Embed Size (px)
Citation preview

Falling Through the Cracks: CRC Screening in Vulnerable PopulationsStephanie B Wheeler, PhD MPHUniversity of North Carolina at Chapel Hill
September 14, 2015

Background/Past Efforts

CDC Special Interest Project 11-041 Behavioral Economics of Colorectal Cancer Screening in
Underserved Populations (PIs: Wheeler and Pignone)
• CRC screening is vastly underutilized, particularly in underserved (poor, rural, minority, uninsured and publicly insured) populations
• Using a behavioral economics lens, we sought to:
– Understand regional variation in CRC screening in NC (Aim 1)
• Public and private insurance claims data analysis
– Learn how underserved individuals make decisions about CRC screening (Aim 2)
• Preference survey using discrete choice experimental methods
– Provide a framework to design efficient & effective interventions that increase CRC screening rates (Aim 3)
• Microsimulation modeling

Aim 1: Methods• Used North Carolina (NC) Medicaid, Medicare, and private health
plan data for 100% of enrollees continuously enrolled 2003-2008*
• Age-eligible for CRC screening*
• Linked to Area Resource File data
• Geolocated patients and endoscopy centers in NC using State Medical Facilities Plan data
• Called endoscopy facilities to verify information
• Calculated distance to nearest endoscopy center
• Used random intercepts model to predict CRC testing
* Reporting only on publicly insured population turning 50 today

Variable Category TotalN=27,178
Medicare N=7,100
Medicaid N=6,457
DualN=13,611
AOR AOR AOR AORGender Male (ref)
Female 2.15 2.65 1.98 1.99Race White (ref)
Black 0.86 0.83 0.88 0.89Other 0.91 0.83 0.95 0.96
Insurance Medicare (ref)
Dual 1.06 - - -Medicaid 0.86 - - -
Distance in Miles 0-5 Miles (ref)
>5-10 0.97 0.92 0.93 1.05>10-15 0.98 1.00 0.93 1.03>15-20 0.93 0.99 0.80 1.02>20-25 1.14 1.33 1.13 1.0325+ 0.78 0.70 0.72 0.82
Proc. Volume* 0 Proc.(ref)1-200 1.09 1.30 1.33 0.98>200-400 0.98 1.14 1.17 0.90>400-600 1.06 1.36 1.10 0.95>600-800 1.12 1.37 1.19 1.03800+ 1.20 1.54 1.39 1.11
Overall % receiving any CRC test during study period: 49% (among those, 53% colonoscopy, 42% FOBT, 3% flex sig, 2% other)
Multilevel Multivariate Logit Model with Random Effects: Odds Ratios for Receipt of CRC Testing in Total Sample and Stratified by Insurance Type
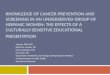
Aim 1 Findings (publicly insured population turning 50)

Aim 1 Findings (publicly insured population turning 50)County-Specific Maps Depicting Adjusted Predicted Probabilities of CRC Testing from Multilevel Models: Total Sample (N=27, 178)

Aim 3 Rationale• Policy makers need to know the most effective and efficient approach
to close the gap between recommendations and practice
– Impact and efficiency depend on context (e.g., current screening behaviors, practice patterns)
• Objective: To estimate the impact and efficiency of distinct, evidence-based approaches aimed at incrementally increasing CRC screening rates in 50-75 year old adults at the population level over 10 years
(1) a Medicaid mailed reminder and registry intervention;
(2) an endoscopy facility expansion initiative to increase access to colonoscopy;
(3) a mass media campaign encouraging African Americans to get screened; and
(4) an intervention offering vouchers to uninsured individuals
7

Aim 3 Methods
• Individual-level discrete-event simulation model programmed in AnyLogic, based on MISCAN-Colon model and work by Subramanian and colleagues (2009, 2011)
• Simulate all cohorts touched by CRC screening over a 10-year intervention window
• Simulated polyp growth begins at age 40
• Simulated polyps can progress to pre-clinical or clinical cancer
– In the absence of screening, incidental clinical diagnosis possible as symptoms progress
– Progression rates are dependent on age, race, and gender
– Screening compliance and modality informed by multi-level statistical models (Aim 1)

Aim 3 Methods: Simulation Model Inputs
9
Underlying Population Screening Patterns Disease Progression Cancer Outcomes Intervention Effects

