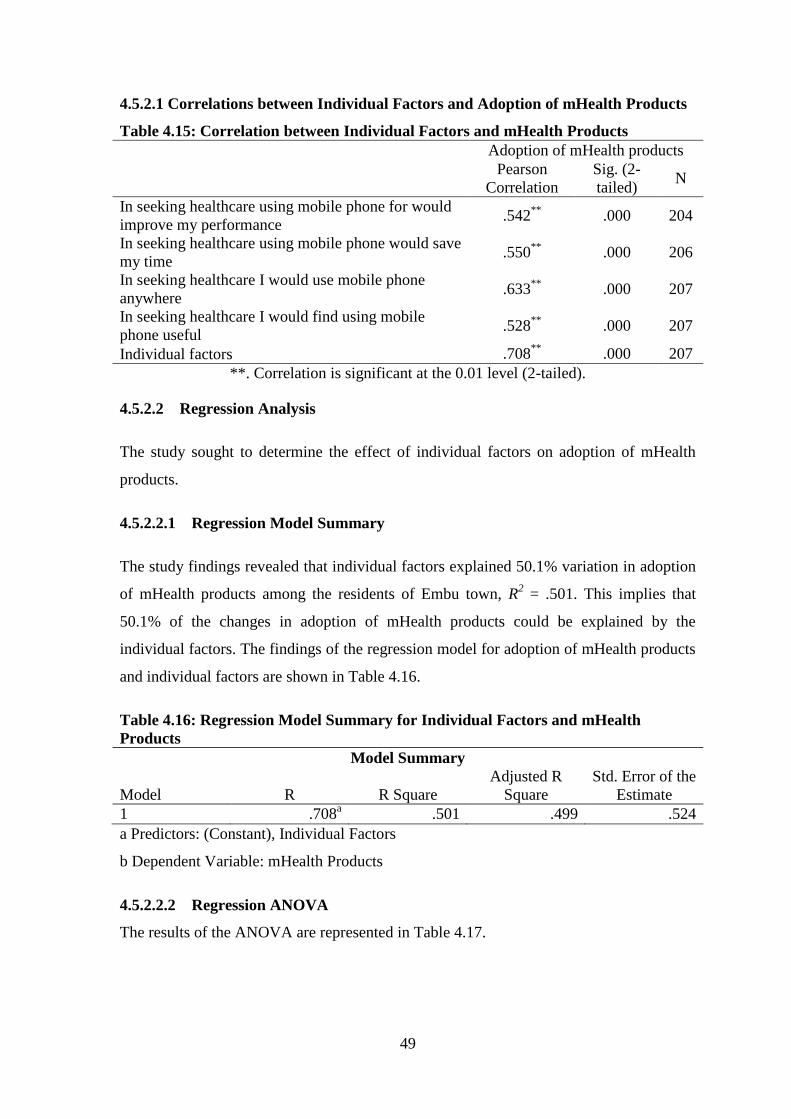
49
4.5.2.1 Correlations between Individual Factors and Adoption of mHealth Products
Table 4.15: Correlation between Individual Factors and mHealth Products
Adoption of mHealth products
Pearson
Correlation
Sig. (2-
tailed) N
In seeking healthcare using mobile phone for would
improve my performance .542
** .000 204
In seeking healthcare using mobile phone would save
my time .550
** .000 206
In seeking healthcare I would use mobile phone
anywhere .633
** .000 207
In seeking healthcare I would find using mobile
phone useful .528
** .000 207
Individual factors .708**
.000 207
**. Correlation is significant at the 0.01 level (2-tailed).
4.5.2.2 Regression Analysis
The study sought to determine the effect of individual factors on adoption of mHealth
products.
4.5.2.2.1 Regression Model Summary
The study findings revealed that individual factors explained 50.1% variation in adoption
of mHealth products among the residents of Embu town, R2 = .501. This implies that
50.1% of the changes in adoption of mHealth products could be explained by the
individual factors. The findings of the regression model for adoption of mHealth products
and individual factors are shown in Table 4.16.
Table 4.16: Regression Model Summary for Individual Factors and mHealth
Products
Model Summary
Model R R Square
Adjusted R
Square
Std. Error of the
Estimate
1 .708a .501 .499 .524
a Predictors: (Constant), Individual Factors
b Dependent Variable: mHealth Products
4.5.2.2.2 Regression ANOVA
The results of the ANOVA are represented in Table 4.17.
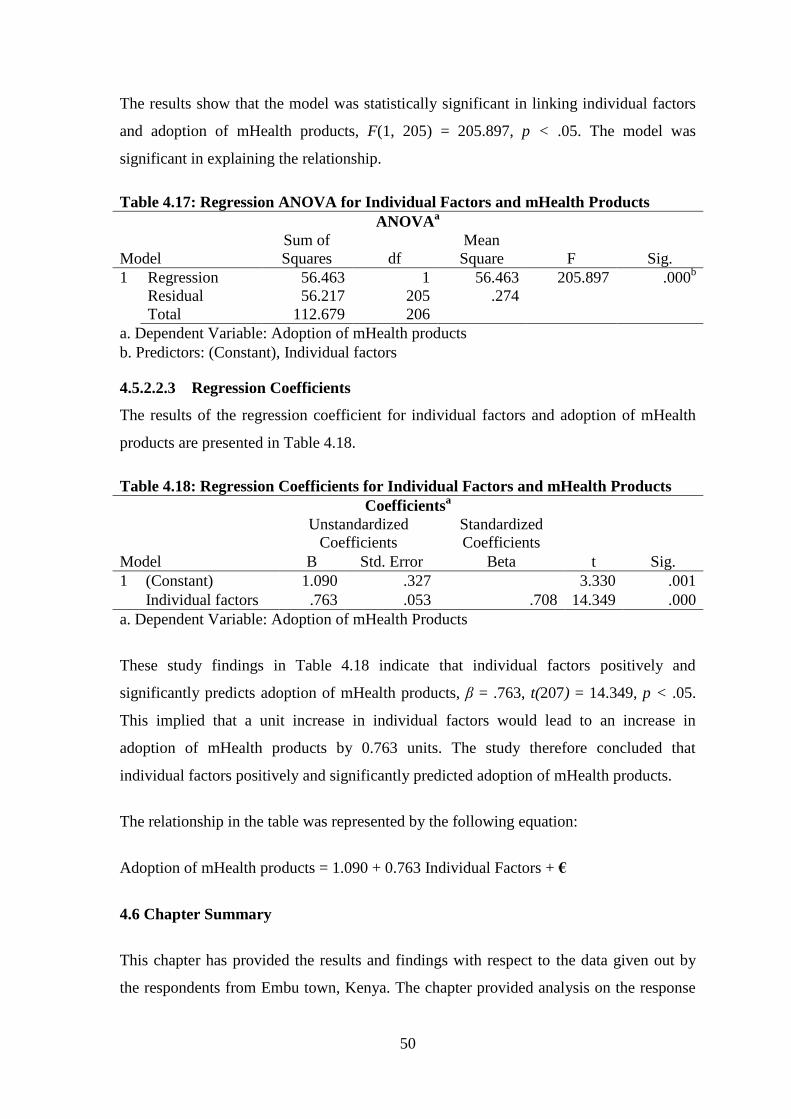
50
The results show that the model was statistically significant in linking individual factors
and adoption of mHealth products, F(1, 205) = 205.897, p < .05. The model was
significant in explaining the relationship.
