Embed Size (px)
Citation preview

FASD Case
Management
Training:
Key Findings Report
2013
Peterborough County FASD Committee

ii

iii
Acknowledgements This project was made possible by the curriculum development of FASD specialist Donna Debolt in
partnership with the Child Welfare Institute Children’s Aid Society of Toronto. Funding and support was
received from the Ontario Trillium Foundation and organizations that saw value in participating in
intensive training on FASD and the collaborative practice required to support individuals with the
disability.
The project would not have been possible without the leadership of Tri County Community Support
Services, training host Five Counties Children’s Services, the FASD Committee executive Sheryl Over,
Debra Lloyd, Joan Moriarty, training coordinator Tammie Hyde, and the Peterborough County FASD
Committee membership.
Our deepest appreciation is extended to caregivers who allowed their life experiences to be used as a
platform for Specialist trainees to transition knowledge from theory to practice during case
management consultations training.
Our thanks are extended to newly established FASD Specialists Resource Team (SR-T). Specialist trainees
brought energy, compassion, and creativity to the learning process. Their feedback and insight created a
synergy that continues to feed momentum toward better practice.

iv
Preface Fetal Alcohol Spectrum Disorder (FASD) is a neurodevelopmental disability that is common in Canada
yet poorly understood. Confusion surrounding FASD has marginalized those individuals living with the
disorder and contributed to profoundly poor outcomes. Challenges regarding the legitimacy of disability,
the degree to which alcohol exposure affects the developing fetus, and the stigma associated with
substance misuse, especially among women, has been unhelpful.
Research is clear and continued inaction is not benign. It negates the very real concerns of caregivers
and dismisses the need for a more informed professional and systemic response. It mutes the call to re-
evaluate and realign mandates and services and impedes the development of programs that could
provide effective and appropriate interventions.
Misunderstanding the genesis of FASD behaviour and learning profiles has resulted in investments in
strategies that fail to consider this disability. This contributes to significant social challenges including
lost opportunities for prevention. The cost of the status quo is staggering. Beyond the $5.3billion spent
annually in Canada to address issues associated with FASD, there is a loss of individual potential and
chronic stress faced by caregivers.
This report explores the impact of cross-sector FASD training and a collaborative case management
model that informs and organizes resources needed to ensure stability, safety and security.
Peterborough County FASD Committee hopes the findings will help other communities build an
improved response to individuals living with FASD.
Author: Sheila Burns is a consultant and specialist in Fetal Alcohol Spectrum Disorder. She was the Law
Foundation of Ontario Community Leadership in Justice Fellow and developed curriculum and
conducted research in the FASD field. She is past Diagnostic co-Lead and Chair of the FASD Ontario
Network of Expertise and is currently the Lead of the Justice Working Group. She has coached the
Peterborough County FASD Committee since 2002.

v
Executive Summary Key Findings Report: FASD Community of Practice
The Peterborough County FASD Committee has been active for over a decade working to address gaps in the diagnosis, treatment, management and prevention of Fetal Alcohol Spectrum Disorder (FASD). The Committee has a history of delivering successful community awareness and professional education events and oversees support groups for caregivers and individuals living with FASD.
The Committee developed the FASD Case Management Training proposal to coordinate, deliver, and evaluate an integrated case management and training curriculum to increase the effectiveness of programs and services. The proposal met the Ontario Trillium Foundation Accelerating Social Innovation grant criteria.
The Child Welfare Institute FASD Certificate Program curriculum best matched the requirements defined by community partners. This included developing a community of practice and enhancing knowledge in the existing system of care. The initiative involved two approaches to training:
workshops open to all community agencies and staff to ensure there was general awareness of the disability
intensive training in FASD and case management consultation for selected staff
The project focused on a shared language and understanding of the impact of prenatal alcohol exposure on fetal development and the resulting disability. It informed community services on how to screen, assess, and manage FASD. It also established a resource team of FASD Specialists (SR-T) to provide FASD-informed strategies to support effective case management. An evaluation process tracked changes in service provision from multiple perspectives to measure the value and impact of the training strategy. This report is a reference for communities across Ontario to help advance a change in practice.
Findings 1. Finding on Training Impact: in-depth training solidified understanding of a complex
neurodevelopmental disorder and improved confidence working with individuals living with the disability. Specialist trainees became the “go to” staff within their organizations.
2. Finding on Impact of Case Consultations: factors that contributed to positive perceptions and satisfaction included knowledge of the disability, a readiness to work collaboratively, flexibility in service or programming options, managed expectations, and shared responsibilities.
3. Finding on Value to Agencies: agency administrators were impressed by the scope and depth of the curriculum and felt the consultation model defined and shared responsibilities appropriately.
4. Finding on Program and Policy: the systemic challenges of integrating FASD-sensitive programs and policies require both local changes and government leadership.
5. Finding on Gaps in Systemic Response: many agencies supporting individuals with or suspected FASD did not participate in the training in a substantive way. The perceived value of the training and cost associated with replacement staff and staff workload were identified barriers.
6. Finding on Community Perception: FASD is often a factor or suspected in complex care consultations and committees. Local expertise will enhance these initiatives.
7. Finding on Diagnostic Capacity: agencies identified the need for better access to local diagnostic services. As a result of this project, medical doctors and clinical specialists have been recruited to take FASD diagnostic training.

vi
8. Finding on Training Trends: professional training is an on-going need. Training themes needs to continue to cover the basics of the disorder (FASD 101) but must also address service-specific interventions and program development.
9. Finding on Benefits: a Specialist Resource Team contributes to enhanced services. Providing FASD-informed supports can ensure the health, justice and social service system will be better positioned to improve the outcomes of individuals with FASD and may reduce the incidence of the disability.
Conclusion FASD presents as a complex profile of learning and behaviour often complicated by trauma and mental illness. It requires understanding of how the brain damage is expressed in order to plan and deliver services that address client needs to optimize outcomes. Providing FASD-informed care can ease many chronic individual and systemic challenges. This results in more effective and efficient use of resources and reduces the marginalization of individuals with this disability. The Peterborough County CWI training strategy demonstrates how building a community of practice improves service delivery across multiple sectors to respond more effectively to the needs of children, youth, adults and families living with FASD.

Table of Contents Acknowledgements ...................................................................................................................................... iii
Preface ......................................................................................................................................................... iv
Executive Summary Key Findings Report: FASD Community of Practice ..................................................... v
Key Findings Report: Building a Community of Practice and FASD Collaborative Response Network ......... 2
Taking Stock: Perceptions of FASD............................................................................................................ 3
Training Needs and Themes ...................................................................................................................... 4
Key Administrator Perspectives .................................................................................................................... 5
Fetal Alcohol Spectrum Disorder Certificate Program: Building Capacity .................................................... 6
Specialist Resources Trainees Feedback ................................................................................................... 9
Impact of Training on Practice .................................................................................................................... 11
Peterborough County FASD Committee ..................................................................................................... 12
Case for Action ............................................................................................................................................ 12
Conclusion ................................................................................................................................................... 13
References .................................................................................................................................................. 15
Appendix ..................................................................................................................................................... 16
About Fetal Alcohol Spectrum Disorder ................................................................................................. 17
FASD Peterborough Case Management Training Initiative Agency Baseline and Snap Shot Survey ..... 20
Community FASD Survey Summary ........................................................................................................ 24
Peterborough County FASD Specialist Resources Team Members ............................................................ 27
Contact Information .................................................................................................................................... 28

