Embed Size (px)
Citation preview

Brain (1999),122,5–16
Fatal familial insomnia: a new Austrian familyG. Almer,1,* J. A. Hainfellner,2,* T. Brucke,1,† K. Jellinger,3 R. Kleinert,4 G. Bayer,5 O. Windl,6
H. A. Kretzschmar,6 A. Hill, 7 K. Sidle,7 J. Collinge7 and H. Budka2
1Clinic of Neurology, University of Vienna,2Austrian Correspondence to: Professor Herbert Budka, Institute ofReference Centre for Human Prion Diseases and Institute Neurology, AKH, Wa¨hringer Gurtel 18–20, POB 48,of Neurology, University of Vienna,3Ludwig Boltzmann A-1097 Wien, AustriaInstitute of Clinical Neurobiology, Hospital Lainz, Vienna, E-mail: H. [email protected] of Pathology, University of Graz,5Institute of
*Both authors contributed equally to this studyPathology, Hospital Oberwart, Austria,6Institute ofNeuropathology, University of Go¨ttingen, Germany and †Present address: Department of Neurology, Hospital7Imperial College at St Mary’s, London, UK Wilhelminenspital, Vienna, Austria
SummaryWe present clinical, pathological and molecular featuresof the first Austrian family with fatal familial insomnia.Detailed clinical data are available in five patients andautopsy in four patients. Age at onset of disease rangedbetween 20 and 60 years, and disease duration between8 and 20 months. Severe loss of weight was an earlysymptom in all five patients. Four patients developedinsomnia and/or autonomic dysfunction, and all fivepatients developed motor abnormalities. Analysis of theprion protein (PrP) gene revealed the codon 178 pointmutation and methionine homozygosity at position 129.In all brains, neuropathology showed widespread corticalastrogliosis, widespread brainstem nuclei and tractdegeneration, and olivary ‘pseudohypertrophy’ with
Keywords: fatal familial insomnia; prion diseases; prion protein; transmissible spongiform encephalopathies
Abbreviations: BSE 5 bovine spongiform encephalopathy; FFI5 fatal familial insomnia; GFAP5 glial fibrillary acidicprotein; HE5 haematoxylin–eosin; PCR5 polymerase chain reaction;PRNP5 PrP gene; PrP5 prion protein; PrPres 5protease resistant form of PrP; SSCP5 single-strand conformational polymorphism
IntroductionFatal familial insomnia (FFI) was first described in 1986 asan autosomal dominant heredopathy, clinically characterizedby progressive untreatable insomnia, dysautonomia and motorsigns (Lugaresiet al., 1986). Meanwhile, the disorder hasbeen recognized as a prion disease, thus enlarging thespectrum of familial spongiform encephalopathies consistingof familial Creutzfeldt–Jakob disease and Gerstmann–Straussler–Scheinker disease (Goldfarbet al., 1992; Medoriet al., 1992b). The neuropathological hallmark of FFI ispredominance of lesions in the thalamus (Manettoet al.,1992; Gambettiet al., 1995). Genetically, FFI is linked to aGAC to AAC point mutation (aspartic acid to asparaginesubstitution) at codon 178 of the prion protein (PrP) gene(PRNP) on chromosome 20 in conjunction with methionine
© Oxford University Press 1999
vacuolated neurons, in addition to neuropathologicalfeatures described previously, such as thalamic and olivarydegeneration. Western blotting of one brain andimmunocytochemistry in four brains revealed quantitativeand regional dissociation between PrPres (the proteaseresistant form of PrP) deposition and histopathology. Inthe cerebellar cortex of one patient, PrPres deposits wereprominent in the molecular layer and displayed a peculiarpatchy and strip-like pattern with perpendicularorientation to the surface. In another patient, a singlevacuolated neuron in the inferior olivary nuclei containedprominent intravacuolar granular PrP res deposits,resembling changes of brainstem neurons in bovinespongiform encephalopathy.
at the polymorphic position 129 of the mutant allele (Goldfarbet al., 1992; Medoriet al., 1992b).
We report here the first Austrian family with FFI in fiveconsecutive generations. We present detailed clinical featuresof five patients, and neuropathological and molecular geneticanalysis of four patients. Data on this new family have beenpublished in part as abstracts (Almeret al., 1997; Budkaet al., 1997; Hainfellneret al., 1997a).
MethodsInformation on the pedigree was collected by reviewing allpertinent medical and non-medical records, and notably byinterviews with family members. In patients III-5, III-13
Dow
nloaded from https://academ
ic.oup.com/brain/article/122/1/5/330287 by guest on 28 D
ecember 2021

6 G. Almeret al.
and IV-13, clinical data were retrieved retrospectively frommedical records. Patients IV-5 and IV-8 underwent personal(G.A. and T.B.) neurological examination, and had severalEEGs, CT and MRI.
Neuropathological and molecular genetic analysis wereperformed in patients III-5, IV-5, IV-8 and IV-13. Autopsyof patients IV-5 and IV-8 was done after 20 h post-mortemand was restricted to the brain including the upper cervicalspinal cord. Numerous tissue blocks of cerebral cortex, basalganglia, brainstem and cerebellar cortex were sampled andfrozen. The remaining brain was immersion-fixed in 4%formalin for 2 weeks and cut. Coronal slices of cerebrum,an axial whole-mount slice of cerebellum and pons, andnumerous smaller tissue blocks including all major brainregions were embedded in paraffin. Archival paraffin blockscontaining various brain regions of patient III-5, whosuccumbed in 1991, and patient IV-13, who succumbed in1986, were retrieved from two municipal Austrian(neuro)pathology laboratories. In addition, paraffin embeddedblocks of lungs, kidney, liver and spleen of patient IV-13were available. Histological work-up was performed on 5µmthick sections with conventional and immunocytochemicalstains. Conventional stains comprised haematoxylin–eosin(HE), luxol fast blue/nuclear fast red, Kanzler method andBielschowsky silver impregnation. Immunolabelling used apolyclonal antibody against glial fibrillary acidic protein(GFAP) (Dako, Glostrup, Denmark), and monoclonalantibodies against neurofilament protein (NFP; clone NE14)(Dako), microtubule associated protein-2 (MAP2; cloneAP20) (Boehringer, Mannheim, Germany), synaptophysin(clone SY38) (Boehringer) and PrP (clone 3F4) (Dr R.Kascsak, Staten Island, NY, USA). For anti-PrPimmunocytochemistry, sections were pre-treated with a three-tiered protocol of hydrated autoclaving, concentrated formicacid and guanidine isothiocyanate (Goodbrandet al., 1995).Antibodies were followed by the avidin–biotin complexmethod (for monoclonals) or the peroxidase–anti-peroxidasetechnique (for polyclonals), with diaminobenzidine aschromogen for visualization. Grey matter lesioning wasevaluated on HE- and GFAP-stained sections bysemiquantitative assessment of neuronal loss, spongiformchange and astrogliosis (Table 1). Lesioning of tracts andwhite matter structures was evaluated by semiquantitativeassessment of regional nerve fibre degeneration on luxol fastblue/nuclear fast red stained sections (Table 2).