Table 4.17: Regression ANOVA for Individual Factors and mHealth Products
ANOVAa
Model
Sum of
Squares df
Mean
Square F Sig.
1 Regression 56.463 1 56.463 205.897 .000b
Residual 56.217 205 .274
Total 112.679 206
a. Dependent Variable: Adoption of mHealth products
b. Predictors: (Constant), Individual factors
4.5.2.2.3 Regression Coefficients
The results of the regression coefficient for individual factors and adoption of mHealth
products are presented in Table 4.18.
Table 4.18: Regression Coefficients for Individual Factors and mHealth Products
Coefficientsa
Model
Unstandardized
Coefficients
Standardized
Coefficients
t Sig. B Std. Error Beta
1 (Constant) 1.090 .327 3.330 .001
Individual factors .763 .053 .708 14.349 .000
a. Dependent Variable: Adoption of mHealth Products
These study findings in Table 4.18 indicate that individual factors positively and
significantly predicts adoption of mHealth products, β = .763, t(207) = 14.349, p < .05.
This implied that a unit increase in individual factors would lead to an increase in
adoption of mHealth products by 0.763 units. The study therefore concluded that
individual factors positively and significantly predicted adoption of mHealth products.
The relationship in the table was represented by the following equation:
Adoption of mHealth products = 1.090 + 0.763 Individual Factors + €
4.6 Chapter Summary
This chapter has provided the results and findings with respect to the data given out by
the respondents from Embu town, Kenya. The chapter provided analysis on the response
51
rate, background information, social factors, technical factors and individual factors
affecting adoption of mHealth products. The next chapter provides the summary,
discussions, conclusions and recommendations.
52
CHAPTER FIVE
5.0 DISCUSSION, CONCLUSIONS AND RECOMMENDATIONS
5.1 Introduction
This chapter presents the discussion, conclusions and recommendations of the study. In
the first part, the summary of the study is presented. The discussion and conclusion of the
study is in part two and three respectively. Part four demonstrates the recommendations.
5.2 Summary
The objective of the study was to determine the factors affecting the adoption mHealth
products amongst patients in Kenya, a case of Embu. This study aimed at determining the
social factors affecting adoption of mHealth products, examining the technical factors
affecting adoption of mHealth products and determining the individual factors affecting
adoption of mHealth products.
The study adopted a descriptive and correlational research method in gathering,
analyzing, interpretation, and presentation of information. The research design helped in
focusing at the strength and direction of relationship between factors influencing the
adoption of mHealth products. The study employed the use of questionnaires to obtain
relevant information from respondents. The study focused on 144,347 adults living in
Embu town. Random sampling technique was used to determine a sample size of 277
respondents of which 207 respondents completed and returned back their questionnaires.
The study adopted a descriptive and inferential statistics in data analysis and presentation.
Correlation analysis and regression analysis was used in the study to determine the effect
of factors on adoption of mHealth products. Data was presented in tables and figures.
The study determined the effect of social factors on the adoption of mHealth products.
The study found that people who influence other people‟s behaviours think that they
should use mobile phone for healthcare. People who are important to others think that
they should use mobile phone for healthcare. The study reveals that people who are
familiar to others think that they should use mobile phone for healthcare. The findings of
the study showed that social factors positively and significantly correlated (r(207) = .793,
p < .05) to adoption of mHealth products. The study findings indicated that social factors
positively and significantly predicts adoption of mHealth products, β = .616, t(207) =

53
18.640, p < .05. The study revealed that social factors are critical factors in enhancing or
rather influencing effective adoption of mHealth products.
The study revealed how technical factors influence the adoption of mHealth products.
The study found that majority of the population own or has access to smartphones hence
they have access to good mobile phone network service at home and at their work places.
People have good and high speed internet available at their homesteads and at their work
places. The study found that most people frequently use internet based applications like
whatsapp and email for communication. The study revealed that people frequently use
social media like facebook, instagram and twitter in their daily endeavours. The findings
of the study showed that technical factors positively and significantly correlated (r(207) =
.931, p < .05) to adoption of mHealth products. The study findings indicated that
technical factors positively and significantly predicts adoption of mHealth products, β =
.730, t(207) = 36.459, p < .05.
The study examined the influence of individual factors on adoption of mHeath products.
The study reveals that individuals perceive that it is very useful to seek healthcare
services using mobile phone. They felt that use of mobile phones enhances
communication and helps in improving efficiency thus improving their performance. The
study found individuals perceive that seeking healthcare using mobile phone would save
time hence majority of people seek healthcare using their mobile regardless of their
location if such an option was available. The findings of the study showed that individual
factors positively and significantly correlated (r(207) = .708, p < .05) to adoption of
mHealth products. The findings indicated that individual factors positively and
significantly predicts adoption of mHealth products, β = .763, t(207) = 14.349, p < .05.
The study depicts that communication plays a critical role in seeking healthcare services
hence in enhancing access to healthcare services; open communication environment
should be encouraged.
5.3 Discussion
5.3.1 Social Factors and Adoption of mHealth Products
The study analyzed the influence of social factors on adoption of mHealth products. The
study found that people who are important to others feel that they should use mobile
phone for healthcare services. The study findings concur the findings of Krauskopf and

54
Wyatt (2012) that many people use smartphones when seeking for health services, in
taking notes and memos, for drug references, for accessing clinical decision support tool,
in viewing medical images among other things. The study confirmed that mHealth
services is very important in the developed world as it is used enhancing health
awareness, education, diagnosis of diseases and other support services like surveillance.
Slobin (1996) on the other hand found that the adoption of mHealth products experienced
several challenges because of it being a new and emerging phenomenon at the time.
There was low confidence by users of these systems due to security fears such as the
disclosure of their private information to a third party. They also found that language
programmed in the mHealth may be a challenge as not all patients understand different
languages hence communication should be made easy by a translator system in the
application.
The study found that social factors are critical to consider as they have a great effect on
the adoption of technology within the health sector by the greater population. The study
findings confirm the findings of Alsaleh and Alshamari (2016) that social factors have a
higher influence on technology adoption especially in the early stages of a new
technology as majority of users have little experience and knowledge of the technologies
and its benefits. Collis and Montgomery (2004) also found that in developed countries
such as the US, Europe, and Canada, mHealth has been fully enhanced and doctors can
perform various tests on a patient and email the results to the patients directly. Contrary,
Mwobobian (2012) revealed that Kenya still faces numerous challenges such as the low
uptake of technology particularly in the rural areas due to poor technology, high poverty
levels and poor health policies. Lorenz, Graf-Vlachy and Buhtz (2017) in their study
found that social factors influence innovation and technology adoption through the factors
such as compliance, subjective norms, group norms, social network configuration and
identification.
The study showed that people who influence other people‟s behaviour feel that they
should use mobile phones for healthcare services. The findings of the study are reflected
in the findings of Singletary et. al. (2002) who conducted a study about social influences
on technology acceptance and found that there was a strong positive significant
relationship that existed between image, social norms, innovative usage behaviour, and
innovative usage. Su-pi et. al. (2013) on the other hand found that social factors
55
specifically social trust related to use positively predicted actual usage of the system.
Social influences have been shown to effects on subjective norms like the acceptance of
new technology.
