Embed Size (px)
Citation preview
CASE REPORT
Fatal Strongyloides hyper-infection in a patient with myastheniagravis
M. Saraei • B. Hosseinbigi •
M. Shahnazi • B. Bijani
Received: 29 January 2014 / Accepted: 19 May 2014
� Springer-Verlag Berlin Heidelberg 2014
Abstract
Purpose We report a fatal case of Strongyloides hyper-
infection as the result of corticosteroid therapy of a patient
with myasthenia gravis.
Case presentation Our patient was a farmer with a past
history of living in an endemic area for Strongyloides sterco-
ralis in Iran. Hyper-infection was diagnosed during the
advanced-stage disease by demonstration of enormous number
of larvae in the direct smears prepared from both the stool and
tracheal secretions. Unfortunately, despite appropriate anti-
parasite therapy, the patient died due to respiratory failure.
Conclusion We recommend the provision of more
awareness in high-risk people prior to immunosuppressive
therapy, through screening for S. stercoralis, even in non-
endemic regions.
Keywords Strongyloides stercoralis � Hyper-infection �Myasthenia gravis � Albendazole
Introduction
Strongyloides stercoralis (S. stercoralis) is the smallest
human intestinal nematode and a unique soil-transmitted
nematode with capability of internal autoinfection and free-
living life cycle. Human infection is acquired through the
cutaneous entry of filariform larvae, which later develop
into adult worms in the small intestine followed by a
migratory phase through the lungs. S. stercoralis has a
short life cycle; however, the ability to produce internal
autoinfection leads to the development of sustained infec-
tion in humans—a phenomenon considered to be the cause
of persistent infection in American veterans after years of
leaving the endemic areas in Vietnam [1]. It is reported that
in a chronic uncomplicated strongyloidiasis, the host and
the parasite live in harmony, autoinfection is well regulated
by the host’s cell-mediated immunity, and the number of
adult worms is low and stable. This balanced condition
may be disrupted in immunocompromised patients, leading
to hyper-infection and eventually production of large
numbers of filariform larvae. These larvae penetrate the
intestinal wall and disseminate in various organs through
circulation. Also, the human intestinal bacteria could be
transported to bloodstream during the larval migratory
phase, causing bacterial sepsis, meningitis, endocarditis,
and pneumonia [2, 3].
Strongyloides stercoralis infections have a wide clinical
spectrum, ranging from asymptomatic eosinophilia in
immunocompetent individuals to fatal disseminated stron-
gyloidiasis in immunocompromised patients. Corticoste-
roid therapy is considered to be a major risk factor for
hyper-infection by the parasite as fatal strongyloidiasis
hyper-infection is reported in patients with ulcerative
colitis [4], multiple myeloma [5], dermatomyositis [6],
renal transplant patients [7], liver transplantation [8],
acquired immunodeficiency syndrome [9], hematopoietic
stem cell transplantation [10], and lymphocytic leukemia
[11]. We present here a case of fatal strongyloidiasis hyper-
infection in a resident of a non-endemic region, who was
M. Saraei � B. Hosseinbigi � M. Shahnazi
Department of Parasitology and Mycology, Faculty of Medicine,
Qazvin University of Medical Sciences, Qazvin, Iran
B. Bijani
Department of Infectious Diseases, Faculty of Medicine,
Qazvin University of Medical Sciences, Qazvin, Iran
B. Bijani (&)
Buali Hospital, Buali St, 34137-86165 Qazvin, Iran
e-mail: [email protected]
123
Infection
DOI 10.1007/s15010-014-0637-x
given corticosteroid therapy for treating his autoimmune
disease.
