-
8/13/2019 Fatigue Fx Military Conscripts
1/73
From the Department o Orthopaedics and raumatology,Helsinki
University Central Hospital, University o Helsinki,
and Centre o Military Medicine, Helsinki
FATIGUE FRACTURES IN MILITARY CONSCRIPTS
A STUDY ON RISK FACTORS, DIAGNOSTICS AND
LONG-TERM CONSEQUENCES
Juha-Petri Ruohola
Academic Dissertation
o be presented with the permission o the Faculty o Medicine o
theUniversity o Helsinki,
or public discussion in the Auditorium o l Hospital, Helsinki
Uni-
versity Central Hospital,On March 9th, 2007, at 12 oclock
noon.
-
8/13/2019 Fatigue Fx Military Conscripts
2/73
Supervised by
Docent Harri Pihlajamki, MD, PhDCentre o Military
MedicineHelsinki, Finland
Reviewed by
Proessor Ilkka Arnala, MD, PhDDepartment o Orthopaedics and
raumatologyKuopio University HospitalKuopio, Finland
Docent Jari Parkkari, MD, PhDUniversity o ampere and UKK
Institute
ampere, Finland
Opponent
Proessor Hannu Aro, MD, PhDDepartment o Orthopaedics and
raumatologyurku University Hospitalurku, Finland
ISBN 978-952-92-1681-9 (paperback)ISBN 978-952-10-3771-9
(PDF)
http://ethesis.helsinki.fiHelsinki University Printing House
-
8/13/2019 Fatigue Fx Military Conscripts
3/73
To my buffers against the world,
Tiina-Mari, Laura and Saku-Petteri
-
8/13/2019 Fatigue Fx Military Conscripts
4/73
4
Contents
ABSTRACT . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . 6
LIST OF ORIGINAL PUBLICATIONS . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . 7
ABBREVIATIONS. . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
8
1. INTRODUCTION. . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
2. REVIEW OF THE LITERATURE . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . 11
2.1. Fatigue ractures . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . 11
2.2. erminology o bone stress injuries . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . 12
2.3. Bone anatomy, remodeling and reaction to stress . . . . . .
. . . . . . . . . 152.4. Incidence o bone stress injuries . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . 16
2.5. Risk actors or bone stress injuries. . . . . . . . . . . .
. . . . . . . . . . . . . . . . . 18
2.6. Diagnosis o bone stress injuries . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . 20
2.6.1. Clinical diagnosis o bone stress injuries . . . . . . . .
. . . . . . . . . 20
2.6.2. Radiological imaging in diagnosis o bone stress injuries.
. . 22
2.7. Differential diagnosis o bone stress injuries . . . . . . .
. . . . . . . . . . . . . 24
2.8. reatment and long-term consequences o bone stress injuries.
. . . 253. AIMS OF THE PRESENT STUDY . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . 28
4. MATERIALS AND METHODS . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . 29
4.1. Patients . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
29
4.2. Methods. . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31
4.2.1. Study description. . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . 31
4.2.2. Clinical diagnosis and treatment . . . . . . . . . . . .
. . . . . . . . . . . . . 33
4.2.3. Imaging methods. . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . 33
4.2.4. Statistical methods . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . 33
-
8/13/2019 Fatigue Fx Military Conscripts
5/73
5
5. RESULTS . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
35
5.1. Serum 25OHD concentration as a potential predisposingactor
or atigue bone stress racture, incidence andanatomic distribution o
these ractures, and their relationshipwith age, weight, height,
BMI, muscle strength, and result o
running test. (I). . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . 355.2. RACP-5b
bone resorption marker as a potential indicator
o enhanced bone remodeling in military conscripts withstress
ractures, and the incidence and anatomic distributiono these
ractures. (II) . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . 37
5.3. Fatigue bone stress injuries associated with anterior
lowerleg pain; incidence and distribution, MRI based injury
gradesdepending on injury location and duration o symptoms. (III).
. . . 38
5.4. Incidence, symptomatology, morphologic characteristics,
clinical course, risk actors, and long-term outcomes odisplaced
and non-displaced atigue ractures o the emoralneck. (IV, V) . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . 40
6. DISCUSSION . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
47
6.1. Prevalence and anatomic distribution o atigue bone
stressinjuries . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
47
6.2. Diagnosis and characteristics o atigue bone stress
injuriescausing stress-related lower leg pain. . . . . . . . . . .
. . . . . . . . . . . . . . . . . 47
6.3. Serum 25OHD concentration as a predisposing actoror atigue
bone stress injury. . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . 48
6.4. RACP-5b bone resorption marker as an indicator oatigue bone
stress injuries . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . 50
6.5. Other risk actors or atigue bone stress injuries . . . . .
. . . . . . . . . . 51
6.6. Te long-term outcomes o atigue ractures othe emoral neck. .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . 52
7. CONCLUSIONS . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 55
8. SUMMARY . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
57
9. ACKNOWLEDGEMENTS . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . 60
REFERENCES. . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
62
ORIGINAL PUBLICATIONS . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . 75
-
8/13/2019 Fatigue Fx Military Conscripts
6/73
6
ABSTRACT
Fatigue racture is an overuse injury commonly encountered in
militaryand sports medicine, and known to relate to intensive or
recently intensi-fied physical activity. Bone responds to increased
stress by enhanced re-modeling. I physical stress exceeds bones
capability to remodel, accumula-tion o microractures can lead to
bone atigue and stress racture. Clinicaldiagnosis o stress ractures
is complex and based on patients anamnesisand radiological imaging.
Bone stress ractures are mostly low-risk inju-ries, healing well
afer non-operative management, yet, occurring in high-
risk areas, stress ractures can progress to displacement, ofen
necessitatingsurgical treatment and resulting in prolonged
morbidity.
In the current study, the role o vitamin D as a predisposing
actor oratigue ractures was assessed using serum 25OHD level as the
index. Teaverage serum 25OHD concentration was significantly lower
in conscriptswith atigue racture than in controls. Evaluating
RACP-5b bone resorp-tion marker as indicator o atigue ractures,
patients with elevated serumRACP-5b levels had eight times higher
probability o sustaining a stressracture than controls. Among the
154 patients with exercise induced an-terior lower leg pain and no
previous findings on plain radiography, MRIrevealed a total o 143
bone stress injuries in 86 patients. In 99% o the cases,injuries
were in the tibia, 57% in the distal third o the tibial shaf. In
patientswith injury, orty-nine (57%) patients exhibited bilateral
stress injuries. In a20-year ollow-up, the incidence o emoral neck
atigue ractures prior to theFinnish Deence Forces new regimen in
1986 addressing prevention o theseractures was 20.8/100,000, but
rose to 53.2/100,000 aferwards, a significant2.6-old increase. In
nineteen subjects with displaced emoral neck atigueractures, ten
early local complications (in first postoperative year) were
evi-dent, and afer the first postoperative year, osteonecrosis o
the emoral head
in six and osteoarthritis o the hip in thirteen patients were
ound.It seems likely that low vitamin D levels are related to
atigue ractures, and
that an increasing trend exists between RACP-5b bone resorption
markerelevation and atigue racture incidence. Tough seldom detected
by plainradiography, atigue ractures ofen underlie unclear lower
leg stress-relatedpain occurring in the distal parts o the tibia.
Femoral neck atigue ractures,when displaced, lead to long-term
morbidity in a high percentage o patients,whereas, when
non-displaced, they do not predispose patients to subsequentadverse
complications. Importantly, an educational intervention can
dimin-
ish the incidence o racture displacement by enhancing awareness
and pro-viding instructions or earlier diagnosis o atigue
ractures.
-
8/13/2019 Fatigue Fx Military Conscripts
7/73
7
LIST OF ORIGINAL PUBLICATIONS
Tis thesis is based on the ollowing papers, which are reerred to
in thetext by their Roman numerals:
I Ruohola J-PS, Laaksi I, Ylikomi J, Haataja RI, Mattila VM,
Sahi, uohimaa PJ, Pihlajamki HK. An Association between
Serum25OHD3Concentrations and Bone Stress Fractures in Finnish
YoungMen. J Bone Miner Res 21:1483-1488, 2006.
II Ruohola J-PS, Mulari M, Haataja RI, Ettala O, Vnnen HK,
Pihla-jamki HK. Elevated Serum Levels o RACP-5b Predict Bone
StressInjuries: A Prospective cohort study, submitted.
III Ruohola J-PS, Kiuru MJ, Pihlajamki HK. Fatigue Bone
InjuriesCausing Anterior Lower Leg Pain. Clin Orthop Relat Res
444:216-223, 2006.
IV Pihlajamki HK, Ruohola J-PS, Kiuru MJ, Visuri . Displaced
Fem-oral Neck Fatigue Fractures in Military Recruits. J Bone Joint
Surg(Am) 88A:1989-1997, 2006.
V Pihlajamki HK, Ruohola J-PS, Weckstrm M, Kiuru MJ, Visuri
I.Long-term prognosis o non-displaced atigue ractures o the
emoralneck in young male adults. J Bone Joint Surg (Br)
88:1574-1579, 2006.
Te publishers have kindly granted permission to reprint the
original
articles.
-
8/13/2019 Fatigue Fx Military Conscripts
8/73
8
ABBREVIATIONS
25OHD 25-hydroxyvitamin D
99mc technetium-99m
BMC bone mineral content
BMI body mass index = a persons weight in kilogramsdivided by
height in meters squared
CECS chronic exertional compartment syndrome
C computerized tomography
HHS Harris hip score
LSD least significant difference
MR magnetic resonance
MRI magnetic resonance imaging
NSAID nonsteroidal anti-inammatory drug
P probability
PH parathyroid hormone
RACP5b tartrate-resistant acid phosphatase 5b
VAS visual analogue scale
-
8/13/2019 Fatigue Fx Military Conscripts
9/73
9
1. INTRODUCTION
Bone stress ractures are overuse injuries associated with
intensive or re-cently intensified physical activity. Consequently,
they are common amongathletes and military conscripts involved in
strenuous training programmes(Pentecost et al. 1964, Milgrom et al.
