Embed Size (px)
Citation preview
GCMAS at the AACPDM, October 21, 2015 Lecture #1: Getting Started 1
New Frontiers: The Role of Motion Analysis in
“Other” Neuromuscular Disabilities
Faculty
Sylvia Õunpuu MSc and Kristan Pierz MD
Connecticut Children’s Medical Center, Farmington, CT
University of Connecticut, Farmington, CT
Haluk Altiok MD and Joseph Krzak PhD PT
Shriners Hospitals for Children, Chicago, Il and
Midwestern University, Downers Grove, IL
Kirsten Tulchin-Francis PhD
Texas Scottish Rite Hospital, Dallas, TX
Kent Heberer MS, Susan Sienko PhD and Michael Sussman MD
Shriner’s Hospitals for Children, Portland, OR and
University of California, Los Angeles, CA
Purpose
• Highlight the role of motion analysis in
understanding complex gait disorders
– Charcot-Marie-Tooth
– Myelomeningocele
– Familial Spastic Paraplegia
– Duchene’s Muscular Dystrophy
• Draw on the following – Clinical experience
– Research
– Case studies

GCMAS at the AACPDM, October 21, 2015 Lecture #1: Getting Started 2
Learning Objectives
• Appreciate limitations of a visual assessment
in understanding gait pathology
• Describe the typical gait patterns characteristic
of a variety of neuromuscular disorders
• Understand the gait indications for specific
treatment options
• Identify “new frontiers” in motion analysis and
how these may influence understanding and
treatment of neuromuscular disorders
Outline
• Setting the Stage
• Charcot-Marie-Tooth
• Myelomeningocele
• Familial Spastic Paraplegia
• Duchene’s Muscular Dystrophy
Setting the Stage
Sylvia Õunpuu, MSc
Center for Motion Analysis
Division of Orthopaedics
Connecticut Children’s Medical Center
Farmington, Connecticut

GCMAS at the AACPDM, October 21, 2015 Lecture #1: Getting Started 3
Disclosure Information
AACPDM 69th Annual Meeting | October 21-24, 2015
Speaker Name: Sylvia Õunpuu, MSc
Disclosure of Relevant Financial Relationships
I have no financial relationships to disclose.
Disclosure of Off-Label and/or investigative uses:
I will not discuss off label use and/or investigational use in this presentation.
Outline
• Definition of Gait Analysis
• Why we need Gait Analysis
• Orientation to Gait Data
Gait Analysis – what is it?
• Systematic and Objective Documentation of Human Locomotion
– kinematics/kinetics/EMG, etc.
• Why?
– Improve understanding of pathomechanics
– Determine causes of gait abnormalities
– Define treatment – based on objective data
– Evaluate treatment – based on objective data
– This level of documentation and understanding is NOT possible in the clinic
GCMAS at the AACPDM, October 21, 2015 Lecture #1: Getting Started 4
Why Important?
• We can be fooled by what we see…
• Provides us additional information we cannot
see…
• Efficient form of documentation
• Objective
• Outcomes evaluation tool
• Provides a systematic approach for treatment
decision-making
Is the clinic appointment enough?
• Pathological
gait =
atypical joint
motion and
position
• Assumption
= What
someone
looks like =
their joint
kinematics
Joint Motion = Visual Impression
GCMAS at the AACPDM, October 21, 2015 Lecture #1: Getting Started 5
Joint Motion vs. Visual Impression?