The study realized the fact that subjective norm is significantly related to perceived
usefulness and perceived ease of use. In addition, Schepers et al.(2008) found that
perceived ease of use is significantly related to the intention of use. The study supports
the findings of Guo et al. (2015) who investigated determinants of acceptance when it
comes to healthcare users. The findings revealed that when it comes to integration of
variables, they realized that perceived ease of use, subjective norm, perceived usefulness,
and trust have a positive significant effect on expert's purpose to use a contrary occasion
reporting system. Trust and perceived usefulness has a direct impact on the perceived
ease of use and subjective norm.
From the study it is found that most people have adopted the use of smartphones and are
becoming increasingly adept in their usage. Rogers (2003) found in their study that in the
current technological environment, most manual systems have rapidly been converted
into automated systems that are quickly turning institutions into paperless workspaces
where the flow of documents is through removable media, emails, optical discs and
computer networks. Chinweike and Ona (2014) found that nowadays products and
services, events and other notices can be placed in an online platform and the users
allowed accessing the information through creation of user accounts and subscriptions.
The study also reveals that people who are familiar to others think that they should use
mobile phone for healthcare services. The study found that diffusion of innovation is
largely influenced by the social context of the population observed. Chinweike and Ona
(2014) argue that power distance reduces the rates of technology adoption and innovation.
Ketter and Arfsten (2015) found that collectivists are more likely to conform to the wants
and needs of a group rather than their own individual choices and preferences. The lack of
individualism is seen to curtail innovation. High masculinity is seen to positively
influence innovation and technology adoption. This is due to the fact that societies high in
masculinity value individualism and incentivize individual performance.
The study findings show that there is a close relationship between social cultural norms
and the diffusion of technology and innovation. William and Dennis (2011) found that it
56
is necessary to achieve societal level changes in order to have sustainable technological
and innovation adoption. Muchiri (2015) found that people exhibit positive attitudes to
already proven beneficial technologies and innovations. Companies and competitors tend
to adopt new innovations seen to give their competitors a competitive advantage. Ketter
and Arfsten (2015) found in their study that the main group that influences an individual‟s
decisions is their family, friends and colleagues.
The study by Slovensky and Malvey (2017) found that some people find it difficult to
interact with the different mHealth products and develop a negative attitude towards the
devices. Contrary, Featherman and Hajli (2015) found in their study that people find the
mHealth products useful in the management of their health, others would still prefer the
traditional face-to-face interactions where they can explain their health issues in details.
Also, the feeling among the healthcare providers that the products are not effective in
capturing critical data from the patients have made it difficult for the healthcare systems
to adopt the technologies.
5.3.2 Technical Factors and Adoption of mHealth Products
The study found that most of people own or have access to smartphones hence they can
easily adopt and use mHealth products to access and utilize health services. The study
concurs with the findings of Mwobobia(2012) who found that globally cell phones have
become a necessity and almost everyone owns a cell phone. The cell phones have made
communication very easy and they keep families in-touch irrespective of the distance. It
also helps in accessing business emails, group communications and sharing of files as
well. Aker and Mbiti (2010) found that in developing countries such as Sub-Saharan
Africa, mobile technologies have evolved into a service delivery tool. The abrupt
advancement cell phone use or smartphone technology is having in the 21st century, is so
impactful that any business or service offered through the use of cell phones covers a
bigger area than anything seen in the past.
From the study, it is found that people have access to good mobile phone network
services at their homesteads. The findings concur with the assertions of Lekhanya
(2013)who found that has been a rapid increase in mobile phone penetration, connectivity
and coverage in the past few decades in Kenya and other countries. Oteri(2015) gives
weight to the findings of Lekhanya (2013) by revealing that Kenya has also seen a rapid
57
increase in network coverage, mostly fuelled by competition within the telecoms industry.
Lorenz (2017) found that technology such as 3G and 4G has enabled mobile access to
internet through mobile telephone service providers. Mobile internet coverage and
utilization has rapidly been on the rise in Kenya and other parts of Africa thus providing
internet access to people who previously lacked it. The study also agrees that proper use
of social media positively influenced diffusion and adoption of new technologies by
individual living in rural areas in South Africa.
The study reveals that technological advancement varies from one region to another.
Most urban areas have witnessed major milestones in technological advancement while in
the rural areas; technology penetration is still at the lower levels. Aker and Mbiti (2010)
found that at times, it is easy to introduce a technology product, however, it might
become more difficult to gain acceptance not only from the healthcare professionals but
also the patients and other users. Lorenz (2017) adds that in most instances, health care
practitioners often believe that technology is meant to take over the roles they play;
however, some technologies help in simplifying work and making it easier for them to
discharge their duties effectively. Alsaleh and Alshamari (2016) established that the most
appropriate way to ensure that change is effected in health behaviour is by understanding
the motivation behind the change itself. It is, therefore, the role of policymakers to ensure
that everyone understands the motivation behind any mHealth product for effective
transition and acceptance of the said change evenly across different regions within the
same country. Our study revealed a high level of acceptance of mHealth products despite
the region being classified traditionally as a rural area, where lower penetration of
technology would be expected.
From the study, it is confirmed that most people have high speed internet available at
their homes and work places. The study agrees with the findings of Oteri (2015) who
found that although large part of the country still remains un-served with internet, some
parts especially the urban areas have high speed internet as a result of wireless local area
networks or fibre optics. Tan and Teo (2000) found that technologies with a high
compatibility are more likely to be adopted than those which lack it. Contrary, Alsaleh
and Alshamari (2016) found that medical equipment usually have a high purchase cost,
and older machinery may not be compatible with new innovations such as mobile
58
connectivity. The cost of upgrading machinery may introduce an additional variable in
adoption of technologies in healthcare.
The study found that most people frequently use internet based applications like whatsapp
and email for communication. Lekhanya (2013) found that social networking
technologies are applications that enable people to connect based on their social bonds
and ties. These include social networking websites such as Facebook and Instagram that
have enabled this to occur through the internet. The study confirms that the use of social
networking platforms have been on the rise throughout the world, African countries
included. Majority of these users in Africa, access the internet using mobile devices such
as smartphones only.
The study found that patients' privacy and security of their data are of high importance,
especially when using mHealth products. Alsaleh and Alshamari (2016) in their study
found that access to patients' data by third parties as even led to numerous lawsuits as the
victims launch court cases with healthcare centres. In such instances, it becomes
extremely expensive for healthcare providers to prove that they can provide maximum
data security through mHealth products.
5.3.3 Individual Factors and Adoption of mHealth Products
The study confirms that individuals believe that seeking healthcare using mobile phone
would improve their performance. The study agrees with the findings of Mwobobia
(2012) who affirms that people have varied views about different technologies depending
on their perceptions and attitude. The adoption of mHealth products by an individual
depends on the ability of such products to meet their needs and expectations. Any
shortcoming with the products could result in an unwillingness to adopt the technologies.
The study finds that exposure to different mHealth products plays a critical role in making
it easy to penetrate the market with new products. McNair et. al. (2018) revealed that
advanced countries take new products as new developments meant to improve their
healthcare experience. They argued that people with little experience in new technology
would otherwise have a negative view of the new developments, and are likely to resist
such developments. On the other hand, Surendran (2013) in his study asserted that for
better penetration of mHealth products in developing countries, there is a need for more
awareness on their importance to drive out the fears among people who believe that
59
technology in the health sector has a higher risk of exposing them to harm such as private
data leakage, as compared to its perceived benefits.
