Embed Size (px)
Citation preview

Familial aggregation of Bicuspid Aortic Valve: is it useful a family screeninng?
Amelia Carro, Gisela Teixidó, Francesca Huguet, María Sanz, Antonio Barros, Artur Evangelista, David García-Dorado
Cardiovascular Diseases. Aortic Pathology
6th VHIR Scientific Session
29th-30th November 2012
Vall d’Hebron University Hospital

Most common congenital heart disease1 (0.5-1%; male predominance 3:1)
High morbility
-Valvular dysfunction /Infectious endocarditis
-Aortic complications
Familial or sporadic
Associated malformations
Introduction: Bicuspid aortic valve
Nistri et al. Am J Cardiol 2005;96(5):718-721
Type 1 Type 2 Antero-posterior Right-left

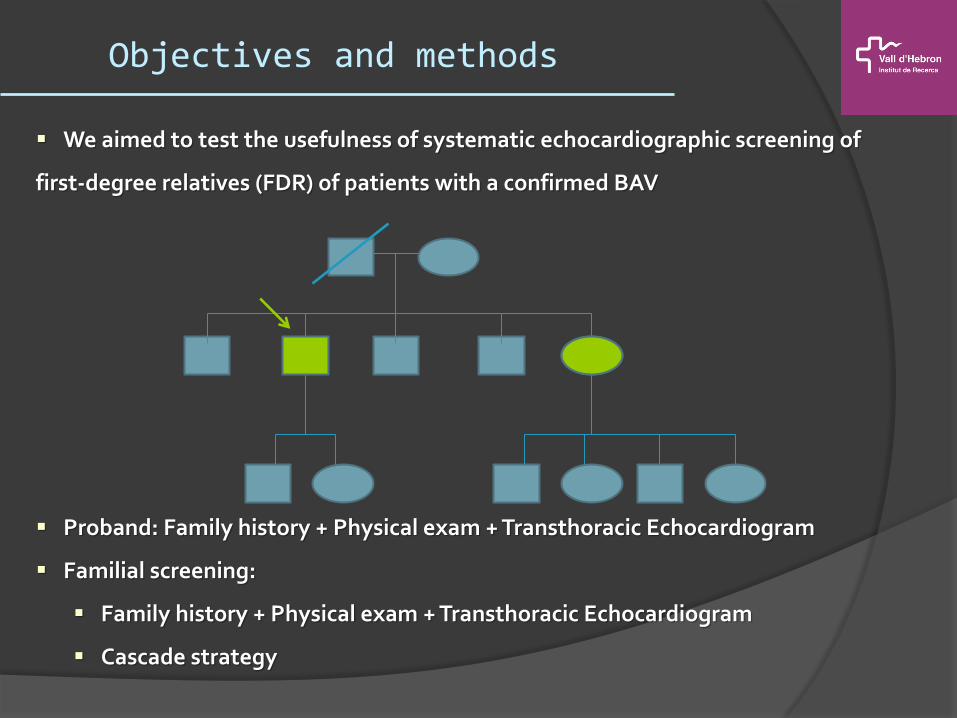
We aimed to test the usefulness of systematic echocardiographic screening of
first-degree relatives (FDR) of patients with a confirmed BAV