Aim 3 Methods: Outcomes
• Impact of interventions
– % of age-eligible individuals who are up-to-date with CRC testing (+ subgroups)
– Number of additional life years up-to-date with testing in the age-eligible population compared to testing as usual
• Cost of interventions
– Total cost of each intervention, summing fixed and marginal expenses over the ten-year policy window (undiscounted)
• Efficiency of interventions
– Cost per additional life year up-to-date with CRC testing
10

Simulated population demographics: NC population age-eligible for CRC screening (50-75) January 2014
Overall Age 50-64 Age 65-75Population size 2,782,559 1,844,279 938,280
SexMale 47.7% 48.0% 47.1%Female 52.3% 52.0% 52.9%
RaceWhite 77.0% 75.3% 80.3%Black 18.4% 19.5% 16.4%Other 4.6% 5.2% 3.3%
InsuranceUninsured 10.3% 15.5% 0.1%Private 49.2% 73.9% 0.4%Medicare 31.6% 3.5% 86.9%Medicaid only 3.1% 4.7% 0.0%Dual 5.8% 2.4% 12.6%
11

Testing as usual projections, 2023
Aim I Stat Models Calibrated to match adjusted BRFSS
Overall 46.3% 53.6%By sex
Males 47.2% 54.7%Females 45.0% 52.4%
By raceWhites 47.0% 54.7%Blacks 44.2% 51.4%Others 41.2% 47.5%
By insurancePrivate 48.0% 56.2%Medicaid 42.0% 50.3%Medicare 44.4% 51.3%Dual 38.3% 44.8%Uninsured 14.6% 14.6%

WHAT DO THESE INTERVENTIONS COST? WHAT IS THEIR IMPACT, COMPARED TO TESTING AS USUAL?
Primary outcome: Additional life-years up-to-date with testing

Intervention cost, impact, and cost-effectiveness, compared to testing as usual
Undiscounted:
Cost of intervention
Additional life years up-to-date
Intervention cost per additional life year up-
to-date
Mailed Reminder $1,619,578 111,516 $14.52
Endoscopy Expansion $3,000,000 11,832 $253.98
Mass Media $3,694,800 148,305 $24.91
Voucher for Uninsured $3,750,000 41,709 $89.91

WHAT ARE THE INCREMENTAL OUTCOMES FOR THESE INTERVENTIONS, COMPARED TO EACH OTHER?Primary outcome: Additional life-years up-to-date with testing

Incremental cost-effectiveness results
WD=weakly dominated; SD=strongly dominated

Cost-effectiveness efficiency frontier: Intervention cost versus additional life-years up-to-date
Number of additional life-years up-to-date over 20 years
Cost
of i
nter
vent
ion
over
10
year
s

What is a reasonable amount to pay per additional life-year up-to-date?
• Consider current test costs…
• If we are willing to pay $25 for each additional life-year up-to-date, then that will effectively:
– Increase the cost of FOBT by $25, as testing is annual;
– And, increase the cost of colonoscopy by $250.
• What interventions should we consider? If we are willing to pay…
…as much as $25/FOBT or $250 per colonoscopy…
Then we should adopt mass media and mailed reminder, but
no more.…as much as $100/FOBT or
$1,000 per colonoscopy… Then we would add the
voucher program too.

Impact on % up-to-date in 10th year of policy windowBaseline and %age point Increases for each Intervention
19
Testing as usual
Mailed Reminder
Endoscopy Expansion Mass Media Voucher for
UninsuredOverall 53.6% +0.3% +0.0% +0.4% +0.1%By sex
Males 54.7% +0.3% +0.0% +0.6% +0.2%Females 52.4% +0.5% +0.0% +0.5% +0.1%
By raceWhites 54.7% +0.3% +0.0% +0.4% +0.1%Blacks 51.4% +0.9% +0.0% +1.4% +0.2%Others 47.5% +0.5% +0.0% +0.4% +0.4%
By insurancePrivate 56.2% +0.0% +0.0% +0.5% +0.0%Medicaid 50.3% +4.6% +0.2% +0.8% +0.0%Medicare 51.3% +0.0% +0.0% +0.4% +0.0%Dual 44.8% +3.5% +0.1% +0.7% +0.0%Uninsured 14.6% +0.0% +0.0% +0.6% +1.1%