• Can be inconsistent
• One of the reasons why 3D gait analysis is
so important
Documentation of Change over Time
• Objective comparison of
kinematic, kinetic, EMG
and foot pressures
changes over time
• Provides evidence of
decline
• Provides further
evidence for need for
intervention
2007 2010
Treatment Decision-Making
• Framework
– Prerequisites of typical gait - which are
compromised? (discussed next lecture)
– Impairments – documented
– Link impairments to movement pathology
(kinematics and kinetics)
– Propose treatment
• Indications and expected outcomes
– Evaluate treatment outcomes objectively
GCMAS at the AACPDM, October 21, 2015 Lecture #1: Getting Started 6
Surgical Decision-Making
• Left rectus femoris procedure - indications
– Rectus femoris spasticity – clinical examination
– Decreased peak knee flexion at in swing – kinematics
– Delayed peak knee flexion in swing – kinematics
– Rectus femoris activity in swing – EMG data
Surgical Decision-Making
• Left rectus femoris transfer - indications
– Rectus femoris spasticity – clinical examination
– Decreased peak knee flexion at in swing – kinematics
– Delayed peak knee flexion in swing – kinematics
– Rectus femoris activity in swing – EMG data
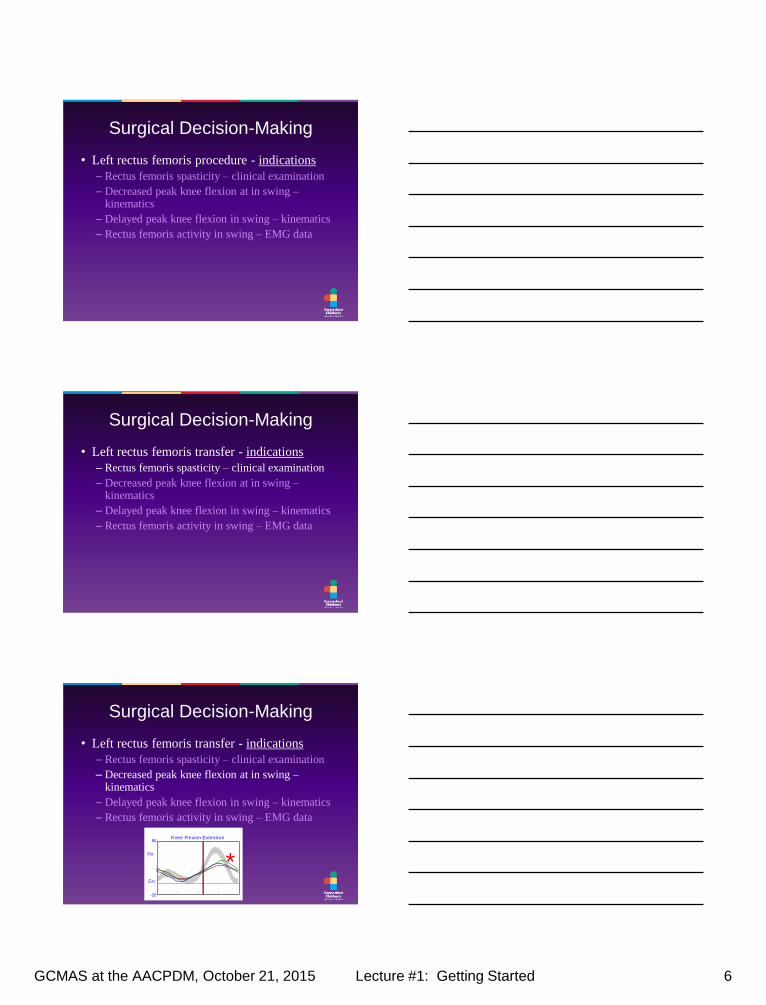
Surgical Decision-Making
• Left rectus femoris transfer - indications
– Rectus femoris spasticity – clinical examination
– Decreased peak knee flexion at in swing – kinematics
– Delayed peak knee flexion in swing – kinematics
– Rectus femoris activity in swing – EMG data
149595M02 Left (10/2/1997) 149595M03 Left (10/2/1997) 149595M04 Left (10/2/1997)
Trunk Obliquity30
-30
Up
Dn
deg
Pelvic Obliquity20
-20
Up
Dn
deg
Hip Ab-Adduction20
-20
Add
Abd
deg
Knee Varus-Valgus
Gait Cycle
30
-30
Var
Val
deg
25% 50% 75%
Trunk Tilt40
-20
Ant
Pos
Pelvic Tilt40
-20
Ant
Pos
Hip Flexion-Extension60
-20
Flx
Ext
Knee Flexion-Extension80
-20
Flx
Ext
Plantar-Dorsiflexion
Gait Cycle
