Embed Size (px)
Citation preview
Fastidious bacteria2
Jan TkadlecDept. of medical microbiology
Winter 2020
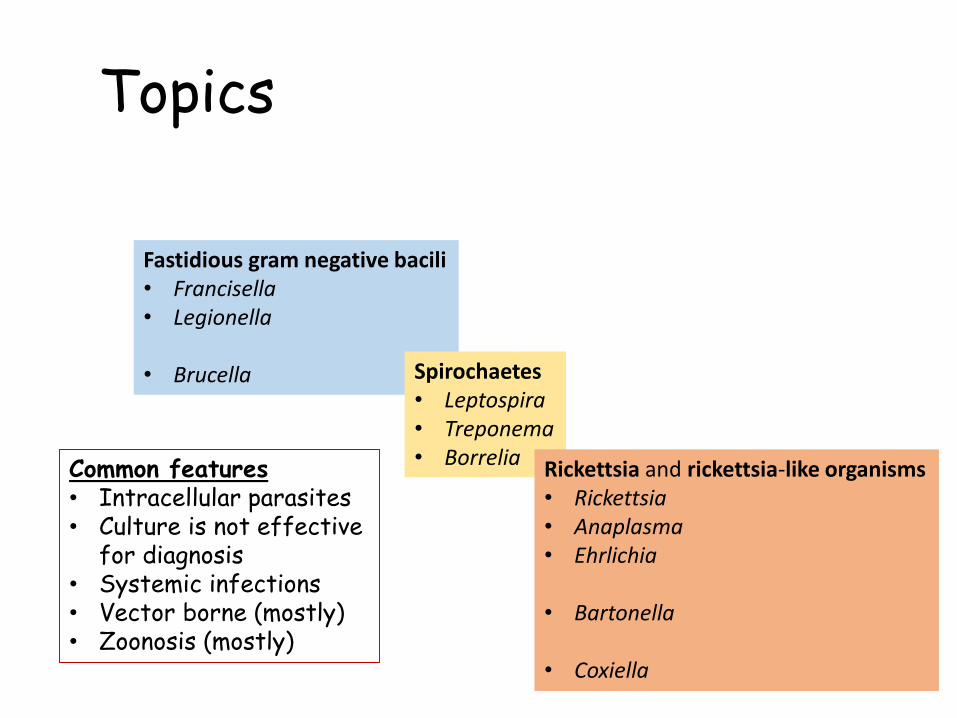
Topics
Fastidious gram negative bacili• Francisella• Legionella
• Brucella Spirochaetes• Leptospira• Treponema• Borrelia Rickettsia and rickettsia-like organisms
• Rickettsia• Anaplasma• Ehrlichia
• Bartonella
• Coxiella
Common features• Intracellular parasites• Culture is not effective
for diagnosis• Systemic infections• Vector borne (mostly)• Zoonosis (mostly)
Diagnosis of rare fastidiousbacteria is challengingWhen infection caused by fastidius patogen occurs rarely outcome could be worsebecause:
1. Looking for non fastidious patogens delays detection of true cause• Patogen will be detected after rulling out more common causes
2. Non fastidious patogen is taken as true cause• Treating wrong patogen
3. Not using apropriated method• Patogen would not be detected at al
It is important to know fastidious patogens and their typical symptomsand risk factors – it could by life-saving knowledge
Logistical challenge
Be aware that not all microbiology departments perform detection offastidious agents
1. It is too rare to be economical to have apropriate method
2. It is too laborious/expensive…
3. It is dangerous (highly infectious agens)
Detection or confirmatin of detection of some fastidious agents is performed only by specialised/reference laboratories
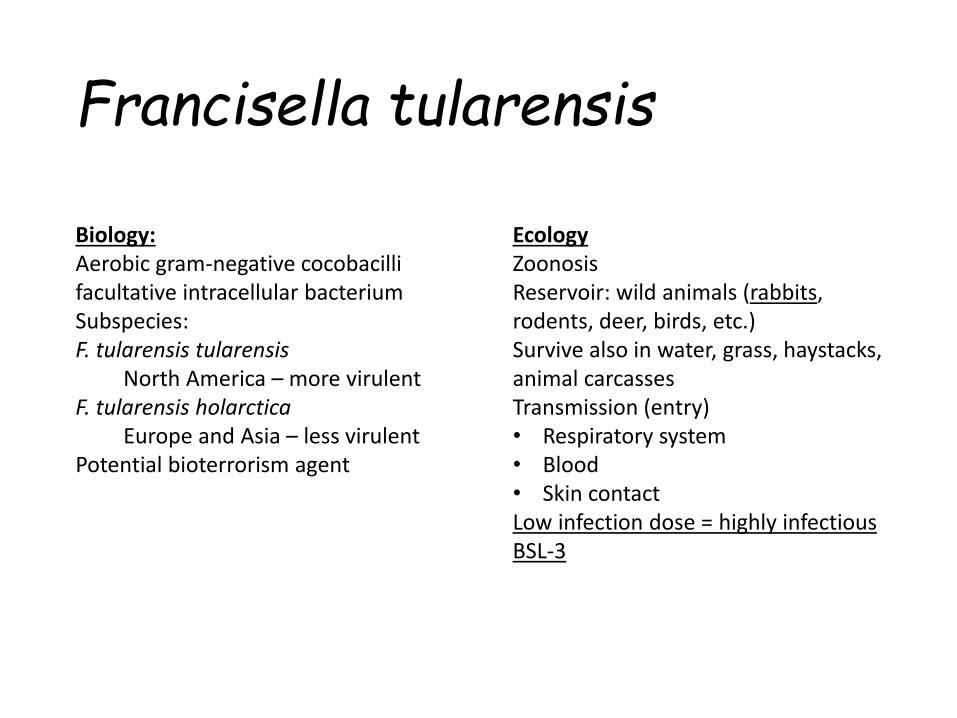
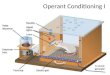
Francisella tularensis
Biology:Aerobic gram-negative cocobacillifacultative intracellular bacteriumSubspecies:F. tularensis tularensis
North America – more virulentF. tularensis holarctica
Europe and Asia – less virulentPotential bioterrorism agent
EcologyZoonosisReservoir: wild animals (rabbits, rodents, deer, birds, etc.)Survive also in water, grass, haystacks, animal carcassesTransmission (entry)• Respiratory system• Blood• Skin contactLow infection dose = highly infectiousBSL-3
Francisella tularensis
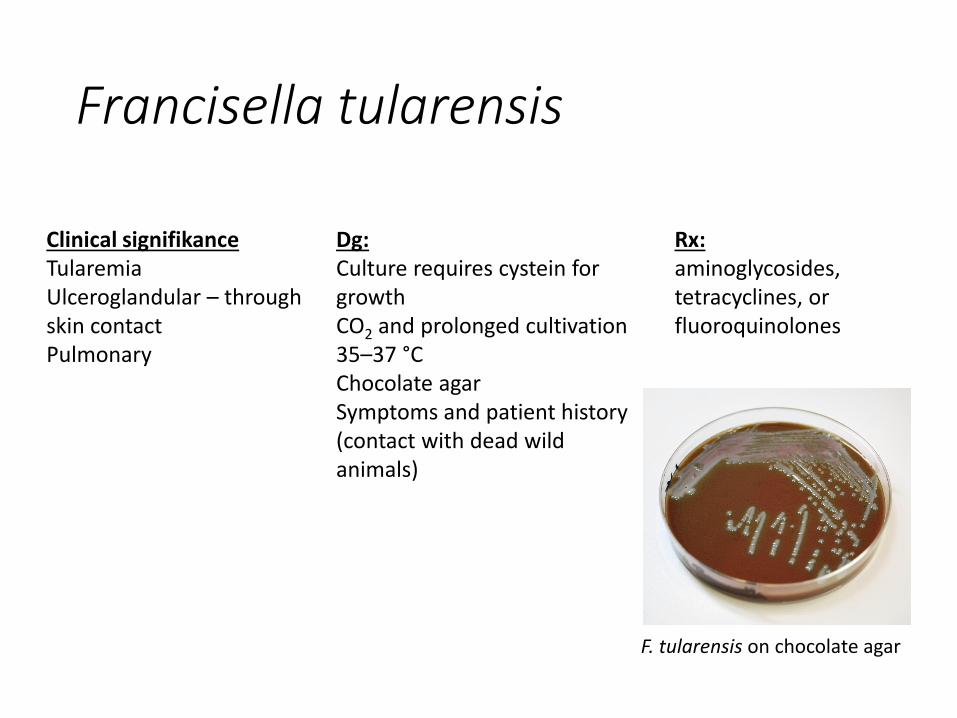
Rx:aminoglycosides, tetracyclines, orfluoroquinolones
Dg:Culture requires cystein forgrowthCO2 and prolonged cultivation35–37 °CChocolate agarSymptoms and patient history(contact with dead wildanimals)
Clinical signifikanceTularemiaUlceroglandular – throughskin contactPulmonary
F. tularensis on chocolate agar
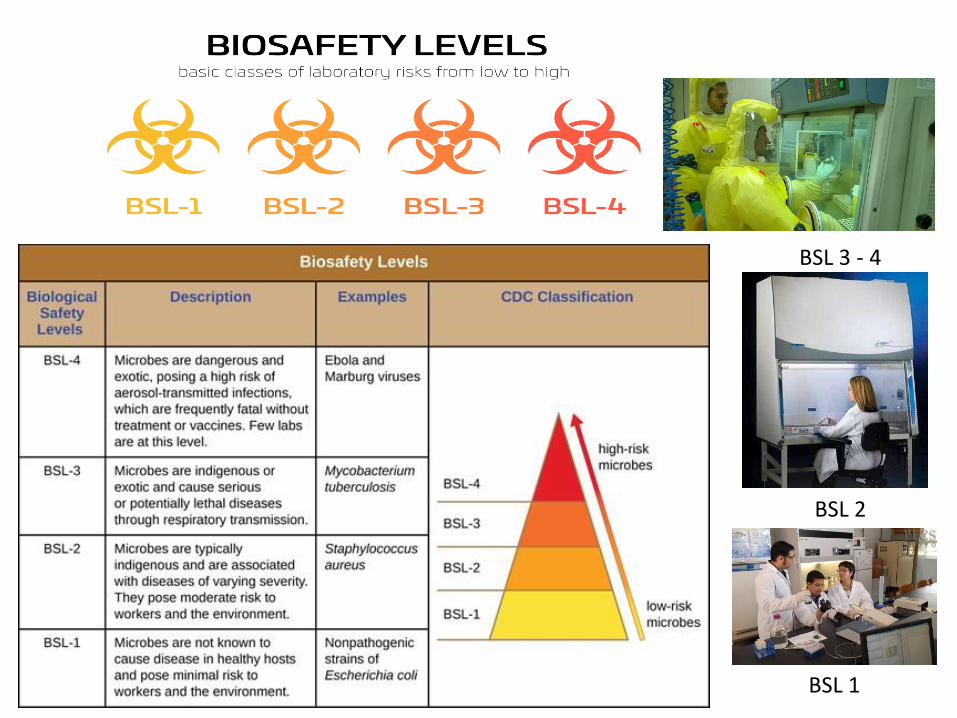
BSL 3 - 4
BSL 1
BSL 2
(A) buffered
charcoal yeast
extract;
(B) chocolate agar
medium;
(C)sheep’s blood
agar;
(D)cysteine heart
agar.
