Embed Size (px)
Citation preview
www.healthinnovationnetwork.com
@HINSouthLondon
Feasibility Study for National Clinical
Audit of Venous Thromboembolism
Prevention in Hospital – Final Report
26 January 2018
Authors:
Professor Roopen Arya, Professor of Thrombosis and Haemostasis, King’s College London Director of King’s Thrombosis Centre, King’s College Hospital NHS Foundation Trust
Claire Palmer, Head of Patient Outcomes, King’s College Hospital NHS Foundation Trust
Donna Boreham-Downey, Programme Manager, Health Innovation Network
Zoë Lelliott, Deputy Chief Executive, Health Innovation Network
Kiran Bhangu, Project Manager, Health Innovation Network

Page 2

Page 3
Contents
Contents ................................................................................................................................................ 3
Foreword ............................................................................................................................................... 4
Executive Summary ............................................................................................................................. 6
1. National and Clinical Context for VTE and VTE Prevention in Hospital .................................... 7
1.1 Background: ..................................................................................................................................... 7 1.2 History and current state of VTE prevention and management: ..................................................... 7
2. Feasibility Study for a National Clinical Audit of VTE Prevention in Hospital .......................... 9
2.1 Background to the study .................................................................................................................. 9 2.2 Requirements of the study ............................................................................................................... 9 2.3 Governance of the study ................................................................................................................ 10
3. Delivery of the feasibility study .................................................................................................... 12
3.1 Step 1 - Determining the context and landscape of VTE and VTE Prevention ............................. 13 3.2 Step 2 - Determining Lessons to be Learned from Existing NCAs ............................................... 17 3.3 Step 3 - Determining the methodology for a NCA of VTE Prevention in Hospital ........................ 18 3.4 Step 4 - Developing and Piloting a Data Collection Tool Prototype .............................................. 23 3.5 Statistical Analysis Plan: ................................................................................................................ 24 3.6 Outcomes measurement................................................................................................................ 24 3.7 Limitations of the feasibility study .................................................................................................. 24
4. National Clinical Audit for VTE Prevention - is this feasible? .................................................. 25
5. Recommended design of a future NCA for VTE prevention in hospital .................................. 26
5.1 Improvement aims ......................................................................................................................... 26 5.2 Patient groups ................................................................................................................................ 26 5.3 Methodology ................................................................................................................................... 26 5.4 Data Analysis ................................................................................................................................. 28 5.5 Reporting ........................................................................................................................................ 29 5.6 Information Governance ................................................................................................................ 29 5.7 Outcome Measurement ................................................................................................................. 29 5.8 Key activities and resource requirements for first phase (three years) ......................................... 29
6. Further recommendations for a future National Clinical Audit for Prevention of VTE in
Hospital ............................................................................................................................................... 31
6.1 Quality improvement activities ....................................................................................................... 31 6.2 Additional audits to consider .......................................................................................................... 31
Appendices ......................................................................................................................................... 32
Glossary, acronyms and abbreviations................................................................................................ 32 Appendix One - Acknowledgements .................................................................................................... 34 Appendix Two - Literature Review Summary ...................................................................................... 38 Appendix Three - Summary of findings from NCA interviews ............................................................. 43 Appendix Four: Data Collection Tool ................................................................................................... 48 Appendix Five - VTE Exemplar Centre Criteria ................................................................................... 51
Page 4
Foreword
Venous thromboembolism (VTE), comprising deep vein thrombosis (DVT) and pulmonary embolism (PE), has an incidence of one to two per thousand and affects adults of all ages. VTE cuts across all of the domains in the NHS Outcomes Framework and unlike other cardiovascular disease, a substantial proportion are healthcare-related. Over half of all episodes are attributable to hospitalisation and up to two-thirds of cases of hospital-associated thrombosis (HAT) are preventable. Although the use of thromboprophylaxis has been described by the Agency for Healthcare Research and Quality as the “number one patient safety practice for hospitals” thromboprophylaxis remains significantly underutilised.
The National Venous Thromboembolism (VTE) Prevention Programme was launched in England in 2010. Its central objective was to reduce morbidity and mortality from preventable VTE through the introduction of a comprehensive and systematic approach. The cornerstone of the programme was the introduction of mandatory documented risk assessment for VTE supported by national thromboprophylaxis guidance developed by NICE. NICE published a Quality Standard that defines what best practice in VTE prevention should look like, incorporating risk assessment, patient information and appropriate thromboprophylaxis.
What is the rationale for a national audit of VTE prevention? To date, success of the national programme has largely been driven through the financial incentive of a national CQUIN. According to the 2017/2018 second quarter figures published by NHS Improvement in December 2017, risk assessment rates remain at 95%. However, underlying the overall figure, there has been a significant fall off in risk assessment rates in some areas. Nineteen percent of providers did not achieve the 95% NHS Standard Contract threshold in Quarter Two of 2017/18 and from the first to the second quarter there was a fall from 84% to 74% in NHS acute providers that risk assessed 95% or more of their admissions for VTE. The quality of risk assessment is uncertain, and we have no data on appropriate thromboprophylaxis rates, nor evidence that clinicians are providing patients with the relevant information, as stipulated by the NICE Quality Standard. The All Party Parliamentary Thrombosis Group data indicates many trusts have not progressed beyond assessing risk; they do not audit the entire VTE prevention pathway and some fail to review outcomes. For the past three years, the VTE CQUIN has no longer been in place and there is a need for a new system lever to support a shift in emphasis beyond risk assessment to appropriate prophylaxis and outcomes.
Despite the 95% risk assessment rates and some evidence of improved outcomes, HAT remains common, affecting tens of thousands of patients in England and causing thousands of deaths each year. HAT can cause distress and poorer clinical outcomes at the individual patient level, as well as higher costs and greater demands on the healthcare service.
The requirement on providers to audit the percentage of patients receiving appropriate thromboprophylaxis following VTE risk assessment and undertake root cause analysis of confirmed cases of HAT have been included in the NHS Standard Contract since 2010/11. Nonetheless, providers are only required to report the results if requested to do so by their lead commissioner. A national audit would directly support the implementation of the contract service conditions for VTE, and drive the intended reduction in harm.

Page 5
On the face of it, the case for a NCA of VTE prevention is a compelling one. HAT remains commonplace and a large proportion is preventable, hence the vital need to audit the prevention pathway and improve outcomes. The NICE Quality Standard for VTE prevention provides a suitable framework for audit, which in turn would help drive its implementation in clinical practice. On the other hand, auditing a process conducted across several areas and stages of care, rather than auditing a specific clinical condition brings with it many challenges.
This feasibility study was commissioned to help answer important questions about need, implementability and proof of concept, as well as the likely impact of a future NCA of VTE prevention.
Professor Roopen Arya
Clinical Lead, Feasibility Study of NCA for VTE Prevention Professor of Thrombosis and Haemostasis, King’s College London
Director of King’s Thrombosis Centre, King’s College Hospital NHS Foundation Trust
Page 6
Executive Summary
Venous thromboembolism (VTE), or hospital-associated thrombosis (HAT), remains a significant cause of preventable harm, despite the introduction of a number of national initiatives and interventions aimed at improving VTE prevention (such as CQUINs, NICE guidelines and root cause analysis).
In March 2015, the National Clinical Audit and Patient Outcomes Programme considered a proposal that a National Clinical Audit (NCA) would be an effective mechanism for driving improvements in VTE prevention, thereby reducing the incidence of VTE and improving patients’ experience and outcomes.
Healthcare Quality Improvement Partnership (HQIP) commissioned the Health Innovation Network (HIN) to conduct a one-year study to explore and evaluate the feasibility, and to inform the design of, an NCA of VTE prevention.
An expert, multi-professional Clinical Steering Group with patient representation provided oversight for the feasibility study. Project management was provided by a study management team, supported by an expert clinical lead, audit specialist and a methodologist.
The study was conducted in four steps:
Reviewing the landscape and context of VTE prevention
Determining lessons to be learned from existing NCAs
Proposing the recommended design of a future NCA on VTE prevention
Developing and piloting a data collection tool
The information and intelligence gathered from steps 1 and 2 of the process was summarised and presented to a range of expert stakeholders in a series of sessions and workshops. As a result of debating this information, it was concluded that an NCA of VTE prevention would be both desirable and feasible, and a proposed methodology was designed.
Reflecting this suggested methodology, the study management team created a data collection tool, and piloted this in a number of sites (both VTE exemplar sites and other local hospitals) in South London. Pilot sites provided feedback on the proposed tool and methodology, which were then finalised by the study management team.
In summary, through a systematic process of exploration of the evidence and testing of a proposed methodology using a multi-professional group of experts, we have concluded that an NCA of VTE prevention should be introduced as a mechanism for driving improvements in VTE prevention and associated outcomes.
Page 7
1. National and Clinical Context for VTE and VTE Prevention in
Hospital
1.1 Background:
Venous thromboembolism (VTE) is a blood clot that forms in a vein, most commonly in the vein of a leg, where it is known as deep vein thrombosis (DVT). Part, or all of the clot, can dislodge and travel through the blood to the lungs where it is called a pulmonary embolism (PE). Whilst blood clots are unusual events, the chance of them developing increases when someone is unwell or less mobile, for example following surgery.
Around half of all VTEs are associated with a hospital admission and are a significant cause of death, long-term disability and chronic ill health in hospital patients. Patients report that experiencing a VTE is extremely frightening and can be painful and debilitating. The incidence of VTE can be significantly reduced through the use of systematic VTE risk-assessment linked to the delivery of preventative measures such as anticoagulant medication or anti-embolism stockings for ‘at risk’ patients (NICE, 2010).
In addition to the potential to improve clinical outcomes significantly, the National Institute for Health and Care Excellence (NICE) estimates substantial savings to the NHS if there were effective VTE prevention and management in hospitals.
1.2 History and current state of VTE prevention and management:
Both NICE and the NHS England National VTE Prevention Programme recommend that all patients receive a risk assessment on admission to hospital to identify those at increased risk of VTE, and that prophylaxis is provided to all patients (where it is not specifically contraindicated). However, prophylaxis is often not received, even amongst those identified as high-risk (Rashid et al, 2005; Cohen et al, 2008; MBRRACE-UK, 2016; Roberts, Durkin & Arya, 2017).
Since 2005, a raft of national initiatives has raised clinical and public awareness of VTE, and leadership for VTE prevention comes both from Government, through the All Party Parliamentary Thrombosis Group, and from hospitals, through the VTE Exemplar Network.
The number of adults who on admission to hospital were assessed for their risk of VTE increased significantly between 2010 and 2014, when the Commissioning for Quality and Innovation Scheme (CQUINS) required trusts to measure and report on the percentage of completed VTE risk assessments. The risk assessment uses the criteria within the NHS National VTE Risk Assessment Tool: http://reception.e-lfh.org.uk/vte/content/VTE_03_01/d/ELFH_Session/457/tab_549.html.

