Embed Size (px)
DESCRIPTION
Â
Citation preview

Factors Influencing the Gastric Residence ofDosage Forms in Dogs
MARILYN N. MARTINEZ,1* MARK G. PAPICH2
1US Food and Drug Administration, Center for Veterinary Medicine, Office of New Animal Drug Evaluation,7500 Standish Place, Rockville, Maryland 20855
2Department of Anatomy, College of Veterinary Medicine, North Carolina State University,Physiological Sciences & Radiology, 4700 Hillsborough Street, Raleigh, North Carolina 27606
Received 28 April 2008; revised 10 June 2008; accepted 11 June 2008
Published online 25 July 2008 in Wiley InterScience (www.interscience.wiley.com). DOI 10.1002/jps.21499
*The views eand do not reflsupport or endoinferred.
Corresponde2768357; Fax: 2E-mail: marilyn
Journal of Pharm
� 2008 Wiley-Liss
844 JOURNA
ABSTRACT: An appreciation of the variables influencing canine gastric transit time isof interest both because of the push to develop pharmaceutical products that meet thetherapeutic needs of the veterinary patient and because of efforts to improve ourunderstanding of the strengths and weaknesses associated with the use of the dog asa preclinical model to support human product development. The gastric transit time ofmonogastric species is influenced by many factors. Physiological variables includethe time of dosing relative to the phase of the interdigestive migrating myoelectriccurrent (IMMC), the sieving properties of the pylorus, the presence or absence of food,and the inherent crushing force of the stomach. Pharmacological factors include particlesize, shape and density, drug solubility, and the hardness of the tablet. Despite theimportance of understanding the factors influencing gastric residence time in dogs, anin-depth examination of currently available information on this topic has not as yet beenpublished. Therefore, this review provides an examination of each of these factors andtheir potential impact on canine oral drug absorption characteristics. � 2008 Wiley-Liss,
Inc. and the American Pharmacists Association J Pharm Sci 98:844–860, 2009
Keywords: preclinical pharmacology;
gastrointestinal transit; bioavailability; foodeffects; oral absorptionINTRODUCTION
A large component of the canine therapeuticarsenal consists of medications intended for oraladministration. Understanding the variables in-
xpressed in this article are those of the authorsect the official policy of the FDA. No officialrsement by the FDA is intended or should be
nce to: Marilyn N. Martinez (Telephone: 240-40-2758350;[email protected])
aceutical Sciences, Vol. 98, 844–860 (2009)
, Inc. and the American Pharmacists Association
L OF PHARMACEUTICAL SCIENCES, VOL. 98, NO. 3, MARC
fluencing the gastric transit of these productsis important for achieving the desired drugabsorption characteristics. The movement of drugproducts through the canine digestive system willalso influence decisions on re-dosing followingregurgitation, methods to minimize intra- andintersubject variability, and the in vitro dis-solution test conditions that are most likely tocorrelate with in vivo drug absorption.
While it may be enticing to define a specific ‘‘ruleof thumb’’ for describing the gastric transit timeof an orally administered product when dosedunder fed or fasted conditions,1 a ‘‘one size fitsall’’ approach is not appropriate because of the
H 2009

GASTRIC RESIDENCE OF DOSAGE FORMS IN DOGS 845
many variables that can influence this estimate.Moreover, applying human estimates to predictcanine stomach emptying time can be misleading.
A large number of variables can influencethe rate of gastric transit, leading to substantialinterstudy deviations in estimates of gastricresidence time. This latter point of concern wasexpressly examined by Wyse et al.,1 in their reporton gastric emptying times in dogs (listed as gastrichalf-emptying time). These authors noted thatestimates of gastric residence times have rangedfrom 66 min to 29 h, depending on the studydesign. This observation underscores the impor-tance of studying gastric transit under biologicallyrelevant conditions.
Fortunately, because of the many publishedstudies using dogs as a model for human oralbioavailability, the literature is rich in informa-tion pertaining to the physiological variablesinfluencing gastric transit time in dogs. However,despite this wealth of information, there remainsa need to link this previously generated informa-tion with the current trends in canine oral productdevelopment. Therefore, this manuscript providesa link between physiological and pharmacologicalfactors in a manner that will assist formulators ofveterinary products, veterinary practitioners, andinvestigators who use dogs as an animal modelfor the evaluation of novel oral delivery systemsintended for human use. Individuals interested inthe veterinary application of this information mayfind it particularly helpful to consider the contentsof this manuscript in conjunction with currentefforts supported by the US Pharmacopeia (USP)to examine physiological differences between dogsand humans that will influence the classificationof highly soluble and highly permeable drugs indogs.2
Anatomic and Physiological Considerations
The stomach acts as a repository for storing foodand fluid. According to a 1943 reference, thestomach capacity in dogs is 100–250 mL/kg, with arange of 0.5–8 L per dog.3 It is capable of rigorousmovements that grind, churn, and propel partiallydigested foods from the stomach through thepylorus. The pylorus serves as a molecular sieve,restricting the passage of materials on the basis ofparticle size, insuring that only digestible-sized
1Throughout this article, the term ‘‘fasted’’ implies the withholding of
food from experimental subjects. Technically, fasting is a voluntary
abstention from food and should not apply to dogs. However, the term
fasted is used here for convenience.
DOI 10.1002/jps JOU
materials enter the small intestine. Althoughsome weak acids, ions, and fluids may be absorbedacross the gastric mucosa, the majority of theabsorption occurs where the absorptive capacity ishighest—in the small intestine.
The stomach wall consists of the mucosal layer,the muscularis mucosa and the submucosal layer.The stomach anatomy of dogs (Fig. 1) is similar tothat of humans.4 From a histological perspective,the mucosal layer, the innermost (luminal) region,is richly populated by surface mucous-producingcolumnar epithelial cells that indent to form thegastric pits, and with the gastric glands thatcontain a variety of cell types. The density andcellular composition of these glands differ acrossthe various regions of the stomach.5
1. C
Fig
RNAL O
ardiac mucosa: The cardiac glands areshort relative to those found in the pyloricand fundic regions. The primary function ofthe cardiac glands is to protect the esopha-geal region from damage by gastric acidsand enzymes. Therefore, within the cardiacmucosa, these glands contain primarilymucous-producing cells and few parietal orchief cells that contain mucous secretingcells.
2. C
orpus: The gastric (fundic) glands areresponsible for the majority of the gastricsecretions and contain the following cells:a. Chief (zymogenic) cells: secrete pepsi-nogen.
b. Parietal or oxyntic cells: Secrete hydro-chloric acid (HCl) to facilitate protein
ure 1
F PHAR
. Illustration of canine gastric anatomy.
MACEUTICAL SCIENCES, VOL. 98, NO. 3, MARCH 2009

JOURN
846 MARTINEZ AND PAPICH
digestion and activate digestingenzymes (e.g., pepsinogens) that be-come active in the stomach’s acid envir-onment and intrinsic factor, essentialfor vitamin B12 absorption from thesmall intestine.
c. Neck mucous cells: mucous secretingcells (mucous layer pH 4–6 comparedto stomach acid pH 1–2)6 to protect thegastric lining from damage by stomachacids.
d. Argentaffin cells (Enterochromaffin-like cells): endocrine cells secreting avariety of hormones including hista-mine, gastrin, motilin, substance P,vasoactive intestinal polypeptide andsomatostatin.
AL OF P
3. A
ntral pylorus region: These glands are veryextensive, secreting an alkaline mucous.Although these glands remain within themucosal layer of the stomach, they extendacross the muscularis mucosa of the duode-num. These glands contain few parietal orchief cells. Similar to the cardiac glands,the primary function of theses structuresis to protect the adjacent structure, theduodenum, from damage by gastric acidand enzymes.The muscularis mucosa is a low density smoothmuscle that is responsible for contractions ofthe rugae (the folds in the gastric mucosa). Thesubmucosal layer is the layer containing bothconnective tissue and the plexi of the entericnervous system. The gastric layer contains thebulk of the muscle mass responsible for thechurning of food (peristalsis) and the forwardthrust of material through the stomach intothe duodenum. It is also within this region thatthe interdigestive migrating myoelectric current(IMMC) initiates (a comparison of human versusIMMC characteristics is discussed later in thisreview). The gastric layer is subdivided intothree distinct muscle regions that are defined bythe direction of the muscle group. The oblique layeris the innermost muscular region, located imme-diately beneath the mucosal layer. The obliquelayer of the muscularis is clearly seen in the fundusand near the lesser curvature of the corpus, butdisappears towards the antrum. The circular layerof the muscularis is continuous with the circularlayer of the esophagus, but is absent in the fundus.The thickness of the circular layer increases in the
HARMACEUTICAL SCIENCES, VOL. 98, NO. 3, MARCH 2009
antrum and especially in the pyloric sphincter, butdoes not continue into the duodenum. The long-itudinal layer contains two muscle groups: themuscle that continues from the esophagus into thecorpus and the muscle that originates in the corpusand moves into the duodenum.
