Embed Size (px)
Citation preview

FOUNDATIONS II
© The Manual Therapy Institute PLLC 1998-2019

Pain Science
The understanding of pain has not changed much since the 17th century. It considers pain to be synonymous with nociception - pain is generated in the tissues of the body and the “pain message” is transmitted along “pain fibers” to the brain, which registers the pain. According to the theory, when pain persists, either the tissues remain damaged or the patient is lying, deluded, or both. It is the Cartesian Model of Pain. Recognize the theory? Of course you do. It is intuitively sensible and seems consistent with our experience. When we hit our thumb with a hammer, it is the thumb that hurts. However, the theory is wrong. It is, in fact, biologically and as an intellectual construct, indefensible.
Why then does this theory still dominate clinical practice, let alone community beliefs? One reason is that there are not enough resources where clinicians and their patients can learn about pain biology. The old theory is deliciously seductive in its simplicity- it would be great if all we had to do for a patient with chronic low back pain was to anaesthetize their back. The new theory is confronting in that it proposes that the brain is actually very clever and wonderfully complex. We need to come to terms with this new theory because as long as we stubbornly bury our clinical reasoning heads in the ground, we are failing the ones who suffer from pain, and leaves us, the clinicians, with limited options to help them. Learn how pain really works. If you don’t understand, find out more. If you still don’t understand, find out even more. And then tell your patients how pain really works.
The following chapter draws heavily from the work of Lorimer Mosely, David Butler, Adrian Louw and Emilio Puentedura. They have been on the forefront of Pain Science research, and how to best incorporate it in our daily practice.
Definition of Pain: The Grand Poobah Pain Theory as proposed by David Butler and Lorimer Mosely14
1. Pain is an unpleasant feeling that is felt somewhere in the body and urges us to protect that bodily location.2. Pain is one of many protective mechanisms. Others include movement, immune, cognitive, endocrine and autonomic.3. Pain is the only protective mechanism we are necessarily aware of and compels us to do something to protect the painful bit.4. Pain is modulated by any credible evidence that protection is warranted.
2

Neurophysiology of acute pain
When there is tissue damage, the action potential is transmitted to the dorsal horn. The fast, myelinated A fibers and the slow, unmyelinated C fibers are responsible for the transport of the nociceptive stimulus. The message that is sent to the spinal cord only says “danger”. It does not say “pain.” The spinal cord and the brain have to receive and analyze these inputs and create meaningful experiences, which may or may not include pain.
The dorsal horn is the main location where pain is modulated. This determines if the danger signal will be transferred to the higher centers in the CNS for interpretation. This modulation is known as the gate control theory. The opening or closing of the gate is determined by the nature and intensity of the danger signal, as well as activity in the descending, pain inhibiting neural pathways of the CNS. The gate control theory makes clear that the brain plays an important role in the acute stage of pain.
The nervous system is highly adaptable and will accommodate most demands it is given. So when impulses from inflamed, scarred, weak or acidic tissues keep arriving at the dorsal horn synapses, or when neurons from the brain release excitatory chemicals, the neuron in the spinal cord adapts to meet the demand- that is to get better at sending danger messages up to the brain. This adaptation begins within seconds of the demand increasing. In the short term, the danger message neuron increases its sensitivity to the incoming excitatory chemicals. This leads to hyperalgesia, things that used to hurt, now hurt more. It also means that things that didn’t hurt before now hurt (allodynia). Hyperalgesia and allodynia just mean increased sensitivity.
The sensors then change the way they work so that they stay open longer each time they are opened. There is also an increase in sensors for excitatory chemicals, including sensors that are inactive until they are needed. All of these things increase the sensitivity of the danger messenger neuron.
Different parts of the brain are involved in the processing of incoming pain signals. There is not just one pain center in the brain, as we used to think. There are many, and those areas are called “ignition nodes.” These brain parts include clusters of nodes used for sensation, movement, emotions and memory. Pain just borrows these parts to express itself. In chronic pain, some of these nodes are hijacked or enslaved by the pain experience. The particular pattern of activity in the brain, which creates the perception of pain, can be considered a “neurotag” for pain. This means that in every person there is a certain built-in matrix of neurons that get activated and ultimately produce pain when the brain decides that this is indicated. This neuronal network is genetically determined and is influenced through life by experience, stress, cognitive processes and sensory input.
The nervous system adaptively changes with both acute and chronic pain. In acute pain, more nociceptors are added and there is increased responsiveness of the nociceptive receptors. This process is called primary hyperalgesia, or peripheral sensitization. This is a local phenomenon. It is a protective action by the body to prevent further use and further damage of the injured tissue. It is part of the normal physiological process that happens when tissue is damaged.
3

Secondary hyperalgesia refers to the adaptations made in the central nervous system. There is increased responsiveness of dorsal horn neurons (the primary source of nociception) to stimuli from the periphery. The secondary hyperalgesia causes increased stimulus-response relation in all the tissues innervated by the involved segment. This means you can feel pain in areas other than where the primary tissue damage took place.
The neurophysiology of chronic pain
When does the brain decide if there is pain, or not?You will have pain when the brain concludes there is more credible evidence of danger related to your body than there is credible evidence of safety related to your body.
Credible evidence of danger: Hearing that “there is nothing wrong with you so your pain is probably not real” Believing you might end up in a wheelchair Receiving a diagnosis that sounds bad without knowing what it really means Going to the same place where you first injured your body
Credible evidence of safety Being aware of a scientifically proven path to recovery Making an appointment to see a good health professional Knowing that your are not the only person to be in this situation Having a local anaesthetic that blocks danger messages being sent to your spinal cord and
brain Loving support
Moseley and Butler coined these DIMs (Danger In Me Neurotags) and SIMs (Safety In Me Neurotags). The more DIMs, the bigger the chance you will be in pain. The more SIMs, the bigger the chance you will have no pain.
4

’From: Moseley GL, Butler DS. The Explain Pain Handbook Protectometer. Adelaide, Australia: Noigroup Publications 2015
In conjunction with this, they developed a so-called “Protectometer”. It indicates the overall level of danger or safety in you. The indicator on the Protectometer will move up and down in response to any evidence of danger or safety in your life.
From: Moseley GL, Butler DS. The Explain Pain Handbook Protectometer. Adelaide, Australia: Noigroup Publications 2015
5

The number and strength of your DIMs and SIMs determine the level of the indicator on your Protectometer. If DIMs are added, it will go up, if SIMs are added it will go down. At a certain level on the Protectometer your brain will start to make pain in order to protect you.
Keep in mind that thoughts can fundamentally alter our pain - powerful stuff – it’s just about as far away from the out of date notions of ‘pain receptors’ and ‘pain pathways’, as you can get. Like pain, you can’t see a thought, but we know that both pain and thoughts are real and involve complex neuroimmune interactions. If a person says “it hurts”, then no one can say it doesn’t - there is only one witness to the event.
Butler and Mosely introduced the notion of ‘thought viruses’ to people experiencing pain. The idea of thought viruses fits perfectly within the paradigm of DIMs (Danger In Me neurotags), SIMs (Safety In Me neurotags) and the Protectometer.
Thought viruses can be powerful DIMs – and likely to be found across the seven categories, for example: - Things You Hear, See, Smell, Taste and Touch - hearing “you have the back of an 80 year old” or seeing normal age-related changes on x-ray (that remain unexplained and threatening)- Things you think and believe – “movement is dangerous” or “pain is forever”Things you do can be influenced by Thought Viruses - “I am not bending forwards” is a logical consequence of the thoughts and beliefs. Thought viruses might be picked up from the People in your Life or the Places you go.They also have a real biological effect on the Things happening in your body such as inflammation.Things you Say - “I am riddled with arthritis”. So be careful how you communicate with your patients. Words matter!
From: Explain Pain Supercharged. Mosely and Butler 2017
6

