Embed Size (px)
Citation preview

FCRIIIa Receptor Polymorphisms Do Not Influence the Outcome of Treatment
with Rituximab Followed by ActiveImmunotherapy with Mitumprotimut-T
David G. Maloney, Barbara Pender, Erin McCarthy, and Daniel P. Gold
Presented December 10, 2007, at the 49th ASH Annual Meeting in Atlanta, Georgia

FCRIIIa Receptor Polymorphisms Do Not Influence the Outcome of Treatment with Rituximab Followed by
Active Immunotherapy with Mitumprotimut-T
• Patient specific active idiotype immunotherapy with immunoglobulin idiotype is a promising new therapy for follicular non-Hodgkin's Lymphoma (NHL).
• Response to therapy may include both humoral and cellular anti-idiotypic immunity, but it is not clear which is most important.
Background
Maloney DG et al. Abstract #3416. Presented December 10, 2007, at the 49th ASH Annual Meeting in Atlanta, Georgia.

FCRIIIa Receptor Polymorphisms Do Not Influence the Outcome of Treatment with Rituximab Followed by
Active Immunotherapy with Mitumprotimut-T
• Prior studies have suggested that immunoglobulin FCgammaRIIIa (FCRIIIa ) polymorphisms at position 158 valine (V) or phenylalanine (F) affect the response to treatment with rituximab as well as outcomes from idiotype immunotherapy following objective response to chemotherapy.
Background
Maloney DG et al. Abstract #3416. Presented December 10, 2007, at the 49th ASH Annual Meeting in Atlanta, Georgia.

FCRIIIa Receptor Polymorphisms Do Not Influence the Outcome of Treatment with Rituximab Followed by
Active Immunotherapy with Mitumprotimut-T
Polymorphisms in FCgRIIIA (CD16) Influence PFS following Single Agent Rituximab• CD16 Amino Acid 158 encodes valine (V) or phenylalanine (F)
- V/V phenotype associated with higher affinity interaction with human IgG1
- F/F phenotype associated with lower affinity interaction and poorer outcome to rituximab
• Initial therapy of low-tumor burden follicular NHL patients treated with rituximab 375 mg/m2 x 4 weeks (Cartron G, Blood
99:754, 2002)- Treatment of patients with relapsed follicular NHL (Weng and
Levy, JCO 21:3940, 2003)- Also observed in Waldenstrom’s but not in CLL (Treon S, ASH
2003, Farag S, Blood 103:1472, 2004)
Background: FCRIIIA
Maloney DG et al. Abstract #3416. Presented December 10, 2007, at the 49th ASH Annual Meeting in Atlanta, Georgia.

FCRIIIa Receptor Polymorphisms Do Not Influence the Outcome of Treatment with Rituximab Followed by
Active Immunotherapy with Mitumprotimut-T
• Mitumprotimut-T is a patient-specific and B-cell tumor-specific idiotype (Id) protein chemically conjugated to keyhole limpet hemocyanin (KLH), a potent non-specific immunogenic protein
• Mitumprotimut-T induces a cellular and humoral immune response to the Id protein expressed by the patient’s own tumor, leading to active immunization against the tumor while sparing normal B-cells
Background
Maloney DG et al. Abstract #3416. Presented December 10, 2007, at the 49th ASH Annual Meeting in Atlanta, Georgia.

FCRIIIa Receptor Polymorphisms Do Not Influence the Outcome of Treatment with Rituximab Followed by
Active Immunotherapy with Mitumprotimut-T
• Mitumprotimut-T is co-administered with granulocyte-macrophage colony-stimulating factor (GM-CSF) to further enhance immune anti-Id immune responses
• The Id protein is produced by proprietary recombinant technology; ~8 weeks from biopsy to final product
Background
Maloney DG et al. Abstract #3416. Presented December 10, 2007, at the 49th ASH Annual Meeting in Atlanta, Georgia.

FCRIIIa Receptor Polymorphisms Do Not Influence the Outcome of Treatment with Rituximab Followed by
Active Immunotherapy with Mitumprotimut-T
• To assess the correlation between long term progression free survival (PFS) following combined rituximab + mitumprotimut-T (Id-KLH) treatment and FCRIIIa (CD16) polymorphism expression
• To assess the correlation of FCRIIIa polymorphisms and outcomes from idiotype immunotherapy following treatment with rituximab
Objective
Maloney DG et al. Abstract #3416. Presented December 10, 2007, at the 49th ASH Annual Meeting in Atlanta, Georgia.