Pathogen profile
dictionary
ppdictionary.com
Francisella tularensis - culture
Brucella
Biology:Strictly aerobic gram-negative cocobacillifacultative intracellular bacteriumSpecies:
B. abortus (cattle)B. melitensis (sheep and goat)B. suis (pig)B. canis (dog)
survive in soil, manure and dustfor weeks or months, and remain viable in dead fetal material for even longer
EcologyZoonosisReservoir: animals (sheep, cattle, orpigs, etc.)Transmission• contaminated food (such as
unpasteurized milk products, meatproducts)
• direct contact with an infected animal
• inhalation of aerosols
Low infection dose - level BSL-3B. melitensis is still prevalent in Mediterranean countries, the Middle East, central and southern Asia, and parts of Africa and South America
BrucellaClinical signifikanceBrucellosissepticaemic illness, undulant fever. Most human disease is caused by Brucella melitensis,B. abortus or B. suis.
Brucellosis can present as an acute or subacute pyrexial illness that may persist for months or develop into a focal infection that can involve almost any organ system. The characteristicintermittent waves of increased temperature that gave the name undulant fever to the human disease are now usually seen only in long-standing untreated cases.Affects gastrointestinal tract including anorexia, abdominal pain, vomiting, diarrhea, constipation, hepatomegaly, and splenomegaly
Less frequently arthritis (hip, knee, and ankle), spondylitis, osteomyelitis, and sacroiliitisRarely endokarditis
Infection in animal has economical impact – in pregnant animals oftenleads to abortion,
Brucella
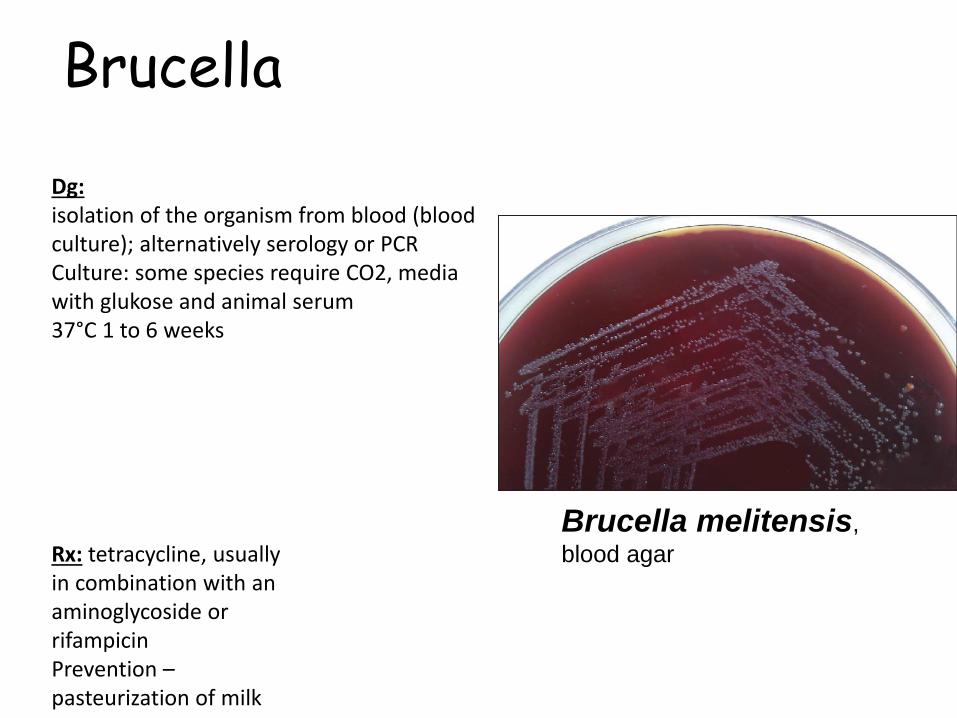
Dg:isolation of the organism from blood (bloodculture); alternatively serology or PCRCulture: some species require CO2, media with glukose and animal serum37°C 1 to 6 weeks
Rx: tetracycline, usuallyin combination with an aminoglycoside or rifampicinPrevention –pasteurization of milk
Brucella melitensis,
blood agar
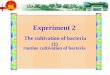
Legionella
Biology:Gram-negative rodsL. pneumophila
Other species less frequente.g. L. longbeachae
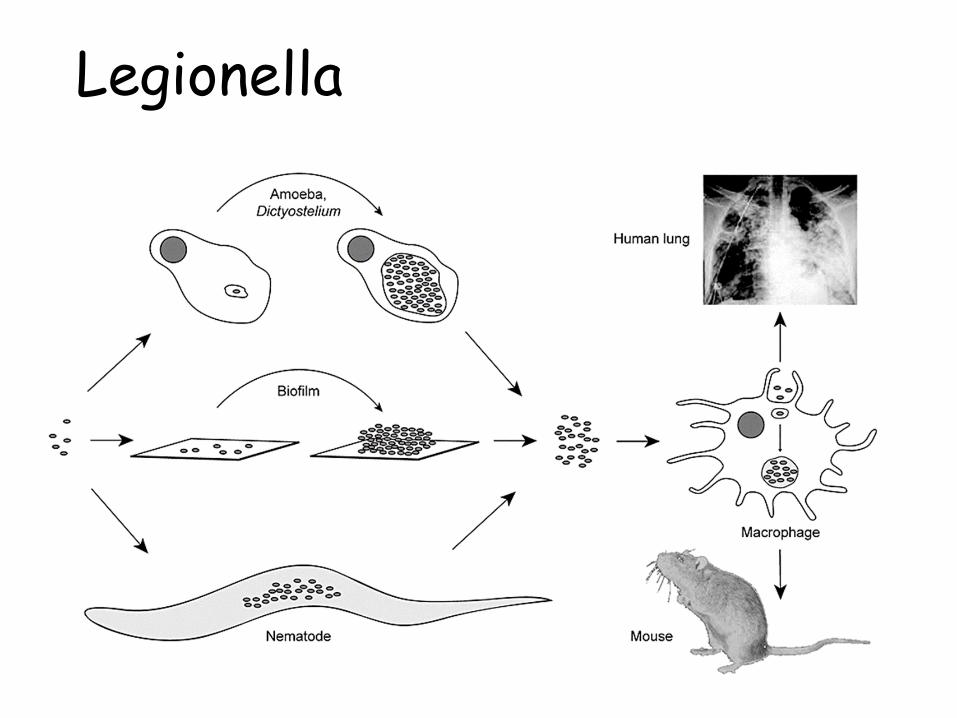
Epidemiology:Frequent in water – intracelularly in amoebas (Acanthamoeba, Naegleria) and other protozoaWarm water sourcesSpread through aircondition and untreatedwater supplyInhaling aerosol or droplets containinglegionellaInhaled bacteria are engulfed by monocytes and can survive therein as intracellular parasites
Legionella
LegionellaClinical significance:Legionnaires disease (mostly L. pneumophila serogroup 1)
pneumonia, up to 10% mortality when not treatedhigh fever, respiratory distress, scanty sputumconfusion, hallucinationsRenal impairement could be presentPotential to cause outbreak (hospitals!!!) –contaminated water supply
Risk factors: immunosuression, higher age (over 40y)Stays in hotels in low income countries
Pontiac fever – non-pneumonic, non-fatal, influenza-likesymptoms, high attack rate – most of the affected peopledevelop disease
History1976 first outbreak of 182 cases of pneumonia, mainly affecting members of the American Legion,occurred at a convention inPhiladelphia = legionnaires diseaseSpread through air condition
LegionellaDg: Sample: sputum and other respiratory specimen, lung biopsy –PCR or culturerequire cystein and iron grow best on buffered charcoal yeastextract agar (BCYE) with antibioticsCulture about 1 week, increased CO2Heat stable – sample could be heated to 50°C for 30 min to diminiss growth of other bacteriaATB testing is not performed (too laborious)Antigen detection in urine (ELISA) – commonly used, Serology – IG could be detected 8-10 days from start of thesymptoms
Rx:Legionnaires disese –intravenous azitromycin, combined withfluoroquinolones and/orrifampicin in severe cases
PreventionWater treatment:• heat• disinfection with chlorine or other biocides,including chlorine dioxide• copper–silver ionization.

