Embed Size (px)
Citation preview

FATTY LIVER DISEASE

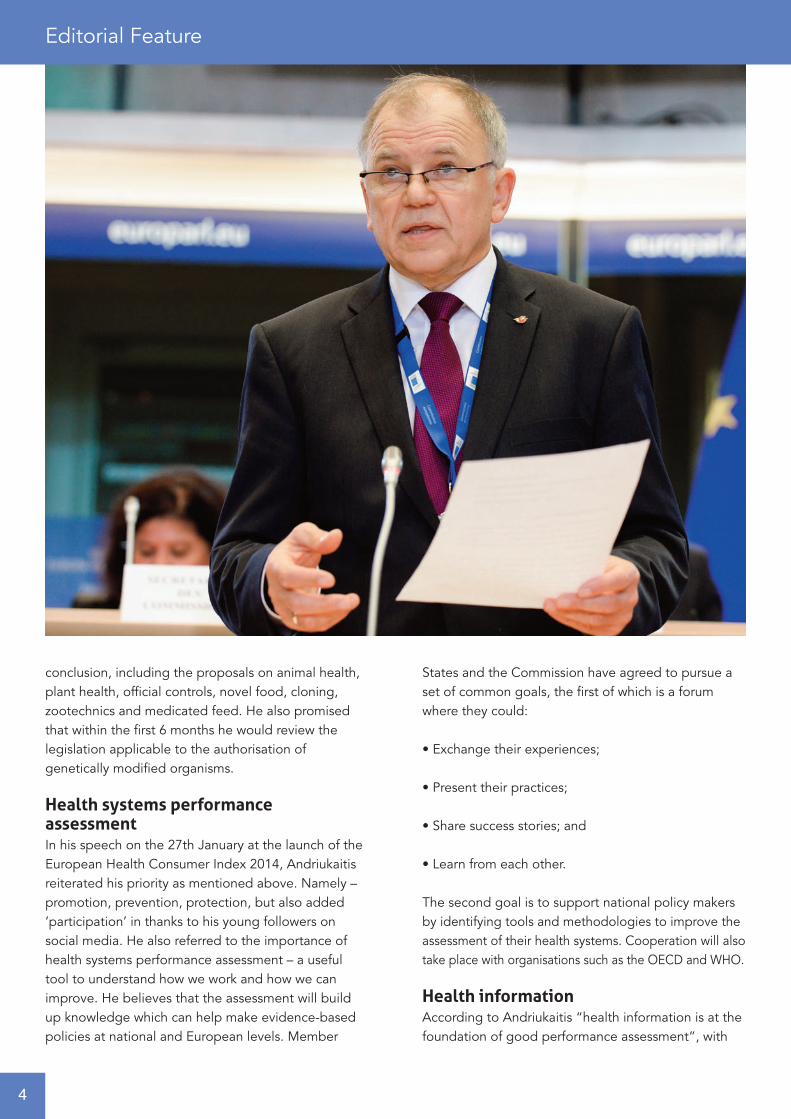
Born in 1951, Vytenis Andriukaitis holds degreesin medicine and history and started his politicalcareer just after high school. He is one of the
authors of the Lithuanian Constitution of 1992 and asignatory to the 1990 Act of the Re-Establishment ofthe State of Lithuania. Andriukaitis entered politics in1976 as an underground Social Democrat, and wasamong those who re-established the Social DemocraticParty of Lithuania in 1989. He was an active memberof the Lithuanian Reform Movement Sąjūdis, fightingagainst the Soviet, before becoming an activepolitician. He has also served as a cardiovascularsurgeon for almost 20 years.
Andriukaitis was also the Minister of Health in theRepublic of Lithuania from 2012-2014, and is currentlythe Vice-President of 67th World Health Assembly.