Conclusions
• Significant regional variation in CRC testing (Aim 1)• Cost (of screening and of follow-up) very important to underserved
populations and fecal testing may be preferred (Aim 2)• Endoscopy expansion not impactful or efficient (Aim 3)
– The other three interventions increase the overall % up-to-date with CRC testing among age-eligible adults, though modestly
– These three interventions do begin to chip away at different disparities
– Reaching Healthy People targets (>70% UTD) or National CRC Roundtable (80% UTD) in NC will require substantial investment
20

Current Directions

CDC Continuation Award through the Cancer Prevention and Control Research Network (CPCRN)
1. Estimate the statewide effect of health insurance coverage (e.g., Affordable Care Act implementation) on costs and benefits of CRC screening in vulnerable populations– Estimate the full costs and benefits of CRC screening in vulnerable populations at the
state level, accounting for follow-up treatments (from our multi-payer insurance claims data), ongoing surveillance (from the published literature), and cancer treatment costs (from the published literature)
– Simulate the role of private insurance expansion via health insurance exchanges (HIE) in uptake of CRC screening
– Simulate the role of Medicaid expansion in uptake of CRC screening2. Partner with other PRCs to replicate claims data and simulation modeling
efforts in other states3. Conduct probabilistic sensitivity analyses on key uncertain parameters4. Determine the resource investment that would be required in a statewide CRC
screening program or combination of programs to achieve CRC screening coverage targets set by Healthy People 2020 (70.5%) and the National Colorectal Cancer Roundtable (80%)

Partnering with other Centers to replicate simulation modeling efforts

Oregon vs. North CarolinaOregon North Carolina
Population, 2014 3,970,239 9,943,964
Persons 65 years and over, 2013 15.5% 14.3%
Females 50.5% 51.3%
Race/Ethnicity (selected), 2013
White alone 88.1% 71.7%
Black or African American alone 2.0% 22.0%
Hispanic or Latino 12.3% 8.9%
Persons below poverty level, 2009-2013 16.2% 17.5%
Land area in square miles, 2010 95,988 48,618
Persons per square mile, 2010 39.9 196.1
Source: http://quickfacts.census.gov/qfd/index.html

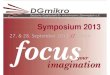
Context – Oregon’s Coordinated Care Organization (CCO) Experiment and Medicaid Expansion
• 2011 Oregon House Bill 3650 authorized CCOs (state’s version of ACOs)
– By 2014, 16 CCOs in operation (see map)
– 60% of 1,000 PCP clinics have become PCMHs with the state
– Quality judged against 17 CCO incentive measures (including CRC screening)
• 2014 Oregon expanded Medicaid coverage from 100% to 138% FPL (~$16,100/yr for single person; or $32,900/yr for family of 4)
– Since then, at least 200,000 new members have joined
For more information see http://www.oregon.gov/oha/ohpb/pages/health-reform/ccos.aspxor http://www.oregon.gov/oha/analytics/Pages/CCO-Baseline-Data.aspx

Context – Oregon’s All Payer All Claims (APAC) Database
• Created in 2009 through Oregon legislation and has been accruing claims since 2011
• Includes medical and pharmacy claims for individuals with commercial, Medicare, and Medicaid insurance
• Provides access to demographic data and allows aggregation at the provider, practice, and regional levels
• The Center for Health Systems Effectiveness (CHSE) is responsible for APAC analyses

Oregon Research Questions
• What is the regional variation in CRC screening within publically and commercially insured populations in Oregon by county? By CCO?
• How have CRC screening patterns changed in publically insured populations following Medicaid expansion?
• What interventions are recommended to increase CRC screening in publically insured populations in Oregon using microsimulation and cost-effectiveness analysis?

Oregon Team
Stephanie Renfro
Melinda Davis John McConnellJackilen Shannon

North Carolina/CDC Team
Stephanie Wheeler
Mike Pignone
Kristen Hassmiller Lich
Anne-Marie Meyer
Trisha Crutchfield
Florence Tangka,CDC
Lisa Richardson, CDC
Maria Mayorga,NC State
Tzy-Mey (May) Kuo
Justin Trogdon

Progress and Challenges
• Progress
– OR team engaged, meeting with NC weekly
– Prelim OR analyses done; drafting paper outlines
• Challenges
– OR claims data not quite as ‘mature’
– OR does not have SMFP data for endoscopy
– How to estimate HIE coverage expansion
– How to estimate Medicaid coverage expansion
– Which new interventions should be evaluated?