1986, Matheson et al 1987b, Jones etal. 1989, Sterling et al. 1992,
Clanton and Solcher 1994). Plenty o researchhas been conducted
investigating actors predisposing to stress ractures,and although
the results have been inconsistent, several proposals havebeen
published (Jones et al. 2002, Vlimki et al.2005). Tat the bone
stress
injuries detected with radiographic imaging methods (e.g.
scintigraphy,MRI) are ofen not only multiple and simultaneous but
also symptomless(Ha et al. 1991, Giladi et al. 1991, Kiuru et al.
2002, Niva et al. 2005) sug-gests, however, a greater
susceptibility to stress ractures among certainpersons compared to
others. Furthermore, considering the wide evidenceregarding the
association o vitamin D with bone health (Compston 1998,Utiger
1998, Lips 2001, Holick 2003a), a possible association o vitamin
Dstatus with stress ractures would seem well worth intensified
research.
When bone is subject to elevated stress levels, it accelerates
its remod-eling process in which the damaged bone cells dissolve
and new matrixis laid down to permit ormation o new cells. Should
the physical stressexceed bones remodeling capacity, the repair
process may remain incom-plete, thus making way to microractures in
the bone and bone atigue.Tese changes in the bone structure
increase proneness to stress ractures(Li et al. 1985, Jones et
al.1989, Boden and Osbahr 2000).
A clinical diagnosis o a atigue bone stress injury, as well as a
differentialdiagnosis distinguishing it rom other imitating
conditions can be compli-cated (Mubarak et al. 1982, McBryde 1985,
Michael and Holder 1985, Mil-grom et al. 1986, Rosors et al. 1992,
Hutchinson and Ireland 1994). Stress
related anterior lower leg pain, which is very common among
military re-cruits and certain athletes (Milgrom et al. 1986,
Clanton and Solcher 1994),is ofen reerred to under categories like
shin splints or medial tibial stresssyndrome that cover a wide
spectrum o conditions behind the pain (Millset al. 1980, Dettmer
1986). Radiographic imaging in its various orms hasbeen widely
exploited to confirm the diagnosis. Since many stress injuriesare
not detectable even by plain radiography, magnetic resonance
imaging(MRI) has been increasingly preerred as offering superior
sensitivity ordetecting these injuries even at an early stage (Lee
and Yao 1988, Anderson
and Greenspan 1996, Kiuru et al. 2002). Unortunately MRI is not
widelyavailable, which can delay the diagnosis and treatment o
stress injury, thus
-
8/13/2019 Fatigue Fx Military Conscripts
10/73
10
possibly contributing to severe consequences and prolonged
morbidity(Salminen et al. 2003). Partly because o this, development
o a new useulinstrument is attracting wide interest to permit more
accurate detectiono bone stress ractures already in primary health
care units with limitedimaging acilities. Here, the knowledge
regarding biochemical markers o
bone resorption, such as RACP5b, which mirror the bodys rate o
boneloss (Stepan 2000), should encourage research about their
potential instress racture prediction.
Generally classified as benign low-risk injuries, bone stress
injurieshave mainly been treated non-operatively with reduced
exercise and non-weight-bearing. Occurring in high-risk areas e.g.
the emoral neck, theseinjuries can, nonetheless, progress to
displacement and other severe conse-quences and prolonged morbidity
(Salminen et al. 2003, Boden and Oshbar2000, Visuri et al. 1988).
However, previous reports on the long-term con-
sequences o emoral neck atigue ractures have mainly been case
reports.Tus, systematically collected data on the long-term outcome
o both dis-placed and non-displaced emoral neck atigue ractures are
lacking.
-
8/13/2019 Fatigue Fx Military Conscripts
11/73
11
2. REVIEW OF THE LITERATURE
2.1. Fatigue fractures
A German military surgeon J. Breithaupt was the first doctor in
history(Breithaupt 1855) to describe atigue racture in literature.
However, heailed to recognize the main reason or painul and swollen
eet associ-ated with marching in Prussian soldiers, mistaking a
atigue racture or
a traumatic inammatory reaction. Since the year 1855, the
majority opublications describing stress reactions o bone have been
based on stud-ies among military recruits until, in the last our
decades, an increasingnumber o studies concerning stress injuries o
bone among athlete popu-lations have appeared in the medical
literature (Jones et al. 1989). Te actthat military publications
are so well presented in medical literature withrespect to bone
atigue ractures is due to military populations having beenin the
past the only populations large enough, with their type and level
ophysical activity, to provide suffi cient amounts o stress
reactions o boneto raise general interest among medical
researchers. Only later, with theever-growing number o people
participating in fitness and sports trainingprograms, have stress
ractures become increasingly common in civilianathlete populations
as well.
Once the condition behind the painul oot was detected using
X-raysinvented by Wilhelm Rntgen in 1895, and actually identified
as bone rac-tures (Stechow 1897), also other bones o the lower
extremities exhibitingsymptoms o stress-related pain were subjected
to observation. During thefirst hal o the 19thcentury, along with
more widely available native radi-ography, it became clear that
sites like tibial and emoral shaf as well as
emoral neck could be affected by atigue racture more ofen than
pre-viously thought. Another obvious finding was that the majority
o theseractures typically occurred during the first weeks or months
o militarytraining when physical activity intensified. For the
atigue racture itsel,several names were used, including march
racture, stress racture, exhaus-tion racture, spontaneous racture,
and others, some o which have re-mained in use until today (Branch
1944, Jones et al. 1989, Ha et. al 1991,Anderson and Greenspan
1996).
Clinically it was, and still is, diffi cult to make differential
diagnosis be-
tween stress racture and other pathological conditions
simulating it. Con-sequently, radiographs played a remarkable role
in the diagnosis until the
-
8/13/2019 Fatigue Fx Military Conscripts
12/73
12
1970s, when scintigraphy and MRI, offering a much better
sensitivity andspecificity, became valuable tools or the purpose.
Interestingly, at same timewhen these improved imaging methods with
higher accuracy were adoptedor diagnosis o stress ractures, the
most diagnosed racture location in thelower extremities moved rom
the metatarsal bones to the tibia in military
populations. Owing to its lower costs and good availability in
primary healthcare units, however, plain radiography has stayed
long as the first line toolor racture imaging. Only recently are
there signs that MRI is becomingcommon in medical practice (Lee and
Yao 1988, Shin et al. 1996, Deutschet al. 1997, Boden and Osbahr
2000, Spitz and Newberg 2002, Kiuru et al.2004, Niva et al. 2005,
Niva et al. 2006a and 2006b, Sormaala et al. 2006a and2006b).
oday, stress-related ractures have been described or nearly
every boneo our body. Te most common sites or stress ractures are
the weight-bear-
ing bones o the lower extremities and the pelvis. Both sites
have been typi-cally noted among military recruits due to the type
o physical training theyundergo, and among athletes, o whom runners
in particular have emergedas the main subgroup suffering rom these
injuries (Hallel et al. 1976, Rupaniet al. 1985, Hulkko and Orava
1987, Matheson et al. 1987b, Boden and Osh-bar 2000, Jones et al.
2002, Kiuru et al. 2004, Kiuru et al. 2002).
2.2. Terminology of bone stress injuries
Stress racture as a term in itsel can be potentially misleading,
because stress
injuries o the bone, although diagnosed and classified under the
rubric o
stress ractures, do not necessarily result in a racture line or
a break in bone
continuity (Jones et al. 1989). Pathophysiology o these injuries
covers a wide
spectrum o events, rom accelerated remodeling to stress racture
(Anderson
and Greenspan 1996).
Stress reaction is the first phase indication that a stress
injury is develop-
ing to a bone. Tis reaction starts, when adaptability o the bone
to increased
repetitive stress is overloaded. In these early phases, native
radiography ofen
shows normal findings, whereas on MRI, marrow edema can be seen
(Lee andYao 1988, Kiuru et al. 2002).
Stress fracture occurs when the abnormal stress continues
without the
needed recovery periods or the bone, and the bone responds by
incomplete
remodeling. Callus or racture line can then be visualized with
plain radi-
ography, and more certainly with MRI (Lee and Yao 1988, Anderson
and
Greenspan 1996). Bone stress ractures can be classified into two
main types,
atigue ractures and insuffi ciency ractures (Pentecost 1964,
Daffner and Pav-
lov 1992).
Fatigue fracturesoccur when normal bone, with normal elastic
resist-ance, is exposed to abnormal repetitive stress (Pentecost
1964, Daffner and
Pavlov 1992).
-
8/13/2019 Fatigue Fx Military Conscripts
13/73
13
Insuffi ciency fracturesoccur when abnormal bone, with deficient
elasticresistance, is exposed to normal stress (Pentecost 1964,
Daffner and Pavlov1992).
Pathological fracturesoccur in bone which is affected and
weakened by
another pathological lesion, such as inection or neoplasm
(Daffner andPavlov 1992).
Compressive fracturesmay occur when bone is exposed to
compressiveorces along the concave margin o the bone. Stress
ractures o the emoralneck located at the inerior surace o the neck
are typical compression-side ractures (Fullerton et al. 1988, Flinn
et al. 2002).
Tension fractures may occur when bone is exposed to tensile
orcesalong the convex margin o the bone. Stress ractures o the
emoral necklocated at the superior surace o the neck are typical
tension-side ractures
(Fullerton et al. 1988, Flinn et al. 2002).Low-risk stress
injuriescan usually be diagnosed on the basis o care-
ul anamnesis, physical examination, and radiographs. Moreover,
they canbe treated with rest periods without a ear o problematic
consequences(Boden et al. 2001). According to Boden et al. (2001),
the low-risk sitesare, with some exceptions, the upper extremities,
the ribs, the pelvis, theemoral shaf, the tibial shaf, the fibula,
the calcaneus, and the metatarsalshaf.
High-risk stress injuriescan, unortunately, progress to complete
rac-ture, displacement, delayed union, or nonunion, and they
thereore requirea more aggressive approach. Tey commonly occur on
the tensile side obone, or in bone areas with critical blood
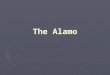
supply. Te problematic sites arethe emoral neck (tension side, Fig
1), the patella, the anterior cortex o thetibia, the medial
malleolus, the talus, the tarsal navicular, the fifh metatar-sal,
the second metatarsal base, and the first digit sesamoids (Boden
andOshbar 2000, Lassus et al 2002).