40
-40
Dor
Pla
deg
25% 50% 75%
Trunk Rotation40
-40
Int
Ext
Pelvic Rotation40
-40
Int
Ext
Hip Rotation40
-40
Int
Ext
Knee Rotation40
-40
Int
Ext
Foot Progression
Gait Cycle
40
-40
Int
Ext
25% 50% 75%
*
GCMAS at the AACPDM, October 21, 2015 Lecture #1: Getting Started 7
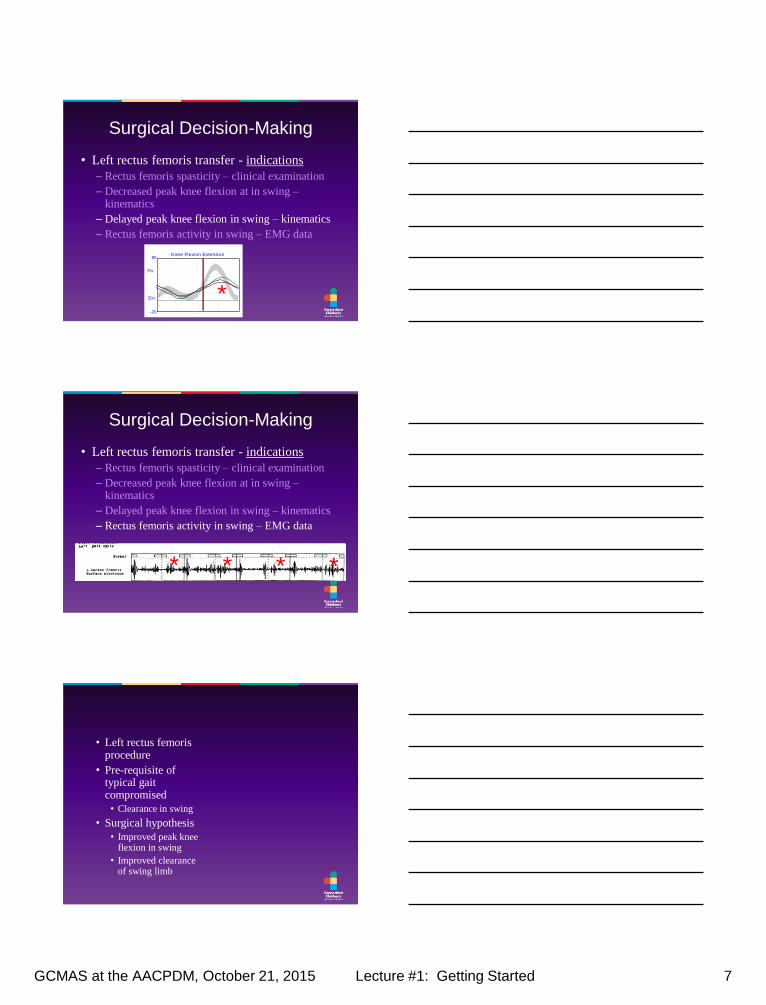
Surgical Decision-Making
• Left rectus femoris transfer - indications
– Rectus femoris spasticity – clinical examination
– Decreased peak knee flexion at in swing – kinematics
– Delayed peak knee flexion in swing – kinematics
– Rectus femoris activity in swing – EMG data
149595M02 Left (10/2/1997) 149595M03 Left (10/2/1997) 149595M04 Left (10/2/1997)
Trunk Obliquity30
-30
Up
Dn
deg
Pelvic Obliquity20
-20
Up
Dn
deg
Hip Ab-Adduction20
-20
Add
Abd
deg
Knee Varus-Valgus
Gait Cycle
30
-30
Var
Val
deg
25% 50% 75%
Trunk Tilt40
-20
Ant
Pos
Pelvic Tilt40
-20
Ant
Pos
Hip Flexion-Extension60
-20
Flx
Ext
Knee Flexion-Extension80
-20
Flx
Ext
Plantar-Dorsiflexion
Gait Cycle
40
-40
Dor
Pla
deg
25% 50% 75%
Trunk Rotation40
-40
Int
Ext
Pelvic Rotation40
-40
Int
Ext
Hip Rotation40
-40
Int
Ext
Knee Rotation40
-40
Int
Ext
Foot Progression
Gait Cycle
40
-40
Int
Ext
25% 50% 75%
*
Surgical Decision-Making
• Left rectus femoris transfer - indications
– Rectus femoris spasticity – clinical examination
– Decreased peak knee flexion at in swing – kinematics
– Delayed peak knee flexion in swing – kinematics
– Rectus femoris activity in swing – EMG data
* * * *
• Left rectus femoris procedure
• Pre-requisite of typical gait compromised
• Clearance in swing
• Surgical hypothesis
• Improved peak knee flexion in swing
• Improved clearance of swing limb
GCMAS at the AACPDM, October 21, 2015 Lecture #1: Getting Started 8
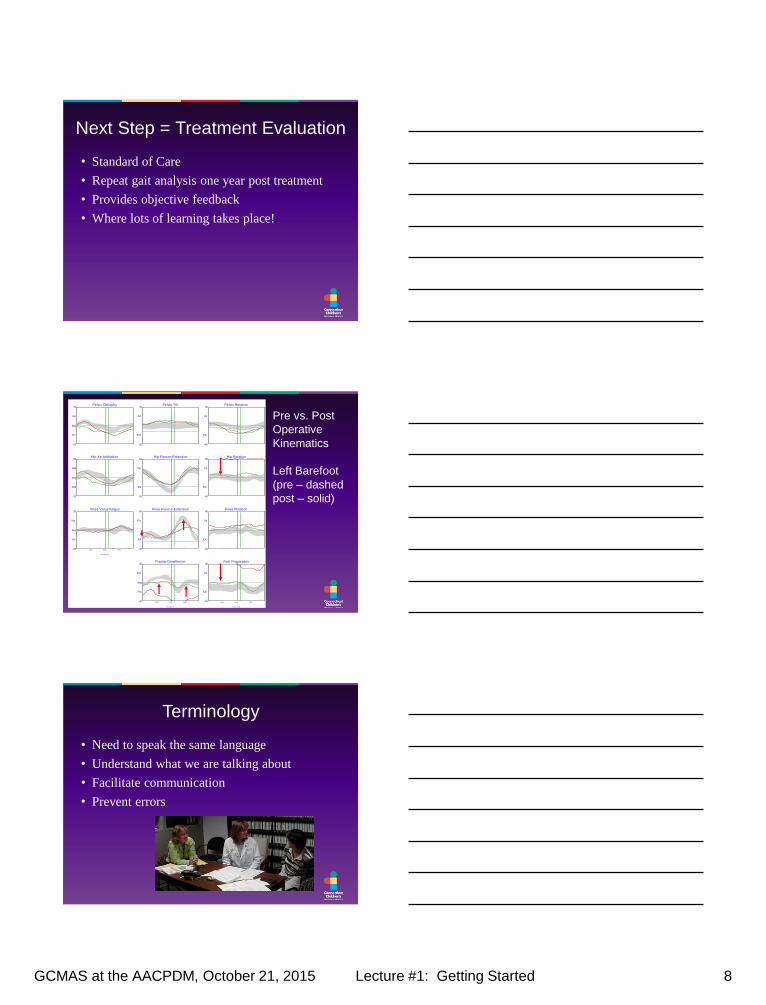
Next Step = Treatment Evaluation
• Standard of Care
• Repeat gait analysis one year post treatment
• Provides objective feedback
• Where lots of learning takes place!