Legionella pneumophila, Gram stain
By courtesy of MUDr. Petra Kabelíková
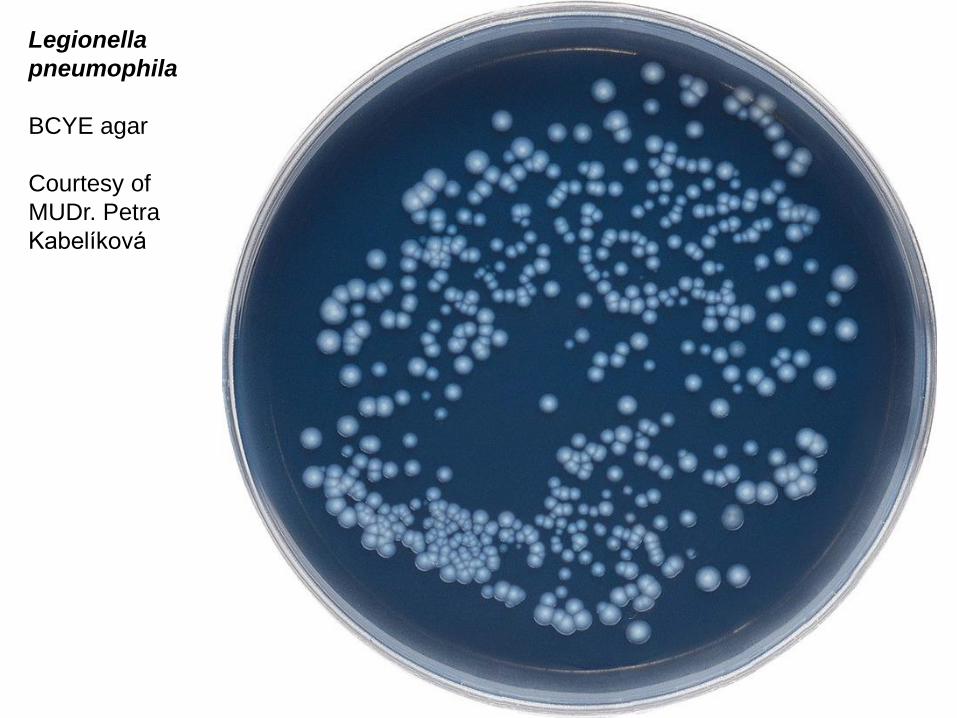
Legionella
pneumophila
BCYE agar
Courtesy of
MUDr. Petra
Kabelíková

Spirochaetes
Spirochaetes
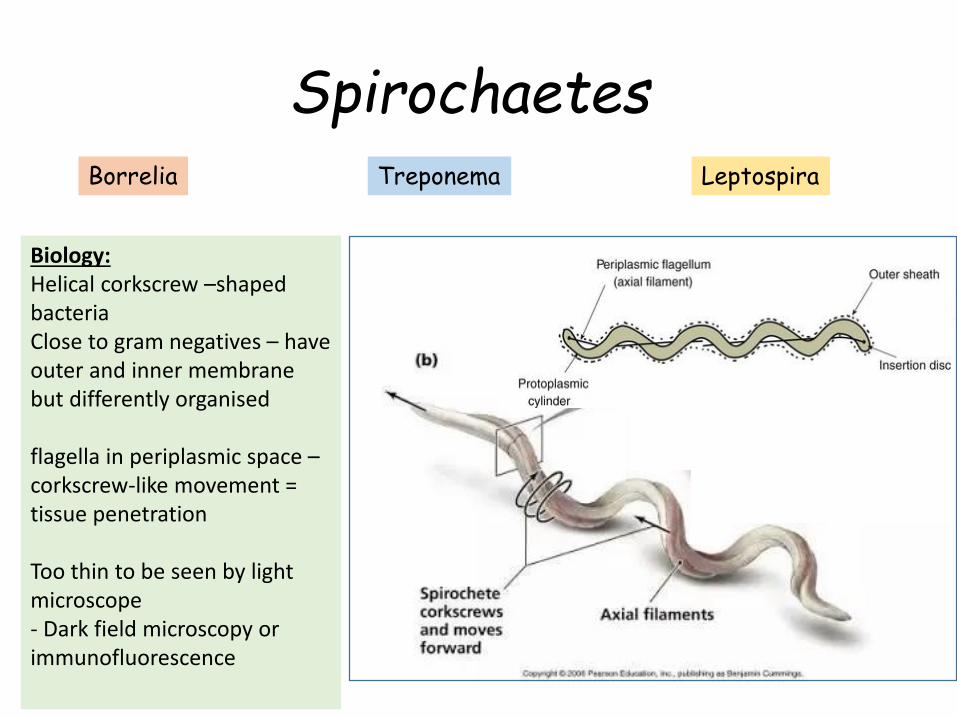
Biology:Helical corkscrew –shapedbacteriaClose to gram negatives – haveouter and inner membranebut differently organised
flagella in periplasmic space –corkscrew-like movement = tissue penetration
Too thin to be seen by lightmicroscope- Dark field microscopy orimmunofluorescence
Borrelia Treponema Leptospira

Different shapes of spiropchaetes
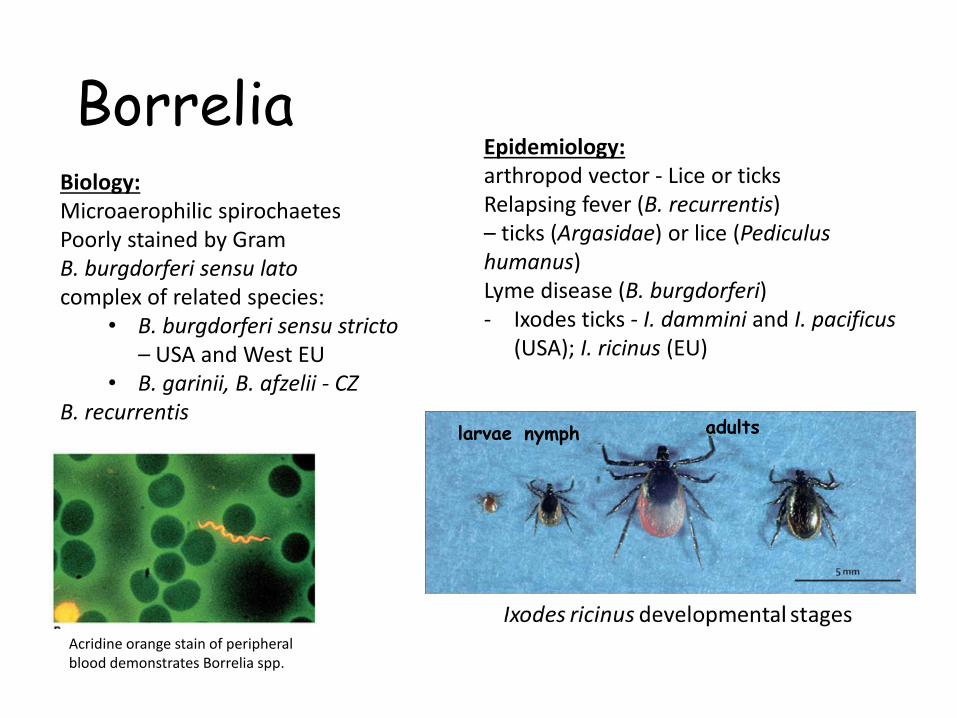
BorreliaBiology:Microaerophilic spirochaetesPoorly stained by GramB. burgdorferi sensu latocomplex of related species:
• B. burgdorferi sensu stricto– USA and West EU
• B. garinii, B. afzelii - CZB. recurrentis
Epidemiology:arthropod vector - Lice or ticksRelapsing fever (B. recurrentis)– ticks (Argasidae) or lice (Pediculushumanus)Lyme disease (B. burgdorferi)- Ixodes ticks - I. dammini and I. pacificus
(USA); I. ricinus (EU)
Acridine orange stain of peripheral blood demonstrates Borrelia spp.