The immune system and pain
The immune system is designed to protect you against dangers, such as infections. However, it has been shown that the immune system also becomes involved when people experience pain. When pain persists, the immune system is obliged to become activated and investigate. In chronic pain, chemicals associated with stress can directly activate nociception pathways.
The basic stress response is the flight or fight response. The body reacts to stress with various systems:
Adrenaline: the fast acting neurotransmitter, very effective in the immediate stress response, which should last no longer than several minutes. Affects just about all tissue in the body. Causes hypervigilance.
Muscles: in an immediate threat response, large muscles are needed to fight or run away. Small muscles (postural muscles or stabilizing muscles) are not needed. Deactivating these muscles in response to threat seems prudent.
GI system: digestion of food is slowed down or even put on hold, allowing for all possible energy and blood flow to be allocated to the immediate system.
Once the threat/stress has been dealt with, all this should be dialed back to normal. It is designed to elevate and then calm down, not continue to run at elevated levels for prolonged periods. It is believed that psychosocial yellow flags will result in a stress response. Clinically the patient may experience pain due to stress, anxiety or fear, not just injured or damaged tissue. This pain response may explain increased pain with high stress scenarios such as surgery, litigation, or whiplash injuries. In chronic pain, the stress response is protracted. If the stressors and yellow flags remain in place for months or years, the resultant chemical activation will have significant repercussions for the nervous system, tissues, and brain. The stress response is initially executed by adrenaline, followed by cortisol changes in the body.
Cortisol is a more potent and longer lasting chemical, similar in effect to adrenaline, but produced to deal with longer lasting threats. It is a hormone produced by the adrenal gland and more formally known as hydrocortisone. Its primary function is to increase blood sugar, suppress the immune system and aid in fat, protein and carbohydrate metabolism. Cortisol prevents the release of substances in the body that cause inflammation. That is why it is used to treat inflammatory conditions, rheumatologic diseases, and allergies. Low strength hydrocortisone is used to treat skin problems like rashes and eczema. Prolonged elevated levels of cortisol can lead to muscle wasting, fatigue, high blood pressure, worsening memory, difficulty sleeping, erectile dysfunction, weight gain, weakened immune response and muscle wasting.
High levels of cortisol also increase the manufacture of cytokines. Cytokines are immune molecules, which impact tissue healing significantly. During infections, trauma, or injury, cytokines increase 1000 fold, allowing for more ion channels specific to cytokines to open up. This potentially leads to increased sensitivity and is thought to be the reason for the allover body aches you experience when having the flu.
7

Recent studies have also shown increased levels of cytokines close to the nerve roots in patients with lumbar disc herniation. High levels of cytokines, but not disc degeneration, were associated with less favorable recovery in patients with lumbar radiculopathy.In summary, elevated levels of cortisol lead to elevated levels of cytokines, which can cause a systemic inflammatory state, including keeping the tissues inflamed and swollen for long periods of time
As a result, the nervous system will increase its sensitivity from a normal resting level to extra sensitive to protect the patient. This increase in sensitivity is driven by the increased manufacture of ion channels
Ion channels are the gateway between the “outside” and the “inside” of the nerve. Ion channels are proteins, clumped together to form a passage in the membrane of the nerve that allows ions to move in or out.
From: Louw A, Puentedura E. Therapeutic Neuroscience Education, teaching patients about pain. Minneapolis, MN: OPTP; 2013
For this passage to take place, they need to be placed in the membrane of an axon. The myelin sheath however, forms a natural barrier. Therefore, ion channels are found in higher concentrations in areas where there is less myelin: dorsal root ganglion, nodes of Ranvier and wherever myelin has been stripped from the axon
From: Louw A, Puentedura E. Therapeutic Neuroscience Education, teaching patients about pain. Minneapolis, MN: OPTP; 2013
8

The opening or closing of the channels is governed by various signals (temperature, light, inflammation, mechanical, chemical etc). When facing a specific threat, ion channels, acting as sensors, will be needed for that threat. Increased expression of a certain type of ion channel may result in a patient developing sensitivity to the stimulus known to activate the ion channel, e.g. adrenaline channels opening due to high levels of stress or anxiety.
For example, it is now well established that following an MVA, patients develop an immediate hypersensitivity of the nervous system. Given the high levels of stress and anxiety in and around an MVA, higher numbers of movement sensitive ion channels may be produced. This causes widespread sensitization of movement of the nervous system after the accident. This increase of mechanosensitive ion channels in response to the threat of movement in the face of high levels of pain may well explain why a patient with whiplash type injury demonstrates increased sensitivity and decreased mobility with the ULTT and Slump test. Nerves adapt to chronic pain levels by making more ion channels, and those ion channels stay open longer.
Whenever the myelin sheath is stripped from the axon, ion channels will insert in the newly exposed axolemma. Myelin is somewhat fragile and can be stripped from a nerve by:
Mechanical force. Injuries as an inversion sprain, can actually strip the myelin of the nerve
Immune processes Chemical. Inflammatory substances may dissolve the myelin. This has been shown in
disc herniation where chemicals released by the disc denervated the adjacent axon.
The demyelination of axons and resultant upregulation of ion channels into the bare axolemma can help clinicians explain some of the pain patients experience after injury or surgery.
SmudgingAll body parts are represented in the brain, primarily within the somatosensory homunculus. The SSH resembles a person. When you regularly use a body part, and when you have little to no pain, the map gets exercised and the bodypart stays healthy, crisp and in focus. Because of this exercise and focus, it is easy to use the body parts as well as determine left from right. When pain prevents somebody from moving, and thus exercising these body maps, the body part becomes a little blurred. The longer the pain persists, the more advanced the changes in the brain become. This is thought to be a defense mechanism of the brain, it basically “looks out” for you, by making the body part difficult to use. It has been shown that apart from “use it or lose it” over activity of your immune system is also a major cause of smudging. Issues like stress, pain, fear, failed treatments etc increase stress chemicals, which in turn activate immune molecules, causing increased smudging.
The more a body part is out of focus, the more pain is present. Even though a body part may not be longer present (amputation) pain may be felt in the missing body part because that pain is still present within the brain. Patients with chronic pain have distorted views of body parts and these views are strongly correlated to pain.
9

Due to pain, the affected body part is not used as much and using the body part is essential to keep the body map healthy and sharply focused. Movement is therefore a key component in recovery. Understanding that these maps are “fed” by movement should help you understand that movement is essential and exercise, even though is seemingly mundane and boring, help keeps the map healthy and directly decreases pain.
From: Louw A, Puentedura E. Therapeutic Neuroscience Education, teaching patients about pain. Minneapolis, MN: OPTP; 2013
10

Psychosocial Risk Factors – the Yellow Flags9
The stress response system is designed to elevate temporarily and then calm down again. It is not designed to run at elevated levels for prolonged periods. What happens then? What about the constant stress patients experience, associated with issues as pain, fear, anxiety, worries about work and money, failed treatments and different explanations for their pain?
Yellow flags are psychosocial risk factors that contribute to the development of chronic back pain and disability. It is important to understand how psychosocial factors can affect illness behavior, chronic pain, and disability. The current consensus is that psychosocial issues rarely cause acute pain, but are more important than physical features in determining which patients proceed on to chronicity and which patients can be helped. It is suggested to screen early.
There are many yellow flags; listed here are a few of the most common ones: Patient believes that LBP is harmful and disabling Decreased activity levels and fear avoidance behavior Tendency to low mood and withdrawal from social activity Expectation of passive treatment Working more than one job Working overtime on a regular basis Job dissatisfaction Sickness benefits Compensation/litigation
When you are injured, the environment that you are in will have an effect on the amount of pain you experience.The environmental influences in which the injury occurs can either be positive (lessening the pain experience) or negative (increasing the pain experience)Positive: kids that play contact sports early in life are likely to have a lower chance of developing chronic pain. Demolition derby drivers have >1500 collisions in their career, yet <10% develop chronic neck pain. In comparison, 33% of people involved in MVA’s will develop chronic pain.Negative: Injuries that occur in high stress environments (MVA’s, injury at a stressful job etc.) are 7-8 times more likely to result in chronic pain
Central sensitization
Central sensitization is the hallmark of chronic pain. Central sensitization is defined as an augmentation of responsiveness of central neurons to input from receptors. In contrast to peripheral sensitization that happens with acute pain, central sensitization requires functional changes in the CNS. This neural plasticity is responsible for the fact that the neurophysiologic mechanisms in chronic pain are very different from the mechanisms in acute pain. Central sensitization encompasses altered sensory processing in the brain, malfunctioning of descending anti-nociceptive mechanisms and/or increased activity of pain facilitatory pathways. At a spinal cord level, floods of sensitivity enhancing chemicals can swamp the synapse, and some of the incoming neurons can go sprouting. For example, neurons that don’t even carry danger messages sprout in close to the danger messenger neuron that the chemicals that release activate that
11

