Embed Size (px)
Citation preview

1
Failure Modes and Effects Analysis
Click to add text
2
Failure Modes and Effects Analysis (FMEA)● Purpose
– Systematically, prospectively, identify ways in which a process (system) can fail: Failure Modes.
– Identify factors potentially contributing to failures.– Estimate risk of failure– Identify countermeasures– Develop requirements
● Method (WSE workbook 2.0)– Copy IDEF0 model nodelist into WSE [Overview] worksheet– Select task on which to perform FMEA– Prepare task FMEA worksheet from [FMEA template] worksheet
● copy [FMEA template] worksheet● copy/type task name into upper left cell● rename new task FMEA worksheet to task's A-number
– Perform FMEA

3
PRIS IDEF0 Model Nodes in WSE Workbook
4
PRIS FMEA in WSE Workbook

5
FMEA Fields● Contributing Factors
– Circumstances, conditions, events, factors, ... anything that might make a failure mode more likely.
● Potential Failure Mode– A way in which the process/system can fail:
● human error (see below)● acute injury (e.g., cut, broken bone)● cumulative injury (e.g., carpal tunnel syndrome)● likely and significant equipment/tool failure● etc.
● Potential Effects of Failure Mode– Consequences of the failure.
6
FMEA Fields (2)● Severity
– Numeric rating of the estimated severity of consequences, of the failure, e.g.,
● negligible● minor● moderate● major● catastrophic
● Probability– Numeric rating of the estimated probability that the failure will
occur, e.g.,1. Remote2. Unlikely3. Occasional4. Common5. Frequent

7
FMEA Fields (3)● Nondetectability
– Numeric rating of the difficulty of detecting the failure in time to prevent or mitigate its consequences, e.g.,
1.Should the failure occur, there is a virtual certainty that the existing controls will detect it.
2.Very high3.Should the failure occur there is a high probability that the existing
controls will detect it.4.Moderately high5.Existing controls have difficulty detecting the failure6.Low7.Controls are weak. Detection could depend on a lucky catch.8.Remote9.Very remote10.No controls for this failure mode exist
● RPN: Risk Priority Number– RPN = Probability x Severity x Nondetectability
8
FMEA Fields (4)● Potential Remediations
– Design strategies that could reduce the likelihood of the failure mode.
● Design Requirements– Abbreviated requirements statements for remediations.– Requirement numbers ([Requirements] worksheet).
9
Chapter 17 Human Error Click to add text
10
IE 366
Human Error in the
● Cockpit
● Operating Room

11
IE 366
China Eastern Airlines Flight 583
Copyright Anthony Cheng, used with permission, downloaded from http://www.airliners.net/open.file/610387/M/ 30 Jun 04
12
IE 366
MD-11 Cockpit
Copyright Harri Koskinen, used with permission, downloaded from http://www.airliners.net/open.file/463667/M/ 30 Jun 04