Pre vs. Post
Operative
Kinematics
Left Barefoot
(pre – dashed
post – solid)
149595M25 Left (1/21/1999) 149595M02 Left (10/2/1997)
Trunk Obliquity30
-30
Up
Dn
deg
Pelvic Obliquity20
-20
Up
Dn
deg
Hip Ab-Adduction20
-20
Add
Abd
deg
Knee Varus-Valgus
Gait Cycle
30
-30
Var
Val
deg
25% 50% 75%
Trunk Tilt40
-20
Ant
Pos
Pelvic Tilt40
-20
Ant
Pos
Hip Flexion-Extension60
-20
Flx
Ext
Knee Flexion-Extension80
-20
Flx
Ext
Plantar-Dorsiflexion
Gait Cycle
40
-40
Dor
Pla
deg
25% 50% 75%
Trunk Rotation40
-40
Int
Ext
Pelvic Rotation40
-40
Int
Ext
Hip Rotation40
-40
Int
Ext
Knee Rotation40
-40
Int
Ext
Foot Progression
Gait Cycle
40
-40
Int
Ext
25% 50% 75%
Terminology
• Need to speak the same language
• Understand what we are talking about
• Facilitate communication
• Prevent errors
GCMAS at the AACPDM, October 21, 2015 Lecture #1: Getting Started 9
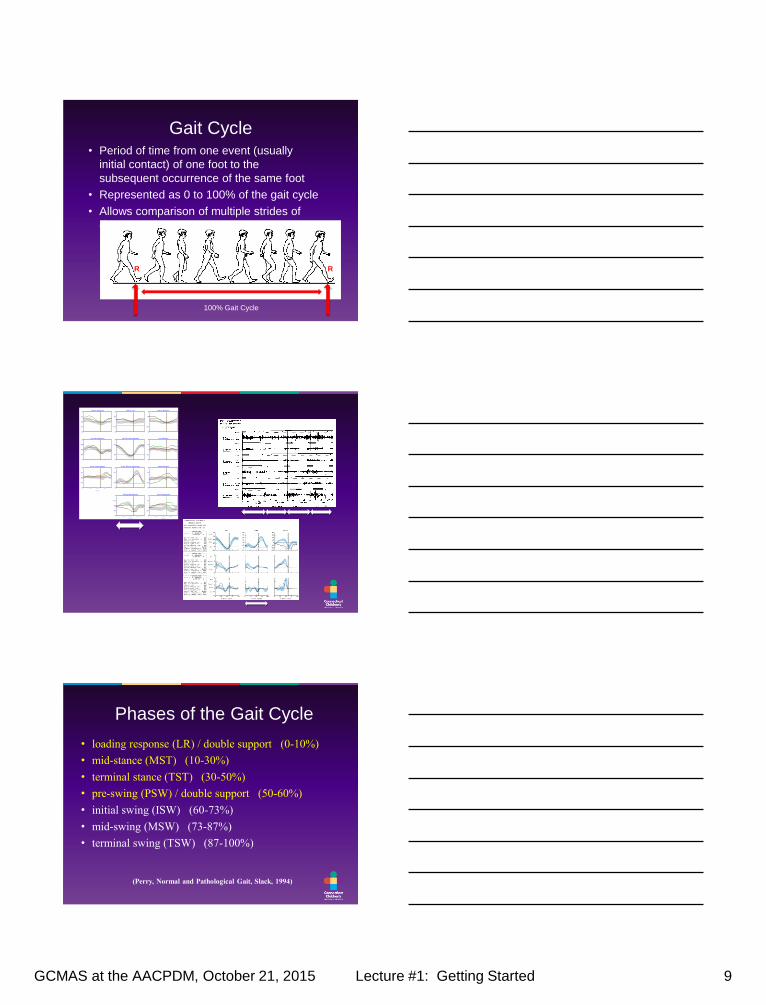
Gait Cycle • Period of time from one event (usually
initial contact) of one foot to the
subsequent occurrence of the same foot
• Represented as 0 to 100% of the gait cycle
• Allows comparison of multiple strides of
data
100% Gait Cycle
R R
149595M25 Right (1/21/1999) 149595M02 Right (10/2/1997)
Trunk Obliquity30
-30
Up
Dn
deg
Pelvic Obliquity20
-20
Up
Dn
deg
Hip Ab-Adduction20
-20
Add
Abd
deg
Knee Varus-Valgus
Gait Cycle
30
