Embed Size (px)
Citation preview

www.integrativeRD.orgFall 2011 Volume 14, Issue 2
ContentsCPE: The Gluten Connection....................................... 25
CPE Objectives and Questions......................................................30
Citicoline: a promising dietary supplement for preventing cognitive decline..................................... 32
The Uplifting Benefit of Downward Dog ................. 35
Resource Review................ 37
“SNiP” Update – Nutritional Genomics 2011 Conference Update. .................................................. 38.
Congratulations to 2010 DIFM
Award Winners ......................... 39
Annual Report .................... 41
Chair’s Corner .................... 41
Editor’s Notes ......................... 42
2010-2011 Leadership Contact Information ......... 43
Upcoming Issues• Winter 2012 Editor’s Deadline, Nov. 1, 2011• Spring 2012 Editor’s Deadline, Feb. 15, 2012• Summer 2012 Editor’s Deadline, April 15, 2012• Fall 2012 Editor’s Deadline, July 15, 2012
Fall 2011 Volume 14, Issue 2
Sheila Dean, DSc, RD, LD, CCN, CDE
It is well-established that a strict gluten-free diet can reverse the
symptoms associated with celiac disease
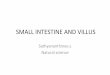
(CD), an autoimmune condition typically defined as a disease of the digestive system that damages the small intestine and interferes with the absorption of nutrients from food.1 Furthermore, for many years, it has been documented that the classical presentation of CD is diarrhea with or without a malabsorption syndrome demonstrated by wasting, edema secondary to hypoalbuminemia, hypocalcemia, vitamin deficiency states and osteomalacia.2 The diagnosis of CD requires the presence of small intestinal mucosal villous atrophy and crypt hyperplasia (Marsh III).3 Marsh type III lesions contain villous atrophy and are associated with typical CD pathology.
Figure 1 demonstrates normal duodenal mucosa with healthy villi (on left) versus atrophied villi of the duodenal mucosa in CD (on right).
Celiac Disease – A Clinical Chameleon CD is not a condition that occurs overnight. Evidence suggests that small bowel mucosal damage in CD progresses gradually from mucosal inflammation to crypt hyperplasia, and finally to partial and subtotal villous atrophy.4 However, as our understanding of CD continues to grow, it is becoming increasingly evident that CD may not always manifest as previously thought. It is now accepted that CD may be characterized by more subtle histological changes; in some subjects only epithelial infiltration may be present.4 In a 2005 paper by Sanders and colleagues in the British Medical Journal, the authors state, “CD used to be perceived as involving gastrointestinal symptoms suggestive of malabsorption, but this manner of presentation is now described as the classic (typical) form.” 5 Furthermore, the authors suggest that patients with CD may have the “silent” or atypical form – that is, without gastrointestinal symptoms — where the condition affects organs other than the small intestine, with manifestations such as altered thyroid function, skin abnormalities, bone disease, iron-deficiency anemia, and even neurological disorders, including depression, mood changes, migraines and inability to focus.5 As a result, one could potentially have CD but be free of the classic GI symptoms for years. More recently, the term “potential” or “latent” CD has been used to describe patients with sub-clinical pathology and other subtle immunological
CPE: The Gluten ConnectionThe Relationship between Celiac Disease and Type 1 Diabetes Mellitus
Image credit: Davidson College. Available at: http://www.bio.davidson.edu/courses/Immunology/Students/spring2006/Mohr/Villi%20Atrophy.jpg
Figure 1. Normal duodenal mucosa vs. duodenal mucosa in CD.
continued on page 28
This issue of the DIFM newsletter is made possible
by an unrestricted educational grant from
Kyowa Hakko USA, makers of Cognizin
and Sustamine.

Fall 2011 Volume 14, Issue 2www.integrativeRD.org
Page
26
abnormalities, such as celiac-like mucosal immunoglobulin pattern and increased density of intra-epithelial T cells, suggesting a significant risk of developing CD later in life.6
The “iceberg” is a common model used to explain the epidemiology of CD (see figure 2). Accordingly, only a minority of individuals has clinically overt CD, while the majority of people with CD have the silent form, which may go undiagnosed because they remain asymptomatic.6 This may explain earlier inaccurately low prevalence figures – 21.8 in 100,000, according to a 1994 study.7 By contrast, Fasano and colleagues found the overall prevalence rate of CD in the United States in not-at-risk groups to be closer to 1 in 133.8 Furthermore, “that gluten sensitivity is regarded as principally a disease of the small bowel is a historical misconception,” according to Hadjivassiliou and colleagues.9 As a result, many practitioners who are not familiar with the countless ways in which CD presents may miss the diagnosis and encourage the patient to continue eating wheat-based foods, per USDA government guidelines, thus making matters worse.
Rubio-Tapia and colleagues investigated the long-term outcome of undiagnosed CD and whether the prevalence of undiagnosed CD changed during the past 50 years. Their results indicate that undiagnosed CD was associated with a nearly four-fold increased risk of death, and the prevalence of undiagnosed CD increased dramatically in the United States during the past 50 years.10 More recently, Katz and colleagues reported that undiagnosed celiac disease affects 1 in 126 individuals and that most were asymptomatic or had atypical presentations.11
To demonstrate just how much of a “clinical chameleon” CD can be, the author of an editorial published in the New England Journal of Medicine
stated “Celiac disease is one of the most common lifelong disorders in both Europe and the United States. The clinical presentation of this condition can range from the typical syndrome of malabsorption (chronic diarrhea, weight loss and abdominal distention) to symptoms and conditions that can affect any organ system.”12 Furthermore,
for every symptomatic patient with CD, there are eight patients with CD who do not experience gastrointestinal symptoms,13 thus suggesting that CD “out of the intestine” is even more frequent than CD “within the intestine.”14
Gluten – The Instigator Gluten, a complex mixture of glutenin and gliadin protein molecules and the major storage protein of wheat, is the primary immune system instigator in CD. This includes the gluten present in all forms of wheat, including durum, semolina, spelt, kamut, malt, couscous, bulgur, triticale, einkorn and faro, as well as related grains, rye and barley.15 Although gliadin, the alcohol-soluble fraction of gluten, has been most studied, other proteins, such as glutenin, are probably also toxic to people who have CD.16 Furthermore, while certain complex carbohydrate-rich foods such as rice, buckwheat, corn, and millet do not contain gluten and are not specific
to CD etiology, they may contribute to escalating symptomatology in sensitive individuals by creating and sustaining an inflammatory response.15
Autoimmune Inflammatory Disease – The “Epidemic of Epidemics” Originally considered a rare malabsorption syndrome of childhood, CD is now recognized as a common
autoimmune condition that may be diagnosed at any age and may affect multiple organ systems.17 In fact, while many individual autoimmune diseases appear rare, collectively they are thought to affect approximately eight percent of the United States population.18 In a 2006 seminar entitled Understanding the Origins and Applying Advanced Nutritional Strategies for Autoimmune Diseases, Jeffrey Bland, Ph.D., explained that “collectively autoimmune diseases have been identified in about 24 million people in the United States, and only one-third are diagnosed.
That means about 72 million people have an autoimmune disease. It’s not looked for [during routine exams or even hospitalizations]. Our system waits until the signs and symptoms are severe enough, with organ failure and irreversible damage, before we identify it.”19 Autoimmune disorders can be classified as either organ-specific, such as Type 1 diabetes mellitus or Hashimoto’s thyroiditis, or systemic, such as CD, systemic lupus erythematous (SLE) and rheumatoid arthritis (RA).20 In a paper on celiac disease-associated autoimmune endocrinopathies, Kumar and associates state, “In organ-specific autoimmune diseases, the autoantibodies are specifically directed against antigens localized in a particular organ and are often detected in circulation.”20 The proposed mechanisms of autoimmune endocrine disease involve a sequence of immune, inflammatory events in a genetically susceptible individual. In most cases, the immune response to the target cell progressively destroys the
The Gluten Connection
Figure 2. Iceberg model depicting prevalence of CD.
Image credit: BMJ. 24 Jul 1999;319:236