Analysis of PRNP was performed on genomic DNAisolated from the blood of patients IV-5 and IV-8 accordingto standard procedures (Sambrook, 1989). One hundrednanograms of DNA was used for PCR (polymerase chainreaction) amplification of the coding region ofPRNPusingthe primers 895W and 896W (Kretzschmaret al., 1986;Nicholl et al., 1995). The PCR product was inspected on a1% agarose gel for potential insertion mutations and deletions.Potential point mutations were screened by the single-strandconformational polymorphism (SSCP) technique (Oritaet al.,1989). For this purpose the coding region ofPRNP was
reamplified in four overlapping fragments which wereanalysed alongside thePRNPgene of patients with knownmutations (Windlet al., 1996). The genotypes of codons 129and 178 were examined by digestion with the restrictionendonucleasesNspI and Tth111I. The final sequenceconfirmation was obtained by solid-phase direct sequencingof the complete coding region ofPRNPafter reamplificationand purification of single-stranded PCR products using 59-biotinylated primers 895W and 896W and streptavidin-coupled Dynabeads M-280 (Dynal, Oslo, Norway). Thesequencing reactions were performed with the SequiThermEXCEL Long-Read Kit-LC (Epicentre Technologies,Madison, Wis., USA), according to the manufacturer’srecommendation, and 59-IRD-41 labelled oligonucleotides5HUSEQ (59-TCTCCTCTTCATTTTGCAGAGC-39) or3HUSEQ (59-GAAAGATGGTGAAAACAGGAAG-39). Thereaction products were loaded on a 4.3% Long-Rangergel (AT Biochem, Malvern, Pa., USA) and separated bydenaturing electrophoresis on an automated system (Model4000L; LI-COR, Lincoln, Nev., USA).
DNA from paraffin embedded brain tissue of patients III-5 and IV-13 was isolated using the QIAamp tissue kit(QIAGEN, Hilden, Germany). The DNA from this materialwas highly degraded. Therefore, two fragments ofPRNPwere amplified with two sets of primers. Primers 5CEN(59-AGGTGGCACCCACAGTCAGT-39) and 3CEN (59-AC-GGTCCTCATAGTCACTGCCG-39) amplified a fragmentencompassing the codons 93–148 ofPRNP, whereas primersP33 (59-CATGGATGAGTACAGCAACCAG-39) and P34(59-TCTGGTAATAGGCCTGAGATTC-39) amplified a frag-ment encompassing codons 166–228. PCR used identicalconditions to those used for the completePRNP codingregion, but two successive rounds of 35 PCR cycles werenecessary for a sufficient yield of PCR product for furtherexamination. Codons 129 and 178 were examined bydigestion with restriction endonucleasesNspI andTth111I aswell as direct sequencing. Sequencing was performed asoutlined above, but the 59-biotinylated primers 5CEN andP33 were used for purification of single-stranded PCRproducts and the 59-IRD-41 labelled primers 3CEN and P34for the sequencing reactions.
Western immunoblotting was performed with samples ofoccipital and precentral cortex, thalamus, basal ganglia,cerebellar cortex, brainstem and cervical spinal cord of patientIV-5. The tissue samples were homogenized in 9 volumes oflysis buffer (100 mM NaCl, 10 mM EDTA, 0.5% sodiumdeoxycholate, 10 mM Tris pH 7.4) by repeated passagethrough needles of decreasing diameter. The homogenateswere spun at 3000 r.p.m. for 5 min and the supernatantremoved to a fresh tube for analysis. Aliquots of thehomogenates were incubated at 37°C for 1 h with proteinaseK (at a final concentration ranging from 12.5–50µg/ml).The reactions were terminated by the addition of Pefabloc(Boehringer) to 1 mM. Samples were electrophoresed on16% Tris–glycine acrylamide gels and blotted as describedpreviously (Collingeet al., 1996). The blots were developed
Dow
nloaded from https://academ
ic.oup.com/brain/article/122/1/5/330287 by guest on 28 D
ecember 2021

A new Austrian family with FFI 7
Table 1 Regional severity of brain tissue lesioning in four Austrian FFI patients
Patient
IV-5 IV-8 III-5 IV-13
NL GL SP NL GL SP NL GL SP NL GL SP
Cerebral cortexFrontal cortex 0 2 0 0 1 1† 0 2 0 0‡ 2‡ 0‡
Precentral gyrus 0 2 0 0 1 0 – – – – – –Temporal cortex 0 2 0 0 1 0 0 2 0 – – –Parietal cortex 0 2 0 0 1 0 0 2 0 – – –Occipital cortex 0 2 0 0 2 0 0 2 0 – – –Cingulate gyrus 0 2 0 0 1 0 – – – – – –Insular cortex 0 2 0 0 1 0 – – – – – –Dentate gyrus 0 1 0 0 1 0 0 1 0 – – –Hippocampus 0 2 0 0 1 0 0 2 0 – – –Subiculum 0 2 0 0 1 0 0 2 0 – – –Pre/parasubiculum 0 2 1 0 2 0 0 2 1 – – –