-30
Var
Val
deg
25% 50% 75%
Trunk Tilt40
-20
Ant
Pos
Pelvic Tilt40
-20
Ant
Pos
Hip Flexion-Extension60
-20
Flx
Ext
Knee Flexion-Extension80
-20
Flx
Ext
Plantar-Dorsiflexion
Gait Cycle
40
-40
Dor
Pla
deg
25% 50% 75%
Trunk Rotation40
-40
Int
Ext
Pelvic Rotation40
-40
Int
Ext
Hip Rotation40
-40
Int
Ext
Knee Rotation40
-40
Int
Ext
Foot Progression
Gait Cycle
40
-40
Int
Ext
25% 50% 75%
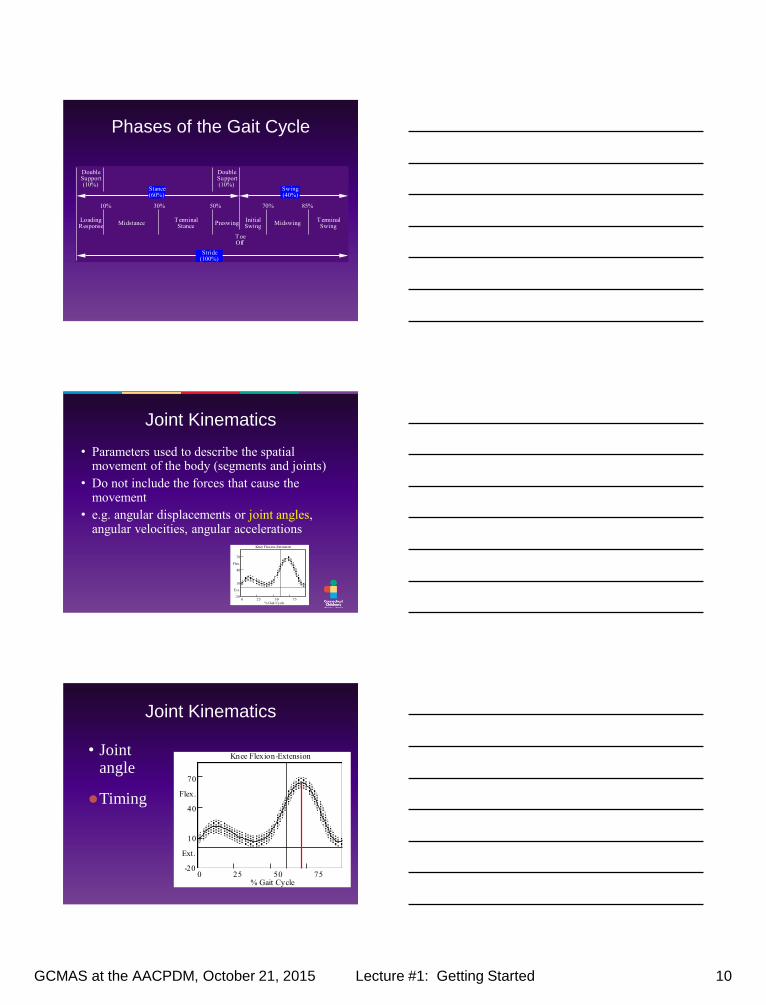
Phases of the Gait Cycle
• loading response (LR) / double support (0-10%)
• mid-stance (MST) (10-30%)
• terminal stance (TST) (30-50%)
• pre-swing (PSW) / double support (50-60%)
• initial swing (ISW) (60-73%)
• mid-swing (MSW) (73-87%)
• terminal swing (TSW) (87-100%)
(Perry, Normal and Pathological Gait, Slack, 1994)
GCMAS at the AACPDM, October 21, 2015 Lecture #1: Getting Started 10
Phases of the Gait Cycle
Loading Response
MidstanceT erminal Stance
PreswingInitial Swing
MidswingT erminal Swing
Stance (60%)
Swing (40%)
Stride (100%)
10% 30% 50% 70% 85%
T oe Off
Double Support (10%)
Double Support (10%)
Joint Kinematics
• Parameters used to describe the spatial movement of the body (segments and joints)
• Do not include the forces that cause the movement
• e.g. angular displacements or joint angles, angular velocities, angular accelerations
Knee Flexion-Extension
70
Flex.