Case presentation
A 57-year-old man who was a known case of myasthenia
gravis and on chronic immunosuppressive therapy (aza-
thioprine and high dose prednisolone) was presented with
abdominal pain, dyspnea, and productive cough of 2 weeks
duration. He was a resident of Qazvin province with a
history of living and working as a farmer in Guilan prov-
ince. Qazvin province is not considered as an endemic
region for S. stercoralis, but Guilan province, with a
Mediterranean climate, is historically an endemic area of
this parasite. On admission to the emergency room, the
patient was febrile, hypotensive, and tachycardic. Pulse
oximetry showed 88 % saturation in room air. Pulmonary
examination was notable for bibasilar rales. His abdomen
was soft and non-tender with no sign of hepatospleno-
megaly. Chest X-ray revealed bilateral pulmonary infil-
trates, especially in the lower portions of the right lung.
Empiric treatment for sepsis due to suspected respiratory or
gastrointestinal source combined with immunosuppressive
therapy was initiated. Neurological examination was
unremarkable. Computed tomographic scan of the brain
was normal. Despite therapeutic measures, dyspnea wors-
ened. The patient was intubated and admitted to the
intensive care unit (ICU). Considering the patient diag-
nosed as having progression of myasthenia gravis with
increased respiratory failure, mycophenolate was added to
immunosuppressive immunotherapy. Complete blood