Page 8
Additionally, the following information is collected each month and submitted quarterly to NHS Improvement via the online data collection system UNIFY2:
1. Number of adults admitted as inpatients in the month who have been risk assessed for VTE on admission to hospital, using the criteria in the National VTE Risk Assessment Tool
2. Total number of adult inpatients admitted in the month
3. Calculated from 1. and 2. the percentage of adult hospital admissions, admitted within the month assessed for risk of VTE on admission
The results are published quarterly on the NHS Improvement website.
In 2015/2016 the NHS Standard Contract introduced additional nationally-mandated quality requirements, with potential financial consequences:
All hospitals must undertake:
VTE risk assessment and prophylaxis in compliance with NICE guidance
Root Causes Analysis of confirmed cases of hospital-associated VTE
Local audit of prophylaxis
To date, there is no national quality improvement initiative targeted at improving prophylaxis for the prevention of VTE. At the 10th anniversary of the VTE Exemplar Network in October 2017, Sir Bruce Keogh, the National Medical Director for NHS England agreed that a national audit of VTE prevention was the “last piece of the jigsaw puzzle” to ensure improved outcomes for NHS patients at risk of VTE.

Page 9
2. Feasibility Study for a National Clinical Audit of VTE
Prevention in Hospital
2.1 Background to the study
At the meeting of the National Clinical Audit and Patient Outcomes Programme (NCAPOP) in March 2015, a proposal for a new National Clinical Audit (NCA) of the Prevention of VTE was submitted by the NHS England National VTE Prevention Programme. The proposal was considered but it was felt to be unclear as to whether an NCA would be the best approach to achieve the desired healthcare improvements. The committee therefore decided that key questions concerning the likely impact of a NCA in this area would be best addressed by a feasibility study in the first instance.
As a result, the Healthcare Quality Improvement Partnership (HQIP) commissioned the HIN (as per the tender specification) to complete a Feasibility Study for a NCA of Venous Thromboembolism (VTE) Prevention in Hospital, covering NHS-funded secondary care inpatient settings in England. The feasibility study was to take place over a 12 month period concluding in December 2017, and would exclude:
Research, including health policy research
Commissioning of an electronic platform for audit data submission
Collection of data direct from patients (PROMs, PREMs), observational or qualitative data
The acquisition of data from primary care
2.2 Requirements of the study
The study sought to establish the feasibility of the proposed NCA by:
1. Determining what the NCA should set out to achieve and how it would be achieved; including the identification of specific improvement aims
2. Determining appropriate quality indicators and outcome measures for the NCA that aligned where relevant with NICE: Clinical Guidance 92 https://www.nice.org.uk/guidance/cg92/chapter/introduction and Quality Standard Three https://www.nice.org.uk/guidance/qs3
3. Developing, testing and evaluating the methodology for the NCA, which would:
Result in robust comparisons between providers; while being
Achieved efficiently and effectively in terms both of local burden to participants and central cost of delivery
4. Identifying the roles, groups and/or professions who would need to be influenced to realise and drive any required change locally, and their needs in terms of reporting and other outputs
5. Identifying the high-level activities (and their time-frames) and resource requirements for the first three years of the NCA
6. Producing a final, evidence-based report

Page 10
2.3 Governance of the study
The Director of Strategy and Performance for HIN, supported by the Medical Director and accountable to the HIN Board, took overall responsibility for the study.
The expert Clinical Lead for the study was Professor Roopen Arya, whose professional roles include:
Professor of Thrombosis and Haemostasis at King’s College London
Director of King’s Thrombosis Centre and Lead for Thrombosis and Haemostasis at King’s College Hospital NHS Foundation Trust
Clinical Lead for the National VTE Prevention Programme at NHS England
Director of the National VTE Exemplar Centres Network
Figure 1 – Governance of study
Study Management Team:
Day-to-day the study was managed by a study management team, which consisted of two HIN employees part-time: A Programme Manager and a Project Manager reporting to the Director of Strategy and Performance.
The study management team contracted the services of Dr Melvina Owusu, a specialist methodologist who provided not only expert advice on the feasibility study’s design but brought invaluable experience as a project manager for an earlier feasibility study commissioned by HQIP.
The Programme Manager in consultation with the Project Working Group (see below) developed a detailed Project Plan for the study, which was agreed with HQIP. Throughout the study the Programme Manager provided HQIP with quarterly Contract Review Reports, reporting on the study’s progress against the project plan’s key milestones. The reports were reviewed at quarterly meetings between the Feasibility Study’s designated HQIP representatives, the study management team and the Clinical Lead.

Page 11
Project Working Group:
The study management team was supported by a Project Working Group, which was chaired by the Director for Strategy and Performance and reported to the study’s Clinical Steering Group (CSG). The group’s remit was to oversee and contribute to the operational delivery of the feasibility study. Initially, the group met weekly, and as the project progressed, the group met fortnightly and members included the study management team, Professor Roopen Arya and Ms Claire Palmer, Head of Patient Outcomes, King’s College Hospital NHS Foundation Trust (clinical audit expert).
The Clinical Steering Group:
The CSG had overall responsibility for the design and delivery of the study and was chaired by HIN’s Medical Director (a consultant radiologist, and National Clinical Director for Clinical Diagnostics for NHS England). Membership of the group included:
Clinical experts (medical, nursing and pharmacy) in VTE management and
prevention
Experts in clinical audit and quality improvement
The study management team and Project Working Group members
A patient representative
Trustee and co-founder of the UK Thrombosis group.
Representatives from HQIP as observers
Although the majority of the members of the CSG were based in South London, several also held significant national roles in VTE management or prevention (see member profiles in Appendix One for full details). This allowed an informed national perspective for the study. Despite repeated invitations, we were unable to recruit representatives from national medical or nursing professional bodies or associations within the short duration of the study.
Although initially the CSG was scheduled to meet monthly, to maximise efficiency the group members agreed that face-to-face meetings should occur only once every two months – with communications between meetings conducted by emails and teleconferences, as required.

Page 12
3. Delivery of the feasibility study
The overall design and methodology used for the feasibility study was developed with the advice and input of the study’s expert Methodologist, Dr Melvina Owusu. To shape the overall approach to the feasibility study, Dr Owusu facilitated three sessions with the Study Management Team:
Two Feasibility Study Mapping Sessions; and
A Stakeholder Identification Session
Based on the outputs from those three working sessions, Dr Owusu produced:
A Methodological Framework for the study;
A Stakeholder Engagement and Communications Strategy; and a
A Stakeholder Matrix.
This suite of documents was discussed by the CSG at its meeting 18th January 2017, and the methodology for the study was agreed.
The feasibility study comprised of four main components or steps, as per the diagram below:
Figure 2 – VTE Feasibility Study Development Process