larvae nymph adults
Lyme disease (Lyme borreliosis)
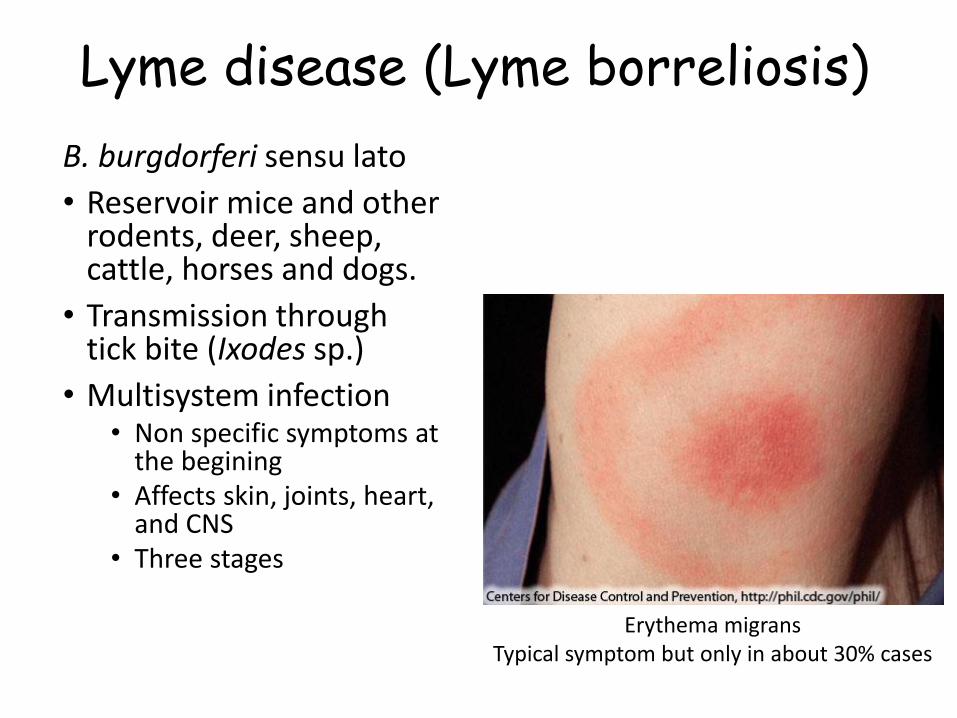
B. burgdorferi sensu lato
• Reservoir mice and otherrodents, deer, sheep, cattle, horses and dogs.
• Transmission throughtick bite (Ixodes sp.)
• Multisystem infection• Non specific symptoms at
the begining• Affects skin, joints, heart,
and CNS• Three stages
Erythema migransTypical symptom but only in about 30% cases
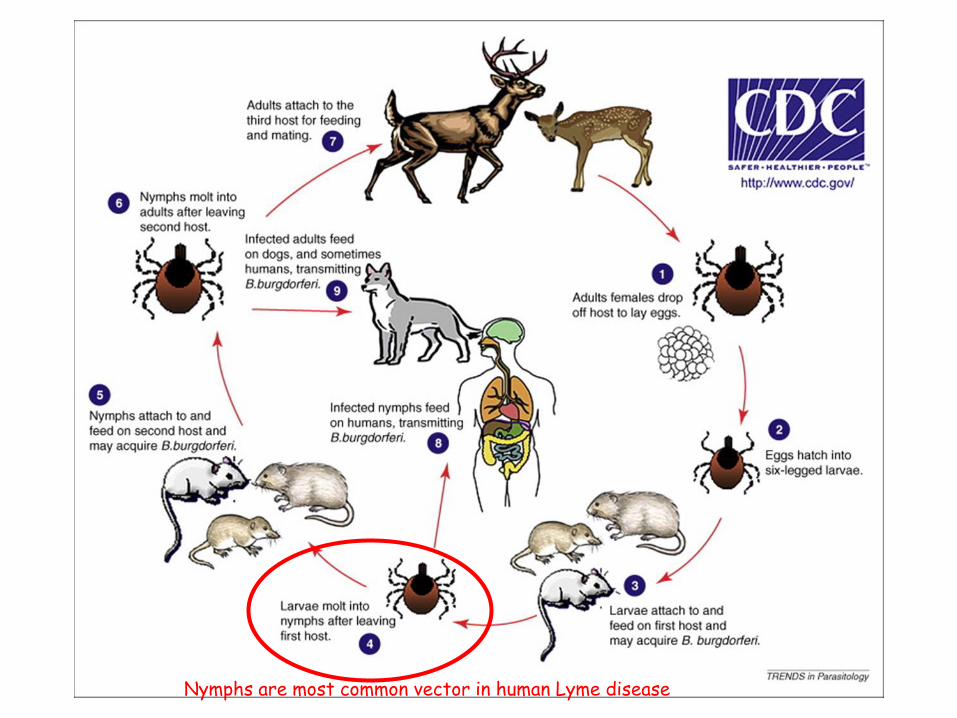
Nymphs are most common vector in human Lyme disease
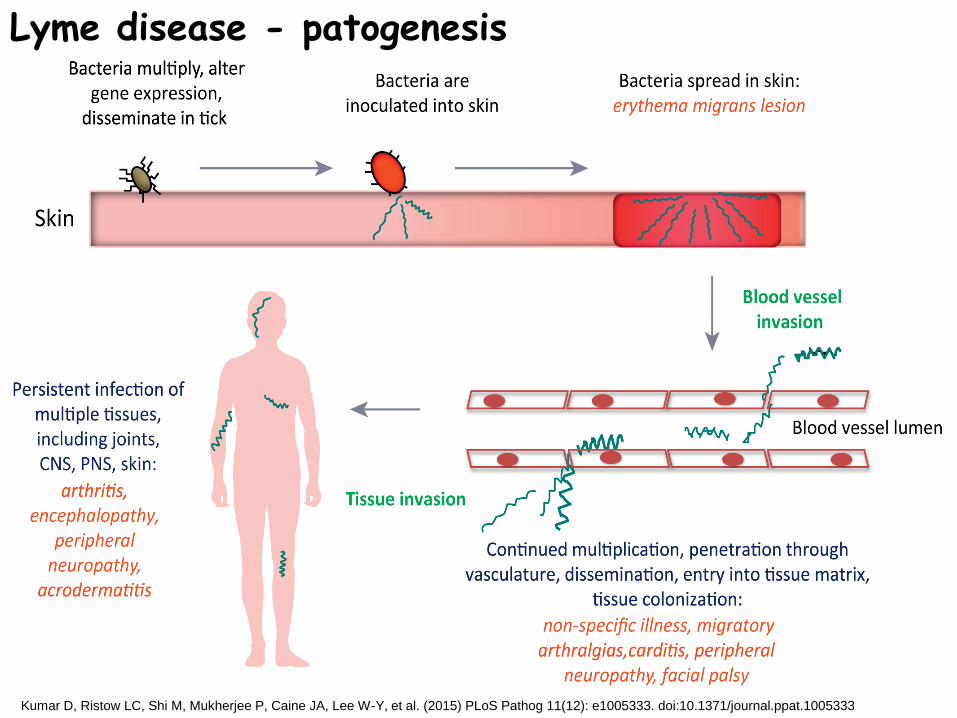
Kumar D, Ristow LC, Shi M, Mukherjee P, Caine JA, Lee W-Y, et al. (2015) PLoS Pathog 11(12): e1005333. doi:10.1371/journal.ppat.1005333
Lyme disease - patogenesis
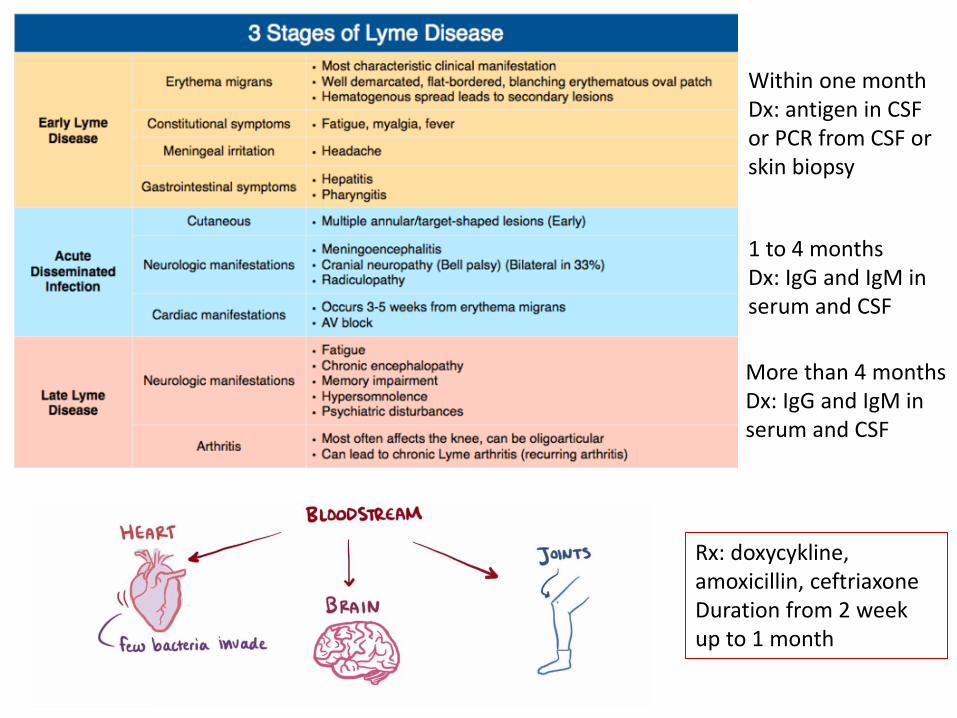
Within one monthDx: antigen in CSFor PCR from CSF orskin biopsy
1 to 4 monthsDx: IgG and IgM in serum and CSF
More than 4 monthsDx: IgG and IgM in serum and CSF
Rx: doxycykline, amoxicillin, ceftriaxoneDuration from 2 weekup to 1 month
Relapsing fever (typhus recurrentis)
• Borrelia recurrentis
• Human is only reservoir
• Transmission: human louse (Pediculus humanus)
• Associated with poor hygiene conditions (low incomecountries, homeless people,…)
• Symptoms: Fever returning each 5-10 days, hepatosplenomegaly, ikterus
• Dx: Serology
• Rx: doxycycline
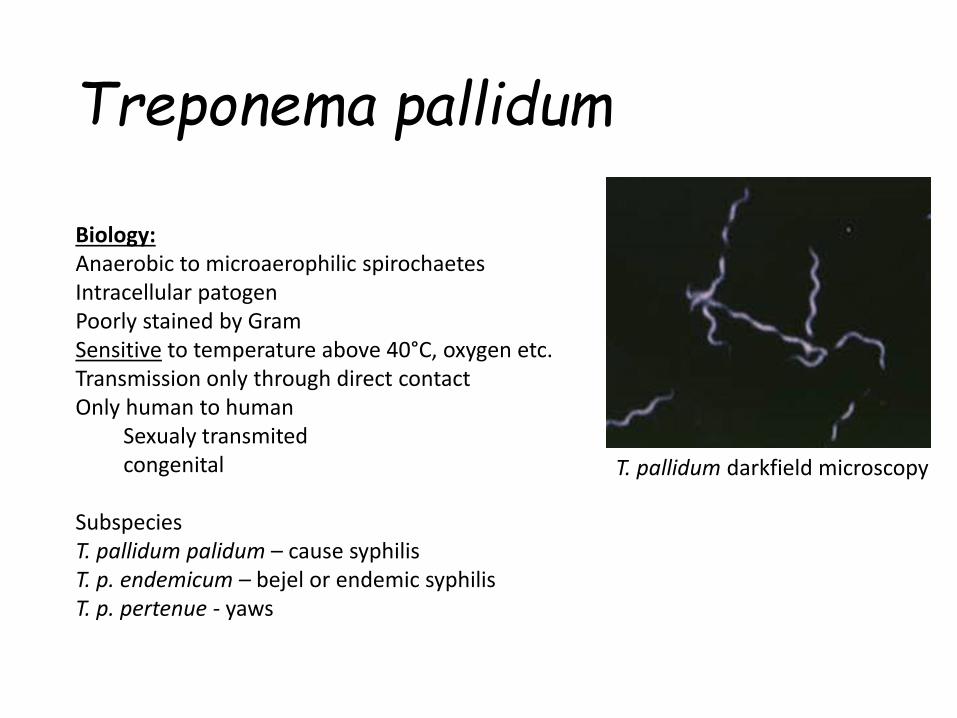
Treponema pallidum
Biology:Anaerobic to microaerophilic spirochaetesIntracellular patogenPoorly stained by GramSensitive to temperature above 40°C, oxygen etc.Transmission only through direct contactOnly human to human
Sexualy transmitedcongenital
SubspeciesT. pallidum palidum – cause syphilisT. p. endemicum – bejel or endemic syphilisT. p. pertenue - yaws
