Embed Size (px)
Citation preview
Familial Lissencephaly With Cleft Palate andSevere Cerebellar Hypoplasia
Berit Kerner,1 John M. Graham, Jr.,1* Jeffrey A. Golden,2 Samuel H. Pepkowitz,3 andWilliam B. Dobyns4
1Medical Genetics Birth Defects Center, Ahmanson Department of Pediatrics, Steven Spielberg Pediatric ResearchCenter, SHARE’s Child Disability Center, UCLA University Affiliated Program, International Skeletal DysplasiaRegistry, UCLA School of Medicine, Cedars-Sinai Medical Center, Los Angeles, California
2Department of Pathology, Children’s Hospital of Pennsylvania and the University of Pennsylvania School ofMedicine, Philadelphia, Pennsylvania
3Department of Pathology, Cedars-Sinai Medical Center, Los Angeles, California4Department of Human Genetics, University of Chicago, Chicago, Illinois
Lissencephaly is a brain malformation char-acterized by absence of gyral formation, re-sulting in a smooth brain surface. Histologicstudy shows severe anomalies of cerebralcortical development. Several lissencephalysyndromes have been described. Here we re-port a familial syndrome of lissencephaly,cleft palate, diffuse agyria, and severe cer-ebellar hypoplasia. Microscopic examina-tion of the abnormally thick cerebral cortexshowed absence of cortical layering, withpreservation of the pia-glial barrier. This isthe first report of recurrent lissencephalywith cleft palate and severe cerebellar hy-poplasia in which these unique neuropa-thology findings are described. Autosomalrecessive inheritance is suggested by recur-rence in sibs within the same family, butgerm cell mosaicism for a dominant muta-tion is not excluded. Am. J. Med. Genet.87:440–445, 1999. © 1999 Wiley-Liss, Inc.
KEY WORDS: lissencephaly; cerebellar hy-poplasia; cerebral cortex ab-normality; cleft palate; ge-netic abnormality; autosomalrecessive lethality
INTRODUCTION
Cortical malformations are relatively common. Cor-tical development involves many highly coordinatedevents, one of which is extensive cell migration.Anomalous cell migration is thought to be the under-lying pathogenesis of more than 25 cortical malforma-tion disorders [Dobyns and Truwit, 1995]. Lissen-cephaly is the most severe and best known entityamong these disorders. Here, we report on 2 sibs withlissencephaly, cleft palate, diffuse agyria, complex mal-formation of the midbrain and hindbrain, a near com-plete absence of the corticospinal tracts, and subtotalabsence of the cerebellum. To our knowledge, this is thefirst report of sibs with this syndrome.
CLINICAL REPORTS
The fetal pathology service at Cedars-Sinai MedicalCenter was asked to examine a male fetus (Case 2)after termination of pregnancy because of recurrence ofsevere intrauterine growth retardation, enlarged ven-tricles, microcephaly, and striking hypoplasia of thecerebellum detected on ultrasound.
Family History
Case 2 was the fifth pregnancy born to a 27-year-oldwoman and her 28-year-old partner, both of AfricanAmerican descent, with four previous pregnancies andno living children; consanguinity was denied. Theirfirst pregnancy ended in miscarriage at 6 weeks. Thesecond child was delivered by cesarian section at 35weeks of gestation after fetal brain anomalies had beennoted by ultrasound. This infant girl died on Day 1with a cleft palate, lissencephaly, and severe cerebellarhypoplasia (Case 1). Because the lissencephaly wassuspected to have a genetic basis, prenatal diagnosiswas offered during subsequent pregnancies, and thenext two pregnancies were terminated at 20 and 24weeks because prenatal ultrasonography at othermedical centers suggested possible anomalies thatcould not be confirmed at autopsy. Their fifth preg-
Contract grant sponsor: SHARE’s Child Disability Center; Con-tract grant sponsor: Steven Spielberg Pediatric Research Center;Contract grant sponsor: National Institutes of Health; Contractgrant number: GM08243; Contract grant sponsor: U.S. Depart-ment of Health and Human Services; Contract grant number:P01 HD22657–06.