Basal gangliaPutamen 0 2 0 0 1 0 0 2 0 0 2 0Caudate nucleus 0 2 0 0 1 0 – – – – – –Globus pallidus 0 2 0 0 1 0 0 2 0 0 2 0Claustrum 0 2 0 0 1 0 – – – – – –Amygdaloid nucleus complex 0 2 0 – – – – – – – – –Basal nucleus 0 2 0 0 2 0 – – – – – –
ThalamusAnterior nucleus 3 3 1 2 3 1 – – – 2¶ 3¶ 1¶
Medial nucleus 3 3 1 2 3 1 2 3 1 2¶ 3¶ 1¶
Ventral lateral nucleus 1 2 1 1 1 1 1 2 1 – – –Pulvinar 2 3 1 – – – – – – – – –Lateral geniculate nucleus 0 1 0 – – – – – – – – –Subthalamic nucleus 0 1 0 0 1 0 0 0 0 – – –
HypothalamusParaventricular nucleus 0 1 0 – – – – – – – – –Supraoptic nucleus 0 1 0 – – – – – – – – –Lateral nucleus 1 2 0 – – – – – – – – –Anterior nucleus 1 1 0 – – – – – – – – –
Cerebellum*Neocerebellum 1 1 0 1 1 0 1 1 0 – – –Vermis 2 1 0 1 1 0 – – – 1# 1# 0#
Archicerebellum 1 1 0 1 1 0 – – – – – –Dentate nucleus 1 2 0 1 1 0 1 1 0 – – –
MidbrainNucleus ruber 1 3 0 1 2 0 – – – – – –Substantia nigra 1 2 0 1 1 0 1 1 0 – – –Central grey mesencephali 1 3 0 1 2 0 1 2 0 – – –Nucleus raphes dorsalis 2 3 0 – – – 1 2 0 – – –Formatio reticularis 2 2 0 1 2 0 1 2 0 – – –Oculomotor nucleus – – – – – – 0 1 0 – – –Trochlear nucleus 0 1 0 – – – – – – – – –Mesencenphatic nucleus of trigeminal nerve 0 2 0 – – – 0 1 0 – – –Superior colliculus – – – 1 2 0 1 2 0 – – –Inferior colliculus 1 2 0 – – – – – – – – –
PonsLocus coeruleus 1 2 0 1 1 0 1 1 0 – – –Superior central nucleus 1 2 0 2 2 0 2 2 0 – – –Formatio reticularis 2 2 0 – – – 2 2 0 – – –Vestibular nuclei 1 2 0 – – – – – – – – –Pontine nuclei 0 1 0 0 1 0 0 1 0 0 1 0
Medulla oblongataVestibular nuclei 0 2 0 0 1 0 – – – – – –Nucleus cuneatus 0 1 0 – – – 1 1 0 – – –
Continued on next page
Dow
nloaded from https://academ
ic.oup.com/brain/article/122/1/5/330287 by guest on 28 D
ecember 2021

8 G. Almeret al.
Table 1 Continued
Patient
IV-5 IV-8 III-5 IV-13
NL GL SP NL GL SP NL GL SP NL GL SP
Nucleus gracilis – – – – – – 1 1 0 0 1 0Hypoglossal nucleus 0 1 0 – – – 0 1 0 – – –Dorsal nucleus of vagus 0 1 0 – – – 1 2 0 – – –Spinal trigeminal nucleus 1 2 0 0 1 0 1 2 0 – – –Nucleus ambiguus 0 1 0 0 1 0 0 1 0 0 1 0Raphe nuclei 2 2 0 1 1 0 2 2 0 – –Formatio reticularis 2 2 0 1 2 0 2 2 0 2 3 0Inferior olivary nucleus 2 3 0 2 3 0 2 2 0 3 3 0Accessory olivary nuclei 2 3 0 2 3 0 3 3 0 – – –
Spinal cordPosterior horn 1 2 0 – – – – – – 1 2 0Lateral horn – – – – – – – – – 1 2 0Intermediate grey 1 2 0 – – – – – – 1 2 0Anterior horn 1 2 0 – – – – – – 1 2 0
0, 1, 2, 35 no, slight, moderate, prominent neuronal loss, gliosis, spongiform change, respectively; –5 not available. NL5 neuronalloss; GL5 astrogliosis; SP5 spongiform change. *Loss of Purkinje cells;†focal SP, colocalizes with PrPres deposition;‡two blocks ofcerebral cortex, region unknown;¶two fragments of thalamus, most likely of anterior and medial nucleus;#two blocks of cerebellarcortex, most likely vermis.
using an enhanced chemifluorescent substrate (Amersham,UK), and analysed on a Storm 840 phosphoimager (MolecularDynamics, Sunnyvale, Calif., USA).
ResultsClinical findingsThe family pedigree is depicted in Fig. 1. The pedigree datawere collected after FFI was genetically diagnosed in a youngman in 1996 with clinical signs of a neurodegenerativedisorder (patient IV-5, see below). Among more than 50members in five generations, probable (according to medicaland non-medical records) or definite (diagnosed by moleculargenetics and neuropathology) FFI was identified in 13 cases.
Patient IV-5At the age of 25 years, this male patient started sufferingfrom progressive tiredness and lethargy. Episodes of diplopiaand complex hallucinations followed (e.g. the patientperformed movements of sawing with a virtual saw andstopped bewildered when told that there was no saw). Despiteincreased appetite, he had continuous loss of weight (.20 kgwithin 6 months) and chronic therapy-resistant constipation.Progressive change of personality with apathy became evidentand endogenous depression was diagnosed. Several clinicalcheck-ups including MRI and EEG were all inconclusive.Four months after onset, dysarthria, hypophonia and reductionof spontaneous speech developed. Speech disorder wasfollowed by gait ataxia and myoclonus with perioral andperiorbital predominance.