Proband: Family history + Physical exam + Transthoracic Echocardiogram
Familial screening:
Family history + Physical exam + Transthoracic Echocardiogram
Cascade strategy
Objectives and methods
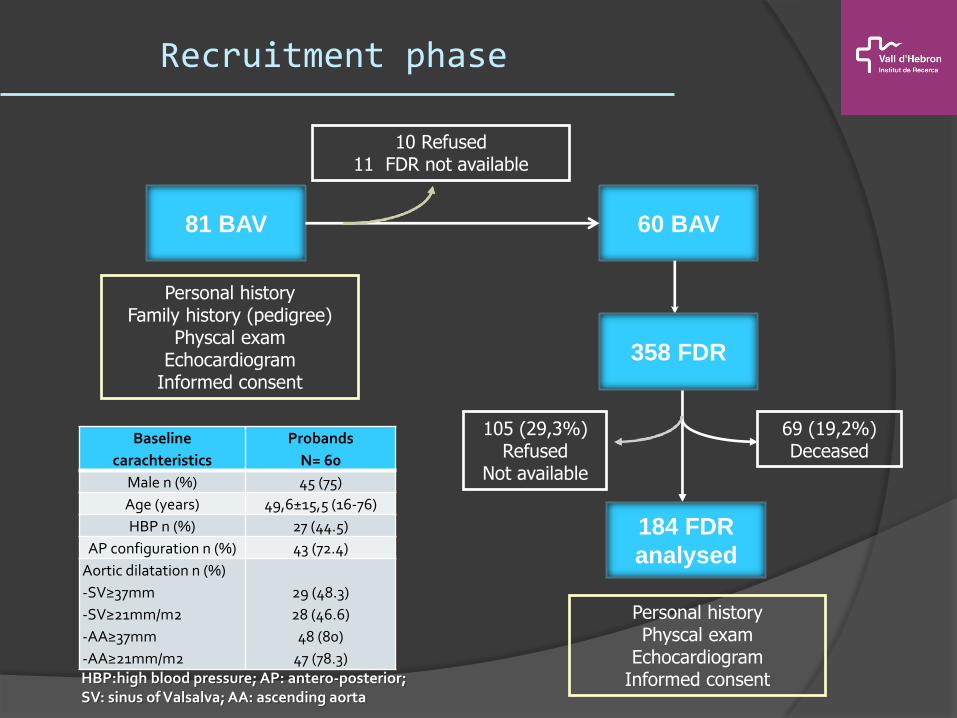
60 BAV
Personal history Family history (pedigree)
Physcal exam Echocardiogram
Informed consent
69 (19,2%) Deceased
105 (29,3%) Refused
Not available
184 FDR
analysed
81 BAV
10 Refused 11 FDR not available
Recruitment phase
Personal history Physcal exam
Echocardiogram Informed consent
358 FDR
Baseline
carachteristics
Probands
N= 60
Male n (%) 45 (75)
Age (years) 49,6±15,5 (16-76)
HBP n (%) 27 (44.5)
AP configuration n (%) 43 (72.4)
Aortic dilatation n (%)
-SV≥37mm
-SV≥21mm/m2
-AA≥37mm
-AA≥21mm/m2
29 (48.3)
28 (46.6)
48 (80)
47 (78.3) HBP:high blood pressure; AP: antero-posterior; SV: sinus of Valsalva; AA: ascending aorta