The separation of muscles into these twodistinct regions allows for the control of movementwithin the stomach. As the pressure within theantrum increases, the movement (persistalsis) ofthe corpus region decreases, allowing for the foodwithin the antrum to pass into the duodenumbefore additional materials move from the corpusto the lower portions of the stomach.
From an evolutional perspective, the caninestomach needs to accommodate large, infrequentmeals. Competition between animals necessitatesthat food be consumed rapidly and with minimalmastication.7 Therefore, the canine stomach needsto be capable of accommodating sudden largeincreases in volume and an ability to retain andgrind these large food chunks into digestibleparticles prior to moving them through to the smallintestine. Adjustment to sudden volume changes isaccommodated through the gastric rugae, whichtend to be substantially larger in the dog ascompared to that seen in the human stomach.The pulverization of consumed material is accom-plished both by the powerful contractile force of thecanine stomach and the restrictive properties of thecanine pylorus. The latter two points are discussedin greater detail later in this review.
METHODS OF STUDYING GASTRICTRANSIT IN DOGS
The estimates of gastric emptying and transittime can vary depending on the method used forstudy. The methods for studying gastric emptyinginclude:
1. G
amma scintigraphy. 2. R adiographic imaging [e.g., use of bariumimpregnated polystyrene spheres (BIPS) orother radio-opaque materials].
3. T
racer studies (13C-labeled substances). 4. A dministration of telemetric capsule (e.g.,SmartPill, BravoTM capsule) to monitorinternal pH and transit.
Gamma Scintigraphy
This method is considered the ‘‘gold standard’’ formonitoring stomach emptying and intestinal
DOI 10.1002/jps

GASTRIC RESIDENCE OF DOSAGE FORMS IN DOGS 847
transit to which other methods are compared.1,8,9
Gamma scintigraphy uses a meal or a dosage formthat is mixed with a radionucleotide to monitor GItransit. After the administration of the gamma-emitting source, the GI transit of the labeledmaterial is monitored with a gamma-camera. Thedata are analyzed by computer fitting to obtain thetransit rates.
Gamma scintigraphy is limited primarily toresearch facilities that have nuclear imagingcapabilities. It also poses a radiation hazard thatlimits use only to licensed facilities. However, thismethod has provided a standard to which othermethods can be compared.
Radiographic Imaging
This method entails the use of radiopaque solids orliquids that are mixed with food and imaged byradiography or fluoroscopy at regular intervals forapproximately 12 h after ingestion. Although itis an accurate method of measuring gastricemptying, it requires either physical or chemicalrestraint (sedative drugs) for proper positioning ofthe dog. The stress of physical restraint mayalter the animal’s gastric transit time becauseof sympathetic nervous system stimulation andsuppression of the parasympathetic system. Useof sedatives for these procedures is discouragedbecause many of the sedatives (e.g., alpha-2agonists, opiates, phenothiazine tranquilizers)are known to affect GI motility.
The use of solid radiopaque markers is perhapsthe best method to examine stomach emptying oforal dosage formulations. Radiopaque markerscan be placed in capsules or on spheres. One of themost commonly used forms is the barium-impreg-nated polyethylene spheres (BIPS). These spherescan range in size from 1.5 to 5 mm, depending onthe phase of gastric emptying to explore. AlthoughBIPS are helpful to examine some phases ofgastric emptying,10 the gastric emptying of BIPSdoes not always correlate with the emptying offood.11
Other imaging methods used in animals includeultrasonography and nuclear resonance imaging(MRI). Ultrasonography is noninvasive and doesnot impose any radiation hazard. However, its useis limited because of the expensive equipmentneeded, making it generally available only atlarge veterinary institutions. A potential pitfallwith this method is that the analysis of the dataoutput is subjective and therefore potentially
DOI 10.1002/jps JOU
operator-specific. Nevertheless, despite this draw-back, it is a useful method for monitoring GItransit, providing a detailed three-dimensionalimage of the GI tract.12
Tracer Studies
These include both systemically absorbed andnonabsorbable compounds. The absorbed tracermaterials can be monitored through exhaled air(breath test) or by measuring plasma/serum drugconcentrations. One such drug that has beenfrequently used for this purpose is acetamino-phen.13,14 Acetaminophen is not absorbed fromthe stomach and can be easily measured in theblood (plasma) of animals. (Note: acetaminophenshould never be used in feline studies because it isvery toxic to cats.). Therefore, when it appearsin the blood, it represents emptying from thestomach into the duodenum. In a recent study,Wyse et al.13 found that acetaminophen was agood marker for determining liquid phase sto-mach emptying because it dissolved in stomachcontents and emptied with liquid. Acetaminophencould potentially be combined in the matrix of acontrolled-release test formulation to measurethe gastric emptying characteristics of a novelformulation.
Breath tracers involve the administration ofa radiolabeled substance (typically involving a13C label) which is usually incorporatedinto medications and meals. An example of sucha marker is 13C-octanoic acid (OCT), a mediumchain fatty acid that is not absorbed in thestomach, but is well absorbed in the duodenum.15
Upon absorption in the proximal small intestine,it undergoes hepatic oxidation, resulting inthe release of 13CO2, which is collected from theexhaled air. Thus, the appearance of 13CO2 isdirectly related to the rate of gastric transit.
Some tracers are not systemically absorbed butcan be serially sampled from the GI tract. Theconcentration of the tracer is measured withimplanted cannulae or fistulae that have beeninserted prior to the study. Similarly, radio-telemetric capsules are used to monitor internalpH and have become a useful technology forpharmaceutical manufacturers, investigators ofGI physiology, and clinicians. One such example isthe BravoTM pH capsule. This is a radiotelemetricpH monitoring device that transmits pH record-ings from the animal’s stomach and intestineto an external source. Its dimensions are
RNAL OF PHARMACEUTICAL SCIENCES, VOL. 98, NO. 3, MARCH 2009

848 MARTINEZ AND PAPICH
2.5 cm� 0.6 cm� 0.4 cm. It can collect pHrecordings every 6 s for 24–48 h and has beensuccessfully used to monitor gastric emptyingtimes of dogs.16
Another example of a radiotelemetric device isthe ‘‘SmartPill,’’ which is a GI monitoring systemthat is designed as an in-office method forassessing gastric motility. The wireless SmartPillpH capsule collects pH, pressure and temperaturedata from throughout the entire GI tract. TheSmartPill was designed for use in evaluatinghuman patients with suspected delayed gastricemptying and has also been used by veterinaryinvestigators to monitor GI transit. The dimen-sions of the SmartPill are 13 mm� 26 mm.Additional details on the SmartPill can be foundat: http://www.smartpillcorp.com/. Examples ofveterinary applications are found on the com-pany’s web site.
Muscular Movement of Materials
There are two types of movements that will beconsidered in this review: the IMMC, which isa propagating electrical current moving fromthe stomach through the small intestine, andthe peristaltic movement. Peristalsis is respon-sible for mixing food with gastric juices and forgenerating the compression force that propels foodfrom the stomach into the small intestine. TheIMMC pushes food through the stomach and the
Figure 2. The interdigestive migrating comdenum of a dog and migrating to the terminal i30–36 h after the onset of fasting. As one complthe stomach and the duodenum. The four phasat each recoding site, being delineated phasefrom the Journal of Physiology, Wiley-Blackw
JOURNAL OF PHARMACEUTICAL SCIENCES, VOL. 98, NO. 3, MARCH 2009
intestine during the fasted state. The IMMCcharacteristics in dogs and people are similar,both being characterized by four distinct phases.17
These are:
Phase 1: Basal
plexes, starting in the stomach and duo-leum during a 6-h recording session madeex ends in the ileum, another one starts ines (I–IV) of each complex were recognizedIII activity. Reproduced with permissionell Publishers, Ref. 18.