The study found that people seeking healthcare services perceived that using mobile
phone is useful as it enhances the efficiency of the service. The study supports the
findings of Akter et al.(2019) who found that the perceived benefit of use of technology is
a major individual influencer for adoption of technology. They revealed that people are
assumed to adopt technology if it is believed to offer or contribute additionally benefit to
the current or existing system of doing things. Morawczynski and Pickens(2009) in their
study reveal that due to advanced technology, the difficulty of using cell phones has
drastically dropped, call quality has increased over time due to improved satellite and
wireless use. Other services like messaging (SMS), voice communication and wireless
communication services have as well improved with advancement in technology.
From the study, it was confirmed that mobile phones can be used anywhere hence it is a
very convenient platform for seeking healthcare services. The study support the findings
of McNair et. al. (2018) who affirm that the health sector has continued to experience
massive changes in operations as a result of technological advancement. The integration
of technology into the different sections of health care systems in Kenya has made service
delivery not only accessible but also affordable. The roll-out of Mobile Health products
has been received overwhelmingly well by most of the health care practitioners as it has
made their work easier. The study by Reem(2017) found that the perceived ease of use of
mHealth has been shown to be directly and positively correlated to adoption on new
technology and information systems. The study show that mHealth can reduce the effort
needed in several aspects of healthcare such as health record because these can be stored
in the cloud servers for easy access on phones for example in accessing all patients‟
history electronically.
The study revealed that individuals believe that using mobile phone in seeking healthcare
services save on time. McGaughey et al.(2014) found that it is important to note that
technology is changing so fast such that organizations are sometimes unable to adopt the
new technology in time and are forced to use traditional methods of production and
delivery. Electronic records management is one of the recent and fast-growing
applications of e-commerce having been embraced with organizations, governments and
personal investors who are seeking great business transactions and, or activities. Its

60
utilization in various organizations has been enabled by its fast evolution, value saving
ability, ease of information entry and high potency. Most developing and developed
countries, for example, are in the run to implementing electronic records management
technologies to enhance efficiency, and transparency while at the same time minimize
losses in their operations
The study found that that with a pre-existing negative attitude towards technology, it
becomes difficult to embrace mHealth products. Nath and Angeles (2007) found in their
study thatwithin the healthcare system, there are some caregivers who are not aggressive
when it comes to technology and thus, they find it difficult to deliver quality services in
instances where complex technology products are involved. Lorenz (2017) on the other
hand found that Behaviour has a lot of doing with personal feelings towards mHealth
products. It can be influenced by the level of education as those individuals who are not
good in technology would readily develop a negative attitude towards technology
products. It is therefore important to ensure that individuals are adequately trained and
have the capacity to use technology products before they are rolled out. However,
mHealth technologies are simple to use and rely on existing knowledge, capabilities and
infrastructure, thus, increasing their likelihood of acceptance and adoption.
The study findings show that adoption of technology can be measured by determining
either the intention to use of the technology or the actual usage of the technology.
Venkatesh et. al. (2003) found that health practitioners who believe technology might
replace them at work are more likely to develop a negative attitude towards mHealth
products. Lorenz(2017) on the other side found that when staff members are provided
with adequate support and training on how to use mHealth technologies, they develop the
right attitude and become part of the implementation process. They go a long way in
helping patients with difficulties to understand mHealth products and appreciate the
products. Health practitioners are the main agents of positive change and the adoption of
mHealth products as they interact with patients most of their time. With the right attitude,
it becomes easy to adopt various mHealth products and implement them to make service
delivery in health care more efficient.
61
5.4 Conclusions
5.4.1 Social Factors and Adoption of mHealth Products
The first specific objective was to determine the influence of social factors on adoption of
mHealth products. Social factors were found to be the 2nd
most influential factor in
determining adoption of mHealth products in Kenya. The study found a positive
relationship between social factors and the adoption of mHealth factors.
The relationship is such that the more an individual believes that the society accepts a
particular technology, they more they are willing to adopt it. The same applies to
companies, the more a company believe that other companies are willing to adopt a
technology or have experienced competitive advantage through technology adoption, they
more likely they are to adopt the technology. However, this is seen to have a negative
effect in times that the society has a negative attitude towards a positive technology. With
such a strong relationship, it is important for companies to carefully study the attitudes of
the society to their technology prior to rollout.
5.4.2 Technological Factors and Adoption of mHealth Products
The second specific objective was to determine the influence of technical factors on
adoption of mHealth products. Technological factors were found to be the most
influential factor in determining adoption of mHealth products in Kenya. The study
showed a strong and positive relationship between technical factors and the adoption of
mHealth technologies. This was in line to the finding in pervious literature on the
influence of technical factors on the adoption of mHealth products.
It is seen that technical factors such as access to internet, smartphones, good mobile
network coverage and high utilization of social media, positively facilities the adoption of
technology. The study found a high penetration of smartphone and social media
utilization amongst the population studied. This shows the current existence of an
enabling environment for growth of a mHealth product.
Our study showed high levels of social media usage amongst the sample population. This
is indicative of the possibly high potential of for adoption of mHealth technologies.
Possibly a lack of awareness of existing solutions, or a lack of appropriate solutions could
be the major reason as to why mHealth product adoption is currently at low levels in the
country.
62
5.4.3 Individual Factors and Adoption of mHealth Products
The third specific objective was to determine the influence of individual factors on
adoption of mHealth products. The study illustrated a positive relationship between
individual factors and the adoption of mHealth products in Kenya. This was based on the
respondents having a high perception of usefulness of mHealth technologies in
conveniently seeking healthcare.
It is notable that human centred design is a fairly new concept in product design. Focus
on solution driven product design may however have led to products that have a poor fit
with the current needs of the users. In which case, it is imperative for mHealth product
designers to take a step back and re-examine if their products address the needs of
patients. Not only that, but do they also have a user interface that are easy to understand
and use.
An approach that maximizes on creating convenience, while maintaining the ethics,
professionalism and reliability associated with a physical hospital visit may be needed to
create the highest perception of user benefit. Therefore, a multifactor approach as to how
might we recreate a better hospital experiencing using mobile devices is needed to
successful increase adoption on mHealth products in Kenya.
The study findings highlight the fact that mHealth products need to create value for their
intended users. This value must be easy to understand from a user perspective. As long as
there is significant positive value created, adoption of mHealth technologies is likely to
increase. Other factors such as perceived ease of use of these technologies are also a
significant influencer. However, this was not studied in the scope of this research paper.
5.5 Recommendations
5.5.1 Recommendation for Improvement
5.5.1.1 Social Factors and Adoption of mHealth Products
Social factors are a major influencer for adoption of technologies. Organizations need to
understand and ensure a positive attitude exist towards the technological solution they
aim to present. If the technology is resisted by the healthcare providers, this may lead to
failure in its adoption. With the diffusion of innovation model in mind, a critical mass of
individuals like innovators and early adopters must begin to use a product before its
63
eventual spread to the rest of the population. There is likelihood, that current mHealth
products have not created the level of awareness needed to reach a critical mass. The
products certainly lack adequate number of users to cause a massive spread/ adoption of
the solutions. The high cost of creating widespread social awareness might be a limiting
factor in this case.
Organizations must actively plan how to break social barriers when introducing mHealth
products. They must carefully select influencing individuals in the society to launch and
spread their products.
5.5.1.2 Technological Factors and Adoption of mHealth Products
It is seen that technical factors are an enabler of technology adoption. Kenya is very well
placed with high smartphone penetration, good network coverage and access to internet.