MEPs approved the new college of 27 Commissioners,including Andriukaitis, as presented by its President-elect Jean-Claude Juncker in October 2014, and is awelcome appointment according to The EuropeanPublic Health Alliance. Andriukaitis spoke at their
annual conference in 2014 where he said, “Health isnot a consequence of growth but also a condition forgrowth. Investments in public health increase productivityand boost job creation. Health should not only beseen as product of growth: health encourages growth.”
Emma Woodford, EPHA Interim Secretary Generalreacted to his appointment stating that, “Better attention should be paid to socio-economic determinantsof health, health promotion and prevention. Once heis confirmed as Health and Food Safety Commissionerby the European Parliament in October, he should putforward an agenda based on greater investments inhealth with a focus on social determinants.”
Andriukaitis has long held the belief that health policyhas a key role to play in economic growth, repeatingagain the sentiment that “healthy people are morecreative and productive. Their well-being sets thefoundations that moves societies forward. Health in allpolicies should be the driving force of our efforts tocut inequalities as it lays the groundwork for socialjustice and economic sustainability”.
Health in Europe: A matter of good economicsAdjacent Government details the priorities and intentions of the new European Health Commissioner, Vytenis Andriukaitis…
Editorial Feature
2
In his written answers to questions from MEPs beforehis official appointment, he provided details of whathis top priorities would be in the fields of public healthand food safety:
• With regard to past crises such as BSE and SARS,which have shown the economic value of strong healthprotection, he intends to pursue the highest standards;
• He believes we need ‘a new boost for health inEurope’ if we are to improve people’s health and boostjobs and growth. He therefore intends to “promoteinvestment in health, as an investment in Europe’shuman capital and an investment in our future”;
• The priorities surround promotion, protection andprevention. Andriukaitis intends to deliver realbenefits to citizens and support key sectors of theEU economy such as the healthcare sector – as wellas the agro-food industry;
• Against a backdrop of population ageing, a growingburden of chronic diseases and increasing demand
for healthcare, he will support efforts to make healthsystems more efficient and innovative; so that theycan provide equitable healthcare to all citizens, whileremaining financially sustainable;
• To assess the performance of health systems reformwithin the European Semester;
• To focus on enhancing prevention, as the morehealth systems invest in this field, the less they willpay for treatment in the future;
• Andriukaitis will seek to make recent EU legislationhaving an impact on the protection of public healthdeliver results to citizens. For example, to ensure thetimely adoption of secondary legislation foreseenunder the Tobacco Products Directive. He intends towork tirelessly with the Member States to ensure theDirective on patients’ rights in cross border healthcaretranslates into citizens’ better access to quality care;into in-depth co-operation on e-Health towardsbetter care; and into joint work on Health TechnologyAssessment to improve patients’ access to innovativetechnologies, business predictability and cost-effectiveness;
• Working with Member States to protect citizensagainst any cross border health threat;
• Promoting healthy and safe food as a means toprevent unnecessary spending in healthcare andhelp Member States improve the long term sustainability of their health systems;
• Endeavour to ensure high levels of animal and planthealth, providing strict controls on the safety ofimported products of both plant and animal origin;
• To work with all stakeholders to maintain andimprove food safety systems contributing toPresident Juncker’s plans for a Europe with morejobs and greater prosperity, particularly for SMEswhich make up the bulk of the food sector.
Andriukaitis made it clear that all legislative proposalscurrently under discussion with the EuropeanParliament and the Council are brought to a successful
3
conclusion, including the proposals on animal health,plant health, official controls, novel food, cloning,zootechnics and medicated feed. He also promisedthat within the first 6 months he would review thelegislation applicable to the authorisation ofgenetically modified organisms.
Health systems performance assessmentIn his speech on the 27th January at the launch of theEuropean Health Consumer Index 2014, Andriukaitisreiterated his priority as mentioned above. Namely –promotion, prevention, protection, but also added‘participation’ in thanks to his young followers onsocial media. He also referred to the importance ofhealth systems performance assessment – a usefultool to understand how we work and how we canimprove. He believes that the assessment will buildup knowledge which can help make evidence-basedpolicies at national and European levels. Member
States and the Commission have agreed to pursue aset of common goals, the first of which is a forumwhere they could:
• Exchange their experiences;
• Present their practices;
• Share success stories; and
• Learn from each other.