D
45–60 min
A period of smooth muscle quiescenceand rare action potentials
Phase 2: Preburst 30–45 minPeristaltic contractions progressivelyincrease in frequency
Phase 3: Burst (housekeeper wave)
5–15 min Rapid, evenly spaced peristalticcontractions and pylorus remains open
Phase 4: Quiescent 0–5 minBrief period of transitionbetween Phases 3 and 1
An example of the IMMC in dogs is seen inFigure 2.18
The majority of IMMCs begin in the stomach,with fewer than half of the recorded complexesbeing recognizable beyond the midpoint of thesmall bowel. Less than 10% of the observedcomplexes reach the distal ileum.18
The third phase of the IMMC results in intenseperistaltic activity and is often referred to as the‘‘housekeeper wave’’17 because it is responsible forpushing residual materials out of the stomach.The housekeeper wave begins in the stomach andsubsequently propagates through all portions of
OI 10.1002/jps
GASTRIC RESIDENCE OF DOSAGE FORMS IN DOGS 849
the small intestine in a sequential pattern. Thepylorus remains open during phase 3 contrac-tions, allowing the stomach to empty the majorityof its contents.17 Therefore, particles that are toolarge to readily pass through the pylorus of thedog during earlier phases, will generally remainin the stomach until the onset of the housekeeperwave. Phase 3 activity occurs approximately every120 min in fasted humans19,20 and approximatelyevery 60–100 min in the fasted dog.10,18,19,21
However, the time to phase 3 activity followinga meal in dog is substantially longer than thetime needed to restore the housekeeper wave inhumans (e.g., 2.6–4.8 h in humans versus 5–13.3 hestimated in dogs).10,22 In addition, in dogs, theonset of the housekeeper wave is associated withan increase in gastric pH, from 2.4 to 8.3.23,24 Anexcellent summary of the IMMC across variousspecies, including dog and man, is provided byItoh et al.19
The effect of food on the IMMC is not simply afunction of gastric stretch. For example, if 400 mLof physiological saline solution is instilled into thecanine stomach, the resulting stretch causes abrief delay in the IMMC. However, the IMMCresumes within about 2 h, largely because salinerapidly exits the stomach. When 400 mL of milkrather than saline is instilled into the caninestomach, there can be a delay of up to 8 h untilthe IMMC resumed. The difference between theeffects of saline solution versus milk demonstratesthat variables other than simply stretch caninfluence the resumption of fasted electricalactivity.18
Although gastric distention inhibits the IMMC,it stimulates the peristaltic movement of foodby activating the vagus nerve and through localmyenteric reflexes in the stomach wall. The role oflocal reflexes in determining the characteristicsof theses contractions was demonstrated bysurgically dividing the canine stomach into anantral and a corpus pouch.25 The response todistention varied as a function of the respectivegastric region being stretched. With bothantral and corpus pouches, an increase in volumeresulted in an increase in peristaltic activity.However, while the antral response significantlyincreased upon simultaneous distention of thecorpus region, peristaltic activity in the corpusregion decreased in response to a simultaneousincrease in antral volume. Thus, the separation oflongitudinal muscles in the corpus versus antralregions allows for the selective contractions ofthese two regions, thereby modifying gastric
DOI 10.1002/jps JOU
emptying time and allowing for adequate diges-tion of a meal.
Gastric electrical pacemaker activity originatesin the cells of Cajal, which are located in thegreater curvature at the junction between theproximal and distal stomach. This current occursat a rate of 3 cycles per minute in humans and5 cycles per min in dogs.26,27 These slow wavespropagate from the proximal body to the pylorus,and although these slow waves do not causecontractions in the unstimulated stomach, peri-staltic contractions follow the spread of theslow waves. Bradygastria occurs when the normaldominant pacemaker fails and other oscillatorysites in the gastric body take over the depolariza-tions. Tachygastria occurs when a rival pace-maker generates an oscillatory pattern at anabnormally high rate, thereby overriding normalgastric pacemaker activity.26
Gastric electrical activity has recently becomean area of intense research as gastric electricalstimulation (GES) is being evaluated as apotential therapy for obesity in humans. In manyof these studies, the dog has served as an animalmodel for studying the relationship betweengastric volume, retrograde GES, and food con-sumption. GES produces an artificial tachy-gastria, leading to gastric hypomotility and areduction in food intake in dogs.26,28 Thiswas shown with gamma scintigraphy, where thegastric emptying of a test meal, administeredafter 30 min of continuous GES (which lasted for atotal duration of 2.5 h) was significantly slowed(gastric emptying was monitored for a total of 4 h).The time for 50% of the meal to exit the stomachincreased from 177.7� 27.1 min with sham GESto 254.6� 71.7 min with GES.29
FACTORS THAT CAN INFLUENCE THE RATEOF GASTRIC TRANSIT IN THE DOG
Particle Size, Shape, and Density
Every small animal veterinarian has had theexperience of examining and treating cases offoreign body ingestion in dogs. Some foreignbodies block the pylorus and cause gastric disease.However, some objects can ‘‘miraculously’’ passinto the duodenum. Small animal veterinarianshave surgically removed items such as tennisballs, socks, play toys, and bones from theintestine of dogs. Despite this apparent amazingability of the dog to pass these large and dense
RNAL OF PHARMACEUTICAL SCIENCES, VOL. 98, NO. 3, MARCH 2009
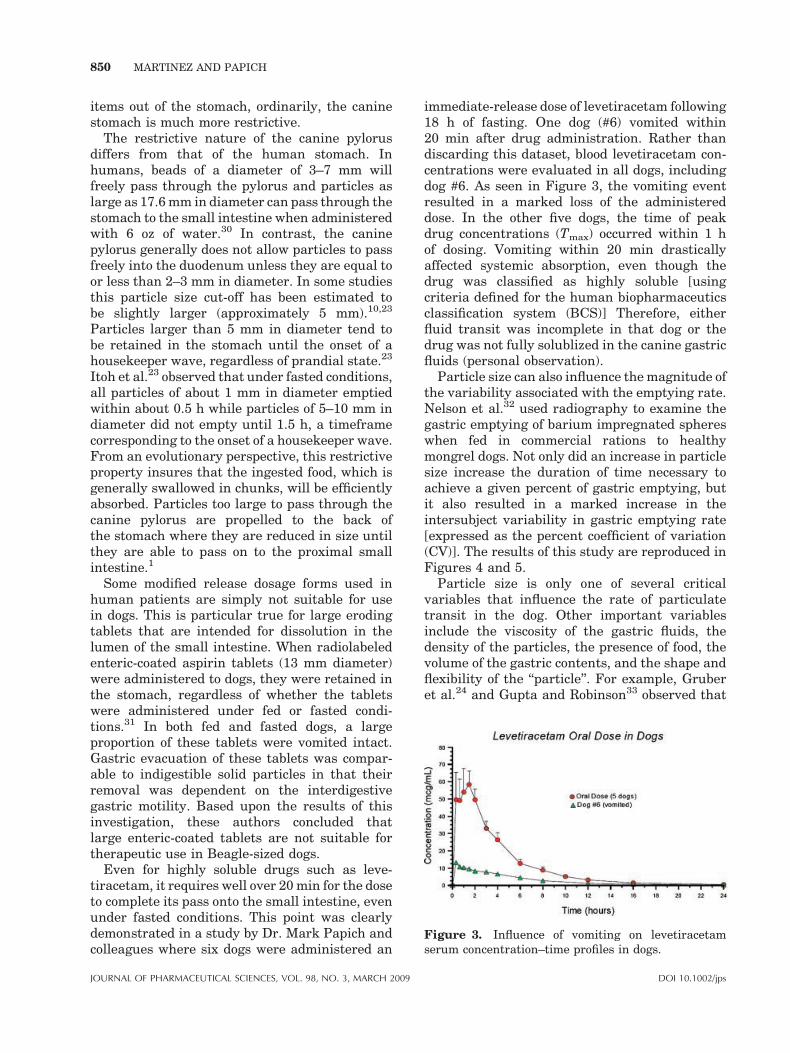
Figure 3. Influence of vomiting on levetiracetamserum concentration–time profiles in dogs.
850 MARTINEZ AND PAPICH
items out of the stomach, ordinarily, the caninestomach is much more restrictive.
The restrictive nature of the canine pylorusdiffers from that of the human stomach. Inhumans, beads of a diameter of 3–7 mm willfreely pass through the pylorus and particles aslarge as 17.6 mm in diameter can pass through thestomach to the small intestine when administeredwith 6 oz of water.30 In contrast, the caninepylorus generally does not allow particles to passfreely into the duodenum unless they are equal toor less than 2–3 mm in diameter. In some studiesthis particle size cut-off has been estimated tobe slightly larger (approximately 5 mm).10,23
Particles larger than 5 mm in diameter tend tobe retained in the stomach until the onset of ahousekeeper wave, regardless of prandial state.23
Itoh et al.23 observed that under fasted conditions,all particles of about 1 mm in diameter emptiedwithin about 0.5 h while particles of 5–10 mm indiameter did not empty until 1.5 h, a timeframecorresponding to the onset of a housekeeper wave.From an evolutionary perspective, this restrictiveproperty insures that the ingested food, which isgenerally swallowed in chunks, will be efficientlyabsorbed. Particles too large to pass through thecanine pylorus are propelled to the back ofthe stomach where they are reduced in size untilthey are able to pass on to the proximal smallintestine.1
Some modified release dosage forms used inhuman patients are simply not suitable for usein dogs. This is particular true for large erodingtablets that are intended for dissolution in thelumen of the small intestine. When radiolabeledenteric-coated aspirin tablets (13 mm diameter)were administered to dogs, they were retained inthe stomach, regardless of whether the tabletswere administered under fed or fasted condi-tions.31 In both fed and fasted dogs, a largeproportion of these tablets were vomited intact.Gastric evacuation of these tablets was compar-able to indigestible solid particles in that theirremoval was dependent on the interdigestivegastric motility. Based upon the results of thisinvestigation, these authors concluded thatlarge enteric-coated tablets are not suitable fortherapeutic use in Beagle-sized dogs.