Users have a high utilization of social media on already existing devices. Therefore,
Kenya is well placed to take up mHealth products. Organizations need to focus on
technologies and products that can work well within the existing infrastructure.
Compatibility has been seen as an existing challenge in healthcare due to the wide variety
of companies, high cost of equipment/ devices and high obsolete rates devices in
healthcare. Solutions that provide wide compatibility are more likely to have a high
adoption rate.
5.5.1.3 Individual Factors and Adoption of mHealth Products
Perceived benefit of use is seen a critical element in adoption of mHealth products. There
is need to create products that easily deliver value to users. A human centred design
approach is needed in development of mHealth products. High empathy and focus on
solution for actual user problems is needed.
Other individual factors such as perceived ease of use work in complement with
perceived benefit of use. mHealth products that will see the highest levels of user
adoption will have delivered products that are easy to use and deliver a very clear solution
to existing users problems.

64
5.5.2 Recommendation for Further Research
The study only focused on individuals living in Embu Town. Further studies on a wider
scope of individuals are needed with a good sample of both rural and urban individuals. A
case study on the factors influencing adoption of mHealth products amongst healthcare
practitioners might give insights useful to the implementation of a new product. In
addition, a deeper understanding of which social factors have the most influence within
healthcare may provide better insight on how to successfully launch a product to reach
critical mass adoption in Kenya.
65
REFERENCES
Ainlay, S. C., Becker, G. & Coleman, L. (1986). The dilemma of difference: a
multidisciplinary view of stigma. New York, NY: Plenum Press.
Ajzen, I. & Fishbein, M. (1980). Understanding attitudes and predicting social behavior.
New Jersey, NJ: Prentice-Hall.
Ajzen, I. (1991). The Theory of Planned Behavior. Organizational Behavior and Human
Decision, 10(2), 179-211.
Aker, J. C. & Mbiti, I. M. (2010). Mobile phones and Economic Development in Africa.
Journal of Economic Perspectives, 12(4), 5-10.
Akter et al. (2019). Determinants of user acceptance of Internet banking: an empirical
study. International Journal of Service Industry Management, 5, 501-519.
Alsaleh, S. & Alshamari, F. (2016). Exploring Factors Affecting Patients Adoption of
mHealth Services in the Kingdom of Saudi Arabia. International Journal of
Health.Wellness & Society, 6(4), 174-185.
Alushula, P. (2019, January 29). M-Pesa users outside Kenya hit 13.4 million. Retrieved
September 05, 2019, from Business Daily Africa:
https://www.businessdailyafrica.com/corporate/companies/M-Pesa-users-outside-
Kenya-hit-13-4-million/4003102-4956208-16s8a9/index.html
Athanasia, P., Xenia, Z. & Konstantina, V. (2003). A Societral perspective on e‐business
adoption. Journal of Information, Communication and Ethics in Society, 8(2),
149-166.
Avers, D. & Brown, M. (2009). White paper: Strength training for the older adult.
Journal of Geriatric Physiotherapy, 32(4), 148–152.
Bangladesh Telecom Regulatory Commission (BTRC). (2015). Country Experience on
Satellite Service Regulatory Framework. Danang City, BD: Bangladesh Telecom
Regulatory Commission.
Chinweike, E. & Ona, E. (2014). Socio-Cultural Influences on Technology Adoption and
Sustainable Development. Industrial and Systems Engineering Research
Conference.2, 253-261.
Communications Authority of Kenya (CCK). (2014). Quartely Sector Statistical Report.
Nairobi, KE: Communications Authority of Kenya.
Cooper, D. R. & Schindler, P. S. (2014). Business Research Methods 12th Edition. New
York, NY: McGraw Hill.
Cooper, R. A. (1990). Information technology implementation research:a technological
diffusion approach. Management Science, 6(2), 123-39.
Cory, M., Christopher, B., Oscar, O., Monica, P. & Shellen, S. (2018). US Digital Users:
eMarketer's Estimates for 2018. New York, NY: eMarketer.
66
Davenport, T., Harris, J. G. & Kohli, A. K. (2001). How do they know their customers so
well? MIT Sloan management Review., 42(2), 63.
Davis, F. D. (1989). Perceived Usefulness, Perceived Ease of Use, and User Acceptance
of Information. MIS Quarterly, 11, 319 - 339.
Doherty, N.E.C. (2003). An analysis of the factors affecting the adoption of the Internet
in the UK retail sector. Journal of Business Research, 6, 887-97.
Embu County Government. (2018). Finance and Economic Planning Annual Progress
Report 2017/2018. Embu: Embu County Government.
Featherman, M. & Hajli, N. (2015). Self-Service Technologies and e-Services Risks in
Social Commerce Era. Journal Of Business Ethics, 8(4), 251-269.
Fishbein, M. A. (1975). Belief, Attitude, Intention and Behavior: An Introduction to
Theory and Research. Reading, BRK: Addison-Wesley.
George, D. & Mallery, P. (2003). SPSS for Windows step by step: A simple guide and
reference. Boston, MA: Allyn & Bacon.
Gerstner, L. (2002). Who says Elephants Can't Dance? Inside IBM's Historic
Turnaround. New York, NY: Harper Collins.
Government of Kenya (GOK). (2010). Consitution of Kenya. Nairobi, KE: Government
printer,Kenya.
Government of Kenya (GOK). (2014). Kenya Demographic and Health Survey. Nairobi,
KE: Kenya Bureau of Statistics.
Groupe Spécial Mobile Association (GSMA). (2014). Digital inclusion. GSMA
Intelligence.
Groupe Spécial Mobile Association (GSMA). (2017). Scaling digital health in developing
markets: Opportunities and recommendations for mobile operator and other
stakeholders. GSMA Intelligence.
GSMA. (2012). Touching lives through mobile health :Assessment of the global market
opportunity. Ahmedabad: PwCPL & GSMA.
Guo, X., Han, X., Zhang, X., Dang, Y. & Chen, C. (2015). Investigating m-Health
Acceptance from a Protection Motivation Theory Perspective: Gender and Age
Differences. Telemed Journal of Educational Health., 196(8), 661-9.
Gupta, A. & Dasgupta, S. (2008). Adoption of ICT in a goverment organization in a
developing country: An empirical study. The Journal of strategic Information
System, 17(2), 140-154.
Haderi, S. M. & Aziz, A. B. (2015). The Effect of Social Characteristic in the Acceptance
and Continue Usage for Information Technology in the Public Sector.
International Journal of Business and Social Science, 14(8), 186-192.
67
Hartwick, J. & Barki, H. (1994). Explaining the role of user participation in information
system use. Journal of Management Science, 40(4), 440-465.
Hofstede, G. (2001). Culture's Consequences: Comparing Values, Behaviors, Institutions
and Organizations Across Nations. SAGE Publications.
Infodev. (2012). Mobile Usage at the Base of the Pyramid in Kenya,. Nairobi, KE:
Infodev.
Jumia Kenya. (2015). White Paper: The Growth of the smartphone market in Kenya.
Nairobi, KE: Sofia Lab.
Kariuki, E. (2016). Adoption of m-health and usability challenges in m-health
applications in Kenya: case of uzazi poa m-health prototype application. Nairobi,
KE: UNITED STATES INTERNATIONAL UNIVERSITY - AFRICA.