The second goal is to support national policy makersby identifying tools and methodologies to improve theassessment of their health systems. Cooperation will alsotake place with organisations such as the OECD and WHO.
Health informationAccording to Andriukaitis “health information is at thefoundation of good performance assessment”, with
Editorial Feature
4

the European Commission making considerable effortsto “reinforce and ensure the sustainability of actionson health information”. Data collection supported bythe Health Programmes has led to:
• Improvements of the methodology of statisticscollection;
• Development and harmonisation of health indicators; and
• The preparation of health reports.
Andriukaitis recognises that these steps don’t go farenough in themselves and wishes to ensure:
• The sustainability of data collection;
• Transparency in the development of indicators; and
• Full participation of Member States in their selection.
For Andriukaitis to realise the intentions and prioritieshe has laid out, he will need all the enthusiasm andstamina he can muster. An immediate topic at theforefront is the potential for a US free-trade dealagreement which could equate to the world’s biggesttrade deal to date. However, with no clear majorityemerging as yet, and with public opposition withinEurope apparent, Andriukaitis will have to work hardto ensure buy-in by all national parliaments. No doubtthe negotiations needed to ratify this deal wouldprovide him with an early legacy, but there is still muchto do, not just with the free-trade agreement, but onhis promises made last year.
Adjacent Governmenteditorial@adjacentgovernment.co.ukwww.adjacentgovernment.co.uk
5

Alterations in our lifestyle over the last decades,including high caloric intake (e.g. through highfructose and high fat diet) combined with a sedentarylifestyle have augmented the worldwide incidence ofoverweight and metabolic syndrome, characterisedby abdominal obesity, insulin resistance and Type-2diabetes, hypertonia and dyslipidemia. This trend isnot only observed in industrialised countries in theUS or Europe but also gradually now in developed aswell as developing countries. At the moment it isbelieved that approximately 90 million Americansand 40 million Europeans suffer from a fatty liver (also called Non-alcoholic fatty liver disease (NAFLD)).
Consequently, the price we will have to pay – from aglobal point of view – for our consequent aim toachieve progressive industrialisation and enhancedeconomic development in the 3rd world as well asdeveloping countries is the adaptation to the ‘Western’unhealthy diet and its concomitant lifestyle. It shouldalso be mentioned that particularly this development –in the long run – will lead to a huge problem asdeveloping and developed countries will contributegreatly to the number of people suffering from themetabolic syndrome and fatty liver disease. It isestimated that more than 100 million people willsuffer from fatty liver disease, the metabolic syndromeand its consequences from China and India alone.From a European point of view, a further increase ofthe metabolic syndrome as well as fatty liver diseaseis to be expected – underlining the need of therapeuticoptions to efficiently treat these patients in the next20 years.
We know today that overweight and metabolicsyndrome lead to diseases of several kinds,including coronary heart diseases, Type-2 diabetesbut also cancer (e.g. liver cancer, colorectal cancer).Epidemiological data clearly indicate that overweightand metabolic syndrome are reaching pandemicdimensions in industrialised countries – and can be
seen to a high degree in the US and in Europe. Asmentioned above, it is prospected that newly developingcountries – as a consequence of industrialisationand adaptation of their lifestyle – will also experiencea steep increase in overweight and metabolicsyndrome-triggered diseases. In the past 10 years,the rate of obesity has doubled in adults and tripledin children in the US. A similar trend has also beenobserved in Europe, and this trend will accelerateand steepen.