*Correspondence to: John M. Graham, Jr., M.D., Sc.D., Direc-tor of Clinical Genetics and Dysmorphology, Cedars-Sinai Medi-cal Center, 444 South San Vicente Blvd. #1001, Los Angeles, CA90048. E-mail: [email protected]
Received 14 April 1999, Accepted 27 August 1999
American Journal of Medical Genetics 87:440–445 (1999)
© 1999 Wiley-Liss, Inc.

nancy (Case 2) resulted in a male fetus with anomaliesidentical to those seen in their earlier pregnancy (Case1).
Case 1. This infant girl was born by cesarian sec-tion because of suspected hydrocephalus at 35 weeks.The pregnancy history was unremarkable until 32weeks, when prenatal ultrasosonography demon-strated increased size of the fetal lateral ventricleswith normal biparietal diameter (BPD). The fetus hada normal female karyotype, and repeat ultrasoundstudies showed progressive cortical thinning. Apgarscores were 6 and 7 at 1 and 5 min, respectively. Birthweight was 1.8 kg (3rd centile), length 43 cm (3rd cen-tile), and head circumference (OFC) was 30 cm (3rdcentile). Cleft palate, bilateral simian creases, and longthumbs and halluces were noted on physical exam. Thechild exhibited abnormal posturing and limb move-ments. Cranial ultrasound study demonstrated an ap-parently normal brainstem with dilated ventricles andabsent corpus callosum. A skeletal survey was normal.The baby died 1 day after delivery due to severe brainmalformations and hyaline membrane disease. Exter-nal examination of the brain at the Armed Forces In-stitute of Pathology showed nearly complete absence ofcerebral gyration and an absent cerebellum. Rudimen-tary primary sulci were found only in the region of theSylvian fissures and central sulci. The brainstem ap-peared flattened in the dorsal–ventral axis, and later-ally two membranous attachments were found nearwhere the cerebellum should have been. Sections of thebrain demonstrated that the cortex was abnormallythick (approximately 1 cm compared to normal cortical
thickness of approximately 3 mm). The lateral ven-tricles were greatly dilated. The aqueduct was patent.The pons and medulla appeared normal on gross ex-amination. No other visceral abnormalities were found.
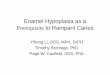
The microscopic examination (J.A.G.) confirmed thediagnosis of lissencephaly. The leptomeninges weredelicate and contained no cellular infiltrate or evidenceof leptomeningeal heterotopia, which excluded cobble-stone (type II) lissencephaly as a possible diagnosis.The cerebral cortex was abnormally thick and showedmarked disorganization of development in all sampledregions. The molecular layer (layer 1) of the cerebralcortex was relatively well preserved with no apparentincreased population of cells; however, Cajal-Retziuscells were not identified within the molecular layer.The remainder of the cortical thickness showed no ob-vious lamination and a heterogenous population ofneurons (Fig. 1). Numerous neurons had a ballooned topyramidal shape; however, those with a pyramidalshape were malaligned, not showing the normal pial-directed orientation of pyramidal neurons (Fig. 1). Theremaining neurons consisted of intermediate size tosmall neurons in no apparent laminar organization.The underlying white matter was thin, with an ap-proximate ratio of cortex to white matter of 5 or 6:1(normal 1:10). There were several small collections ofheterotopic neurons in the cerebral white matter; how-ever, this was not a prominent aspect of the pathologicchanges. The cerebral white matter and cortex showedmild to moderate fibrillary gliosis.
Sections of the midbrain showed a normally devel-oped cerebral aqueduct. The third nerve nucleus was
Fig. 1. Immunohistochemistry using an antibody to neurofilament protein highlights the marked disorganization of the cerebral cortex. A: A lowpower view of the cerbral cortex. The surface of the brain is to the top (pia4pia arachnoid) and the ventricle is to the bottom. The thickness of themolecular layer (ML) is defined by black bars, as is the thickness of the white matter (WM). Between the ML and the WM is the cerebral cortex. Largepyramidal type neurons are scattered randomly throughout the cortex (brown cells). No evidence of lamination is present. B: High power view ofdysplastic pyramidal neurons showing disorganization of the dendritic processes. (Scale bar is 500 mm for panel A and 50 mm in panel B.)