Page 13
3.1 Step 1 - Determining the context and landscape of VTE and VTE
Prevention
3.1.1 Literature Review
An extensive review of clinical and academic literature on the history and current state of VTE, VTE prevention (including existing VTE prevention initiatives) and clinical audit was completed by Ms Claire Palmer. This document was reviewed and accepted by the Project Working Group and the Clinical Steering Group.
Key findings of the review are as follows:
VTE is extremely frightening and unpleasant for patients (NHS Choices)
VTE remains a significant safety issue that affects a substantial number of hospital patients (NICE, 2010)
Around half of VTEs are associated with hospital admissions and the incidence can be significantly reduced with the use of prevention interventions (Geerts et al, 2008; Roberts, Durkin & Arya, 2017)
Patients often do not receive prevention interventions (Rashid et al, 2005; Cohen et al, 2008; MBRRACE-UK, 2016; Roberts, Durkin & Arya, 2017)
NICE has published evidence-based Quality Standards that can be used as the basis against which to audit (NICE Quality Standard 3, 2010)
Effective management of VTE would result in a net saving to the NHS estimated at £0.8 million annually (NICE, 2010b)
A national approach to the measurement of VTE prevention in hospitals is likely to achieve improvements (Catterick & Hunt, 2014; Lau & Haut, 2014)
A national audit would support the features of clinical audit methodology that increase the likelihood of it being effective, as identified by a Cochrane Review (Ivers et al, 2012) plan
There are significant methodological issues related to using VTE occurrence as a measurement of the quality of care provided by hospitals, including:
o Surveillance bias (Bilimoria et al, 2013; Kinnier et al, 2016),
o Difficulty with risk adjustment (Lau & Haut, 2014)
o The accuracy of clinical coding (Roberts, Durkin & Arya 2017)
Data collected on risk assessments completed in hospitals (UNIFY2) and deaths from VTE related events (NHS Outcomes Framework) are the only VTE data routinely collected nationally
Local audit is recommended by both NICE and the US Agency for Healthcare Research and Quality (AHRQ, 2016), and is a requirement of the NHS Standard Contract although there is evidence that it is not routinely undertaken by trusts nor monitored by Clinical Commissioning Groups (All Party Parliamentary Thrombosis Group, 2016)
Page 14
No UK or international literature was found on routine centralised collection of performance information on the use of VTE prophylaxis
There are clear recommendations on audit methodology that can be adopted by an NCA to improve the likelihood of it achieving its intended outcome (Dixon, 2014; Healthcare Quality Improvement Partnership, 2014)
In conclusion, the literature indicates that VTE remains a significant patient safety issue that affects a substantial number of patients. A substantial proportion of VTEs can be prevented but prevention interventions are often not taken and there is clear evidence of scope for improvement. Preventing VTE will reduce mortality and other patient harm, improve quality of life and reduce costs to the NHS. A national audit of VTE would support current NHS priorities, as well as the NHS regulatory and contractual framework. There is nationally-endorsed evidence on the interventions that lead to improved prevention of VTE, and there is evidence that measurement and feedback would lead to improvement. A more detailed summary of the literature review can be found in Appendix Two.
3.1.2 Data Review
The Informatics Team at the HIN completed an extensive review of relevant data which is summarised below:
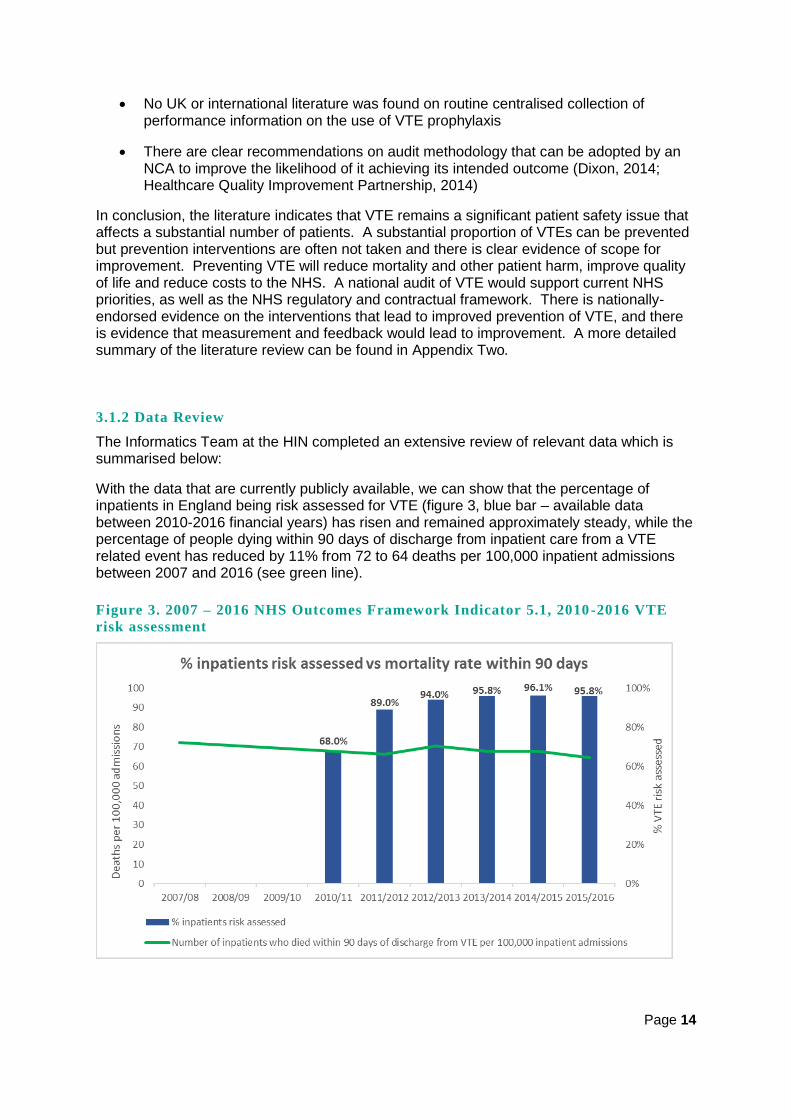
With the data that are currently publicly available, we can show that the percentage of inpatients in England being risk assessed for VTE (figure 3, blue bar – available data between 2010-2016 financial years) has risen and remained approximately steady, while the percentage of people dying within 90 days of discharge from inpatient care from a VTE related event has reduced by 11% from 72 to 64 deaths per 100,000 inpatient admissions between 2007 and 2016 (see green line).
Figure 3. 2007 – 2016 NHS Outcomes Framework Indicator 5.1, 2010-2016 VTE
risk assessment
Page 15
General data quality issues:
Significant data quality issues impact on the reliability of this information, including:
Surveillance bias – increased awareness following the national VTE prevention programme leads to increased identification/coding
Coding of VTE – coding does not separate preventable from non-preventable VTE
Data accuracy relies on availability, skills and knowledge of front-line staff, and will therefore be subject to variability between trusts
Publicly available data:
1: NHS outcomes framework: Indicator 5.1 – available by year for England
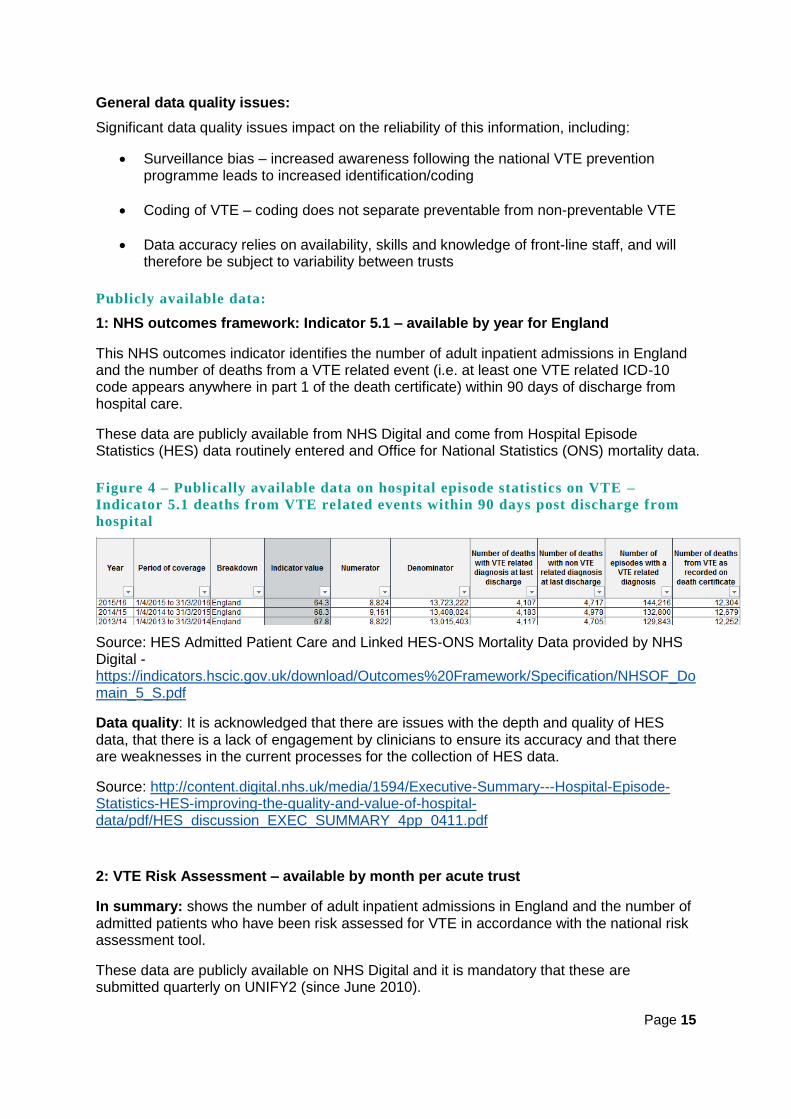
This NHS outcomes indicator identifies the number of adult inpatient admissions in England and the number of deaths from a VTE related event (i.e. at least one VTE related ICD-10 code appears anywhere in part 1 of the death certificate) within 90 days of discharge from hospital care.
These data are publicly available from NHS Digital and come from Hospital Episode Statistics (HES) data routinely entered and Office for National Statistics (ONS) mortality data.
Figure 4 – Publically available data on hospital episode statistics on VTE –
Indicator 5.1 deaths from VTE related events within 90 days post discharge from
hospital
Source: HES Admitted Patient Care and Linked HES-ONS Mortality Data provided by NHS Digital - https://indicators.hscic.gov.uk/download/Outcomes%20Framework/Specification/NHSOF_Domain_5_S.pdf
Data quality: It is acknowledged that there are issues with the depth and quality of HES data, that there is a lack of engagement by clinicians to ensure its accuracy and that there are weaknesses in the current processes for the collection of HES data.
Source: http://content.digital.nhs.uk/media/1594/Executive-Summary---Hospital-Episode-Statistics-HES-improving-the-quality-and-value-of-hospital-data/pdf/HES_discussion_EXEC_SUMMARY_4pp_0411.pdf
2: VTE Risk Assessment – available by month per acute trust
In summary: shows the number of adult inpatient admissions in England and the number of admitted patients who have been risk assessed for VTE in accordance with the national risk assessment tool.
These data are publicly available on NHS Digital and it is mandatory that these are submitted quarterly on UNIFY2 (since June 2010).

Page 16
Figure 5 – Number of adult inpatient admissions in England who have been risk
assessed for VTE by trust
Source: https://www.england.nhs.uk/statistics/wp-content/uploads/sites/2/2015/05/NHSE-VTE-Guidance-September-2015.pdf
Data quality: This relies on front-line staff entering data and it is likely that both the level of data capture, and the quality of the data entered, varies from trust to trust.
3: Safety Thermometer Data
At each organisation, front-line teams record, and a coordinator submits the number of new VTEs across a variety of settings (at provider level detail) on a monthly basis from December 2012 onwards. They also record the percentage of persons not given prophylaxis who were at risk of VTE in acute hospital wards only. It records a patient’s ward/location, age band and sex.
Source: http://content.digital.nhs.uk/catalogue/PUB22775/nati-safe-rep-dec-2015-dec-2016.pdf
Data quality: Accuracy depends on front-line staff and will vary from provider to provider.
Non-Publicly available data:
VTE module of HED (Healthcare Evaluation Data) provided by University Hospital Birmingham NHS Trust
Data of varying levels of detail for individual trusts. Data sources for HED are HES and UNIFY22 – HED provides a front-end to these data that enables comparison across all English trusts:
VTE Risk assessment compliance – data source is number 2 discussed above
Pulmonary embolism deaths after hospital discharge (only available for individual
trusts). These are available by month and updated each month
VTE-related readmission rate (available for all trusts)
Data Quality: Unknown for Unify2 data. As mentioned for source 1, HES data quality is a known issue. Improving local and thereby national data quality may be an important additional objective for a national audit of VTE. It is also limited due to local case-mix issues and lack of risk adjustment. In its current form it is not suitable for use in benchmarking or outlier identification.