The patient was hospitalized at the Clinic of Neurology,
University of Vienna, 6 months after onset of disease. Onadmission, he presented with markedly impaired vigilance,lack of spontaneous speech, dysarthria, severe gait ataxia,myoclonus and tremor. He had mild sleep disturbances. Hewas fully oriented, but had severe deficiencies in short-term memory, and psychomotor speed was reduced. Duringhospitalization, autonomic dysfunction manifested withhyperhidrosis, hyperthermia, tachycardia, recurrent flushes,dyspnoe and irregular breathing. Within several months,marked insomnia with nocturnal motor unrest and stereotypemovements developed.
MRI showed mild supratentorial atrophy and discretehyperintense white matter lesions. EEG displayed mild tomoderate signs of diffuse non-specific parenchymaldysfunction. In the late phase of disease, epileptiformdischarges were observed. Periodic or pseudoperiodic activitywas not recorded. Other clinical tests, such as electro-oculography, visual evoked potentials and analysis of theCSF revealed no pathology. ACTH and cortisol levels werewithin normal range. DNA analysis of blood leukocytesdetected the pathognomonic genotype of FFI (seePRNPanalysis below). The patient died from pneumonia 13 monthsafter onset of disease in a condition of severe cachexiaand stupor.
Patient IV-8An elder brother of patient IV-5 had onset of disease at theage of 36 years. He had severe loss of weight and chronicconstipation, and developed later mild gait ataxia anddysphagia. Autonomic dysfunction followed, notablyprominent hypersalivation and hyperthermia.
Dow
nloaded from https://academ
ic.oup.com/brain/article/122/1/5/330287 by guest on 28 D
ecember 2021

A new Austrian family with FFI 9
Table 2 Nerve fibre degeneration in the CNS of fourAustrian FFI patients
Patient
IV-5 IV-8 III-5 IV-13
CerebrumFrontal white matter 0 1 1 1*Central white matter 2 1 – –Temporal white matter 1 1 1 –Parietal white matter 0 1 1 –Occipital white matter 0 1 1 –Corpus callosum 0 0 – –Internal capsule 2 1 1 1Anterior commissure 0 – 0 –Fornix 2 1 – –Mamillothalamic tract – – 2 –Optic chiasm 0 0 – –Optic tract 0 0 – –
CerebellumNeocerebellar white matter 1 1 1 –White matter of vermis 2 2 – 1†
Archicerebellar white matter 1 1 – –Brainstem/spinal cord
Crus cerebri 1 1 1 –Superior cerebellar peduncle 2 1 1 –Middle cerebellar peduncle 1 – 1 1Inferior cerebellar peduncle 1 2 0 –Medial longitudinal fasciculus 2 2 1 1Central tegmental tract 2 2 2 2Medial lemniscus 0 0 1 1Lateral lemniscus 1 0 1 –Fasciculus gracilis 1 – 1 1Fasciculus cuneatus 1 – 1 1Pyramidal tract 0 1 1 1Posterior spinal nerve root 1 – – –
0, 1, 2 no, single, multiple nerve fibre degenerations, respectively,as indicated by myelin balls in luxol fast blue/nuclear fast redstain; –5 not available. *Two blocks of cerebral cortex, regionunknown;†two blocks of cerebellar cortex, most likely vermis.
On admission to the Clinic of Neurology, University ofVienna, the patient reported a 2-week episode of severe sleepdisturbance, which had improved 6 months previously undertreatment with benzodiazepines. During hospitalization, thepatient had mild difficulty in falling asleep. Neurologicalexamination revealed myoclonus of face, tongue and upperlimbs, and mild ataxia of limbs and gait. Mild spasticparaparesis was considered a residue of a car accident in1983 which had resulted in a fracture of the lumbar spineand affection of spinal cord. There was mild cognitiveimpairment, and apathy and lethargy.
CSF analysis revealed no abnormalities. CT disclosed milddiffuse brain atrophy. EEG displayed signs of diffuse non-specific parenchymal dysfunction. Three months afterdischarge from the clinic the patient died from pneumonia,11 months after onset of disease. No progression of sleepdisorder was reported by his family doctor.
Patient III-5This patient was the mother of patients IV-5 and IV-8.Disease manifested with initial insomnia and nocturnal motorunrest, memory impairment, and perioral and periorbitalmyoclonus. Severe loss of weight, progressive apathy,dysarthria and episodic irregular breathing and inspiratorystridor followed. EEG showed moderate to prominent signsof diffuse non-specific parenchymal dysfunction. CT revealedmoderate brain atrophy with frontocerebellar accentuation.The patient died at the age of 58 years from broncho-pneumonia 8 months after onset of disease.
Patient IV-13Disease manifested in this second cousin of patients IV-5and IV-8 at the age of 20 years with severe loss of weight.She then developed vertigo and ataxia. Diplopia, dysarthria,tremor, autonomic dysfunction (hyperthermia and chronicconstipation), progressive apathy and amnestic deficienciesfollowed. Sleep disturbances or insomnia have not beenrecorded. EEG showed mild diffuse non-specific parenchymaldysfunction. CT was normal. She died severely cachecticfrom pneumonia 20 months after onset of disease.
Patient III-13The mother of patient IV-13 had onset of disease at the ageof 62 years. Initial symptoms comprised loss of weight,tiredness and short-term memory impairment. Within severalmonths, nocturnal insomnia, dysarthria and episodes ofdiplopia developed. Her family then noticed progressiveapathy and confusions, notably at night. In the late phase ofdisease, she developed progressive gait ataxia and perioralmyoclonus. Dysautonomia has not been recorded.Haematological and biochemical findings were normal. EEGshowed moderate signs of diffuse non-specific parenchymaldysfunction. CT disclosed pronounced cerebral and cerebellaratrophy. The patient died 18 months after onset of disease.