358 FDR
11 AoV abnormalities
184 FDR
analysed
Probands FDR
N 60 184
Male n (%) 45 (75) 94 (55.1)
Age (years) 49,6±15,5 (16-76) 43.1±19.2 (8-91)
HBP n (%) 27 (44.5) 42 (22.8)
Diabetes n (%) 4 (6.6) 35 (19)
Dislipemia n (%) 22 (36.6) 35 (19)
Aortic Dilatation n (%)
-SV≥37mm
-SV≥21mm/m2
-AA≥37mm
-AA≥21mm/m2
29 (48.3)
28 (46.6)
48 (80)
47 (78.3)
26 (14.1)
22 (11.9)
26 (14.1)
24 (13)
FDR: first degree relatives; HBP:high blood pressure; SV: sinus of Valsalva; AA: ascending aorta; AoV: aortic valve
FDR prevalence: 5.9% Familial prevalence: 16.6%
Necessary Number of FDR to screen:13
Distributed in 10 families
Results (1)
60 BAV

FDR: first-degree relative; AP: Antero-posterior; RL: Rigth-left; M: male; F: female; AoR: aortic regurgitation; AoS: aortic stenosis
Results (2)
Relation to proband
Proband phenotype
FDR phenotype Age Gender Symptoms Valve function
1 Son AP
Quadricuspid 16 M No Normal
2 Son RL 10 M No Mild AoR
3 Son AP AP 31 M No Mild AoR
4 Son AP AP 22 M No Mild AoR
5 Son AP AP 10 M No Normal
6 Brother AP AP 57 M No Mild AoR
7 Sister AP AP 48 F No Mild AoR
8 Father RL Unreadable 61 M Dyspnea Severe AoR
9 Mother RL RL 56 F No Moderate AoR
10 Father RL RL 59 M No Mild AoR
11 Uncle AP Unreadable 90 M Dyspnea Moderate AoS + AoR
Male predominance 4:1 Antero-posterior 60%
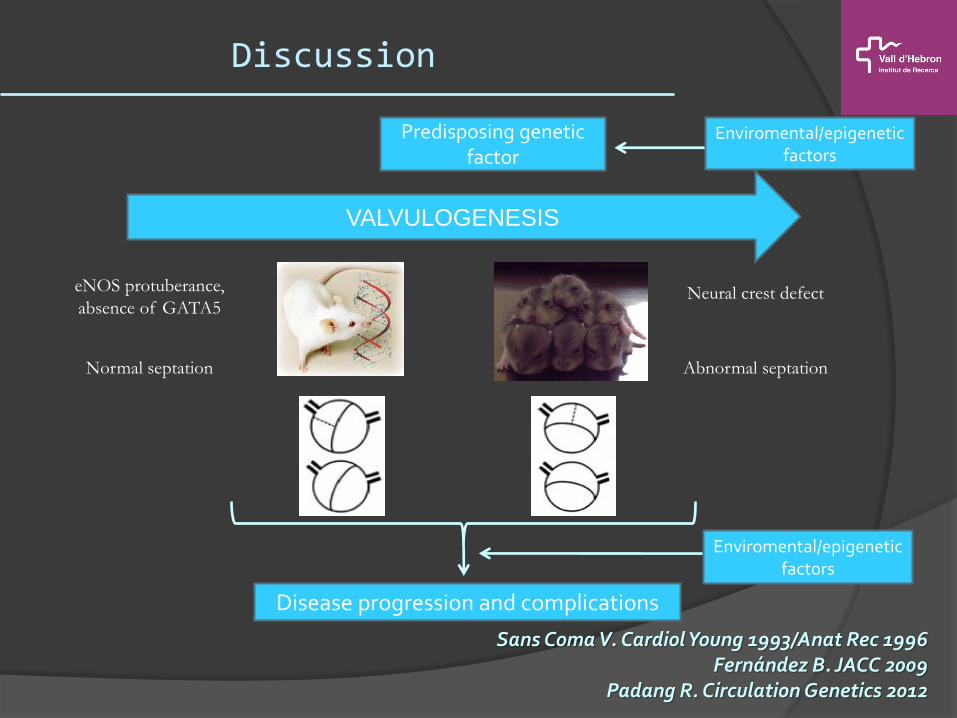
Discussion
Sans Coma V. Cardiol Young 1993/Anat Rec 1996 Fernández B. JACC 2009
Padang R. Circulation Genetics 2012
VALVULOGENESIS
Predisposing genetic factor
eNOS protuberance,
absence of GATA5 Neural crest defect
Abnormal septation Normal septation
Disease progression and complications
Enviromental/epigenetic factors
Enviromental/epigenetic factors

Discussion
Valvulopatí
a Aortopatí
a
Malf
asociada
s
Calloway T. Am J Med Genet 2011 Sans Coma V. J Anat 2012

Conclusions
The prevalence of bicuspid aortic valve is higher in first-degree relatives of
affected patients than in the general population.
Echocardiographic screening of first-degree relatives is a useful approach for
identifying asymptomatic cases, and should therefore be offered to all first-degree
relatives of bicuspid aortic valve individuals.
Different patterns of aortic valve configuration within the same family reinforce
the complexity of inheritance and deserve furhter investigation.

THANK YOU VERY MUCH!















![Effect of Bicuspid Aortic Valve Cusp Fusion on Aorta Wall ...The congenital bicuspid aortic valve (BAV) is a valvular defect present in 1% - 2% of the general population[1]. While](https://img.pdfslide.net/doc/110x75/5f34ae6844f7a3568d255217/effect-of-bicuspid-aortic-valve-cusp-fusion-on-aorta-wall-the-congenital-bicuspid.jpg)