Acknowledgments
• CDC SIP 11-041 “Behavioral economics of colorectal cancer screening in underserved populations” (Co-PIs: Pignone and Wheeler)
• AHRQ 1-K-12 HS019468-01 Mentored Clinical Scientists Comparative Effectiveness Development Award (PI: Weinberger; Scholar: Wheeler)
• NIH K05 CA129166 Established Investigator Award in Cancer Prevention and Control: Improving Cancer-Related Patient Decision Making (PI: Pignone)
• NC Translational and Clinical Sciences Institute Pilot Grant “Using systems science methods to improve colorectal cancer screening in North Carolina” (PI: Lich)
• CMMI‐1150732 CAREER: Incorporating Patient Heterogeneity and Choice into Predictive Models of Health and Economic Outcomes”. National Science Foundation (PI: Mayorga)
• University of North Carolina at Chapel Hill Cancer Research Fund• Integrated Cancer Information and Surveillance System (ICISS)

Extra Slides

Mailed reminder (+ Registry) in Medicaid
• Strategy: Letters will be mailed to Medicaid enrollees when they turn 50 and are not up-to-date.
– Letters include information about CRC screening and recommended screening guidelines, instructions for scheduling a screening test or requesting additional information
– Limited registry – NC Medicaid claims database query conducted annually to identify enrollees without claim for FOBT or colonoscopy, excluding those with CRC
• Impact: Receiving a letter results in a 5 percentage point increase in the probability of being screened. (Leone et al., 2013)
• Resources required: Start-up costs (create registry, design letter), annual personnel costs (query and mail letters), per-letter material costs. Acknowledging imperfect information in registry, we assume 10% of those up-to-date receive a letter in error.
• Key uncertainties: Impact on probability of screening
33

Endoscopy expansion
• Strategy: Provide financial incentives for six new endoscopy facilities, to be opened in areas of greatest need across the state based on current levels of access (Sampson, Hyde, Caswell, Dare, Duplin, and Bladen Counties).
34

Endoscopy expansion
• Strategy: Provide financial incentives for six new endoscopy facilities, to be opened in areas of greatest need across the state based on current levels of access (Sampson, Hyde, Caswell, Dare, Duplin, and Bladen Counties).
• Impact: Facilitating access to a colonoscopy increases the probability of compliance and alters regional practice patterns. Impact is based on AIM I statistical models.
• Resources required: Monetary incentive sufficient to stimulate an organization to realize a favorable “business case” for geographic expansion.
• Key uncertainties: Compliance probability as determined by geographic proximity to a colonoscopy and volume of procedures within the selected counties. May require greater investment to create business case and/or ensure facilitates are adequately staffed.
35

Culturally-tailored mass media campaign
• Strategy: Annual month-long mass media campaign (TV, print and radio) to communicate the importance of CRC screening, tailored to African-American NC residents.
• Impact: Campaign will reach 80% of African-Americans, whose probability of screening compliance will increase by 2 percentage points in that year. The campaign will also reach 40% of non-African-Americans, whose probability of compliance will increase 1 percentage points in that year. (Dignan et al. 1994)
• Resources required: Cost to develop ads (one time) and annual costs for ad purchases in newspapers, TV and radio.
• Key uncertainties: Campaign reach and impact on compliance among residents.
36

Voucher for uninsured• Strategy: 500 uninsured individuals turning 50 will gain access to
colonoscopy, as GI docs will be reimbursed for these screens through a voucher program.
• Impact: All 500 individuals will receive colonoscopies, though some would already be screened on their own.
• Resources required: For every voucher used, the provider completing the colonoscopy will receive a pre-negotiated fee of $750, which covers the cost of routine screening colonoscopies as well as of any needed polypectomies and biopsies.
• Key uncertainties: Extent to which intervention encourages screening among those who would have already gotten screened. Other programmatic costs, including personnel to distribute and reimburse for vouchers, marketing to make voucher availability known, and downstream costs of further tests and CRC treatment, if no other resources are available.
37

Intervention Cost Break Down
Intervention Cost Components Base ($) Notes
Medicaid Mailed Reminder
Develop registry & reminder content (one-time)
$10,000 Programmer and physicians’ time
Programming time to identify enrollees $200 / year
Materials (postage, paper, ink) $0.71 / reminder
Mail reminders $3,850 / year 200 hours staff time
Endoscopy Expansion
Financial incentive to locate facility in underserved areas
$500,000 / facility
Mass Media Content development (one-time) $368,000 From campaign promoting seat belt use
Advertising purchase of month long campaign
$332,000 / year
Voucher for uninsured
Voucher for colonoscopy $750 / person 2013 Medicare physician fee schedule
38