Lissencephaly with Cerebellar Hypoplasia 441

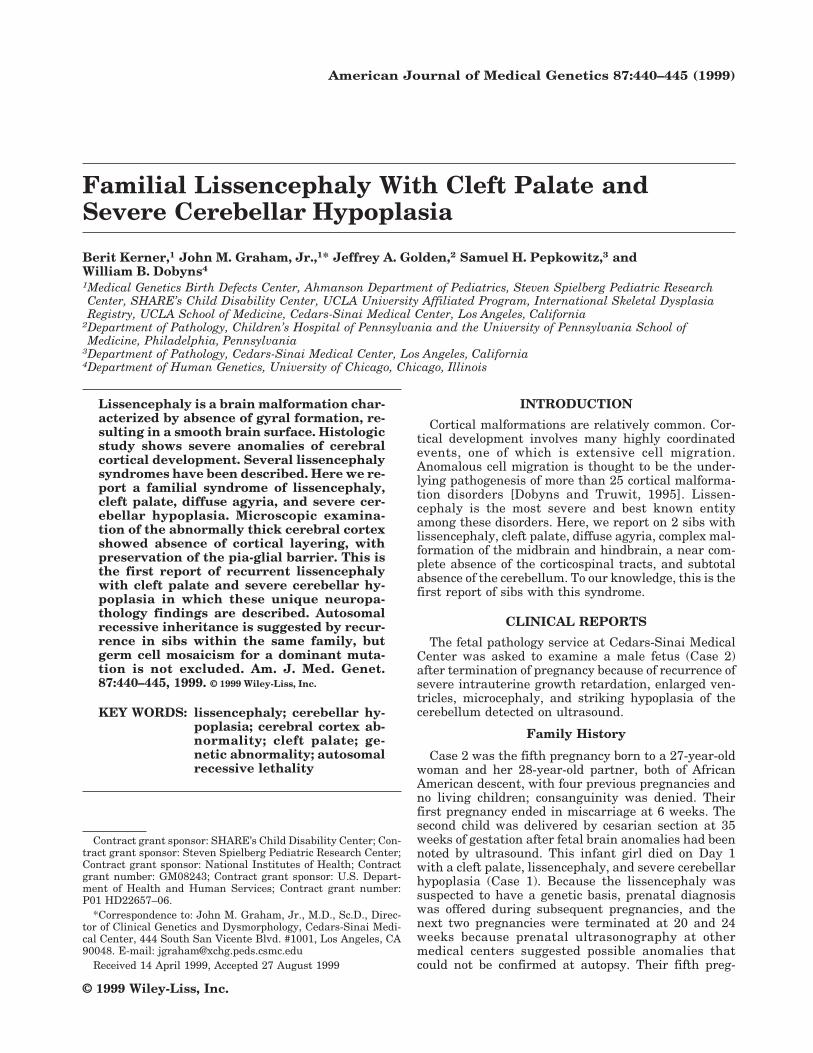
intact and showed normal myelinated third nerve fi-bers exiting the midbrain. The fourth nerve nucleusand fibers of the fourth nerve were also identified. Allother structures of the midbrain were markedly disor-ganized. The collicular plate was underdeveloped andneither the superior nor the inferior colliculus wasclearly identified. The substantia nigra was underde-veloped, although some neurons consistent with nigralneurons were present. The nucleus ruber was identi-fied and largely unremarkable. The cerebral pyramidswere hypoplastic and somewhat displaced into the me-dial proportions of the midbrain. In the ventral aspectof the inferior midbrain, several large nodules of het-erotopic gray matter with no clear origin from withinthe midbrain were seen in the inferior, ventral mid-brain (Fig. 2).