Fall 2011 Volume 14, Issue 2www.integrativeRD.org
Page
27
endocrine gland, and hypofunction is the main clinical manifestation.21
The Celiac Disease and Type 1 Diabetes Mellitus Connection Indeed, several autoimmune disorders are more prevalent in CD patients and their close relatives. For this population, risk of developing other autoimmune diseases is related to the duration of exposure to gluten.22 The most frequently reported CD-associated conditions are type 1 diabetes mellitus (T1DM) and autoimmune thyroiditis.22 In fact, the association between CD and T1DM was recognized more than 30 years ago.23 After the introduction of serological antibody tests, such as antiendomysial and antigliadin antibodies, a number of studies have been carried out to assess the frequency of CD in patients with T1DM. Virtually all studies have shown an increased frequency of the disorder compared to that of the general population (0.5-1.0%).23 Statistics show that the prevalence of CD in people with T1DM is an astounding 10-30 times that found in the general population.20 Additionally, 3-8% of individuals who have T1DM have CD, while at least 5% of individuals who have CD have T1DM.20 Similar to those with silent CD, about one in 20 people with T1DM have asymptomatic CD but have not developed classic CD symptoms of the gut. 20
It is well-established that specific antibodies, glutamic acid decarboxylase (GAD) and islet cell antibodies (ICAs), are considered to be predictive markers of T1DM. Interestingly, in a review of associated autoantibodies in CD, at least one T1DM-related autoantibody was present in 11.1% of 90 CD subjects at diagnosis and resolved within 12 months on a gluten-free diet.22 In fact, in a 2002 article by Nelson published in the American Family of Physicians, T1DM was described as the most prevalent autoimmune disorder associated with CD followed by autoimmune thyroid disease.24 However, the question remains: What is the common
denominator between CD and T1DM? While they are both autoimmune diseases, the latter is organ-specific and the former is not. It appears that gluten consumption may be a shared causative factor, as both share a similar genetic basis. That is, both conditions have the same human leukocyte antigen (HLA), which genetically predisposes an individual to both CD and T1DM.25 A recent article by Barker and Liu confirms this connection. They state, “The HLA association with celiac disease is largely accountable for its link to other autoimmune diseases, including type 1 diabetes and autoimmune thyroid disease, and the majority of risk for celiac disease in these populations is related to HLA genotype. Celiac disease also carries an increased risk for type 1 diabetes and autoimmune thyroid disease.”26
Traditionally, children with T1DM also have an increased risk of CD, with T1DM coming first, followed by gluten intolerance. Furthermore, the prevalence of T1DM is related to the duration of exposure to gluten,27,28 and the older the patient is when diagnosed with CD, the higher the probability of being diagnosed with other autoimmune diseases. Therefore, it appears that the elimination of dietary gluten is associated with a lower frequency of T1DM. However, this is no longer the case when patients already reveal islet-autoantibodies and beta cell destruction.29 Collin and colleagues examined the influence of a strict gluten-free diet on the metabolic control of individuals with diabetes in a prospective, controlled one-year trial. Even though a definite improvement in adherence to the gluten-free diet was achieved in the celiac group, this had no effect on the metabolic control of diabetes.23 Moreover, the impact of a gluten-free diet on the metabolic control of diabetes may depend on the symptoms of CD in individuals with both conditions. In severely malnourished subjects with T1DM, the treatment of newly detected celiac disease has had
an unequivocal positive effect: intestinal symptoms were rapidly alleviated and a significant weight gain was evident. In addition, the metabolic control of T1DM improved in general, and in particular the number of severe hypoglycemic episodes declined.30,31 Importantly, however, James Braly, MD, author of Dangerous Grains, reminds us that “after the complete autoimmune destruction of insulin-producing islet cells, a gluten-free diet does not reverse or stabilize Type 1 diabetes.”32
The question remains whether or not untreated celiac disease worsens the rate and progression of diabetic complications. In any case, it appears that neurological complications commonly occur in CD, and it has not been excluded that untreated CD may predispose individuals with diabetes to neuropathy.33 A study by Smyth, et al., published in the New England Journal of Medicine, described a genetic susceptibility to both T1DM and CD, which shares common alleles.34 This suggests that common biologic mechanisms, such as autoimmune-related tissue damage and intolerance to dietary antigens, such as gluten, are etiologic features of both diseases.
Salivary Testing for Antibodies in Celiac and Type 1 Diabetes The problem with conventional blood-analysis testing for CD is that it will not reveal intolerance to gluten unless there is extensive damage to the intestinal villi.35 Animal studies have demonstrated that when a bacterial antigen – from milk or gluten, for example – is consumed, anti-gliadin IgA (AGA) and anti-tissue transglutaminase antibodies (tTG-Abs) are not always detected in the blood. However, these antibodies can be detected in the animal’s stool or saliva.36 As a result, salivary assays have been developed to test for AGA and tTG-Abs. A recent study demonstrated that it is possible to detect salivary tTG-Abs with high sensitivity not only at CD diagnosis, but also during a gluten-free diet.37 This contradicts previous data that
The Gluten Connection

Fall 2011 Volume 14, Issue 2www.integrativeRD.org
Page
28
showed conflicting results regarding salivary assays for CD.38 Essentially, patients who have AGA in their saliva are considered to be gluten intolerant. A positive test for both AGA and tTG-Abs confirms celiac disease. A positive test for only tTG-Abs, which is present in T1DM, demonstrates an autoimmune disease.39 Taken together, it’s important for someone with a positive salivary tTG-Abs to try a gluten-free diet for several months, since gluten-containing foods are immunoreactive in many people with autoimmune disease.
The Unifying Hypothesis It appears that gluten consumption is a dietary factor in T1DM leading to the alteration of gut immune system function and its effects on the pancreatic immune system.34 Furthermore, insulin and its precursors are major targets of the T and B lymphocyte autoreactive response in T1DM. Knip and colleagues speculate that “you may need a triggering gastrointestinal infection inducting primary target cell damage and/or a proinflammatory cytokine milieu in the gut epithelium to initiate the disease process subsequently driven by dietary gluten toward clinical celiac disease in genetically predisposed individuals”.40 Additionally, genes that are classified as autoimmunity genes, due to their association with T1DM, may contribute to CD. The latter, according to Knip et al., explain about half of the familial clustering in both diseases, while the former must be due to non-HLA genes and/or a shared environment.40
Take Home Message for Integrative and Functional Medicine PractitionersThere is no doubt that many patients with CD primarily contact specialists other than gastroenterologists. The majority of cases thus remain undetected. A close association between T1DM and CD has been shown in numerous studies. The diagnosis of CD requires a small-bowel biopsy. However, sensitive and specific antibody serological assays, including antiendomysial and
antitissue transglutaminase tests, and salivary tests, are helpful in preliminary screening for gluten intolerance in cases where symptoms are atypical, appear outside the gastrointestinal tract, or are entirely absent (the latter being of possible interest in those individuals with an immediate family history of CD). Prevention of T1DM advocates the early diagnosis and treatment of even asymptomatic CD. The benefits of screening for CD in T1DM remain to be confirmed by prospective follow-up studies. However, there seems to be a good case for this type of extensive screening.
Dr. Sheila Dean, DSc,RD,LD,CCN,CDE is a registered and licensed dietitian, board certified clinical nutritionist, certified diabetes educator and exercise physiologist. Currently, Dr. Dean is the owner of Palm Harbor Medical Nutrition, a private practice based in Palm Harbor, Florida. Contact Dr. Dean at [email protected] or 727-781-4326.
References1. Answers.com. Celiac Disease.
Available at http://www.answers.com/topic/coeliac-disease. Accessed December 16, 2008.
2. Green PH, Alaedini A, Sander HW, Brannagan TH3rd, Latov N, Chin RL. Mechanisms underlying celiac disease and its neurologic manifestations. Cell Mol Life Sci. 2005;62:791-799.
3. Salmi TT, Collin P, Jarvinen O, Haimila K, Partanen J, et al. Immunoglobulin A autoantibodies against transglutaminase 2 in the small intestinal mucosa predict forthcoming celiac disease. Aliment Pharmacol Ther 2006; 24:541-552
4. Valentino R, Savastano S, Maglio M, Paparo F, Ferrara F, et al. Markers of potential celiac disease in patients with Hashimoto’s thyroiditis. Eur J Endocrin. 2002; 146:479-483.
5. Sanders D, Hurlstone DP, McAlindon ME, Hadjivassiliou M, Cross SS, Atkins CJ. Antibody negative celiac disease presenting in elderly people-
an easily missed diagnosis. BMJ. 2005;330:775-776.
6. Feighery C. Coeliac Diease. BMJ. 1999;319:236-239.
7. Talley NJ, Valdovinos M, Petterson TM, Carpenter HA, Melton LJ. Epidemiology of celiac sprue – a community-based study. Am J Gastroenterol. 1994; 89:843-846.
8. Fasano A. Prevalence of Celiac Disease in At-Risk and Not-At-Risk Groups in the United States. Archives of Internal Medicine. 2003;163:286-292.
9. Hadjivassiliou M, Grunewald R, Davies-Jones G. Gluten Sensitivity As A Neurological illness. J Neurol Neurosurg Psychiatry. 2002; 72:560-563.
10. Rubio-Tapia A, Kyle R, Kaplan E, Johnson D, Page W, et al. Increased Prevalence and Mortality in Undiagnosed Celiac Disease. Gastroenterology. 2009;137:88-93.
11. Katz KD, Rashtak S, Kahr BD, Melton LJ 3rd, Krause PK et al. Screening for celiac disease in a north American population: sequential serology and gastrointestinal symptoms. Am J Gastroenterol. 2011;106:1333-1339.
12. Fasano A. Celiac Disease – How to Handle a Clinical Chameleon. NEJM. 2003;348:2568-2570.
13. Fasano A. Current Approaches to Diagnosis and Treatment of Celiac Disease: An Evolving Spectrum. Gastroenterology. 2001;120:636-651.
14. Kamin DS, Furuta GT. The Iceberg Cometh: Establishing the Prevalance of Celiac Disease in the United States and Finland. Gastroenterology. 2004;126:359-361.
15. Helms S. Celiac Disease and Gluten-Associated Diseases. Alternative Medicine Review. 2005;10:172.
16. Green P. Mechanisms Underlying Celiac Disease and Its Neurologic Manifestations. Cell Mol Life Sci. 2005; 62:791-799.
17. Green P. Celiac Disease. NEJM. 2007;357:1731.
18. US Dept of Health and Human
The Gluten Connection