FCRIIIa Receptor Polymorphisms Do Not Influence the Outcome of Treatment with Rituximab Followed by
Active Immunotherapy with Mitumprotimut-T
• Key Inclusion Criteria:– Histologically confirmed Grade 1 or 2 follicular
B-cell lymphoma (WHO classification)
– Treatment-naïve, relapsed/refractory to chemotherapy, or relapsed following prior ≥ 6-month response to rituximab
– ≥8 weeks between completion of any prior lymphoma therapy and start of rituximab on study
– Measurable disease (≥2 cm) following node biopsy
– Performance status (ECOG) of 0, 1 or 2
Methods
Maloney DG et al. Abstract #3416. Presented December 10, 2007, at the 49th ASH Annual Meeting in Atlanta, Georgia.

FCRIIIa Receptor Polymorphisms Do Not Influence the Outcome of Treatment with Rituximab Followed by
Active Immunotherapy with Mitumprotimut-T
• Key Exclusion Criteria:– >3 prior chemotherapy or anti-CD20 regimens
– Prior fludarabine
– Concurrent immunosuppressive therapy (e.g., high-dose steroids)
Methods
Maloney DG et al. Abstract #3416. Presented December 10, 2007, at the 49th ASH Annual Meeting in Atlanta, Georgia.

FCRIIIa Receptor Polymorphisms Do Not Influence the Outcome of Treatment with Rituximab Followed by
Active Immunotherapy with Mitumprotimut-T
• PCR primers were designed to specifically amplify the regions of interest in FCRIIIa
• The FCRIIIa genotypes of 55 rituximab-naïve patients treated on a Phase II trial of mitumprotimut-T were determined using a SSCP method with genomic DNA
• Bands were sequenced to confirm the presence of the polymorphism
Methods
Maloney DG et al. Abstract #3416. Presented December 10, 2007, at the 49th ASH Annual Meeting in Atlanta, Georgia.

SSCP Analysis for FCRIIIa Polymorphism at position 158
Maloney DG et al. Abstract #3416. Presented December 10, 2007, at the 49th ASH Annual Meeting in Atlanta, Georgia.
H2O V/V V/F F/F V/V V/F F/F
200 bp100 bp
PCR SSCP

FCRIIIa Receptor Polymorphisms Do Not Influence the Outcome of Treatment with Rituximab Followed by
Active Immunotherapy with Mitumprotimut-T
• Rituximab: 375 mg/m2 weekly infusion x 4 weeks. Subjects with stable disease (SD) or an objective response (CR or PR) to rituximab were eligible for mitumprotimut-T
• Mitumprotimut-T: 1 mg sc on Day 1 of each course. Courses administered monthly x6, bimonthly x6, and then every 3 months until disease progression or significant toxicity
• GM-CSF: 250 mcg/day sc on Days 1-4 of each course; same injection site as mitumprotimut-T
• CT scans: Obtained every 3 months; read by an independent radiologist blinded to clinical data
• Response assessment: Central review using modified IWG response criteria (Cheson et al, J Clin Oncol 1999;17:1244-1253)
Study Schema And Treatment Regimen
Maloney DG et al. Abstract #3416. Presented December 10, 2007, at the 49th ASH Annual Meeting in Atlanta, Georgia.

Study Schema and Treatment Regimen
Maloney DG et al. Abstract #3416. Presented December 10, 2007, at the 49th ASH Annual Meeting in Atlanta, Georgia.
0 3 6 9 12 15 18 21 24Months
CT Scans
Mitumprotimut-T+ GM-CSF
Rituximab
Mitumprotimut-TProduction
Biopsy
Cytoreduction Induction Maintenance

FCRIIIa Receptor Polymorphisms Do Not Influence the Outcome of Treatment with Rituximab Followed by
Active Immunotherapy with Mitumprotimut-T
• DNA was isolated from all 55 patients and successfully analyzed by SSCP for polymorphisms at position 158 of FCRIIIa:– V/V: 9 (16%)
– 27 (49%)
– V/F 19 (35%)
Results
Maloney DG et al. Abstract #3416. Presented December 10, 2007, at the 49th ASH Annual Meeting in Atlanta, Georgia.

FCRIIIa Receptor Polymorphisms Do Not Influence the Outcome of Treatment with Rituximab Followed by
Active Immunotherapy with Mitumprotimut-T
• 95 patients received rituximab and were evaluable.• 38 Treatment-naïve (T-N) patients• 57 Relapsed/Refractory (R/R) patients
- 25 of the 57 R/R pts were rituximab-naïve- 32 of the 57 R/R pts had previously received rituximab
± chemotherapy• 6 of 95 patients were progressive disease (PD) following
rituximab and were ineligible to receive mitumprotimut-T (IdKLH)
• 89 patients received mitumprotimut-T following rituximab
Patient Enrollment:
Maloney DG et al. Abstract #3416. Presented December 10, 2007, at the 49th ASH Annual Meeting in Atlanta, Georgia.