Karongo, C. (2011, November 24). Capital News:'Now you can ‘dial a doctor’. Retrieved
April 26, 2019, from Capitalfm: https://www.capitalfm.co.ke/news/2011/11/now-
you-can-dial-a-doctor/
Kenya Ministry of Medical Services. (2011). Kenya e-Health Strategy 2011-2017.
Nairobi, KE: Government of Kenya.
Kenya National Bureau of Statistics (KNBS). (2009). National Population and Housing
Census. Nairobi, KE: Kenya National Bureau of Statistics.
Kenya National Bureau of Statistics (KNBS). (2013). Exploring Kenya's Inequality.
Nairobi, KE: Kenya National Bureau of Statistics.
Ketter, C. K. & Arfsten, M. C. (2015). Cultural Value Dimensions and Ethnicity within
Kenya. International Business Research, 8(12), 69-79.
Krauskopf, P. & Wyatt, T. (2012). E-health and nursing:using smartphones to enhance
nursing practice. Online Journal of Nursing Infomatics.(QJNI)., 16(2).1706.
Lekhanya, L. M. (2013). Cultural Influence On The Diffusion And Adoption Of Social
Media Technologies By Entrepreneurs In Rural South Africa. International
Business & Economics Research Journal, 15, 63-74.
Lorenz, Graf-Vlachy & Buhtz, K. (2017). Social Influence In Technology Adoption
Research: A Literature Review And Research Agenda. In Proceedings of the 25th
European Conference on Information Systems (pp. 2331-2351). Guimarães: AIS
Electronic Library (AISeL).
Luborsky, M. R. (1993). Sociocultural Factors Shaping Technology Usage: Fulfilling the
promise. Technology Disability, 2(1), 71–78.
Mbwesa, K. J. (2006). Introduction to management research; A student handbook.
Nairobi, KE: Jomo Kenyatta Foundation.
McGaughey, R., Gunasekaran, A. & Ngai, E. (2008). Information technology and systems
justification in Evaluating Information System. Routledge.
68
McKinsey and Company. (2013). iConsumers: Life online.. McKinsey and Company.
McNair, C., Bendtson, C., Orozoo, O., Peart, M. & Sham, S. (2018). US Digital Users:
eMarketer's Estimates for 2018. New York, NY: eMarketer.
Moore, G. C. (1996). Integrating Diffusion of Innovations and Theory of Reasoned Action
Models to Predict Utilization of Information Technology by End-Users. London,
UK: Chapman and Hall.
Morawczynski, O. & Pickens, M. (2009). Poor People Using Mobile Financial Services:
Observations on Customer Usage and Impact from M-PESA. Washington DC:
CGAP.
Morawczynski, O. (2008). Surviving in the ‘Dual System’: How M-PESA is Fostering
Urban to Rural Remittances in a Kenyan Slum; Working Paper. Edinburgh: Social
Studies Unit, University of Edinburgh:.
Muchiri, M. I. (2015). Factors Affecting The Adoption Of Technological Innovation In
Selected Organizations In Nairobi, Kenya. Nairobi, KE: United State International
University, Africa.
Mwambia, E. (2015). Factors Affecting Adoption Of Technological Innovation In Kenya:
A Case Of Kenya Revenue Authority Medium Taxpayers Office . Nairobi, KE:
United States International University- Africa.
Mwobobia, F. M. (2012). The challenges facing small-scale women enterprenuers:A case
of Kenya. International Journal of Business Administration, 3(2), 112.
Nath, R. & Angeles, R. (2007). Business to business e-procurement:Sucess factors and
challenges to implementation.Supply Chain Mangement. International Journal
Supply Chain Management, 12(2), 104-115.
Osterwalder, A. & Pigneur, Y. (2002). An eBusiness Model Ontology for Modeling
eBusiness,. In the Proceedings of the 15th Bled Electronic Commerce Conference
– eReality: Constructing the eEconomy (pp. 75-91). Bled: 15th Bled Electronic
Commerce Conference.
Oteri, M. P. (2015). Mobile Subscription, Penetration and Coverage Trends in Kenya‟s
Telecommunication Sector. International Journal of Advanced Research in
Artificial Intelligence, 6, 1-7.
Reem, K., Aliki, P., Muhammad, I., Zahra, H., Pedro, B. & B., J. (2017). Awareness and
Use of mHealth Apps: A Study from England. Pharmacy (Basel), 8(3), 33.
Rifkin, J. (2011). The Third Industrial Revolution, How Lateral Power is Transforming
Energy, the Economy, and the World. Palgrave Macmillan.
Rogers E.M., S. (1971). Communication in Innovation. New York, NY: Free Press.
Rogers, E. M. (1962). Diffusion of innovations. New York, NY: Free Press of Glencoe.
Rogers, E. M. (1995). Diffusion of Innovation. New York, NY: Free Press.
69
Rogers, E. M. (2003). Diffusion of Innovations (5th edition). New York, NY: Free Press.
Schepers, J., deJong, A., Wetzels, M. & deRuyter, K. (2008). A multi-level assessment in
education. Computers & Education, 51(2), 757-775.
Scott, W. R. (2004). Institutional Theory: Contributing to a Theoretical Research
Program, Great Minds in Management: The Process of Theory Development.
Oxford: Oxford University Press.
Singletary, L., Akbulut, A. & Houston, A. (2002). Innovative software use after
mandatory adoption. AMCIS 2002 proceedings (p. 156). Americas Conference on
Information Systems.
Slobin, D. I. (1996). Rethinking Linguistic Relativity. Dublin: Cambridge University
Press.
Slovensky, D. & Malvey, D. (2017). Introduction to Focused Issue on mHealth
Infrastructure: issues and solutions that challenge optimal deployment of mHealth
products and services. Mhealth, 3(1), 52-52.
SNS Telecom & IT. (2017). The mHealth (Mobile Healthcare) Ecosystem: 2017 - 2030 -
Opportunities, Challenges, Strategies & Forecasts. Dubai: SNS Telecome & IT .
Stroetmann, K. (2018). Digital Healthcare Ecosystem for African Countries: A guide for
public and private actors for establishing holistic Digital Health Ecosystems in
Africa. Berlin: Federal Ministry for Economic Development.
Su-pi, S., Chung-hung, T. & Wei-lin, H. (2013). Extending the TAM Model to Explore
the Factors Affecting Intention to Use Telecare Systems. Journal of Computers,
12, 525-532.
Surendran, P. (2013). Technology Acceptance Model: A Survey of Literature.
International Journal of Business and Social Research, 5(2), 175-178.
Tan, M. & Teo, T. S. (2000). Factors Influencing the Adoption of Internet Banking.
Journal of the Association for Information Systems. Journal of the Association for
Information Systems, 9, 1-44.
Taylor, S. A. (1995). Assessing IT usage: Taylor, S. and Todd, P.A. MIS quarterly, 11,
561‐570.
Teo, T. A. (1998). An empirical study of adopters and non-adopters of the Internet in
Singapore. Information & Management, 6, 339-45.
Tseng, A., Hsia, J. W. & Chang, C. C. (2014). Effects of individuals locus of control and
computer self-efficacy on their e-learning acceptance in high-tech companies.
Behaviour & Information Technology., 33(1), 51-64.
United Nations (UN). (2019, July 18). Envision2030: UN. Retrieved January 21, 2019,
from UN website:
https://www.un.org/development/desa/disabilities/envision2030.html
70
Vadapalli, A. A. (1997). Business use of the Internet: an analytical framework and
exploratory case study. International Journal of Electronic Commerce, 15(6), 57-
69.