Fall 2011 Volume 14, Issue 2www.integrativeRD.org
Page
29
Services – NIH Autoimmune Diseases Coordinating Committee. Autoimmune Disease Research Plan. 2006.
19. Bland J. Understanding the Origins and Applying Advanced Nutritional Strategies for Autoimmune Diseases Seminar. Presented March 25, 2006. Orlando, FL.
20. Kumar V, Rajadhyaksha M, Wortsman J . Celiac Disease-Associated Autoimmune Endocrinopathies. Clin Diagn Lab Immunol. 2001; 8: 678-685.
21. Sategna-Guidetti C, Volta U, Ciacci C, Usai P, Carlino A, et al. Prevalence of Thyroid Disorders in Untreated Adult Celiac Disease Patients and Effect of Gluten Withdrawal: An Italian Multicenter Study. Cell Mol Life Sci. 2005. 62:791-799.
22. Shaoul R. Associated Autoantibodies In Celiac Disease. Autoimmunity Reviews. 2007;6:559-565.
23. Collin P, Kaukinen K, Valimaki M, Salmi J. Endocrinological Disorders and Celiac Disease. Endocrine Reviews. 2002;23:464-483.
24. Nelson D. Gluten-Sensitive Enteropathy (Celiac Disease): More Common Than You Think. Amer Fam Phy. 2002; 66:2259-2266.
25. Shanahan F. Coeliac disease and diabetes mellitus; a study of 24 patients with HLA typing. Quart J Med. 1982;51:329-335.
26. Barker J, Liu E. Celiac Disease: Pathophysiology, clinical manifestations, and associated
autoimmune conditions. Adv Pediatr. 2008;55:349-365.
27. Ventura A, Magazzù G, Greco L. Duration of exposure to gluten and risk for autoimmune disorders in patients with celiac disease. SIGEP study group for autoimmune disorders in celiac disease. Gastroenterology. 1999;117:297-303.
28. Berti I, Trevisiol C, Tommasini A, Città A, Neri E, et al. Usefulness of screening program for celiac disease in autoimmune thyroiditis. Dig Dis Sci. 2000;45:403-406.
29. Fuchtenbusch M, Ziegler A-G, Hummel M. Elimination of dietary gluten and development of type 1 diabetes in high risk subjects. Rev Diabetes Stud. 2004;1:39-41.
30. Thain M, Hamilton JR, Ehrlich RM. Coexistence of diabetes mellitus and celiac disease. J Pediatr 1974; 85:527–529.
31. Shanahan F. Coeliac disease and diabetes mellitus: a study of 24 patients with HLA typing. Q J Med. 1982; 51:329–335.
32. Braly J, Hoggan R. Dangerous Grains. New York: Avery;2002.
33. Hadjivassiliou M, Gibson A, Davies-Jones GA, Lobo AJ, Stephenson TJ, et al. Does cryptic gluten sensitivity play a part in neurological illness? Lancet. 1996; 347:369–371.
34. Smyth D, Plagnol V, Walker NM, Cooper JD, Downes K, et al. Shared and Distinct Genetic Variants in Type 1 Diabetes and Celiac Disease. NEJM.
2008;359:2767-2777.35. Reeves G, Squance M, Duggan
A, Murugasu R, Wilson R, et al. Diagnostic accuracy of celiac serological tests: a prospective study. Eur J Gastroenterol & Hepatol. 2006;18:493-501.
36. Kappler M, Krauss-Etschmann S, Diehl V, Zeihofer H. Detection of secretory IgA antibodies against gliadin and human tissue transglutaminase in stool to screen for celiac disease in children: validation study. BMJ. 2006; 332:213-214.
37. Bonamico M, R Nenna, Luparia R P, Perricone C, M Montuori, et al. Radioimmunological Detection of Anti-transglutaminase Autoantibodies in Human Saliva: A Useful Test to Monitor Coeliac Disease Followup. Aliment Pharmacol Ther. 2008;28:364-370.
38. Baldas V, Tommasini A, Santon D, Not T, Gerarduzzi T, et al. Testing for Anti-Human Transglutaminase Antibodies in Saliva Is Not Useful for Diagnosis of Celiac Disease. Clin Chemistry. 2004;50:216-219.
39. Lieberman S. The Gluten Connection. New York, Rodale; 2007.
40. Knip M, Veijola R, Virtanen SM, Hyöty H, Vaarala O, et al. Environmental triggers and determinants of type 1 diabetes. Diabetes 2005;54:Suppl 2:S125-S136.
The Gluten Connection

Fall 2011 Volume 14, Issue 2www.integrativeRD.org
Page
30
CPE Objectives and Questions The Gluten Connection
Objectives, Learning Codes, and CPE questions for Fall 2011 CPE—The Gluten Connection
Objectives:After reading this CPE article, the nutrition professional will be able to:
1. Describe the classic presentation of celiac disease (CD).2. Identify at least four ways in which atypical CD may present.3. State the prevalence of CD among individuals with type 1
diabetes mellitus (T1DM) and vice versa (i.e., the prevalence of T1DM among those with CD).
4. Identify the shared genetic factor affecting risk for both CD and T1DM.
5. Explain the relationship between gluten consumption and T1DM.
6. Explain the potential benefit of screening for CD in individuals with T1DM.
The Gluten Connection: The Relationship Between Celiac Disease and Type 1 Diabetes Mellitus CD = Celiac disease T1DM = type 1 diabetes mellitus Pick the one best answer.1. Classic presentation of celiac disease is characterized by which
of the following? a. Epithelial infiltration of the jejunum, fever, and
dermatitis b. Gastrointestinal symptoms, diarrhea and possibly
malabsorption c. Vitamin B12 deficiency related anemia and elevated
homocysteine levels d. Altered thyroid function, bone disease and possible
neurological disorders 2. Atypical celiac disease is characterized by which of the
following? a. Diarrhea, bloating, hyper-thyroidism, and low levels of
intra-epithelials T cells b. Malabsorption syndrome, hypoalbuminemia related
edema, and incontinence c. Megaloblastic anemia, malaborption syndrome,
wasting, and crypt hypoplasia d. Iron deficiency anemia, altered thyroid function,
dermatitis, and bone disease 3. Compared to the general population, what is the prevalence
of CD among individuals with T1DM? a. No reported difference b. 2 to 4 times greater c. 5 to 8 times greater d. 10 to 30 times greater
4. Approximately what percentage of people living with CD have T1DM, and what percentage of those with T1DM have CD?
a. 2% b. 3% c. 4% d. 5% 5. What is the shared genetic factor affecting risk for CD and
T1DM? a. Association with the same human leukocyte antigen
(HLA) b. Association with the same IgE and IgM antibodies c. Association with opposing human leukocyte antigen
alleles 6. Which of the following describes a relationship between
gluten consumption and T1DM a. Elimination of gluten can reverse beta cell destruction
and T1DM b. Elimination of gluten is associated with lower
frequency of T1DM c. Limiting consumption of gluten is associated with
lower frequency of T1DM d. Longer exposure to gluten decreases risk of T1DM in
the aging population 7. Which of the following confirms CD? a. Positive salivary assay for anti-gliadin IgA and anti-
tissue transglutaminase antibodies b. Biopspy from the right ascending bowel mucosa with
presence of crypt hyperplasia c. Serology confirming vitamin E, D, and B12 deficiencies d. Serology confirming IgA, IgE and IgM antibodies
higher than normal 8. Which of the following could be considered potential
screening methods for CD? a. Serology for vitamin D deficiency b. Serology for vitamin B12 deficiency c. Saliva assays for anti tissue transglutaminase and anti
gliadin IgA antibodies d. Saliva assays for proinflammatory cytokines such as
alpha interferon and interleukin 6 9. Which of the following might be recommended for a person
with a positive salivary assay for anti-tissue transglutaminase antibodies?
a. Limit fructose consumption and add fish oil daily b. A probiotic supplement for 3 months c. A gluten free diet for several months

Fall 2011 Volume 14, Issue 2www.integrativeRD.org
Page
31
ANSWER KEY: 1. B 2. D 3. D 4. D 5. A 6. B 7. A 8. C 9. C
CPE answer sheet for questions for Fall 2011 CPE: The Gluten Connection
This article is approved for 1.0 hour of continuing professional education by the Commission on Dietetic Registration. Possible Learning Codes: 2000, 2010, 2020, 4000, 4040, Level 2. This activity has been approved for one hour of CPE credit. You will be notified if the hours are not approved. Please circle the letter that corresponds to the correct answer to the questions.
Instructions to receive credit:1) After reading the article, answer the questions listed on this page. For each question, select the one best response.
2) Mail, fax or email the application for CPE credit with answers to DIFM DPG c/o Shari Pollack, CPE Editor 4500 Keeney Street Skokie, IL 60076 [email protected] Fax: 312-569-6118
3) Once this information has been received, Shari Pollack, CPE Editor , will email verification of completion for the CPE credit along with the Certificate of Completion for this activity.
1. a b c d 2. a b c d 3. a b c d 4. a b c d 5. a b c d 6. a b c d 7. a b c d 8. a b c d 9. a b c
CPE Reporting Form • Fall 2011 • The Gluten Connection. Expiration Date September 30, 2012 Please print or type
Name: ________________________________________________________________________________
Address: ______________________________________________________________________________
ADA Membership #: _____________________ Phone: _________________________________________
Email Address: _________________________________________________________________________
DIFM Member Yes No Date Test Completed: ____/____/____
This activity had been approved for one hour of CPE credit. You will be notified if hour is not approved.