FCRIIIa Receptor Polymorphisms Do Not Influence the Outcome of Treatment with Rituximab Followed by
Active Immunotherapy with Mitumprotimut-T
• 4 patients who progressed following rituximab and therefore did not receive mitumprotimut-T were excluded from this analysis
• All 55 patients in this analysis had follicular NHL with a median age of 55 years
• 35 patients were treatment naïve and 20 had relapsed following prior chemotherapy
Treatment
Maloney DG et al. Abstract #3416. Presented December 10, 2007, at the 49th ASH Annual Meeting in Atlanta, Georgia.

FCRIIIa Receptor Polymorphisms Do Not Influence the Outcome of Treatment with Rituximab Followed by
Active Immunotherapy with Mitumprotimut-T
• 4 patients who progressed following rituximab and therefore did not receive mitumprotimut-T were excluded from this analysis
• All 55 patients in this analysis had follicular NHL with a median age of 55 years
• 35 patients were treatment naïve and 20 had relapsed following prior chemotherapy
DNA Sample Availability
Maloney DG et al. Abstract #3416. Presented December 10, 2007, at the 49th ASH Annual Meeting in Atlanta, Georgia.

FCRIIIa Polymorphism at Position 158: Distribution Among Evaluable Subjects
T-N = treatment-naïve, R/R = relapse-refractory.Maloney DG et al. Abstract #3416. Presented December 10, 2007, at the 49th ASH Annual Meeting in Atlanta, Georgia.
Group N V/V V/F F/F
All 84 12 (14%) 34 (41%) 38 (45%)
R/R 46 7 (15%) 18 (39%) 21 (46%)
T-N 38 5 (13%) 16 (42%) 17 (45%)
Rituximab naïve 61 (38T-N, 23R/R)
10 (16%) 21 (34%) 30 (49%)
Results

FCRIIIa Receptor Polymorphisms Do Not Influence the Outcome of Treatment with Rituximab Followed by
Active Immunotherapy with Mitumprotimut-T
• The 3 month response (post rituximab) was: – V/V: 5/9 (56%)
– V/F: 9/19 (47%)
– F/F: 17/27 (63%)
• The best response was:– V/V: 6/9 (67%)
– V/F: 12/19 (63%)
– F/F: 21/27 (78%)
Results
Maloney DG et al. Abstract #3416. Presented December 10, 2007, at the 49th ASH Annual Meeting in Atlanta, Georgia.

Initial Overall Response Rate to Single Agent Rituximab Therapy, Among Rituximab-Naïve Patients According to FCRIIIa Polymorphism at Position 158
The overall response rate is equal to the incidence of complete response and partial response: ORR = CR + PR.Maloney DG et al. Abstract #3416. Presented December 10, 2007, at the 49th ASH Annual Meeting in Atlanta, Georgia.
Group N Rituximab ORR
All 61 54%
V/V 10 50%
V/F 21 52%
F/F 30 57%
Any V 31 52%
Any F 51 55%
ORR = CR+PR

Best ORR Achieved, TTP, and PFS with Combined Rituximab + Mitumprotimut-T Among Rituximab-Naïve Patients According to FCRIIIa Polymorphism at Position 158
ORR = overall response rate; TTP = time to progression; PFS = progression free survivalMaloney DG et al. Abstract #3416. Presented December 10, 2007, at the 49th ASH Annual Meeting in Atlanta, Georgia.
Group N*
Best ORR to combined rituximab+ Id-KLH treatment
Med. TTP(months) 1 Yr. PFS 4 Yr. PFS
All 57 70% 17.7 59% 30%
V/V 9 67% 19.6 55% 29%
V/F 21 62% 20.8 58% 34%
F/F 27 78% 17.7 62% 28%
Any V 30 63% 19.6 57% 33%
Any F 48 76% 17.7 60% 30%
* 4 Patients ( 3 FF & 1 VV) who were PD post rituximab did not qualify for mitumprotimut-T Id-KLH treatment and are excluded from the analysis for the combined treatment

FCRIIIa Receptor Polymorphisms Do Not Influence the Outcome of Treatment with Rituximab Followed by
Active Immunotherapy with Mitumprotimut-T
• Median TTP was:– V/V: 19.5 months
– V/F: 22.3 months
– F/F 18 months
• The PFS at 1 year post initiation of rituximab was: – V/V: 57%
– V/F: 61%
– F/F: 68%
Results
Maloney DG et al. Abstract #3416. Presented December 10, 2007, at the 49th ASH Annual Meeting in Atlanta, Georgia.