A section of the pons showed disorganization of thetegmentum and the basis pontis. The basis pontis wasmarkedly devoid of neurons and the descending corti-co–spinal tract was not well formed. The tegmentumdid not show obvious nuclear organization with the ex-ception of a laterally placed nucleus, which may repre-sent either the 6th nerve nucleus or a medialy placedprincipal nucleus of the trigeminal nerve, although de-finitive identification was impossible. The medulla washighly disorganized with no clear corticospinal tracts,no evidence of inferior olivary nuclei, and absence ofthe 12th nerve nuclei. The dorsal motor nucleus of the10th cranial nerve was underdeveloped, but present.
Lateral and dorsal to the pons were the cerebellarrudiments that showed evidence of external and inter-
nal granular neurons indicating that some degree ofmigration had occurred. The Purkinje cells were alsopresent. This tissue was markedly gliotic, suggestingthat there had been secondary disruption of the cer-ebellum; however, the pathogenesis of the near com-plete aplasia of the cerebellum could not clearly beidentified on the pathologic slides available.
The third pregnancy was terminated at 20 weeks ofgestation for suspected malformations. Pathologyexam was performed at the Armed Forces Institute ofPathology. There was no cleft palate, and microscopicsections of the fetal brain showed a rudimentary six-layered cortex and germinal matrix tissue compatiblewith a 20-week gestation fetus. Sections of brainstemand spinal cord were unremarkable. The amniocentesiskaryotype was 46,XX.
The fourth pregnancy was followed at another ter-tiary care center where ultrasonography at 18.5 weekswas normal, but follow-up ultrasonography at 23.5weeks suggested ventriculomegaly thought to repre-sent a recurrence, and the pregnancy was terminatedat 24.5 weeks. Autopsy evaluation of this infant girl ata local medical center showed a crown–heel length of32.5 cm with weight of 632 g and intact palate. Thebrain weighed 32 g, and sections of cerebral and cer-ebellar cortex appeared orderly. Chromosomes ap-peared normal (46,XX) and no gross cytogenetic dele-tion of chromosome 17p was evident.
Case 2. This 28-week male fetus (by dates),weighed 425 g (50th centile for a 22- to 23-weeks’ ges-tation fetus). Crown–heel length measured 33.5 cm(50th centile for a 26-weeks’ gestation fetus), and thecrown–rump length was 21.5 cm. Thus, the child ap-peared underweight for length. The OFC could not bedetermined with accuracy due to pregnancy termina-tion via dilatation and evacuation with cephalocente-sis. The thorax and abdomen measured 18 cm and 18.5cm, respectively (50th centile for a 25-weeks’ gestationfetus). Ears were abnormal with thickened, rounded,and overfolded superior helices (Fig. 3). The corneaeappeared large with asymmetrically dilated pupils.There was a V-shaped cleft of the hard and soft palate.The limbs appeared relatively deficient in muscula-ture. There was bilateral fifth finger clinodactyly, withabsent distal finger creases on Digits 2 through 5 andhypoplastic palmar creases, more so on the right thanon the left. There were rocker-bottom feet bilaterally,and the external genitalia were male with undescendedtestes. The cord stump was positioned normally, butwas thick and “rubbery.”
The internal findings were unremarkable with theexception of a mildly decreased muscle mass through-out, and early ossification of the vertebrae. All organsexcept the brain were normal, including the eyes. Ex-amination of the brain was limited to the spinal cord,brainstem, and fragments of the cerebral hemispheres.Sections of the spinal cord from multiple levels showeda normal organization of the grey and white matterwith normal populations of anterior horn cells. The lat-eral corticospinal tracts were extremely small. Thebrainstem was small and the nuclear organizationmarkedly disrupted. The dorsal nuclei could not be de-fined and the inferior olivary nuclei were disorganized
Fig. 2. Section of the midbrain showing a large heterotopian in theventral region (outlined in black dots). The cerebral aquaduct (Aq) is in theupper right corner. (Scale bar is 500 mm.)