Even for highly soluble drugs such as leve-tiracetam, it requires well over 20 min for the doseto complete its pass onto the small intestine, evenunder fasted conditions. This point was clearlydemonstrated in a study by Dr. Mark Papich andcolleagues where six dogs were administered an
JOURNAL OF PHARMACEUTICAL SCIENCES, VOL. 98, NO. 3, MARCH 2009
immediate-release dose of levetiracetam following18 h of fasting. One dog (#6) vomited within20 min after drug administration. Rather thandiscarding this dataset, blood levetiracetam con-centrations were evaluated in all dogs, includingdog #6. As seen in Figure 3, the vomiting eventresulted in a marked loss of the administereddose. In the other five dogs, the time of peakdrug concentrations (Tmax) occurred within 1 hof dosing. Vomiting within 20 min drasticallyaffected systemic absorption, even though thedrug was classified as highly soluble [usingcriteria defined for the human biopharmaceuticsclassification system (BCS)] Therefore, eitherfluid transit was incomplete in that dog or thedrug was not fully solublized in the canine gastricfluids (personal observation).
Particle size can also influence the magnitude ofthe variability associated with the emptying rate.Nelson et al.32 used radiography to examine thegastric emptying of barium impregnated sphereswhen fed in commercial rations to healthymongrel dogs. Not only did an increase in particlesize increase the duration of time necessary toachieve a given percent of gastric emptying, butit also resulted in a marked increase in theintersubject variability in gastric emptying rate[expressed as the percent coefficient of variation(CV)]. The results of this study are reproduced inFigures 4 and 5.
Particle size is only one of several criticalvariables that influence the rate of particulatetransit in the dog. Other important variablesinclude the viscosity of the gastric fluids, thedensity of the particles, the presence of food, thevolume of the gastric contents, and the shape andflexibility of the ‘‘particle’’. For example, Gruberet al.24 and Gupta and Robinson33 observed that
DOI 10.1002/jps

Figure 4. Time for gastric emptying for 50% of sub-jects. Based upon data from Ref. 32.
Figure 6. Mean gastric emptying of particles ofvarious densities when co-administered with 300 mL2.0% methocel solution. Percent particles recoveredhave been plotted as a function of time after adminis-tration. Each data point is the average value from ninestudies. Reprinted with permission from Elsevier, theInternational Journal of Pharmaceutics, Ref. 33.
GASTRIC RESIDENCE OF DOSAGE FORMS IN DOGS 851
polystyrene and amberlite emptied from thestomach in a similar manner. However, thissimilarity was dependent upon solution viscosityand the volume of fluid administered with theparticles. Generally, high viscosity fluids im-proved particle distribution and slowed the rateof particle emptying. When the fluid volumewas 50 mL, amberlite particles transited morerapidly than did the polystyrene or glass beads (allparticles were of similar diameter and shape).However, when the volume increased to 300 mL,the amberlite and the polystyrene particlesemptied at similar rates. In contrast, the glassbeads did not empty until most of the fluid wasgone (long lag time), but they emptied quicklyonce the high antral activity (phase 3 contrac-tions) began. Nearly 100% of the glass beadsexited the stomach within 20–30 min after thefirst set of glass beads were observed in theduodenum. Thus, there appears to be an optimalparticle density, above and below which particlesof the same size tend to empty more slowly (Fig. 6).With the higher volume, the dosage form isdispersed in the fluids, causing a longer duration
Figure 5. Variability in gastric emptying timeincreases as a function of particle size. Based upon datafrom Ref. 32.
DOI 10.1002/jps JOU
of time for complete emptying. When highviscosity fluids are administered, the stomachmay respond as it does during feeding, therebylimiting the passage of the more dense materialsuntil high antral activity is resumed.10,33
Even when particles are of uniform size anddensity, emptying depends on the time of drugadministration relative to the onset of the house-keeper wave. This was observed in a study byGruber et al.24 where small amberlite particleswere administered to fasted dogs with or withoutregard to the timing of the housekeeper wave.When the IMMC was ignored, the particlesemptied within 10 and 120 min. However, whenthe same amberlite particles (0.7–6.4 mm indiameter and with densities ranging from 0.5 to2.9 gm/cm3) were administered 10 min prior to theonset of the housekeeper wave, all emptied within90 min.
Effect of Food
An important function of the postmeal period ofperistaltic contractions is the facilitation of themechanical breakdown of food and the mixing ofthis food with the gastric fluids to form a semi-liquid chyme (a process known as trituration).This process is achieved by repeated contractionsof the antral circular muscles. The amplitude ofthese contractions increases as the wave movesdistally. These antral contractions generate a
RNAL OF PHARMACEUTICAL SCIENCES, VOL. 98, NO. 3, MARCH 2009

852 MARTINEZ AND PAPICH
back and forth oscillating movement against acontracted pylorus, resulting in the fragmentationof digestible solids.With regard to food effects,variables to be considered include:
� T
JOURN
he energy density of the meal: the moreenergy rich meal results in a greater slowingof gastric emptying.34,35
� T
he viscosity and volume of the meal: thegreater the volume and viscosity, the slowerthe rate of gastric emptying.33,36–38� O
smolarity: an increase in osmolarity slowsgastric transit of the ingested meal.39Figure 7. Fractions of enteric-coated tablets ofbarium sulfate remaining in the stomach of individualdogs (n¼ 4) under fasting (- - -) and nonfasting (—)conditions. Five tablets were administered to eachdog except for one dog, which was given four tablets.The paired t test (p¼ 0.01) revealed a significantdifference between fasting and nonfasting conditionsin the time required for 50% of the tablets to be emptied.Reprinted with permission of Wiley-Liss, Inc., a sub-sidiary of John Wiley & Sons, Inc., Journal of Pharma-ceutical Sciences, Ref. 42.
High viscosity meals may affect stomachmotility by inducing a slowing of gastric transitthat is more pronounced in the dog as comparedto that observed in humans.40 However, thisviscosity effect is unlikely to have clinical re-levance in dogs because the majority of caninemeals have a viscosity on the order of approxi-mately 100 cP, which results in a relatively smallincrease in the viscosity of the gastric contents.40
Once the majority of the digestible solids haveemptied from the stomach, the IMMC is restoredand remaining stomach contents are propelledthrough the stomach and small intestine.17
Liquids, digestible food and indigestible solidsare emptied in separate phases,1 with the liquidphase emptying substantially sooner than thesolid phase.1,13,22,33 Since liquids tend to emptyseparately from solids, it would logically followthat food would have minimal impact on theshape of the blood concentration/time profile ofhighly soluble compounds. However as seen whenmetoprolol tartrate and cephalexin tablets wereadministered to dogs, this may not always be thecase. In an in vitro and an in vivo study (the latterusing Labrador Retrievers of approximately 30 kgbody weight), fed conditions delayed the disin-tegration and dissolution of immediate releasemetoprolol tartrate tablets. Under both in vivoand in vitro conditions, this delay was attributedto the formation of a film around the tablets.The varying the composition of binders anddisintegrants when formulating these tabletssucceeded in modifying the impact of this foodeffect. It is suggested that the film around thetablets both slowed the water penetration intothe tablet and prevented particles from leavingthe tablet.41
The magnitude of the food effect also dependsupon particle size, leading to a substantial magni-fication of the particle size-related differences in
AL OF PHARMACEUTICAL SCIENCES, VOL. 98, NO. 3, MARCH 2009
gastric transit time. For example, under fastedconditions, 100% of the administered sphericaltablets (6 mm diameter, 1.5 mm thick, 1.52 g/cm3
density: 5 tablets/dog) or smaller cylindricalgranules (1 mm diameter, 1.5–2.5 mm thick,1.34 g/cm3 density: 50 granules/dog) emptiedwithin about 2 h after dosing (Figs. 7 and 8,respectively). Food caused a large and highlyvariable delay in the emptying of the tablets(emptying time ranged between 18 and 35 h) butonly a moderately increase in the gastric empty-ing time of the smaller-size cylindrical granules(where the time for gastric transit was approxi-mately 4–6 h).42 Itoh et al.23 showed that whileparticles up to 10 mm in diameter could beemptied with the housekeeper wave in fasted dogs(within 1.5 h), particles greater than 5 mmin diameter were retained for over 7.5 h whenadministered after a meal.