FCRIIIa Receptor Polymorphisms Do Not Influence the Outcome of Treatment with Rituximab Followed by
Active Immunotherapy with Mitumprotimut-T
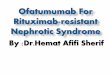
• At the median follow-up of 3.5 years the PFS was: – V/V: 31%
– V/F: 42%
– F/F: 31%
Results
Maloney DG et al. Abstract #3416. Presented December 10, 2007, at the 49th ASH Annual Meeting in Atlanta, Georgia.

PFS for V/V vs. V/F vs. F/F FCRIIIa at Position 158
Maloney DG et al. Abstract #3416. Presented December 10, 2007, at the 49th ASH Annual Meeting in Atlanta, Georgia.
0 10 20 30 40 50 600
10
20
30
40
50
60
70
80
90
100
V/F
V/V
F/F
Months
Pro
gre
ssio
n F
ree
%

PFS for V/V vs. V/F vs. F/F FCRIIIa at Position 158
Maloney DG et al. Abstract #3416. Presented December 10, 2007, at the 49th ASH Annual Meeting in Atlanta, Georgia.
0 10 20 30 40 50 600
10
20
30
40
50
60
70
80
90
100
Any F
Any V
Months
Pro
gre
ssio
n F
ree
%

Antibody Responses to KLH and Id Among Long Term (> 3 years) Progression Free Survivors* (n=13)
positive (+) negative (-)
Maloney DG et al. Abstract #3416. Presented December 10, 2007, at the 49th ASH Annual Meeting in Atlanta, Georgia.
PatientFCRIIIa
Genotype KLH Id
1 V/V + –
2 V/V + +
3 V/F + +
4 V/F + +
5 V/F + +
6 V/F + –
7 V/F + –
PatientFCRIIIa
Genotype KLH Id
8 F/F + –
9 F/F – –
10 F/F + +
11 F/F + –
12 F/F + –
13 F/F + –
*As measured by ELISA

FCRIIIa Receptor Polymorphisms Do Not Influence the Outcome of Treatment with Rituximab Followed by
Active Immunotherapy with Mitumprotimut-T
• FCRIIIa polymorphisms were not associated with response rate or time to progression following a treatment program consisting of single agent rituximab followed by idiotype vaccination with mitumprotimut-T in rituximab- naive patients
• Results from an ongoing randomized Phase III study will assess the efficacy of this combined therapy, but these data suggest that long term PFS in patients receiving an idiotype vaccine following rituximab may rely more on a cell mediated immune response rather than a humoral response to idiotype
Conclusions
Maloney DG et al. Abstract #3416. Presented December 10, 2007, at the 49th ASH Annual Meeting in Atlanta, Georgia.

FCRIIIa Receptor Polymorphisms Do Not Influence the Outcome of Treatment with Rituximab Followed by
Active Immunotherapy with Mitumprotimut-T
• The distribution of FCRIIIA polymorphisms at Position 158 in this study population is comparable to
previously published data among FL patients.
• In the population of Rituximab Naïve FL patients (23 R/R and 38 T-N), there is no correlation with
FCRIIIA polymorphisms at Position 158 and initial response to 4 course Rituximab therapy nor with
time to progression following idiotype immunotherapy with mitumprotimut-T +GM-CSF.
Summary
Maloney DG et al. Abstract #3416. Presented December 10, 2007, at the 49th ASH Annual Meeting in Atlanta, Georgia.

FCRIIIa Receptor Polymorphisms Do Not Influence the Outcome of Treatment with Rituximab Followed by
Active Immunotherapy with Mitumprotimut-T
Long term progression free survival (> 3 years) following combined Rituximab plus mitumprotimut-T (Specifid™, Id-KLH, FavId®) therapy does not correlate with production of anti-idiotypic antibody suggesting long term PFS may rely more on a cell mediated immune response.
Summary
Maloney DG et al. Abstract #3416. Presented December 10, 2007, at the 49th ASH Annual Meeting in Atlanta, Georgia.

FCRIIIa Receptor Polymorphisms Do Not Influence the Outcome of Treatment with Rituximab Followed by
Active Immunotherapy with Mitumprotimut-T
• Lack of correlation with FCRIIIA polymorphisms and long term PFS may suggest that if such an association does occur with Rituximab monotherapy, the addition of idiotype vaccine overrides the FCRIIIA advantage.
• Results from an ongoing randomized PIII study due to be reported in July 2008 will assess the efficacy of this combined therapy and any potential role for FCRIIIA polymorphisms.
Summary
Maloney DG et al. Abstract #3416. Presented December 10, 2007, at the 49th ASH Annual Meeting in Atlanta, Georgia.