40
10
Ext.
-200 25 50 75 100
% Gait Cycle
Joint Kinematics
• Joint angle
Knee Flexion-Extension
70
Flex.
40
10
Ext.
-200 25 50 75 100
% Gait Cycle
Timing
GCMAS at the AACPDM, October 21, 2015 Lecture #1: Getting Started 11
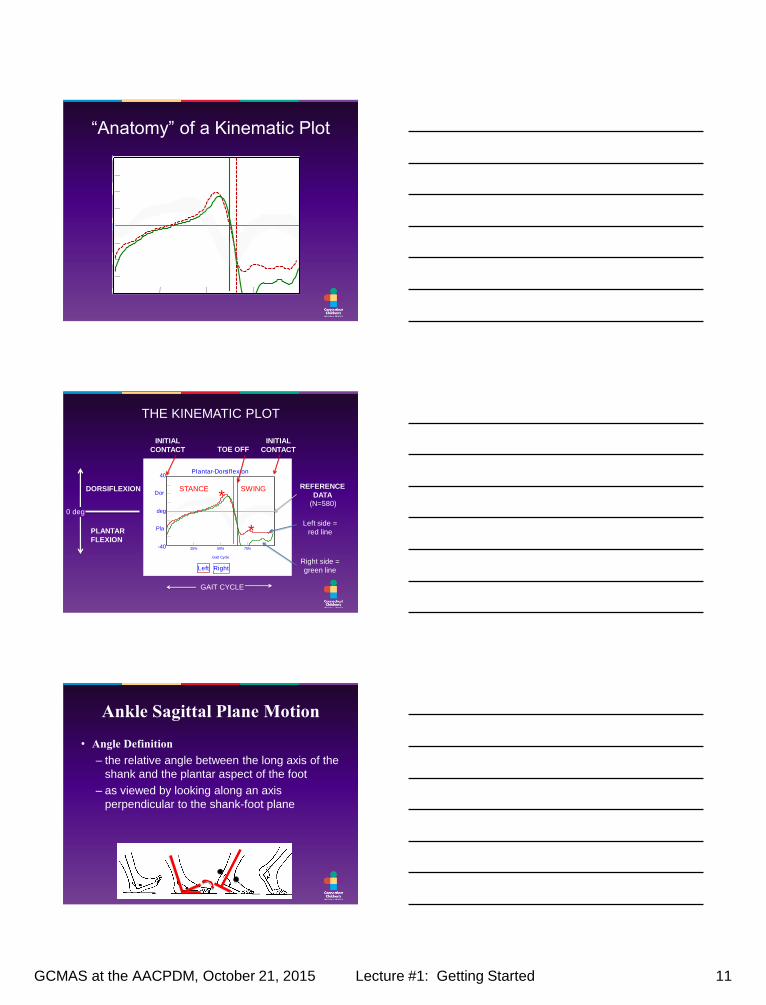
“Anatomy” of a Kinematic Plot
Left Right
Plantar-Dorsiflexion
Gait Cycle
40
-40
Dor
Pla
deg
25% 50% 75%
Left Right
Plantar-Dorsiflexion
Gait Cycle
40
-40
Dor
Pla
deg
25% 50% 75%
STANCE SWING DORSIFLEXION
PLANTAR
FLEXION
THE KINEMATIC PLOT
TOE OFF INITIAL
CONTACT
INITIAL
CONTACT
GAIT CYCLE
Right side =
green line
Left side =
red line *
* REFERENCE
DATA (N=580)
0 deg
Ankle Sagittal Plane Motion
• Angle Definition