Vassilopoulou, K. Z. (2003). Examining E-Business Models: Applying a Holistic
Approach in the Mobile Environment. New Paradigms in Organizations, Markets
and Society: Naples: Proceedings of the 11th European Conference on
Information Systems (ECIS).
Venkatesh, V. & David, F. (2000). A Theoretical Extension of the Technology
Acceptance Model:. Management Science, 9, 186‐204.
Venkatesh, V., Morris, M. G., Davis, G. B. & Davis, F. D. (2003). User acceptance of
information technology: Toward a unified view. MIS Quarterly, 14, 425-478.
Vital Wave Consulting. (2009). mHealth for development:the opportunity of mobile
technology for healthcare in the developing world. Washington DC: UN
Foundation.
Vogelsang, K., Steinhuser, M. & Hoppe, U. (2013). A qualitative approach to examine
technology acceptance. Thirty Fourth International Conference on Information
Systems. Milan: International Conference on Information Systems.
WHO, W. H. (2011). mHealth-New horizons for health through mobile technologies.
WHO.
William, J. & Dennis, J. (2011). Entrepreneurship, Small Business and Public Policy
Levers. Journal of Small Business Management, 49(2), 92-106.
World Health Organization (WHO). (2005). Resolution WHA58.33. Sustainable health
financing, universal coverage and social health. In: Fifty-eighth World Health
Assembly. Geneva: World Health Organization.
World Health Organization (WHO). (2011). Global HIV/AIDS response:epidemic update
and health sector progress towards universal access. WHO.
World Health Organization (WHO). (2011). mHealth new horizons for health through
mobile technologies. World Healh Organization.
World Health Organization (WHO). (2016). Global Diffusion of eHealth: Making
universal health coverage achievable. Geneva: World Health Organization.
World Health Organization (WHO). (2018). Public Spending on Health: A Closer Look at
Global Trends. Geneva: World Health Organization.
World Health Organization. (2019, July 17). ehealth: who. Retrieved January 18, 2019,
from www.who.int: https://www.who.int/ehealth/about/en/
Yalcinkaya, R. (2007). Police Officers’ Adoption Of Information Technology: A Case
Study Of The Turkish Polnet System. Huston: University Of North Texas.

71
Zola, I. (1982). Missing pieces: chronicle of living with a disability. Philadelphia: Temple
University Press.
APPENDICES
Appendix I: Letter of introduction
Appendix II: Research License
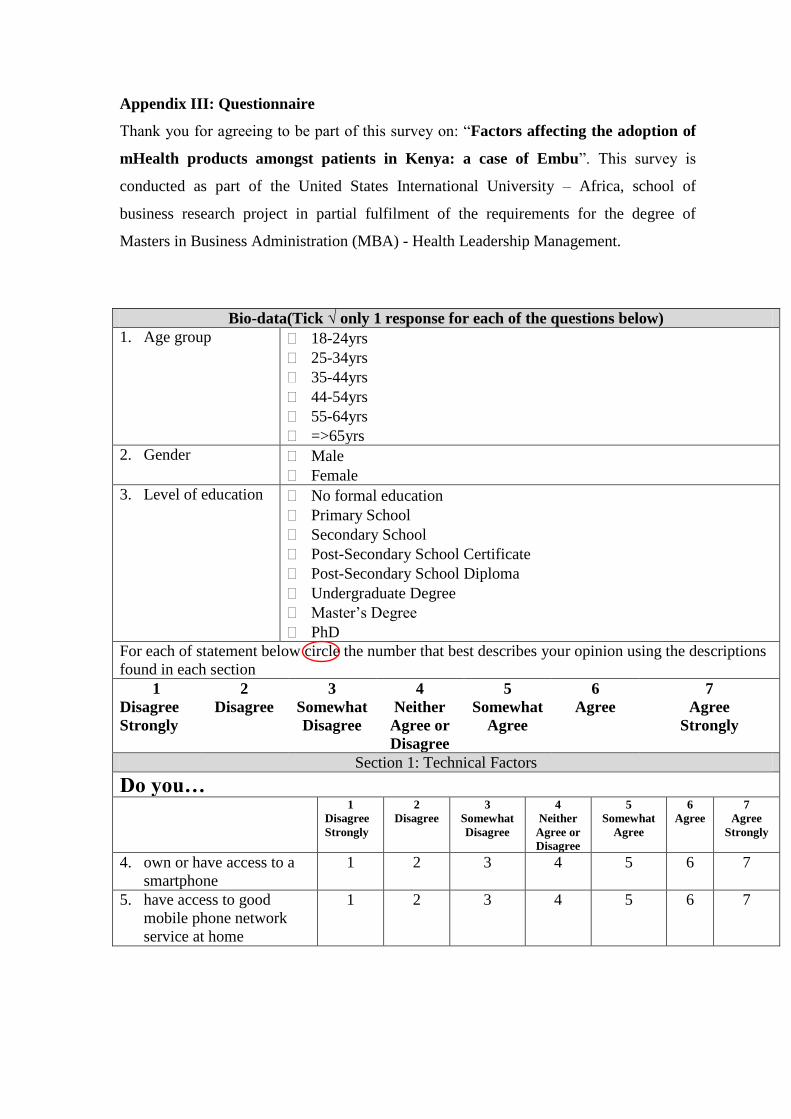
Appendix III: Questionnaire
Thank you for agreeing to be part of this survey on: “Factors affecting the adoption of
mHealth products amongst patients in Kenya: a case of Embu”. This survey is
conducted as part of the United States International University – Africa, school of
business research project in partial fulfilment of the requirements for the degree of
Masters in Business Administration (MBA) - Health Leadership Management.