Fall 2011 Volume 14, Issue 2www.integrativeRD.org
Page
32
Citicoline: a promising dietary supplement for preventing cognitive decline
Sarah Harding Laidlaw, MS, RD, CDE
As the world’s population continues to
age and grow, so too grows interest in preventing cognitive decline, decreasing
the severity of damage caused by cerebrovascular disease and stroke, and ameliorating the effects of traumatic brain injury and Parkinson’s disease. Cognition and mental performance are dependent upon neurotransmitters, chemical messengers that support communication between nerve cells. Associated with many age related cognitive changes and other brain disorders are declines in cholinergic neurons, the neurotransmitter actetylcholine, and choline-containing phospholipids. Changes in these phospholipid compounds result in the alteration of cell membrane composition.1
One such compound, phosphatidylcholine, is a major structural phospholipid in brain cell membranes. Cytidine 5’-diphosphocholine (CDP-choline) is a precursor for the synthesis of phosphatidylcholine that may protect cell membranes by accelerating the resynthesis of phospholipids and suppressing the release of free fatty acids, which lessens the progression of ischemic cell damage. CDP-choline is produced in the human body; it also serves as a choline donor in the biosynthesis of acetylcholine.1 Citicoline, a supplement taken orally or given intravenously in research studies, is metabolized in the gut into cytidine and choline, thus providing an exogenous source of these compounds.
Citicoline has shown promise in the treatment of age-related cognitive decline, cerebrovascular disease, ischemic stroke and traumatic brain injury. Limited improvements have
been seen in persons with Parkinson’s disease and glaucoma. Citicoline has been used extensively in a number of settings for the treatment of these neurodegenerative disorders and based on its effectiveness, may play a role in prevention when taken as a dietary supplement.
Alzheimer’s Disease and Age Related Cognitive DeclineOnce recognized for their role in the normal catabolism of triglyceride-rich lipoproteins in cardiovascular disease, the alipoprotein E (APOE) class of lipoproteins is now being studied for its role in Alzheimer’s disease (AD) and cognition. A member of this lipoprotein class, E4, is the largest known genetic risk factor for late on-set sporadic AD.2
Biochemical markers of cholinergic nerve transmission have been found to be deficient in AD and other conditions characterized by degeneration of cholinergic neurons. Citicoline has been shown to modestly improve cognitive function in AD by serving as an acetylcholine precursor.2
A double-blind placebo-controlled randomized study of 30 patients with mild to moderate Alzheimer’s-type dementia investigated the efficacy and safety of treatment with citicoline. Examinations were conducted at baseline and after 12-weeks of treatment with citicoline. Compared to the placebo, the cognitive performance of patients with APOE E4 improved. In addition, cerebral blood flow velocities increased and an increase in the brain bioelectrical activity pattern of AD patients was seen. Citicoline appeared to be well tolerated at the study dose of 1000 mg/day.2
Citicoline supplementation for six weeks in 16 healthy middle-age individuals was shown to significantly alter membrane phospholipids and improve memory performance by facilitating tissue perfusion and oxygenation in the frontal lobe and temporal regions of the brain. Increased support of steady-state
concentrations of ATP and its utilization were consistent with the increased bioenergetic state that was observed. The brain regions specifically targeted are involved in a variety of cognitive functions including attention and memory; changes to energy metabolism in these regions may mitigate cognitive declines associated with aging. Studies using phosphorus magnetic resonance spectroscopy (P MRS) have shown increased energy reserves and utilization in the brain, and that increased amounts of the essential phospholipid membrane components are needed to synthesize and maintain cell membranes.3
Brain InjuryTraumatic brain injury (TBI) is a major cause of death and multiple cognitive and behavioral disabilities. TBI may result from motor vehicle accidents, falls from moving and stationary objects, assault, and strikes to the head. There is no standard pharmacologic treatment for TBI; the preparations used are known to treat only one portion of the cascade of injuries that occur after the TBI-instigating event. In addition, available pharmacologic treatments are time-limited in their ability to provide neuroprotection and do not contribute to neuro-restorative process.4
Injuries to the brain impact the production of cell membrane phospholipids; this results in edema caused by the accumulation of intracellular water. In animal studies of brain trauma, CDP-choline has been shown to decrease edema formation and blood-brain barrier disruption following TBI. CDP-choline considerably prevented brain damage caused by neuronal loss in the hippocampus, decreased cortical contusion volume and improved neurological recovery.5
One major clinical trial of citicoline’s use in TBI is currently being conducted. The Citicoline Brain Injury Treatment (COBRIT) Trial is a randomized double-blind, placebo controlled, multicenter

Fall 2011 Volume 14, Issue 2www.integrativeRD.org
Page
33
Citicoline: a promising dietary supplement for preventing cognitive decline
trial based in the United States. The trial is evaluating the effect of citicoline given for 90 days (1000 mg twice a day) versus a placebo, on functional outcomes in patients with complicated mild, moderate, or severe TBI. The study will be conducted over 32 months and include 1292 patients.4
In other trials related to traumatic coma, individuals treated with citicoline demonstrated better recovery of motor function and walking ability as compared to persons given a placebo. Citicoline appeared to reduce the duration of coma and the severity, incidence, and duration of mental and motor declines associated with TBI.6
Cerebral Ischemia and StrokeCognitive decline after a stroke is known to be more common than stroke recurrence. The risk of dementia is almost doubled in stroke patients and stroke is a major contributor to vascular dementia (VaD). The incidence of (VaD) has been shown to increase from 7% in the first year post stroke to 48% 25 years later. Vascular cognitive impairment (VCI) includes many types of cognitive impairment—excepting dementia—and reflects the effects of the vascular burden on higher mental function.7
Within six months of a stroke 44%-74% of patients exhibit some cognitive disturbance. VCI without dementia is more common than VaD, however, within five years, half of patients with VCI have dementia. Patients with the apolipoprotein E 4 allele appear to be at higher risk, suggesting a link with Alzheimer’s disease. This risk decreases over time after the initial stroke event and is independent of demographic information or presence of vascular risk factors.7
In a data-pooled analysis of 4 clinical trials in the U.S. with a total of 1372 patients, oral citicoline administered within 24 hours from the onset of symptoms enhanced the neurological and functional recovery of acute
ischemic stroke patients. Evidence from this study indicated that when given within 24 hours of the event, citicoline increased the probability of a full recovery after three months from moderate to severe stroke.8 A Cochrane review of 14 studies examined the efficacy of CDP-choline in the treatment of cognitive, emotional, and behavioral deficits associated with chronic cerebral disorders in the elderly. This review concluded evidence supported the benefit of CDP-choline on memory function and behavior.9
A clinical trial assessed the safety and efficacy of citicoline on neurocognitive function after a first stroke. Patients were given citicoline for six weeks, and then randomly assigned to stop the therapy or to continue citicoline up to month six. Patients not continuing with citocoline therapy showed significantly higher cognitive impairment in attention and executive functions. The authors concluded that citicoline was safe and effective after a first ischemic stroke and does in fact improve neurocognitive impairment.10
The ICTUS trial (International Citicoline Trial in acUte Stroke), in Europe is a sequential phase three study of citicoline’s use in ischemic stroke. Beginning in 2006 in 56 treatment centers, ICTUS has an upper limit of 2600 patients. The objective of the study is to demonstrate the effectiveness of citicoline as compared to a placebo in improved recovery over a twelve week period.11 Results are not available at this writing, however, there is hope that this trial along with COBRIT will help to confirm the benefit of long term treatment with citicoline with better functional, cognitive, and neurological recovery for patients with brain trauma and cerebral ischemia.
Other Therapeutic UsesCiticoline has been studied for other conditions that may be related to neuronal damage, including glaucoma
and Parkinson’s disease. Studies are ongoing and have mixed results thus far.
While glaucoma—a group of eye diseases leading to damage of the optic nerve—s a leading cause of blindness in the elderly, persons of all ages can develop the condition. There is no known cure, but if caught early, progression of glaucoma can be slowed. Citicoline has been demonstrated to repair optic nerve damage occurring in glaucoma. Citicoline appears to enhance the synthesis of phosphatidylcholine and other cell-membrane phospholipids thereby providing neuroprotection to the retina.1,6
Preliminary research has demonstrated decreased rigidity and bradykinesia, but not tremors, in patients with Parkinson’s disease. It is hypothesized that citicoline’s ability to improve dopaminergic function accounts for this effect. Patients given 500 mg/day citicoline intramuscularly in conjunction with conventional treatment of L-dopa and a decarboxylase inhibitor showed improvement over a placebo group.1
Recently Studied ApplicationsPrecursors for neuronal membrane repair provided by citicoline show promise in treating the neurological disorders of infectious conditions. A recent study showed that citicoline may play a role in adjunctive therapy for treatment of some infectious diseases, especially the neurological abnormalities that arise from the overwhelming immune response dysregulation that occurs within the host. Treatment for infectious disease-causing agents are successful, however little is available to address the underlying pathology of the damage done by the disease.6 Although not cited in current literature, this author raises the question of whether citicoline may also play a role in neurological damage inflicted by poorly controlled blood sugar in persons with diabetes.
Citicoline may play a role in weight management by modulating appetite.

Fall 2011 Volume 14, Issue 2www.integrativeRD.org
Page
34
Based on research showing an increase in dopamine and a reduction in craving in cocaine addicted individuals, researchers postulated that the supplement may have an effect on brain responses to food, including appetite and food cravings. A six week study evaluating changes in appetite ratings, weight, and cortico-limbic responses to images of high-calorie foods using functional magnetic resonance imaging (fMRI) was undertaken. No significant change in weight was seen, although significant declines in appetite ratings were observed after six weeks in subjects taking citicoline. A significant increase in functional brain responses to food stimuli within was also seen. The increased activity in the amygdala, insula, and lateral orbitofrontal cortex correlated with declines in appetite ratings.12
Take Home MessageCiticoline was originally developed in Japan for acute cerebrovascular events and was subsequently introduced as a prescription drug in over 40 countries where it is now frequently prescribed for cognitive impairment related to chronic cerebrovascular disease.9,13 In 2004, citicoline was approved for use as a dietary supplement in the U.S.. Citicoline has been studied in more than 11,000 volunteers and patients and is one of the most studied substances for neurologic conditions.10,13 Citicoline appears to be well tolerated and is safe for long term use as a dietary supplement from 250mg to 500 mg. Given its safety profile and sound research on its benefits for brain health, citicoline’s major side effects are few: diarrhea and nausea are the most common, but do not seem to occur more often than in persons taking a placebo.9 Given citicoline’s demonstrated neuroprotective, neurorecovery, and neurofacilitation properties in a variety of cognitive related conditions, and recent studies of its possible role in appetite suppression, it appears that this dietary supplement has promise in multiple applications. Although studies have
shown it to be beneficial in preventing future damage after brain injury, stroke, or in age related dementia, there appears to be few studies that document its use for prevention in healthy individuals. However, from the studies currently available and the relative safety of the supplement, citicoline’s use for early prevention of cognitive decline deserves consideration.
Sarah Harding Laidlaw, MS RD CDE is the newsletter editor for the Dietitians in Integrative and Functional Medicine. She practices integrative and functional medicine and provides diabetes counseling and education in Southern Nevada. Contact Sarah at [email protected] or 970-216-2356.
References1. Conant R, Schauss AG. Therapeutic
applications of citicoline for stroke and cognitive dysfunction in the elderly: a review of the literature. Alt Med Rev. 2004; 9:17-31.
2. Alvarez XA, Mouza R, Pichel V, Perez P, Laredo M, et al. Double-blind placebo-controlled study with citicoline in APOE genotyped Alzheimer’s disease patients. Effects on cognitive performance, brain bioelectrical activity and cerebral perfusion. Methods Find ExpClin Pharmacol. 1999;21:633-644.
3. Silveri MM, Dikan J, Ross AJ, Jensen JE, Kamiya T, et al. Citicoline enhances frontal lobe bioenergetis as measured by phosphorus magnetic resonance spectroscopy. NMR Biodmed. http://www.interscience-wiley.com) DOI:10.1002/nbm. Published 2008. Accessed August 22, 2011.
4. Zafonte R, Friedewald WT, Lee SM, Levin B, Diaz-Arrastia R, et al. The Citicoline brain injury treatment (COBRIT) trial: design and methods. J Neurotrauma. 2009;26:2207-2216.
5. Dempsey RJ, Raghavendra RVL. Cytidinediphosphocholine treatment
to decrease traumatic brain injury-induced hippocampal neuronal death, cortical contusion volume, and neurological dysfunction in rats. J Neurosurg. 2003; 98:867-873.
6. Qureshi I, Endres JR. Citicoline: a novel therapeutic agent with neuroprotective, neuromodulatory, and neuroregenerative properties. Nat Med J.2010; 2:11-25.
7. Alvarez-Sabin J, Roman G. Citicoline in vascular cognitive impairment and vascular dementia after stroke. Stroke. 2011;42:S40-S43.
8. Davalos A, Castillo J, Alvarez-Sabin J, Secades JJ, Mercadal J, et al. Oral citacoline in acute ischemic stroke: an individual patient data pooling analysis of clinical trials. Stroke. 2002:33:2850-2857.
9. Fioravanti M, Yanagi M. Citidinediphosphocholine (CDP-choline) for cognitive and behavioural disturbances associated with chronic cerebral disorders in the elderly. Cocrane Database Syst Rev. 2005;18: CD000269.
10. Davalos A, Secades JJ. Citicoline preclinical and clinical update 2009-2010. Stroke. 2011;42:S36-S39.
11. Bolland K, Whitehead J, Cobo E, Secades JJ. Evaluation of a sequential global test of improved recovery following stroke as applied to the ICTUS trial of Citicoline. Pharm Stat. 2009;8:136-149.
12. Kilgore WD, Ross AJ, Kamiya K, Kawada Y, Renshaw PF, Yurgelun-Todd DA. Citicoline effects appetite and cortico-limbic response to images of high calorie foods. Int J Eat Disord. 2010;43:6-13.
13. Saver JL. Citicoline: update on a promising and widely available agent for neuroprotection and neurorepair. Rev Neurol Dis. 2008;5:167-177.
Citicoline: a promising dietary supplement for preventing cognitive decline