Risk factoris an attribute or circumstance associated with
enhanced risko developing a specific disease. Identification and
understanding o a riskactor can provide an opportunity to create
preventive strategies against
the disease related to that particular risk actor.
-
8/13/2019 Fatigue Fx Military Conscripts
14/73
14
Figure 1. ension and compression sides o the emoral neck.
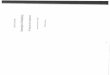
Figure 2. Te macroscopic and microscopic structure o bone
-
8/13/2019 Fatigue Fx Military Conscripts
15/73
15
2.3. Bone anatomy, remodeling and reaction to stress
Bone consists o two different components characterizing the
widelyvarying gross arrangement o this connective tissue. Te gross
anatomyis greatly inuenced by the position and unction o the bone
within the
body. Cortical bone is typically present along the outer margin
o longbones. Cancellous (trabecular or spongy) bone is usually ound
at the endo long bones and internal to cortical bone, or it can
compose some bones,e.g. the calcaneus, almost alone (Fig 2). Te
basic histological structure othese bone types is equal to both,
but differences exist. Cortical (compactor dense) bone has, as
justly indicated by its name, a solid architecture,which only the
narrow canals o the Haversian systems interrupt. Corti-cal bone has
a low surace-to-volume ratio, with the cells completely sur-rounded
by bone matrix. Cancellous bone is a meshwork o longitudinal
(primary) and transverse (secondary) trabeculae separated by
hematopoi-etically active red marrow or hematopoietically inactive,
yellow (atty)marrow. Cancellous bone has a high surace-to-volume
ratio, with the cellsdirectly inuenced by bone marrow cells,
ensuring that the bone is undera better metabolism control when
compared to cortical bone. Te extracel-lular matrix o bone tissue,
with its chemical composition o both organicand inorganic elements,
enables bone to withstand physical stresses betterthan other
tissues.
Trough a microscope, bone is composed mainly o extracellular
ma-trix and cells that represent the lesser amount o organic matter
in bone.Osteoblasts, osteoclasts, osteocytes and osteoprogenitor
cells are the ouractive matrix cell types ound in bone. Bone
metabolism is regulated bybone cells and the regulation depends on
the cell activity. Since osteob-lasts main unction is to synthesize
and mineralize bone matrix, they areregarded as bone orming cells.
I the osteoblast becomes surrounded bythe matrix it has been
producing, it can become an osteocyte with meta-bolically inactive
appearance. Osteocytes are numerous in the mineralizedbone matrix o
both cancellous and cortical bone. Teir unction is notcompletely
understood, but they are assumed to play a role in the mechani-
cal regulation and regeneration o bone (Cowin et al. 1991,
Lanyon 1993,Mullender and Huiskes 1995 and 1997). Osteoclasts are
cells that unctionin the resorption process o calcified bone
matrix. Osteoprogenitor cellsare ound throughout the bones, and,
under relevant stimulation, they candifferentiate into unctional
osteoblasts (Buckwalter et al. 1995).
Bone is a dynamic connective tissue that requires stress or
normal de-velopment and health (Sterling et al. 1992).
Metabolically, bone is never atrest. In a continual ormation,
resorption and remodeling process takingplace throughout the bone,
the osteoblasts orm and the osteoclasts remove
bone matrix without remarkably affecting the shape or density o
the bone.In healthy bone, under a constant load, normal bone
remodeling occurs
-
8/13/2019 Fatigue Fx Military Conscripts
16/73
16
through osteoclast resorption and osteoblast reconstruction o
the bonetissue, meaning that these two are in balance with each
other. One com-ponent both contributing to osteoclast activity and
enhancing the differ-entiation o osteoclast and osteoblast
precursors is vitamin D (Riggs 1997,Utiger 1998, Holick 2003b),
which also lowers intact parathyroid hormone
(iPH) secretion and controls both calcium absorption and
reabsorption(Utiger 1998). With the calcium and phosphate
homeostasis having a ma-jor effect on bone mineralization, in the
event o dietary calcium inad-equacy, vitamin D causes osteoclasts
to mature and resorb calcium romthe bone (Compston 1998, Lips 2001,
Vlimki et al. 2004). A possible re-lationship between calcium
intake and stress racture has been investigatedin some studies, but
the evidence is still lacking (Lips et al. 1991, McKaneet al.
1996).
Under an increasing load, with the bone subject to prolonged,
recurrent
or excessive stress, the remodeling process accelerates through
stimulatedbone resorption, resulting in incomplete remodeling
response (Li et al.1985, Burr et al. 1990). Dominant osteoclastic
activity at bone stress sitesmay cause local weakening o the bone,
thus predisposing it to microdam-age (Werntz and Lane 1993). With
continuing abnormal loading, thesemicrodamages, also called
microractures, can gradually progress to com-plete ractures (Knapp
and Garrett 1997). On the other hand, i the load isreduced,
diminishing stress to the bone and giving the remodeling
processtime to normalize, the development o bone racture can be
avoided.
2.4. Incidence of bone stress injuries
Stress racture is a commonly seen injury type in sports clinics
as well asthe primary health care units o military health services
(able 1) (Morrisand Blickenstaff 1967, Mills et al.1980, Milgrom et
al.1985, Hulkko andOrava 1987, Matheson et al. 1987b, Beck et al.
1996). Te overall incidenceo stress ractures in military recruits
has varied between 0.9% and 12.3%,but incidences as high as 31%
have been reported (Brudvig et al. 1983, Sahi
1984, Milgrom et al. 1985, Jones et al. 1993, Macleod et al.
1999, Givon etal. 2000, Armstrong et al. 2004, Lappe et al. 2005).
In the Finnish DeenceForces, the current published incidences o
bone stress injuries have stayedwithin these values (Sahi et al.
1996, Vlimki et al. 2005). However, withmost o the stress ractures
in the Finnish Deence Forces occurring dur-ing the first two or
three months o military service, the military conscriptsrepresent a
homogenous exposure group regarding physical stress duringthe
8-week basic training period equal or all. In contrast, there is
consid-erable variation internationally between armed orces, and
even military
branches, with respect to training procedures, physical fitness
o traineesand methodology o diagnosis (Kiuru et al. 2004).
-
8/13/2019 Fatigue Fx Military Conscripts
17/73
17
Table 1. Previous studies o bone stress injuries o the lower
extremities
Author and year Participants Number of participants,
male/female
Method Incidence of bone
stress injuries,
male/female (%)
Hallel et al. 1976 military not reported prospective 5/-
Protzman and Griffi s, 1977 military 1228/102 prospective
1.0/9.8
Brudvig et al. 1983 military 20442 overall retrospective
0.9/3.4
Milgrom et al. 1985 military 295/- prospective 31/-
aimela et al. 1990 military 108/- prospective 7.4/-
Finestone et al. 1991 military 392/- prospective 24/-
Jones et al. 1993 military 124/186 prospective 2.4/12.3
Goldberg and Pecora, 1994 athletes approx. 1000 overall
retrospective 1.9 overall
Johnson et al. 1994 athletes 914 overall prospective 2.6
overall
Beck et al. 1996 military 626/- prospective 3.7/-
Bennell et al. 1996 athletes 49/46 prospective 20.4/21.7
Macleod et al. 1999 military 3367/855 retrospective 2.8/10.8
Armstrong et al. 2004 military 1021/203 prospective 2.3/8.4
Lappe et al. 2005 military -/4139 prospective -/4.7
Vlimki et al. 2005 military 179/- prospective 8.4/-
In the general athletic population, the incidence has remained
below3.7% (Matheson et al. 1987b, Jones et al. 1989, Goldberg and
Pecora 1994).In runners and some other groups o athletes, the
occurrence o bone stressinjuries might be somewhat higher, rom 10%
to 31% (Matheson et al.1987b, Boden and Oshbar 2000, Jones et al.
2002, Kiuru et al. 2004).
Almost all stress ractures among military trainees and athletes
areound in the lower extremities or the pelvis (Milgrom et al.
1985, Math-
eson et al. 1987a, Jones et al. 1989, Ha et al. 1991, Jones et
al. 2002, Kiuruet al. 2002, Kiuru et al. 2004, uan et al. 2004).
Although the variation re-ported in different studies concerning
the distribution o stress injuries inthe lower extremities is
remarkable, these injuries have been encounteredin nearly every
bone o the oot and leg, as well as around the hip joint(Visuri et
al. 1988, Visuri 1997, Williams et al. 2002, Lee et al. 2003, Song
etal. 2004, Niva et al. 2005). However, the most common sites or
bone stressinjuries are the tibia and the metatarsal bones.
(Milgrom et al. 1985, Joneset al. 1989, Bennell et al. 1996).
-
8/13/2019 Fatigue Fx Military Conscripts
18/73
18
2.5. Risk factors for bone stress injuries
Numerous reports have documented that the main cause
predisposingbone to stress injuries is repeated or recently started
mechanical loading(Lassus et al. 2002, uan et al. 2004). In
addition, various potential risk
actors have been proposed to explain, more or less, why some
sustain astress racture while others do not. Tese etiological risk
actors can becategorized as extrinsic (external) or intrinsic
(internal) (able 2). Ex-trinsic actors are characteristics o the
environment in whose activitiesthe individual participates.
Extrinsic causes include training conditions,methods and equipment,
and training errors, such as excessive intensity orvolume, duration
and change o each strain cycle, excessive muscle atigue,and aulty
or wrong technique. Intrinsic actors, e.g. mechanical, muscu-lar,
nutritional or hormonal actors, are characteristics o the
individuals
themselves. Intrinsic causes include muscle atigue leading to
transmis-sion o excessive orces to underlying bone (Blickenstaff
and Morris 1966,Boden and Osbahr 2000), muscle imbalance, insuffi
cient exibility dueto generalized muscle tightness, ocal muscle
thickening, limited range ojoint motion, lack o bone strength due
to decreased bone mineral density(Pouilles at al 1989), and
psychological actors like nutritional intake andeating disorders
(Matheson et al 1987b, Bennell et al. 1999)
Table 2. Possible risk actors or bone stress injuries according
to Bennell et al. 1999
Intrinsic risk factors Extrinsic risk factors
Bone mineral density . . . . . . . . . . . . . . . . . . . . . .
. Volume o training
Bone geometry . . . . . . . . . . . . . . . . . . . . . . . . .