– the relative angle between the long axis of the
shank and the plantar aspect of the foot
– as viewed by looking along an axis
perpendicular to the shank-foot plane
GCMAS at the AACPDM, October 21, 2015 Lecture #1: Getting Started 12
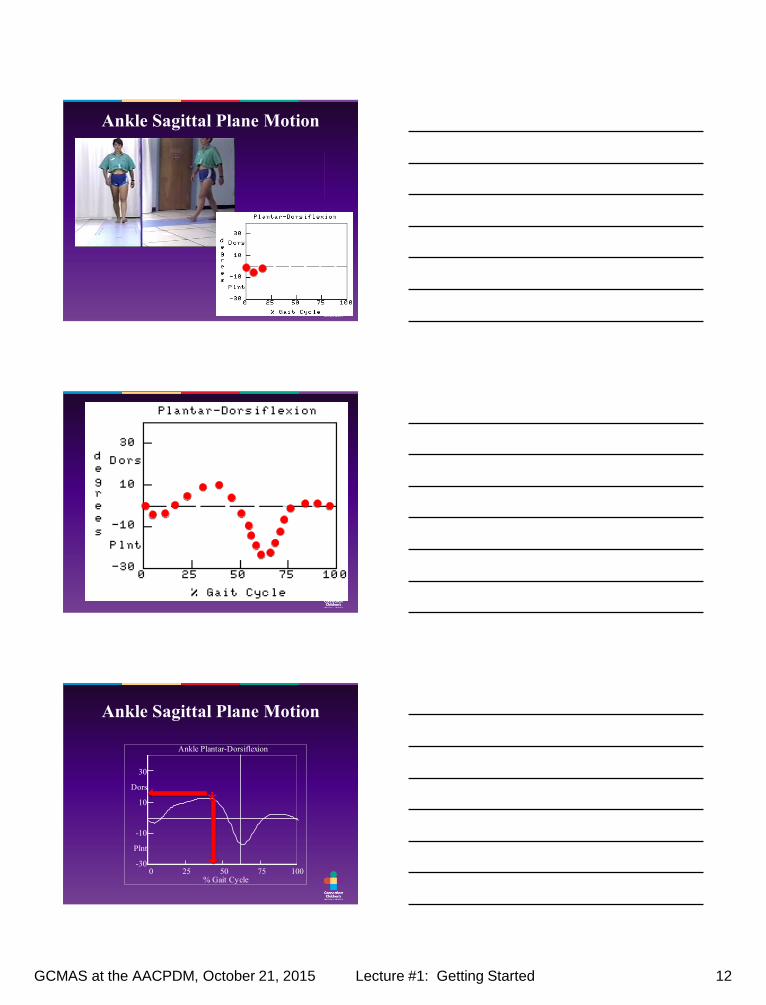
Ankle Sagittal Plane Motion
Ankle Sagittal Plane Motion
0 25 50 75 100 % Gait Cycle
Ankle Plantar-Dorsiflexion
30
Dors
10
-10
Plnt
-30
*
GCMAS at the AACPDM, October 21, 2015 Lecture #1: Getting Started 13
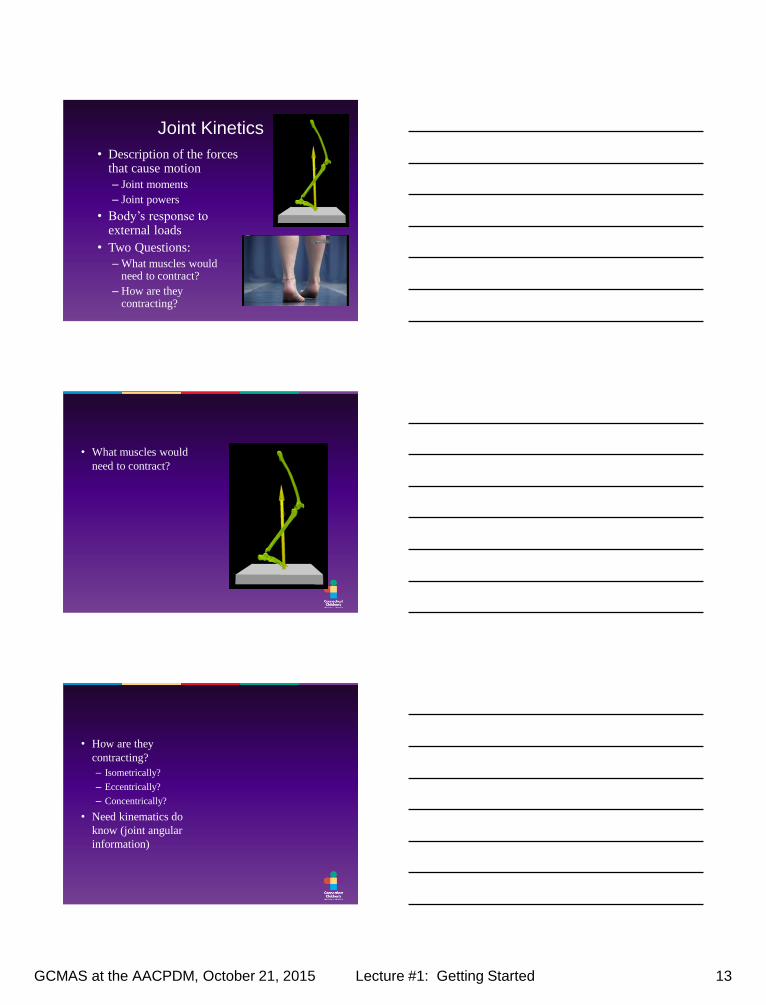
Joint Kinetics
• Description of the forces that cause motion
– Joint moments
– Joint powers
• Body’s response to external loads
• Two Questions:
– What muscles would need to contract?