2
Key Findings Report: Building a Community of Practice and FASD Collaborative
Response Network
Prenatal exposure to alcohol can cause an array of damage to the developing fetus resulting in Fetal Alcohol Spectrum Disorder. FASD is an umbrella term that refers to a number of diagnoses that reflect profound neurodevelopmental impairments caused by diffuse brain damage. Stigma, lack of professional awareness, limited diagnostic capacity, postnatal trauma, and concurrent disorders has resulted in misapplied interventions and poor outcomes for individuals born with this disorder.
FASD has a significant impact on multiple sectors (Appendix A). Revising what we know and revamping how we work is a critical step toward improving the use of resources and long-term outcomes. Bridging the service delivery gap has proven to be complicated. Studies suggest common language and community of practice reinforces and sustains the services needed to accommodate hard to serve children, youth, adults and families1. It also provides a platform to discuss policy and program implications that are barriers to effective service delivery.
A community of practice (Lave & Wenger 1991) is built on two pillars: education and common interest. It is a useful approach for FASD as the disability touches many different resources and spans a lifetime. The FASD Case Management Training Initiative grant provided the opportunity to put this approach into practice. Community agencies were able to solidify and reinforce staff knowledge and build a collaborative network based on common language and understanding.
The FASD Case Management Training Initiative set out to:
Facilitate the coordination of services from different sectors i.e. developmental services, education, family supports, child welfare, justice, and mental health.
Respond to emerging local diagnostic needs with informed and enhanced interventions.
Make treatment and case management planning more effective.
Broaden the exchange of knowledge on FASD-related issues within an organization and across related services.
Improve programs and services to meet short and long-term client needs to achieve better outcomes.
Inform conversations with funders on the needs of individuals with a lifelong, chronic neurodevelopmental disorder
The project focused on a shared language and understanding of the impact of prenatal alcohol exposure on the developing brain and resulting disability. It informed community services on how to assess, manage, and coordinate services using a collaborative case management model. The training was limited to 30 staff selected from thirteen agencies that had demonstrated an interest in providing FASD-informed services. Evaluation from all perspectives was undertaken throughout the initiative to foster the development and delivery of evidence-based practice.
3
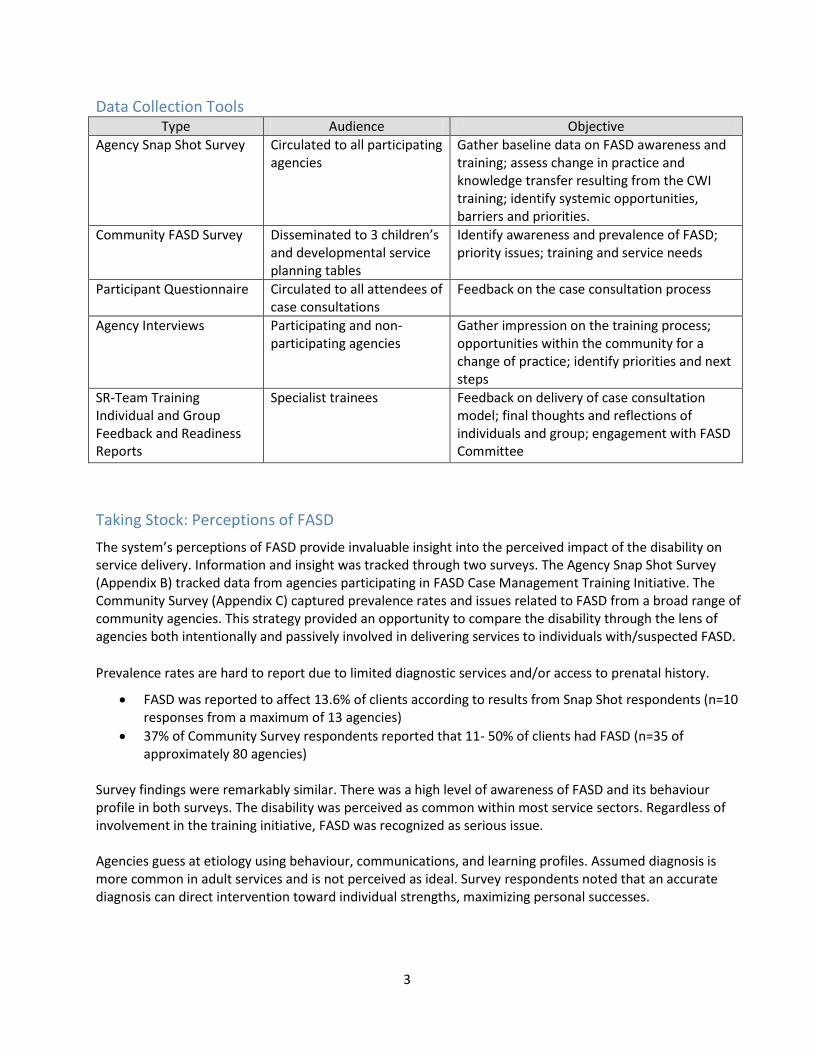
Data Collection Tools Type Audience Objective
Agency Snap Shot Survey Circulated to all participating agencies
Gather baseline data on FASD awareness and training; assess change in practice and knowledge transfer resulting from the CWI training; identify systemic opportunities, barriers and priorities.
Community FASD Survey Disseminated to 3 children’s and developmental service planning tables
Identify awareness and prevalence of FASD; priority issues; training and service needs
Participant Questionnaire Circulated to all attendees of case consultations
Feedback on the case consultation process
Agency Interviews Participating and non-participating agencies
Gather impression on the training process; opportunities within the community for a change of practice; identify priorities and next steps
SR-Team Training Individual and Group Feedback and Readiness Reports
Specialist trainees Feedback on delivery of case consultation model; final thoughts and reflections of individuals and group; engagement with FASD Committee
The system’s perceptions of FASD provide invaluable insight into the perceived impact of the disability on service delivery. Information and insight was tracked through two surveys. The Agency Snap Shot Survey (Appendix B) tracked data from agencies participating in FASD Case Management Training Initiative. The Community Survey (Appendix C) captured prevalence rates and issues related to FASD from a broad range of community agencies. This strategy provided an opportunity to compare the disability through the lens of agencies both intentionally and passively involved in delivering services to individuals with/suspected FASD.
Prevalence rates are hard to report due to limited diagnostic services and/or access to prenatal history.
FASD was reported to affect 13.6% of clients according to results from Snap Shot respondents (n=10 responses from a maximum of 13 agencies)
37% of Community Survey respondents reported that 11- 50% of clients had FASD (n=35 of approximately 80 agencies)
Survey findings were remarkably similar. There was a high level of awareness of FASD and its behaviour profile in both surveys. The disability was perceived as common within most service sectors. Regardless of involvement in the training initiative, FASD was recognized as serious issue. Agencies guess at etiology using behaviour, communications, and learning profiles. Assumed diagnosis is more common in adult services and is not perceived as ideal. Survey respondents noted that an accurate diagnosis can direct intervention toward individual strengths, maximizing personal successes.
Taking Stock: Perceptions of FASD