. Pace o training
Skeletal alignment. . . . . . . . . . . . . . . . . . . . . . .
. . Intensity o training
Body size and composition. . . . . . . . . . . . . . . . . . . .
Recovery periods
Bone turnover . . . . . . . . . . . . . . . . . . . . . . . . .
. . Faulty training technique
Muscle exibility and joint range o motion . . . . . . . . . .
raining surace
Muscular strength and endurance . . . . . . . . . . . . . . . .
Footwear/insoles/orthotics
Calcium intake . . . . . . . . . . . . . . . . . . . . . . . . .
. External loading
Caloric intake/eating disorders
Nutrient deficiencies
Sex hormones
Menarcheal age
Other hormones
Physical fitness
Age
Gender
-
8/13/2019 Fatigue Fx Military Conscripts
19/73
19
Several publications have studied risk actors contributing to a
predis-position to stress ractures, and quite ofen the results have
been, in wholeor in part, conicting with each other. Moreover,
there exists a possibil-ity that risk actors have the potential to
predispose bone to developingstress ractures alone or through the
joint effect o various actors. O the
risk actors or stress ractures, emale gender, age, body
composition,bone characteristics, low bone density and bone
strength, low aerobic fit-ness, low past physical activity level,
smoking, and excessive running havebeen identified in an
epidemiologic review (Bennell et al. 1999, Jones et al.2002).
Several studies based on bone scintigraphy or MRI regarding the
lowerextremities or the pelvis, have reported occurrence o multiple
simultane-ous bone stress injuries in the same individual (Ha et
al. 1991, Giladi et al.1991, Nielens et al. 1994, Kiuru et al.
2002, Niva et al. 2005). Multiple rac-
tures may imply that the subjects overall bone composition is
deective,and thus some general actor be present or predisposing
bone to stressractures (Fig 3AB).
Figure 3AB.A 19-year-old male conscript suffering rom knee pain.
Plain radiographyreveals bone stress injuries in both the right (A)
and the lef (B) knee.
A B
-
8/13/2019 Fatigue Fx Military Conscripts
20/73
20
2.6. Diagnosis of bone stress injuries
2.6.1. Clinical diagnosis of bone stress injuries
Clinical diagnosis o bone stress injuries with no specific signs
or findings
is a diffi cult task. However, the complexity should not deter
the physicianrom action, since an early suspicion and diagnosis o a
possible stress in-jury is essential or adequate treatment (Fig
4AB). Te clinical diagnosis obone stress injury is based on the
patient history o physical activity, dura-tion and type o symptoms,
and a number o uncertain clinical findingsneeding confirmation by
radiological imaging methods.
Figure 4AB.An 18-year-old male conscript suffering rom oot pain.
Te stress racturein the third metatarsal bone is hardly detectable
on the primary radiographic image (A),yet despite a rest period,
displacement o racture is observed a week later (B).
Te symptoms o a developing stress injury ofen appear 2 to 3
weeksafer the beginning or remarkable intensification o training.
However, du-
ration o the evolution o injury may vary rom days to months
(Greaney etal. 1983, Jones et al. 1989, Ha et al. 1991). At the
early stages o stress injury,
A B
-
8/13/2019 Fatigue Fx Military Conscripts
21/73
21
the patient may be symptomless on clinical examination.
Stress-related painwith no previous trauma can occur suddenly or
gradually, and may varyrom radiating to very unspecific.
Furthermore, at least among military re-cruits, the motivation or
duty and service combined with personal charac-teristics can
produce very diverse reactions to exercise-induced pain (Hallel
et al. 1976). At the onset, pain can be exercise-induced only,
generally disap-pearing with rest. However, even then, and more
probably so i loading con-tinues non-reduced, pain will be present
also at rest and during nights. Telocation o pain and suspected
racture can be clinically very important, a-ecting decision making
concerning appropriate treatment. Some high-riskstress ractures,
e.g. displaced emoral neck racture, can cause severe com-plications
and prolonged recovery, leading all the way to avascular
necrosisand joint replacement surgery (Blickenstaff and Morris
1966, Fullerton andSnowdy 1988, Visuri et al. 1988, Johansson et
al. 1990, Mendez and Eyster
1992). In these specific locations o suspected racture, early
suspicion andaccurate diagnosis are even more important to avoid
racture displacementand surgical treatment.
Swelling and discolouration with local warmth (Anderson and
Green-span 1996) may be seen, and localized pain and possible
periosteal thicken-ing indicating new bone ormation, callus, may be
palpable (Sterling et al.1992). Pain at a distant site produced by
the percussion o bone, e.g. in thetibia, can signal a stress
injury. A ew special tests exist, the ulcrum test orexample, or
diagnosing a stress injury (Johnson et al. 1994) in the emoralbone,
which is otherwise diffi cult to palpate due to strong muscles
coveringit (Fig 5).
No appropriate laboratory tests exist to assist the diagnosis o
stressractures in primary health care units with no advanced
imaging modali-ties. However, biochemical markers o bone resorption
reecting the rateo bone loss (Stepan 2000) have been the ocus o
recent research, aimedat developing an adequate diagnostic test.
Tese markers are relatively in-expensive, widely available and,
expressing both bone quantity and qual-ity, they would be
conceivable aspossible racture predictors.One o thesepotential bone
turnover markers, RACP5b is secreted into circulation
during osteoclast resorption, mirroring this osteoclastic
activity in enzymesecretion and bone degradation (Nesbitt and
Horton 1997, Salo et al. 1997,Vrniemi et al. 2004). RACP5b has been
suggested to be an independ-ent, specific, and sensitive serum
markero bone resorption (Halleen et al.,2000, Halleen 2003, Nenonen
et al. 2005). It has so ar been successullyused in monitoring
response to the treatment o bone metastases in cancerpatients (Wada
et al. 1999, erpos et al. 2003).
-
8/13/2019 Fatigue Fx Military Conscripts
22/73
22
Figure 5.Fulcrum test: Patient is seated with the lower legs
dangling. Examiners arm isused as ulcrum under the patients distal
thigh moving the arm towards the proximalthigh, while applying
gentle pressure to the dorsum o the patients knee with the
oppo-site hand. Pain occurs when the arm as ulcrum is located under
the stress racture.
2.6.2. Radiological imaging in diagnosis of bone stress
injuries
Imaging studies are needed to confirm the diagnosis o stress
injuries(McBryde 1985, Michael and Holder 1985, Milgrom et al.
1986, Clantonand Solcher 1994, Anderson and Greenspan 1996). Plain
radiography hasgenerally been used as the primary imaging tool
since the end o the 19 thcentury. Only two years afer Wilhelm
Rntgen discovered X-rays was thetechnology already used to detect
stress ractures in the metatarsals (Ste-chow 1897), and it has
maintained its position as the first-line imagingtool owing to its
common availability and cost effectiveness. However, inimaging o
stress injuries, the sensitivity o radiography at the early stageso
injury may be as low as 10%, although in the ollow-up o these
injuries,
it rises to 30% and up to 70% (Prather et al. 1977, Orava 1980,
Greaneyet al. 1983, Rupani et al. 1985, Matheson et al 1987a,
Nielsen et al. 1991).Because o the somewhat low sensitivity,
diagnosis has ofen been based onbone scintigraphy or MRI in
patients with stress related pain and no visiblestress injury on
radiographs.
Bone scintigraphy was considered the gold standard or detecting
earlystages o bone stress injuries rom the 1970s until the early
2000s, when itbegan to give way to MRI (Kiuru et al. 2002).
Acceleration in bone metabo-lism related to stress injuries is
visible on scintigraphy long beore changes
are seen on radiography. Bone scintigraphy is substantially more
sensitive(nearly 100% sensitivity) than radiography, but its
specificity is inerior,
-
8/13/2019 Fatigue Fx Military Conscripts
23/73
23
so that identification o pathological conditions in particular,
such as tu-mors, inections and traction periostitis, remains
deficient (Anderson andGreenspan 1996, Kanstrup 1997). Te radiation
dose received at a scinti-graphic examination is equal to a dose o
two years o background radia-tion (Kanstrup 1997). oday, MRI is
overriding scintigraphy in terms o
availability as well.Magnetic resonance imaging (MRI) offers not
only a high sensitivity
but also a superior specificity in detecting the early changes
related to bonestress injury, yet without exposing the body to
ionizing radiation (Lee andYao 1988, Anderson and Greenspan 1996,
Kiuru et al 2002). It is thereoreully understandable that MRI is
currently considered the gold standardin stress injury imaging.
Moreover, its high contrast and spatial resolutionpermit
visualization oassociated sof tissue involvement (Anderson et
al1997, Deutsch et al. 1997). On MRI, a developing bone stress
racture can
be detected already at its earliest stages, with the initial
signs o bone stressinjury being displayed as periosteal or
endosteal marrow edema. However,as such endosteal edema may signal
other pathological conditions as well,the finding should be
considered non-specific (Schweitzer and White 1996,Lazzarini et al.
1997). Endosteal bone marrow edema has also been docu-mented in
healthy, physically active asymptomatic patients, and becausethese
asymptomatic low grade injuries do not seem to possess a tendencyto
progress to higher grade injuries, MR imaging o asymptomatic
militarytrainees or athletes is not recommended (Kiuru et al.
2005). Evolution o astress-related bone injury comprises several
varying stages, characterizedby an equally large variety o MRI
signs. For the purpose o assessmento these signs, several stress
reaction or racture grading scales have beenpublished (Lee and Yao
1988, Kiuru et al. 2001). According to the scalingsystem by Kiuru
et al. bone stress injuries are classified on the basis o
MRIfindings as: Grade I, endosteal marrow edema; Grade II,
periosteal edemaand endosteal marrow edema; Grade III, muscle
edema, periosteal edema,and endosteal marrow edema; Grade IV,
racture line; and Grade V, callusin cortical bone. A disadvantage o
MR imaging is still today the generalunavailability o the
technology. Moreover, its costs might be considered as
another limitation to its use.