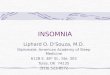
NeuropathologyThe fresh brain of patient IV-5 weighed 1360 g. Brain weightsof other autopsied patients are not on record. Grossly, thebrains of patients IV-5 and IV-8 showed diffuse oedemawith narrowing of external and internal CSF spaces. Brainsectioning revealed thalamic atrophy with a marbled aspectof the cut surface (Fig. 2).
Tables 1 and 2 summarize grey and white matter lesioningin patients III-5, IV-5, IV-8 and IV-13. Regionalhistopathology was similar in all patients. Cerebral cortexshowed no unequivocal neuronal loss. Neuronal loss wasmoderate to conspicuous in thalamus (most prominent inmedial and anterior thalamic nuclei) and inferior olivarynuclei, and slight to moderate in dorsal raphes and superiorcentral nuclei, in hypothalamus, some brainstem nuclei and
Dow
nloaded from https://academ
ic.oup.com/brain/article/122/1/5/330287 by guest on 28 D
ecember 2021

10 G. Almeret al.
Fig. 1 The pedigree of the Austrian FFI family comprises more than 50 members in five generations.
spinal grey matter. Cerebellar cortex displayed slight tomoderate reduction of Purkinje cells and the granular layercontained some torpedoes. Astrogliosis involved all greymatter structures and was particularly conspicuous in thalamicnuclei (in anterior and medial nuclei more than in ventrallateral nuclei) (Fig. 3D), nucleus ruber, periaqueductal, tectaland tegmental grey, and raphe and olivary nuclei (Fig. 4Aand B). Cerebral cortex showed bilaminar accentuation ofastrogliosis (Fig. 3B). Spongiform change was discrete anddetectable in thalamic nuclei (Fig. 3C) of all four brains, inpre/parasubiculum of two brains and in a small focus offrontal cortex of one brain (Fig. 3A). Deposits of proteaseresistant PrP (PrPres) detected by immunocytochemistry werediscrete and occurred only in brains III-5, IV-5 and IV-8.In brain III-5, patchy and strip-like PrPres deposits withperpendicular orientation to the surface were localized in themolecular layer in one out of three blocks of cerebellar cortex(Fig. 5A and B); pre/parasubiculum harboured discrete, fine-granular synaptic type deposits. In brain IV-5, a singlevacuolated neuron in the inferior olivary nuclei (see below)contained prominent intravacuolar granular PrPres deposits(Fig. 5C). A few other neurons displayed discrete granularPrPres deposits on the surface and/or in the vacuoles, but the
majority was negative. In brain IV-8, a small area of frontalcerebral cortex showed spongiform change and synaptictype PrPres deposits with perivacuolar accentuation weredetectable. A few patchy PrPres deposits were confined to asmall focus in the molecular layer of cerebellar cortex. Afew vacuolated neurons in the inferior olivary nuclei haddiscrete granular PrPres deposits on the surface and/or in thecytoplasmic vacuoles. Internal organs of patient III-13 weredevoid of detectable PrPres deposits.
White matter of cerebrum and cerebellum showed scatteredmyelin balls indicating widespread Wallerian type of nervefibre degeneration (Table 2). The nerve fibre degenerations arepossibly the pathological substrate, as lesions accompanied byoedema, of discrete supratentorial MRI findings in patientIV-5 (see Clinical findings). Primary demyelination withpreserved axons was not detectable. Flourishing nerve fibrebreakdown was most conspicuous in brainstem tracts (Table 2,Fig. 4E). Alveus and hilus of inferior olives, and hilus ofdentate nuclei showed prominent depletion of nerve fibres.Residual olivary neurons showed signs of transneuronaldegeneration (Fig. 4C and D) with vacuolation of cell bodiesand hypertrophied antler-like dendrites (olivary‘pseudohypertrophy’) in all brains.
Dow
nloaded from https://academ
ic.oup.com/brain/article/122/1/5/330287 by guest on 28 D
ecember 2021
A new Austrian family with FFI 11
Fig. 2 A coronal slice of brain IV-5 shows diffuse oedema with narrowing of external and internal CSFspaces. The thalami are atrophic and display a marbled aspect.
Western blottingAt a final proteinase K concentration of 50µg/ml, PrPres wasnot detectable in any of the seven investigated regions.Reduction of proteinase K concentration to 12.5µg/mlresulted in a positive signal from the basal ganglia, precentralregion and thalamus (Fig. 6). Glycoform ratios are similarto those previously reported for FFI, with the diglycosylatedPrPres band being the most abundant (Gambettiet al., 1995;Parchiet al., 1995). In the basal ganglia the average ratiosfor the three PrPres glycoforms are: high: 58.43%, low:33.40%, unglycosylated: 8.17%, taken from an average offour separate blots.
PRNP analysisPCR amplification of the complete coding region ofPRNPgenerated a single product of 874 bp, thus excluding aninsertion mutation or deletion. SSCP analysis revealed anaberrant migration pattern indicating a point mutation in theC-terminal half of the gene. Close inspection of this regionby digestion of the PCR product with enzymeTth111I anddirect sequencing defined this mutation as aspartic acid(GAC) to asparagine (AAC) substitution at codon 178 ofPRNP (D178N). SSCP analysis,NspI digestion and directsequencing revealed homozygous codon 129 for methioninein all four patients.
DiscussionOnset of disease was insidious in our FFI family, with initialor early loss of weight in all five patients with detailedhistories. The first neuropsychiatric symptoms were insomniain one patient, lethargy in one patient, cognitive impairmentin one patient and ataxia in two patients. In the course ofdisease, four patients developed progressive insomnia, fourpatients autonomic dysfunction and all five patients motorabnormalities. Symptomatology of our patients is thus typicalfor FFI (Lugaresiet al., 1986; Manettoet al., 1992; Nagayamaet al., 1996). According to medical records, patient IV-13presented clinically with some unusual features. Age at onsetof disease was 20 years. Together with a recent FFI patientfrom Australia (Silburnet al., 1996), this patient is theyoungest reported so far. Insomnia was not recorded duringthe whole course of disease. However, evaluation of sleeppatterns by polysomnography was not performed.