13
IE 366
China Eastern Airlines Flight 583● Background
– McDonnell Douglas MD-11– 6 April 1993– Beijing → Los Angeles– 235 passengers, 20 crew on board
● Conditions– 950 nmi S of Shemya, Alaska– 33,000 ft MSL– 298 kt
● Events– inadvertent deployment of leading edge wing slats– series of violent oscillations– diverted to USAFB Shemya
14
IE 366
China Eastern Airlines Flight 583 (continued)● Consequences
– 2 passengers fatally injured– 53 passengers, 7 crew seriously injured– 96 passengers with minor injuries– passenger cabin substantially damaged
● NTSB Findings– deficient flap/slat handle design– captain (in right seat) inadvertently moved flap/slat handle while making
corrections to MCDU● Interpretation
– System factors• highly mode-sensitive control• positive control bias• inadequate protection against inadvertent operation• proximity to other control
– Human factors• limits to motor accuracy• inability to divide attention/distraction• cost of concurrence
15
IE 366
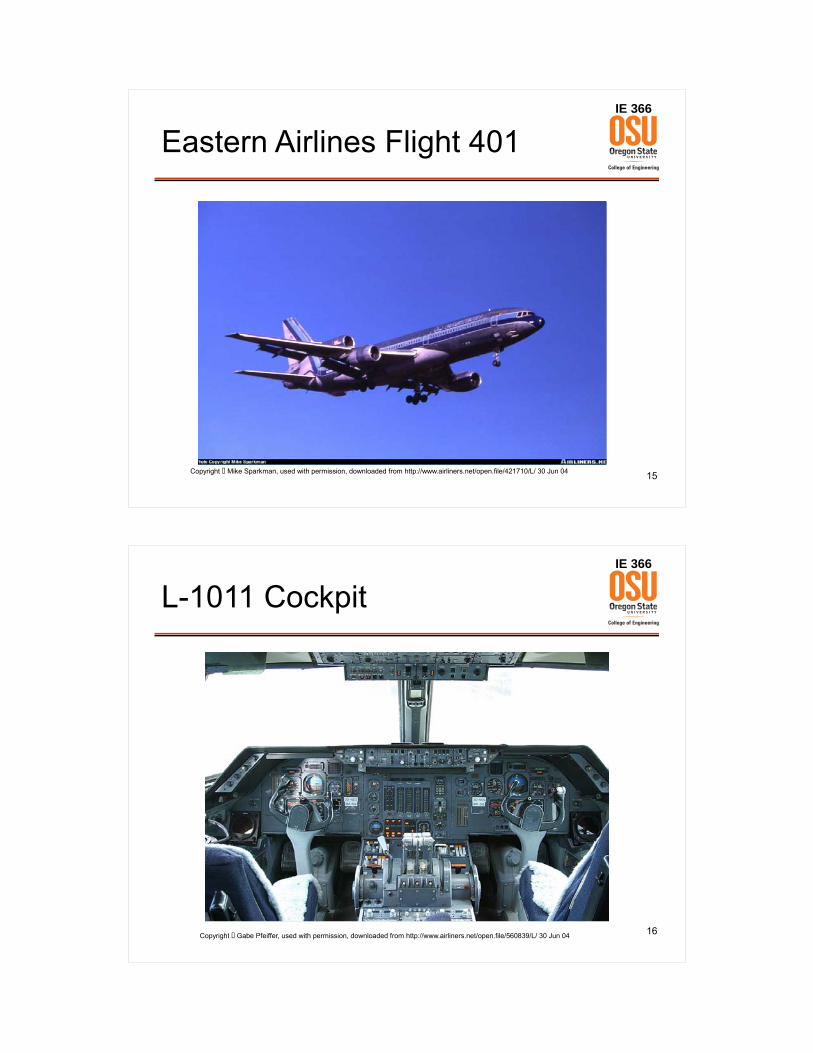
Eastern Airlines Flight 401
Copyright Mike Sparkman, used with permission, downloaded from http://www.airliners.net/open.file/421710/L/ 30 Jun 04
16
IE 366
L-1011 Cockpit
Copyright Gabe Pfeiffer, used with permission, downloaded from http://www.airliners.net/open.file/560839/L/ 30 Jun 04

17
IE 366
Eastern Airlines Flight 401● Background
– Lockheed L-1011– 29 December 1972– JFK → Miami– 163 passengers, 13 crew on board
● Conditions– approaching Miami– < 2,000 ft MSL
● Events– landing gear handle down, nose gear green light failed to illuminate– climbed to 2,000 ft, set autopilot– entire flightcrew + observer tried to diagnose problem
• mechanical indicator in electronics bay• nose gear light
– began gradual descent– crashed into Everglades
18
IE 366
Eastern Airlines Flight 401 (continued)● Consequences
– 96 passengers, 5 crew fatally injured– 65 passengers, 10 crew non-fatally injured
● NTSB Findings– Flightcrew was
• pre-occupied with nose gear problem• distracted from monitoring instruments
– Captain failed to assure that someone was monitoring altitude● Interpretation
– System factors• susceptibility to minor malfunctions• low altitude• high speed• subtle autopilot behavior
– Human factors• inability to divide attention• stress-induced narrowing of attention

19
IE 366
4%
4%
5%
12%
14%
62%
0% 20% 40% 60% 80% 100%
Airport/ATC
Maintenance
Miscellaneous /Other
Weather
Airplane
Flightcrew
Human Error and Aviation Safety
Source: Boeing Commercial Airplanes
Primary Causes of Aircraft AccidentsHull Loss Accidents – Worldwide Commercial Jet Fleet – 1994 Through 2003
20
IE 366
Human Error and Operating Room Performance● Patient Safety
– Health Care, in general● 44,000 - 98,000 deaths in the US annually due to errors● 8th leading cause of death in US● Exceeds motor vehicle accident deaths, etc. ● $17 - $29 billion spent annually (Institute of Medicine,
2000)– In the hospital
● 3.7% of hospital admissions experience an adverse event
(Leape et al, 1991)– In the OR
● 41% of hospital adverse events occur in the OR