Bio-data(Tick √ only 1 response for each of the questions below)
1. Age group 18-24yrs
25-34yrs
35-44yrs
44-54yrs
55-64yrs
=>65yrs
2. Gender Male
Female
3. Level of education No formal education
Primary School
Secondary School
Post-Secondary School Certificate
Post-Secondary School Diploma
Undergraduate Degree
Master‟s Degree
PhD
For each of statement below circle the number that best describes your opinion using the descriptions
found in each section
1
Disagree
Strongly
2
Disagree
3
Somewhat
Disagree
4
Neither
Agree or
Disagree
5
Somewhat
Agree
6
Agree
7
Agree
Strongly
Section 1: Technical Factors
Do you… 1
Disagree
Strongly
2
Disagree
3
Somewhat
Disagree
4
Neither
Agree or
Disagree
5
Somewhat
Agree
6
Agree
7
Agree
Strongly
4. own or have access to a
smartphone
1 2 3 4 5 6 7
5. have access to good
mobile phone network
service at home
1 2 3 4 5 6 7
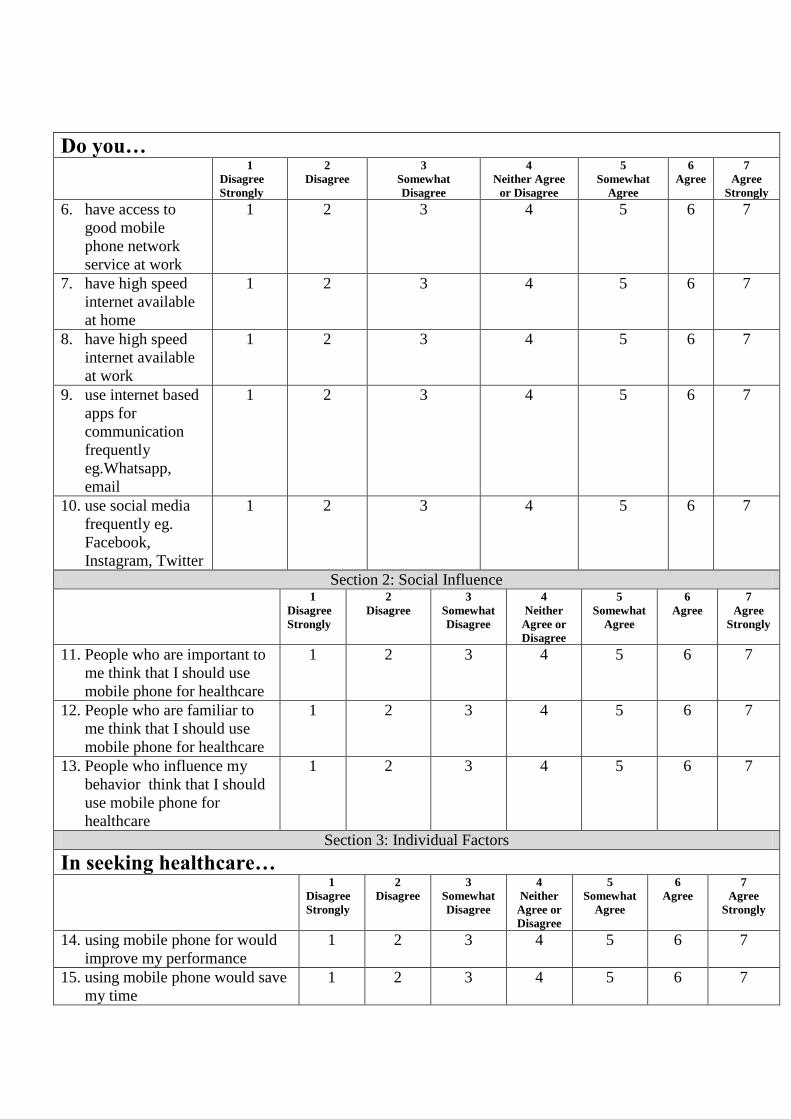
Do you…
1
Disagree
Strongly
2
Disagree
3
Somewhat
Disagree
4
Neither Agree
or Disagree
5
Somewhat
Agree
6
Agree
7
Agree
Strongly
6. have access to
good mobile
phone network
service at work
1 2 3 4 5 6 7
7. have high speed
internet available
at home
1 2 3 4 5 6 7
8. have high speed
internet available
at work
1 2 3 4 5 6 7
9. use internet based
apps for
communication
frequently
eg.Whatsapp,
1 2 3 4 5 6 7
10. use social media
frequently eg.
Facebook,
Instagram, Twitter
1 2 3 4 5 6 7
Section 2: Social Influence
1
Disagree
Strongly
2
Disagree
3
Somewhat
Disagree
4
Neither
Agree or
Disagree
5
Somewhat
Agree
6
Agree
7
Agree
Strongly
11. People who are important to
me think that I should use
mobile phone for healthcare
1 2 3 4 5 6 7
12. People who are familiar to
me think that I should use
mobile phone for healthcare
1 2 3 4 5 6 7
13. People who influence my
behavior think that I should
use mobile phone for
healthcare
1 2 3 4 5 6 7
Section 3: Individual Factors
In seeking healthcare… 1
Disagree
Strongly
2
Disagree
3
Somewhat
Disagree
4
Neither
Agree or
Disagree
5
Somewhat
Agree
6
Agree
7
Agree
Strongly
14. using mobile phone for would
improve my performance
1 2 3 4 5 6 7
15. using mobile phone would save
my time
1 2 3 4 5 6 7
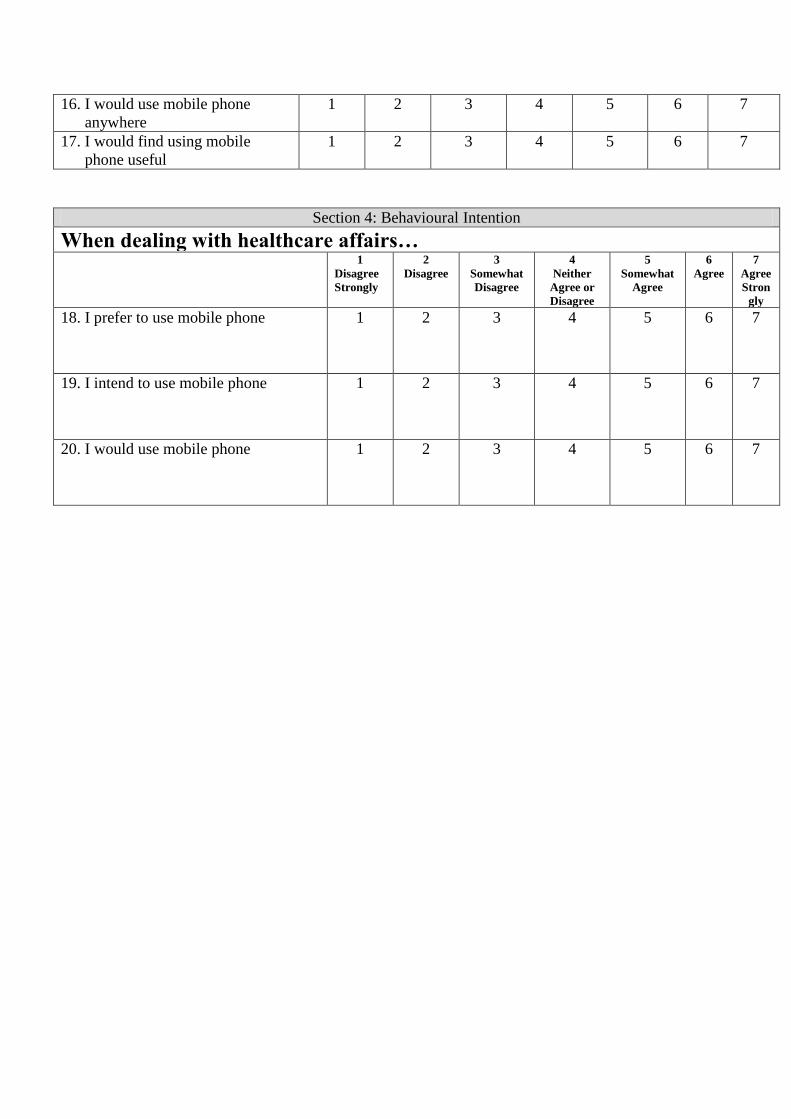
16. I would use mobile phone
anywhere
1 2 3 4 5 6 7
17. I would find using mobile
phone useful
1 2 3 4 5 6 7
Section 4: Behavioural Intention
When dealing with healthcare affairs… 1
Disagree
Strongly
2
Disagree
3
Somewhat
Disagree
4
Neither
Agree or
Disagree
5
Somewhat
Agree
6
Agree
7
Agree
Stron
gly
18. I prefer to use mobile phone 1 2 3 4 5 6 7
19. I intend to use mobile phone 1 2 3 4 5 6 7
20. I would use mobile phone 1 2 3 4 5 6 7





