4
Finding: Many agencies identify FASD within their served population. Regardless of age of clients there is perceived value in accurate diagnosis to improve the effectiveness of interventions.
Screening and Prenatal History
The Community and Snap Shot surveys sought to identify if, how and when agencies track information on prenatal alcohol exposure. In both surveys fifty percent of respondents did not gather a prenatal history. Thirty percent tracked prenatal exposure at some point in the service process. A more detailed question was asked in the Community Survey with additional findings that 17.7% asked about prenatal alcohol exposure after intake, 11.8% in context of the therapeutic relationship, and 35.3% when they began to suspect FASD.
Responses from both the Community and Snap Shot surveys suggest that screening tools would be useful. Canadian Association of Paediatric Health Centres with funding from The Public Health Agency of Canada is leading the FASD National Screening Tool Kit project and is in the process of recommending screening tools, verifying factors including specificity, validity, time, ease of use, and cost.
Finding: Many agencies document prenatal histories and alcohol exposure. There are multiple opportunities to collect the information and formal screening tools would be useful.
FASD training is an ongoing need. Agencies perceive that their staff has an average amount of knowledge on the disability but both surveys suggest a significant (50%) need for training on the basics of FASD. This is somewhat surprisingly considering the number of events hosted in the community. Staff turnover is one factor but there may be other barriers to translating knowledge to practice. Barriers may include subtle resistance to delivering services differently; complications interpreting or using new information; more trained staff may be needed to influence program delivery; and mandates and policy may hinder change.
Beyond FASD 101 training, incorporating emerging effective practice into programming and interventions was a common theme. This includes classroom strategies, tailoring approaches to mental health treatment, managing age-related transitions, the diagnostic process, and the use of screening tools. Interagency collaboration, wrap-around support, and training for families were also identified needs. Success comes from integrating knowledge and cohesive programming; from a community of practice perspective training needs should be addressed concurrently.
Finding: There is an ongoing need for training on FASD and effective interventions. This gap could be efficiently addressed through postsecondary curriculum. Finding: Integration of FASD-informed strategies into services requires tacit and direct agency approval with concrete supports in policy and program design.
Training Approach
The survey findings were similar in responses related to the level of staff training. One third indicated that having all staff with a baseline of knowledge on FASD would be appropriate. Just less than 60% responded that their agency and community needs would best be served having some staff with specialized expertise. Nine percent (9%) suggested that all staff encounter clients with FASD and it is necessary to have both levels of training to ensure effective interventions.
Training Needs and Themes

5
Finding: Agencies identify value in having all staff aware of FASD and having some staff with in-depth knowledge of the disability.
There is a number of training format options: in-service, short and long workshops, day or evening, and conferences. Each provides a different learning experience. Preference to training formats was based on themes, costs, and time. Cost of training including replacing staff was cited as an issue for many agencies regardless of the size of their workforce. Workshops of 3 hours or less and agency in-services were slightly favored over longer training initiatives. However, comments reflected that cost factors and topics were the primary consideration.
Finding: Continuous, inexpensive and accessible professional and caregiver training both general and discipline-specific is required. This will fill a gap identified across the spectrum of services and improve the response to clients with FASD and their caregivers.
FASD Resources
The Community Survey sought to understand what resources and services were needed to strengthen the local response to FASD. The survey list was based on agency responses in Snap Shot Survey and from participant feedback given during training. Screening tools, diagnosis, and case consultation are perceived as having significant value.
Community Survey Response
Tools and resources would benefit your agency and/or clients Responses
Screening tools 57.58% 19
Referral process and understanding of the diagnostic pathway 60.61% 20
Local diagnostic services 66.67% 22
Case consultation for clients with/suspected of having FASD 69.70% 23
FASD resource lending library 51.52% 17
Website with links to research and resources 60.61% 20
Caregivers Support Group 45.45% 15
Individuals with FASD Support Group 42.42% 14
Finding: Agencies are looking for information on a number of areas to improve the effectiveness of their work; they are interested in a variety of resources to fill gaps.
Key Administrator Perspectives Administrator feedback was sought from two groups: agencies participating in the training initiative and others who were not participating but who likely served individuals with the disability. The perspectives of these two groups contribute to a better understanding of the impact of FASD on services as well as agency and client needs. Administrators from ten participating agencies and six non-participating agencies were interviewed. The conversations explored perceptions on the value of shared knowledge and common language, elements that contribute to a better FASD response, and systemic issues and opportunities.

6
All agency administrators were aware of a client cohort with/suspected FASD. Some agencies reported a higher prevalence rate of FASD than they had expected to find and agencies with only a few clients with/suspected FASD noted that those clients consumed significantly more resources than clients without FASD. Administrators described some services and programs that intuitively responded to the needs of clients with FASD; the successful programming elements were not always well understood. Agencies with programming flexibility reported the most optimism in meeting the needs of clients with FASD. Developmental Services seem most able to address a broad range of system and service delivery challenges. They were able to identify and work with the “cloak of competence”2 that hides deficits common to individuals with FASD. Organizations with strict reporting requirements or legislative mandates were less likely to see a strong role in addressing the individual and systemic needs of clients with the disability. There are a number of existing collaborative committees that oversee complex care needs of children, youth and adults who may have FASD. Feedback strongly suggests that having local expertise will enhance the effectiveness of these committees. Access to local diagnostic services is a missing component to improving the response to complex care clients. Findings:
Building a community of practice with shared language is perceived as a positive way to clarify roles and highlight the value of cross-sector collaboration. It acknowledges that FASD requires multiple services and coordination of a continuum of care across the lifespan.
Local expertise increased the perceived value of an FASD diagnosis as service responses can be tailored to address specific needs of clients.
Some sectors and agencies have regulatory issues that impede program innovations that could meet the needs of clients with/suspected FASD.
Compassion and care is needed when approaching women regarding alcohol use during pregnancy. Many of these women have faced significant trauma in their lives and many have FASD themselves.
Clarification of FASD as a neurodevelopmental disorder was helpful for some sectors as this seems to communicate the needs of clients more accurately.
Fetal Alcohol Spectrum Disorder Certificate Program: Building Capacity
Training Initiative, Child Welfare Institute, Children’s Aid Society of Toronto
Parenting, education, corrections, and treatment programs were originally designed using assumptions of learning and development that are incongruent with FASD. Replacing what is not working with evidence-based practice can change the chronically poor outcomes of individuals with FASD and build more effective programs. Evidence-based practice is emerging in the FASD field3 and is incorporated in the FASD Certificate Program developed by Donna Debolt in conjunction with the Child Welfare Institute (CWI) Children’s Aid Society of Toronto. The CWI FASD curriculum provided a platform for learning about FASD for multiple sectors and provided a model for collaborative case management consultation. The training approach enhanced existing resources and skills across the mainstream of services, a strategy with broad support in Peterborough County. Tri County Community Support Services took the lead on the training initiative and found ready partners across Peterborough County.