neuron. This means that just touching the skin, or a slight change in temperature, might cause danger messages to be sent to the brain. In a way, your brain is being tricked. It is operating on faulty information about the condition of your tissues.
Central sensitization is also characterized by temporal summation of second pain (or wind up) where more input further sensitizes the system. Be aware of this phenomenon when applying joint or soft tissue mobilizations, as it is very easy to increase the patient’s pain with even lower grade mobilizations or soft tissue techniques.
The amount of pain experienced by the patient does not necessarily relate to the amount of tissue damage sustained. What happens in the tissues is just one part of the pain experience. For example, many of us have bulging discs, or nerve compression, yet may never have any symptoms. It is also very likely that an X-ray of an older person’s spine reveals arthritic changes, but the patient has no symptoms.
Simply, if there is no pain it means that these changes in tissues are not perceived by your brain to be a threat. Many and varied cues may relate to the pain experience, but it is the brain which decides whether something hurts or not, 100% of the time, with no exceptions.
So when there are changes in the spinal cord, the brain may no longer receive accurate information about what is happening in the tissues. Instead of a nice clear view of the tissues, there is now a “magnifier,” or “distorter” in the dorsal horn of the spinal cord. In this sensitized state, the brain is being fed information that no longer reflects the true health and abilities of the tissues at the end of the neurons. Basically, the brain is being told that there is more danger at the tissues than there actually is. The gain of the system is increased. Brain responses such as movement, thoughts, autonomic and endocrine responses are now based on faulty information about the health of the tissues at the end of the neurons.
Under normal circumstances, the brain decodes the incoming messages and decides if it needs to be interpreted as pain. The incoming signals travel through various parts of the brain for the appropriate interpretation: the pain neuromatrix. This matrix changes with chronic pain (different brain patterns, increased activity of certain parts of the brain, increased manufacture of sensors in the pain ignition nodes and increased manufacture of chemicals to activate these sensors). The result of these changes is that potentially non-threatening signals will be interpreted as threatening and that nociceptive signals will generate a longer and more intense pain sensation. The more chronic the pain becomes, the more advanced the changes in the brain become.
Chronic pain also leads to persistent changes in sympathetic and parasympathetic nervous systems, endocrine, immune and motor systems. These systems can combine to perpetuate the pain neurotag.
In patients with chronic pain, the descending pain inhibition fails, and is linked to psychological factors. Common factors are abnormal pain cognition (catastrophizing), fear of movement, passive coping, hypervigilance, fear, and depression.
In summary, central sensitization includes both top down and bottom up mechanisms.
12

How to recognize central sensitization:The patient with central sensitization will have increased responsiveness to peripheral stimuli (mechanical, pressure, chemical substance, light, sound, cold, heat, stress). Clinically, the presence of central sensitization will result in:
Increase in complexity of the clinical picture Increase in unrelated symptoms More difficult clinical reasoning process Decreased odds of a favorable rehabilitation outcome
Despite there being no definitive test to diagnose central sensitization, it is suggested that by gathering information from the following 4 different sources, you can recognize patients with this condition:
1.) Medical diagnosis2.) History3.) Clinical examination4.) Analysis of treatment response
1.) Medical diagnosisCentral sensitization is characteristic of the following disorders:
Chronic whiplash Fibromyalgia Irritable bowel syndrome Chronic fatigue syndrome
Central sensitization is frequently present in a subgroup of the following musculoskeletal disorders:
Chronic low back pain Subacute whiplash TMJ disorders Rheumatoid arthritis Chronic headaches Osteoarthritis
2.) History There is a general intolerance to physical and emotional stresses. Ask about sensitivity to bright lights (having to wear sunglasses inside), smells, loud noises (having to turn the radio down even when the volume is low already), hot/cold and touch. If any of these answers is affirmative, inquire if the response is local, or more of a general widespread sensitivity.Other symptoms that might indicate central sensitization are fatigue; sleep disturbances, unrefreshing sleep, concentration difficulties, swollen feeling, tingling, and numbness.
None of those symptoms on their own offer any evidence will of central sensitization, but each one provides a clue. When 2-3 of them are present, it warrants further investigation.
13

Presence of a local pain condition prior to trauma or injury increases the probability for developing peripheral or central sensitization. This pain can be located at the same site or distant site to the new injury or trauma
3.) Clinical ExaminationWhen central sensitization is suspected based on medical diagnosis and patient history, examination of responses to certain stimuli is warranted. None of these tests by itself is indicative of central sensitization. Use it in combination with other tests, history, and medical diagnosis. It will also establish a bottom line and give you an indicator of the severity of the condition.
Pressure pain thresholdManual palpation can be used. Findings of generalized hypersensitivity to manual palpation should alert you to the possibility of central sensitization. The amount of pressure should be at 4kg/cm2. It is normal to have some areas more sensitive than others. Look for generalized soreness vs. localized soreness.
Sensitivity to heat, cold, vibrationPlace the hot/cold/vibration on the skin for a few seconds. Sensation perceived by the patient should be either hot/cold/vibration, but not pain.
Joint endfeel. Increased sensitivity during muscle and joint endfeel testing can also be an indicator of central sensitization
Brachial plexus provocation testA heightened response to the bilateral brachial plexus provocation test has been proposed as a sign of central sensitization in patients with chronic whiplash disorders. A bilateral loss of elbow extension greater than 30 degrees with moderate complaints of pain can be an indicator of central sensitization.
Exercise responseIn healthy individuals, pain threshold increases during physical activity, and can stay augmented for 30 minutes post exercise. This is caused by the release of endogenous opioid release and activation of several spinal anti-nociceptive mechanisms. In certain chronic pain populations those anti-nociceptive mechanisms are unable to respond to a variety of stresses, including exercise. These patients will have an increased pain perception in response to exercise, which can be indicative of a deregulated anti-nociceptive mechanism. Keep in mind that you cannot generalize findings of anti-nociceptive mechanisms during exercise to all chronic pain populations. For example, in chronic LBP, pain thresholds increase normally in response to exercise.
To test pressure pain threshold in response to exercise you can have the patient ride the stationary bike at low resistance, constant speed. Start at 10-50 kW, gradually increasing the resistance 20-50kW/min. Reassess PPT every 2 minutes at a site distant from the primary nociceptive source (i.e. the skin web between thumb and finger in patients with low back pain).
14

The test is terminated when pattern of pain is established (increase, decrease or no change). Don’t push it so hard that the patient feels worse afterwards.
A normal response is a gradual increase in pain threshold during exercise. Constant or decrease in pain threshold suggests a malfunctioning of anti-nociceptive mechanisms, hence central sensitization. The patient may be susceptible to all kinds of nociceptive stimuli during exercise, indicative of general stress loading intolerance. So caution is required when applying time contingent exercise interventions like a graded exercise program with these patients.
4.) Analyzing treatment response to recognize central sensitizationCentral sensitization may not be present at the start of treatment, but may become apparent during the rehab process. This can occur when physical and emotional stressors combine to increase the overall stressor load to a level greater than the patient’s load tolerance. Be aware that therapy itself can be a stressor. The patient can complain of new symptoms during treatment, or existing symptoms may be exacerbated. A strong increase in symptom severity post-treatment represents another possible sign of central sensitization. PT’s can trigger the symptoms with too vigorous exercises, or too aggressive hands on therapy. Other factors indicative of central sensitization: non-responders, post-exertional malaise, decreased pain threshold during hands on treatment.
OutcomesConsider the presence of central sensitization in poor treatment outcomes, but keep in mind that not all poor treatment outcomes are due to central sensitization.
15

Pain management essentials
There is no single solution for all pains. Pain is an experience that occurs as a result of the merging of your body, brain, environment, and community.
Of the many management tools that have been suggested for managing pain, there are three tools that have consistently shown to be helpful:
1. Activity2. Pain education3. Appropriate short-term drug therapy
Education, knowledge, and the ability to act on that knowledge provide the foundation for therapeutic activity. It reduces the threat associated with pain. Educated movement not only increases tissue health and the health of your circulatory/respiratory systems. Educated movement nourishes the brain because it establishes and re-establishes fine functional sensory and motor representation in the brain, using pathways laid low by fear and ignorance.
There are many other tools that are useful for different people at different times. For example: medication, diet, skilled attention to unhealthy tissue, cognitive and behavioral therapy, relaxation strategies, spiritual enlightenment, love.
It is recommended you use validated outcome measures similar to the ones found in pain education studies. The NDI, ODI, DASH and FABQ are excellent choices. Asking patients with chronic pain for their pain rating does not provide any significant value. Despite this, asking for patient’s pain ratings is often mandated by insurance carriers or health care policies. Keep in mind that the word “pain” is considered a provocative word and may be a significant source for firing up the pain neurotag. Asking them over and over about their pain may increase the pain ratings.
The pain drawingThe pain drawing describes the pain, but the way in which patients draw their pain can also tell us a lot about their psychological state. The simplest signal is the sheer quantity of the drawing – how large an area and how densely they fill it in. Pain may be widespread or non-anatomic. It may expand to other areas of the body. It may even spread outside the body outline. They may put excessive detail into the drawing. They may add emphasis or comments on the severity of their pain. All these features reflect the patient’s psychological state. So the simple pain drawing gives us both physical information about the pain and psychological information about the patient. We must not over-interpret the pain drawing. It is crude and cannot give a complete psychological profile or diagnosis, and for that reason you might not want to go into detailed ways to score the drawing. All that is important is to recognize that the patient’s description of pain includes both sensory and emotional elements. The pain drawing may be the first clue that you should assess the patient in more depth. However, you cannot rely on the pain drawing alone. Most patients with an exaggerated pain drawing are distressed, but 50% of patients with distress will give a normal pain drawing (Waddell).
16

