Embed Size (px)
Citation preview


Familial Adenomatous
Polyposis• 1 in 10,000 incidence
• 100’s to 1000’s of colonic adenomas by teens
– Cancer risk: colon, gastric, duodenum (periampulla), small bowel, pancreas, papillary thyroid, childhood hepatoblastoma
• 7% risk of CRC by 21 yrs; 93% by 50 yrs
• Autosomal dominant: APC gene mutations
• Variants: Gardner (extracolonic), Turcot(medulloblastoma)


FAMILIAL ADENOMATOUS POLYPOSISFAMILIAL ADENOMATOUS POLYPOSIS

Inherited PolyposesFAP/Gardners

NORMAL MUCOSANORMAL MUCOSA

HYPERPLASTIC POLYP LINED BY BENIGN EPITHELIUMHYPERPLASTIC POLYP LINED BY BENIGN EPITHELIUM

TUBULOVILLOUS ADENOMATUBULOVILLOUS ADENOMA

INVASIVE ADENOCARCINOMAINVASIVE ADENOCARCINOMA
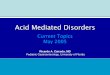
Rectal zone Sigmoid colon
“apple core” lesion of distal sigmoid: www.medlib.med.utah.edu/WebPathwww.medlib.med.utah.edu/WebPath

Inherited PolyposesFAP/Gardners
• Associated with mutation of the adenomatouspolyposis coli (APC) gene on chromosome 5 -encodes tumor suppressor gene
• Polyps appear usually in the second or third decade; malignant changes have occurred as young as 9 years of age
• Polyps are typically small and sessile; endoscopic resection difficult because of huge numbers

Inherited PolyposesFAP/Gardners
• Association with osteomas (skull), desmoids (intra-abdominal), or epidermoid cysts, along with small bowel tumors (those in duodenum have high malignant potential) : Gardners
• Association with medulloblastoma or glioblastoma : Turcots
• Each of the above shares the genetic defect with FAP.




Polyps and tumors
• Colon: Adenomas, less than 1 cm, multiple, numbers may correlatewith site of mutation
• Gastric: – Fundic retention polyps - - no malignant potential– Adenomatous polyps – probably malignant potential – but no
increased gastric Ca risk• Duodenum – clustered around papilla – found in 33-92% FAP
patients– Spigelman staging – suggests therapy
• Desmoids– Not malignant but may be nasty– Usually in mesentery, also abdominal wall and extremities– Occur in 10% - cause of death in 1%

Other FAP stuff
• Osteomas - usually mandible• Epidermoid, sebaceous cysts• Fibromas, lipomas• CHRPE – retinal lesions asymptomatic – correlates with
mutation

Natural History
Adenomas begin to develop in early adolescence
100-5000 colorectal adenomas
Cancer risk increases with number of adenomas
If untreated100% colorectal cancer risk
Median life expectancy – 42 years

FAP – surveillance
• Colon– Annual sigmoidoscopy, age 10-12 yrs– Prophylactic colectomy following polyp detection
w/continued surveillance of rectum, ileal pouch• Duodenal/gastric
– EGD age 25, repeat 1-3 yrs• Thyroid
– Annual PE, age 10• Hepatoblastoma
– Annual screen by abd U/S & AFP from birth to 5 yrs.
Gastroenterology 2001; 121: 195. AGA Statement

Inherited PolyposesFAP/Gardners
• Affected proband should have genetic testing -disease is inherited in autosomal dominant fashion
• If defect is identified in proband, family members can also be screened to identify those at risk
• Otherwise, children should begin screening with annual flexible sigmoidoscopy by age 10-13
• Dx: > 100 POLYPS• Surgery: > 5 mm, > 6-9 per cm2 . Timing in others is
controversial; post op need screening EGD’s

Genetic Testing: FAP/AFAP
• Test an affected family member first!
– After genetic counseling and informed consent
• APC gene testing can confirm a suspected diagnosis
• Family members of a person with a known APC mutation can have mutation-specific testing
• Genetic testing for children at risk for FAP can be considered before beginning colon screening

Inherited PolyposesFAP/Gardners
• Sulindac:– In a variety of animal studies, NSAIDs have been
shown to decrease tumor growth– In early human FAP trials, sulindac caused tumor
regression.– This effect replicated in subsequent randomized,
placebo controlled, double-blinded trials– Problems:
• Tumors recur when drug stopped• Side effects limit utility; specific COX 2 inhibitors
needed