T. pallidum darkfield microscopy
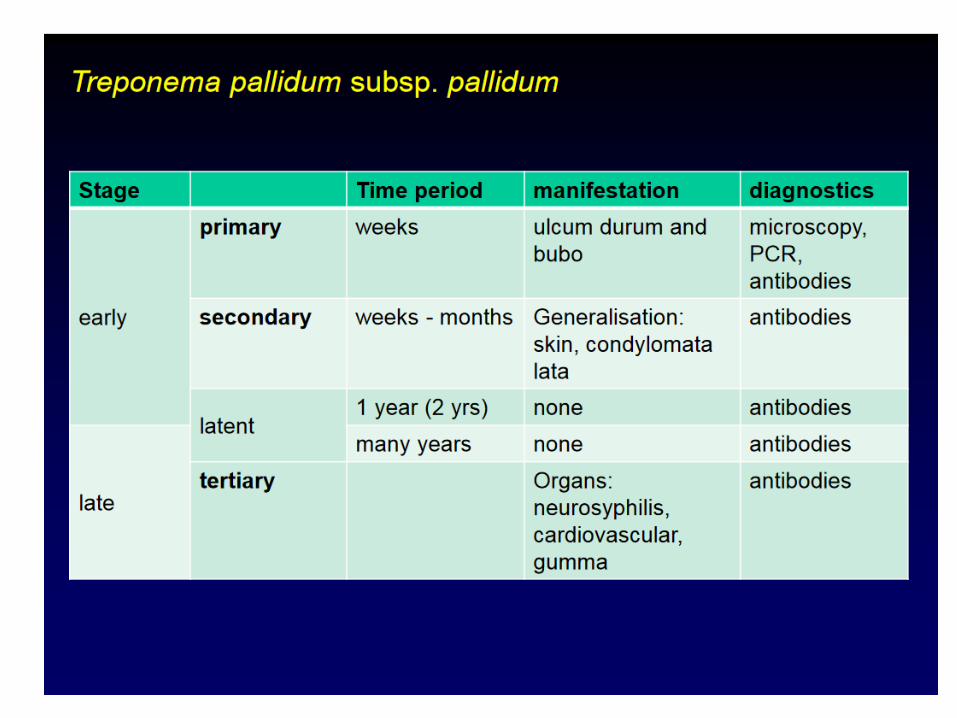
Treponema pallidumClinical significance:Syphilis – STD
Penetration through skin lessions or through mucousmembranesTisuse destruction due to immune response
Forms/stages1. Primary
Localised necrosis and ulceration(ulcus durum) lymphadenophaty, highly infectious detectable Ig
2. SecondarySkin, mucous epitelia and systemic symptoms, CNS (encephalitis), highy infectious, detectable Igs
3. Latent – non infectious live long stage4. Tertiary – after 10 to 25 y - cardiovascular and CNS
(neurosyphilis) symptoms progressive paralysis• Congenital
Treatment - Penicilin
Prevention
Mandatory screening newborns etc
Monitoring of STDs
Dg:SampleUrineSwab (urethra, cervix, vagina)Swab from skin lessionsSerum
MethodsMicroscopy dark field or fluorescent antibody staining.PCR – only early stageSerologyNontreponemal (reagin) antibodies
Venereal Disease Research Laboratory (VDRL) test – CSF, flockulation, agglutinationRapid plasma reagin (RPR) test
Treponemal antibodiesT. pallidum indirect hemagglutination (TPHA), agglutinationT. pallidum particle agglutination (TP-PA) test, agglutinationELISA
Treponema pallidum
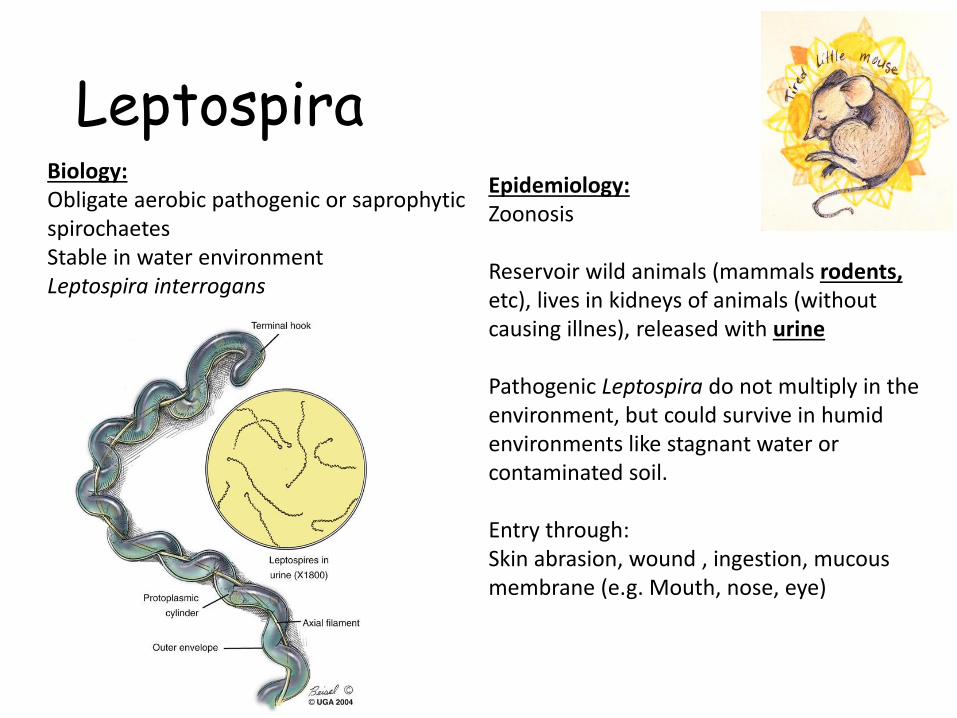
LeptospiraBiology:Obligate aerobic pathogenic or saprophyticspirochaetesStable in water environmentLeptospira interrogans
Epidemiology:Zoonosis
Reservoir wild animals (mammals rodents, etc), lives in kidneys of animals (withoutcausing illnes), released with urine
Pathogenic Leptospira do not multiply in the environment, but could survive in humidenvironments like stagnant water or contaminated soil.