The Oswestry Low Back Pain QuestionnaireOne of the biggest problems in assessing low back pain is the lack of reliable subjective methods. The Oswestry pain questionnaire was developed to give a percentage score of the patient’s level of function. The patient fills it out. The questionnaire is divided into 10 sections that were found to be most relevant to the problems suffered by people with low back pain. Each section contains 6 statements. Each statement describes a greater degree of difficulty in that activity than the preceding statement. Each section is scored on a 0-5 scale, 5 representing the greatest disability. The scores for all sections are added together, giving a possible score of 50. The total is doubled and expressed as a percentage. If a patient marks 2 statements, the highest scoring statement is recorded as a true indication of his disability. New patients complete the questionnaire when they first attend. The disability score is used as a guide to the treatment program. Changes in the score on subsequent testing can be used to monitor progress. The self-administered questionnaire avoids any interview bias and ensures uniformity of presentation. The combination of closed questions and self-administration gives a reliable format.
Interpretation of disability scores0-20% Minimal disabilityPatients can cope with most ADL’s. Usually no treatment is indicated other than advice on body mechanics, posture and physical fitness.20-40% Moderate disabilityThis group experiences more pain and problems with sitting, lifting and standing. Travel and social life are more difficult. The condition can usually be managed by conservative means.40-60% Severe disabilityPain remains the main problem in this group. They require detailed investigation.60-80% CrippledBack pain impinges on all aspects of these patient’s lives both at home and at work and positive intervention is required.80-100%These patients are either bed bound or exaggerating their symptoms. This can be evaluated by careful observation during the examination.
During the first 2 weeks post injury, the scores can be fairly high, up to the 80-100% category. However, after the first 2 weeks you should see a significant drop in the score, preferably to below 20%.
Reference1. Fairbanks, J et al. The Oswestry low back pain disability questionnaire. Physiotherapy. 1980;
Vol. 66, No. 8
17

Fear Avoidance Beliefs Questionnaire (FABQ)Patients who believe that physical activity may aggravate their pain, whether from past experience or because of their understanding of the pain, will expect and fear more pain if they are active. Note that this is all a matter of fears and expectations about what may happen. Waddell found that low back disability depends more on fear avoidance than on pain or physical pathology. Fear of pain may be more disabling than pain itself. It may at first seem that fear avoidance beliefs are a natural and accurate interpretation of pain as a signal of injury. However by the time pain becomes chronic, there is very little relation between fear avoidance beliefs and pain itself. Avoidance behavior itself reinforces fear avoidance beliefs in a vicious circle. It’s like the dog that barks every time the postman appears. The postman never has and never will break into the house, but the dog believes that is because it has chased him away. The very fact that the threat never materializes encourages the dog to go on barking. The Fear Avoidance Beliefs Questionnaire measures beliefs about physical activity and work. Research has demonstrated a strong relationship between elevated fear avoidance beliefs and chronic disability due to LBP. A research study by Fritz and George in 2002 shows that the FABQ work subscale may be able to serve as a useful screening tool to identify increased risk from prolonged work absence for patients with acute work related LBP. A score of 29 or less has a negative LR of 0.08. A score >34 has a positive LR of 3.33 The reliability for the FABQ is .77 for back painA treatment regimen consisting of graded exercise and issuing an educational pamphlet has been shown to be successful.
References1. George, SZ et al. The effect of a fear avoidance based physical therapy intervention for patients
with acute low back pain: results of a randomized clinical trial. Spine. 20032. Fritz JM, George SZ. Identifying psychosocial variables in patients with acute work related low
back pain: the importance of fear avoidance beliefs. Phys Ther. 2002; Vol 82 No 10
18

Pain education There is compelling evidence that pain education can have a positive effect on pain, disability, catastrophizing and physical performance. The patient will move better, have less pain and decreased central sensitization. Pain education informs patients about what to expect from the evolution of their pain, deemphasize the patho-anatomical content, and focus on the factors tat contribute to the development of pain, all within a biopsychosocial framework16. Biomedical education models are not helpful in altering pain, and may actually make it worse.
A multicenter RCT in patients undergoing surgery for lumbar radiculopathy demonstrated that one pre-operative Pain Education session supplemented by reading material resulted in significantly lower levels of health care use and costs up to 3 years post surgery compared to patients receiving only usual care 15. One year post op, health care expenditure in patients who received preoperative Pain /Education was 45% lower compared with those receiving usual care only. These expenses remained 37% lower at 3 years postsurgery despite similar levels of low back pain, leg pain and disability.
A publication by Goudman et al16 proposes a Pain Education approach for patients undergoing surgery for lumbar radiculopathy. Approximately 20% of these patients will develop chronic pain after surgery, leading to a high socioeconomic burden. Current perioperative interventions are not always effective in preventing this. They propose a shift in educational intervention from a biomedical to a biopsychosocial approach as utilized in Pain Education
The goals of pain education for patients with chronic pain and central sensitization: Increase the knowledge of the neurophysiological mechanisms of chronic pain Provide insight in the role of biopsychosocial issues in chronic pain It decreases the threat value of pain by reconceptualizing it
The more recent studies suggest pain education in 30-minute sessions spread over time, 6-8 weeks. For patients undergoing surgery for lumbar radiculopathy, two 1- hour sessions are suggested16. One session in the week leading up to the surgery, and one session between 1 day post operative and discharge from the hospital. Additionally, to maximize retention, the use of an informational booklet or an online module is strongly recommended17,18, 19. An example of an interactive online module can be found at www.retrainpain.org
There is a bit of a misconception that pain education crosses over to counseling, and does not involve good PT anymore. Don’t get the idea that manual therapists should be psychologists. Psychology has its own declarative knowledge. The central tenet of manual therapy is faulty movement. If faulty movement comes from a simple fear of movement, fear of re-injury or lack of understanding of the meaning of certain symptoms, then the managing therapist should deal with this fear. There is little to no evidence to suggest that pain education is helpful all on its own; there is greater evidence for its use in conjunction with manual therapy and exercise.
A few helpful things to point out: It does not help if it is boring People without any training in health professions or biology can understand the biology
of pain
19

Learning about pain biology reduces the threat value of pain Combining pain biology with movement approaches will increase physical capacity,
reduce pain and improve quality of life Understanding why so many things affect pain actually reduces their effect on pain
Make sure the patient understands that when they are in pain, it does not necessarily mean they are damaging themselves. If the pain has persisted for longer than the tissues take to heal, then increases in pain are far less likely to relate to changes in the state of your tissues and are far more likely to be due to other threats.
If the patient has had recurrent pain for many years, each recurrence does not necessarily mean you have re-injured that muscle, joint, ligament or nerve. It makes more sense scientifically to conclude that recurrences occur because some cue has been sufficient to activate the virtual representation of the old injury. It may be your brain checking up on you to make sure your body is OK, safe and sound, or it has decided to play the pain tune to make sure it doesn’t forget it.
So hurt does not always equal harm. However this does not mean you can go out and do a monstrous workout. The patient’s body likely is not prepared for such a big step and the already sensitized nervous system will take drastic measures to stop you from doing that again. In fact, when the central nervous system gets really desperate to prevent you from damaging yourself, it can do all sorts of things: stop your muscles from working properly, make you faint, vomit or want to sleep all the time. This all means that the nervous system will only allow incremental increases in activity or exercise level.
Pacing and graded exposureIf a patient is in pain for a long time, it feels like they are trapped by their pain. To increase activity levels, patience and persistence are required.
Decide what you want to do more of, and what you need to do more of Find the baseline activity that you know the pain won’t flare up. Plan incremental progressions. Use of time is a good measure. Stick to the plan. Don’t be
tempted to break the plan and push on. Don’t flare up, but don’t freak out if you do. The nervous system is so sensitive, it is very
difficult to completely avoid flare ups. When it does flare up it is tempted to just give up. Don’t. Be persistent.
It is a lifestyle change.
The perils of explaining painPain education is difficult, very involved, time consuming, and an area where we as PT’s are not necessarily content experts, although we should be. So what we are seeing now is that dumbed down versions of explaining pain science are all the rage. However, a simple 5 minute video clip, on its own (cleverly made as they are), is not enough to alter deeply held pain concepts, or prescriptive treatments that assume pain is a universal experience for all, with a minute on this and two minutes on that.
Also not helpful are interventions that include some useful explanations of pain, followed by a “traditional treatment” based on out-dated assumptions that pain starts in the periphery - thus
20