-
8/13/2019 Fatigue Fx Military Conscripts
24/73
24
2.7. Differential diagnosis of bone stress injuries
Stress-related pain in the lower extremities is common in
military recruitsand athletes (Milgrom et al. 1986, Clanton and
Solcher 1994). It is diffi cult,or even impossible, to
differentiate a bone stress injury rom other patho-
logical conditions mimicking it based on clinical examination
alone, eventhough a patient history in terms o physical activity
level and symptoms isusually quite typical when concerning stress
injuries to bone (able 3). Tus,in the majority o cases, the history
combined with characteristic radio-graphic findings suffi ces to
reach the diagnosis. Diagnosis can, however, beurther conused by
imitating conditions, including exertional conditionslike the
compartment syndrome, and nonexertional inammatory,inectious,
vascular, neurological and tumorous conditions in sof tissuesand
bones (DAmbrosia 1977, Mubarak et al. 1982, McBryde 1985,
Michael
and Holder 1985, Milgrom et al. 1986, Rosors et al. 1992,
Hutchinson andIreland 1994). Tis again emphasizes the importance o
sensitivity and spe-cificity o the imaging method used in unclear
cases to ensure rapid andadequate diagnosis and treatment, usually
meaning the MRI. Stress-relatedpain in the lower extremities is
most commonly located in the anteriorlower leg. Although a
stress-related bone injury is by no means an unusualcause o lower
leg pain, yet with no findings suggestive o bone injury, thepain is
ofen reerred to as shin splints (traction periostitis), or the
medialtibial stress syndrome(Mills et al 1980, Detmer 1986).
However, the termslack accuracy covering so broad a spectrum o
possible conditions behindthe pain (Johnell et al 1982, Mubarak et
al. 1982, Michael and Holder1985, Gerow et al. 1993, Beck 1998). Te
differential diagnosis can be evenmore demanding, because
conditions like traction periostitis, chronic ex-ertional
compartment syndrome and bone stress injury can occur sepa-rately
or combined, and urthermore, because stress injuries ofen
affectseveral bones simultaneously. Such cases o simultaneous and
combinedsymptoms, diffi cult or both the patient and the physician
to pinpoint, cangreatly disturb the diagnosis (Giladi et al. 1991,
Ha et al. 1991, Kiuru etal. 2002, Niva et al. 2005). In patients
with lower grade injuries, treated by
reducing load with rest period, there exists already a suspicion
o a possiblestress racture. Nonetheless, the final diagnosis may
remain open, because,with decreased stress, the bone can heal a
developing stress injury beoreit becomes visible on radiographs,
and later, with less or no symptoms, apatient is likely never to
undergo repeated plain radiography or MRI scanto confirm the
diagnosis (Devas 1958, Li et al. 1998, Kiuru et al. 2005).
-
8/13/2019 Fatigue Fx Military Conscripts
25/73
25
Table 3.Differential diagnosis o bone stress injuries
Conditions imitating bone stress injuries
Exertional compartment syndrome
Bone tumors and metastaseInammatory disease
Inectious condition
ransient bone marrow edema
raction periostitis
Osteonecrosis
Vascular pathological condition
Neurological pathological condition
Osteomyelitis
Osteomalacia
Bursitis
Iliotibial band syndrome
Distal emoral cortical deect
Femoral cortical excavation
Internal derangement o the knee
Mortons neuroma
Osteochondral racture
2.8. Treatment and long-term consequences of
bone stress injuries
Te anatomic location o the injury carries mentionable prognostic
im-portance or the possible long-term consequences o bone stress
injury,since some injuries involving bones like the emoral neck are
more prone
to displacement and severe complications than those ound at
other bonesand sites (able 4). Te majority o low-risk stress
ractures seen in clinicsare managed conservatively with reduced
exercise, and heal with no earo complications (Fig 6AB). In more
severe cases, use o crutches, splints,or casts may be necessary. In
displacements or other ractures where non-operative treatment is
insuffi cient, surgical treatment, mainly internal fixa-tion, is
warranted (Hulkko and Orava 1987). Regarding the nature andextent o
reduced exercise as a treatment method, these depend on the siteand
grade o injury, varying rom a period o cutting down daily
physical
exercise to a hal to a period o complete inactivity including a
possiblenon-weight-bearing period or up to 8 weeks. In military
service, this o-
-
8/13/2019 Fatigue Fx Military Conscripts
26/73
-
8/13/2019 Fatigue Fx Military Conscripts
27/73
27
Figure 6AB.A stress acture in the third metatarsal bone o a
20-year-old male conscript
(A) was treated conservatively with rest periods and reduced
exercise. Te healed ractureshown six months later (B).
A B
-
8/13/2019 Fatigue Fx Military Conscripts
28/73
28
3 AIMS OF THE PRESENT STUDY
I. o assess the effect o serum 25OHD concentration as a
predisposingactor on atigue bone stress injuries, and to evaluate
the incidence andanatomic distribution o these injuries and their
relationship with age,weight, height, BMI, muscle strength, and
result o running test.
II. o determine i RACP-5b bone resorption marker indicates
enhancedbone remodeling in military conscripts with stress
ractures, and to evalu-ate the incidence and anatomic distribution
o these bone stress injuries.
III. Based on MR imaging, to determine the incidence o atigue
bonestress injuries causing stress related anterior lower leg pain,
and to assesstheir anatomic distribution, grade o injury with
respect to location, andduration o symptoms beore diagnosis.
IV/V. o evaluate the incidence, symptomatology, morphologic
charac-teristics, clinical course, risk actors and long-term
outcomes o displacedand non-displaced atigue ractures o the emoral
neck, and to assess theeffects o instructions by the Finnish Deence
Forces, Department o Medi-cal Services in 1986 or the prevention o
emoral neck atigue ractures inmilitary service.
-
8/13/2019 Fatigue Fx Military Conscripts
29/73
29
4 MATERIALS AND METHODS
Te two prospective cohort studies (I, II) were conducted at the
Pori Bri-gade, Skyl, at the Research Institute o Military Medicine,
Central Mili-tary Hospital, Helsinki, at the University o ampere
(I), ampere, and atthe University o urku (II), urku. Te third,
retrospective study (III) wasconducted at the Department o
Radiology and at the Research Institute oMilitary Medicine, Central
Military Hospital, Helsinki. Te studies IV andV were conducted at
the Departments o Radiology and Surgery, and theResearch Institute
o Military Medicine, Central Military Hospital, Hel-
sinki. All the studies (I-V) were approved by the appropriate
Ethics Com-mittees. All study designs (I-V) were approved by the
Deence Staff o theFinnish Deence Forces.
4.1. Patients
All the participants included in Studies I-V were or had been
conscriptsperorming their military service in the Finnish Deence
Forces. All malecitizens o Finland become liable or a mandatory
military service at theage o 18, whereas emale citizens have had
the opportunity to volunteeror the service since year 1995.
Annually, on average 26,500 male con-scripts and 500 emale
conscripts underwent military training within thetime periods o
studies I-III, and the annual number o male conscriptswas between
34,723 and 36,606 during studies IV and V.
Study I
In July 2002, eight hundred young men (aged 18-28 years, mean
19.8years) entering into military training as conscripts o the same
inantry
unit (Pori Brigade) o the Finnish Deence Forces were randomly
selectedor the study. Tey had no known diseases or medications and
they all hadpassed the entrance medical examinations as healthy. Te
subjects repre-sented the common conscript population o the Finnish
Deence Forceswith no specific eatures. During their military
service, the conditions werehomogenous in that physical activity,
nutrition, clothing, accommodation,and exposure to sunlight were
the same or all participants. From the origi-nal sample, we
excluded patients whose ollow-up data was incomplete asa result o
ailed blood samples drawn during the study, and patients who
were compelled to interrupt their military service, which lef
the total o756 patients or the ollow-up.
-
8/13/2019 Fatigue Fx Military Conscripts
30/73
30
Study II
Eight hundred and twenty Finnish young men and women (aged
18-28years, mean 19.8 years; mean BMI 23.4) entering military
training in July2002 as conscripts o the same inantry unit (Pori
Brigade) o the FinnishDeence Forces were randomly selected or the
study. Tey had no previous
medication or diseases and they all passed their entry medical
examinationas healthy. Te subjects represented the general
conscript population othe Finnish Deence Forces without specific
eatures. During the militaryservice, the conditions related to
physical activity, nutrition, clothing, andaccommodation were
homogenous or all subjects.
Study III
Material or Study III covered a study period o five years, rom
March1, 1997 to February 28, 2002. A total o 154 patients, seven
emale and
147 male (age range, 1725 years; mean, 19.6 years) meeting the
inclu-sion criteria were identified rom the MRI archives o the
Central MilitaryHospital. Te inclusion criteria or the present
study were exercise-inducedanterior lower leg pain during military
service, at least one negative plainradiograph taken at a primary
health care unit, physical examinationbyan orthopaedic surgeon,
diagnosis o injury still unclear, and one MR im-age taken at the
Central Military Hospital. Patients with a recent traumaor
presentingsymptoms on arrival at their military service were
excludedrom the study.Te patients came rom different units and
represented thegeneral conscript population o the Finnish Deense
Forces with no spe-cific eatures. Te mean population at risk per
year during the study periodconsisted o 14,640 conscripts within
the service area o the hospital.
Studies IV and V
During the study periods o twenty years, rom January 1, 1975 to
Decem-ber 31, 1994 (IV) and twenty-one years, rom January 1, 1970
to Decem-ber 31, 1990 (V), a total o twenty-one consecutive
displaced (IV) and 106non-displaced (V) emoral neck atigue ractures
were treated in militaryconscripts within the catchment area o
concern in the present study. Iden-
tification o the ractures was perormed by running a computer
searchon the National Hospital Discharge Register, using the
appropriate diag-nostic codes o the 8th (1969-86) and the 9th
(1987-1995) editions o theInternational Classification o Disease
(ICD), and by linking them with thecodes o the military hospitals
nationwide. During the study periods, inStudy IV, on average 34,723
males, and in Study V, on average 36,606 malesstarted their
military service annually, constituting the populations at riskor
sustaining a stress racture o the emoral neck. At the beginning o
themilitary service, the majority o the conscripts were 19 to 20
years old in
both studies.