Fall 2011 Volume 14, Issue 2www.integrativeRD.org
Page
35
Monique Richard East Tennessee State University Dietetic Intern
Yoga roughly translates from its Sanskrit roots to mean “union”,
describing not only the mind, body, and spirit connection, but also the unity the practice of yoga can create with others. After thousands of years, yoga seems to have just about as many variations as it does the variety of yogis who practice it. Members of the Dietitians in Integrative and Functional Medicine Dietetic Practice Group (DIFM DPG) have read and studied the research on the many benefits yoga can have on physical and mental health; from lowering lab values that contribute to cardiovascular disease risk, diabetes and other co-morbidities, to elevating mood, attitude, and promoting self-acceptance.1,2 These can be significant and profound changes in health, brought about by lifestyle and behavior interventions in conjunction with nutrition guidance for a healthy diet. Sharing our notes, experience, and gathered evidence is critical to introducing yoga practice to other areas of dietetics and seeing positive results.
What is Wanderlust?I had the incredible opportunity to volunteer at the Wanderlust Festival in Bondville, Vermont this year from June 23-26th. Wanderlust is a festival about combining three key elements—Yoga, Music, and Nature—a powerful and essential combination. Creator and founder of Wanderlust, Schulyer Grant interwove those components while featuring four day events all over the country to deliver on the true definition of ‘Wanderlust’— a strong desire to travel. Festivals take place across the country in beautiful places like Colorado, California, Vermont, and Nevada, as well as single day events in cities, like New York and Atlanta, throughout the country.
Yoga: Something for EveryoneAn amazing variety of classes were offered at the venue. Anasura yoga was commonly practiced throughout the festival, even devoting an “Anasura Village” to this variation. Examples of other types of yoga were: Ashtanga, Ananda, Vinyasa flow, Kundalini, and Hatha. Each has their own unique framework and format, but they all still share similar qualities in the mind and body connection. Classes focused on every health-improving opportunity, including addressing addiction and depression, finding your voice, and increasing flexibility, balance, and strength. Christina Runkel was a participant in the “LifeForce” yoga class, which was led by instructor Sofi Dilof and specifically targeted depression. She was willing to share her thoughts and experience about the session:
“The class was small and intimate, and I felt a real sense of community and the empathy of the other yogis about what I go through in my battles with depression. We were all there to fight our negative and/or sad thoughts. In stopping my monkey mind, focusing on breathing, and moving my body, I was no longer a “depressed”
wanderer of the world. I became focused on me, not my thoughts, and even the cold Vermont rain could not get me down.”
A lecture series, titled “Speakeasy”, was scheduled in between yoga classes. Topics included learned life lessons shared by yoga teachers, spiritual connectivity, overcoming physical obstacles, and surviving cancer or debilitating life situations with diet and yoga. As a dietitian-in-training and with a minor in psychology, I appreciated the education and content of the messages. Deepak Chopra spoke about the mind and scientific capacity of reality and the depth of the spirit. The psychology of yoga and the depth of concentration and reflection intrigues me; yoga really needs to be understood and incorporated more into dietetics for all its magnificent power.
MusicFeatured musical guest at Wanderlust, Michael Franti, said “Music has the power to bring people together like no other art form.” Anyone who has ever danced, moved, or been touched by music knows the power of vibrational harmony and sound. The festival music consisted of upbeat hits from Michael Franti and Spearhead, Andrew Bird, and Krishna Das. Inspiring favorites like “Hey, I Love you...”were performed live by Franti while renowned yoga instructor Seane Corne led Warrior I and II, Chaturanga Dandasana, and Downward Dog; the poses were followed by participants jumping back on our feet and clapping. It was the most extraordinary amount of energy and connectedness I have ever experienced with hundreds of others.
NatureMother Nature was not up for shining that weekend, but the rain and damp air did not detract from the magic and zest of the festival. Stratton Mountain was covered with an opaque blanket of fog most of the weekend, but in the lush greenness of summer, the birds, grass,
The Uplifting Benefit of Downward DogAn Observational Review from Wanderlust Yoga Festival, Stratton Mountain, Bondville, VT

Fall 2010 Volume 14, Issue 2www.integrativeRD.org
Page
36
The Uplifting Benefit of Downward Dog Con’t
and trees still lingered with a warmth and beauty hard to forget. Large classes were housed in massive white tents with solid floors; barefoot yogis embraced
the coolness when the practice began driving up their internal temperatures.
So many times we easily forget the impact our environment has on our mental clarity and physical wellbeing. With no plasma TV’s blaring, treadmills hissing, or fluorescent lights shining, what is truly present is an awareness of the elements. Hearing the sounds of birds, wind, and rain, feeling the temperature, breathing the fresh air, seeing the composition of the surroundings, touching the ground, and tasting the cool water engages awareness and mindfulness. The five senses work in unison. Once again yogic “union” is transcended and translated to tranquility. Albert Einstein said “Look deep into nature, and then you will understand everything better.”
Reaching Beyond Yoga, Music, and NatureDuring the festival we learned that Instructor Seane Corne helped establish an organization as part of the non-profit program, The Engage Network, called “Off the mat, into the world” (OTM). The website for the organization is www.offthematintotheworld.org/. This organization uses yoga to inspire change and bring awareness to all of the suffering, need, and crises in the world while establishing ways to contribute to solutions in addressing them. It is a leadership training program that helps participants find their own purpose
through yoga or meditational exercise, and provides organizational skills to their community outreach and service projects. For example, OTM’s work has included teaching yoga to impoverished prostitutes and street children in Cambodia, Africa, and India, educating them while raising funds for HIV/AIDS prevention and outreach. At Wanderlust in Vermont, many attendees used their phone to instantly text a donation to OTM, specifically for the people of Haiti; the donations support work being done to improve Haitians’ quality of life with regards to providing clean drinking water and adequate housing. OTM brings together community, support, and action and is an amazing opportunity to apply a beneficial practice in the world beyond our own mat space.
How Yoga Complements Dietetics Self-acceptance and autonomy is at the heart of what we counsel our clients to conceptualize while we give them the tools and education to choose healthy, nutrient dense foods. DIFM members recognize the importance of the mind and body connection, but it is a hard concept to teach clients. Showing clients and letting them discover the connection for themselves is a powerful and influential tool. As coaches, it is a responsibility and priority we should take seriously. The very act of breathing and taking a moment to process what is happening physically and mentally is an awareness and mindfulness that some dietitians have long taught, believed in, and seen work with individuals. Yes, evidence based practice is the framework to dietetic science, but we are also human and the connectivity and compassion of human nature can be far more profound than statistical analysis. The practice of yoga, accompanied by music and nature when possible, positively and effectively complements nutrition education and behavior modification. It is a dynamic and untapped area ripe for further exploration in dietetics.
DIFM will co-sponsor, with the ADA Foundation, yoga sessions at the Food
& Nutrition Conference & Expo (FNCE) once again this year. I can’t wait to slap down my mat, get into downward dog, and take in a thankful deep breath for all the wonderful people and opportunities that surround me while acknowledging how capable my body really is. Whether you are new to yoga, a devout yogi, or a health practitioner who just wants to experience something different, I invite you all to join us. Discover the power and benefits of the practice itself or as it may be used to supplement the area of dietetics in which you practice.
Monique Richard has a BS in dietetics and a minor in psychology and is currently a dietetic intern pursuing a Master of Science at East Tennessee State University. She is Student Committee Chair for DIFM, Student Editor for the Vegetarian Newsletter with the Vegetarian Nutrition (VN) DPG and the first Student Representative Chair for the American Overseas Dietetic Association. Contact Monique at [email protected] or 615-525-8670.
References:1. Kay A. Therapeutic Yoga for
Nutrition related Chronic-Disease: State of Literature, the Field and the Opportunity for the Nutrition Professional. Nutrition in Complimentary Care Newsletter. 2008;10(4):61,64-66.
2. Ross A, Thomas S. The Health Benefits of Yoga and Exercise: A Review of Comparison Studies. J Alt Comp Med. 2010;16a (Number 1):3–12.