Molecular analysis ofPRNP in our family revealed thecodon 178 point mutation and methionine homozygosity atposition 129 in all four patients examined. Codon 178mutation in conjunction with methionine at position 129 ofthe mutant allele is the diagnostic genotype for FFI (Goldfarbet al., 1992; Medoriet al., 1992b). It has been shown thatthe genotype of polymorphic codon 129 associates in FFIwith characteristic neuropathological features (Gambettiet al., 1995; Parchiet al., 1995). Patients with homozygouscodon 129 have prominent thalamic pathology, whereas
Dow
nloaded from https://academ
ic.oup.com/brain/article/122/1/5/330287 by guest on 28 D
ecember 2021

12 G. Almeret al.
Fig. 3 Cerebral histopathology in the Austrian FFI family. Spongiform change (A) is detectable in a focus of frontal cortex (brain IV-8;HE; 3110), and (C) is discrete in thalamic nuclei (brain IV-5; HE,3140). Anti-GFAP immunocytochemistry shows (B) corticalastrogliosis with bilaminar accentuation (brain IV-5;325) and (D) prominent astrogliosis in the thalamus (brain IV-5;3170).
lesioning of cerebral cortex is minor or absent (Gambettiet al., 1995; Parchiet al., 1995; Rederet al., 1995; Nagayamaet al., 1996; Silburnet al., 1996). However, two recentpatients of two different kindreds with homozygous codon129 showed prominent lesioning of cerebral cortex (McLeanet al., 1997; Rossiet al., 1998). Patients with heterozygouscodon 129 have prominent lesioning of the cerebral cortexin addition to thalamic pathology (Gambettiet al., 1995;Parchi et al., 1995). Our patients were all homozygous atposition 129; neuropathology showed prominent thalamiclesioning, whereas cerebral cortex displayed only minorhistopathology with spongiform change confined to smallareas. However, anti-GFAP immunocytochemistry detectedwidespread laminar astrogliosis. Astrogliosis also involvedregions that are not supposed to receive thalamocorticalprojections, i.e. the occipital cortex. Widespread corticalastrogliosis in the absence of neuronal loss and spongiformchange has been observed in members of other FFI kindreds(Manetto et al., 1992; Medori et al., 1992a). Corticalastrogliosis indicates submicroscopical lesioning of brainparenchyma. Possible targets of lesioning are neuronalsubpopulations of the cortex. In Creutzfeldt–Jakob diseasebrains, subtotal loss of the parvalbumin positive subset of
GABAergic neurons has been observed despite ‘normal’appearance of tissue (Guentchevet al., 1997).
Brainstem histopathology in FFI has been described asvariable in distribution and limited in extent. Neuronal lossand gliosis are most conspicuous and frequent in inferiorolives and minor in other nuclei (Manettoet al., 1992;Gambettiet al., 1995; Rederet al., 1995; Nagayamaet al.,1996; Silburnet al., 1996; McLeanet al., 1997; Rossiet al.,1998). In nine patients from five different FFI families, theperiaqueductal grey matter showed slight to moderate gliosis(Parchiet al., 1995). In one out of four patients of anotherkindred, brainstem lesioning involved locus coeruleus, raphenucleus and reticular formation (McLeanet al., 1997). OneFFI patient had prominent neuronal loss in the tectum (Rederet al., 1995). In contrast, all our neuropathologically analysedpatients consistently had widespread and conspicuousbrainstem histopathology, although disease duration was shortto moderate (8, 11, 13 and 20 months, respectively).
In bovine spongiform encephalopathy (BSE) and scrapie ofsheep, vacuolation of brainstem neurons is pathognomonic(Wells and Wilesmith, 1995; DeArmond and Prusiner, 1997).In human prion disease, conspicuous neuronal vacuolation hasbeen observed only in kuru (Hadlow, 1959; Klatzoet al.,
Dow
nloaded from https://academ
ic.oup.com/brain/article/122/1/5/330287 by guest on 28 D
ecember 2021

A new Austrian family with FFI 13
Fig. 4 Brainstem pathology in the Austrian FFI family (brain IV-5). (A) In the pons, gliosis (dark blue colour) is conspicuous inperiaqueductal grey and raphe (Kanzler stain;33). (B) In medulla oblongata, gliosis is prominent in inferior olivary nuclei (Kanzlerstain;34). Residual olivary neurons show signs of transneuronal degeneration with (C) neuronal vacuolation (HE;3400) and(D) hypertrophied antler-like dendrites (Bielschowsky;3260). (E) flourishing nerve fibre breakdown with myelin balls in olivocerebellartract (luxol fast blue/nuclear fast red;3430).
1959; Hainfellneret al., 1997b). The olives of our FFI patientsshowed severe neuronal loss, and residual neurons werehypertrophied and vacuolated. Neuronal vacuolation in ourpatients is reminiscent of that in BSE and scrapie. However, weinterpret neuronal vacuolation in our patients as transneuronaldegeneration because vacuolation was confined to the olives,central tegmental tracts showed conspicuous degeneration andhypertrophied antler-like dendrites were found as well. Olivary‘pseudohypertrophy’ with neuronal vacuolation is a wellknown pattern of transneuronal degeneration which has beendescribed as a sequel of central tegmental tract lesioning, mostcommonly due to ischaemic infarction within the brainstem(Gautier and Blackwood, 1961).