The liver – which is the most important metabolicorgan – is strongly affected by a chronic state ofoverweight and metabolic syndrome. Non-alcoholicfatty liver disease (NAFLD), which is the most frequentliver disease worldwide, is a clinical manifestation ofoverweight and metabolic syndrome. NAFLD is achronic disease that can last several decades,characterised by predominant macrovesicular steatosisof the liver and that can easily become more. Althoughthe prevalence of NAFLD is increasing globally,epidemiology and demographic characteristics ofNAFLD vary worldwide. It is becoming increasinglyclear that a number of pathways are involved in thepathogenesis of NASH, and its progression toadvanced stages of liver disease. These pathwaysmay be diverse in different cohorts of patients withNASH. Understanding of which pathways play a rolein the development of NASH will be critical beforelaunching treatment modalities.
A significant number of NAFLD patients developnon-alcoholic steatohepatitis (NASH), fibrosis andconsequently hepatocellular carcinoma (HCC). Inrecent years, obesity leading to metabolic syndrome,steatosis and steatohepatitis has attracted increasedattention due to an increased HCC incidence in theUS and Europe. In line, the most common etiology forHCC in industrialised countries has recently switchedfrom chronic viral infections (e.g. Hepatitis B andHepatitis C virus) to obesity, making HCC the most
Fatty Liver Diseaseand the future consequencesfor Europe
6
rapidly increasing type of cancer in the US, with asimilar trend observed in Europe. Today, we lack adetailed understanding how chronic steatosisdevelops into NASH and what factors control itstransition from NASH to HCC. At the same time notherapeutics exist to efficiently treat NASH, andtreatment options for the therapy of late stage HCCare limited and only prolong the life span of patientsbetween 3 to 6 months.
In laboratory mice, NASH can be induced by severaldifferent diets such as methionine/choline-deficientdiet (MCD) or choline-deficient diet (CD) but not byhigh fat diet (HFD) alone. However, C57BL/6 mice fedwith MCD or CD do not develop obesity or metabolicsyndrome and the diet has to be discontinued after afew months due to weight loss (up to 40%) or occasionalcachexia. Thus, these approaches do not recapitulate
NASH and its consequences (e.g. transition to HCC)in humans and appropriate mouse models forgenetically and mechanistically dissecting NAFLDinduced NASH and NASH triggered HCC developmenthave been thus far lacking.
Deficiency in the essential nutrient choline wasdescribed in NAFLD patients to exacerbate NAFLDand NASH. Moreover, humans with inadequatecholine uptake were shown to have defects in hepaticlipoprotein secretion, oxidative damage caused bymitochondrial dysfunction and ER stress.