-
8/13/2019 Fatigue Fx Military Conscripts
31/73
31
4.2. Methods
4.2.1. Study description
Study I
In this study, the effect o serum 25OHD concentration on atigue
bonestress injuries was evaluated. For this purpose, serum samples
were gath-ered rom all participants o the study at the beginning o
their militaryservice. Te samples were rozen or later analysis
perormed with OCEIAenzyme immunoassay by IDS (Immunodiagnostic
Systems Inc, Foun-tain Hills, AZ, USA). Computer-based data on
conscript height, weightand physical fitness obtained during the
first weeks o their service werecollected. Physical fitness was
assessed using a 12-min running test and
five measures o muscle strength. Te conscripts were ollowed or
threemonths to identiy possible stress injuries to bone. All the
patients whoby clinical examination and anamnesis were suspected to
have developeda bone stress injury during the said period underwent
plain radiographicimaging, and those whose symptoms continued and
radiographs remainednegative urther underwent MR imaging. Te
subjects without stress rac-tures under observance constituted
controls or the stress racture cases.
Study II
In this study, serum RACP-5b concentrations were measured to
deter-mine whether they can be used to identiy enhanced bone
remodeling re-lated to bone stress ractures. Te baseline blood
samples or determiningRACP-5b levels were drawn rom all subjects o
the study at their arrivalto military service. Tese subjects were
then ollowed or three months toidentiy possible occurrence o stress
ractures. Te subjects with symp-toms suggestive o bone stress
injury were clinically examined, and, later,the diagnosis was
confirmed by plain radiography, subsequently repeatedi necessary.
From the patients with diagnosed or strongly suspected
stressracture, our additional blood samples were drawn at 3-4-day
intervals to
measure RACP-5b activity. Blood was also drawn rom two
non-symp-tomatic controls with matching BMIs or each racture case.
Te analysiso serum samples rom patients with a confirmed stress
racture togetherwith corresponding samples rom controls was
subcontracted to SuomenBioanalytiikka Oy (SBA sciences, Oulu,
Finland), and conducted by usingan immunoassay protocol described
by Alatalo et al. (Alatalo et al. 2000)
Study III
In this study, the original medical records and MR images o the
conscripts
who underwent MRI or unclear stress-related anterior lower leg
pain wereretrospectively obtained and evaluated. Te MR images were
interpreted
-
8/13/2019 Fatigue Fx Military Conscripts
32/73
32
with the aim to determine the incidence, anatomic location and
grade othe possible stress injury involved. Te normal procedure
among the or-thopaedic surgeons at the Central Military Hospital
was to prescribe MRIor cases with prolonged stress-related lower
leg pain when no other, cleardiagnosis was known.
Studies IV and V
Inormation retrieved rom the medical records and imaging
examinationsconcerning the military service period o the subjects
was evaluated, and thelong-term outcome data o the subjects was
collected by asking all the pa-tients in the studies (IV, V) to
participate in a ollow-up examination. imerom the initial injury to
ollow-up examination varied between eight andthirty-two years. In
Study IV, o the 21 patients with a diagnosed displacedemoral neck
atigue racture, long-term ollow-up data was available on
19 patients. In Study V, 66 o 106 patients invited agreed to
participate inthe ollow-up. Moreover, in connection with the
long-term ollow-up visit,inormation regarding possible examinations
and treatments perormed inother hospitals afer patients previous
visits to the military hospital wereasked, and the medical records
and radiographs rom those hospitals wereretrieved or review and
analysis. Fracture patterns were determined ac-cording to Garden
and Orthopaedic rauma Association classifications(Garden 1961,
Muller et al. 1990, Orthopaedic rauma Association Com-mittee or
Coding and Classification 1996). Te body mass index (BMI) atthe
time the racture was detected was computed (World Health
Organiza-tion 1995)and classified according to Llwellyn-Jones and
Abraham clas-sification (Llwellyn-Jones and Abraham 1984). Te BMIs
o the patientsin the study were compared with those o 223
conscripts born in 1958and serving their time o compulsory military
service in 1978 (Dahlstrm1981).
Te impact o the new instructions implemented in the army
nation-wide in 1986, designed to increase awareness o the diagnosis
and treat-ment o atigue ractures, was assessed by calculating the
incidence o allatigue ractures o the emoral neck as well as the
incidences o displaced
and non-displaced emoral neck atigue ractures beore and afer
1986within the time periods o the studies.
Te ollow-up visit consisted o a physical examination, including
esti-mation o the unctional status o the hip joint using the Harris
Hip Score(Harris 1969), conventional anteroposterior radiography,
and MRI o thepelvic area. A ten-point (0 to 100 mm) visual analogue
scale (VAS), withzero denoting none, rom 10 to 30 light, rom 40 to
60 moderate, rom 60to 90 hard, and 100 denoting the worst
imaginable pain, was used to assessthe degree o subjective pain
experienced by the patients one week beore
the ollow-up examination.
-
8/13/2019 Fatigue Fx Military Conscripts
33/73
33
4.2.2. Clinical diagnosis and treatment
In Studies I-III, the physical examinations conducted at
patients primaryhealth care units adhered to identical care
policies, including careul his-tory taking, inspection o skin
changes, and palpation. In addition, the or-thopaedic examination
(III-V) included observation o joint movements
and ligamentous stability o the lower extremities as well as
checking ordistal pulse and sensation. Each unit participating in
the studies ollowedidentical procedures or diagnosis, treatment,
and patient reerral or addi-tional examinations. Beore orthopaedic
evaluation, patients were treatedconservatively, as necessitated by
pain, with rest periods or reduced exer-cise, NSAID, and prescribed
crutches i walking caused pain.
4.2.3. Imaging methods
In all studies, the same accepted radiological assessment
procedure was
adhered to during the plain radiographic examinations at both
the primaryhealth care units and the Central Military Hospital
(Kiuru et al. 2004). Tegrey cortex sign, periosteal callus,
endosteal callus, sclerotic band, andracture line were accepted as
the radiographic signs marking a bone stressinjury. In Study III,
based on MRI, bone stress injuries were classified as:Grade I,
endosteal marrow edema; Grade II, periosteal edema and end-osteal
marrow edema; Grade III, muscle edema, periosteal edema,
andendosteal marrow edema; Grade IV, racture line; and Grade V,
callus incortical bone (Kiuru et al. 2001). In Study IV, in the
radiographic classifi-cation o osteonecrosis o the emoral head, the
method o Ficat and Arlet(Ficat and Arlet 1980) was used, and in
Studies IV and V, the radiographicseverity o osteoarthritis was
classified according to the criteria o nnis(nnis 1987). In study V,
MRI was used in the detection o osteonecrosiso the emoral head and
osteoarthrotic changes o the hip joint. Both hipjoint spaces were
measured rom the original digital MR imaging data andstatistically
compared with each other in each patient. Moreover, in Stud-ies IV
and V, the original diagnoses o the stress ractures were
thoroughlychecked and verified at the ollow-up examination by means
o evaluatingthe whole series o radiographic images or each patient.
All the images
were evaluated by a musculoskeletal radiologist.
4.2.4. Statistical methods
Te data analyses or all studies (I-V) were perormed using SPSS
or Win-dows (versions 11.0/11.5/12.0/12.0.1, SPSS Inc, Chicago,
Illinois, USA). InStudy II, logistic regression analysis was
perormed using Stata or Win-dows (version 7.0). Te limit or
statistical significance was set at a P-valueequal to 0.05. Various
methods were used or statistical analysis in the di-erent
studies.
-
8/13/2019 Fatigue Fx Military Conscripts
34/73
34
In Study I, the differences in serum 25OHD levels between the
twogroups ormed by dividing the skew continuous data based on the
me-dian were tested by the Pearson chi-square test, and the results
were cor-roborated by the Mann-Whitneys U-test using the original
values. TeStudents t-test was used to test differences in age, BMI,
height, weight,
muscle strength, and result o 12-min running test between the
groups.Te association between these variables and stress racture
was studied us-ing logistic regression. Odds ratios were calculated
with a 95% confidenceinterval.
In Study II, the relationship between RACP-5b activity and an
out-come o being a case or a control was estimated using
conditional logis-tic regression. Sensitivity and specificity were
investigated using area un-der the ROC curve with confidence
interval and coordinate points o theROC curve. Because the values
were not normally distributed, logarithmic
transormations were used to analyze changes in RACP-5b activity.
estswere perormed using analysis o variance or repeated
measures.
In study III, the relationship between the locations o tibial
stress in-juries and their MRI grades was tested using the Fishers
test. Differencesbetween the groups were tested using the
Kruskal-Wallis test or skew con-tinuous data.
In Studies IV and V, the Chi-square test was used to determine
the sig-nificance o differences between two independent groups at
the 0.05 P-level. Te Students t-test and the Mann-Whitney exact
U-test were usedor comparing independent means. Incidence rate
ratios with 95% confi-dence intervals were calculated or the
ractures occurring in 1975-86 and1987-1994 in Study IV, and or the
ractures occurring in 1970-1985 and1986-1990 in Study V,
correspondingly.
Te Least Significant Difference (LSD) test in Study II and the
Mann-Whitney U test in Study III were used as post-hoc tests or
additional in-ormation.
-
8/13/2019 Fatigue Fx Military Conscripts
35/73
35
5 RESULTS
5.1. Serum 25OHD concentration as a potential
predisposing factor for fatigue bone stress fracture,
incidence and anatomic distribution of these fractures,
and their relationship with age, weight, height, BMI,
muscle strength, and result of running test. (I)
Te median serum 25OHD level was 75.8 nmol/l (25.2-259.0) or all
theconscripts in Study I, but it was significantly lower in
conscripts with stressracture than in controls (p = 0.017). In the
multivariate regression model,the conscripts with serum 25OHD
levels below the median were at 3.6(95% CI: 1.2-11.1) times higher
risk or stress racture than conscripts withconcentrations above the
median level, a difference ound statistically sig-nificant (p =
0.002) (able 5).
In Study I, conscripts results in the 12-min running test and in
the mus-cle strength test were significantly poorer compared with
controls (mean2480 m vs. 2670 m, p = 0.007; and mean 7 vs. 9, p =
0.025, respectively).However, in the multivariate regression model,
when all significant varia-bles rom the univariate observation were
adjusted, a non-significant asso-ciation emerged with stress
ractures. No significant associations betweendaily smoking, BMI,
age, height, and weight and bone stress racture wereound in this
study population.