count revealed anemia (hemoglobin = 8 mg/dl, with
normal peripheral blood leukocyte count without eosino-
philia). While in the ICU, the patient, in addition to other
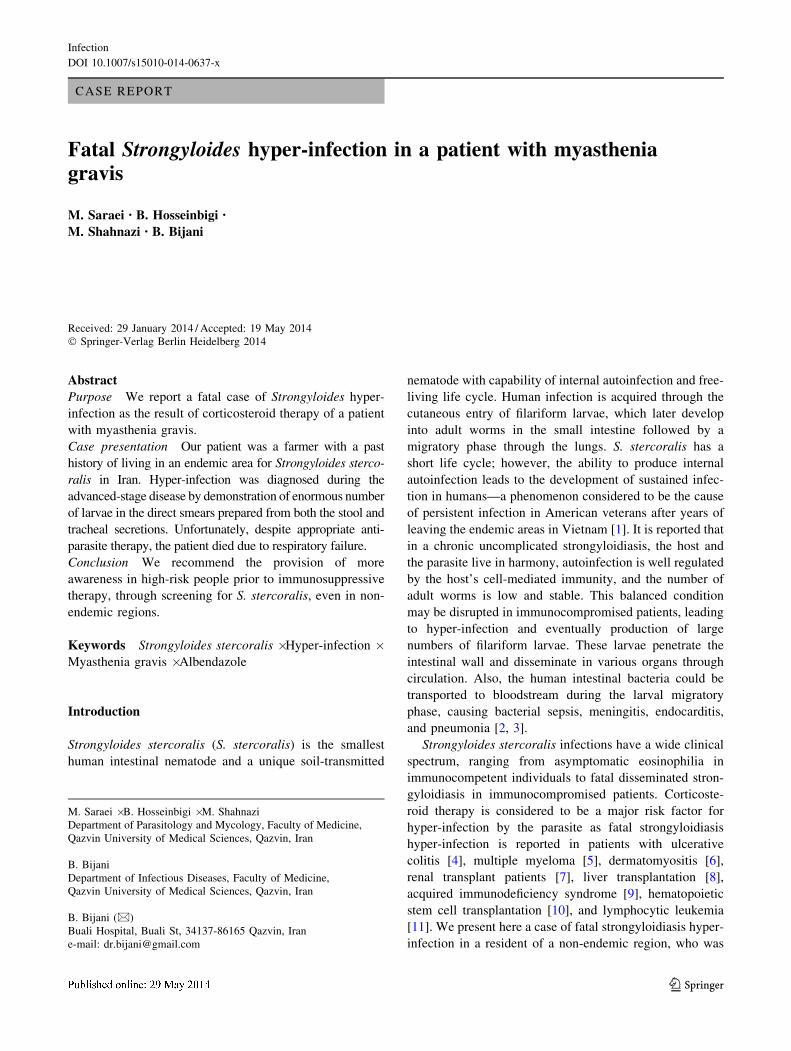
clinical complaints, developed diarrhea. Stool examination
revealed abundant amounts of rhabditiform and filariform
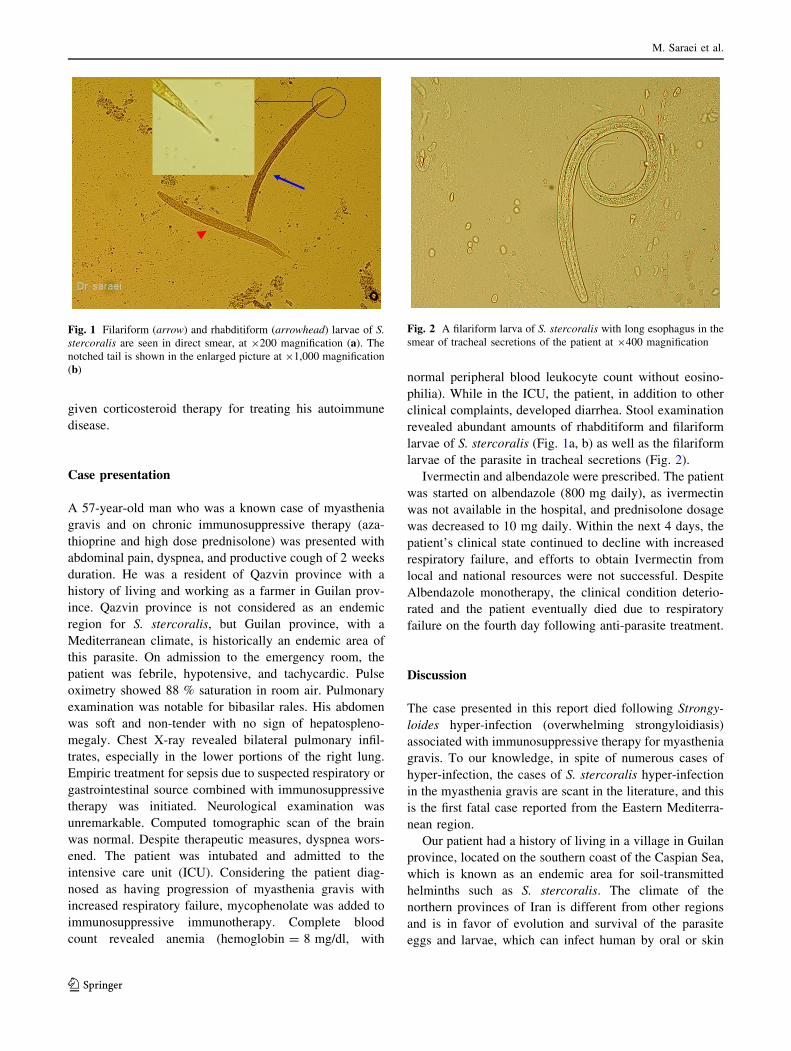
larvae of S. stercoralis (Fig. 1a, b) as well as the filariform
larvae of the parasite in tracheal secretions (Fig. 2).
Ivermectin and albendazole were prescribed. The patient
was started on albendazole (800 mg daily), as ivermectin
was not available in the hospital, and prednisolone dosage
was decreased to 10 mg daily. Within the next 4 days, the
patient’s clinical state continued to decline with increased
respiratory failure, and efforts to obtain Ivermectin from
local and national resources were not successful. Despite
Albendazole monotherapy, the clinical condition deterio-
rated and the patient eventually died due to respiratory
failure on the fourth day following anti-parasite treatment.
Discussion
The case presented in this report died following Strongy-
loides hyper-infection (overwhelming strongyloidiasis)
associated with immunosuppressive therapy for myasthenia
gravis. To our knowledge, in spite of numerous cases of
hyper-infection, the cases of S. stercoralis hyper-infection
in the myasthenia gravis are scant in the literature, and this
is the first fatal case reported from the Eastern Mediterra-
nean region.