Entry through:Skin abrasion, wound , ingestion, mucousmembrane (e.g. Mouth, nose, eye)

Faisal S.M., McDonough S.P., Chang YF. (2012) Leptospira: Invasion, Pathogenesis and
Persistence. In: Embers M. (eds) The Pathogenic Spirochetes: strategies for evasion of host
immunity and persistence. Springer, Boston, MA. https://doi.org/10.1007/978-1-4614-5404-5_8
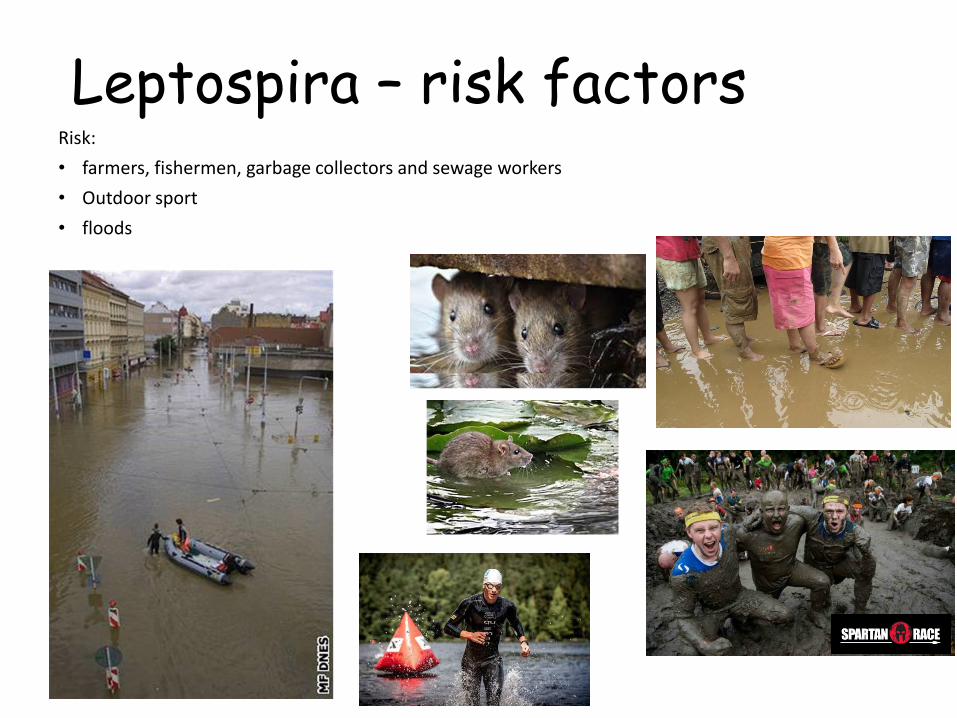
Leptospira – risk factorsRisk:
• farmers, fishermen, garbage collectors and sewage workers
• Outdoor sport
• floods
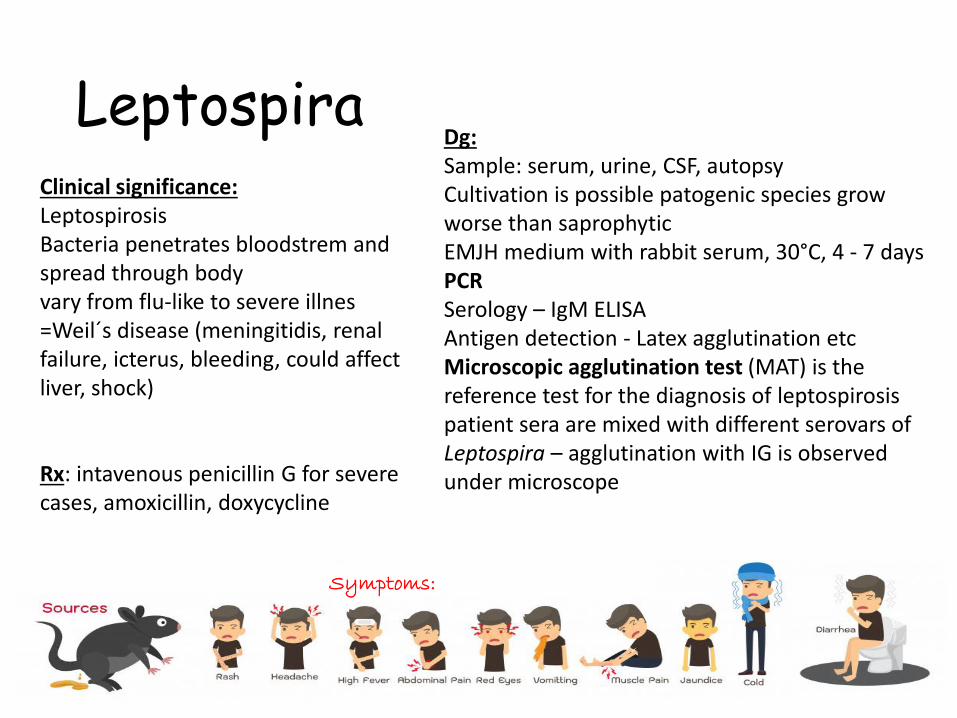
LeptospiraDg:Sample: serum, urine, CSF, autopsyCultivation is possible patogenic species growworse than saprophyticEMJH medium with rabbit serum, 30°C, 4 - 7 daysPCRSerology – IgM ELISAAntigen detection - Latex agglutination etcMicroscopic agglutination test (MAT) is the reference test for the diagnosis of leptospirosispatient sera are mixed with different serovars of Leptospira – agglutination with IG is observedunder microscopeRx: intavenous penicillin G for severe
cases, amoxicillin, doxycycline
Clinical significance:LeptospirosisBacteria penetrates bloodstrem and spread through bodyvary from flu-like to severe illnes=Weil´s disease (meningitidis, renalfailure, icterus, bleeding, could affectliver, shock)
Symptoms:
Rickettsia and related patogens
RickettsialesRickettsiaAnaplasmaEhrlichia
Bartonella Coxiella
Rickettsia in general
Biology:Gram-negative, highly pleomorphic bacteria, obligateintracellular patogensSmall genomePrimar human patogenSensitive to environmentalchanges
Spoted fever groupR. rickettsiiR. akari
Typhus groupR. prowazekiiR. typhi
EpidemiologyzoonosesAnimal or human host arthropod vector
Dg:Symptom based suspitionSerology: Weil–Felix testMixing patient serum with rickettsial antigenWhen antibodies present agglutination appearsPCR
Penetrrates through skin into blood stream, infects endothelium of bloodstream vessels in multiple organs
Rx: tetracyclines - doxycycline

Spoted fever group