Page 17
3.2 Step 2 - Determining Lessons to be Learned from Existing NCAs
The Project Working Group completed an analysis of all NCAs commissioned by HQIP to determine their impact in achieving quality improvement and their burden on participants, with a view to informing a proposed NCA of VTA prevention.
The analysis identified seven audits, which were ranked in order of relevance by the CSG. The Project Working Group agreed that study management team would conduct interviews with representatives from five of the seven audits (based on their similarities of approach, as well as effectiveness and impact on achieving quality improvement) which were:
1. National Hip Fracture Database (NHFD) 2. Sentinel Stroke National Audit Programme (SSNAP) 3. National Emergency Laparotomy Audit (NELA) 4. National Diabetes Inpatient Audit (NaDIA) 5. National Joint Registry (NJR)
The interviews focused on the ‘lessons learned’, i.e. what had worked well, and what had been less successful when establishing these NCAs. A full summary of findings can be found in Appendix Three.
Key points included:
Establishing an NCA - A number of challenges are likely to be encountered when establishing a new NCA. These include setting up data collection and information governance processes, and developing links and engagement with both audit staff and clinical teams in provider trusts who will be responsible for implementing any improvement plans identified. A strong multi-professional central team will need to be appointed early on (including a full-time programme manager, clinical lead and methodology expert) who can help build relationships and support trusts (one NCA set up a help-desk to support teams involved in the audit process). Engagement is more challenging when incentives to participate do not exist
Methodology - The NCAs considered by the team employed different audit methodologies, from snapshot audits (for example, looking at 20% of inpatients at a single point in time) to others that considered complete patient pathways. For four of the five audits, data was submitted electronically (including through a web-based tool), and it was suggested that data collection be kept simple (using a lean data set) with a focus on completeness of fields and validation. Patient identifiable data should be avoided if possible, although trusts may wish to keep this locally to support improvement activities
Reporting – Quarterly audits are not too onerous for participants and allow timely feedback for trusts to conduct improvement activities. Data can be presented in a number of ways for different audiences, and some NCAs reported holding an annual conference, which complements the publication of comparative data
Quality improvement – The NCAs used a range of strategies to drive improvement, including publications and policies, annual events, and more hands-on support, such as peer review teams and site visits
Patient involvement - All five NCAs recognised the importance of patient involvement throughout the audit cycle, and included patients in a variety of ways. This included representation on steering groups, links to major charities, through patient questionnaires, or ad hoc focus groups
Page 18
3.3 Step 3 - Determining the methodology for a NCA of VTE Prevention in
Hospital
The literature and data review concluded that an NCA of VTE prevention has significant potential to improve patient outcomes and experience, as well as reducing cost to the NHS. It also concluded that there are significant methodological challenges for an NCA, including population size, the operation of surveillance bias and the lack of risk-adjustment models.
The review of existing NCAs established that none of the current NCAs have prevention of harm as their key focus, and that therefore there is limited current NCA methodology that can be directly adopted for an NCA of VTE prevention. For an NCA of VTE prevention to be a feasible proposition, a new methodological approach would need to be identified.
Three sequential multi-professional sessions were organised to establish whether such a methodology could be developed.
Methodology Session One: Brainstorming Session - April 2017
This initial session was undertaken by the Project Working Group and attended by members of the CSG (one clinical expert and one clinical audit expert) as well as additional invited clinical audit specialists. The aim of the group was to brainstorm whether, given the information collated so far and the group’s combined expertise, a methodology for an NCA of VTE prevention in hospital could be developed.
Conclusions:
The overall conclusion of the group was that a methodology could be developed to enable an NCA of VTE prevention in hospital.
Specific recommendations:
NICE Quality Standard QS3 provides a robust evidence-base from which to develop clinical audit indicators, and to facilitate local improvement without overburdening trusts. The scope of the NCA should be restricted to the NICE QS3 standards.
Measuring the outcomes of VTE prevention is challenging due to the issues of data quality and reliability described in the literature review. The NHS Outcomes Framework, which provides data on deaths from a VTE-related event within 90 days of discharge from hospital, should therefore be considered as the key source of outcomes data in relation for the NCA.
The only existing dataset that provides information on the adoption of NICE’s evidence-based interventions for VTE prevention is UNIFY2, which provides data on VTE risk assessment but not on the other important aspects of VTE prevention. A new data collection exercise is therefore required to achieve an audit against key NICE recommendations for VTE prevention.
The whole population for a VTE prevention audit is all patients admitted to hospital, and as this is a vast number the NCA would need to be based on a sample of patients, rather than the entire inpatient population.
As VTE prevention interventions are common, a small sample from each participating trust would be sufficient to establish compliance with nationally agreed standards of care.
There are groups within the patient population that are of key clinical interest: medical patients, surgical patients, critical care patients and maternity patients.
Page 19
These can be further divided into diagnostic groups that are of specific interest (for example, cancer patients and orthopaedic patients) and/or into high-risk and low-risk patient groups. The NCA may wish to obtain samples from each of these groups.
To avoid data collection bias driven by variation in the availability of staff within trusts, sampling should not be based on a nationally-defined ‘snapshot’ day or week.
There must be the facility to enable both electronic and manual data entry, as the information technology (IT) capability of trusts is extremely variable.
To ensure validity of results, it is recommended that there is a facility to enable trusts to review and approve data before it is finalised in a national report (good practice example cited was the National Emergency Laparotomy Audit).
To support local rapid quality improvement, it is recommended that there is a facility to enable trusts to compare local practice with the audit standards at least quarterly, in advance of a national report providing trust comparative data (good practice examples cited included the National Hip Fracture Database and the National Emergency Laparotomy Audit).
The group’s conclusion and recommendations were presented to the CSG in May 2017 meeting, where:
It concluded that existing data is insufficient for an NCA of VTE prevention, and that new data is required
It endorsed the use of NICE QS3 as the evidence-base for the audit standards, and the use of a sampling approach
It commissioned a further group to develop and propose specific audit methods
Methodology Session Two: Methodology Proposal Deve lopment - May 2017
This session consisted of a small, focused group of clinical audit experts (who also took part in the Methodology Brainstorming Session). The group used the findings from Session One to develop specific proposals for NCA methods that could be adopted. The proposals, along with specific areas for discussion and decisions to be made, were outlined for the following aspects of the NCA: the audit population, sample size and frequency, sampling approaches, audit indicators, retrospective/prospective data collection, approach to data returns, information governance data quality review and reporting, audit of information-giving to patients, organisational audit and outcomes measurement.
This provided a clear framework for discussion and decision-making for Methodology Session Three: The Advisory Board Workshop.
Methodology Session Three: Advisory Board Workshop - June 2017
This session was conducted by the Project Working Group, and led by an experienced facilitator who took advice on the format from the CSG’s patient representative. Attendees included members of the CSG, public/patient group representatives, multi-disciplinary clinical experts and experts in clinical audit and quality improvement.
The remit of the group was to:
Consider the recommendations from Sessions One and Two; and then
Make specific recommendations to the CSG on the methodology to be adopted for the NCA
Page 20
The group endorsed the recommendations from Session One and proposed the following:
Exclusion criteria:
The following patient groups are not included in NICE QS3, and the evidence for VTE prevention in these groups is not currently clear, so it is recommended that these groups be excluded from the NCA:
Patients not admitted to the hospital, including emergency department patients
Patients admitted to mental health services
If the evidence-base and NICE recommendations change in future, this can be reviewed by a central NCA team and the NCA developed accordingly.
Sampling approach:
The group supported the need for sampling identified in Session One, and agreed that ‘snapshot’ sampling (for example of a day a week or a week a month) would not be appropriate, as it can be influenced by atypical circumstances. This could be a particular issue for the smaller trusts, for example when key staff members are on annual leave and audit data is likely to be collected by just one or two people.
The group debated a range of sampling options, including whether the NCA should provide a strict sampling framework to encompass all sub-groups of interest (e.g. high-risk/low-risk patients or patients admitted under different specialties). When appraising these options, the group considered that:
The workload burden for trusts must be kept to an absolute minimum
The purpose of the project is to audit current practice to drive quality improvement, and not to be a rigorous research study
Trusts have a vested interest in identifying samples of patients that will gain the most benefit from clinical audit and improvement activities
For these reasons, the group agreed that, with the provision of guidance from the central NCA team, it is desirable to allow trusts to identify their own patient samples and not impose a rigid sampling framework.
The group supported the view that the sample should include information on patients which falls within the following time parameters - from the first 24 hours of admission but no later than 10 days post admission. This would include the majority of hospital in-patients and would exclude very long-stayers, who are atypical of the general hospital population.
Sample size:
The group gave careful consideration to the size of sample that would need to be collected in order to assess whether care provided met the audit criteria. As VTE prevention interventions should be taken for the majority of patients it was concluded that a large sample size is not required to enable the identification of actions of interest to the audit. Mindful of the need not to impose unnecessary burden on trust staff, the group recommended a small sample – equivalent to 10% of the hospital bed numbers or 50 patients per trust, whichever is greatest. It was agreed that very little value would be added by increasing this sample size.
Page 21
Prospective or retrospective data collection:
The group agreed that data should be collected prospectively to allow real-time observation of patients, direct queries of both staff and patient records and real-time adjustments to care as required. With the project aim being to improve the care and outcomes of patients, rather than to undertake research into current practice, achieving immediate improvements in care during the process of the project was regarded as supportive of the project aim, and to be encouraged.
Clinical audit indicators:
The group supported the conclusion that the seven Quality Statements within NICE Quality Standard 3: Venous thromboembolism in adults: reducing the risk in hospital should be used as the evidence-base from which to develop the clinical audit indicators. In addition, the group supported feedback from the current NCA providers that the number of clinical audit indicators should be kept to the absolute minimum required to deliver the NCA’s aims.
The group reviewed each quality statement and concluded:
An audit against Quality Statement 1, relating to risk assessment for VTE, replicates data that trusts are already required to collect (monthly) and submit (quarterly) to Unify2 and the group concluded that a national audit against this Quality Statement would not add value
The group considered that an audit against Quality Statements: 2, 3 and 5, which cover the admission process and the admission episode, address the current gap in the availability of information on the quality of prevention of VTE in hospital:
o Quality Statement 2: Patients/carers are offered verbal and written information on VTE prevention as part of the admission process
o Quality Statement 3: Patients are provided with anti-embolism stockings have them fitted and monitored in accordance with NICE guidance
o Quality Statement 5: Patients assessed to be at risk of VTE are offered VTE prophylaxis in accordance with NICE guidance
It was concluded that an audit against these Quality Statements would provide significant opportunity for trusts to improve care and prevent a significant number of hospital-associated VTEs.
The group reviewed the utility of including audit against Quality Statement 4, the reassessment of patients within 24 hours of admission for risk of VTE and bleeding. Whilst the value of reassessing patients was not disputed, the group considered that this would be difficult to define and measure in a real-world situation, and recommended that it be excluded from the initial phase of the NCA.
Finally, the group considered Quality Statements 6 and 7, which relate to the discharge process and events post-discharge. Whilst an audit of practice against these Statements would provide feedback that would support improvements in practice, it would require an additional approach to data collection.
In conclusion, the group considered that focusing on Quality Statements 2, 3 and 5 would provide the most opportunity for quality improvement with the least burden and financial cost to trusts, and recommended that audit criteria be developed against these Quality Statements in the first instance.
Page 22
Once evidence of improvement in care in these key areas is achieved, the group recommended that an NCA provider review the utility of developing an audit approach to address Quality Statements 4, 6 and 7.
Data Collection:
The group considered feedback from those working in trusts across England, which described the wide variability in access to IT support, in particular, mobile technology that would enable data entry at the patient bedside. All trusts will, however, have access to computers that would allow data entry into a web-based tool following completion of a paper form at the bedside.
It was recognised that the staff collecting data for the NCA are likely to be VTE nurses, pharmacists and doctors, and staff numbers and grades, and ways of working, will vary to a great degree between organisations. To enable trusts to manage data collection and entry in a way that minimises the burden, the group recommended that both paper and web-based data entry forms be developed, that data can be entered on individual patients or in batches, and that data can be entered at any time over a three-month period, to fit with individual trusts’ competing priorities.
Data quality and validation:
The group concluded that an NCA should recommend that data be collected by senior medical staff, specialist haematology and/or VTE medical staff, VTE nurses or pharmacists in order to ensure the data collected will meet the required standard.
This group supported the conclusions of Methodology Session One that the best practice from the National Emergency Laparotomy Audit in relation to data validation should be adopted. It therefore recommended that trusts receive guidance on local validation from the central NCA team, and are then provided with a 4-week window after the data entry period for local validation, during which trusts will be able to review and edit their data entries. After the 4-week window period, data will then be ‘locked down’.
In addition, the group supported the approach taken by several other NCAs whereby the central audit team will provide a window of time for trusts to review their annual data, address any data quality issues and provide the facility for trusts to add contextual information to the annual report.
Information governance and patient confidentiality:
The group considered the value of collecting patient-identifiers at a national level, for example to enable subsequent triangulation of national data with other data sources. It concluded that the use of patient-identifiable data would not add value to the NCA and should, therefore, be avoided in line with Caldicott recommendations.
The group concluded that trusts may wish to keep patient-identifiers locally, in order to achieve rapid improvement in patient care, e.g. to follow-up patients who should have received VTE prophylaxis and for whom no evidence of prophylaxis provision was identified. This can be achieved through the application of trusts’ local clinical audit and confidentiality policies.
Data analysis and reporting:
The group supported feedback from NCA providers which recommended that analysis be limited to simple statistics, provided graphically and focus specifically on the clinical audit indicators.