Our patient had a history of living in a village in Guilan
province, located on the southern coast of the Caspian Sea,
which is known as an endemic area for soil-transmitted
helminths such as S. stercoralis. The climate of the
northern provinces of Iran is different from other regions
and is in favor of evolution and survival of the parasite
eggs and larvae, which can infect human by oral or skin
Fig. 1 Filariform (arrow) and rhabditiform (arrowhead) larvae of S.
stercoralis are seen in direct smear, at 9200 magnification (a). The
notched tail is shown in the enlarged picture at 91,000 magnification
(b)
Fig. 2 A filariform larva of S. stercoralis with long esophagus in the
smear of tracheal secretions of the patient at 9400 magnification
M. Saraei et al.
123

penetration. On the other hand, the consumption of raw
vegetables and direct contact with the moist soil in rice
fields are the main risk factors in the province. Half a
century ago, more than 50 % of people in the area were
positive for at least one of the intestinal nematodes, but it
has decreased to \1 % in recent decades. Promotion of
health services, easy access to effective and broad-spec-
trum anti-nematode drugs, increase in the level of literacy
and knowledge about the prevention of parasitic infections,
and improvement in human waste disposal systems are the
major measures which have led to a substantial decrease in
the prevalence of parasites within the areas, so that these
parasitic infestations are not considered as major health
problems any longer [12].
Immigration of Guilanian villagers to non-endemic areas
for S. stercoralis in Iran can be regarded as a risk factor for
parasitic hyper-infection. Our patient was a Guilanian vil-
lager working in rice fields, who immigrated to Qazvin
province around 30 years ago. Qazvin province, a non-
endemic area for S. Stercoralis, is the southern neighbor of
Guilan province and highly attractive for Guilanian rural
migrants because of the availability of jobs within the large
number of commercial and manufacturing companies
located in several industrial cities throughout the province.
In non-endemic areas of Iran, strongyloidiasis may be
misdiagnosed due to three major reasons: (1) educational
negligence: physicians educated in non-endemic areas may
not find the opportunity to visit such patients during their
medical educations. Therefore, infection with this parasite
may be neglected by clinicians. (2) laboratory negligence:
stool examination is usually requested for the detection of
intestinal parasites, which is routinely performed through
wet direct smear or rarely by concentration method, both
with lower sensitivity compared to agar plate test for the
detection of chronic infections with S. stercoralis, and (3)
lack of guideline for the screening of S. stercoralis in
patients under therapy with immunosuppressive agents.
Infection with S. stercoralis may be identified during the
advanced stage of hyper-infection when it is too late for
anti-parasite treatment, and therefore with high mortality as
observed in our case reported here.
Although S. Stercoralis is reported to be the major
parasitic agent for the appearance of eosinophilia in clinical
cases in Guilan province [13], nevertheless, no eosinophilia
was found in our patient who showed a large number of S.
stercoralis larvae in both stool and sputum examinations.
The low rate of eosinophilia in hyper-infection or dis-
seminated strongyloidiasis is attributed to the suppressive
effect of corticosteroids [14]. It is proposed that cortico-
steroids induce the hyper-infection of S. stercoralis by
three mechanisms: (a) increased production of ecdysteroid-
like substances, which are effective in the evolution of
rhabditoid to filariform larvae in the intestine, (b) mast
cells dysfunction, and (c) T-cell dysfunction by the reaction
with specific receptors on the CD4 ? Th2 cell membrane,
which increase the apoptosis of Th2 cells [15]. Further-
more, this drug can affect the female parasites, leading to
increased oviposition [16].
We recommend the provision of more awareness over
the high-risk people through screening for S. stercoralis
using more sensitive diagnostic methods prior to immu-
nosuppressive therapy.