7
Alone we can do so little; together we can do so much. Helen Keller
CWI FASD training has been delivered in Toronto, Ontario since 2005. This was the first time it was delivered to a single community with Specialist trainees from a broad range of geographically linked services. The training model reinforced continuity of care and a continuum of services that best address the needs of individuals with FASD. It acknowledges that many agencies already serve this population. In addition to the specialized training, two 2-day workshops were hosted for professionals and caregivers.
The Specialist Resource Staff and Agency Selection Process
The complement of staff that comprised the Specialist Resource Team (SR-T) was selected from agencies across Peterborough County. Representation reflected a life span of services to build continuity of care. Agency representation included early intervention, education, mental health, addictions, corrections, First Nation Metis and Inuit, child welfare and developmental programs and services. A two-year commitment was required of both the SR-T and the agency. Additional selection criteria were outlined in the CWI program.
CWI Criteria for Admission
Certificate Program candidates must have: 1. A degree or diploma in a human or social service, allied health or early childhood education
discipline; AND 2. A minimum of two years full-time relevant practice experience working with children and their
parents; AND 3. Current employment in a related position
Recommendation: SR-T who felt the most confident in their new skill set also had case coordination experience. They were comfortable organizing and running meetings with multiple community partners and caregivers. Participants without this experience should be prepared to hone those skills to maximize the use of the training/learning experience.
Learning Outcomes
1. Recognize the presentation of FASD in your practice including the developmental trajectory of FASD, issues for justice, education, mental health and addiction services.
2. Understand how children, adolescents, and adults with FASD interface with the community and what their families need to provide long term placement stability and relationships.
3. Understand how women who are at risk of having children with FASD present in the community, what they need from service delivery and your role in prevention efforts.
4. Understand how to assist caregivers to help develop strengths based strategies to manage behaviours and how they can build community capacity for care.
5. Develop a case plan and make decisions within the framework of “best practice” with FASD. 6. Evaluate case plans with respect for the developmental needs of affected children, adolescents
and adults and their families and caregivers. Participants will ensure that the plans are: o Realistic o Focused on secondary disability prevention o Focused on finding permanent placements and creating placement stability

8
o Reflective of the need for family connections (including previous placements) o Creating meaningful futures o Framed to deal with case plan setbacks
Curriculum Elements
The curriculum was broken into three segments. In addition, two half-day workshops were requested by the Committee and trainees:
FASD diagnostic process and diagnostic models was delivered by developmental paediatrician Dr. S.M.L. Peggy Kirkpatrick. Dr. Kirkpatrick participates on a virtual (community collaborative) diagnosis team.
Grief, Loss and Chronic Sorrow was led by David Kennedy, Grief Matters counselling and Consulting. Mr. Kennedy was past co-facilitator of the Peterborough FASD Caregiver Support Group.
Curriculum Outline
Identification of Risk: screening for alcohol related disabilities
exploring factors that contribute to drinking during pregnancy and other adverse events in a child’s life
FASD Considerations for practice
children, adolescents and adults with FASD have complex medication, psychological and social needs
they are difficult to provide stability for and existing resources are not often user friendly for these families
Case management of FASD
providing participants with an opportunity to learn how to plan for the care of individuals with FASD and to recognize the impact that the developmental trajectory of this disability has on care planning
care plan review that includes those who have direct influence in the life of the client, exchange knowledge and teach about the impact of FASD on the client, and advocate and expands skills and knowledge beyond the care manager’s capacity
o collective wisdom o support trends of resources issues and needs
Added: Grief, Loss and Chronic Sorrow
recognizing the role of grief and the importance of facilitating the grieving process to help caregivers, including professionals, take on the work of supporting the individual with the disability
Added: Diagnosing an alcohol related disability
reviewing the Canadian diagnostic guidelines including multidisciplinary clinical elements, diagnostic criteria, process for determining diagnosis and local options for diagnostic pathways
Recommendation: The original curriculum provided in-depth understanding into multiple issues associated with the disability. Additional training components contributed to a fuller understanding of the diagnostic process and the collaboration required for a more meaningful diagnosis. The grief and loss work provided insight into the challenges of caring for individuals with this chronic condition and has application in caregiver and professional resilience.

9
SR-T members described the training’s positive impact on their work. The training has been immediately useful in responding to FASD queries with added confidence. They describe probing issues using different questions that explore areas of impairment, environment, and the system’s response. Their thinking on FASD changed the way they described the disability resulting in more success for clients. The level of training provided a platform to integrate or improve interventions. They used other SR-T members to help brainstorm for optimal solutions. All SR-T members engaged in formal or informal discussions and/or trainings and shared information and best practice strategies. All this contributed to improved interest and buy-in of colleagues.
The depth of training ensured a better understanding of the brain-based disability and the trajectory of outcomes. Most valuable was the message of where, why and how to focus energy and resources. SR-T suggest that care needs to be taken around a shift in language and terminology i.e. what does treatment or behaviour management look like when the client has FASD? This will be an evolving process enriched by the collaborative elements of the community of practice.
SR-T members identified gaps in agency representation and trust that new FASD training opportunities will include key agencies. They recognized that organizations respond at different speeds based on the agency culture and mandates and that this results in a “Pandora’s Box of next steps”. However, most SR-T feel that FASD is firmly on their agency’s agenda and the training will result in new relationships and service pathways.
Case Management Consultation Model
The CWI case management consultation model recognizes that individuals with FASD are profoundly vulnerable and that the complex issues that put their safety at risk are best resolved through coordinated agency collaboration rather than individual responsibility. The curriculum includes a consultation tool to help plan around critical issues related to the long-term support of individuals with FASD. Individuals with FASD are represented in case consultations by caregivers. This ensures that planning is informed by their wishes and interests and services can organize around their needs.
The case management consultation tool includes reviews of school/employment, health, psychological assessments, placement history, family dynamics, and legal issues. This helps identify planning priorities, defines next steps, and assigns responsibilities for action. This simple but thorough tool captures multiple components of the lifespan of needs and maximizes continuity.
Recommendation: Additions to the tool were made to include programming options and strategy prompts.
Case Management Consultations: Theory to Practice
Twelve training case consultations involving children, youth, and adults and a broad spectrum of education and social service agencies were hosted as part of the training curriculum. The use of active cases presented some challenges but gave the most realistic learning experience.
Specialist Resources Trainees Feedback

10
A Participant Survey was designed to gather impressions from all those involved in a case consultation. The survey was available in hard copy, electronic format, or by phone interview; responses were received by administrative staff then forwarded to ensure anonymity. Participants reported that the case consultations were valuable though managing expectations was an issue. The relationship between the SR-T member organizing the consultation and invited participants had a bearing on the comfort of participants and level of positive feedback.
An analysis of feedback from all participants’ responses suggests the following meeting protocols:
an opportunity to submit priorities questions/issues for discussion
the list of invitees
the purpose of the consultation and outline of priority issues to be discussed
the consultation should include all parties connected to the client/caregiver
2-2.5hrs in length though satisfaction was not dependent on time
location and directions Consultation should include:
formal introductions
chairperson
an agenda
clarification of expectations
recording of discussion decisions
follow-up plan with responsibilities defined
determine follow-up contact to participants by the case manager/lead
resources to assist caregivers and professional integrate FASD-informed strategies
post-consultation participant feedback
Finding: Clearly defined expectations have a significant impact on the consultation experience. Introduction letters that explain the process were insufficient for some participants. A video introducing the process could improve participant readiness and comfort.
Consultations covered diverse ages and family arrangements though there were common elements in planning, the process, and follow-up. Several SR-T members provided information on available services or resources during the consultations. This resulted in more dynamic, interactive, and helpful sessions. It also demonstrated effective and efficient collaboration.
Consultations exposed vulnerabilities of some placements i.e. older parents or families with many other children, was obvious and the need to coordinate services to stabilize placements was evident. A child with a genetic disorder was found to have FASD as well; one disorder masked the other – a common issue for those with FASD. Approaching the child and caregiver needs through the FASD lens resulted in immediate improvement and relief.
There is overwhelming consensus on the value of the case consultation training. Though all SR-T members completed the program, the degree of readiness to lead a consultation varied. Most were ready to work as part of a team rather than alone. This will facilitate the integration of their new skills and build confidence. Mandates and geographic considerations were anticipated barriers for case consultations. The Community Survey found that 70% of agencies needed these services but few require more than 3 per month. The SR-Team represents agencies across the community so there is a good match of resources and needs.