Fall 2011 Volume 14, Issue 2www.integrativeRD.org
Page
37
Resource Review
The Inside Tract: Your Good Gut Guide to Great Digestive Health By Gerard Mullin MD, and Kathie Madonna Swift MS, RD, LDN
Rodale Books (New York), 2011, 368 pages, softcover, $19.99, ISBN-10: 1605292648 ISBN-13: 978-1605292649.
As we educate our clients and patients about complex issues like digestive health, often there is a dance between providing adequate and compelling information to support healing and motivate change without overwhelming those we seek to serve. Gerard Mullin, MD, director of Integrative Gastroenterology Nutrition Services at The Johns Hopkins Hospital, and leading integrative and culinary dietitian Kathie Madonna Swift MS, RD, LDN deliver that balance in their new offering, The Inside Tract.
The book begins with Dr. Mullin’s compelling story of his own near-death by medical mismanagement. He recovered using food and mind-body practices with the aim of healing his gastrointestinal (GI) tract and thus his body. Mullen’s experience motivated him to integrate these concepts into his practice, and the many testimonials from those he has helped attest to his success. Swift also healed from a complex illness through a self-managed exploration of nutrition and integrative medicine. Ms. Swift’s personal experience launched her decades-long career on the forefront of holistic nutrition, at Canyon Ranch, Mark Hyman’s UltraWellness Center, the Kripalu Center for Yoga & Health, and as past-chair of DIFM.
The book includes an overview of how and why digestive imbalances happen, and a simple self-assessment of digestive symptoms. The reader is then
led into exploring food sensitivities and healing their GI tract with an integrated whole-foods approach. Specific suggestions for various conditions and helpful supplements are provided. This individual food-as-healing, the flavor-driven food plans, recipes, shopping lists, and other resources are both sophisticated from an evidence perspective and accessible for readers
of any culinary skill level. This book provides a concise overview for the clinician, and can be a helpful teaching aid for patients interested in improving and managing their digestive health.
Reviewed by Annie Kay MS, RD, RYT, author, yoga teacher and Lead Nutritionist at the Kripalu Center for Yoga & Health. Contact Annie at [email protected],www.kripalu.org
The American Dietetic Association will present its prestigious 2011 Medallion Awards to eight members in recognition of their outstanding service and leadership to ADA and the dietetics profession. Medallion Awards have been given each year since 1976. The winners will receive their awards at an Honors Breakfast on Sunday, September 25, during ADA’s Food & Nutrition Conference & Expo, September 24-27 in San Diego, Calif. DIFM-ADA 2011 Medallion Award recipients are:
Karen P. Lacey, MS, RD, CD, Green Bay, Wis.An ADA member since 1968, Karen is a recognized authority on dietetics education. As the director of the dietetics program and internship at the University of Wisconsin–Green Bay, she envisioned and implemented a standardized nutrition care process and spearheaded the NCP into a formal, universally accepted practice. Karen has served as program reviewer for ADA’s Commission on Accreditation for Dietetics Education since 2002. She is a former member of ADA’s House of Delegates and past chair of ADA’s Quality Management Committee. She currently serves on ADA’s Association Position Committee and is president of the Wisconsin Dietetic Association. As co-investigator since 2007 of the U.S. Department of Agriculture’s Collaborative Grant for Increasing Public Health Opportunities for Dietetic Students, she continues her passion for supporting the strong future of dietetics education. She is a graduate of Valparaiso University, completed a dietetic internship at the University of Michigan Hospital and received a master’s degree from Mount Mary College.
Linda Van Horn, PhD, RD, Chicago, Ill.A member of ADA since 1972, Linda is a professor of preventive medicine and associate dean for faculty development at Northwestern University’s Feinberg School of Medicine. She has been editor-in-chief of the Journal of the American Dietetic Association since 2003 and chaired the 2010 U.S. Dietary Guidelines Advisory Committee. She is a principal investigator for the landmark Women’s Health Initiative—the nation’s largest controlled study of the effects of dietary change on the health of postmenopausal women—and chaired the initiative’s Nutrition Advisory Committee for five years. Her current research focuses on preventing childhood obesity and educating children, families and medical students on how to develop and maintain a healthy lifestyle. Linda is a graduate of Purdue University. She received a master’s degree from the University of Pittsburgh and a doctorate from the University of Illinois–Chicago.
CONGRATULATIONS TO DIFM ADA AWARD WINNERS

Fall 2011 Volume 14, Issue 2www.integrativeRD.org
Page
38
ALCAT looks forward to seeing you at the 2011 ADA Food & Nutrition Conference & Expo
September 24-27, 2011
If you won’t be attending this year’s conference, you will still have the opportunity to listen to Dr. Jamie Wright speak about
Gut Health: Adverse Food Reactions at an upcoming webinar:
October 26th, 20117:30 pm – 8:30 pm EST
Go to www.integrativerd.org to register
Cell Science Systems, Corp.
1(800) US-ALCAT (872-5228)
1-954-426-2304 www.ALCAT.com
*stop by booth 517
Don’t miss Dr. Jamie Wright speaking at the 2011 Integrative and Functional Medicine PreFNCE Workshop on September 24, 2011
ALCAT is the worldwide market leader in Food Sensitivity testing
“SNiP” Update – Nutritional Genomics 2011 Conference Update
Colleen Fogarty Draper MS, RD, LDN Nutritional Genomics Chair, DIFM DPG
I receive many questions from our members about how to further their education in the field of nutritional genomics. You can check out the Nutritional Genomics button on our website, www.integrativeRD.org, to learn about some of our favorite resources.
Also, my three favorite genetics conferences hosted by excellent professional organizations are coming up this fall. I have summarized them for you below.
I will be attending NuGO in September and I am looking forward to providing you with a summary of the week.
Have a Happy Fall 2011!Warmly,Colleen
Date Organization Annual Congress Link6-9th September 2011, Wa-geningen, The Netherlands
European Nutrigenomics Organization (NuGO)
NuGO Week: Measuring Health: How to apply nu-trigenomics for measuring metabolic health
http://www.nugo.org/publicpage.m?key=nugoweek2011&trail=/nugoweek2011
October 11-15, Montreal, Canada
American Society of Human Genetics and International Federation of Human Genetics Societies (IFHGS)
12th International Congress of Human Genetics (ICHG) and the 61st ASHG Annual Meet-ing...
http://www.ichg2011.org/
Beijing, China, October 16–18, 2011
International Society of Nutrigenetics/Nutrigenomics (ISNN)
5th Congress of the Interna-tional Society of Nutrigenet-ics/Nutrigenomics (ISNN)
http://www.isnn.info/con-gress.html

Fall 2011 Volume 14, Issue 2www.integrativeRD.org
Page
39
Reaching the Goal: New Research in Performance NutritionThursday, October 27, 20118:00 p.m - 9:00 p.m. EDT
Athletes and weekend warriors alike are looking for products with safe, scientifically substantiated nutraceutical ingredients that can help them reach their fitness goals. One of the keys to any successful fitness program is muscle rehydration and recovery. Join Dr. Jay Hoffman to learn about the amino acid dipeptide Sustamine™ L-Alanyl-L-Glutamine and its crucial role as a source for enhancing fluid and electrolyte absorption. Dr. Hoffman will highlight the latest research on Sustamine L-Alanyl-L-Glutamine, its mechanism of action in the body and implications for exercise.
Reserve your Webinar seat now at: www1.gotomeeting.com/register/365576624
We invite you to join us for an informative webinar
Jay R. Hoffman, Ph.D., FACSM, FNSCA
Professor, Department of Sport and Exercise, University of Central Florida
President, National Strength and Conditioning Association
Sustamine™ is a trademark of Kyowa Hakko Bio Co., Ltd. Copyright ©2011 Kyowa Hakko U.S.A., Inc.
Mary Alice Gettings - Excellence in Service
Mary Alice Gettings is a registered dietitian and certified diabetes educator and has been with Penn State University Extension
for the past 17 years. In her role as nutrition, health, and food safety educator with Penn State Extension, Mary Alice conducts nutrition and food safety programs for the citizens of Beaver and Butler counties. In her various nutrition classes, she incorporates integrative nutrition strategies to help consumers take charge of their health. Prior to her time with Penn State, she was an in-patient and an out-patient dietitian with Good Samaritan Hospital in Pottsville, PA and at Crozer-Chester Medical Center in Chester, PA. She
received her bachelor’s degree in Nutrition from Penn State University and master’s degree in Technical and Science Communications from Drexel University in Philadelphia. Mary Alice completed her dietetic internship at Miami Valley Hospital in Dayton, Ohio and became a registered dietitian in 1985. She has been a certified diabetes educator since 1990.
Mary Alice has been a tireless advocate for the registered dietitian and has been active at the local, state, and national levels of the dietetic association. She is a past president of the Pittsburgh Dietetic Association and a past chair of Dietitians in Integrative and Functional Medicine, a dietetic practice group of the American Dietetic Association. In 2009, the PA Dietetic Association awarded her with its Outstanding Dietitian of the Year award.
Dr. Sheila Dean - Excellence in Practice
Dr. Sheila Dean, DSc,RD,LD,CCN,CDE is a registered and licensed dietitian, board certified clinical
nutritionist, certified diabetes educator and exercise physiologist. She received her undergraduate training through Rutgers University, completed her internship and graduate training with University of Rhode Island and Brown University’s teaching hospitals, received doctoral training in nutritional genomics and pharmacology through the University of Medicine and Dentistry of New Jersey (UMDNJ) and completed her Doctorate of Science degree through Hawthorn University. Dr. Dean is a graduate of the Institute for Functional Medicine where she received advanced training
Congratulations to 2010 DIFM Award Winners