Based on the clinical observations of cholinedeficiency to exacerbate NAFDL and NASH patients,we have recently combined choline deficiency with ahigh fat diet (CD-HFD) as a chronic diet for laboratorymice, which may lead to metabolic syndrome,
7
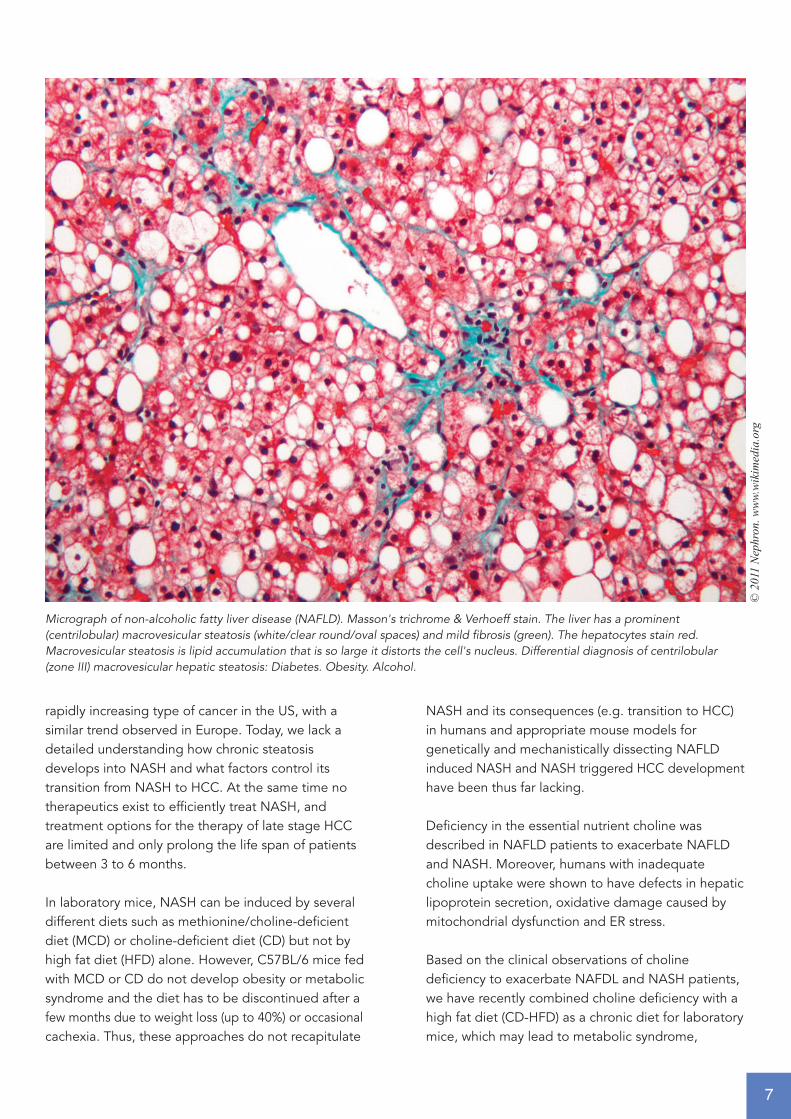
Micrograph of non-alcoholic fatty liver disease (NAFLD). Masson's trichrome & Verhoeff stain. The liver has a prominent(centrilobular) macrovesicular steatosis (white/clear round/oval spaces) and mild fibrosis (green). The hepatocytes stain red.Macrovesicular steatosis is lipid accumulation that is so large it distorts the cell's nucleus. Differential diagnosis of centrilobular(zone III) macrovesicular hepatic steatosis: Diabetes. Obesity. Alcohol.
© 2
011
Nep
hron
. ww
w.w
ikim
edia
.org
steatosis, liver damage and NASH, thus deliveringthe ‘second hit’ that promotes dietary-induced livercarcinogenesis – similar to the human situation. Thisapproach enabled us to establish a chronic mousemodel of NASH and metabolic syndrome, triggeringsubsequent HCC in a wild-type C57BL/6 mouse, inthe absence of chemical carcinogens or geneticmutations predisposing to NASH or HCC development(Wolf et al., Cancer Cell, 2014). CD-HFD treated micedisplay obesity, overweight, insulin resistance, liverdamage and fibrosis and hepatic mitochondrial damage,dyslipidemia and NASH as observed in humanpatients. HCC developed 12 months post CD-HFDstart and resembled histologically, genetically andmorphologically human HCC. Interestingly, by usingthis novel model we could investigate the cellular andmolecular mechanisms that drive NASH and NASHto HCC transition. Results of our work show thatadaptive immune cells (e.g. cytotoxic T-cells as well asNatural Killer T cells) greatly contribute to the dietinduced liver pathology and affect the degree ofliver damage as well as the degree of lipid uptake inhepatocytes, thus priming the liver to develop from afatty liver to a liver with NASH pathology. Moreover,
we could show that some of those immune cellsexpressed and secreted several inflammatory cytokinesthat appeared to be the underlying effector moleculesto drive pathology. The most prominent candidate ofall cytokines tested was a tumor necrosis factor superfamily member called LIGHT, which stands for“homologous to Lymphotoxins, Inducible expression,competes with HSV Glycoprotein D for HVEM, areceptor expressed on T-lymphocytes“. Geneticablation of this cytokine sufficed to prevent NASH aswell as NASH to HCC transition. Thus, this cytokinewould potentially represent a therapeutic target forpharmacological interventions.