Similarly, Kaniwa et al.43 observed thatacetaminophen soluble powder, enteric coatedpyridoxal phosphate tablets, and aspirin granuleswere all well absorbed when administered tofasted dogs, but that food had a very differenteffect on the absorption of these three differentdosage forms. When administered to dogs after ameal, the peak plasma concentration (Tmax) wasvirtually unchanged for the soluble acetamino-phen powder but the absorption was eithersignificantly delayed or curtailed for the granulesand tablets, respectively. In contrast, a markedlysmaller food effect was observed in humans whowere administered these same three formulationsunder fed or fasted conditions. The canine andhuman blood level profiles associated with these
DOI 10.1002/jps

Figure 8. Fractions of ethyl cellulose-coated gran-ules of barium sulfate remaining in the stomach ofindividual dogs (n¼ 4) under fasting (- - -) and nonfast-ing (—) conditions. The paired t-test (p¼ 0.05) revealeda significant difference between fasting and nonfastingconditions in the time required for 50% of the granulesto be emptied. Reprinted with permission of Wiley-Liss,Inc., a subsidiary of John Wiley & Sons, Inc, Journal ofPharmaceutical Sciences, Ref. 42.
GASTRIC RESIDENCE OF DOSAGE FORMS IN DOGS 853
formulations are shown in Figures 9 and 10,respectively.
Differences between the impacts of food onhuman versus canine oral bioavailability arealso seen when comparing the results of studiesinvolving cephalosporin oral bioavailability. In
Figure 9. Plasma concentration–time curvetration of acetaminophen in powder (a), aspyridoxal phosphate in an enteric-coated tabin dogs. Reproduced with permission fromcopyright 1988, the Pharmaceutical Society o
DOI 10.1002/jps JOU
dogs, a markedly greater food effect was seen onthe oral bioavailability of the cefadroxil (a poorlywater soluble compound) as compared the water-soluble compound, cephalexin. Food delayed theTmax of cephalexin but had a negligible effect on itsAUC. With cefadroxil food markedly delayedthe Tmax as compared to the profiles observedunder fasted conditions, but food also resulted ina marked increase in cefadroxil AUC values(Fig. 11).44 In contrast to that seen in dogs, whencefadroxil and cephalexin were administered tohumans, there was no effect of food for eitherdrug.45
Nutrient-rich meals cause a delay in gastricemptying, at least in part through the stimulationof chemoreceptors located in the proximal smallintestine.39 In so doing, the small intestinalchemoreceptors tightly control the rate of gastricemptying and the efflux of nutrients from thestomach. This hormonal regulation of gastricemptying appears to be dependent on mealcomposition. The ingestion of lipids is known toslow gastric emptying, likely via reflex reactionstriggered by the lipolytic products liberated bythe activity of pancreatic lipase in the smallintestine.46,47 In addition, while some reflexreactions are caused by exposure of duodenumto the contents of the chyme (causing bluntingof peristaltic activity), others are related to thedirect gastric effects of the stomach contents.
s of drugs and metabolites after adminis-pirin in enteric-coated granules (b) orlet in the fasting and nonfasting statesthe Journal of Pharmacobio-Dynamics,f Japan, Ref. 43.
RNAL OF PHARMACEUTICAL SCIENCES, VOL. 98, NO. 3, MARCH 2009

Figure 10. Excretion rate-curves of metabolites after an administration of acetamino-phen in powder (a), aspirin in enteric-coated granules (b) or pyridoxal phosphate in anenteric-coated tablet in the fasting and nonfasting states in human subjects. Reproducedwith permission from the Journal of Pharmacobio-Dynamics, copyright 1988, thePharmaceutical Society of Japan, Ref. 43.
854 MARTINEZ AND PAPICH
For example, in the dog stomach, peristalsis isinhibited by the presence of L-tryprotphan in thestomach in a dose-dependent manner. A similareffect does not occur in response to D-tryptophan,indicating that response is stereospecific. Theeffect of tryptophan on gastric emptying rate isbelieved to be, at least in part, due to a reflexrelease of intestinal cholecystokinin (CCK). Asimilar effect is seen in humans, but the aminoacid responsible for eliciting this effect in humansis phenylalanine rather than tryptophan. Gastricmotility is also inhibited by increasing the
Figure 11. Left Panel: Mean serum cefadroxof 30 mg/kg with and without food in five dogconcentration (�SE) after oral administrationdogs. Reproduced with permission from theTherapeutics, Blackwell Publishers, Ref. 44.
JOURNAL OF PHARMACEUTICAL SCIENCES, VOL. 98, NO. 3, MARCH 2009
osmolality of the stomach contents, with nutritiveand nonnutritive substances exerting similareffects.48
STRATEGIES FOR DEVELOPINGCONTROLLED-RELEASE AND GASTRICRETENTION DEVICES FOR USE IN DOGS
Very few oral sustained release formulations havebeen approved for use in dogs because of theirrapid intestinal transit. The small intestinal
il concentration after oral administrations. Right Panel: Mean serum cephalexinof 30 mg/kg with and without food in fiveJournal of Veterinary Pharmacology &
DOI 10.1002/jps

GASTRIC RESIDENCE OF DOSAGE FORMS IN DOGS 855
transit time is approximately 2 h in the dog and3–4 h in humans, and total GI transit time isapproximately 6–8 h in the dog versus 20–30 h inhumans.49,50 Furthermore, the crushing force ofthe canine stomach is greater than that associatedwith the human stomach. The gastric ‘‘destructiveforce’’ is approximately 3.2 N in the dog (fed orfasted) and 1.5 N (fasted) versus 1.9 N (fed) inhumans.51,52 Accordingly, formulations (parti-cularly sustained release tablets) that functionappropriately when administered to people mayfail when administered to dogs.
The dissimilarity between human and caninecrushing force can be particularly importantwhen attempting to use the dog as an animalmodel during the development of gastro-retentivedevices for use in human patients,53 or whentrying to develop colon-targeted delivery systemsthat must remain relatively intact to preservetheir controlled-release action. Human–caninedifferences in oral bioavailability have been atleast in part attributed to this difference incrushing force for a several products includingcyclandelate capsules,54 indomethacin capsules,55
and griseofulvin tablets.56 When extended-releasetheophylline formulations intended for humanuse were administered to dogs (Theochron tabletsand TheoCap capsules, Inwood Laboratories,Inwood, NY), there was little evidence of anextended-release profile.57 The mean canineterminal half-life for IV theophylline, the oralextended-release tablets, and oral extended-release capsules were all similar (8.4, 10.9, and12.7 h, respectively). This observation indicated arapid (rather than the intended prolonged) in vivodrug release, and a nearly complete intestinalabsorption of the theophylline contained in theextended release tablets and capsules. We suspectthat absorption must have occurred via a rapidrelease of the drug, and absorption in the smallintestine because theophylline is ordinarily con-sidered a Class IV drugs in the human BCSclassification scheme. Therefore, the strong crush-ing force of the canine stomach should beconsidered when developing sustained releaseoral dosage forms, particularly those that areintended for gastric retention.
To overcome this problem, there are severalmethods for achieving gastric retention thatmay be worthy of consideration. These includeparticle flotation, particle sinking, mucosal adhe-sion, product expansion (unfolding), and swellingdevices.58 An example of an expandable oraldevice is the levodopa gastro-retentive dosage
DOI 10.1002/jps JOU
form that is formulated to unfold to a size of5 cm� 2.5 cm. This device was successfullyretained in the dog stomach for at least 24 h,thereby extending the release of the medication,levodopa.59 One disadvantage of this particulargastric retention device, however, was that a lowpH was needed to ‘‘unfold’’ the device into theshape needed for gastric retention. Because thefasted dog stomach is not sufficiently acidic forthis to occur, the dogs in this study were co-administered a 400 mL dose of an acidic buffer(pH 1.5).