11
Impact of Training on Practice Tracking change in practice was done using a number of tools. SR-T feedback was gathered using questionnaires and facilitated group discussions. The impact on agencies was gathered in the Snap Shot Survey and Administrator interviews. The training initiative opened the discussion on the impact of FASD on programming and set a tone for a dialogue about a change in practice. The training provided a deeper, more textured response that was seen to improve outcomes and client wellbeing. It also had a direct impact on the development of local diagnostic capacity. Awareness of FASD at intake directed staff assignments so expertise could be tapped. One agency developed new protocols and others reported that the information improved understanding of behaviour and changed interactions with families. Those in the developmental disabilities field recognized overlap with other neurodevelopmental disabilities i.e. Autism Spectrum Disorder and acquired brain injury, and could see the value in retooling resources so they were applicable to clients with FASD. Agencies reported that change in practice and policy was underway including:
Twenty-six formal FASD workshops were given to audiences supporting children, youth and adults.
A Grand Round at the area hospital resulted in commitments from medical doctors and other clinical specialists to take diagnostic training.
Seven of ten responding agencies reported recommendations had been made for program or service delivery changes and two agencies had already made policy changes
Half of the trainees had already participated in interagency case consultations.
All trainees participated in knowledge exchanges; eight of thirteen agencies reported an increase in staff understanding of FASD and its implications.
Trainees incorporated their knowledge and became the “go to” people for programming ideas. They reported more confidence discussing FASD when engaging with colleagues.
Relationships that developed through the training initiative facilitated the exchange of knowledge and a better understanding of the issues and community resources.
The training initiative provided a helpful approach to case management by clarifying aspects of the disability, validating the experiences of caregivers, sharing responsibility, and providing a language of hope that had often been missing from the FASD dialogue.
The training days were long and intense; SR-T felt a tighter schedule would help retain momentum and solidify skills. They indicated that the length of training was appropriate but wanted more case management consultation training and coaching.
Recommendation: For continuity of learning, the training schedule should be established in advance with 2days per training session not more than 6 weeks apart.
Recommendation: Case Management Consultation Training format to optimize learning needs: o One consultation per 1/2day to ensure adequate time to review and discuss the process,
outcomes and strategies o All trainees should have an opportunity to lead a consultation o Trainees should already have skills and experience organizing and leadings meetings o Ongoing consultation coaching will help SR-T members integrate their new skills

12
Peterborough County FASD Committee Coordinating an effective response to FASD currently rests with the Peterborough County FASD Committee. At the end of the training fifteen Specialists, representing their agencies, joined subcommittees. In addition one Specialist has become a co-facilitator of the caregiver support group and others provided practical support to the Youth FASD Summer Program. This will help the community move toward its goal of having FASD informed and responsive programs and services. It will help maximize the effective use of local, regional and provincial resources.
Peterborough County FASD Committee Organizational Chart
Recommendation: A book-club model can provide continued professional development where SR-T members identify then research a topic for a Team discussion. This strategy will link the SR-Team and their agencies with emerging research, best practices, and resources while reinforcing local partnerships.
Case for Action Doing nothing about FASD is extremely expensive: $5.3 billion a year in Canada4 and growing. This is the cost of delivering services that fail to consider this neurodevelopmental disorder. Recognizing and addressing the
•establishing protocols for the coordination and delivery of consultation support services
•working with clinicians and agencies to secure local, accessible diagnosis
•conference planning, agency in-services, and community workshops
•developing programs &/or proposals to address identified gaps in service and primary prevention
Program Development & Enhancement
Professional Development and Training
FASD Specialist Resource Team
Diagnostic Capacity Development

13
needs of individuals living with FASD and constructing an informed response will be more cost effective. Individuals with FASD already rely heavily on services:
raised by others (80% of children with FASD are not raised by the birth parents5)
child protection services (30.5-52% of children in care have FASD6)
youth corrections (youth with FASD are 19 times more likely to be in prison than their non-effected peers7)
adult corrections (10-30% of inmates have FASD8)
welfare recipients (there is strong correlations in the behaviour profile of FASD and adults receiving financial assistance for 1 year or more9)
Cost savings will grow with time but for this to happen the system must recalibrate its focus and design and provide FASD-informed services. There will be a significant return on investment with the delivery of:
daily living supports for children, youth and adults
training and coaching for caregivers and professionals
respite and relief for caregivers
screening, assessment and diagnostic pathways
programs that accommodate the complex expression of deficits and strengths
flexibility in the justice system and corrections services
design and delivery prevention and harm reduction programs Change will not occur in a vacuum. A larger dialogue is required to respond to the macro-systemic issues associated with the unintended discrimination associated with this disorder. Policies that exclude this vulnerable population from appropriate levels of service contribute to inefficacies and adverse outcomes. Legislative reform can shift policies and direct program modifications. Service delivery strategies need to address the chronic and lifelong implications of the disability. Cross-ministry collaboration is needed to coordinate and foster effective programming. Leadership from the justice, education, child welfare, addictions, mental health, income and employment, First Nation Metis and Inuit and developmental service sectors can build a better understanding of FASD to ensure more informed responses.
Finding: FASD occurs in all sectors of society. Ministry leadership will fast-track not only systems’ collaboration but the development of evidence-based practice and delivery of training that will have a positive impact on communities across the province.
Conclusion
Living a full life, a dependent life, lived as independently a possible. Barbra Turnbull
Individuals with FASD need help to navigate their community through a variety of services. They are currently excluded from many services that would stabilize and enrich their lives. Instead they have developed a chronic reliance on expensive or intrusive services that cannot address their long-term needs. Developing a community of practice by training a cross-sector of staff in FASD effective practice improves the response to clients with FASD.

14
Training has resulted in better community collaboration and improved responses to those living with FASD. A better understanding of FASD has taken the guess work out of interventions, education, and program planning. It adds another perspective when considering the needs of individuals and families seeking service. Training improves the understanding of challenges in communication, sensory, processing, adaptive and executive functioning. It shifts the focus from deficits and adverse outcomes to strengths and effective intervention. A barrier to developing local diagnostic capacity had been access to informed community services. The depth and breadth of the CWI training has addressed this issue. Physicians and other clinical specialists see the value in the diagnosis and contributions diagnostic recommendations can have on enhanced outcomes. Surveys and interviews identify simple actions that improve the lives of individuals with/suspected FASD. Training of caregivers and staff, access to diagnostic services, and collaboration among all the agencies are paramount and urgently needed. Each would make service delivery more effective and efficient. Administrators from services across the County identify policy challenges affecting their ability to construct an improved response for clients with/suspected FASD. Training front line staff to be fluent in FASD is one step but management has a role to play to make the training transformative across the system. Leadership, found in community collaboration and a community of practice, can improve the response to this and other neurodevelopmental disorders.
Finding: Providing FASD-informed supports ensures the health, justice and social service system are positioned to improve the outcomes of individuals with FASD and may reduce the incidence of the disability.