– How are they contracting?
• What muscles would
need to contract?
• How are they
contracting?
– Isometrically?
– Eccentrically?
– Concentrically?
• Need kinematics do
know (joint angular
information)
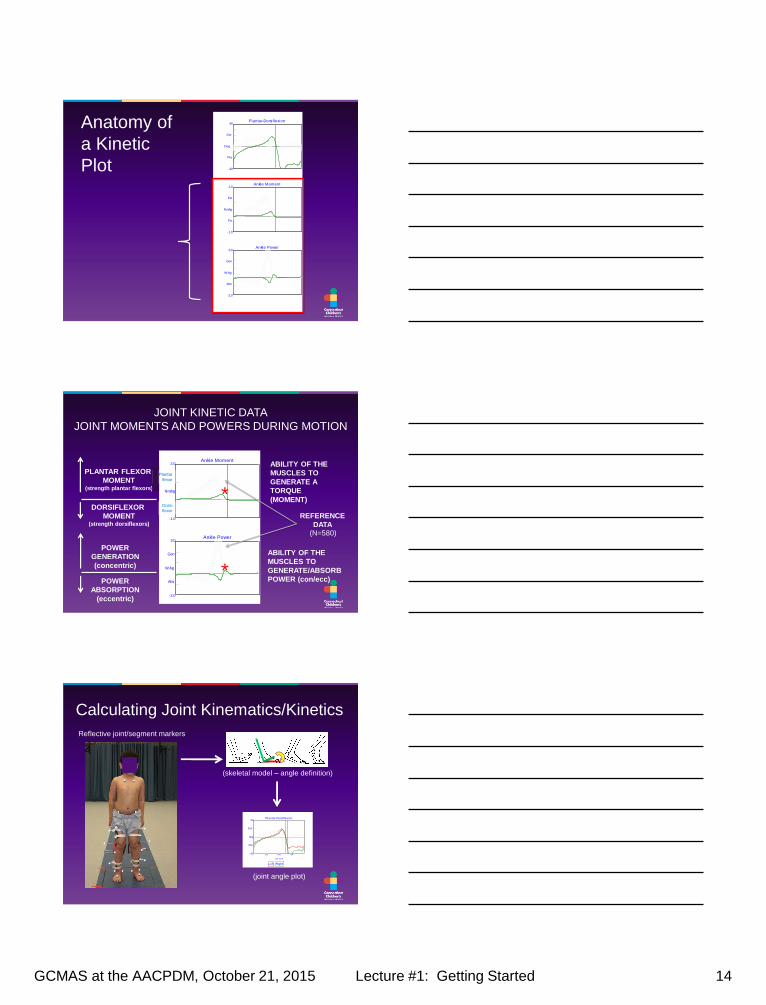
GCMAS at the AACPDM, October 21, 2015 Lecture #1: Getting Started 14
Anatomy of
a Kinetic
Plot
Left Right
Plantar-Dorsiflexion40
-40
Dor
Pla
Deg
Ankle Moment2.0
-1.0
Ext
Flx
Nm/kg
Ankle Power3.0
-2.0
Gen
Abs
W /kg
JOINT KINETIC DATA
JOINT MOMENTS AND POWERS DURING MOTION
Left Right
Plantar-Dorsiflexion40
-40
Dor
Pla
Deg
Ankle Moment2.0
-1.0
Ext
Flx
Nm/kg
Ankle Power3.0
-2.0
Gen
Abs
W /kg
ABILITY OF THE
MUSCLES TO
GENERATE A
TORQUE
(MOMENT)
ABILITY OF THE
MUSCLES TO
GENERATE/ABSORB
POWER (con/ecc)
*
*
PLANTAR FLEXOR
MOMENT (strength plantar flexors)
DORSIFLEXOR
MOMENT (strength dorsiflexors)
POWER
ABSORPTION
(eccentric)
POWER
GENERATION
(concentric)
REFERENCE
DATA (N=580)
Dorsi
flexor
Plantar
flexor
Calculating Joint Kinematics/Kinetics
Left Right
Plantar-Dorsiflexion
Gait Cycle
40
-40
Dor
Pla
deg
25% 50% 75%
(joint angle plot)
Reflective joint/segment markers
(skeletal model – angle definition)
GCMAS at the AACPDM, October 21, 2015 Lecture #1: Getting Started 15
Summary
• Comprehensive motion analysis provides a
wealth of information to improve our
understanding movement pathology
• Gaining the knowledge needed to interpret
motion analysis data is worth the effort!
Benefits of this Approach
• Comprehensive and objective patient
assessment using motion analysis
• Treating all gait related issues at one point in
time
– Single surgery and rehabilitation (time/cost)
– Maximizing patient specific outcomes
• Ability to learn from experience and objective
documentation of outcomes
Thank You