Page 23
Recommendations from the Advisory Board Workshop were reviewed and refined at the July CSG and endorsed at the September CSG.
3.4 Step 4 - Developing and Piloting a Data Collection Tool Prototype
A draft Data Collection Tool and accompanying guidance was developed, based on the outputs of the Advisory Board Workshop and feedback from the CSG, the Study Management Team and Project Working Group.
Following review by medical, nursing and pharmacy experts the tool was piloted in three exemplar and two non-exemplar trusts in South London (see Appendix One for full list).
The pilot was conducted over three weeks in September 2017 and each participating trust was asked to assess a minimum of 40 patients (ten from each area of care- medical, surgical, critical care and maternity teams) using the Data Collection Tool. It should be noted that all auditors involved in the pilot were consultants, pharmacists or nurses who were specialists in VTE prevention and management. There was no induction to the form or guidance given, as it was recognised this would not be provided with the introduction of an NCA. Participating trusts were, however, able to contact the Study Management Team for advice.
Once the pilot was concluded, feedback sessions were held with participating trusts who could also provide feedback via an online survey tool. Feedback was requested on the tool (the clarity of its questions, ease of use and the time it took to complete) and on the guidance (usefulness, accuracy and completeness).
Comments included:
While it took time for auditors to become familiar with the tool, overall it was clear and succinct
Collecting the required information to complete the data collection tool would take more time for those without electronic patient records as locating the patient notes / drug charts can be time consuming:
o Once the records were located a site without electronic records took approximately three minutes per patient to complete the tool
o A site with electronic patient records found it took five to eight minutes per patient
Final guidance should include a Frequently Asked Questions section
All feedback was considered by the Project Working Group before accepted amendments and additions were made to create final versions of the documents (see Appendix Four).
Conclusions:
While further refinement will be required, the final data collection tool prototype provides a comprehensive base for the development of a tool for use within the NCA that is clear, easy to use and acceptably quick to complete.

Page 24
3.5 Statistical Analysis Plan:
Building on the opinion of the Advisory Board, and following consultation with the King’s College London Unit for Medical Statistics, it was determined that the feasibility study did not require the input of a statistician, and that the NCA would need just basic calculations in the form of percentages and averages.
Based on these recommendations a statistical analysis plan was not commissioned as part of the feasibility study.
3.6 Outcomes measurement
From the outset, the aim of the CSG was to ensure that the feasibility study specifically focused on the ability of an NCA of VTE Prevention to drive improvements in patient outcomes. The literature review identified that there are significant methodological challenges with hospital-level outcome measurement due to surveillance bias, the lack of standardised risk adjustment models, and the lack of patient reported outcomes measures (PROMs). There is, however, the NHS Outcomes Framework Indicator 5.1 which uses Hospital Episode Statistics and Office for National Statistics data to report on deaths from VTE within 90 days of discharge from hospital at a national level. The CSG concluded that this indicator should be used as the outcomes metric for a national clinical audit of VTE.
3.7 Limitations of the feasibility study
The study scope set by the commissioners excluded the collection of any information directly from patients.
The pilot only included sites in South London, and three of the five sites are part of the National VTE Exemplar Network.

Page 25
4. National Clinical Audit for VTE Prevention - is this feasible?
In 2010 VTE prevention was named the top clinical priority for hospitals and the national VTE prevention programme came into being. Seven years on, risk assessment rates for VTE appear excellent and there has been a demonstrable improvement in outcomes. However, a substantial burden of hospital-associated thrombosis remains, and many trusts have failed to progress beyond the focus on VTE risk assessment to audit the delivery of appropriate prophylaxis, as well as the provision of information to patients. System levers supporting VTE prevention have either fallen away or fail to be enforced at a local or commissioning level. Including VTE as an NCA will ensure it remains high on the quality and patient safety agenda for trusts and CCGs alike.
This study examined the feasibility of an NCA for VTE prevention in hospital. The first step was an exhaustive literature review confirming the very considerable burden of disease due to HAT and the ability to prevent such events by use of prophylaxis. Available data sources for the different elements of the VTE prevention pathway and outcome measures were examined, with particular emphasis on the utility of such data as well as data quality. Rather than to ‘reinvent the wheel’, we determined to learn the lessons from existing NCAs.
Five NCAs were selected, based on similarities of approach as well as effectiveness and impact on achieving quality improvement. Many valuable insights were gained from this process, regarding the set-up and ongoing management of NCAs and strategies to drive quality improvement. This included optimising communications and engagement with stakeholders and a focus on patient involvement throughout. Practical tips on data collection as well as design of electronic data entry tool were especially useful. Following this process, sequential methodology based sessions and an advisory board workshop informed development of the methodology for the VTE prevention NCA. The last step was development of a prototype data collection tool that was piloted in five trusts in South London.
This study confirmed that it is feasible for VTE prevention to be audited using a systematic approach. The NICE QS3 provides a perfect framework for audit, and inclusion in the NCA would offer an ideal opportunity to drive its implementation in clinical practice. A sound methodological approach to the NCA was developed and the pilot suggests that such an audit would be practicable and not overly burdensome. Such an audit would be useful both at local and national level and help to drive improvements in VTE prevention, which should ultimately impact on HAT rates and mortality.

Page 26
5. Recommended design of a future NCA for VTE prevention in
hospital
5.1 Improvement aims
To support implementation of the national VTE prevention programme that aims to reduce avoidable harm and death from VTE.
To support adherence to the NICE Quality Standard for VTE prevention (QS3)
5.2 Patient groups
Included:
All adult (18 years +) patients admitted for NHS funded care (within an NHS trust or independent sector providers of NHS services) under the following teams: medical, surgical (including day surgery patients recorded as in-patients), maternity and critical care.
Excluded:
Patients not admitted to an acute NHS trust, including emergency department patients, outpatients; and patients admitted to NHS mental health trusts.
5.3 Methodology
5.3.1 Sample
A random sample, identified by trusts using guidance to be provided by the NCA team, of patients anytime from the first 24 hours of admission but no later than 10 days post admission.
5.3.2 Sample Size
Ten percent of the hospital bed numbers (patients) per hospital and a minimum of a total of 50 for each trust.