15
References 1 The FASD (Fetal Alcohol Spectrum Disorder) Community of Practice in Alberta Human Services: Leading from
Within Initiative (Alberta, Canada), Project Funder: Alberta Centre for Child, Family and Community Research, Badry, D, 2013 2 Term used by CHMA program manager
3 Towards a Provincial Strategy: Advancing Effective Service Provider Practices in Fetal Alcohol Spectrum Disorder
(FASD) Hall, Cunningham & Jones, 2010 4 Revised Estimate of The Cost Burden of Prenatal Exposure to Alcohol in Canada, Stade, Brenda; Ali A et al 2009
5 Understanding the Occurrence of Secondary Disabilities in Clients with Fetal Alcohol Syndrome (FAS) and Fetal
Alcohol Effects (FAE); Streissguth Ann et al 1996 6 Systematic Review on the prevalence of Fetal Alcohol Spectrum Disorders, Ospina M., Institute for Health
Economics Alberta Canada, April 2013 7 Fetal Alcohol Spectrum Disorder Prevalence Estimates in Correctional Systems: A Systematic Literature Review,
Popova S. et a; Can J Public Health 2011;102(5):336-40 8 FASD in a Correctional Population: Preliminary Results from an Incidence Study MacPherson P. Chudley A. 2007
9 FASD and Adults on Social Assistance: Considerations for serving clients with chronic, complex needs, Durham
Region Department of Social Services, The Region of Durham, 2008

16
Appendix

17
Appendix A
Fetal Alcohol Spectrum Disorder is an umbrella term that refers to diagnoses of physical and neurodevelopmental disabilities caused by prenatal exposure to alcohol. Alcohol impedes cell growth and development in the fetus causing damage that results in a complex range of symptoms that are primarily brain based. This includes difficulties with learning, regulation of behaviour and mood, and impairments in social communication. The degree of injury varies based on time, dose, maternal, and fetal factors.
The Canadian Diagnostic Guidelines were established in 20051 to standardize diagnostic criteria and assessment process. The process incorporates not only a physical examination but also evaluation of brain function, most commonly completed by psychologists, occupational therapists, and speech pathologists. A specialized tool is used to measure facial features; standard tools and tests evaluate growth and brain function. Each element of diagnosis is ranked using a 4 point Likert scale; the rankings classify the diagnosis.
The threshold for all diagnoses in the spectrum is impairments of 1.5-2 standard deviations below the norm in a minimum of three (3) areas of brain function. This indicates diffuse brain damage with measurable and significant deficits in memory, language and sensory processing, social communication, internal regulation, and executive and adaptive functioning.
Diagnosis Growth Face Brain Alcohol
Fetal Alcohol Syndrome
(FAS) 1-3:1000 births X X x x/o
Partial-FAS (pFAS) some but not all of these x x
Alcohol Related Neurodevelopmental
Disorder (ARND) 6-8:1000 births 0 0 x x
X = required 0 = absent
Impairments, specifically in executive and adaptive function, put the complex expression of deficits into the purview of a developmental disability service sector, though not entirely. Individuals with the disability often fail to meet eligibility requirements due to scatter or uneven scores in brain function. Strengths hide impairments often making the individual look and sound more capable than they are.
Individuals with FASD at 18 years of age exhibit an uneven, confusing, and conflicting constellation of skills. Their chronological and developmental age is out of sync. They look and speak like same-aged peers but are profoundly and permanently delayed in critical aspects of living. 1 Fetal alcohol spectrum disorder: Canadian guidelines for diagnosis Chudley, A et al 2005 CMAJ March 1, 2005
vol. 172 no. 5 suppl doi: 10.1503/cmaj.1040302
About Fetal Alcohol Spectrum Disorder

18
Secondary disorders or adverse outcomes occur when expectations and ability are incongruent. This contributes to high rates of mental illness including depression and anxiety disorders and correlates with school failure, substance misuse, homelessness, victimization, sexualized behaviour, having children in care, and criminal activity234.
Streissguth 96, Streissguth, Sampson 97, Conroy 2011, CAS-Toronto 2009
2 Understanding the Occurrence of Secondary Disabilities in Clients with Fetal Alcohol Syndrome (FAS) and Fetal
Alcohol Effects (FAE); Streissguth Ann et al 1996 3 The Challenge of Fetal Alcohol Syndrome: Overcoming Secondary Disabilities Streissguth , Kanter J et al 1997
4 Secondary Disabilities Among Adults with Fetal Alcohol Spectrum Disorder in British Columbia, Clark E, Lutke J.,
et al, J FAS Int 2004;2:e13 Oct. 2004 The Hospital for Sick Children
0
10
20
30
40
50
60
70
80
90
100
generalpopulation
crown wards raised byothers
school failuremental illnessyouth conflictwith law
adult conflictwith law
Adverse Outcomes for youth and adults with FASD

19
Daily living skills direct and inform the kinds of services needed by individuals with FASD that enhance client success and engagement. Individuals living with FASD require interdependent living opportunities to ensure they are safe and can contribute to their community.
Elements of effective practice5 inform programming options and contribute to improved service delivery. Effective practice acknowledges clients have FASD with/without a diagnosis; ensure staff and caregivers receive on-going training in FASD; apply positive, strength-based approaches using the FASD lens when designing interventions plans; ensure structure, support, and routine to ameliorate weakness in executive and adaptive functions; modify communication strategies; address Sensory Integration Disorders (SID); collaborate with other services to coordinate more effective responses; plan for lifelong, continuum of supports to address the permanent nature of the disability. The elements mirror seminal research findings on protective factors that contribute to the prevention of secondary disorders other adverse outcomes. These include early diagnosis, supportive nurturing home life, absence from abuse/witnessing abuse, access to developmental services and appropriate services6. Individuals with FASD have been heavy users of services, services that become more intrusive and expensive. Interventions are often ineffective because they fail to address and cannot fix the underlying neurodevelopmental disability. For this reason FASD has emerged as a critical issue in service delivery including early intervention, education, mental health, addictions, justice, child welfare and adult crisis and support services. Those with the disability can be hard to serve and drain significant resources across multiple sectors with costly interventions and limited success.
Individuals living with FASD require a systemic response that combines mainstream and developmental services to achieve optimal outcomes. This approach directs the individual toward supported interdependent living reducing their vulnerability, victimization and providing a platform for pro-social contributions to their community.
5 Towards a Provincial Strategy: Advancing Effective Service Provider Practices in Fetal Alcohol Spectrum Disorder
(FASD) Hall, Cunningham & Jones, 2010 6 Risk Factors for Adverse Life Outcomes in Fetal Alcohol Syndrome and Fetal Alcohol Effects Streissguth A et al
Developmental and Behavioral Pediatrics Vol. 25, No. 4, August 2004