Secondary outcomes: Intervention cost, impact, and efficiency in preventing CRC deaths and saving life years
Undiscounted:
Intervention Cost
CRC Deaths averted
Intervention cost per CRC Death averted
Fewer Life-Years Lost to
CRCMailed Reminder $1,619,578 86 $18,823.00 778
Endoscopy Expansion $3,000,000 7 $291,666.67 45
Mass Media $3,694,800 96 $38,487.50 801
Voucher for Uninsured $3,750,000 28 $134,099.62 337
Combination scenarios:
Mailed reminder + Mass media $5,302,918 182 $29,142.05 1,603
Mailed reminder + Mass media + Voucher
$9,049,371 213 $42,595.74 1,970
All interventions $12,047,517 219 $55,028.58 2,032

Aim 2 Rationale
• Better understanding of the preferences of vulnerable populations may allow design of more effective and efficient programs to encourage screening
• Discrete choice experiment (DCE) is one technique for eliciting preferences about “products” such as screening programs
• Objective: To understand preferences of vulnerable populations with regard to CRC screening program design

Aim 2 Methods
• Paper survey with embedded DCE
– Attributes and levels drafted from literature review and prior research
– Formative research and pilot testing
• Selected communities with low CRC screening rates, high CRC mortality, and sparse screening infrastructure:
• Community-based recruitment and data collection
• Purposeful sampling: targeted low income, unscreened, uninsured individuals ages 50-75

CRC screening programs- attributes and levels
Attribute Levels
Program Testing Options Stool Test onlyColonoscopy onlyChoice of Stool Test or ColonoscopyChoice of Stool test, Colonoscopy or CT Colonography
Travel Time No Travel Time15 Minutes30 Minutes45 Minutes1 Hour or More
Money Paid for Screening $1000 Copay$100 Copay$25 Copay$0$10 Reward$100 Reward
The Portion of the Cost of Follow-up Care You Pay
0%5%20%50%100%

Participant Characteristics
N=150
Mean Age (SD) 57.9 (6.2)
% Female 55%
% White 76%
% HS education or less 40%
% Household Income < $30,000 87%
% Never screened for CRC 76%
% Uninsured 51%
Need help reading (sometimes or more) 17%

DCE(Comparison Questions)
Attribute Level Meanutilities
AttributeImportance
Test Choice FOBT onlyCOLO onlyChoice FOBT OR COLOChoice: FOBT, COLO OR CT
0.601-0.418-0.6130.429
0.140(0.128, 0.151)
Travel Time No Travel15 minutes30 minutes45 minutes1 hour +
1.0300.9170.320-0.960-1.307
0.131(0.122, 0.140)
Money Paid for Screening $100 Reward$10 Reward$0$25 Copay$100 Copay$1000 Copay
2.494-0.0600.2941.081-0.148-3.661
0.274(0.260, 0.287)
% Follow-up Care Cost You Pay
0%5%20%50%100%
2.7881.6820.422-1.478-3.415
0.283(0.262, 0.304)
None Given these options, I would not get screened -3.191 0.170
(0.154,0.186)

-5-4-3-2-101234
0 20 40 60 80 100
% Follow-Up Cost
Utilities
-5-4-3-2-101234
0 20 40 60
Travel
-5-4-3-2-101234
-1000 -800 -600 -400 -200 0 200
Money Paid for Screening
-5-4-3-2-101234 Choice
1 Choice: 1 Choice: 2 Choices: 3 Choices: FOBT Colonoscopy FOBT or COLO FOBT, COLO, CT

DCE-based most important attributes
N (%)
Testing options 9 (6%)
Travel time 1 (1%)
Screening test costs / rewards
50 (33%)
Follow-up care costs 71 (47%)
No testing 19 (13%)
Total 150

Aim 2 Implications
• Vulnerable adults generally prefer some form of CRC screening program
• Screening programs should offer low-cost options and cover follow-up costs (travel time not very important)
• Aim III uses modeling to compare cost-effectiveness of different options for reaching vulnerable adults with CRC screening