perpetuating the fantasy of pain generators and pain endings in the tissues. The attempts at simplification that ‘dumb down’ rather than add any value, the misconceptions that persist, and continuing outright rejection in some therapy quarters, all threaten to derail this evidenced based intervention. All of this at a time when we are also seeing some positive signs too – pain science education making inroads into professions other than its traditional ‘home’ of physical therapy, clever clinicians the world over truly embracing a biopsychosocial approach and integrating quality pain education with modern thinking about manual and movement based therapies, and a new breed of young researchers contributing to the body of knowledge.
Overall, this is a call to be careful with explaining pain – to understand what it is, as well as realize what it isn’t, to acknowledge the skills required to effectively deliver pain education, and develop them where necessary, and finally, to recognize the need to think differently and more broadly.
So what to do if the patient does not buy in to the pain education model? There are three possibilities:
1. It is the PT’s fault2. The information is not good. Sometimes the information is just too difficult/complicated
for the patient to understand. You might want to simplify things at that time. 3. It is the patient’s fault. Sometimes the patient is so convinced of his own illness
perceptions that there is no room for another possible explanation (“I know for sure that with my current slipped disc I should not move too much” or “ I am just waiting for the surgeon to operate on my spine”).
When you notice that the patient just does not buy in to the pain education model, it is probably best to refer him/her back to the physician. It does not make a whole lot of sense to start with treatment at that time.
The other possibility is that the patient does not come back to see you again. That is never any fun from the PT’s perspective, because you put in so much time and effort. Keep in mind though that treating chronic pain is very challenging. The patient might just not be ready to accept the pain message, the patient still is looking for passive treatment, the patient might still believe the answer is in the tissues, or the patient has numerous emotional issues that may need resolving prior to progressing accordingly.
5-10% of the patients will fall in this category. They don’t return to PT, and they are likely communicating they do not want to pursue this treatment option. We advise you not to call the patient to reschedule.
21

References1. Nijs J, van Houdenhove B, Oostendorp R. Recognition of central sensitization in patients with
musculoskeletal pain: application of pain neurophysiology in manual therapy practice. Man Ther. 2010;15, 135-141
2. Nijs, J. Podcast transcript “central sensitization”. EIM Journal Club Vol 9, 2012. Available from www.eim.com
3. Butler D, Mosely L. Explain Pain, 2nd edition. Adelaide, Australia: Noigroup Publications; 20134. Louw A, Puentedura E. Therapeutic Neuroscience Education, teaching patients about pain.
Minneapolis, MN: OPTP; 20135. Mosely, GL. Evidence for a direct relationship between cognitive and physical change during
education intervention in people with chronic low back pain. European Journal of Pain, 2004; 8;39-45
6. Mosely, GL. Joining forces – combining cognition targeted motorcontrol training with group or individual pain physiology education: a successful treatment for low back pain. JMMT 2003; 11, 88-94
7. Moseley GL, Butler DS. The Explain Pain Handbook Protectometer. Adelaide, Australia: Noigroup Publications 2015
8. Mosely GL, Butler D, Beames T, Giles T. The graded motor imagery handbook. Adelaide, Australia: Noigroup Publications;2012
9. Waddell G. The back pain revolution. Churchill Livingstone; 200010. Waddell G. Illness behavior in low back pain. AAOMPT 2000, Charlottesville VA11. Werneke M. et al. Clinical effectiveness of behavioral signs for screening chronic low back pain
patients in a work oriented physical rehabilitation program. Spine. 1993;18(16)12. Nee R ,Butler D. Management of peripheral neuropathic pain: integrating neurobiology,
neurodynamics, and clinical evidence. Physical Therapy in Sport 200613. Schistad E, EspelandA, Pedersen L, Sandvik L, Gjerstad J and Roe C. Association between
baseline IL-6 and 1 year recovery in lumbar radicular pain. EJP 2014; 18, 1394-140114. Mosely L and Butler D. Explain Pain Supercharged. Adelaide, Australia: Noigroup
Publications;201715. Louw A, Diener I, Landers MR, Zimney K, Puentedura EJ.Three-year follow-up of a randomized
controlled trial comparing preoperative neuroscience education for patients undergoing surgery for lumbar radiculopathy. J Spine Surg. 2016;2:289–298.
16. Goudman L et al. A modern pain neuroscience approach in patients undergoing surgery for lumbar radiculopathy: a clinical perspective. Phys Ther.2019;99(7) 933-945
17. Louw A, Butler DS, Diener I, Puentedura EJ. Development of a preoperative neuroscience educational program for patients with lumbar radiculopathy. Am J Phys Med Rehabil. 2013;92:446–452.
18. Malfliet A, Kregel J, Meeus M et al. Blended-learning painneuroscience education for people with chronic spinal pain:a randomized-controlled multicenter trial. Phys Ther. 2018;98:357–368.
19. Ickmans K, Moens M, Putman K et al. Back school or brain school for patients undergoing surgery for lumbar radiculopathy: protocol for a randomised, controlled trial. J Physiother. 2016;62:165.
20. van Wilgen CP, Nijs J. Pijneducatie: Een Praktische Handleiding Voor (para)Medici. Houten, the Netherlands: Bohn Stafleu van Loghum; 2010.
22

Graded Motor ImageryLucas Pratt PT, DPT, OCS, FAAOMPT
Graded Motor Imagery (GMI) is an evidence-based, three-stage treatment sequence that modulates the brain’s neuromatrix by dampening sensitization and promoting inhibition of pain neurotags. David Butler, Lorimer Moseley, and their team designed the GMI program based on their several decades of research on pain neuroscience. GMI has been proven to be effective in treating complex regional pain syndrome (acute and chronic) and phantom limb pain, two of the most difficult neuropathic pain states to treat. The latest emerging evidence also shows GMI to be effective for carpal tunnel syndrome, osteoarthritis, chronic neck pain, and other neuropathic pain syndromes.
More on NeurotagsA neurotag is a representation or map of interconnected neurons that are distributed throughout the brain, including in the premotor, primary motor, and primary sensory cortexes. When incoming signals and information activates a brain neurotag, it produces an output experience, such as the experience of smelling bread…or the experience of feeling neck pain.
In chronic pain states, the pain neurotag becomes sensitized and disinhibited. Sensitization of the pain neurotag refers to the decreased firing threshold and increased excitability of the neurotag. Sensitization explains why chronic pain is more easily evoked and by a wider array of internal and external stimuli than in an acute pain condition. Disinhibition of the pain neurotag refers to the decrease in the inhibition of non-member neurons, whereby the pain neurotag loses its precision and becomes “smudged”. Disinhibition leads to cortical reorganization of both the primary somatosensory cortex and the primary motor cortex. This explains why chronic pain spreads, often to an entire limb, body region, and does not follow the typical pattern of a peripheral nerve or nerve root. Disinhibition is why chronic pain patients may have difficultly describing the location and quality of their pain, and why they present with a decrease in motor control of the involved body region.
23

When a pain neurotag has become sensitized and disinhibited, normal stimuli of touch and movement of the involved body part will fire the pain neurotag; in extreme cases, watching someone else moving--or even imagining one’s own involved body part moving--can fire the pain neurotag; this occurs because both watching and imagining movement fires neurons in the premotor cortex, which then fires neurons in the primary motor cortex. It has been shown that in a left/right discrimination task, (which is when one looks at a picture of a specific body part and is required to discriminate if it is a left or right body part), the brain fires some of the same neurons that it uses to move the body part, but it does not require the premotor cortex to send messages to the primary motor cortex. Using this information, the GMI treatment sequence begins with left/right discrimination, or implicit motor imagery, to modulate the pain neurotag without firing it, effectively “sneaking under the pain radar".
Setting the Stage: EducationIt is imperative for the patient to gain an understanding of how chronic pain works and what the GMI stages are designed to accomplish. There is evidence to show that clinicians who are better at explaining the mechanisms of chronic pain and who are better at endorsing the GMI process have been shown to achieve better outcomes for patients with chronic pain. Moseley suggests educating and constantly reminding patients that chronic pain rehabilitation requires patience, persistence, courage, and commitment. Butler recommends the use of metaphors and stories to change the patient’s mindset and perspective.
Stage 1: Implicit Motor ImageryThis stage consists of left/right discrimination tasks that modify the pain neurotag withoutactivating them. These tasks can be performed using the Recognise online program, smart phone applications, and/or flashcards. It can also be performed with cutouts from magazines, but this method will much harder to quantify improvements in accuracy and response time, and the context of the magazine picture may fire the pain neurotag. The left/right discrimination tasks must be performed as quickly as possible so that it is an unconscious guess. For extremities, the patient will need to choose if he or she is looking at a right or left extremity, and for the spine, he or she will choose if the spine is rotated or side bending to the right or left.
24