20
Appendix B
Agency response rate: 10 of 13 n=10 unless otherwise specified
Rating Scale: 1 (Strongly Disagree) 2 (Disagree) 3 (Neutral) 4 (Agree) 5 (Strongly Agree)
1. FASD/suspected FASD is an issue for 13.6% of agency clients n=7 2. FASD/suspected FASD is an emerging issue for agency clientele 1 2 3 4 5 n= 4.3 3. Most staff have a strong knowledge of FASD and its implications 1 2 3 4 5 n= 2.7
Training Plan
Number of FASD trainings for agency staff: Fall 2009 until Fall 2011 (2yrs) (excluding FASD case management training)
#61trainings 174# of hours of training #6.1 per agency 19.3 hrs average Range 1-500 n=9 #754 of staff participating n=9 10.9% agency staff involved n=8
% of staff currently trained in FASD
24.2% of current staff trained n=9 (caveats include front line staff only or high rates among specific departments)
How has training changed practice? See need for deeper textured training needed for all Importance recognizing clients’ wellbeing Awareness at intake, treatment intervention programming Update staff regularly, clie3nts are assigned to staff with expertise Staff awareness, understanding impact on families Trained frontline New protocols and information change interactions > understanding behaviour better Case management, advocacy for services, recommend programs Incorporate student needs SR-T = go to people Case management services, understood process to engage professionals, cope daily, nurture capacity building programs and services and training More requests for support
To meet the needs of your agency and clients who have/suspected FASD, it is better to (check)
train all staff
have a few staff with expertise in FASD
other
4 train all staff 8 have a few staff with expertise in FASD 1 other Comments: all staff may encounter FASD General knowledge plus key support people Train all staff so they all know Have some experts – all general knowledge Experts can train others Too many clients for just one case manager
Number of FASD training initiatives planned in 2012-14 8.1# n=8 many said they would send staff to any providing they be in the community
Priority training themes or topics Priority 1
Basics to recognize
Programming strategies
Practical recommendations for affected and their caregivers
Priority training themes or topics Priority 2
Awareness of services/resources in community
Research development
3 challenge for caregivers
4 Interagency collaboration
FASD Peterborough Case Management Training Initiative Agency Baseline and Snap Shot Survey

21
Diagnostic training = medical directors
FASD and young adults
Assessment procedures for psychology staff
P.p. sr-t = will use 2hr presentation for 17 staff
G-7 conference (on FASD in Sudbury)
FASD 101
In-depth consultations by case manager
Training opportunities for staff
Diagnosis in suspected children
Managing classroom environments
3 knowing wrap-around for families
4 understanding learning profiles for students
Best practice support
3 on-going education
Capacity building = frontline health education social series and justice
3 workshops = prenatal and other groups
Programs for FASD
Case Management Training Initiative Number Comment
How many agency staff participated in training
conducted by Donna Debolt (November 17 & 18, 2011)
36 in total n=9 – average
4per agency
How many agency staff participated in training to become part of FASD Specialists Resource Team (SR-Team) (training November, January, February/March)
22
How many agency staff will be on the SR-Team Subgroup (making recommendations and reporting outcomes and opportunities to Peterborough FASD Committee)
11
Impact of Case Management Training on Agency Yes No Unsure Comment
SR-Team Staff
shared knowledge with colleagues formally
7 3 Presented at 2 staff meetings Presentation to leadership team
shared knowledge with colleagues informally 10 0
increased agency understanding of FASD and its implications
8 1 na, service improvement on clients with FASD BRIEF assessment added Plans to continue to build staff capacity
made recommendations for changes in policy
2 7 1 Agency policy under review Possibility of involvement I diagnosis Case by case per student Under discussion
made recommendations for changes in programming or service delivery
7 3
identified changes that require approval/input beyond this agency i.e. head office, ministry, funder, other (specify)
3 5 2 if not dd, after 13 client dropped but diagnosis might keep from falling through STAY MCSS rep and other funded agencies
have participated in interagency case consultation to share their knowledge
5 3 2 shared ongoing with both school boards – teachers supporting youth with FASD
have trained others in the case consultation strategy
1 6 3 more evidence in interagency dialogues and planning Not as confident

22
FASD PETERBOROUGH CASE MANAGEMENT TRAINING INITIATIVE AGENCY SNAP SHOT
Activities that contribute to effective programming for clients with/suspected FASD
Exists Minimal change
required
Change is underway
Needs to be developed
Screening for prenatal exposure to alcohol na-3 1 1 5
Gathering information related to prenatal alcohol exposure during intake process na=2
2 1 1 4
Process to get history of prenatal alcohol exposure after intake (within the context of service delivery or a therapeutic relationship) na = 3
1 1 3 2
Defined pathway for diagnosis na = 2 3 0 2 3
Referral process to access diagnosis na = 2 3 1 3 1
Agency policy supports referrals for FASD diagnosis na = 3
4 1 0 2
Agency can contribute to FASD diagnosis (specify): MD, Speech pathologist, occupational therapist, psychologist, case management, other na = 2
5 0 1 2
Policies of agency address the developmental or chronic needs of clients who have/may have FASD Na = 2
3 0 4 1
School board all na – no current role
Activities that contribute to effective programming for clients with/suspected FASD
Exists Minimal change
required
Change is underway
Needs to be developed
Programs or Services of agency reflect the developmental or chronic needs of clients who have/may have FASD (circle appropriate)
Adults 1 0 1 1
Child 3 0 3 2
Youth 2 0 1 1
Families 1 0 1 1
Diverse agency partners collaborate to plan and coordinate services delivery to clients with FASD
1 2 6 1
What steps is your agency taking/considering to bridge gaps in programming or in policy?
Staff participation; reviewing agency policy and active in FASD planning; community committee; partner on committee exploring diagnostics; reviewing programs; staff capacity building; staff training and reviewing best practice and policy; interagency partnership
Describe any barriers to a more effective response: PROGRAMMING/SERVICES
Macro level programming (across province) Interagency collaboration Mandate limitations Funding for staff Funding to implement services Integrating knowledge = theory to practice Professional development $$ for teachers, support staff
Review current approach considering best practice/meeting client’s needs > try to eliminate barriers Lack of diagnosis Perceived as someone else’s responsibility

23
Describe any barriers to a more effective response: POLICY
Marco (see above) probation Marco (head office) to clarify policy, practice for clients with FASD FASD developmental disability at ministry Coordinated community response with defined agency roles
MCSS developmental delay 1%precentile, FASD above this Diagnosis, incidence rate/prevalence in services; maintaining FASD community members/funding/hard to develop policies without stable committed agencies Lack of trained people
Describe any barriers to a more effective response: OTHER
Our own education to 1) recognize 2) deliver resources/services that are appropriate and 3) coordinate with others Challenge of interagency collaboration and current “conventional” medical thinking DD services and local diagnosis
Duplication of services and funding for a coordinated response Theory to practice when challenge by untrained aggressive agency/stakeholders Stigma and denial Not enough people trained Court staff training
List PRIORIY actions that would improve the response to individuals with/suspected FASD, caregivers and/or community responsiveness R= repeat responses
Training/education R = 5
Awareness of services/ resources R = 2
Agency roles: who does what R = 2
Diagnostics R = 4
Interagency collaboration R = 4
Education/information for parents/community at large R = 2
Access to psych assessments, supports, and services R = 2
FASD as a developmental delay
Reducing waitlist/paediatricians and training more MDs
More (school) psychologists/OT trained/hired
SR-T training expanded to more communities
Screening tools/strategies
More training
Lead officers in the organization and courts

24
Appendix C
1. Approximately what percentage of your clients have or are suspected of having FASD
0-10% 11-20% 21-35% 36-50% 51-75% 76 or more
unknown Total Response
Average Rating
60% 22.86% 8.57% 5.71% 0% 0% 2.86% 1.74
21 8 3 2 0 0 1 35
2. When does your agency seek information related to alcohol use in pregnancy/prenatal alcohol exposure to determine if a client may need a referral for assessment and/or FASD diagnosis?
(check all)
Answer % of R R
On intake 29.41% 10
After intake 17.65% 6
When FASD is suspected 35.29% 12
In the context of a therapeutic relationship 11.76% 4
We do not gather a prenatal history 50% 17
Total Respondents: 34
3. Most staff have a strong knowledge of FASD and its implications Strongly Disagree
Disagree Neutral Agree Strongly
Agree Total
Average Rating
8.57% 31.43% 28.57% 28.57% 2.86% 2.86
3 11 10 10 1 35
4. More training in FASD would benefit our agency Strongly Disagree
Disagree Neutral Agree Strongly Agree
Total Average Rating
0% 2.94% 11.76% 50% 35.29% 4.18
5. To meet the needs of agency clients who have FASD or are suspected of having FASD is it better to:
Answer Choices % R R
Train all staff 30.30% 10
Have a few staff with expertise in FASD 57.58% 19
Refer to other agencies 3.03% 1
Other (please specify)
It is important to train all staff, however realistically having a few staff with
9.09% 3
Community FASD Survey Summary