Attenuated FAP
• 20 to 100 polyps, usually more proximal– Onset later than FAP, average AOO = 50
– Lifetime risk of CRC = 80%
• Extracolonic tumors occur at same rate as FAP
• Variant of FAP, mutations in same APC gene
• Surveillance: – annual colonoscopy starting late teens or early 20’s
– Option of subtotal colectomy

APC gene mutation in Ashkenazi Jews
• Missense mutation (I1307K) associated with increased risk of CRC and adenomas in Ashkenazi Jews (AJ)
• Found in 6% of the general AJ population
– 12% of AJs with CRC
– 29% of AJs with CRC and a positive family history
• Lifetime risk of CRC in mutation carrier is 10-20%
• Screening: colonscopy every 2-5 yrs starting at 35 yrs

MAP syndrome/MYH gene
• Multiple adenomatous polyposis (MAP) syndrome– Autosomal recessive; mutations in the MYH gene
– Median number of polyps = 55
– Mean age of polyp diagnosis = 30-50 years
– Polyps mainly small, mildly dysplastic tubular adenomas. Some tubulovillous, hyperplastic, serrated adenomas, microadenomas
• 30% of individuals with 15-100 polyps have homozygous mutations in the MYH gene
• Genetic testing should be offered if >15 polyps (and APC gene testing negative)

Peutz-Jeghers syndrome
• <1% of all CRC cases• Hamartomatous polyps of GI tract as early
as 1st decade• Mucocutaneous hyperpigmentation
– lips, mouth, buccal mucosa, fingers – Usually seen in children < 5 yrs
• Cancer risk: – colon, small intestine, stomach, pancreas,
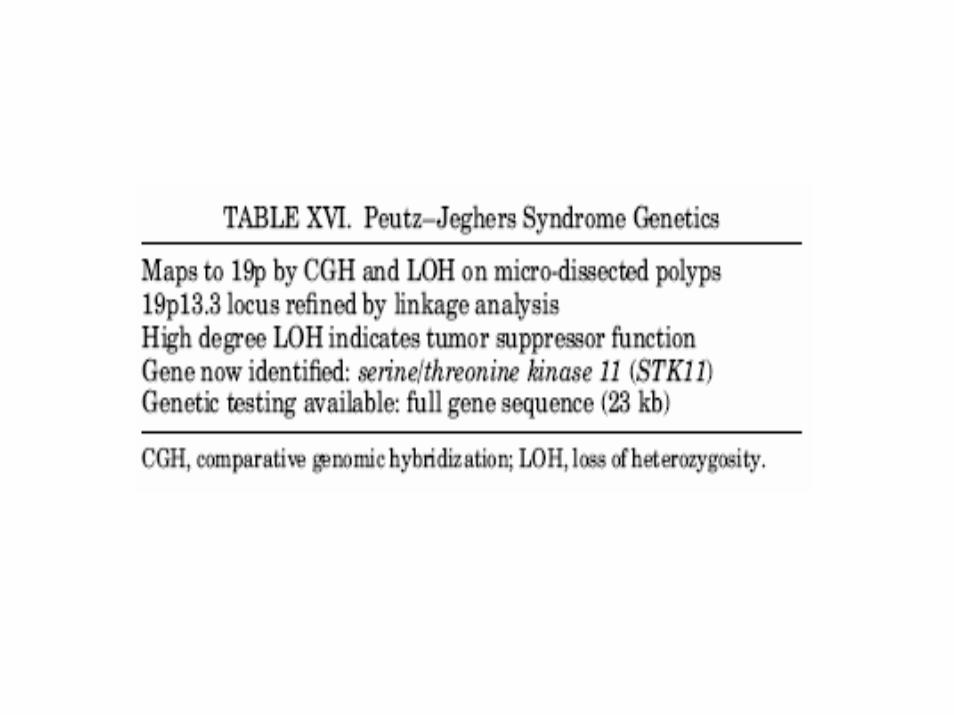
breast, ovaries, uterus, testes, lungs, kidneys• Mutations in STK11 gene
– found in 70% of familial cases and 30-70% of sporadic cases