Page 27
5.3.3 Clinical audit indicators
Clinical audit indicators should be explicitly based on NICE QS3 Quality Statements 2, 3 and 5 as follows:
NICE Quality Standard 3 The NCA clinical audit indicators:
Quality statement 2 Clinical audit indicator 1: There is evidence of that written patient/carer information on VTE prevention was provided to patients/carers as part of the admission process
Quality statement 3 Clinical audit indicator 2: There is evidence that the patient has been provided with anti-embolism stockings
Clinical audit indicator 3: There is evidence that patients have anti-embolism stockings fitted and monitored in accordance with NICE guidance
Quality statement 5 Clinical audit indicator 4: There is evidence that patients assessed to be at risk of VTE are offered anticoagulant VTE prophylaxis in accordance with NICE guidance
5.3.4 Data collection and data entry
Electronic and paper copies of the data collection form (based on the prototype developed in the feasibility study (see Appendix Four) should be developed.
Data should be collected quarterly, with trusts having the ability to enter data at any time within the quarter.
The NCA guidance should recommend that the data is collected by senior and/or specialist haematology/VTE medical staff, nurses or pharmacists. It should also include the detail of NICE guidance in relation to the fitting and monitoring of anti-embolism stockings and the prescription of VTE prophylaxis medication.
Data should be entered electronically and submitted a web-based form.
5.3.5 Validation
The following should be provided by the central NCA team:
Guidance on local validation of data
A four week window after the data entry period should be provided for local validation before the data is ‘locked down’
A one-month validation period at the end of the data entry year to enable review, completion and editing of data annually prior to publication of results within an annual report
The facility for trusts to add contextual data to the annual report
5.3.6 Information governance and patient confidentiality
Page 28
No patient identifiable information to be submitted centrally.
5.4 Data Analysis
Data should be analysed by the central NCA team specifically against the clinical audit indicators based on the NICE Quality Statements (as shown in table above in 5.3.3) using the following numerators and denominators:
Clinical Audit Indicator 1
Proportion of patients/carers who are offered verbal and written information on VTE prevention as part of the admission process.
Numerator: the number of patients/carers who are offered verbal and written information on VTE prevention as part of the admission process
Denominator: the number of patients in the audit sample.
Clinical Audit Indicator 2
Proportion of patients assessed as requiring anti-embolism stockings who have them provided
Numerator: number of patients with stockings
Denominator: number of patients in the audit sample who are risk-assessed as requiring stockings
Clinical audit Indicator 3
Proportion of patients that have anti-embolism stockings fitted and monitored in accordance with NICE guidance
Numerator: number of patients with anti-embolism stockings fitted and monitored in accordance with NICE guidance
Denominator: number of patients in the audit sample provided with anti-embolism stockings.
Clinical Audit Indicator 4
Proportion of patients assessed to be at increased risk of VTE who are offered anticoagulant VTE prophylaxis in accordance with NICE guidance
Numerator: the number of patients who are prescribed anticoagulant thromboprophylaxis in accordance with NICE guidance
Denominator: the number of patients in the audit sample assessed to be at increased risk of VTE without a contra-indication for anticoagulant thromboprophylaxis.
As per the statistical report, simple descriptive statistics will be used for the data analysis.
Page 29
5.5 Reporting
Trusts should have access to their quarterly results against the clinical audit indicators as soon as possible following the quarterly ‘lock-down’ of data entry. This will facilitate rapid local quality improvement and the generation of a participation rate report at a frequency that supports their audit and quality improvement cycles.
The annual report should include trust (and site) identifiable comparison data against the clinical audit indicators. To ensure that the context of the audit results is understood, the annual report must provide the facility for trusts to add comments on their results should they wish to do so.
The report should include data on NHS performance against the NHS Outcomes Framework VTE indicator to provide the opportunity for association between the national audit results and patient outcomes.
5.6 Information Governance
As patient-identifiable data will not be collected at a national level, information governance requirements will be minimal. Trusts may choose to collect and store patient identifiable information locally and this will be subject to trusts’ own confidentiality and information governance policies.
5.7 Outcome Measurement
The NHS Outcomes Framework: Indicator 5.1: Deaths from venous thromboembolism related events within 90 days post discharge from hospital should be used as the key outcome measure for an NCA of VTE prevention and, as outlined above, information on NHS performance against this indicator should be included in the NCA Report.
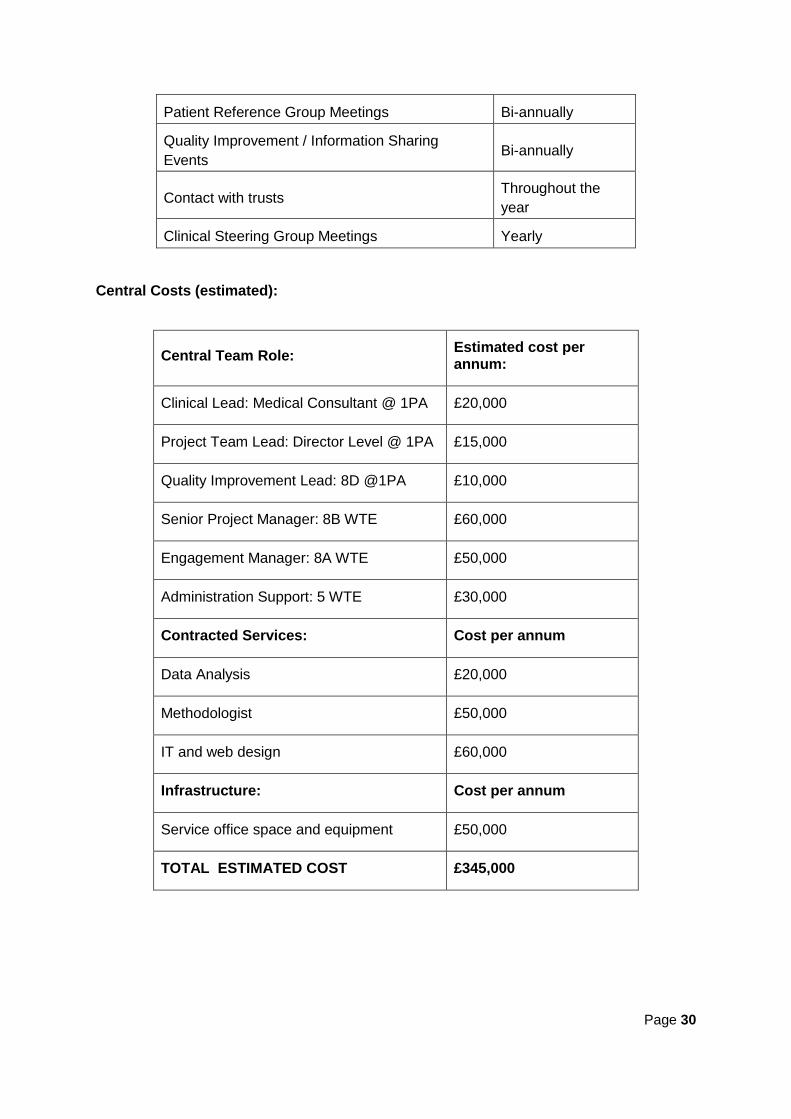
5.8 Key activities and resource requirements for first phase (three years)
During the first phase we anticipate that the first year would be a period of set-up, in order to establish the NCA. This would include recruiting to a central NCA team, and further developing the audit methodology, for example setting up data collection tools and information governance processes. Throughout this initial year it would also be important to develop links and engagement with VTE and audit specialists across all trusts nationally, and involve patients in the development process. Once the audit is fully established, we would expect the activities in the table below to be carried out routinely (i.e. years 2 and 3):
Activities: Timeframes:
Project Team Meetings Monthly
Export and Analysis of data Quarterly
Provision of local reports pre-data validation Quarterly
Provision of local reports post-data validation Quarterly
Publication of National Report Annually
Project Board Meetings Bi-annually
Page 30
Patient Reference Group Meetings Bi-annually
Quality Improvement / Information Sharing
Events Bi-annually
Contact with trusts Throughout the
year
Clinical Steering Group Meetings Yearly
Central Costs (estimated):
Central Team Role: Estimated cost per annum:
Clinical Lead: Medical Consultant @ 1PA £20,000
Project Team Lead: Director Level @ 1PA £15,000
Quality Improvement Lead: 8D @1PA £10,000
Senior Project Manager: 8B WTE £60,000
Engagement Manager: 8A WTE £50,000
Administration Support: 5 WTE £30,000
Contracted Services: Cost per annum
Data Analysis £20,000
Methodologist £50,000
IT and web design £60,000
Infrastructure: Cost per annum
Service office space and equipment £50,000
TOTAL ESTIMATED COST £345,000
Page 31
6. Further recommendations for a future National Clinical Audit
for Prevention of VTE in Hospital
6.1 Quality improvement activities
It will be vital that avenues be created for the NCA central team to share information with participants and for participants to share information with one another. It is envisaged that information shared would include best practice, challenges faced/solutions found and notification of any relevant publications or upcoming events.
Ideally, in the set-up phase of the NCA, the central team would canvas participants to establish any preferences and views on the most effective approach.
Options could include:
Monthly / bi-monthly newsletters (via email) published by the central team including:
o contributions from participating trusts
o news, updates and general information related to the NCA
VTE exemplar network events – regional and local (meetings, conferences,
workshops)
Exhibits / poster presentations at relevant conferences, forums and scientific events
An outlier alert process to be developed by the central national audit team, to ensure
that the Chief Executive and Medical Director of trusts with the poorest performance
are alerted and can take urgent improvement actions
In addition, the future NCA would be supported by the National VTE Exemplar Centres Network which was established by Department of Health in 2007 to develop and disseminate best practice in VTE prevention. There are currently 28 centres of excellence for VTE across the country, with demonstrable high levels of compliance with the national VTE prevention programme and excellent engagement with VTE audit and root cause analysis of HAT. Such centres can provide regional hubs to promote quality improvement activities around VTE prevention as well act as a resource to support implementation of a NCA of VTE prevention. Under the aegis of such an audit, the Exemplar Network would also participate in collaborative audit and research to inform improvements in quality improvement methodologies and ultimately in VTE care and outcomes.
6.2 Additional audits to consider
The first phase of the NCA will focus on standard audit to establish the national context:
This will identify those areas and issues of concern and in need of improvement, the
intention being to investigate these further through ‘themed’ audits, such as VTE
prevention for cancer patients and/or VTE prevention for patients with additional
communication needs
Feedback from trusts during the feasibility study was that an organisational audit
would be of limited value due to the difficulty in assessing the comparability of roles
and titles within trusts. A national audit team may wish to reconsider and/or take
more views. For example, it may be useful specifically to consider an audit of the
training needs of trust staff to establish a baseline, standards and action required
Page 32
Appendices
Glossary, acronyms and abbreviations
Listed as they appear in the report:
VTE: venous thromboembolism
DVT: deep vein thrombosis
PE: pulmonary embolism
A venous thromboembolism is a blood clot that forms in a vein, most commonly a leg vein where it is known as a deep vein thrombosis (DVT) or pulmonary embolism (PE) if the thrombus is dislodged and travels through the circulation to the lungs
HAT: Hospital Associated Thrombosis
A thrombosis associated with a hospital admission
NCA: National Clinical Audit
An audit covering national performance in the management of particular health conditions and diseases
NHS England NHS England leads the National Health Service (NHS) in England, setting its priorities and direction and encourages and informs the national debate on improving health and care
NICE: National Institute for Health and Care Excellence
National Institute for Health and Care Excellence exists to improve outcomes for people using health and social care service by providing national evidence based advice, quality standards and performance indicators and a range of information, including:
- Clinical Guidance 92 VTE: reducing the risk for patients in hospital
- Quality Standard 3 VTE in adults: reducing the risk in hospital
NHS England National VTE Prevention Programme
Instituted in 2010 to make VTE prevention a top clinical priority for hospitals. The programme aimed to ensure that all adult patients admitted to hospital were risk assessed for VTE and where necessary given prophylaxis in line with recognised clinical guidance
All Party Parliamentary Thrombosis Group
The All-Party Parliamentary Thrombosis Group is a cross-party group of MPs and peers, which seeks to raise awareness about the risk and management of venous thromboembolism (VTE) through research reports, meetings in parliament and monitoring the implementation of government initiatives
National VTE Exemplar Centres Network
Consists of NHS trusts and private healthcare providers awarded exemplar status in recognition of an established record of accomplishment in excellence in VTE prevention, care and education
Page 33
CQUINS:
Commissioning for Quality and Innovation Scheme
Commissioning for Quality and Innovation Scheme is a financial incentive scheme to drive improvement within the NHS
NHS National VTE Risk Assessment Tool
The NHS tool endorsed by Department of Health and NICE for the risk assessment of all adults admitted to hospital
PROMs: Patient related outcome measures
Patient Reported Outcome Measures (PROMs) assess the quality of care delivered to patients from the patient perspective
UNIFY2 An online collection system used for collating, sharing and reporting NHS and social care data
NHS Improvement NHS Improvement is responsible for overseeing trusts (Foundation and NHS) and independent providers that provide NHS-funded care
NHS Standard Contract The contract mandated by NHS England for use by commissioners for all contracts for healthcare services other than primary care
HQIP NCAPOP
Healthcare Quality Improvement Partnership
National Clinical Audit and Patient Outcomes Programme
The Healthcare Quality Improvement Partnership is responsible for the management and commissioning of the National Clinical Audit and Patient Outcomes Programme on behalf of NHS England, the Welsh Government and other devolved authorities
HIN Health Innovation Network
Health Innovation Network is the Academic Health Science Network for South London – one of 15 across England
NHS Outcomes Framework
Framework and indicators that hold the NHS to account for improvements in health outcomes
Page 34
Appendix One - Acknowledgements
Name Role Contribution
Richard Armstrong
Head of Health Solutions, Northgate Public Services
NCA Interviewee
Professor Roopen Arya
Professor of Thrombosis and Haemostasis, King’s College London and Director of King’s Thrombosis Centre, King’s College Hospital NHS Foundation Trust
Clinical Lead for Study,
Member: Clinical Steering Group and Project Working Group
Dr Sangeeta Atwal
Consultant Haematologist, Kingston Hospital NHS Foundation Trust
Member, Clinical Steering Group and pilot participant
Kiran Bhangu Project Manager, Health Innovation Network
Member: Study Management Team & Project Working Group
Donna Boreham-Downey
Programme Manager, Health Innovation Network
Lead, Study Management Team and Member, Project Working Group
Chris Boulton Programme Manager, Falls and Fragility Fracture Audit Programme
NCA Interviewee
Sally Brearly Patient Representative Member, Clinical Steering Group
Andy Cantrell Quality Improvement and Patient Safety Manager, Guy’s & St Thomas’s NHS Foundation Trust
Participant, Methodology Development Sessions
Rebecca (Becky) Chanda
Senior Pharmacist – Anticoagulation, Guy’s and St Thomas’ NHS Foundation Trust
Member, Clinical Steering Group and Pilot participant
Nancy Dixon Director of Strategic Services, Healthcare Quality Quest
Participant, Advisory Board Workshop
Simon D’Mello, Haemostasis & Anticoagulation Pharmacist, St George’s University Hospitals NHS Foundation Trust
Pilot Participant
Simon Freathy Venous Thromboembolism Specialist Practitioner, Portsmouth Hospitals NHS Trust
Participant, Advisory Board Workshop
Page 35
Emma Gee
VTE Consultant Nurse, King’s College Hospital NHS Foundation Trust and Lead, National Nursing and Midwifery VTE Exemplar Centre Network
Member, Clinical Steering Group and participant: Methodology Development Sessions, Advisory Board Workshop and pilot
Tracy Graham Anticoagulation and Thrombosis Clinical Nurse Specialist, University Hospital Southampton NHS Foundation Trust
Participant, Advisory Board Workshop
Richard Greenall
VTE Prevention Clinical Nurse Specialist, King’s College Hospital NHS Foundation Trust
Pilot participant
Dr Sophie Harris
Innovation Fellow and Honorary Diabetes Registrar, Health Innovation Network
Member, Clinical Steering Group
Sasha Hewitt Associate Director, Healthcare Quality Improvement Partnership
Observer, Clinical Steering Group
Alex Hoffman Stroke Programme Manager, Sentinel Stroke National Audit Programme
NCA Interviewee
Tasneem Hoosain
Project Manager, Healthcare Quality Improvement Partnership
Observer, Clinical Steering Group
Professor Beverley Hunt
Professor of Thrombosis and Haemostatis, Kings College London, Consultant, Guy’s and St Thomas’ NHS Foundation Trust, Clinical Lead in Haematological Sciences at Viapath and Medical Director, Thrombosis UK
Member, Clinical Steering Group and Pilot participant
Jo Jerome CEO, Thrombosis UK Participant, Advisory Board Workshop
Zoë Lelliott Director for Strategy and Performance, Health Innovation Network
Deputy Chair, Clinical Steering Group and Member of Project Working Group
Jose Lourtie Programme Manager, National Emergency Laparotomy Audit
NCA Interviewee
Kirsty MacLean Steel
Project Manager, National Confidential Enquiry into Patient Outcomes and Death
Member, Clinical Steering Group & Participant, Methodology Development Sessions