Fall 2011 Volume 14, Issue 2www.integrativeRD.org
Page
40
in functional medicine and nutritional biochemistry. She has also worked with the Duke University Medical Center’s Endocrinology and Metabolism Disorders Clinic and the Joslin Center for Diabetes as a certified diabetes educator.
Currently, Dr. Dean is the owner of Palm Harbor Medical Nutrition, a private practice based in Palm Harbor, Florida. An educator at heart, she has taught for 14 years as adjunct nutrition science professor at St. Petersburg College and currently teaches at the University of Tampa. She has conducted dozens of local and national public presentations for groups from preschool age to the professional, has written continuing education credit functional medicine modules for both nutritionists and nurses, and has authored numerous book reviews and articles.
Dr. Dean is the current editor of the ADA publication The Health Professional’s Guide to Popular Dietary Supplements, a contributing author of the medical textbook Integrative Gastroenterology and the clinical nutrition textbook Krause’s Food & Nutrition Therapy; 13th ed. Dr. Dean currently serves on the advisory board for the nationally acclaimed Center For Mind-Body Medicine’s Food As Medicine professional education course and was the Professional Advancement Director for the Dietitians in Integrative and Functional Medicine dietetic practice group of the American Dietetic Association. She is the author of Nutrition & Endurance: Where Do I Begin?, and is a certified health and fitness instructor with the American College of Sports Medicine (ACSM), the Aerobics and Fitness Association of America (AFAA), and the YMCA of America.
Ashley Dunham - Student Stipend Award
Ashley Dunham is working towards her master’s degree in nutrition science and anticipates graduating in May 2012. She is completing her dietetic internship at the Francis Stern Nutrition Center, Tufts Medical Center. She has an interest in
food sensitivities and looks forward to practicing in the field of functional medicine once she graduates. She also works with the Women, Infants, and Children (WIC) program in Malden, MA. The student stipend was awarded to her for attending the 10th Annual Complementary Medicine Conference held in New Paltz, NY April 3, 2011 sponsored by the Breast Cancer Options, a not-for-profit organization that offers support groups and other services to women who have been diagnosed with breast cancer. Her article reviewed a panel presentation and one lecture on nutrition and its role in cancer prevention and management of treatment side effects.
Congratulations to 2010 DIFM Award Winners Con’t

Fall 2011 Volume 14, Issue 2www.integrativeRD.org
Page
41
Dietitians in Integrative and Functional Medicine (DIFM) had another successful year of providing members exceptional offerings for professional development, networking, and leadership opportunities.
Results of this successful year included:
• A frequent update of DIFM website content.
• Enhanced professional development programs including webinars and free continuing professional education from DIFM-DPG newsletter articles.
• DIFM networks with the American Botanical Council, Arizona Center for Integrative Medicine, Omega 3 Learning, Center for Mind Body Institute¸ and Institute for Functional Medicine. Networking relationships provide members with opportunities to expand their knowledge base on integrative and functional medicine.
• The DIFM newsletter continues to be a much anticipated member benefit.
• Access to the Natural Medicines Comprehensive Database, an outstanding resource for practitioners.
• Publication of Standards of Practice and Standards of Professional Performance (SOP/SOPP) for Registered Dietitians (Competent, Proficient, and Expert) in Integrative and Functional Medicine (JADA, June 2011).
• An increase in membership.
• Sale of past PreFNCE symposium CDs.
• Co-sponsoring yoga sessions at FNCE.
• The Food and Nutrition Conference and Exhibition (FNCE) in Boston provided members with networking opportunities and several sessions with fantastic attendance.
• The pre-FNCE Symposium: Cognitive Function Throughout the Lifecycle was most informative and well received.
• The Spotlight Session: Integrative Medicine in Depression and Mood Disorders: Taking Research to Practice with David Mischoulon, MD, PhD, Associate Professor at Harvard Medical School and Gretchen Vannice, MS, RD received rave attendee reviews.
• The ever popular DIFM breakfast sponsored by Nutrilite provided free CPEUs on phytonutrients.
Our accomplishments could go on and on. The success of DIFM is due to this year’s outstanding leadership team, ADA staff, executive assistant, Amy Jarck, and most importantly our members. With your support, encouragement, and ideas DIFM continues to grow and be the great DPG we can all be proud of.
Respectfully submitted,Deborah S Ford MS RD CCNPast Chair DIFM DPGCo-Chair SOP/SOPP
Annual Report June 2010 - June 2011Report to members: Another Successful Year
Chair’s.Corner:.Kathy.Moore,.RD,.CCN
Greetings from your DIFM Chair!
I hope you made some good memories this summer. But time marches on and with fall and cooling weather upon us,
comes a new frame of mind. Our clients and patients are also in the mindset to renew efforts to improve their health. There is no better time than now to polish our own skills to help others achieve the healthy lifestyle they desire using whole foods, a myriad of integrative therapies, and a host of functional tests, nutrition physicals, and even insights using nutrigenomics.
Whether you are an accomplished and experienced DIFM-RD, or just getting
started, a great way to hone your skills is at the DIFM Pre-FNCE Workshop: Integrative Nutrition: Essential Tools for Practice…Building Your Future Now. It will be held on Saturday, September 24, 2011. Please see the agenda and details on our website, www.IntegrativeRD.org for registration information. Early registration is accepted until September 14th. This is a can’t-miss-it event! You will go away with new tools to use in your practice.
A sampling of DIFM Members received a survey this summer from our Credentialing Task Force and we are happy to announce ten winners from those who responded to the survey. These lucky members will receive a complimentary recording of the 2011 Pre-FNCE Workshop! Winners are
Barbara Cissell, Christine Craig, Esther Trepal, Janice Turner, Kim Matwiejow, Judy Klavens-Giunta, Marsha McCulloch, Marilyn Scott, Renee Bordeaus, and Stefanie Manetti.
DIFM’s website is being revamped!! We are excited about the opportunity to make significant upgrades, which will start to phase in soon. Check in often at www.IntegrativeRD.org to see how we’ll make this the one portal you can easily use to find information and enhance your integrative and functional medicine skills.
In August we conducted a New Member Webinar to introduce our members to the many benefits and features of membership. We were grateful that a representative of Natural Medicines Comprehensive Database gave a guided tour to using this free service. If you

Fall 2010 Volume 14, Issue 2www.integrativeRD.org
Page
42
Summer has come and gone, and here in the west, the heat is still hanging on. School has started and it is now time
to focus on fall cleaning and updating of all that is important to us—our homes, cars that we took the long vacations in, and most importantly our bodies and minds. Just as we think of spring as a time to clean, fall can be a great time to renew as well. A time to
clean out what was accumulated over the summer, or maybe over many years as in my case, and to look forward to renewal of old friends and learning new information at the Food & Nutrition Conference & Expo (FNCE) in San Diego later this month.
FNCE promises to be information packed and will be providing DIFM members many opportunities to move forward as integrative and functional medicine practitioners. The pre-FNCE conference will be introducing us to the concepts that will be essential to our credentialing as functional medicine practitioners while the conference offerings will include sessions to enhance this knowledge. Some sessions of interest include: Sunday - Inflammation: What Do practitioners Need to Know Today; Omega-3 Fatty Acids in Depression and Mood Disorders: Applications for Practice; Integrative Nutrition Therapy for Irritable Bowel Syndrome and Inflammatory Bowel Disease, Monday - Genes, Environment and Chronic Disease: What
is the Relationship?; Diet and Autism, and Tuesday - Dietary Supplements. Not to mention the wonderful networking opportunities at Tuesday’s DIFM breakfast, the DPG Showcase, and Product Marketplace.
Not only are there opportunities at FNCE, but we also have two excellent webinars from our sponsors planned for October – see more information in this issue. In addition, the Institute for Functional Medicine (IMF), a DIFM networking partner, is offering DIFM members a significant discount for their Functional Nutrition Course (FNC): Applying Functional Nutrition for Chronic Disease Prevention and Management October 21-23, 2011 in Denver, CO. And for budding nutrition geneticists, there are three conferences around the world that may spark your interest and add to your knowledge; Colleen Fogarty Draper has provided information for these upcoming events on page 38. She will also update us on cutting edge information she receives at NuGO week in the winter issue of the newsletter.
I hope all of this excitement is rubbing off on you and that I am able to meet many of you in person at FNCE this year. Please stop by the DPG Showcase or Product Marketplace and introduce yourself and tell me what you like about the newsletter and your ideas for future issues and articles. Better yet, stop by and volunteer for one of the many opportunities to become involved with the newsletter or DIFM DPG.
See you in September!
Editor’s.Notes:.Sarah.Harding.Laidlaw,.MS,.RD,.MPA,.CDE
missed it and need help, do not hesitate to contact them directly. They are here to help us get the most from our access to this wealth of information!
Thank you to so many of you who have decided to volunteer to serve DIFM! We will soon have all of our newly-created positions filled, but there is always an opportunity to help. Elections are just around the corner, and we have seven positions to fill for the 2012-2013 year. If you are interested in learning more, please contact Nominating Chair, Marlisa Brown at [email protected].
We are most grateful to Kyowa-Hakko for their generous support, as they have provided sponsorship of this newsletter. They are the source of Cognizin, the raw ingredient citicoline, an agent that has demonstrated neuroprotective, neurorestorative, and neurofacilitative properties in a variety of cognitive related conditions. A review of citicoline research is featured in an article written by our own newsletter editor, Sarah Laidlaw. Kyowa-Hakko will also be the sponsor for a DIFM Webinar on October 27, 2011, which will feature cutting edge information on another unique raw ingredient,
Sustamine, designed for active persons to help in rehydrating and refueling post exercise. For more information, access their website from the link on the DIFM website. Educating our members on things like these “nutrients-turned-drugs” are one way we help you stay up to date! Watch your eBlast and our website for registration information for this educational webinar.
Wishing you blessings for a colorful fall, KathyKathy Moore, RD, CCNDIFM Chair 2011-2012
Chair’s.Corner.Con’t:.Kathy.Moore,.RD,.CCN
Those of you who would like to contribute an article or have topics that you would like to see in future issues, please feel free to drop me an email or give me a call – [email protected] or 702-346-7968 – or contact any one of the capable DIFM leaders listed on the back of the newsletter.