Modification of particle density can be atechnique for creating gastric flotation devicesthat achieve prolonged gastric residence. How-ever, the potential impact of prandial state onthe performance of these devices needs to beconsidered. For example, despite the presence ofhousekeeper waves in fasted dogs, an experi-mental floating tablet (a gastric-retentive formu-lation) was retained for approximately 4 h.60
Conversely, fasting significantly influenced theperformance of superporous hydrogels (SPH)administered in hard gelatin capsules. Uponexposure to the gastric fluids, the SPH swellsto a size that causes gastric retention. Whenadministered to dogs, the SPH composite re-mained in the stomach for 2–3 h, after which theywere crushed and into smaller pieces and sub-sequently emptied into the small intestine. Whenfood was given immediately prior to dosing, theSPH composite remained in the stomach for morethan 24 h, even though the fed condition wasmaintained for only the first few hours.
Impact of Stress on Animal Subjects
Experimental conditions that increase release ofstress hormones can decrease the rate of gastricemptying. This point was shown in severalstudies. Gue et al.61 examined the influence ofacoustic stress on postprandial GI motility, gastricemptying, and the plasma gastrin levels ofpancreatic polypeptide, motilin, and somatostatinin conscious dogs. Six dogs were equipped withstrain-gauge transducers and were exposedfrom 1 to 3 h after the meal to prerecorded music(80–90 dB broad frequency noise). The acousticalstress resulted in a statistically significantlengthening of the gastric (31.2%) and jejunal(37.0%) postprandial motility pattern. In fourother dogs equipped with gastric cannulae, a 2-hsession of acoustic stress beginning just after
RNAL OF PHARMACEUTICAL SCIENCES, VOL. 98, NO. 3, MARCH 2009

856 MARTINEZ AND PAPICH
eating a radiolabeled standard meal induced aslowing of gastric emptying of both liquid (45.7%)and solid (47.1%) phases. These results indicatethat acoustic stress affects gastric and intestinalpostprandial motility in dogs, delaying the re-covery of the IMMC, inducing a transient slowingof gastric emptying, and enhancing the feeding-induced release of gastrin, pancreatic polypeptide,and somatostatin. The transport of dogs to anunknown environment can also decrease inantropyloral motor activity and therefore prolonggastric residence time.62
These investigations demonstrate that whenoral medications are administered to treat seriousdiseases, when the dog is in an unfamiliarenvironment (e.g., veterinary hospital), or if thereare conditions that can elicit the release of stresshormones, the resulting effects on GI transit,as described above, could potentially influencethe success of the oral drug therapy. It alsounderscores the importance of evaluating oraldrug products in clinical studies that provideinformation on product performance in a naturalsetting.
CANINE BREED DIFFERENCES
There has been substantial debate in the litera-ture regarding the potential difference in gastrictransit time across canine breeds. Although someinvestigators have concluded that no differencesexist, others have concluded that the rate ofgastric emptying may be breed-dependent.
Breed-related differences in gastric transit wassuggested in a study that used the OCT breathtest in 24 healthy dogs (3 Miniature Poodles,1 Beagle, 6 Schnauzers, 5 Giant Schnauzers,5 Great Danes, 3 Labrador Retrievers and1 Argentine Dane). Gastric emptying rate wasdetermined on a single occasion after a standardmeal. The time for 25% of the AUC to be exhaledwas highly correlated to body weight, wherelarger dogs had a longer gastric residence timeas compared to smaller dogs.15 The time to 25%AUC ranged from 60 to 120 min. The correspond-ing equation was as follows (r¼ 0.76, p< 0.001,n¼ 24):
Time to 25%AUC ¼ 0:87 � body weight þ 63
Tmax was also highly correlated (polynomialrelationship), with Tmax values ranging between75 and 160 min. In this case, a polynomialequation was associated with the best fit of
JOURNAL OF PHARMACEUTICAL SCIENCES, VOL. 98, NO. 3, MARCH 2009
the datapoints (r¼ 0.78, p< 0.001, n¼ 24). Thecorresponding equation was as follows:
Time to peak concentration
¼ 78:8 � ð1:38 � body weightÞ
þ ð0:05 � body weight2Þ
Differences in the gastric transit times of Beaglesand mongrels were shown using a radiotelemetricdevice (Bravo capsule).16 Gastric pH and gastricemptying was monitored with gamma scinti-graphy. Gastric emptying of the capsule in fedmongrel dogs ranged from 16 to 23 h. In contrast,the gastric emptying of the capsule in fed Beagledogs was only 7.5–8 h. Under fasted conditions,the difference in gastric emptying was lessmarked with emptying occurring within 1–3 hin mongrels versus 0.25–1.92 h in Beagles.These studies demonstrated differences and aprofound effect of food on the emptying of thesecapsules. (Dimensions of the Bravo capsule are2.5 cm� 0.6 cm� 0.4 cm.)
There are also breed-related differences inthe relationship between particle size andgastric retention, where the minimum restrictivesize for a device retained by the stomachdepended on the size of the breed. A tetrahe-dron-shaped device (2-cm per arm) was retainedin the 10-kg Beagle dog for 24 h, but was rapidlyemptied in the 35 kg American Foxhounds. Inhumans, the gastric residence of the deviceranged from about 1 h to about 5 h in the fastedstate and increased to less than 7.5 h in all butone subject when administered the capsule aftera meal.63
Breed may also influence the effect of motility-altering agents on gastric transit. In a study byBurger et al.64 the effect of atropine, glycopyrro-late, metoclopramide and cisapride on antralmotility was investigated in eight dogs (fourBeagles and four Labradors) using passive tele-metry. Both anticholinergics induced a pro-nounced and lasting reduction of the intensityand frequency of the contractions. However,marked differences were seen across breeds interms of their responses to the prokinetic agents.In Beagles, low-dose metoclopramide (0.3 mg/kgBW), or low-dose cisapride (0.2 mg/kg BW)resulted in a significant increase in the amplitudeof gastric contraction. Conversely, in Labradorsthese doses had either no effect (cisapride) or onlya transient effect (metoclopramide) on antralcontraction. Cisapride did not affect the frequency
DOI 10.1002/jps

GASTRIC RESIDENCE OF DOSAGE FORMS IN DOGS 857
of antral contractions in either Beagles orLabradors. In Beagles, metoclopramide resultedin a dose-related increase in the frequency ofcontraction. Metoclopramide did not increase thefrequency of contraction in Labradors. Whetherthis breed difference reflected differences indrug pharmacokinetics or in gastric response tothe respective agents was not determined. Still,considering that two different prokinetic agentselicited similar breed differences, it is likely thatthere are indeed some differences in the respon-siveness of the gastric smooth muscle to theseagents.
Figure 12. Variables influencing the gastric resi-dence time of materials.
SUMMARY
When considering the difference in the eatingbehavior of dogs and humans, it is not surprisingthat there are adaptive differences in theirrespective digestive systems. The human GItract is acclimated to an omnivorous diet thathas been well masticated prior to swallowing.The canine GI tract has evolved to accommodatea carnivorous diet, consumed as large, poorlymasticated chunks that are high in protein andfat content. Accordingly, there are human–canine differences in the strength of antralcontractions, in the sieving behavior of thepyloric sphincter, and in the time needed totransfer food from the stomach to the proximalintestine.
Although target values or ‘‘rules of thumb’’estimates for gastric transit characteristics areoften sought, attempts to generate such genera-lizations are fraught with pitfalls. There is also noabsolute consensus on the minimal size particleassociated with gastric retention because it isdependent on food effects, volume of meal or fluidchase, particle density, and time of administrationrelative to the IMMC. Similarly, there is no‘‘universal’’ gastric residence time that one canassign without considering other variables suchas prandial status, particle size, particle density,and possibly even breed. Perhaps, the mostgeneral statement that can be made is that ifthe drug rapidly dissolves into solution, or if theparticles are small enough to pass through thepylorus (2 mm in diameter or less), if the animalis in a fasted state, and if the volume of the fluidchase is small (e.g., 50 mL in a Beagle dog), wecan assume that it will take approximately 30 minfor the dose to be nearly completely emptied from
DOI 10.1002/jps JOU
the canine stomach. This may impact what isconsidered to be a rapidly dissolving dosage formin a dog. However, even in this situation, there issome variability across and within animals,depending upon such variables as breed, stress,and time of dosing relative to the time of thehousekeeper wave. As was seen in the decrease inlevetiracetam exposure, most of the dose appearedto have been lost when a dog vomited 20 min afterdosing, even though the drug is classified ashighly soluble.
Ultimately, the gastric emptying of oral dosageforms in dogs depends upon a host of variables, assummarized in Figure 12.
The relationship between the variablesdescribed in Figure 12 and how they mayinfluence the gastric residence of products whenadministered to humans versus dogs is describedin Table 1.