In this study, the incidence o stress ractures was 11.6 (95%
confidenceinterval 6.8-16.5) per 100 person-years (2.9%). A total o
thirty stress rac-tures were diagnosed in the twenty-two patients o
this study. Tirteen
ractures (43%) were located in the tibia, ten (33%) in the
metatarsal bones,three (10%) in the calcaneus, two (7%) in the
tarsal navicular bone, oneracture in the inerior ramus, and one in
the emur.
-
8/13/2019 Fatigue Fx Military Conscripts
36/73
36
Table 5. Te characteristics o the study population by stress
racture status.
VariableStress fracture group
(n=22)
Control group
(n=734)
Significance
(Test)
Median (Range)
Concentration of 25OHD,nmol/l
64.3 (40.1-159.0) 76.2 (25.2-259.0) 0.017 (M-W)
Number (Frequency)
25OHD (nmol/l)
< median
median (75.8 nmol/l)
Missing N
18 (81.8%)
4 (18.2%)
0
362 (49.3%)
372 (50.7%)
0
0.002 (P)
Daily smoking
Yes
No
missing
7 (36.8)
12 (63.2)
3
93 (34.7)
175 (65.3)
466
0.85 (P)
Mean (Range)
Age (years)
Missing N
20.0 (18.6-22.3)
0
19.8 (18.0-28.5)
0
0.27 ()
BMI (kg*m-2)
Missing N
24.0 (15.4-37.4)
1
23.2 (16.6-39.2)
14
0.41 ()
Height (cm)
Missing N
177 (168-184)
1
179 (161-203)
14
0.15 ()
Weight (kg)
Missing N
75.3 (47.2-121.1)
1
74.3 (50.3-139.4)
13
0.70 ()
Muscle strength
Missing N
7 (0-15)
67
9 (1-15)
67
0.025 ()
Cooper test/12-minute run(m)
Missing N
2480 (1650-3200)
0
2670 (1540-3580)
49
0.007 ()
M-W:Mann-Whitney U-test
P: Pearson Chi-square test
T: Students -test
-
8/13/2019 Fatigue Fx Military Conscripts
37/73
37
5.2. TRACP-5b bone resorption marker as a potential
indicator of enhanced bone remodeling in military
conscripts with stress fractures, and the incidence and
anatomic distribution of these fractures. (II)
Te conscripts with elevated serum RACP-5b activity levels had an
eighttimes higher probability o stress racture existence than
controls whencomparing the ratio o sample IV (taken within 10-11
days afer detectiono stress racture) to baseline sample in the
racture and control groups(OR 7.95 95% CI 0.41-153.72) (able
6).
Although an increasing trend in the RACP-5b levels was ound
whencomparing the baseline samples to samples I-IV in the
conscripts o theracture group, the finding did not show statistical
significance (p = 0.072).
It is noteworthy, however, that the difference between the
baseline andsample III was statistically significant (p = 0.039)
(Fig 7).
Using a cut-off value o 1.09 or the ratio between sample IV and
base-line, both the sensitivity (0.62) and the specificity (0.65) o
RACP-5b levelas an indicator o stress racture exceeded 0.6.
Sensitivity (0.62-0.54) andspecificity (0.55-0.70) were both over
0.5 when the cut-off point varied be-tween 1.05 and 1.14. Te area
under the ROC-curve, as calculated or theratio between sample IV
and baseline, was 0.60.
Table 6.Results o comparisons o the RACP-5B activity between
racture and control
groups
Fracture group Control group Regression analysisa Area under
ROC-curve (AUC)b
n mean(sd) n mean(sd) n P OR(95%CI) AUC (95%CI) Pc
Baseline 13 3.40(0.77) 20 3.31(0.93) 33 0.780 1.12(0.51, 2.46)
0.54(0.34, 0.74) 0.726
IV 14 3.91(1.13) 28 3.65(1.13) 42 0.471 1.23(0.70, 2.18)
0.55(0.37, 0.73) 0.603
IV/Baseline 13 1.21(0.34) 20 1.09(0.19) 33 0.170
7.95(0.41,153.72) 0.60(0.38, 0.82) 0.338
a Conditional logistic regression analysis
b Te test result variable(s): Baseline and IV has at least one
tie between the positive actual state group and the negativeactual
state group. Statistics may be biased.
c Null hypothesis: true area = 0.5
-
8/13/2019 Fatigue Fx Military Conscripts
38/73
38
In this study, the prevalence o stress ractures was 2.4%. A
atigue rac-ture was detected in a total o twenty patients. Six
patients were lost to finalanalysis on account o unsuccessul serum
samples, incomplete ollow-updata, and termination o military
service caused by a long recovery timeafer stress injuries. In the
remaining ourteen patients, altogether twenty-
one stress ractures were diagnosed. welve ractures (57%) were
locatedin the tibia, six (29%) in the metatarsal bones, and three
(14%) in the cal-caneus.
Figure 7. Changes in RACP-5b activity o racture group.
Calculations were doneusing logarithmic transormation and the
values were retranserred to original scale(N=14).
5.3. Fatigue bone stress injuries associated with anterior
lower leg pain; incidence and distribution, MRI based
injury grades depending on injury location and
duration of symptoms. (III)
During the 5-year period o this study, the incidence o bone
stress injuries
requiring orthopaedic consultation and MRI among conscripts was
117per 100,000 person-years o military service. Te findings on MRI
revealed143 bone stress injuries in 86 patients (56%) o the study
population o154 patients. In 141 cases, the injury was located in
the tibia and in twocases, in the fibula. Forty-nine patients had
stress injuries bilaterally. Fourpatients had two injuries in the
same lower leg, and two patients had threeinjuries in the same
lower leg. One patient had simultaneous bone stressinjuries in the
tibia and in the fibula. In the tibia, 57% o the injuries werenoted
in the distal, 30% in the middle, and 10% in the proximal third
o
the tibial shaf, and 3% in the medial condyle. Moreover, the
findings in-cluded two legs with symptomatic osteoid osteomas,
seven with tractionperiostitis, and three with sof tissue edemas.
Other, clinically irrelevant
3
3,1
3,2
3,3
3,4
3,5
3,6
3,7
3,8
TRACP5b
Baseline I II III IV
-
8/13/2019 Fatigue Fx Military Conscripts
39/73
39
findings consisted o two non-ossiying fibromas and one healed
corticaldeect. In 53 patients, all findings on MRI were normal. O
all the 143 a-tigue stress injuries detected by MRI, 17% (24)
appeared in legs withoutany symptoms.
According to the MRI grading system that was used, 50% (71) o
the
tibial stress injuries represented grade I, 33% (47) grade II,
8% (11) gradeIII, 7% (9) grade IV, and 2% (3) grade V. Te
correlation between the loca-tions o tibial stress injuries and the
MRI grades I-V was statistically sig-nificant (p < 0.001) (able
7). Te injuries displayed higher grades in themedial condyle and
the proximal third compared to the middle and distalthirds o the
tibia. Symptom duration beore the stress injury diagnosiswas
significantly dependent on the MRI grade o the injury (p =
0.002).Patients with minor bone lesions (Grade I) on MRI had a
greater mediano symptom days compared with Grade II (p < 0.001)
and Grade IV (p =
0.040). Statistical significance was also seen in the
relationship betweenpatients symptom duration and MRI based injury
location in the tibia (p= 0.025) (able 8). Symptom duration
preceding the injury diagnosis wassignificantly shorter in the
medial condyle than in the middle (p = 0.004)and distal tibia (p =
0.006), whereas in the proximal tibia, the differencebordered
significance (p = 0.053). No changes were noted in the resultsafer
persons with more than one bone stress injury finding were
excludedrom the data.
Due to a clinical suspicion o a chronic exertional compartment
syn-drome (CECS), 44 patients (with 74 legs involved) o this study
also un-derwent an intracompartmental pressure measurement,
perormed using aslit catheter technique (Rorabeck et al. 1981, Moed
and Torderson 1993).Values o 40 mmHg or higher were considered
pathological (Whitesideset al. 1975, Hutchinson and Ireland 1994).
In these 44 patients, 11 o the39 legs were confirmed by MRI to
suffer rom bone injuries with elevatedpressure in the anterior
tibial compartment.
Table 7.Locations o tibial stress injuries and mri findings
classified as grades iv
Location MRI grade of bone stress injury Total
GI GII GIII GIV GV
Medical condyle 0 3 0 2 0 5
Proximal tibia 2 4 2 4 2 14
Middle tibia 20 18 2 2 0 42
Distal tibia 49 22 7 1 1 80
Fishers test, p value < 0.001
-
8/13/2019 Fatigue Fx Military Conscripts
40/73
40
5.4. Incidence, symptomatology, morphologiccharacteristics,
clinical course, risk factors, and long-
term outcomes of displaced and non-displaced
fatigue fractures of the femoral neck. (IV, V)
Study IV
Incidence (per service-years) o displaced emoral neck atigue
racturesduring 1975-1986, prior to the new regimen o 1986
addressing preven-tion o atigue ractures, was 5.3/100,000,
decreasing 2.3 old during1987-1994 to 2.3/100,000 (95% CI
0.11-1.31). Detection o non-displacedsymptomatic emoral neck atigue
ractures increased rom 15.5/100,000to 53.2/100,000 (95% CI
2.27-5.21) service-years, correspondingly. Tetotal incidences o the
emoral neck atigue ractures in the correspond-ing years were
20.8/100,000 and 53.2/100,000 service-years (in 1987-90no
displacements were observed), respectively, indicating a
significant 2.6old increase (95% CI 1.7-4.0). Garden-type IV
ractures decreased sig-nificantly rom 3.8 to 0/100,000 (95% CI
0-0.66) service-years between thetime-periods concerned.
Nineteen ractures were ollowed up in the study (ables 9A and
9B),including eight ractures o Garden-type III and eleven o
Garden-type IV.Assessment o the ractures using the system o the
Orthopaedic raumaAssociation revealed eighteen transcervical
(type-31B2) ractures and onesubcapital (type-31B1) racture. During
the first postoperative year, tencases showed early local
complications, but in the remaining nine cases,racture healing was
uneventul. Altogether six cases sustained delayed ornonunion o the
racture. In our cases, a repeat operation was necessaryduring the
first postoperative year.