Fall 2011 Volume 14, Issue 2www.integrativeRD.org
Page
43
EXECUTIVE COMMITTEEChair 2011-2012sKathy Moore, RD, LD, CCNPO Box 487 Tijeras, NM 87059-0487Phone: 505-286-2428 Cell: 505-410-1922Fax: [email protected] Past Chair 2011-2012s Deborah Ford, MS, RD, CCN1031 S. Shannon StreetVan Wert, OH 45891-2548 Phone: [email protected]
Chair Elect 2011 - 2012Alicia Trocker, MS, RDs
4078 Black Bird WayCalabasas, California 91302Cell: 818-970-1990Fax: [email protected]
Treasurer 2010-2012 sLeslie Kay Getzinger, MS, RD3147 Ferncreek Ln Escondido, CA 92027Phone: 714-454-1813Fax: 858-408-3318 [email protected]
Treasurer-Assistant 2011-2012Julie Starkel, MS, MBA, RD6329 20th Ave NESeattle, WA 98115-6909Phone: 206-729-5111Fax: 206-588-2625 Cell: 206-617-2729 [email protected]
Secretary 2011-2013 Erica Kasuli, MS, RDs
20 West 64th Street, Apt 35NOne Lincoln PlazaNY, NY 10023 Phone [email protected]
sIndicates Voting Member
Communications Chair 2011-2012Robin Foroutan, RD, HHC527 East 6th Street, #2W New York, NY 10009-6649 Cell: 917-453-2517 Phone: 212-677-7218 [email protected] Development Chair 2010-2012Lea Russell, MBA, RD, LDN605 20th Ave NESt Petersburg, FL 33704Phone: 727-822–6633Cell: 813-857–[email protected]
Development Associate 2011-2012 Leigh Wagner, RDKU Program in Integrative Medicine3901 Rainbow Blvd.Mailstop 1017Kansas City, KS 66160Phone: 913-945-6809Fax: 913-588-0012Cell: [email protected] [email protected]
DPG Delegate 2010-2013Ane Marie Kis, MS, RD, LDNPO Box 146Ardmore, PA 19003 - 0146Phone: 610-688-3990Cell: 610-453-1193 Fax: [email protected] Executive Asst/Website Mgr/ EML Coordinator 2011-2012Amy Jarck 6 Juliana DrivePittsfield, MA 01201 Phone: 800-279-6880Cell: 413-448-1734 Fax: [email protected]
Website Editor- Associate 2011-2012 Emily D. Moore, RD, LDN202 Oak DriveMiddletown, DE 19709Phone: [email protected]
Website Editor- Associate 2011-2012Sarah D’Emilio, RD, LDN923 Grosstown RoadStowe, PA 19464Phone: [email protected]
Fulfillment Chair 2011-2012 Angela B. Moore, MS, RD7150 E Berry Ave Greenwood Village, CO 80111 Phone: 720-201-1128 [email protected]@fitlifeofcolorado.com
Member Services Chair 2011-2012Jacki Glew, MS, RD, CSO, LDNClinical Nutrition ManagerBlock Center for Integrative Cancer Treatment5230 Old Orchard RdSkokie, IL 60077Phone 847-505-0822 Fax 847-505-0822Cell [email protected]
Member Services Chair – Associate 2011-2012Christine Doolittle MS RD CSSD LDN CLTNominating Committee Chair 2010-2011730 Bridle Path DriveWexford, PA 15090-6815Phone: 724-272-6351Fax: [email protected]
Network Chair 2011-2012 Kathie Madonna Swift, MS, RD, LDN248 Mountain DrivePittsfield, MA 01201Phone: 413-238-1421Fax: [email protected]
Network Associate 2011-2012Lisa L Powell, MS, RD8110 E Rockgate RdTucson, AZ 85750-9735Phone: 520-749-9655Fax: [email protected]
Network Associate 2011-2012Mary M Gocke, RD4 Burbank AveBedford Hills, NY 10507-1704914-261-8870 [email protected]
Newsletter Editor 2011-2012Sarah Harding Laidlaw, MS, RD, MPA, CDE1045 Raptor CircleMesquite, NV 89027Phone: 702-346-7968Fax: [email protected]@mesaviewhospital.com
Newsletter Editor-Associate 2011-2012Jacqueline Santora Zimmerman, MS, RD41 West Hitchcock AveFloral Park, NY 11001Phone: [email protected]
Newsletter Copy Editor 2011-2012 Emily D. Moore, RD, LDN202 Oak DriveMiddletown, DE 19709Phone: [email protected]
Newsletter CPE editor Shari B Pollack, MPH, RD4500 Keeney St.Skokie, IL 60076Phone: 847-213-0424Fax: [email protected]
Newsletter CPE Item WriterJanelle L’Heureux, MS, RD10920 Fairbanks WayCulver City, CA 90230Phone: 213-201-1556 Cell: [email protected] [email protected]
Nominating Committee Chair 2011-2012 Marlisa Brown, MS, RD, CDE, CDN 160 Howells Rd, Suite 6Bay Shore, NY 11706-5320 Phone: 631-666-4297 Cell: 631-987-9406 Fax: 631-666-5284 [email protected] Nominating Committee Chair Elect 2011-2012 Diana Noland, MPH, RD, CCN9018 Balboa Blvd #535 Northridge, CA 91325 Phone: 818-606-8457 Fax: 818-895-2454 [email protected]
Nominating Committee Member 2011-2012Stephen J Roch Jr., RD, LDN, CFT 3716 Page Dr Metairie, LA 70003Phone: 504-455-5813 [email protected] Nutritional Genomics Advisor 2011-2013Colleen Fogarty Draper, MS, RD, LDN7 High Rock RoadStoneham, MA 02180-2869Phone: 781-438-4749Cell: 617-680-3082Fax: [email protected]
Professional Advancement Chair 2010-2012 Elizabeth Redmond, PhD, MS, RD, LD2312 Spring Creek RoadDecatur, GA 30033Phone: 678-638-2954Cell: [email protected]
Professional Advancement Associate 2010-2012Esther Trepal, RD, MS, CDN God’s Love We Deliver 166 Avenue of the Americas New York, NY 10013Phone: 212-294-8165Cell: 646-831-1613Fax: 212-294-8139Email: [email protected] Public Policy/Reimbursement Chair 2011-2013Rita Kashi Batheja, MS, RD, CDN825 Van Buren StreetBaldwin Harbor, NY 11510Phone: 516-868-0605Cell: [email protected]
Student Committee Chair 2011-2013Monique M Richard1752 Red Jacket Dr.Antioch, TN 37013Phone: 615-781-6762Cell: [email protected]
DIFM Credentialing Task Force Co-Chair 2011Lisa A Dorfman, LMHC, MS, RD, CSSDPO BOX 565505Miami, FL 33256-5505Phone: 305-854-1065Cell: [email protected]@miami.edu
DIFM Credentialing Task Force Co-Chair 2011Mary Beth Augustine CDN, RD10 Nancy RoadBrewster, NY 10509Phone: 845-278-0530Cell: [email protected]@gmail.com
Technical Advisor 2011-2013Ruth DeBusk, PhD, RDDeBusk Communications, LC3583 Doris DriveTallahassee, FL 32303-2304Phone/Fax: [email protected]
ADA Practice Manager 2011-2012 Jeanette White, MS, RD, FADAManager, DPG/MIG/Affiliate RelationsAmerican Dietetic Association120 S. Riverside Plaza Suite 2000Chicago, IL 60606-6995Phone: 800-877-1600 x 4778 Fax: 312-899-4778 [email protected]
DIFM Office Address Dietitians in Integrative and Functional Medicine P.O. Box 3624Pittsfield, MA 01202Phone: 800-279-6880 Fax: 877-862-8390 email address: [email protected] website: www.integrativerd.org
2011 - 2012 LEADERSHIP CONTACT INFORMATION
August 26, 2011

THANK.YOU.TO.OUR.SPONSORSWithout your generous contributions, many of the opportunities
and member benefits would not be possible.
Fall 2010 Volume 14, Issue 2www.integrativeRD.org
Page
48
Titanium
Platinum
Editor
Sarah Harding Laidlaw, MS, RD, CDE
Associate.Editor
Jacqueline Santora Zimmerman, MS, RD
Copy.Editor
Emily D. Moore, RD, LDN
CPE.Editor
Shari B. Pollack, MPH, RD.
Communications.Chair
Robin Foroutan, RD, HCC
Editors
Christian Calaguas, MPH, RD
Danielle Torisky, PhD, RD
Newsletter.CPE.Item.Writer
Janelle l’Heureux, MS, RD
The views expressed in this newsletter are those of the authors and do not necessarily reflect the policies and/or official positions of the American Dietetic Association.We invite you to submit articles, news and comments. Contact us for author guidelines.Send change-of-address notification to the American Dietetic Association, 120 South Riverside Plaza, Ste. 2000, Chicago, IL 60606-6995.Copyright © 2011 Dietitians in Integrative and Functional Medicine, a Dietetic Practice Group of the American Dietetic Association. All material appearing in this newsletter is covered by copyright law and may be photocopied or otherwise reproduced for noncommercial scientific or educational purposes only, provided the source is acknowledged. For all other purposes, the written consent of the editor is required.
Annual Subscription Rates (payable in U.S. funds):Individuals ineligible for ADA membership.................................................................................................................................................................................... $60/yearADA members ........................................................................................................................................................................................................................................... $30/yearStudent members .................................................................................................................................................................................................................................... $15/year
For international orders for individuals ineligible for ADA membership, please add $5 shipping and handling for the printed issue available in the fall. Make checks payable to DIFM DPG#18 and mail to DIFM DPG Dietitians in Integrative and Functional Medicine, PO Box 3624, Pittsfield, MA 01202. ISSN 1524-5209
DIFM.EDITORIAL.STAFF