A recent US Pharmacopeia (USP) ad hoccommittee has been convened to define thecriteria for highly soluble and highly permeabledrugs in dogs. This canine-adjusted BCS will beinvaluable for predicting drug oral bioavailabilityin dogs and those situations when gastricresidence time may be the rate determiningstep in product absorption. The resulting insightsinto the many variables impacting canine gastrictransit time will be impact the development ofsustained release oral dosage forms. Ultimately,it is anticipated that tailoring the BCS tocanine physiology will help predict canine oralbioavailability and situations where canine drug
RNAL OF PHARMACEUTICAL SCIENCES, VOL. 98, NO. 3, MARCH 2009

Table 1. Factors Influencing the Similarity and Differences of Gastric Transit Times between Dogs and Humans
Attribute Dog–Human ComparisonPotential Consequence on
Oral Drug Absorption
DifferencesGastric crushingforce
Canine gastric crushing forcemarkedly exceeds that observed in people
The dog stomach may crush controlledrelease dosage forms (resulting in‘‘dose dumping’’) that might otherwiseremain intact in the human stomach
Restrictive natureof the pylorus
The canine pylorus is substantiallymore restrictive than the human pylorus
The movement of particles/dosage formsthat might readily transit the humanstomach can be stopped by the caninepylorus. This will prolonged its gastricresidence in the dog
Food effects Observed interspecies differences include theimpact of specific nutrients on peristalticactivity and the longer postprandialdelay for restoring Phase 3 ofthe IMMC in dogs
Human–canine differences in oral drugabsorption are likely to be magnifiedwhen the drug is administered underfed versus fasted conditions
SimilaritiesGastric anatomy The stomachs of dogs and humans have
effectively the same microscopic anatomy.However, the relative compositions of thevarious regions differ across dogsand humans
Similarities in gastric anatomy resultsin the comparability of gastric motoractivities and particle movementsduring the gastric phase of digestion.This is an important similarity whenusing the dog as a model for studyingpotential electrical anti-obesitytherapies
IMMC Essentially the same in dogs and peopleunder fasted conditions, but delays occur indogs under fed conditions (see food effects)
Under fasted conditions, small particles(e.g., 2–3 mm in diameter) and fluidstraverse the fasted dog and fastedhuman stomachs at a similar rate
858 MARTINEZ AND PAPICH
absorption characteristics may differ from that inhumans.
REFERENCES
1. Wyse CA, McLellan J, Dickie AM, Sutton DG, Pre-ston T, Yam PS. 2002. A review of methods forassessment of the rate of gastric emptying in thedog and cat: 1898–2002. J Vet Int Med 17:609–621.
2. Martinez MN, Papich MG, Riviere JE. 2004. Stimulito the Revision Process: Veterinary application of invitro dissolution data and the biopharmaceutics clas-sification system. USP Pharmacopeial Forum. 30,November–December.
3. Ellenberger W, Baum H. 1943. Handbuch dervergleichenden Anatomie der Haustiere. 18th Ed.Berlin, Springer. as cited in: Miller ME, Christen-sen GC, & Evans HE. Anatomy of the Dog. WBSaunders Co, Philadelphia. Chapter 13 The Di-gestive System and Abdomen, pp 645–712.
4. Kararli TT. 1995. Comparison of the gastrointest-inal anatomy, physiology, and biochemistry of
JOURNAL OF PHARMACEUTICAL SCIENCES, VOL. 98, NO. 3, MARCH 2009
humans and commonly used laboratory animals.Biopharm Drug Dispos 16:351–380.
5. Evans HE. 1993. Miller’s anatomy of the dog, 3rdedition. St. Louis, MO: Elsevier. 1130 pp.
6. Patronella CK, Vanek I, Bowen JC. 1988. In vivomeasurement of gastric mucous pH in canines:Effect of high luminal acidity and prostaglandin E2.Gastroenterology 95:612–6618.
7. Bradshaw JW. 2006. The evolutionary basis forthe feeding behavior of domestic dogs (Canis famil-iaris) and cats (Felis catis). J Nutr 136:1927S–1931S.
8. Parkman HP, Miller MA, Fisher RS. 1995. Role ofnuclear medicine in evaluating patients with sus-pected gastrointestinal motility disorders. SeminNucl Med 25:289–305.
9. Abell TL, Camilleri M, Donohoe K, Hasler WL, LinHC, Maurer AH, McCallum RW, Nowak T, Nusy-nowitz ML, Parkman HP, Shreve P, Szarka LA,Snape WJ, Jr., Ziessman HA. 2008. Consensusrecommendations for gastric emptying scintigra-phy: A joint report of the American Neurogastroen-terology and Motility Society and the Society of
DOI 10.1002/jps

GASTRIC RESIDENCE OF DOSAGE FORMS IN DOGS 859
Nuclear Medicine. Am J Gastroenterol 103:753–763.
10. Meyer JH, Dressman J, Fink A, Amidon G. 1985.Effect of size and density on canine gastric empty-ing of nondigestible solids. Gastroenterology 89:805–813.
11. Lester NV, Roberts GD, Newell SM, Graham JP,Hartless CS. 1999. Assessment of barium impreg-nated polyethylene spheres (BIPS) as a measure ofsolid-phase gastric emptying in normal dogs—Comparison to scintigraphy. Vet Radiol Ultrasound40:465–471.
12. Rubin DL, Muller HH, Young SW. 1991. Methodsfor the systematic investigation of gastrointestinalcontrast media for MRI: Evaluation of intestinaldistribution by radiographic monitoring. MagnReson Imaging 9:285–293.
13. Wyse CA, Marshall WG, Preston T, Yam PS. 2007.Retention of acetaminophen in an in vitro model ofsolid-phase gastric emptying of animals. Am J VetRes 68:895–898.
14. Takeda M, Mizutani Y, Yamano M, Tsukamoto K,Suzuki T. 2001. Gastric emptying in diabetic gas-troparetic dogs: Effects of SK-951, a novel proki-netic agent. Pharmacology 62:23–28.
15. Bourreau J, Hernot D, Bailhache E, Weber M,Ferchaud V, Biourge V, Martin L, Dumon H,Nguyen P. 2004. Gastric emptying rate is inverselyrelated to body weight in dog breeds of differentsizes. J Nutr 134:2039S–2041S.
16. Peters E, Vickers A. 2006. Preclinical evaluation:The characterization of preclinical researchdogs using a combination of pH monitoring &gamma scintigraphy. Drug Deliv Technol 6:50–53.
17. Minami H, McCallum R. 1984. The physiology andpathophysiology of gastric emptying in humans.Gastroenterology 86:1592–1610.
18. Code CF, Marlett JA. 1975. The interdigestive myo-electric complex of the stomach and small bowel ofdogs. J Physiol 246:289–309.
19. Itoh Z, Aizawa I, Sekiguchi T. 1982. The interdi-gestive migrating complex and its significance inman. Clin Gastroenterol 11:497–521.
20. Hwang S-J, Park H, Park K. 1998. Gastro-retentivedrug delivery systems. Crit Rev Ther Drug CarrierSyst 15:243–284.
21. Cunningham JG. 1997. Movements of the gastro-intestinal tract. In: Cunningham JG, editor.Textbook of veterinary physiology, 2nd edition.Philadelphia: Saunders. pp 272–289.
22. Sutton SC. 2004. Companion animal physiologyand dosage form performance. Adv Drug DelivRev 56:1383–1398.
23. Itoh T, Higuchi T, Gardner CR, Cladwell L. 1986.Effect of particle size and food on gastric residencetime of non-disintegrating solids in beagle dogs.J Pharm Pharmacol 38:801–806.
DOI 10.1002/jps JOU
24. Gruber P, Rubinstein A, Li V-HK, Bass P, RobinsonJR. 1987. Gastric emptying of nondigestible solidsin the fasted dog. J Pharm Sci 76:117–122.
25. Grundy D, Hutson D, Rudge LJ, Scratcherd T.1989. Pre-pyloric mechanisms regulating gastricmotor function in the conscious dog. Q J Exp Physiol74:857–865.
26. Owyang C, Hasler WL. 2007. Physiology and patho-physiology of the interstitial cells of Cajal: Frombench to bedside. VI. Pathogenesis and therapeuticapproaches to human gastric dysrhythmias. Am JPhysiol Gastrointest Liver Physiol 283:G8–G15.
27. Xu S, Wang Z, Hayes J, Chen JDZ. 2002. Is there aone-to-one correlation between gastric emptying ofliquids and gastric myoelectric or motor activity indogs? Dig Dis Sci 47:365–372.
28. Zhang J, Xu X, Chen JD. 2007. Chronic tachygas-trial electrical stimulation reduces food intake indogs. Obesity 15:330–339.