25
expertise in FASD is more likely to meet the needs of a large agency.
Because our agency is so small and resource dollars tight, it may be better to have a few staff with expertise to share knowledge to other staff who support specific individuals it pertains to
It is most useful to have all staff trained with a general level of knowledge and a identified few staff with expertise.
Total Responses 33
6. What type of training approach works best for your agency/staff Answer Choices Responses R
Agency in-service 24.24% 8
Daytime workshops of 3 hours or less 33.33% 11
Evening workshops 0% 0
Full-day conference with options for workshops 9.09% 3
Full-day training by one presenter/theme 15.15% 5
Other (please specify) 18.18% 6
Total Responses 33
7. Training topics: Rank the topics you feel are most valuable Ranking 1 2 3 4 5 6 7 8 9 Total
Basics of FASD 48.28% 14
3.45% 1
3.45% 1
6.90% 2
10.34% 3
0% 0
6.90% 2
3.45% 1
17.24% 5
29
Diagnostic process and pathway
12.50% 3
8.33% 2
8.33% 2
4.17% 1
8.33% 2
12.50% 3
16.67% 4
16.67% 4
12.50% 3
24
Reading psychological assessments
8.33% 2
8.33% 2
4.17% 1
4.17% 1
33.33% 8
4.17% 1
20.83% 5
16.67% 4
0% 0
24
Teaching children with FASD
14.81% 4
18.52% 5
11.11% 3
7.41% 2
7.41% 2
7.41% 2
14.81% 4
7.41% 2
11.11% 3
27
Implications of FASD on mental health interventions
3.45% 1
13.79% 4
20.69% 6
10.34% 3
10.34% 3
10.34% 3
10.34% 3
10.34% 3
10.34% 3
29
Collaboration & case management
7.41% 2
7.41% 2
11.11% 3
7.41% 2
18.52% 5
18.52% 5
14.81% 4
7.41% 2
7.41% 2
27
Managing transitions
3.70% 1
22.22% 6
18.52% 5
11.11% 3
3.70% 1
7.41% 2
3.70% 1
11.11% 3
18.52% 5
27
How to ask about prenatal alcohol use in pregnancy
13.04% 3
8.70% 2
13.04% 3
17.39% 4
4.35% 1
4.35% 1
4.35% 1
13.04% 3
21.74% 5
23
Justice 8.33% 2
8.33% 2
12.50% 3
16.67% 4
0% 0
20.83% 5
4.17% 1
4.17% 1
25% 6
24
Screening tools 13.04% 3
21.74% 5
13.04% 3
8.70% 2
8.70% 2
8.70% 2
4.35% 1
17.39% 4
4.35% 1
23
Other 0% 0
25% 1
0% 0
25% 1
0% 0
0% 0
0% 0
0% 0
50% 2
4

26
8. What tools and resources would benefit your agency and/or clients (check all that apply) Answer Choices Responses R
Screening tools 57.58% 19
Referral process and understanding of the diagnostic pathway 60.61% 20
Local diagnostic services 66.67% 22
Case consultation for clients with/suspected of having FASD 69.70% 23
FASD resource lending library 51.52% 17
Website with links to research and resources 60.61% 20
Caregivers Support Group 45.45% 15
Individuals with FASD Support Group 42.42% 14
Total Respondents
33
9. Individuals with FASD are often heavy users of community services. Their needs are most effectively address through coordinated case management. How often would your agency use in-kind case management consultation supports for clients with FASD or suspected FASD?
Answer Choices Responses R
weekly 3.57% 1
bi-weekly 0% 0
monthly 17.86% 5
bi-monthly 14.29% 4
less than 5 times per year 42.86% 12
once a year or less 21.43% 6
Total
28
10. Demographics and About your agency: the service delivery area our agency covers is Peterborough County only
Answer Choices % Responses R
YES 12.12% 4
NO 87.88% 29
Total 33

27
Peterborough County FASD Specialist Resources Team Members
Alternatives Community Program Services Julie Wilson, Kim Carson, Kimberly Hoard-Miller Community Living Kawartha Lakes Joan Moriarty Community Living Peterborough Tanya Birch, Shelley Davis Tri-County Community Support Services Debra Lloyd, Brittany Thompson, Sandra McAlpine Family and Youth Clinic, Peterborough Regional Health Centre Kelly Burkholder Five Counties Children’s Centre Sheryl Over Kawartha Haliburton Children’s Aid Society Erin Hentig, Trisha Farrar Kawartha Pine Ridge District School Board Deborah Chapman, Tammy Best, Beth Sheedy, Linda Turner- Phillips Kinark Child and Family Services, Peterborough and Cobourg Offices Dr. Lucia Bohorquez, Michelle Arndt, Michelle Gavin, Helen Casmey, Annette Vlieg, Kris Koster-Lilly, Yvonne Carol Lindsay Adult Probation and Parole Services Samantha Brooks Peterborough Victoria Northumberland Clarington Catholic District School Board Elaine Mason Peterborough-Lakefield Community Police Services Sherry Jank Union of Ontario Indians
Chochi Knott, Lynda Banning, Laura Liberty, Laurie McLeod-Shabogesic

28
Contact Information
“
“The case consultation allowed me to advocate more
successfully by giving Best Practice methods for FASD. I used
that to guide the IEP process. Having the case consultation with
my child’s educators resulted in more ownership for success in
school. We all understand key principles of non-competency vs.
non-compliance and this helps get buy-in from the school. It has
reduced calls to pick up my child and eliminated the use of
restraints.” Parent
“This initiative allowed me the opportunity to access the training needed to
better serve families in our area living with Fetal Alcohol. It has not only
helped me build a broader knowledge range of FASD but it contributed to
the efficiency in which I can serve the clients in our region.” SR-T member
FASD Peterborough Office Tri-County Community Support Services Debra Lloyd FASD Manager 349A George Street North, Suite 303 Peterborough, Ontario K9H 3P9 Phone: (705) 876-9245 #226 Fax: (705) 876-9247 Email: [email protected] http://www.fasdpeterborough.ca
Chair, Peterborough County FASD Committee Sheryl Over Five Counties Children's Centre 872 Dutton Road, Peterborough, Ontario K9H 7G1 Phone: (705) 748-2221 #359 Fax: (705) 748-3526 Email: [email protected]
Report produced by: Sheila Burns, FASD Consultant, M.S. & Associates, Ajax Ontario Email: [email protected] Phone: 905-426-6453 October 2013





























![1 CHILDREN AND NEURODEVELOPMENTAL BEHAVIOURAL INTELLECTUAL DISORDERS (NDBID) TRAINING FOR THE HEALTH SECTOR [Date …Place …Event…Sponsor…Organizer] Children's](https://img.pdfslide.net/doc/110x75/56649e035503460f94aeeb53/1-children-and-neurodevelopmental-behavioural-intellectual-disorders-ndbid.jpg)