Acknowledgments We would like to thank Dr. Ali-Asghar Pahl-
evan for the time generously spent in thoroughly revising the
manuscript.
Conflict of interest On behalf of all authors, the corresponding
author states that there is no conflict of interest.
References
1. Hakim SZ, Genta RM. Fatal disseminated strongyloidiasis in a
vietnam war veteran. Arch Pathol Lab Med. 1986;110:809–12.
2. Sasaki Y, Tanigushi T, Kinjo M, McGill RL, McGill AT, Tsuha
S, Shiiki S. Meningitis associated with strongyloidiasis in an area
endemic for strongyloidiasis and human T-lymphotropic virus-1:
a single-center experience in Japan between 1990 and 2010.
Infection. 2013;41:1189–93.
3. Al-Hasan MN, McCormick M, Ribes JA. Invasive enteric
infections in hospitalized patients with underlying strongyloidi-
asis. Am J Clin Pathol. 2007;128:622–7.
4. Moghadam KG, Khashayar P, Hashemi M. Gastrointestinal
strongyloidiasis in immunocompromised patients: a case report.
Acta Med Indones. 2011;43:191–4.
5. Yassin MA, El Omri H, Al-Hijji I, Taha R, Hassan R, Aboudi
KA, El-Ayoubi H. Fatal Strongyloides stercoralis hyperinfection
in a patient with multiple myeloma. Braz J Infect Dis.
2010;14:536–9.
6. Basile A, Simzar S, Bentow J, Antelo F, Shitabata P, Peng SK,
Craft N. Disseminated Strongyloides stercoralis: hyperinfection
during medical immunosuppression. J Am Acad Dermatol.
2010;63:896–902.
7. Mokaddas EM, Shati S, Abdulla A, Nampoori NR, Iqbal J, Nair
PM, et al. Fatal strongyloidiasis in three kidney recipients in
Kuwait. Med Princ Pract. 2009;18:414–7.
8. Vilela EG, Clemente WT, Mira RR, Torres HO, Veloso LF,
Fonseca LP, et al. Strongyloides stercoralis hyperinfection syn-
drome after liver transplantation: case report and literature
review. Transpl Infect Dis. 2009;11:132–6.
9. Bava AJ, Troncoso AR. Strongyloides stercoralis hyperinfection
in a patient with AIDS. J Int Assoc Physicians AIDS Care (Chic).
2009;8:235–8.
10. Wirk B, Wingard JR. Strongyloides stercoralis hyperinfection in
hematopoietic stem cell transplantation. Transpl Infect Dis.
2009;11:143–8.
11. Kia EB, Rahimi HR, Mirhendi H, Nilforoushan MR, Talebi A,
Zahabiun F, et al. A case of fatal strongyloidiasis in a patient with
chronic lymphocytic leukemia and molecular characterization of
the isolate. Korean J Parasitol. 2008;46:261–3.
12. Rokni MB. The present status of human helminthic diseases in
Iran. Ann Trop Med Parasitol. 2008;102:283–95.
13. Ashrafi K, Tahbaz A, Rahmati B. Strongyloides stercoralis: the
most prevalent parasitic cause of eosinophilia in gilan province.
Northern Iran. Iran J Parasitol. 2010;5:40–7.
Fatal Strongyloides hyper-infection
123
14. Fardet L, Genereau T, Poirot JL, Guidet B, Kettaneh A, Cabane J.
Severe strongyloidiasis in corticosteroid-treated patients: case
series and literature review. J Infect. 2007;54:18–27.
15. Concha R, Harrington W Jr, Rogers AI. Intestinal strongyloidi-
asis: recognition, management, and determinants of outcome.
J Clin Gastroenterol. 2005;39:203–11.
16. Nagalotimath SJ, Ramaprasad AV, Chandrashekhar NK. Fatal
strongyloidiasis in a patient receiving corticosteroids. Indian J
Pathol Bacteriol. 1974;17:190–2.
M. Saraei et al.
123