29. Song G-Q, Hou X, Sun Y, Yang B, Qian W, ChenJDZ. 2007. Effects of retrograde gastric electricalstimulation with pulse trains on gastric emptying ofsolids and plasma hormones in dogs. Am J Surg194:122–127.
30. Park HM, Chernish SM, Rosenek BD, Brunelle RL,Hargrove B, Wellman HN. 1984. Gastric emptyingof enteric-coated tablets. Dig Dis Sci 29:207–212.
31. Nap RC, Breen DJ, Lam TJGM, DeBruyne JJ. 1990.Gastric retention of enteric-coated aspirin tablets inbeagle dogs. J Vet Pharmacol Ther 13:148–153.
32. Nelson OL, Jergens AE, Miles KG, ChristensenWF. 2001. Gastric emptying as assessed by bar-ium-impregnated polyethylene spheres in healthydogs consuming a commercial kibble ration. J AmAnim Hosp Assoc 37:444–452.
33. Gupta PK, Robinson JR. 1995. Effect of volume andviscosity of coadministered fluid on gastrointestinaldistribution of small particles. Int J Pharm 125:185–193.
34. Meyer JH, Elashoff JD, Domeck M, Levy A, Jehn D,Hlinka M, Lake R, Graham LS, Gu YG. 1994.Control of canine gastric emptying of fat by lipolyticproducts. Am J Physiol Gastrointest Liver Physiol266:G1017–G1035.
35. Wyse CA, Preston T, Love S, Morrison DJ, CooperJM, Yam PS. 2001. Use of the 13C-octanoic acidbreath test for assessment of solid-phase gastricemptying in dogs. Am J Vet Res 62:1939–1944.
36. Lin HC, Zhao XT, Chung B, Gu YG, Elashoff JD.1996. Frequency of gastric pacesetter potentialdepends on volume and site of distension. Am JPhysiol Gastrointest Liver Physiol 270:G470–G475.
37. Ehrlein HJ, Prove J. 1982. Effect of viscosity of testmeals on gastric emptying in dogs. Q J Exp Physiol67:419–525.
38. Reppas C, Dressman JB. 1992. Viscosity modulatesblood glucose response to nutrient solutions in dogs.Diabetes Res Clin Pract 17:81–88.
RNAL OF PHARMACEUTICAL SCIENCES, VOL. 98, NO. 3, MARCH 2009
860 MARTINEZ AND PAPICH
39. Lin HC, Elashoff JD, Gu YG, Meyer JH. 1993.Nutrient feedback inhibition of gastric emptyingplays a larger role than osmotically dependent duo-denal resistance. Am J Physiol 265:G672–G676.
40. Reppas C, Eleftheriou G, Macheras P, SymillidesM, Dressman JB. 1998. Effect of elevated viscosityin the upper gastrointestinal tract on drug absorp-tion in dogs. Eur J Pharm Sci 6:131–139.
41. Abrahamsson B, Albery T, Eriksson A, GustafssonI, Sjoberg M. 2004. Food effects on tablet disinte-gration. Eur J Pharm Sci 22:165–172.
42. Aoyagi N, Ogata H, Kaniwa N, Uchiyama M,Yasuda Y, Tanioka Y. 1992. Gastric emptying oftablets and granules in humans, dogs, pigs, andstomach-emptying-controlled rabbits. J Pharm Sci81:1170–1174.
43. Kaniwa N, Aoyagi N, Ogata H, Ejima A. 1988.Gastric emptying rates of drug preparations. I.Effects of size of dosage forms, food and specieson gastric emptying rates. J Pharmacobiodyn 11:563–570.
44. Campbell BG, Rosin E. 1998. Effect of food onabsorption of cefadroxil and cephalexin in dogs.J Vet Pharmacol Ther 21:418–420.
45. Pfeffer M, Jackson A, Ximenes J, de Menezes JP.1977. Comparative human oral clinical pharmacol-ogy of cefadroxil, cephalexin, and cephradine. Anti-microb Agents Chemother 11:331–338.
46. Meyer JH, Elashoff JD, Domeck M, Levy A, Jehn D,Hlinka M, Lake R, Graham LS, Gu YG. 1994.Control of canine gastric emptying of fat by lipolyticproducts. Am J Physiol 266:G1017–G1035.
47. Meyer JH, Elashoff JD, Lake R. 1999. Gastric emp-tying of indigestible versus digestible oils and solidfats in normal humans. Dig Dis Sci 44:1076–1082.
48. Stephens JR, Woolson RF, Cooke AR. 1975. Effectsof essential and nonessential amino acids on gastricemptying in the dog. Gastroenterology 69:920–927.
49. Klausner EA, Lavy E, Friedman M, Hoffman A.2003. Expandable gastroretentive dosage forms.J Control Release 90:143–162.
50. de Zwart LL, Rompelberg CJM, Sips AJAM, WelinkJ, van Engelen JGM. 1999. Anatomical and phy-siological differences between various species usedin studies on the pharmacokinetics and toxicologyof xenobiotics. A. review of literature. RIVM Rap-port 623860010. http://www.rivm.nl/bibliotheek/rapporten/623860010.pdf, Accessed 3-18-2008.
51. Kamba M, Seta Y, Kusai A, Nishimura K. 2001.Evaluation of the mechanical destructive force inthe stomach of dog. Int J Pharm 228:209–217.
52. Kamba M, Seta Y, Kusai A, Ikeda M, Nishimura K.2000. A unique dosage form to evaluate themechanical destructive force in the gastrointestinaltract. Int J Pharm 208:61–70.
53. Klausner EA, Lavy E, Stepensky D, Friedman M,Hoffman A. 2002. Novel gastroretentive dosage
JOURNAL OF PHARMACEUTICAL SCIENCES, VOL. 98, NO. 3, MARCH 2009
forms: Evaluation of gastroretentivity and its effecton riboflavin absorption in dogs. Pharm Res 19:1516–1523.
54. Kaniwa N, Ogata H, Aoyagi N, Ejima A, TakahashiT, Uezono Y, Imasato Y. 1991. Bioavailability ofcyclandelate from capsules in beagle dogs and dis-solution rate: Correlations with bioavailability inhumans. J Pharmacobio-dyn 14:152–160.
55. Aoyagi N, Ogata H, Kaniwa N, Ejima A, Nakata H,Tsutsumi J, Fujita T, Amada I. 1985. Bioavaila-bility of indomethacin capsules in humans (III):Correlation with bioavailability in beagle dogs.Int J Clin Pharmacol Ther Toxicol 23:578–584.
56. Aoyagi N, Ogata H, Kaniwa N, Koibuchi M, Shiba-zaki T, Ejima A, Tamaki N, Kamimura H, KatougiY, Omi Y. 1982. Bioavailability of griseofulvin fromtablets in beagle dogs and correlation with dissolu-tion rate and bioavailability in humans. J PharmSci 71:1169–1172.
57. Bach JE, Kukanich B, Papich MG, McKiernan BC.2004. Evaluation of the bioavailability and phar-macokinetics of two extended-release theophyllineformulations in dogs. J Am Vet Med Assoc 224:1113–1119.
58. Rocca JG, Park K. 2004. Oral drug delivery: Pro-spects and challenges. Drug Delivery Technologies.Volume 4, #4, http://www.drugdeliverytech.com/cgi-bin/articles.cgi?idArticle¼237, Accessed 03-18-08.
59. Klausner EA, Eyal S, Lavy E, Friedman M, Hoff-man A. 2003. Novel levodopa gastroretentivedosage form: In-vivo evaluation in dogs. J ControlRelease 88:117–126.
60. Baumgartner S, Kristel J, Vreer F, Vodopivec P,Zorko B. 2000. Optimisation of floating matrixtablets and evaluation of their gastric residencetime. Int J Pharm 195:125–135.
61. Gue M, Peeters T, Depoortere I, Vantrappen G,Bueno L. 1989. Stress-induced changes in gastricemptying, postprandial motility, and plasmagut hormone levels in dogs. Gastroenterology 97:1101–1107.
62. Mistiaen W, Blockx P, Van Hee R, Bortier H, Har-risson F. 2002. The effect of stress on gastric empty-ing rate measured with a radionuclide tracer.Hepatogastroenterology 49:1457–1460.
63. Fix A, Cargill R, Engle K. 1993. Controlled gastricemptying. III. Gastric residence time of a nondisin-tegrating geometric shape in human volunteers.Pharm Res 10:1087–1089.
64. Burger DM, Wiestner T, Hubler M, Binder H, Kei-ser M, Arnold S. 2006. Effect of anticholinergics(atropine, glycopyrrolate) and prokinetics (metoclo-pramide, cisapride) on gastric motility in beaglesand labrador retrievers. J Vet Med A Physiol PatholClin Med 53:97–107.
DOI 10.1002/jps