Rickettsia rickettsii (Western Hemisphere)• Rocky Mountain spotted fever• Tick-borne Dermacentor sp = Dog tick• Reservoir dogs and rodents• Infection in children during spring (tick activity)• Suden fever, headache, myalgia• Typical rash spreading from limbs to trunk• Fatal if untreated
Rickettsia akari (USA, former Soviet Union)• Rickettsialpox• Mite-borne Liponyssoides sp• Reservoir mice• Mild disease, nonfatal, self-limiting• Vesicular rash, fever, lymphadenopatty
Petechial rash on the arm caused by Rocky Mountain spotted fever
Rickettsialpox rash
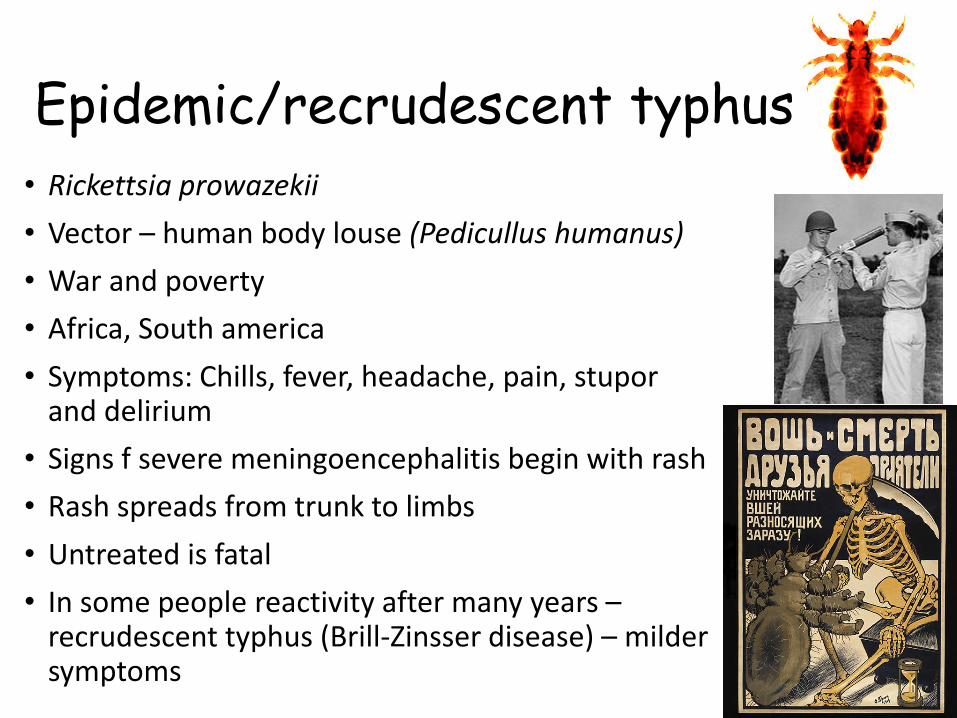
Epidemic/recrudescent typhus
• Rickettsia prowazekii
• Vector – human body louse (Pedicullus humanus)
• War and poverty
• Africa, South america
• Symptoms: Chills, fever, headache, pain, stuporand delirium
• Signs f severe meningoencephalitis begin with rash
• Rash spreads from trunk to limbs
• Untreated is fatal
• In some people reactivity after many years –recrudescent typhus (Brill-Zinsser disease) – mildersymptoms
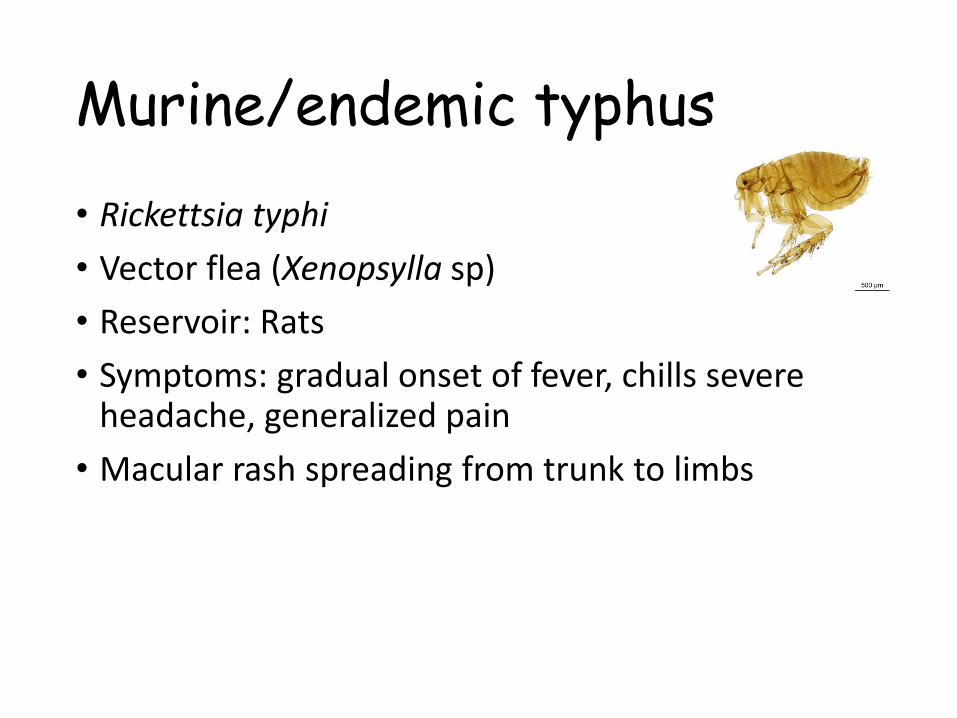
Murine/endemic typhus
• Rickettsia typhi
• Vector flea (Xenopsylla sp)
• Reservoir: Rats
• Symptoms: gradual onset of fever, chills severe headache, generalized pain
• Macular rash spreading from trunk to limbs

Ehrlichia and Anaplasma
Biology:Obligate intracellular patogensPreference to WBC – mononuclear cells
EpidemiologyZoonosisTick borne, reservoir: wild animals and dogs
Dg:PCR (blood)Serology
Rx: doxycycline
Clin. significanceHuman monocytic ehrlichiosis (HME)
Ehrlichia chaffeenisUSA
Human granulocytic ehrlichiosisAnaplasma phagocytophilumUSA but also EU and Asia
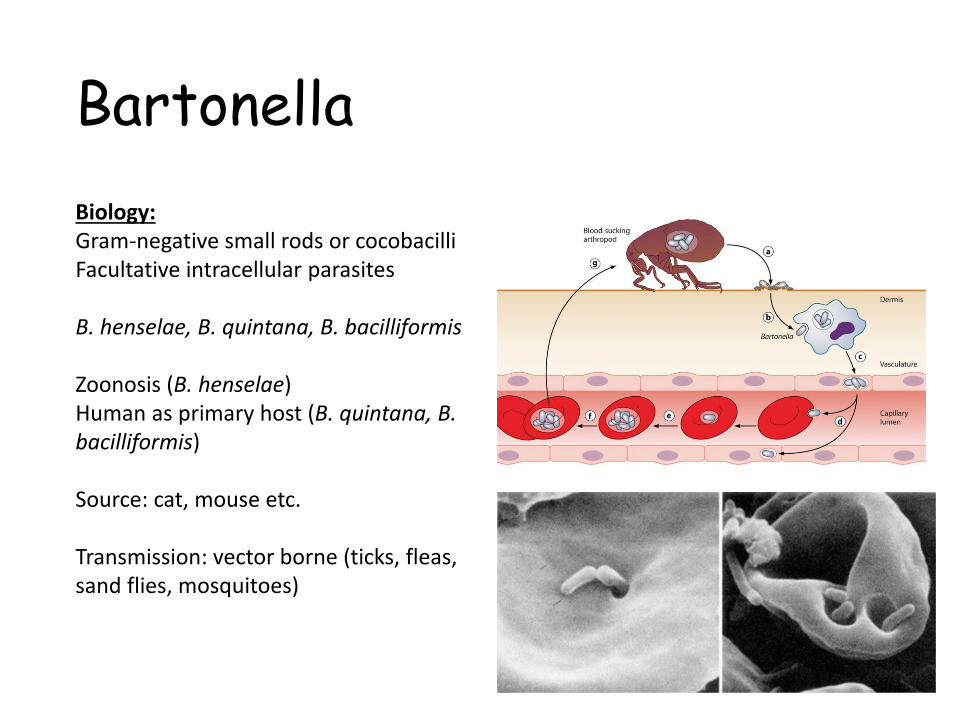
Bartonella
Biology:Gram-negative small rods or cocobacilliFacultative intracellular parasites
B. henselae, B. quintana, B. bacilliformis
Zoonosis (B. henselae)Human as primary host (B. quintana, B. bacilliformis)
Source: cat, mouse etc.
Transmission: vector borne (ticks, fleas, sand flies, mosquitoes)
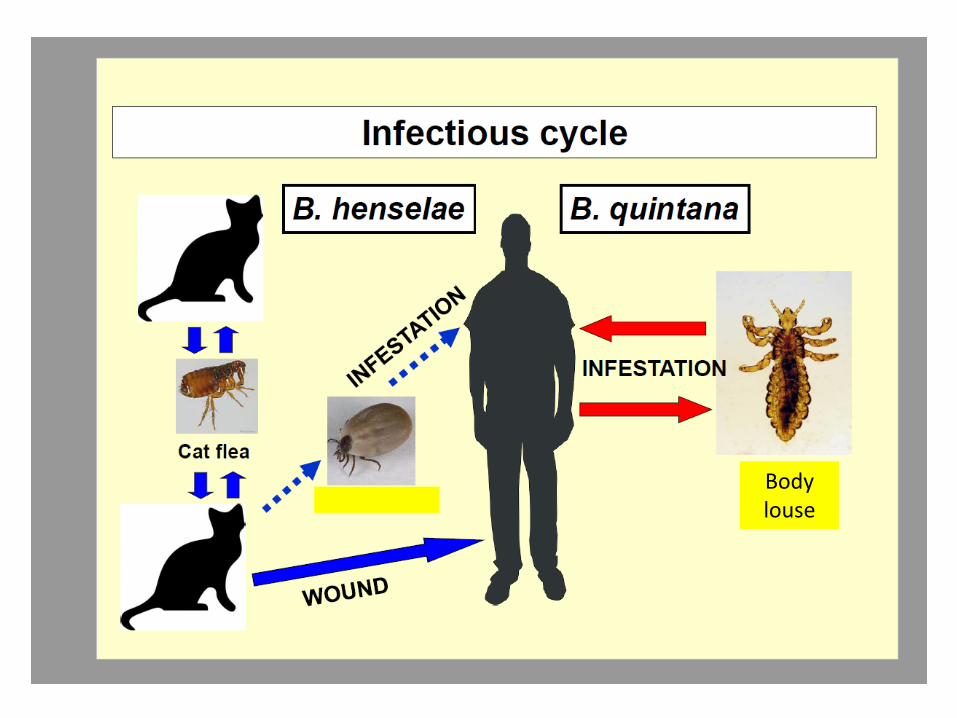
Body louse
Bartonella
Clinical signifikance• Cat-scratch disease – felinosis (B.