Inherited PolyposesPeutz-Jeghers
• Hamartomatous polyps associated with mucocutaneous pigmentation.
• Brown-black freckles involving lips, oral mucosa and other sites - may fade with age
• Polyps, 1-3 cm in size, involve jejunum, colon, stomach and duodenum
• Sx: abdominal pain (intussusception), anemia• Risk of Ca (18 fold increase) of
duodenum/stomach, small bowel, and ovary

Inherited PolyposesPeutz-Jeghers
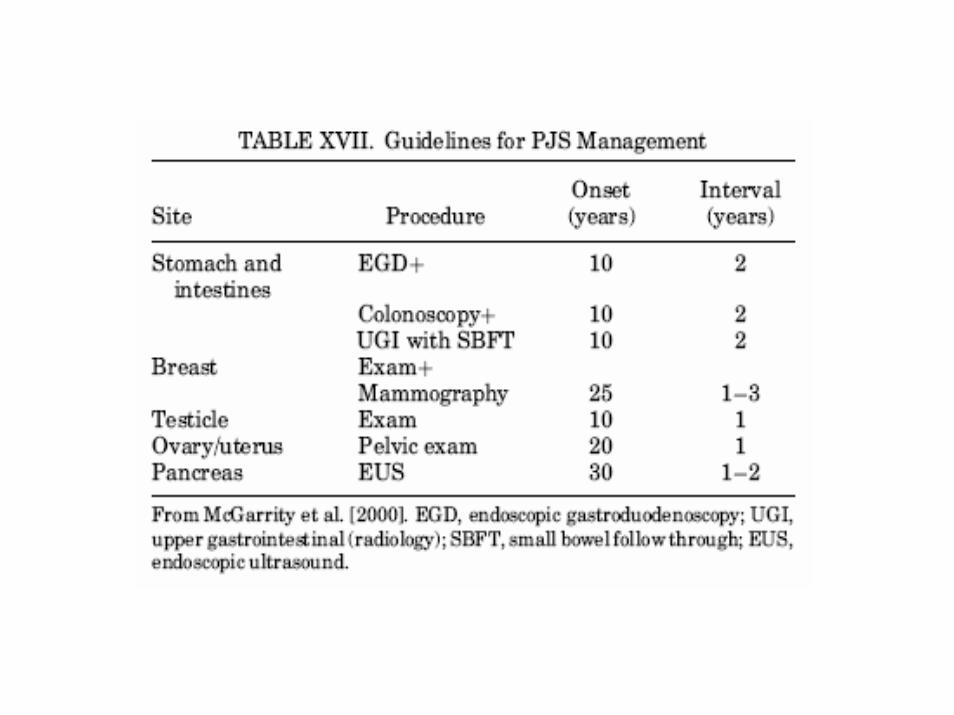
• Fundic or duodenal polyps should be removed promptly because of malignant potential
• Female patients should have periodic pevic examinations
• Genetic lesion: serine/threonine kinase, located 19p13.3 (most families)


Peutz-Jegher

Familial Juvenile Polyposis
• <1% of all CRC cases
• Autosomal dominant
• 5 or more juvenile polyps in colon or GI tract – Appear in 1st or 2nd decade
– 50% lifetime risk of CRC; AOO in 30’s
– Increased risk gastric, GI, pancreatic CA
• ~50% of cases have mutations in either the MADH4 or BMPR1A genes



Inherited PolyposesJuvenile polyposis
• Defined as the presence of 5 or more juvenile polyps within the colon
• Usually diagnosed within the first decade of life: typically presents with bloody stools
• May present with rectal prolapse or intussusception
• Genetically heterogenous• Three fold increase in risk of colorectal cancer:
screen with colonoscopy every two years

Inherited PolyposesCowden’s disease
• Hamartomatous polyps throughout the GI tract; most common in the colon and stomach
• Mucocutaneous lesions include hyperkeratoticpapillomas of lips, tongue and nares
• 30% incidence of breast Ca in females; also risk of thyroid tumors
• Lesion on chromosome 10q22-23 - tumor suppressor gene PTEN encoding a dual specificity phosphatase



www.genetests.org
PRINCIPAL INVESTIGATOR: Roberta A Pagon, MD
SPONSORING INSTITUTIONUniversity of WashingtonSeattle, WA
FUNDED BYNational Institutes of HealthContract No. N01-LM-3503


Sequencing ofentire coding region
Mutationscanning
Proteintruncation
testing
Prenataldiagnosis
Clinical confirmation of mutations identified in a
research lab