Page 36
Joscelin Miles National Clinical Audit and Outcome Review Lead, Royal Free Hospital NHS Trust
Participant, Methodology Development Sessions
Anneka Mitchell
Specialist Trauma and Orthopaedic Pharmacist, University Hospital Southampton NHS Foundation Trust
Participant, Advisory Board Workshop
Dr Tony Newman-Sanders
Medical Director, Health Innovation Network (HIN)
National Clinical Director for Clinical Diagnotics, NHS England
Chair, Clinical Steering Group
Dr Melvina Owusu
Expert Methodologist, Purple Pen Expert Advice
Claire Palmer Head of Patient Outcomes, King’s College Hospital NHS Foundation Trust
Member: Clinical Steering Group and Project Working Group
Jig Patel
Clinical Senior Lecturer and Honorary Consultant Pharmacist in Anticoagulation, King’s College Hospital NHS Foundation Trust
Facilitator, Advisory Board Workshop
Sheena Patel Lead Anticoagulation Pharmacist, Chelsea and Westminster NHS Foundation Trust
Member, Clinical Steering Group and Participant, Advisory Board Workshop
Christina Perkins
Patient Representative and Volunteer, Thrombosis UK
Participant, Advisory Board Workshop
Mathew Porteous
Chair, Regional Clinical Coordinators Committee, National Joint Registry
NCA Interviewee
Professor Gerry Rayman
Consultant Diabetologist, The Ipswich Diabetes Centre and Research Unit, Ipswich Hospital NHS Trust,
Honorary Professor University of East Anglia and Clinical Lead of the National Diabetes Inpatient Audit, NHS Digital
NCA Interviewee
Stephanie Rivera
VTE Prevention Clinical Nurse Specialist, King’s College Hospital NHS Foundation Trust
Pilot participant
Dr Lara Roberts
Consultant Haematologist, King’s College Hospital NHS Foundation Trust
Member, Clinical Steering Group
Page 37
Dr Shalini Solanki
Consultant Haematologist, Croydon Health Services NHS Trust
Pilot Participant
Dr Susie Shapiro
Consultant Haematologist, Oxford University Hospitals NHS Foundation Trust
Participant, Advisory Board Workshop
Dr James Uprichard
Consultant Haematologist, St George’s University Hospitals NHS Foundation Trust
Member, Clinical Steering Group and pilot Participant
Dr Bob Young
Clinical lead National Diabetes Audit; formerly Consultant Physician and Director of Clinical Effectiveness Salford Royal Hospital
NCA Interviewee

Page 38
Appendix Two - Literature Review Summary
Introduction:
The literature review included a review of online and published information in relation to venous thromboembolism (VTE). Its scope included the clinical and national organisational context of VTE prevention, VTE best practice, measuring VTE prevention performance and achieving improvement in VTE prevention practice. It also included a review of literature on national clinical audit methodology best practice.
Summary: Clinical context
VTE is extremely frightening and unpleasant for patients (NHS Choices). VTE is an important cause of death in hospital patients (NICE, 2010a), with nearly 9,000 deaths associated with hospital admission in 2015-16, a prevalence of 64.3 per 100,000 admissions in 2015-16 (NHS Digital – NHS Outcomes Framework, Feb 17). Non-fatal VTE is a significant cause of long-term disability and chronic ill-health (NICE, 2010a, NHS England online).
Approximately half of VTEs are associated with hospital admission and the mean rate of hospital-associated thrombosis is 1.26 per 1000 admissions, increasing to 3.83 per 1000 admissions after exclusion of low risk VTE cohorts (Roberts et al, 2013). Effective management of VTE would result in a net saving to the NHS estimated at £0.8 million annually (NICE, 2010b).
The incidence of VTE in hospital settings can be significantly reduced with the use of anticoagulant and/or mechanical thromboprophylaxis (Geerts et al, 2008; Roberts, Durkin & Arya, 2017), however studies indicate that even high-risk patients often do not receive mechanical or pharmacological VTE prevention (Rashid et al, 2005; Cohen et al, 2008; MBRRACE-UK, 2016; Roberts, Durkin & Arya, 2017).
Both NICE and the national VTE Prevention Programme recommend that all patients are assessed on admission to identify those at increased risk of VTE and that prophylaxis is provided to all patients where it is not specifically contraindicated.
Summary: National organisational context
A raft of national initiatives since 2005 have raised clinical and public awareness of VTE, and leadership for VTE prevention comes from Government (All Party Parliamentary Thrombosis Group) as well as from hospitals themselves (VTE Exemplar Network). Financial incentives applied through CQUINs between 2010 and 2014 led to a significant increase in the risk-assessment of VTE (Roberts, Durkin & Arya, 2017). The current NHS Standard Contract (NHS England, 2016) requires all hospitals to undertake VTE risk assessment and prophylaxis in compliance with NICE guidance, root causes analysis of confirmed cases of hospital-associated VTE and local audit of prophylaxis. There is evidence that local audit is not routinely undertaken by Trusts nor is it monitored by CCGs (All Party Parliamentary Thrombosis Group, 2016) and, to date, there has been no national quality improvement initiative targeted at improving prophylaxis for the prevention of VTE.
Summary: VTE best practice
NICE Quality Standard QS3 Venous thromboembolism in adults: reducing the risk in hospital (NICE, 2010b) sets out the priority areas for improving VTE prevention in 7 evidence-based statements, providing a clear framework against which NHS practice can be measured:
Page 39
Statement 1. All patients, on admission, receive an assessment of VTE and bleeding risk using the clinical risk assessment criteria described in the national tool.
Statement 2. Patients/carers are offered verbal and written information on VTE prevention as part of the admission process.
Statement 3. Patients provided with anti-embolism stockings have them fitted and monitored in accordance with NICE guidance.
Statement 4. Patients are re-assessed within 24 hours of admission for risk of VTE and bleeding.
Statement 5. Patients assessed to be at risk of VTE are offered VTE prophylaxis in accordance with NICE guidance.
Statement 6. Patients/carers are offered verbal and written information on VTE prevention as part of the discharge process.
Statement 7. Patients are offered extended (post hospital) VTE prophylaxis in accordance with NICE guidance.
Summary: Measuring VTE performance
Measurement of the process of risk assessment for VTE became a mandatory requirement for the NHS in 2010 (DH, 2010) and national submissions on the numbers of risk assessments undertaken are made through the online data collection system UNIFY2.
The review did not identify any UK or international literature on routine centralised collection of performance information on the use of VTE prophylaxis, although local audit is recommended by both NICE and the US Agency for Healthcare Research and Quality (AHRQ, 2016), as well as being a requirement of the NHS Standard Contract.
There are significant methodological issues in using VTE occurrence as a measurement of the quality of care provided by hospitals, including surveillance bias (Bilimoria et al, 2013; Kinnier et al, 2016), difficulty with risk adjustment (Lau & Haut, 2014) and the accuracy of clinical coding (Roberts, Durkin & Arya 2017).
The literature review concluded that the only routinely-collected data available for a national clinical audit of VTE prevention to use is:
UNIFY2 data on risk assessments
NHS Outcomes Framework data on deaths from venous thromboembolism (VTE) related events.
Summary: Achieving improvement in VTE practice
The literature found some evidence that the collection and feedback of national data may lead to improve VTE practice. Catterick & Hunt (2014) identified an association between the use of the national VTE risk assessment tool and improved patient outcome (Catterick & Hunt, 2014). Local clinical audit and feedback was found to improve VTE prophylaxis (Lau & Haut, 2014), including one study where was linked this to a decrease in preventable VTE.
A Cochrane Library review of audit and feedback (Ivers et al, 2012) concludes that audit and feedback is most effective when healthcare professionals are not performing well to start out with, where the person responsible for audit and feedback is a supervisor or colleague, feedback is provided more than one, given verbally and in writing and includes clear targets
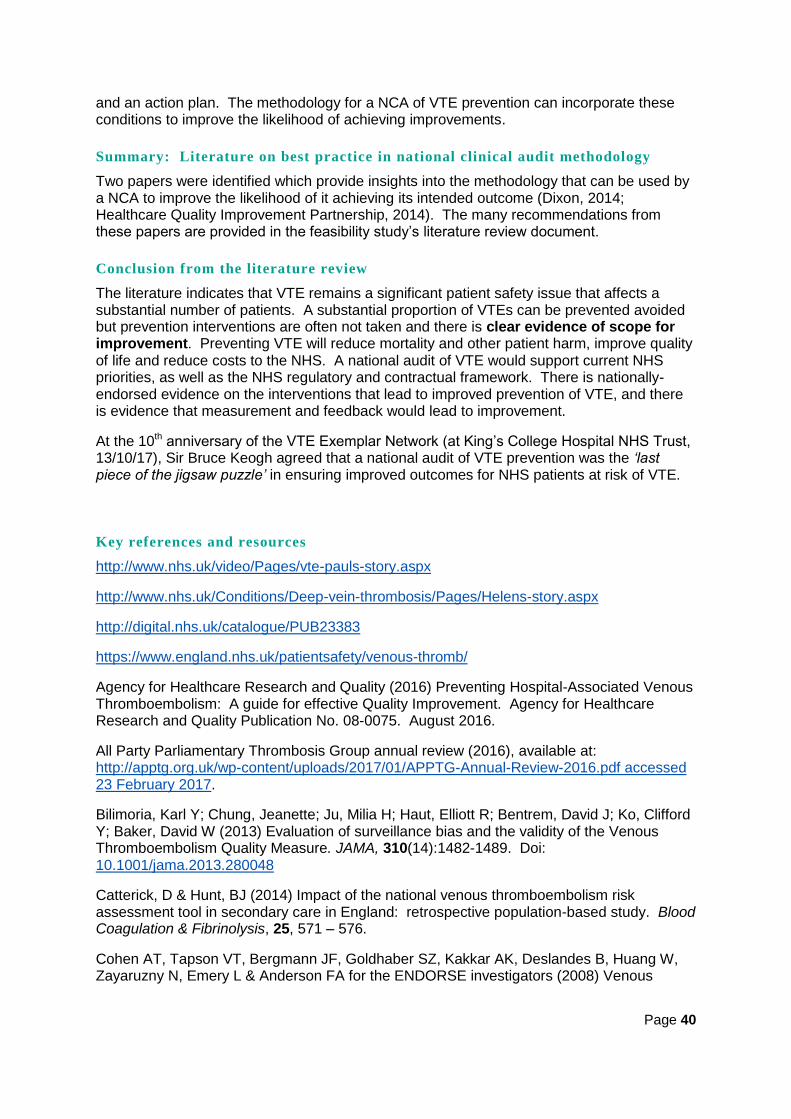
Page 40
and an action plan. The methodology for a NCA of VTE prevention can incorporate these conditions to improve the likelihood of achieving improvements.
Summary: Literature on best practice in national clinical audit methodology
Two papers were identified which provide insights into the methodology that can be used by a NCA to improve the likelihood of it achieving its intended outcome (Dixon, 2014; Healthcare Quality Improvement Partnership, 2014). The many recommendations from these papers are provided in the feasibility study’s literature review document.
Conclusion from the literature review
The literature indicates that VTE remains a significant patient safety issue that affects a substantial number of patients. A substantial proportion of VTEs can be prevented avoided but prevention interventions are often not taken and there is clear evidence of scope for improvement. Preventing VTE will reduce mortality and other patient harm, improve quality of life and reduce costs to the NHS. A national audit of VTE would support current NHS priorities, as well as the NHS regulatory and contractual framework. There is nationally-endorsed evidence on the interventions that lead to improved prevention of VTE, and there is evidence that measurement and feedback would lead to improvement.
At the 10th anniversary of the VTE Exemplar Network (at King’s College Hospital NHS Trust, 13/10/17), Sir Bruce Keogh agreed that a national audit of VTE prevention was the ‘last piece of the jigsaw puzzle’ in ensuring improved outcomes for NHS patients at risk of VTE.
Key references and resources
http://www.nhs.uk/video/Pages/vte-pauls-story.aspx
http://www.nhs.uk/Conditions/Deep-vein-thrombosis/Pages/Helens-story.aspx
http://digital.nhs.uk/catalogue/PUB23383
https://www.england.nhs.uk/patientsafety/venous-thromb/
Agency for Healthcare Research and Quality (2016) Preventing Hospital-Associated Venous Thromboembolism: A guide for effective Quality Improvement. Agency for Healthcare Research and Quality Publication No. 08-0075. August 2016.
All Party Parliamentary Thrombosis Group annual review (2016), available at: http://apptg.org.uk/wp-content/uploads/2017/01/APPTG-Annual-Review-2016.pdf accessed 23 February 2017.
Bilimoria, Karl Y; Chung, Jeanette; Ju, Milia H; Haut, Elliott R; Bentrem, David J; Ko, Clifford Y; Baker, David W (2013) Evaluation of surveillance bias and the validity of the Venous Thromboembolism Quality Measure. JAMA, 310(14):1482-1489. Doi: 10.1001/jama.2013.280048
Catterick, D & Hunt, BJ (2014) Impact of the national venous thromboembolism risk assessment tool in secondary care in England: retrospective population-based study. Blood Coagulation & Fibrinolysis, 25, 571 – 576.
Cohen AT, Tapson VT, Bergmann JF, Goldhaber SZ, Kakkar AK, Deslandes B, Huang W, Zayaruzny N, Emery L & Anderson FA for the ENDORSE investigators (2008) Venous