During the subsequent long-term ollow-up, starting rom the
2nd
post-operative year, late, slowly developing complications, such
as osteonecrosiso the emoral head in six and osteoarthritis o the
hip in thirteen patients,
Table 8.Median (range) duration o symptoms in locations o MRI
findings
Location o mri finding N Duration o symptoms (days) P value*
medial condyle 5 36(23,59)^~ 0.025
proximal condyle 14 51(30, 105)^
middle tibia 42 66(16, 210)
distal tibia 80 67(2, 224)~
* Kruskal-Wallis test
Mann-Whitney u-test was used as a post-hoc test, significant or
almost significant p-values:^0.053, 0.004, ~0.006
-
8/13/2019 Fatigue Fx Military Conscripts
41/73
41
were detected among the nineteen cases (Fig 8A-E). According to
nnisclassification, we discovered our Grade 1, one Grade 2, and
eight Grade 3cases o osteoarthritis o the hip. Te correlation
between severe (nnisGrade 2 and Grade 3) hip osteoarthritis and
osteonecrosis o the emoralhead was statistically significant (p =
0.020). Revision surgery was neces-
sary in our cases due to these complications. Altogether three
patientsreceived total hip prostheses by the final ollow-up
examination.
In thirteen patients, a mean 32.7% (range 4 to 100%) shortening
o theemoral neck compared to the uninjured contralateral side was
observedat the latest radiological ollow-up examination.
Garden-type IV atigueracture emerged as a significant risk actor
both or osteonecrosis o theemoral head (p = 0.018) and or the
shortening o the emoral neck (p= 0.009). A significant association
was also noted between osteonecrosisand shortening o the emoral
neck in that the shortening was significantly
greater in patients with than without osteonecrosis (p =
0.001).
Study V
Te incidence (per service-years) o non-displaced emoral neck
atigueractures was examined separately or the period prior to and
the periodafer the new regimen o 1986 or the prevention o atigue
ractures was in-troduced. In the ormer period, 1970-1985, the
incidence was 10.2/100,000and in the latter period, 1986-1990, it
was 51.2/100,000, indicating a 5 oldincrease (p < 0.000). Te
overall incidence or the 21-year study period was19.4/100,000
service-years.
None o the non-displaced emoral neck atigue ractures
diagnosedduring the study progressed to displacement. With only one
exception, allconscripts included in the study returned to normal
duty service ollowingrecovery afer conservative treatment.
Te risk actor analysis perormed or the two studies (IV, V) ailed
toreveal any predisposing or risk actors. A significant deviation
(p = 0.013)was, however, ound between the BMIs o the contemporary
control con-scripts (born in 1958) and the conscripts with
displaced emoral neck a-tigue ractures (IV) (able 10). Measurements
o the neck-shaf angle rom
the radiographs (V) did not reveal any angles outside normal
limits (125to 135). MRI assessments o the average joint spaces in
the injured 2.05mm (SD 0.63) and uninjured 1.97 mm (SD 0.61) hips
(V), respectively,showed no significant deviations (p = 0.297).
At the final ollow-up (V), the intensity o subjective pain and
pain ex-periences was expressed by 62 patients using VAS. Te mean
score o painintensity was 5.85 mm (SD 10.48) on a scale o 100 mm.
Forty-three pa-tients were completely painless and two patients
reported pain levels be-tween 40 mm and 44 mm, correspondingly. Te
mean HHS was 97 (70
to 100). Tirty-seven (60%) patients did not report any physical
disabilityaccording to HHS, seven (11%) patients had HHS o 70 to 90
and 19 (31%)had HHS o 91 to 99.
-
8/13/2019 Fatigue Fx Military Conscripts
42/73
Table9AC
linicaldatao19patientswithdisplace
datigueractureotheemoralneck,typeoprimarytreatment,earlycomplicationsandsecondarym
easures
Casenoandyea
r
offractureonset
Age(yr)/
affectedside
Bmi*
(kg/m2)
Smoker
Durationofmilitary
serviceatonsetof
fracture(months)
Activitypreceding
fractu
re
Ongoingevent
leadingto
onsetoffracture
Fracture
type**
Primary
treatment
Early
complicationsandsec-
onda
rymeasureswithinone
year
afterprimaryoperation
1/1975
20/right
20.2
-
6
Marching
Stumbling
III/type-31B2
raction
Malunion(varusangulation)
2/1977
18/lef
19.1
+
2
Combattraining
None
IV/type-31B2
AngledplateDelay
edunionwithbrokenscrews
otheplate
3/1977
20/right
19.6
-
7
Marching
None
IV/type-31B2
DHS
Delay
edunionwithbrokenscrews
oDH
Splate
4/1977
18/lef
17.7
-
5
Marching
Stumbling
IV/type-31B2
DHS
5/1978
20/right
20.6
+
4
Marching
Stumbling
IV/type-31B2
DHS
Nonu
nion,removalohardwareand
finallymalunion
6/1979
19/lef
21.0
-
3
Running
Stumbling
IV/type-31B2
AngledplateNonu
nion,refixationwithDHS,and
bonegrafing(6mo.)
7/1981
20/right
20.1
-
4
Running
Ridinghard
onabicycle
IV/type-31B2
AngledplateDeep
inection,removalohardware
andbonegrafing(3mo.)
8/1983
19/right
20.8
+
4
Combattraining
Stumbling
IV/type-31B2
DHS
Heterotopicossification
9/1983
20/right
19.6
-
2
Marching
Slipping
IV/type-31B2
DHS
Nonu
nion,intertrochantericoste-
otomy,bonegrafing(7mo.)
10/1983
20/lef
23.5
-
3
Marching
Stumbling
IV/type-31B2
DHS
11/1983
23/lef
18.6
+
5
Marching
None
III/type-31B2
DHS
12/1983
19/right
18.9
+
1
Bicyclemarch
None
IV/type-31B1
DHS
Failur
eofixation,refixation(1mo.),
delayedunionandfinallymalunion
13/1984
20/right
16.1
+
6
Running
Applyingcarbrakes
III/type-31B2
DHS
14/1985
19/lef
20.2
+
4
Marching
Stumbling
III/type-31B2
DHS
15/1986
20/right
26.1
-
2
Marching
Stumbling
IV/type-31B2
DHS
16/1991
19/right
26.2
+
3
Marching
None
III/type-31B2
DHS
17/1993
19/right
19.3
-
2
Running
None
III/type-31B2
DHS
18/1993
20/lef
22.2
-
6
Marching
None
III/type-31B2
DHS
19/1994
27/right
24.0
-
6
Marching
None
III/type-31B2
DHS
Break
ageoDHS
Mean:
Range:
20years
18-27years
20.716.1-26.2
3.9months
2-7months
*BMI=BodyMassIndex,**GardenClassification/ClassificationSystemotheOrthopaedicra
umaAssociation,DHS=DynamicHipScrew,OA=Osteoarthritis,OFH=O
steonecrosisotheFemoralHead,
=NoEarlyComplicationsorSecondaryMeasuresWithinOneYearAferPrimaryOperation
-
8/13/2019 Fatigue Fx Military Conscripts
43/73
Table9B
Finalollow-updataonthePatients
Case
Follow-up
time
(years)
Latecomplicationsand
reoperationsmore
thanoneyearafterprimary
operation
(timeofreoperationinmon
thsafter
primaryoperation)
Radiographic
findings
Vas-score
Professionoremploymen
t
attimeoffinalfollow-up
Shorteningofthe
femoralneck
(%)*
Gradeof
osteoarthritis**
1
26
OA
10
Gr3
10
Assistantmanager
2
9
0
Gr0
NR
Lawyer
3
25
0
Gr0
0
Projector
4
26
OFHandOA,HA(231mo.)du
etoOFH
60
Gr3***
NR
Engineer
5
23
OFHandOA
100
Gr3
50
Service-man
6
22
OFHandOA
10
Gr3
13
Chieinspector
7
20
OA,HA(228mo.)duetoOA
10
Gr3***
50
Masterbuilder
8
19
OA
30
Gr1
36
Plumber
9
18
OFHandOA,HA(172mo.)du
etoOFH
100
Gr3***
55
Retired
10
19
OFHandOA
20
Gr3
NR
Engineer
11
19
OA
0
Gr1
45
Lawyer
12
20
OFHandOA,1
)vascularboneg
raf,(25mo.)dueto
OFH2)osteotomy(59mo.)duetoOFH
50
Gr3
28
Qualitysupervisor
13
22
0
Gr0
25
Sparepartssalesman
14
18
10
Gr0
0
Appraiser
15
16
OA
11
Gr2
2
Officemanager
16
11
OA
4
Gr1
0
Cook
17
9
0
Gr0
61
Farmer
18
11
0
Gr0
0
Waiter
19
8
OA
10
Gr1
0
echnicalmanager
Mean:
Range:
20years
8-26years
22.4%
0-100%
23mm
0-61mm
*Ascomparedwith
theuninjuredhip,**Accordington
nisClassification,***BeoreHA,
=NoLateComplicationsorReoperationsMoreTanOneYearAferPrimaryOperation,
HA=otalHipArthroplasty,DHS=DynamicHipScrew,NR=NotReported,OA=Osteoarth
rosis,OFH=OsteonecrosisotheFem
oralHead,VAS-score=VisualAnalogueScalescore
-
8/13/2019 Fatigue Fx Military Conscripts
44/73
44
A B
C D
-
8/13/2019 Fatigue Fx Military Conscripts
45/73
45
Figure 8A-E.
A. Case 5. A 20-year-old recruit with Garden-type IV atigue
racture o the right emoral neck 10days afer a long march.
B. Acceptable anatomical position afer open reduction and
fixation o the racture with dynamichip screw shows in ollow-up
radiograph six weeks afer the index operation. Minor signs
obeginning osteonecrosis in the medial aspect o the emoral neck can
be seen.
C. Advanced resorption o the emoral neck, varus bending, and a
still detectable racture line canbe seen three and a hal months
afer the index operation.
D. Dynamic hip screw has been removed as its supportive and
fixative unction was lost due toadvanced osteonecrosis. Because o
the condition, refixation was not possible. Malposition, astill
visible racture line, advanced emoral neck shortening and increased
osteonecrosis o theemoral head developed ourt