21
IE 366
Laparoscopy: Minimally Invasive Surgery of the Abdomen
Photo courtesy of Alex Gandsas, MD. Used with permission.
22
IE 366
Laparoscopy
Patient’sabdominalcavity
Overhead ViewSide View

23
IE 366
Laparoscopy: Trocar Injuries● Trocar should
– penetrate abdominal wall– just enter abdominal cavity
● Trocar may– penetrate too far– nick bowel (especially if adhesions present from previous surgery)– damage major blood vessels (especially aorta)
● Trocar injuries– US
● 10,000 trocar injuries ~1991 – 2001● 50 – 240 fatalities / year
– Europe● 1 injury / 1,000 surgeries (0.1%)● 1 fatality / 100,000 surgeries (0.001%)
24
IE 366Patient Mortality in US Laparoscopic Cholecystectomies, 1991-2000(source: Hunter, 2006)
Totals
Year All Laparoscopic Mortality (Laparoscopic)
19901991199219931994199519961997199819992000
494,541517,433506,980470,692465,703429,439428,901421,583406,817405,367431,605
N/A270,988 (52.37%) a
324,794 (64.06%)319,837 (67.95%)315,956 (67.84%)296,245 (68.98%)300,364 (70.03%)299,710 (71.09%)292,651 (71.94%)299,099 (73.78%)324,783 (75.25%)
N/A900 (0.33%) b
1,424 (0.44%)1,381 (0.43%)1,097 (0.35%)1,201 (0.41%)1,305 (0.43%)1,332 (0.44%)1,685 (0.58%)1,613 (0.54%)1,630 (0.50%)
N/A, Case volume not available due absence of specific ICD-9 code for LC or partial LC a LC volume projected for first 3 quarters of 1991, based on last quarter data b Mortality derived from last quarter 1991 data only

25
IE 366
Lessons Learned from Aviation and Medicine● Causes of Adverse Events
– Rarely• individual incompetence• lack of due diligence• bad luck
– Commonly• Vulnerable Systems*• Fallible Humans*
* from E.L. Wiener, “Fallible Humans and Vulnerable Systems: Lessons Learned from Aviation,” 1987
26
IE 366Human Fallibility + System Vulnerability → Human Error
● Human Error– an occasion “… in which a planned sequence of mental or physical
activities fails to achieve its intended outcome, and when these failures cannot be attributed to the intervention of some chance agency.”
– James Reason, Human Error● Broad Classes of Human Errors
– Planning Failures: Mistakes• inappropriate plan, misdirected intention• plan carried out as intended• e.g., wrong medication prescribed & administered
– Execution Failures• Slips
– appropriate plan, intention– part of plan performed incorrectly– e.g., trocar injury
• Lapses– appropriate plan, intention– part of plan omitted– e.g., forget to remove sponge before closing