In our hands, immunocytochemistry on numerous blocks
detected PrPres deposits in only three out of four patients. Inpatient III-3, conspicuous PrPres deposits accumulated in oneout of three blocks in the molecular layer of cerebellarcortex, and minor PrPres deposits were detectable in pre/parasubiculum. Patients IV-5 and IV-8 had discrete PrPres
deposits in the inferior olivary nuclei. Patient IV-8 had, inaddition, a small focus of PrPres deposition in frontal cortexand scant deposits in the molecular layer of cerebellar cortex.Thus, the diagnostic value of anti-PrP immunocytochemistryis limited in FFI, and immunocytochemical PrPres detectionrequires examination of numerous tissue blocks includingareas with minor histopathology. In contrast to immuno-cytochemistry, Western blot analysis of brain IV-5 detectedPrPres in three out of seven CNS regions after mild protease
Dow
nloaded from https://academ
ic.oup.com/brain/article/122/1/5/330287 by guest on 28 D
ecember 2021

14 G. Almeret al.
Fig. 5 PrPres deposition patterns in the Austrian FFI family. In patient III-5 (A andB), patchy and strip-like PrPres deposits are confinedto the molecular layer and show perpendicular orientation to the surface (anti-PrP) (A,350; B, 3145). (C) A single vacuolated neuronin the inferior olivary nuclei of patient IV-5 shows prominent intravacuolar accumulation of granular PrPres deposits. Other neurons aredevoid of PrPres deposits (anti-PrP) (3160; inset:3730).
K digestion. This confirms that Western blotting is superiorto immunocytochemistry in detecting PrPres in FFI.
Descriptions of the immunomorphology of PrPres in FFIare scant. In two out of four patients of an Australian kindred,a weak fine granular staining of the neutropil has beenobserved (McLeanet al., 1997). In one of our patients, focalPrPres deposits in the frontal cortex showed a synaptic typepattern with perivacuolar accentuation. In two out of four ofour patients, a few vacuolated neurons in the inferior olivarynuclei had discrete fine granular PrPresdeposits on the surfaceand/or in the cytoplasmic vacuoles; a single neuron hadprominent intravacuolar deposits (Fig. 5C). This is a uniqueobservation in FFI, resembling changes of brainstem neuronsin BSE (Wells and Wilesmith, 1995). In another of ourpatients, PrPres deposits in the molecular layer of cerebellarcortex showed a peculiar strip-like pattern with perpendicularorientation to the surface. A comparable pattern of PrPres
deposition has not been described in FFI so far and hasnot been observed in sporadic Creutzfeldt–Jakob disease(Hainfellner and Budka, 1996), kuru (Hainfellneret al.,1997b) or Gerstmann–Stra¨ussler–Scheinker syndrome(Hainfellner et al., 1995), but has been observed in some
cases of familial Creutzfeldt–Jakob disease (J.A.H. and H.B.,unpublished observation).
Western blot analysis of the regional distribution of PrPres
in FFI has shown that histopathology is confined to brain areaswith PrPresaccumulation. Conversely, PrPreswas detectable inareas with and without histopathology. On the basis of thisobservation, it has been hypothesized that tissue lesioning inFFI develops only in the presence of critical amounts ofPrPres and that vulnerability of brain parenchyma to thepresence of PrPres is regionally variable (Parchiet al., 1995).However, immunocytochemistry detected little PrPres, in spiteof severe and widespread histopathology. Moreover, in ourpatient IV-5, Western blotting did not detect PrPres in theseverely damaged brainstem. Thus, PrPres accumulation inour FFI patients dissociates not only quantitatively but alsotopographically from histopathology. With regard to theunresolved pathogenic role of PrP in prion diseases, thisdissociation supports a loss of function model (Whittingtonet al., 1995) rather than neurotoxicity (Brown andKretzschmar, 1997). Experimental data suggest that loss offunctional PrP impairs the maintenance and normal functionof synapses. Thus, synapses are a likely target of lesioning,
Dow
nloaded from https://academ
ic.oup.com/brain/article/122/1/5/330287 by guest on 28 D
ecember 2021

A new Austrian family with FFI 15
Fig. 6 Western blot analysis of a normal brain and of FFI brainIV-5. Positive signals are present in FFI in basal ganglia,precentral and thalamus regions. The diglycosylated PrPres band isthe most abundant. All samples were treated with proteinase K(PK) at a concentration of 12.5µg/ml before electrophoresis.Molecular weight standards are shown on the left.
following loss of functional PrP in prion disease (Whittingtonet al., 1995).
AcknowledgementsWe wish to thank Dr G. R. Trabattoni for helping withneuropathological analysis and Mrs H. Flicker for excellenttechnical assistance. This work is part of the EuropeanUnion Biomed-2 Concerted Action ‘Human transmissiblespongiform encephalopathies (prion diseases): neuro-pathology and phenotypic variation’ (project leader:H. Budka).
ReferencesAlmer G, Hainfellner JA, Budka H, Bru¨cke T. Clinical, pathologicaland molecular features of the first Austrian family with fatal familialinsomnia [abstract]. Eur J Neurol 1997; 4 Suppl 1: S1.
Brown DR, Kretzschmar HA. Microglia and prion disease: a review.Histol Histopathol 1997; 12: 883–92.
Budka H, Hainfellner JA, Almer G, Bru¨cke T, Windl O, KretzschmarHA, et al. A new Austrian family with fatal familial insomnia:brain pathology without detectable PrPres [abstract]. Brain Pathol1997; 7: 1267.
Collinge J, Sidle KC, Meads J, Ironside J, Hill AF. Molecularanalysis of prion strain variation and the aetiology of ‘new variant’CJD. Nature 1996; 383: 685–90.
DeArmond SJ, Prusiner SB. Prion diseases. In: Graham, DI, LantosPL, editors. Greenfield’s neuropathology, Vol. 2. 6th ed. London:Arnold; 1997. p. 235–80.
Gambetti P, Parchi P, Petersen RB, Chen SG, Lugaresi E. Fatalfamilial insomnia and familial Creutzfeldt-Jakob disease: clinical,pathological and molecular features. Brain Pathol 1995; 5: 43–51.
Gautier JC, Blackwood W. Enlargement of the inferior olivarynucleus in association with lesions of the central tegmental tract ordentate nucleus. Brain 1961; 84, 341–61.
Goldfarb LG, Petersen RB, Tabaton M, Brown P, LeBlanc AC,Montagna P, et al. Fatal familial insomnia and familial Creutzfeldt-Jakob disease: disease phenotype determined by a DNApolymorphism. Science 1992; 258: 806–8.