When to progress to GMI Stage 2:1. Accuracy and response time should be equal L to R2. Accuracy greater than 80% 3. Response time < 1.6 seconds for spine, < 2.0 seconds for extremities4. Consistently achieving the three criteria above for at least one week, and results should not
decrease when performed under stress. Regarding this fourth point: This is really a clinical judgment call. The one-week
requirement is based on the evidence from clinical trials with CPRS and phantom limb pain patients; however, Butler has said that in less extreme chronic pain cases, the patient may be ready to progress to stage 2 right away in the first training session.
Stage 2: Explicit Motor ImageryThis stage consists of using the imagination to practice movements and activities without actually moving the involved body part. During this stage, the patient must imagine the movement purposefully—it cannot be an absent-minded task. The imagined movements should take just as long as it would take to actually perform the movement.
Using the same pictures and format that were used in the first stage, the patient will look at each image and imagine moving the body part into the position depicted, and then imagine comfortably returning to the original position. Observation of movement is a regression option when the patient is experiencing adverse effects or if the pain neurotag is highly sensitized.
The imagined movements training should start in the least threatening and pain-provoking context possible. Try to reduce the patient’s contextual DIMs and promote the SIMs. Then following principles of graded exposure, the goal is to altering the patient’s context until they can perform the imagined movements in their functional context without firing the pain neurotag. Examples of context options/parameters:
Length of training session Number of training sessions per day, time of day Image options:
o display time lengtho number of imageso context of images --> plain background to high contextual interference
Training location - peaceful room, home, coffee shop, work Psychoemotional context –
o Performed with the PT, with a trusted friend, alone, in a crowded public areao Performed in a quiet context, with music—classical, rock, dubstepo Performed while in different moods
Patient posture – supine, sitting, standing; eyes open, eyes closed
When to progress to GMI Stage 3This again is a clinical judgment call. Based on published clinical trials of CRPS and phantom limb patients, it is recommend that the patient is fully comfortable with imagined movements, which may take up to 2 weeks, before progressing to stage three. However, in less extreme chronic pain cases, the clinician may choose to progress to stage three much sooner, even in the same treatment session.
25

Stage 3: Mirror TherapyMirror therapy involves the patient looking into a mirror and viewing the uninvolved side, giving the illusion that he or she is viewing the hidden involved side. Brain activation patterns within the pre-motor and primary motor cortexes during mirror therapy are less than when actual movement is performed, but slightly more than when imagining movements. It is imperative to use a proper mirror, as evidence demonstrates that a slightly distorted image in the mirror will increase the patient’s pain. The mirror effect should be believable, so the patient should take off jewelry/watch and cover up tattoos
26

References1. Moseley G, Butler D, Beames T, Giles T. The Graded Motor Imagery Handbook. 1st ed.
Adelaide, Australia: Noigroup Publications; 2012.2. Moseley GL. Graded motor imagery for pathologic pain: A randomized controlled trial.
Neurology. 20063. Moseley GL. Graded motor imagery is effective for long-standing complex regional pain
syndrome: a randomised controlled trial. Pain. 20044. Parsons LM., Integrating cognitive psychology, neurology and neuroimaging. Acta Psychologica
2001;107:155-81.5. Schwoebel J, Coslett HB, Bradt J, et al. Pain and the body schema: effects of pain severity on
mental representations of movement. Neurology 2002;59:775-7.6. Wallwork S, Butler DS, Darmawan I, et al., Motor Imagery of the neck. Age, gender, handedness
and image rotation affect performance on a left/right neck rotation judgment task. 2012.7. Bowering J, Butler DS, Fulton I, et al., Implicit motor imagery in people with a history of back
pain, current back pain, both or neither. Submitted 2012.8. Ehrson HH, et al. Imagery of voluntary movement of fingers, toes, and tongue activates
corresponding body-part-specific motor representations. J Neurophysiol. 2003 Nov;90(5):3304-16.
9. Is successful rehabilitation of complex regional pain syndrome due to sustained attention to the affected limb? A randomised clinical trial. Moseley, G.L., Pain 2005
10. Daly, A. E., Biolocerkowski, A. E., Does evidence support physiotherapy management of adult Complex Regional Pain Syndrome Type One? A systematic review. European Journal of Pain, 2008.
11. Diers M., et al. Mirrored, imagined and executed movements differentially activate sensorimotor cortex in amputees with and without phantom limb pain. Pain 2010.
27

Joint Mobilization
Mobilization/manipulation: the skilled passive movement to a joint and or the related soft tissues at varying speeds and amplitudes including a small amplitude, high velocity therapeutic movement (DACP AAOMPT 1998).
Mobilization/manipulation: a manual therapy technique comprised of a continuum of skilled passive movements to joints and/or related soft tissues that are applied at varying speeds and amplitudes, including a small amplitude/high velocity therapeutic movement (Guide 2000).
A joint mobilization may be performed to restore joint play, and may take place either within or at the end of the available range.
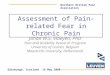
Graded oscillations have been widely promoted by Maitland. He describes 5 grades of oscillations, each with their own indications.
The grades are described below:Grade ISmall amplitude movement performed at the beginning of the range.Grade IILarge amplitude movement performed within the range but not reaching the limit of range.Grade IIILarge amplitude movement performed up to the limit of the range.Grade IVSmall amplitude movement performed at the limit of the range.Grade VManipulation: high velocity thrust at endrange of movement.
A. Grades of oscillations. B. Grades of oscillations in relation to a joint with limited motion1. Starting position 2. Point of limitation 3. Anatomical limit of motion
(From Gould JA: Orthopedic and Sports Physical Therapy, ed 2, St Louis, 1990, Mosby)
28

Effects of joint mobilizations
1.) Mechanical2.) Neurophysiological 3.) Psychological
1.) Mechanical effects:a. Restore joint playb. Stretch out tight capsulesc. Stretch out adhesiond. Snap adhesione. Alter positional relationships
2.) Neurophysiological effects:
Type I and II mechanoreceptors are activated by Grade I and II mobilizations and oscillations. These movements provide an excellent way of reducing pain and muscle guarding. Codman was the first to realize that repeated motion tends to decrease pain. McKenzie applies the same principle for centralization of pain although he feels that results are due to disc reduction.Type III mechanoreceptors are activated by joint manipulation or a strong stretch to the capsule. It provides a reflex muscle relaxation.
It is also suggested that a mechanical force from joint manipulation initiates a cascade of neurophysiological responses from the peripheral and central nervous system, which are then responsible for the clinical outcomes.
3.) Psychological effects:
The laying on of skilled hands provides confidence and assurance to the patient that something good will result. The psychological effects are not why we use manipulation, but they must be considered.
29

Patient Handling
Handling can be positive or negative and although variables exist beyond the control of examination (hand size, length of fingers, padding etc.), the way the hands are applied makes an important difference. Handling includes picking up and putting down, requires constant thought and attention and should promote confidence, control and comfort. Take an appropriate grip and support the structures. Cause no pain. Your hands should be caring, confident and sure. Take off your watch and inappropriate jewelry. Mobilizations should not be fast, jerky or rough.
Indication for manipulation
Presence of dysfunction Neurophysiological effects for the relief of pain
Contra indications
Presence of serious pathology that mobilization may affect adversely Relative to skill and experience
Contra indications
Fracture Ligament rupture No working hypothesis Multi level nerve root pathology Worsening neurological function Unremitting, severe non mechanical pain Unremitting night pain (preventing patient from falling asleep) Empty endfeel and severe multidirectional spasm, which can be the result of various
serious pathologic findings Upper motor neuron lesions
Cautions
Anything that can weaken bone: local infection, osteoporosis, neoplasm Pharmacology: steroidal drugs, anti coagulants, drugs you don’t know Pregnancy. Risk of coinciding with miscarriage Inflammatory disease Depleted general health Patient unable to relax Physique Undiagnosed pain Lack of patient consent When you sense that the joint will not ‘give’ Adverse reactions to previous manual therapy
30