henselae) – local lymphadenopathy, mild disease (fever, headachetiredness), slow recovery – 4 – 12 months, speed up by ATB
Endocarditis (B. henselae, B. quintana)
Trench fever (B. quintana)Soldiers (WWI) or today homeless people
Bacillary angiomatosis (B. henselae, B. quintana) – skin lessions(papules ornodules) – vascularisedPresent in internal organs – potentiallyfatal if not treated
Rx:Long term terapy (6 weeks and more)Tetracyclines, aminoglycosides, macrolides
Dg.Culture – CO2, at least two weeks, enriched mediaSample has to be treated withdetergent to release intracelularbacteria
Serology – antibody cross reactivitywith other bacteria, antibodies are often not producedPCR
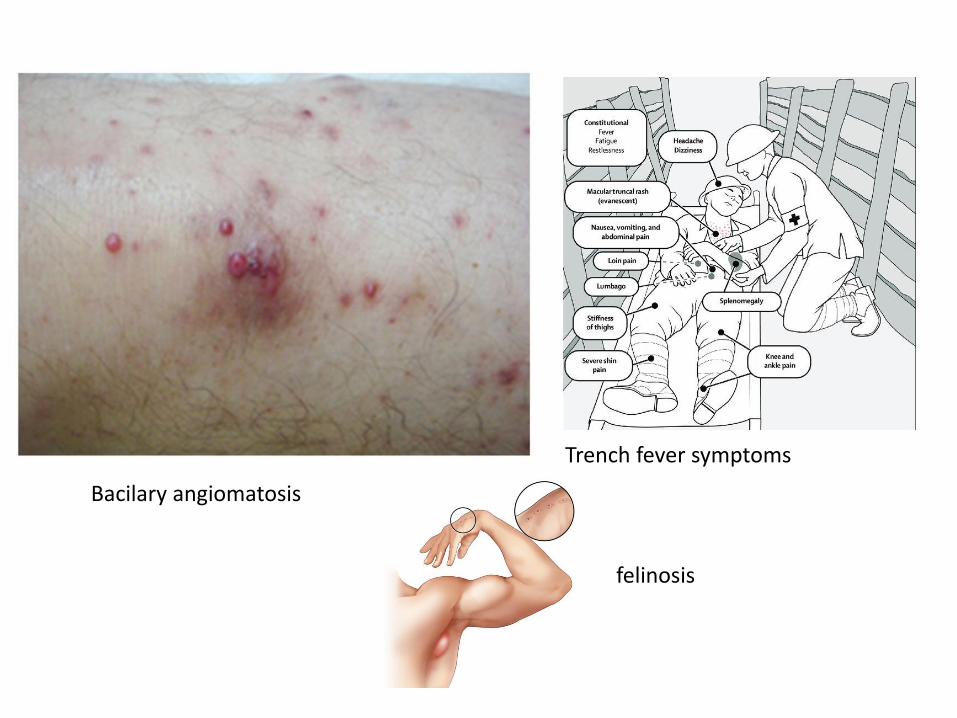
Bacilary angiomatosis
Trench fever symptoms
felinosis
Coxiella burneti
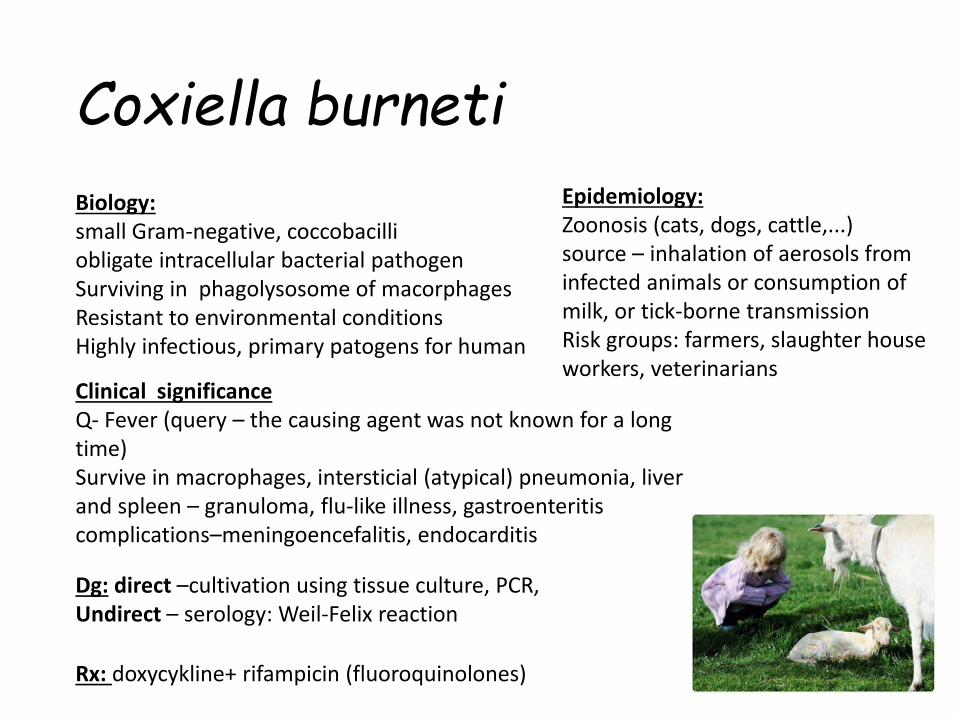
Biology:small Gram-negative, coccobacilliobligate intracellular bacterial pathogenSurviving in phagolysosome of macorphagesResistant to environmental conditionsHighly infectious, primary patogens for human
Epidemiology:Zoonosis (cats, dogs, cattle,...)source – inhalation of aerosols frominfected animals or consumption ofmilk, or tick-borne transmissionRisk groups: farmers, slaughter house workers, veterinarians
Clinical significanceQ- Fever (query – the causing agent was not known for a long time)Survive in macrophages, intersticial (atypical) pneumonia, liver and spleen – granuloma, flu-like illness, gastroenteritiscomplications–meningoencefalitis, endocarditis
Dg: direct –cultivation using tissue culture, PCR,Undirect – serology: Weil-Felix reaction
Rx: doxycykline+ rifampicin (fluoroquinolones)
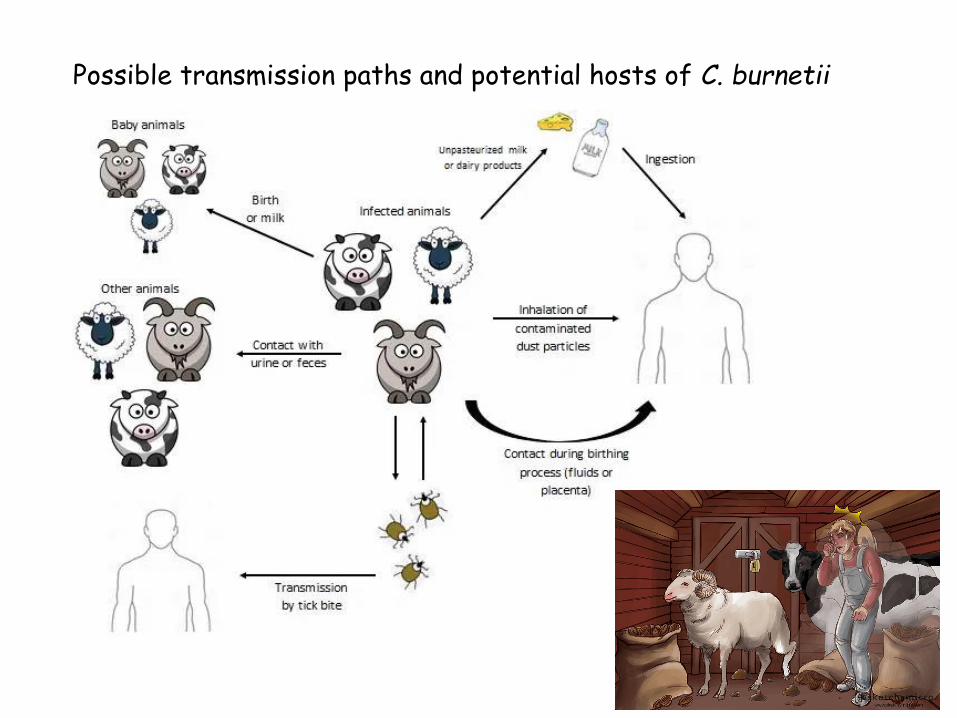
Possible transmission paths and potential hosts of C. burnetii
Take home messageFastidious bacteria (Francisella, Brucella, Legionella, Spirochates, Ricketssia etc.)
• Intracellular
• Culture is not possible or usefull – poor sensitivity and long time to result
• Serology! (or PCR, but not always)
• Symptoms (rash, lymphadenopaty, etc) and risk factors!
• Multi-organ infection, long term diseases = long term treatment.
• Zoonosis, vector borne (with exceptions e.g.T. pallidum)
Biggest thread in dealing with rare fastidious pathogens is that they could be easily forgotten and not treated in right time.