Consequently, we took the next step and askedwhether our NASH mouse model would indeedreflect human pathology. Thus, we also analysedNASH patients and patients suffering from other liverdiseases with concomitant lipid deposition (e.g.Chronic HCV infection, alcoholic steatohepatitis) andcould find comparable activated immune cells inlivers of NASH patients. Moreover, we found similarcytokines expressed in the livers of NASH patientsas we had found in our mouse model to be causally
8
“Alterations in our lifestyle over thelast decades, including high caloricintake (e.g. through high fructoseand high fat diet) combined with asedentary lifestyle have augmentedthe worldwide incidence ofoverweight and metabolicsyndrome, characterised byabdominal obesity, insulinresistance and Type-2 diabetes,hypertonia and dyslipidemia.”

linked to NASH and HCC disease development.Remarkably, upregulation of LIGHT, a cytokien thatbelongs to the TNF superfamily, was highlycharacteristic for NASH when compared to other diseasesthat contain increased lipid deposition (see above).
We thus believe that our mouse model recapitulatesseveral pathophysiological aspects of human NASHand provides a mouse model enabling to study thedevelopment of NASH and NASH to HCC transition.In the future the link between activated T-cells in theliver and their crosstalk to hepatocytes could give usimportant insights in how we can generate noveltherapeutics for treating NASH as well as NASHinduced HCC in industrialised countries. Theforeseeable development of NASH into a pandemicdisease in Europe will force health authorities to act.To some extent first measures have been taken butthe wave of cases that is expected to come will notbe prevented with the current political initiatives aswell as with the current attempts to support educationand research. It will need strong political efforts tochange the thinking of our idea about living, aboutnutrition as well as about preventive measures each
individual person can take to lead a more healthylife. Moreover, research has to be strongly supportedto find – besides a European wide political strategyof prevention – therapeutic measures to prevent,to early diagnose and to treat NASH as well assubsequent diseases of NASH. The monetary effortfor such political, educational as well as researchprograms will surely be just a small proportion towhat will be needed in 20 years from now to treatpeople with established metabolic syndrome andsubsequent diseases such as NASH, cardiovascularproblems and liver caner. From my point of view theclock is ticking and unfortunately it appears as ifEuropean political decision makers rather want towait to become active until this problem is evident.This of course is the worst case scenario but it wouldnot be the first time that only if a severe problem ispresent measures will be taken. This is what clinicianswould call therapeutic approach. I propose a preventiveand therapeutic approach: Support research and findnovel drugs to treat the present disease but combineit with preventive measures (e.g. workout) in thoseindividuals who are at high risk to develop metabolicsyndrome, NASH and liver cancer.
References:
Wolf MJ, Adili A, Piotrowitz K, Abdullah Z, Boege Y, Stemmer K, Ringelhan
M, Simonavicius N, Egger M, Wohlleber D, Lorentzen A, Einer C, Schulz S,
Clavel T, Protzer U, Thiele C, Zischka H, Moch H, Tschöp M, Tumanov AV,
Haller D, Unger K, Karin M, Kopf M, Knolle P, Weber A, Heikenwalder M.
Metabolic activation of intrahepatic CD8+ T cells and NKT cells causes
nonalcoholic steatohepatitis and liver cancer via cross-talk with hepatocytes.
Cancer Cell. 2014 Oct 13;26(4):549-64. doi: 10.1016/j.ccell.2014.09.003
9
Mathias Heikenwalder Institute of Virology, Technische Universität München,
Schneckenburgerstr. 8, 81675 München
Institute of Virology, Helmholtz Zentrum München,
German Research Center for Environmental Health (GmbH),
Institute of Virology, Ingolstädter Landstraße 1, 85764
Neuherberg, Germany
E-mail: [email protected]
Tel: +49 89 4140 7440
Fax: +49 89 4140 7444
Homepage: http://www.virologie.med.tu-muenchen.de