Goodbrand IA, Ironside JW, Nicolson D, Bell JE. Prion proteinaccumulation in the spinal cords of patients with sporadic andgrowth hormone associated Creutzfeldt-Jakob disease. Neurosci Lett1995; 183: 127–30.
Guentchev M, Hainfellner JA, Trabattoni GR, Budka H. Distributionof parvalbumin-immunoreactive neurons in brain correlates withhippocampal and temporal cortical pathology in Creutzfeldt-Jakobdisease. J Neuropathol Exp Neurol 1997; 56: 1119–24.
Hadlow WJ. Scrapie and kuru. Lancet 1959; 2: 289–90.
Hainfellner JA, Budka H. Immunomorphology of human priondiseases. In: Court L, Dodet B, editors. Transmissible subacutespongiform encephalopathies: prion diseases. Amsterdam: Elsevier;1996. p. 75–80.
Hainfellner JA, Brantner-Inthaler S, Cervenakova L, Brown P,Kitamoto T, Tateishi J, et al. The original Gerstmann-Stra¨ussler-Scheinker family of Austria: divergent clinicopathologicalphenotypes but constant PrP genotype. Brain Pathol 1995; 5: 201–11.
Hainfellner JA, Almer G, Bru¨cke T, Jellinger K, Kleinert R,Bayer G, et al. Fatal familial insomnia in a new Austrian family:dissociation of brain pathology from PrP deposition [abstract]. ClinNeuropathol 1997a; 16: 261.
Hainfellner JA, Liberski PP, Guiroy DC, Cervena`kova L, Brown P,Gajdusek DC, et al. Pathology and immunocytochemistry of a kurubrain. Brain Pathol 1997b; 7: 547–53.
Klatzo I, Gajdusek DC, Zigas V. Pathology of kuru. Lab Invest1959; 8: 799–847.
Kretzschmar HA, Stowring LE, Westaway D, Stubblebine WH,Prusiner SB, DeArmond SJ. Molecular cloning of a human prionprotein cDNA. DNA 1986; 5: 315–24.
Lugaresi E, Medori R, Montagna P, Baruzzi A, Cortelli P, LugaresiA, et al. Fatal familial insomnia and dysautonomia with selectivedegeneration of thalamic nuclei. N Engl J Med 1986; 315: 997–1003.
Manetto V, Medori R, Cortelli P, Montagna P, Tinuper P, BaruzziA, et al. Fatal familial insomnia: clinical and pathologic study offive new cases. Neurology 1992; 42: 312–9.
McLean CA, Storey E, Gardner RJ, Tannenberg AE, CervenakovaL, Brown P. The D178N (cis-129M) ‘fatal familial insomnia’mutation associated with diverse clinicopathologic phenotypes inan Australian kindred. Neurology 1997; 49: 552–8.
Medori R, Montagna P, Tritschler HJ, LeBlanc A, Cortelli P, Tinuper
Dow
nloaded from https://academ
ic.oup.com/brain/article/122/1/5/330287 by guest on 28 D
ecember 2021

16 G. Almeret al.
P, et al. Fatal familial insomnia: a second kindred with mutation ofprion protein gene at codon 178. Neurology 1992a; 42: 669–70.
Medori R, Tritschler HJ, LeBlanc A, Villare F, Manetto V, ChenHY, et al. Fatal familial insomnia, a prion disease with a mutationat codon 178 of the prion protein gene. N Engl J Med 1992b; 326:444–9.
Nagayama M, Shinohara Y, Furukawa H, Kitamoto T. Fatal familialinsomnia with a mutation at codon 178 of the prion protein gene:first report from Japan. Neurology 1996; 47: 1313–6.
Nicholl D, Windl O, de Silva R, Sawcer S, Dempster M, IronsideJW, et al. Inherited Creutzfeldt-Jakob disease in a British familyassociated with a novel 144 base pair insertion of the prion proteingene. J Neurol Neurosurg Psychiatry 1995; 58: 65–9.
Orita M, Iwahana H, Kanazawa H, Hayashi K, Sekiya T. Detectionof polymorphisms of human DNA by gel electrophoresis as single-strand conformation polymorphisms. Proc Natl Acad Sci USA 1989;86: 2766–70.
Parchi P, Castellani R, Cortelli P, Montagna P, Chen SG, PetersenRB, et al. Regional distribution of protease-resistant prion proteinin fatal familial insomnia. Ann Neurol 1995; 38: 21–9.
Reder AT, Mednick AS, Brown P, Spire JP, Van Cauter E, WollmannRL, et al. Clinical and genetic studies of fatal familial insomnia.Neurology 1995; 45: 1068–75.
Rossi G, Macchi G, Porro M, Giaccone G, Bugiani M, ScarpiniE, et al. Fatal familial insomnia: genetic, neuropathologic, andbiochemical study of a patient from a new Italian kindred. Neurology1998; 50: 688–92.
Sambrook J. Molecular cloning: a laboratory manual. 2nd ed. NewYork: Cold Spring Harbor Laboratory Press; 1989.
Silburn P, Cervenakova L, Varghese P, Tannenberg A, Brown P,Boyle R. Fatal familial insomnia: a seventh family. Neurology 1996;47: 1326–8.
Wells GA, Wilesmith JW. The neuropathology and epidemiologyof bovine spongiform encephalopathy. Brain Pathol 1995; 5: 91–103.
Whittington MA, Sidle KC, Gowland I, Meads J, Hill AF, PalmerMS, et al. Rescue of neurophysiological phenotype seen in PrP nullmice by transgene encoding human prion protein. Nat Genet 1995;9: 197–201.
Windl O, Dempster M, Estibeiro JP, Lathe R, de Silva R, EsmondeT, et al. Genetic basis of Creutzfeldt-Jakob disease in the UnitedKingdom: a systematic analysis of predisposing mutations andallelic variation in the PRNP gene. Hum Genet 1996; 98: 259–64.
Received May 21, 1998. Revised September 3, 1998.Accepted September 7, 1998
Dow
nloaded from https://academ
ic.oup.com/brain/article/122/1/5/330287 by guest on 28 D
ecember 2021