442 Kerner et al.

showing no dentiforme architecture. The medullarypyramids were markedly hypoplastic. The pons showeda disorganization similar to that of the medulla. Nocerebellar tissue was present, although several frag-ments of pial-lined cystic structures were found. Theorigin of these remnants remains unknown; however,they may represent the cerebellar remnants. Alterna-tively, they could be the membranes over the foraminaof Luschka. The disrupted architecture precluded de-finitive determination. The cerebral cortex showedmarked distortion of the neurons with severe shrink-age as a result of the termination procedure. Althoughwe were unable to assess cellular details, the cerebralcortex architecture was preserved and markedly thick-ened, and the findings closely resembled those in Case1. In addition, a small fragment of periventricular tis-sue was identified, most likely representing the thala-mus or hypothalamus. This tissue showed clusters ofdisorganized neurons indicative of dysplasia.
Chromosome analysis on cultured skin fibroblastsshowed a normal male karyotype with no deletions of17p13 by fluorescent in situ hybridization. Sections ofthe brainstem were stained for the presence of the L1cell adhesion molecule (L1CAM), which is absent inX-linked hydrocephalus, X-linked spastic paraplegia,and MASA syndrome [Jouet et al., 1994]. No signal wasdetected in the brainstem, whereas nearby tissue rep-
resenting peripheral nerves stained well with anti-L1antibodies on approximately 20% of the fibers.
DISCUSSION
We report on 2 sibs with a previously undescribedconstellation of anomalies including cleft palate andsevere disruption of cerebral cortical developmentknown as lissencephaly. Lissencephaly refers to thesmooth, agyric surface of the brain. Histologically, lis-sencephaly may demonstrate a variety of abnormali-ties; however, all implicate disruption of cell migrationas the pathogenesis.
Progenitor cells for the cerebral cortex reside adja-cent to the ventricular surface deep within the brain ina region known as the ventricular zone [Sidman andRakic, 1973]. As cells exit the cell cycle they migratefrom inside the brain toward the outside, where theyreside as mature neurons [McConnell, 1995]. In hu-mans, this migration begins at approximately 7 weeksof gestation. The major pathway of cell migration intothe cerebral cortex is radially, from the inside to theoutside of the cerebral wall [Rakic, 1990]. Specializedglial cells, known as radial glia, guide cell migrationalong this pathway. Many molecules have been shownto participate in guiding neurons along radial glial fi-bers [Pearlman et al., 1998; Rakic et al., 1994]. These
Fig. 3. Case 2 at 26 weeks of gestation. The fetus appeared kachectic with underdeveloped musculature and rocker-bottom feet bilaterally. Thickenedand rounded helices and a V-shaped cleft of the hard and soft palate were the major anomalies present.
Lissencephaly with Cerebellar Hypoplasia 443

include extracellular matrix molecules, cell surface re-ceptors, and cell surface and secreted ligands. Disrup-tion of normal neuronal cell migration can result in avariety of brain disorders such as lissencephaly andsubcortical heterotopia (agyria–pachygyria–subcorti-cal heterotopia “spectrum”), polymicrogyria and nodu-lar heterotopia [Dobyns and Truwit, 1995].
Classical lissencephaly (or type 1 lissencephaly) ap-pears to result from a migratory defect between the 9thand 13th weeks of gestation. Consequently, the cere-bral cortex is abnormally thick and generally organizedinto four layers. Genetic and molecular studies havebegun elucidating the cause of lissencephaly in somepatients. Haploinsufficiency of LIS1, on chromosomeband 17p13.3, was recently found to cause this disorder[Dobyns et al., 1993; Lo Nigro et al., 1997; Reiner et al.,1993]. This gene encodes the non-catalytic beta subunitof the platelet activating factor (PAF) acetylhydrolase[Hattori et al., 1994]. The brain isoform of this enzymeinactivates PAF, which in high concentrations can in-hibit neuronal movement [Clark et al., 1995; Korneckiand Ehrlich, 1988]. It has been shown that LIS1 cansuppress microtubule dynamics by interaction with tu-bulin [Sapir et al., 1997]. Recently, LIS1 mutant micehave demonstrated a unique and important role ofLIS1 in neuronal migration [Hirotsune et al., 1998].