33
IE 366
Reducing Human Error in the Cockpit● Universality of pilot error widely acknowledged.● Most pilot error due to innate human fallibility.● Contribution of pilot error to aircraft accidents well understood.● Pilot error anticipated, prevented, mitigated.● Countermeasures, e.g.,
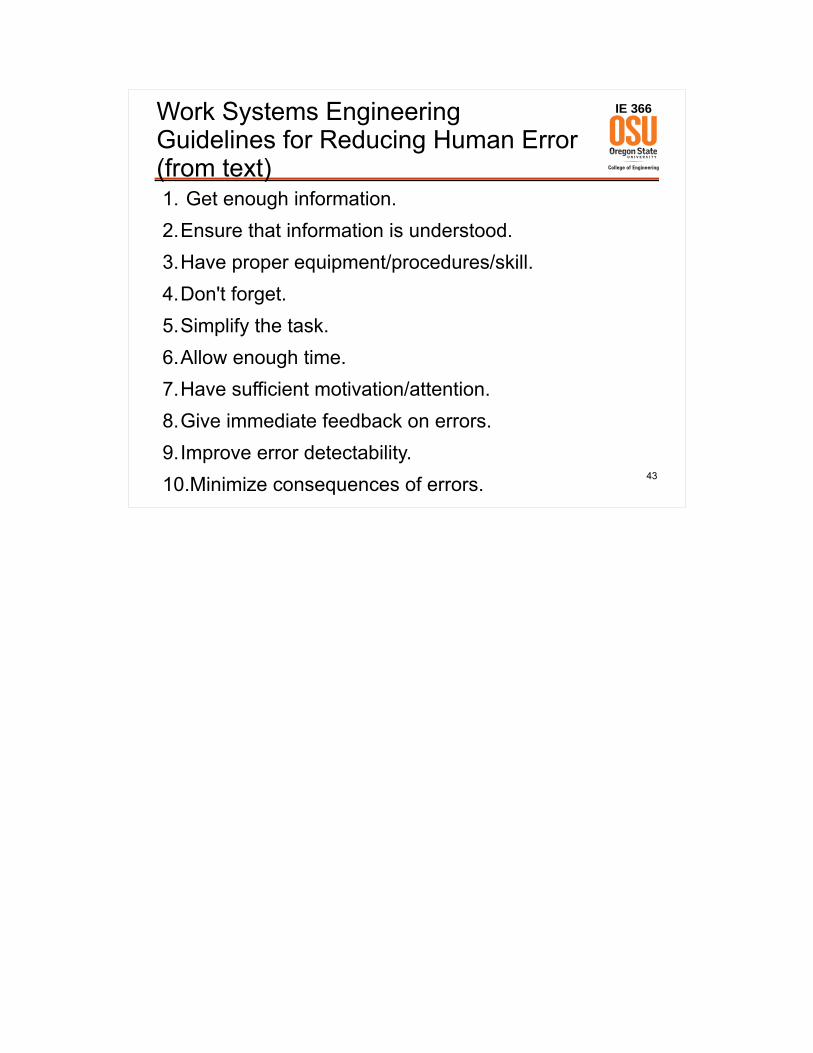
– pointer/counter altimeter– moving “tape” altimeter– moving map display– checklists– other mnemonics (memory aids)– Crew Resource Management (CRM) training
34
IE 366
Three-Pointer Altimeter
5
7
6
8
9
01
2
3
4

35
IE 366
Pointer-Counter Altimeter
5
7
6
8
9
01
2
3
4
7 8 03 1
36
IE 366
Moving Tape Altimeter
37
IE 366
Moving Map Display
38
IE 366
Checklistse.g., Boeing 757

39
IE 366
Other Mnemonics(Memory Aids)
● Before-Landing Mnemonic: GUMPS
– Gas (fuel system configuration)– Undercarriage (landing gear down)– Mixture (engine fuel/air mixture)– Props (propeller pitch)– Systems (other system settings)
40
IE 366
Crew Resource Management (CRM) Training● Communication / Interpersonal Skills● Situational Awareness● Problem Solving / Decision Making / Judgment● Leadership / “Followership” / Teamwork● Task Management● Stress Management● Critique

41
IE 366
Results(not attributable solely to Human Factors Engineering)
● Hull loss rate (per million departures)– 1959-1990: 1.91– 1994-2003: 0.96
● Hull loss accidents due to flightcrew error– 1959-1990: 75%– 1994-2003: 62%
42
IE 366
Human Factors Engineering Principles to Reduce Human Error
● Display Design Principles– Typography– Display Coding (color, size, location, ...)– Pictorial Realism
● Control Design Principles– Control Coding (type, location, size, shape, ...)– Movement Compatibility– Prevention of Inadvertent Activation
● Workstation Design Principles– Accessibility– Accommodation– Frequency of Use– Order of Use– Spatial Compatibility– Standardization
● Job Performance Aids– Mnemonics, Memory Aids– Checklists– Decision Aids– Computation Aids
and many more …
43
IE 366Work Systems Engineering Guidelines for Reducing Human Error (from text)1. Get enough information.2.Ensure that information is understood.3.Have proper equipment/procedures/skill.4.Don't forget.5.Simplify the task.6.Allow enough time.7.Have sufficient motivation/attention.8.Give immediate feedback on errors.9.Improve error detectability.10.Minimize consequences of errors.