Disc herniation/prolapse Pain with psychological overlay Children or teenagers When spinal movements and /or palpation reproduces distal symptoms Chronic pain and fibromyalgia- type syndromes. Inadequate signs to explain the patient’s
widespread symptoms, long-term dependency without much hope of benefit. Emotionally dependent patients. Desire manipulation, long term dependency without
much hope of benefit
General rules for manipulation
Keep your knees slightly flexedThis will sharpen the impact. There will be less flexion in your spine. Changes in direction can be easily accommodated
Keep your head upThis keeps the spine straight. More force can be directed to the patient. It avoids too close proximity. It brings the elbows close to your sides for improved control.
Move your hips with your hands followingHands follow, which allows you to maintain local control. Easier acceleration. Hands are less uncomfortable for the patient when you hold them steady. Proprioceptive palpation with operator body
Keep your center of gravity lowBetter balance. Easier to accommodate changes in direction. Better transmission of force
Try and visualize the procedureHow is your posture. Are you using max efficiency. Do you understand the principle of the procedure. What would your posture look like in the mirror.
Keep the objective in mindAre you struggling with the wrong aspects. Is control of the structures a problem. Is another way better
31

Sidelying distraction, specific
Hips are flexed 60 - 90 degrees. Rotate trunk to cranial vertebra of segment to be treated. Cranial forearm and hand are placed against spine with index and middle finger fixating the cranial vertebra of the segment to be treated. The caudal arm and hand are placed on the sacrum, with the index and middle finger on the caudal vertebra of the segment. To apply traction, move caudal arm and body as a unit in caudal direction.
FlexionPatient sidelying. Hips and knees flexed. Rotate spine down to cranial vertebra of segment to be treated. Cranial hand fixates the transverse or spinous processes of the cranial segment of the targeted segment. Caudal hand is placed on the caudal vertebra. The PT’s body contacts the patient’s knees. The caudal hand and body produce flexion in the spine.
32

Mid cervical manual traction, towel techniqueTowel placed so that the inferior edge lies over the spinous process of the upper vertebra of level affected. Have patient tuck the chin.
Mid cervical flexionPatient supine. Stabilize lower vertebra of affected segment by molding index finger and thumb around spinous process. Other hand molds around neck and vertebra above. Place delto-pectoral groove on fore head. Flex up to level. Mobilizing hand draws vertebra up and forward.
33

Mid cervical rotationFor right rotation. Patient supine. Radial aspect of left index finger is placed lateral / posterior on the articular process of the upper level. Rotate down to the level, mobilize up and forward in the direction of the nose.
Side glide METFor side glide right. Can be done in neutral, semi- flexion/ extension. Side glide head to right up to restriction barrier. Creates left side bending. Instruct patient to push head to right. Hold 6 sec. Then pick up slack in right side gliding.
34

Soft tissue mobilization
Soft Tissue Mobilization (STM) is a component of a complete manual therapy program that includes evaluation and treatment of articular neuromuscular dysfunctions. The approach encompasses the evaluation of the soft tissue system and application of specifically directed manual therapy techniques to facilitate normalization of soft tissue dysfunctions (Greg Johnson).
Physical therapy is a health profession whose primary purpose is the promotion of optimal human health and function through the application of scientific principles to prevent, identify, assess, correct or alleviate acute or prolonged movement dysfunctions.
Regular Connective Tissue TendonRegular bundles of mostly collagenous tissue in parallel alignment.Formed from a continuum of the muscles connective tissue, i.e., epimysium, perimysium, and endomysium.Bound by a layer of loose connective tissue.
LigamentDense collagenous tissue less regular than tendon with a spiral and oblique arrangement.Tough, pliant, and flexible without resisting movement and unyielding.
Irregular Connective TissueIrregular connective tissue includes dense connective tissue and loose connective tissue. We will emphasize irregular connective tissue fascia, which is composed of both dense and loose connective tissue.Fascia is composed of irregular sheaths of collagen and elastin fibers.Composed of irregular sheets of collagen plus elastin.Sheaths are continuous, interweaving and enveloping all structures from basement membrane of dermis to periosteum of the bone.Separates muscle and supports, but allows independent function while joining together a functional unit.Absorbs shock and transmits mechanical force.Responsible for the exchange of metabolites from fibrous elements to circulatory and lymphatic systems.
Connective Tissue FibersCollagenMost common fiber There are four types of collagen:
Type I: Skin, bone, tendon, meniscus, dentine, annulus High tensile strength
Type II : Cartilage, vitreous humor, nucleus pulposus More elastic, withstands pressure
Type III : Dermis, heart, blood vessel, synoviumType IV: Basement membrane
35

Of these, the Type I is the primary fiber evaluated and treated with soft tissue mobilization. It has high tensile strength and is able to withstand about one half of the stress tolerated by cortical bone. Collagen is found primarily in tendons, ligaments, fascia, and capsules.
Ground SubstanceGround substance is the fluid, semi-fluid, or solid material that occupies the intercellular spaces in fibrous connective tissue, cartilage, or bone. (Tabers)Non-fibrous element of the connective tissue matrixViscous gel composed of long chains of water (the predominant component, 60-70%) and carbohydrate molecules.Chains are composed mainly of glycosaminoglycans (GAGs), proteoglycans, and tropocollagen.
GAGs functions:1. Non-sulfated hyaluronic acid has the ability to hold water, act as a lubricant and a buffer for
the fibrous elements, may prevent crosslinking.2. Chondroitin sulfates 4 and 6 determine the cohesiveness, viscosity and rigidity of the tissues.
The water component is important in facilitating diffusion of metabolites, electrolytes, and gases between the cellular elements and the vascular and lymphatic systems.The extent of fiber formation can be influenced by the consistency of the ground substance.It has been shown that the mobility of the ground substance decreases with age, immobility, atrophy of muscles, or trauma, which is related to dehydration.Collagen is relatively inelastic and inextensible. The stress/strain curve diagrams the process of connective tissue extensibility. Some elongation occurs through the removal of the inherent crimp within the fiber and its visco-elastic properties. With greater force breaking of covalent bonds and fibers occurs as demonstrated through stress/strain curve. (Bogduk and Twomey)
Mast cellsReleases histamine and serotonin, which are agents in inflammatory changes and heparin, which is an anticoagulant.Histamine and serotonin are released during mechanical trauma, chemical trauma, or reaction to previous antigens.Release is associated with inflammatory reactions, allergies, and hypersensitive states.
Intermolecular cross linkingResearch has shown that during periods of immobilization that there is up to a 30-40% reduction in the level of GAGs within the ground substance, precipitating a loss of 4-5% of the water content causing ground substance dehydration (Akeson, Woo, & Amiel).This ground substance dehydration reduces the necessary critical fiber distance and lubrication between the fibrous elements increasing the resistance to movement.Intermolecular cross-linking may occur between the fibers of the functional intercept points further limiting the extensibility of the tissues.
Repair of regular and irregular connective tissueResponse to trauma, infection, or immobilization. Begins with inflammatory stages or local reactive processes where leukocytes and macrophages migrate from the capillaries and
36

surrounding area to the affected portion and begin phagocytotic action against bacteria and foreign materials.Fibroblasts proliferate and begin fibrogenesis.If appropriate motion does not occur, reparative process may produce non-neoplastic fibrous tissue, which is immobile to restrictive.Immobilization often occurs due to pain, edema or the mode of treatment.It has been found that regular mobility of affected tissues helps to maintain lubrication critical fiber distance.It has been found that connective tissue does not repair itself or reinforce itself effectively in dermatomes supplied by an impaired nerve root; therefore, other problems often arise in these regions.
Scar tissue remains adaptable up to 8-10 weeks post trauma. Maximum strength will be reached at 1 year post injury
Soft Tissue Mobilization (STM)Even though there is not any scientific research that has identified the exact cause of restricted soft tissue mobility, it is possible that this clinically identifiable state may be related to the following possibilities:
Intermolecular cross linking – mechanical changes Scar tissue adhesions Ground substance dehydration Lymphatic stasis and interstitial swelling Neuroreflexive causes Electrochemical causes
The improved mobility following soft tissue mobilization may be related to:
Breaking of restrictive intermolecular cross links – Mechanical Alteration of scar tissue matrix – Mechanical Mechanical elongation of collagen tissue – Viscoelastic The redistribution of interstitial fluids – Hydration The stimulation of GAG synthesis restores normal lubrication and hydration Neuroreflexive changes Electrochemical changes
37