An X-linked lissencephaly syndrome has also beendescribed in which affected males present with a phe-notype resembling classical lissencephaly and affectedfemales display subcortical band heterotopia or doublecortex [Berg et al., 1998; Dobyns et al., 1996]. The genefor X-linked lissencephaly and double cortex wasmapped to Xq22.3-Xq23 and was recently cloned [desPortes et al., 1998; Dobyns et al., 1992; Gleeson et al.,1998]. Protein homology suggests a role for this geneproduct in intracellular calcium-dependent signalingpathways [Sossey-Alaoui et al., 1998].
Microlissencephaly is a severe, neonatally lethalmalformation characterized by congenital microcepha-ly resulting from hypoplasia of the cerebral cortex andcerebellum, with the term brain weight usually below50 g compared to 250 g for an 1800-g baby [Barth et al.,1982). This syndrome seems to be an autosomal reces-sive trait and resembles classical lissencephaly in thatthe cortex has only four layers. In contrast to theformer, the neopallidum is thinner than normal (0.2–3mm). The brainstem and cerebellum are severely un-derdeveloped and dysplastic. The optic nerves are un-derdeveloped, the olfactory nerves absent, the cerebralcommissures missing, and the thalami described asstreaklike. The underlying defect is unknown.
Cobblestone lissencephaly (type II lissencephaly) isthought to result from a failure to inhibit the migrationof neurons at the pial barrier [Squier, 1993]. This re-sults in glial and neuronal ectopia in the leptomenin-ges, and complete absence of cortical layers. Markedvascular and connective tissue proliferation is charac-teristic of this disorder. In contrast to classic lissen-cephaly, the early stages of neuronal migration seem tobe intact. The molecular defect in cobblestone lissen-cephaly is presently unknown.
An entity known as lissencephaly with cerebellar hy-poplasia most closely resembles that present in our
cases. In this malformation syndrome, a near-normalhead circumference is found at birth and the hypopla-sia of the brain is limited to the cerebellum. A smoothcerebral surface results from generalized agyria–pachygyria; however, no information concerning the cy-toarchitecture of the cortex has been reported in anypublished cases. The cases presented herein have sev-eral findings in common with this malformation:nearly normal head circumference for gestational age,cerebellar hypoplasia (although secondary degenera-tion has not been excluded), and complete absence ofcortical gyration. The abnormally thick, dysplastic cor-tex, with preservation of layer 1 but no other evidenceof lamination distinguishes our case from classical lis-sencephaly and microlissencephaly, in which layerscan be distinguished. Some resemblance of our case canbe found to a case with cleft palate, lissencephaly, ab-normally thin cortex, and extreme cerebral and cer-ebellar hypoplasia published by Kroon et al. [1996].Our cases differ from this case in near-normal headsize at birth, an abnormally thick cortex, and hypopla-sia limited to the cerebellum. No brain pathology waspresented in that case, limiting comparison of thesetwo cases. Another recent report described a Bedouinkindred with cerebellar hypoplasia and myoclonic epi-lepsy [Farah et al., 1997]. No autopsy findings werereported.
The brain in our cases showed numerous and com-plex malformations. Starting in the most rostral part ofthe brain, there was a diffuse malformation of the ce-rebral cortex. The pial–glial boundary and the molecu-lar layer were both preserved, but the remainder of thecerebral cortex showed no lamination, and layers IIthrough VI of the cerebral cortex could not be delin-eated. Instead, the cortical plate was composed of adisorganized band of neurons and glia. White matterhetertopia were not prominent in these cases. The ratioof five to six times as much cerebral cortex to whitematter with an intact pial surface and molecular layeris most similar to classical lisssencephaly and pre-cludes cobblestone (type II) lissencephaly. In classicallissencephaly, four layers can usually be identified inthe cerebral cortex including the molecular layer, a su-perficial largely pyramidal layer, a narrow band of my-elinated cortex, and then an extremely thickened anddisorganized band of cells. Our cases showed only themolecular layer and then a diffuse band of disorganizedneurons and glia. The midbrain and hindbrain anoma-lies did not fit into any recognizable pattern. The mal-formations included abnormal organization of thenuclear structure as well as disorganization of whitematter tracts, including absence of some tracts. Thecerebellar changes were difficult to place into anypathogenetic category. They potentially represent aprimary malformation of the cerebellum; however, asecondary degeneration of the cerebellum could not beexcluded.
The fact that a boy and girl were affected within thesame family suggests autosomal recessive inheritance,though germ cell mosaicism of an autosomal dominanttrait cannot be excluded. Cerebellar hypoplasia can bedetected on prenatal ultrasound prior to 24 weeks ofgestation and can facilitate a prenatal diagnosis. To
444 Kerner et al.

our knowledge, this is the first report of this inherited,neonatally lethal syndrome with cleft palate, lissen-cephaly, and cerebellar hypoplasia, in which completeabsence of a layered cortical structure was found.
ACKNOWLEDGMENTS
We are indebted to Dr. Vance Lemmon, Ph.D. of CaseWestern Reserve School of Medicine for providing an-tibodies to stain for LI, and we appreciate autopsyevaluations by Dr. R.E. James of Ventura CountyMedical Center, and by Drs. Robert McMeeken, RobertKarnei, Joseph Parisi, and Michael Kanzer of theArmed Forces Institute of Pathology. We appreciatethe generous support of SHARE’s Child Disability Cen-ter and the Steven Spielberg Pediatric Research Cen-ter. In addition, this work was supported by the UCLAIntercampus Training Program Grant GM08243 fromthe National Institutes of Health, and Grant P01HD22657–06 from the U.S. Department of Health andHuman Services, Public Health Service.
REFERENCESBarth PG, Mullaart R, Stam FC, Slooff JL. 1982. Familial lissencephaly
with extreme neopallial hypoplasia. Brain Dev 4:145–151.
Berg MJ, Schifitto G, Powers JM, Martinez-Capolino C, Fong CT, MyersGJ, Epstein LG, Walsh CA. 1998. X-linked female band heterotopia-male lissencephaly syndrome. Neurology 50:1143–1146.
Clark GD, McNeil RS, Bix GJ, Swann JW. 1995. Platelet-activating factorproduces neuronal growth cone collapse. Neuro Report 6:2569–2575.
des Portes V, Pinard JM, Billuart P, Vinet MC, Koulakoff A, Carrie A,Gelot A, Dupuis E, Motte J, Berwald-Netter Y, Catala M, Kahn A,Beldjord C, Chelly J. 1998. A novel CNS gene required for neuronalmigration and involved in X-linked subcortical laminar heterotopia andlissencephaly syndrome. Cell 92:51–61.
Dobyns WB, Andermann E, Andermann F, Czapansky-Beilman D, DubeauF, Dulac O, Guerrini R, Hirsch B, Ledbetter DH, Lee NS, Motte J,Pinard JM, Radtke RA, Ross ME, Tampieri D, Walsh CA, Truwit CL.1996. X-linked malformations of neuronal migration. Neurology 47:331–339.
Dobyns WB, Elias ER, Newlin AC, Pagon RA, Ledbetter DH. 1992. Causalheterogeneity in isolated lissencephaly. Neurology 42:1375–1388.
Dobyns WB, Reiner O, Carrozzo R, Ledbetter DH. 1993. Lissencephaly. Ahuman brain malformation associated with deletion of the LIS1 genelocated at chromosome 17p13. JAMA 270:2838–2842.
Dobyns WB, Truwit CL. 1995. Lissencephaly and other malformations ofcortical development: 1995 update. Neuropediatrics 26:132–147.