Evaluation
Observation Weight bearing position of footUpper leg on lower legPelvis on hipLumbar on pelvis and so on like blocksLook anterior/posterior, lateral and rotational componentMechanical stress points – sharp angles
Questions to ask yourself Does each component appear to be supported from below?Where are symptoms occurring and where do they have the potential to occur?Which segment is most responsible for deviations?Is the deviation structural or functional? (holding pattern)What movements are or are not available?
Tests
Vertical Compression Test Vertical pressure applied through shoulders. Look and feel for “weak links” and “giving way” of certain areas.
Elbow Flexion Test To test strength of biceps in both normal and corrected alignment. Look for weak links and areas of increased stress, especially in the neck.
Lumbar Protective Mechanism TestEvaluate straight and diagonal directions of the flexors and extensors for muscle initiation response.
Palpation EvaluationThe specific evaluation of the condition and mobility of each structure. It should be noted that any tenderness secondary to appropriate palpation is often indicative of tissue dysfunction. Specific Evaluation
SkinTemperature/moistureTexture
Skin and Superficial FasciaMobility – Freedom in relationship of skin to underlying structuresExtensibility – Tension during elongationEnd Feel – Quality of tissue tension – Normal being springy and dysfunctional being hard or non-compliant. Identify specific location and direction of restriction.
38

Elasticity – Recoil
MuscleContourPosition – Is it appropriate for biomechanical pull of joints it crosses?Muscle Play – Accessory mobility – Evaluated in both lengthened and shortened range of motion Muscle play is dependent on the condition of the connective tissues.
a. Independent mobility from surrounding structures – Skin, muscle, bone, etc.b. End Feel – Pliability of tension
Clinical palpation of soft tissue elements can identify areas of dysfunction in which the muscle play (accessory mobilization of muscle) skin mobility and flexibility of the structures are restricted. These regions can often be identified to contribute to changes in posture and movements with specific soft tissue mobilization techniques; the condition of these dysfunctions can be improved or completely eliminated. Upon re-evaluation an improvement in posture and movement is usually noted. The exact physiological process, which causes the palpable changes and their quick response to specific techniques, has not been explained to this point in the literature.
Dysfunction Any area of impaired or altered function related to components of the musculoskeletal system (muscle, fascia, tendon, ligament, bursa, etc.) and associated and/or related parts of the vascular, lymphatic or nervous system (Rumney).
Dysfunction consists of: Soft tissue changes – increased resistance, decreased pliability Changes in coordination and strength Changes in mobility of soft tissue Changes in neural elements Changes in joints
Dysfunction can result from the following restrictions:
Scar/adhesions from previous injury/operations Immobility – illness, sedentary lifestyle, sustained postures, etc. Repeated micro traumas:
1. Environmental – chairs, shoes, cars, etc.2. Employment – sitting, lifting, carrying3. Recreation – lifestyle, hobbies, sports4. Holding Patterns –alterations in posture and movements due to excessive and
unnecessary muscular contractions. These alterations may lead to clinical signs and fixed structural deviations (Judith Aston).
Contraindications/Precautions Malignancy Inflammatory skin condition Fracture
39

Sites of hemorrhage Obstructive edema Localized infections Aneurysm Acute rheumatoid arthritis Fibrotic state Osteomyelitis Advanced osteoporosis Advanced diabetes Increased symptoms Fibromyalgia – in inflammatory state
Purpose of Soft Tissue MobilizationTo evaluate and treat specific restrictions of skin and superficial fascia
EvaluationThe specific direction of restriction is identified through quality of end feel of tissues. Restrictions at end feel are hard and non-springy. Evaluate for location, depth, and direction of maximum restriction.
Skin Sliding demonstration with spine, towel rolls and sheet1. General – use palm to evaluate ability of skin to slide on underlying region.2. Pulling on skin with fingertips – to evaluate how skin slides over underlying
structures. Perform skin sliding in all directions to determine normality of tissue.
Finger sliding Used for identifying specific restrictions by using middle finger or thumb to evaluate ease of gliding through the skin above underlying structures. In normal tissue the finger slides with ease creating a wave of skin in front. In restricted regions there is diminished ease of sliding. Restrictions are identified by specific location and direction of maximum restriction.
Skin rolling Lifting skin between thumb, index, and middle fingers to evaluate skin’s ability to lift from underlying structures. Rolling is accomplished by keeping a wave of skin in front of the thumb while the finger pulls ahead.
Soft Tissue Techniques
40

Treatment HandPull with fingertip(s) – usually medial aspect of middle finger. Tension applied in specific direction of restriction. Therapist positions body in midline. Maintain pressure on same level slowly allowing restriction to release and re-evaluate.
PushUnlocking spiral - apply small amplitude lateral or rotating motions may assist release. This is similar to the motion of using a screwdriver.
Assisting HandTissue lengthened – tension placed on restriction by stretching away surrounding tissue of same layer.Tissue shortened – treatment hand maintains tension, assisting hand creates slack.
Evaluation and Treatment of Contractile TissueTo identify the condition of the contractile tissue for muscle play, tone, length, and specifically define identified dysfunctions.
Evaluation ProceduresPerpendicular (transverse) deformation Fingertips or thumb pressure directed at right angles to muscle belly to locate regions of decreased muscle play. Specific restrictions identified by depth and directions of maximal limitation.
Parallel (longitudinal) deformationAngled pressure directed parallel to muscle belly or the seam between it and other structures for restrictions to muscle play.
Muscle belly palpation for increased tone
41

1. Identify specific points of increased tone. These areas are noted by palpable state of increased tissue density (trigger points). Find epicenter and direction.
2. Patient can assist in finding these points, as they are generally tender to palpation.* Any tenderness to normal palpation indicative of soft tissue dysfunction. A normal healthy muscle should never be tender to palpation.
3 Some causes of increased tone are protective and reflex spasm, holding patterns, tensions, emotional/mental response, and habitual patterns of misuse.
Treatment Procedures
Perpendicular (transverse) strummingFingertips or thumbs in straight lineApply perpendicular pressure onto muscle belly, deforming it until the end range is met. Allow muscle to spring back, but maintain contact. Then slide over muscle or just butt against belly.Oscillate whole body with strumming. Consistent rhythm
Associated oscillationsTechnique applied to regions of increased tone beginning superficial and proceeding deeper as muscle relaxes.Do not remain over one point too long. Move parallel along muscle belly.
Mobilization to improve Muscle PlayPerpendicular (transverse) mobilizationSpecific mobilization techniques – treatment hand directly on restriction while assisting hand can lengthen or shorten the surrounding tissues or perform an associated oscillation to assist in facilitating a release.
Oscillatory technique Rhythmically deform muscle in the direction of specific restriction – maintain contact and appropriate layer.Patient’s body should move with oscillation. Assisting hand may perform associated oscillation. Speed of oscillation will vary with depth of restriction and size of patient.
General TechniquesGrasp belly of muscle between fingers and thumbHeel of hand rhythmically deforming muscle belly
Parallel (longitudinal) mobilizationUtilize all previous techniquesWith assisting hand place muscle on slack over restriction, then as release occurs, stretch away from restriction.
Sustained pressure (SP) to reduce muscle toneTreatment directed towards facilitating relaxation. Patient participation is important for retraining neuromuscular relaxation and longevity results. “Breaks up trigger point.”
42

Amount of pressure always less than what would cause patient to tense. Consistent pressure should be applied and with relaxation, the fingers should sink further into tissues. Specific mobilization techniques already covered may be used.
Sustained pressure while breathing through pressure Sustained pressure while utilizing imagery/visualization (ice cube) Sustained pressure while patient attempting to selectively contract the muscle underneath
the pressure Sustained pressure during resisted contraction (isotonic or isometric) Sustained pressure with oscillation or associated oscillation Sustained pressure with active movement
Centralizing parallel (longitudinal) mobilization – utilizing specific or general contact, apply pressure to center of muscle and progress along belly attempting to broaden muscle.
STM with movementCan do STM with oscillations by therapist, active oscillations by patient, passive stretching by therapist, active stretching by patient, active patient contractions or movements, during an exercise or test position etc.
43

STM Techniques
Clear bony prominencesSacrum, iliac crest, groove between spinous processes and transverse processes, occiput, greater trochanter, patella, scapula, clavicle, etc.
clearing iliac crest
Cleaning the gutter
44

Iliopsoas
Scapula
ITB
45

Scalene
Thoracolumbar fascia
References1. McGonigle, T. and Matley K.W. Soft tissue treatment and muscle stretching. JMMT
Vol. 2, No. 2, 19942. Morgan, D. Principles of soft tissue treatment. JMMT Vol. 2, No. 2, 1994
46