Farah S, Sabry MA, Khuraibet A, Khaffagi S, Rudwan M, Hassan M,Haseeb N, Abulhassan S, Abdel-Rasool MA, Elgamal S, Qasrawi B,
Al-Busairi W, Farag TI. 1997. Lissencephaly associated with cerebellarhypoplasia and myoclonic epilepsy in a Bedouin kindred: a new syn-drome? Clin Genet 51:326–330.
Gleeson JG, Allen KM, Fox JW, Lamperti ED, Berkovic S, Scheffer I,Cooper EC, Dobyns WB, Minnerath SR, Ross ME, Walsh CA. 1998.Doublecortin, a brain-specific gene mutated in human X-linked lissen-cephaly and double cortex syndrome, encodes a putative signaling pro-tein. Cell 92:63–72.
Hattori M, Adachi H, Tsujimoto M, Arai H, Inoue K. 1994. Miller-Diekerlissencephaly gene encodes a subunit of brain platelet-activating fac-tor. Nature 370:216–218.
Hirotsune S, Fleck MW, Gambello MJ, Bix GJ, Chen A, Clark GD, Led-better DH, McBain CJ, Wynshaw-Boris A. 1998. Graded reduction ofPafah1b1 (Lis1) activity results in neuronal migration defects andearly embryonic lethality. Nature Genetics 19:333–339.
Jouet M, Rosenthal A, Armstrong G, MacFarlane J, Stevenson R, PatersonJ, Metzenberg A, Ionasescu V, Temple K, Kenwrick S. 1994. X-linkedspastic paraplegia (SPG1), MASA syndrome, and X-linked hydroceph-alus result from mutations in the L1 gene. Nature Genetics 7:402–407.
Kornecki E, Ehrlich YH. 1988. Neuroregulatory and neuropathological ac-tion of the ether-phospholipid platelet-activating factor. Science 240:1792–1794.
Kroon AA, Smit BJ, Barth PG, Hennekam RCM. 1996. Lissencephaly withextreme cerebral and cerebellar hypoplasia. A magnetic resonance im-aging study. Neuropediatrics 27:273–276.
Lo Nigro C, Chong CS, Smith AC, Dobyns WB, Carrozzo R, Ledbetter DH.1997. Point mutations and an intragenic deletion in LIS1, the lissen-cephaly causative gene in isolated lissencephaly sequence and Miller-Dieker syndrome. Hum Mol Genet 6:157–164.
McConnell S. 1995. Constructing the cerebral cortex: neurogenesis andfate determination. Neuron 15:761–768.
Pearlman AL, Faust PL, Hatten ME, Brunstrom JE. 1998. New directionsfor neuronal migration. Curr Opin Neurobiol 8:45–54.
Rakic P. 1990. Principles of neural cell migration. Experientia 46:882–891.
Rakic P, Cameron R, Komuro H. 1994. Recognition, adhesion, transmem-brane signaling, and cell motility in guided neuronal migration. CurrOpin Neurobiol 4:63–69.
Reiner O, Carrozzo R, Shen Y, Wehnert M, Faustinella F, Dobyns WB,Caskey CT, Ledbetter DH. 1993. Isolation of a Miller-Dieker lissen-cephaly gene containing G protein b-subunit-like repeats. Nature 364:717–721.
Sapir T, Elbaum M, Reiner O. 1997. Reduction of microtubule catastropheevents by LIS1, platelet-activating factor acetylhydrolase subunit.Embo J 16:6977–6984.
Sidman R, Rakic P. 1973. Neuronal migration, with special reference todeveloping human brain: a review. Brain Research 62:1–35.
Sossey-Alaoui K, Hartung AJ, Guerrini R, Manchester DK, Posar A,Puche-Mira A, Andermann E, Dobyns WB, Srivastava AK. 1998. Hu-man doublecortin (DCX) and the homologous gene in mouse encode aputative Ca2+-dependent signaling protein which is mutated in humanX-linked neuronal migration defects. Hum Mol Genet 7:1327–1332.
Squier MV. 1993. Development of the cortical dysplasia of type II lissen-cephaly. Neuropathology and Applied Neurobiology 19:209–213.
Lissencephaly with Cerebellar Hypoplasia 445