Page 41
thromboembolism risk and prophylaxis in the acute hospital care setting (ENDORSE study): a multinational cross-sectional study. Lancet, 371, 387 – 394.
Department of Health (2010a) Risk assessment for venous thromboembolism (VTE) http://webarchive.nationalarchives.gov.uk/20130107105354/http:/www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/@dh/@en/@ps/documents/digitalasset/dh_113355.pdf, Accessed 31 January 2017
Dixon, N (2013) Proposed standards for the design and conduct of a national clinical audit or quality improvement study. International Journal of Quality in Health Care 25 (4): 357-365. DOI: https://doi.org/10.1093/intqhc/mzt037
Geerts WH, Bergqvist D, Pineo GF, Heit JA, Samama CM, Lassen MR & Colwell CW (2008) Prevention of venous thromboembolism: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th ed.). Chest, 133, 381 – 431.
Healthcare Quality Improvement Partnership (HQIP) (2014) National Clinical Audit Quality Assessment: Overview of the self-assessment survey: “audit of audits”. Report to the Healthcare Quality Improvement Partnership, 19 December 2014. Imperial College London, HQIP and Centre for Healthcare Improvement.
Ivers N, Jamtvedt G, Flottorp S, Young JM, Odgaard-Jansen A, French SD, O’Brien MA, Johansen M, Grimshaw KJ, Oxman AD. Audit and feedback: effects on professional practice and patient outcome. Cochrane Library, 13/6/2012.
Kinnier, Christine V; Ju, Mila H; Kmiecik, Thomas; Barnard, Cindy; Halverson, Terri; Yang, Anthony D; Caprini, Joseph; Kreutzer, Lindsey; and Bilimoria, Karl Y. Development of a novel composite process measure for venous thromboembolism prophylaxis. Medical Care (2016); 54(2)
Lau, Brandyn D and Haut, Elliott R. (2014) Practices to prevent venous thromboembolism: a brief review. BMJ Quality & Safety 23(3).
Mothers and Babies Reducing Risk through Audit and Confidential Enquiries across the UK (MBRRACE-UK) (2015) Saving Lives, Improving Mothers’ Care Surveillance of maternal deaths in the UK 2011-13 and lessons learned to inform maternity care from the UK and Ireland Confidential Enquiries into Maternal Deaths and Morbidity 2009-13. https://www.npeu.ox.ac.uk/downloads/files/mbrrace-uk/reports/MBRRACE-UK%20Maternal%20Report%202015.pdf accessed 23 February 2017.
NHS England (2016) NHS Standard Contract 2017 – 2019) Available at https://www.england.nhs.uk/nhs-standard-contract/17-18/ accessed 23 February 2017.
NICE (2010a) Venous thromboembolism: reducing the risk for patients in hospital. Clinical Guideline [CG92]. National Institute for Health and Care Excellence. London. http://guidance.nice.org.uk/CG92. Accessed 23 February 2017.
NICE (2010b) Venous thromboembolism in adults: reducing the risk in hospital. Cost impact and commissioning assessment. Quality standard [QS3] National Institute for Health and Care Excellence, London. https://www.nice.org.uk/guidance/qs3/resources/cost-impact-and-commissioning-assessment-quality-standard-for-venous-thromboembolism-vte-prevention-252274141
Rashid ST, Thursz MR, Razvi NA et al (2005) Venous thromboprophylaxis in UK medical inpatients. Journal of the Royal Society of Medicine, 98, 507 – 12.

Page 42
Roberts LN, Porter G, Barker RD, Yorke R, Bonner, L, Patel RK and Arya, R (2013) Comprehensive venous thromboembolism prevention programme incorporating mandatory risk assessment reduces the incidence of hospital-associated thrombosis. Chest, 144, 1276-1281.
Roberts LN, Durkin M & Arya R (2017) Developing a national programme for VTE prevention. British Journal of Haematology, 178, 162-170.
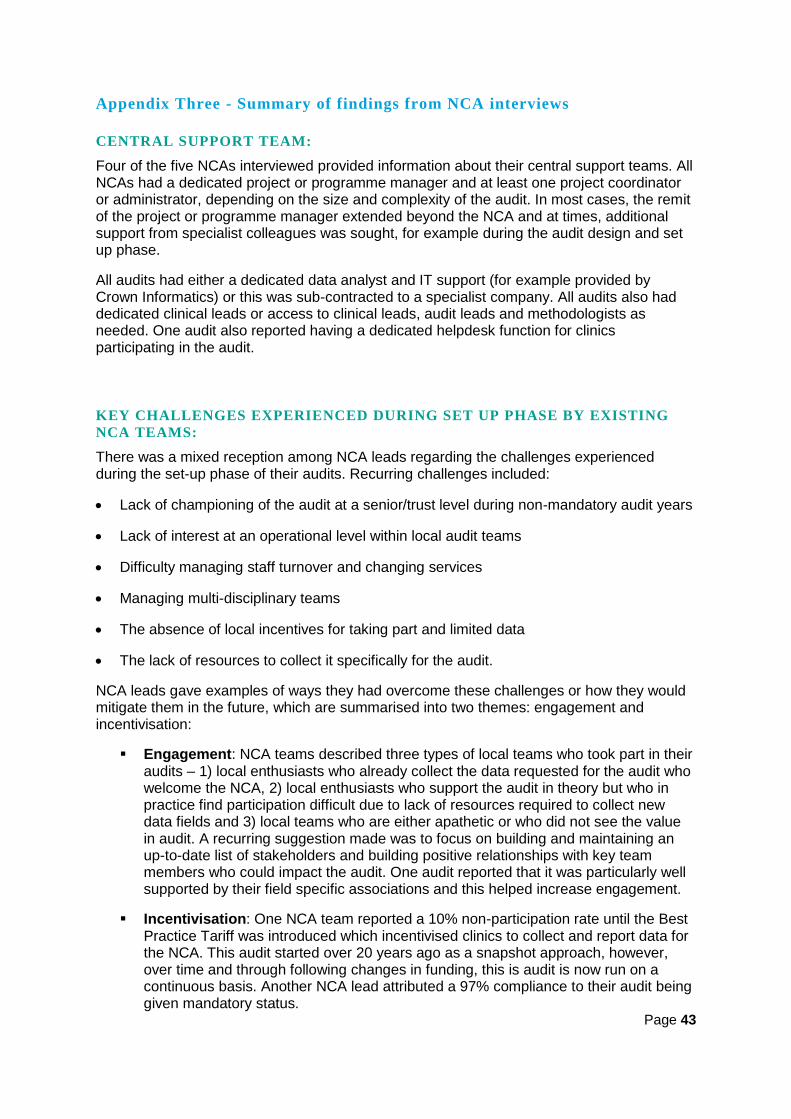
Page 43
Appendix Three - Summary of findings from NCA interviews
CENTRAL SUPPORT TEAM:
Four of the five NCAs interviewed provided information about their central support teams. All NCAs had a dedicated project or programme manager and at least one project coordinator or administrator, depending on the size and complexity of the audit. In most cases, the remit of the project or programme manager extended beyond the NCA and at times, additional support from specialist colleagues was sought, for example during the audit design and set up phase.
All audits had either a dedicated data analyst and IT support (for example provided by Crown Informatics) or this was sub-contracted to a specialist company. All audits also had dedicated clinical leads or access to clinical leads, audit leads and methodologists as needed. One audit also reported having a dedicated helpdesk function for clinics participating in the audit.
KEY CHALLENGES EXPERIENCED DURING SET UP PHASE BY EXISTING
NCA TEAMS:
There was a mixed reception among NCA leads regarding the challenges experienced during the set-up phase of their audits. Recurring challenges included:
Lack of championing of the audit at a senior/trust level during non-mandatory audit years
Lack of interest at an operational level within local audit teams
Difficulty managing staff turnover and changing services
Managing multi-disciplinary teams
The absence of local incentives for taking part and limited data
The lack of resources to collect it specifically for the audit.
NCA leads gave examples of ways they had overcome these challenges or how they would mitigate them in the future, which are summarised into two themes: engagement and incentivisation:
Engagement: NCA teams described three types of local teams who took part in their audits – 1) local enthusiasts who already collect the data requested for the audit who welcome the NCA, 2) local enthusiasts who support the audit in theory but who in practice find participation difficult due to lack of resources required to collect new data fields and 3) local teams who are either apathetic or who did not see the value in audit. A recurring suggestion made was to focus on building and maintaining an up-to-date list of stakeholders and building positive relationships with key team members who could impact the audit. One audit reported that it was particularly well supported by their field specific associations and this helped increase engagement.
Incentivisation: One NCA team reported a 10% non-participation rate until the Best Practice Tariff was introduced which incentivised clinics to collect and report data for the NCA. This audit started over 20 years ago as a snapshot approach, however, over time and through following changes in funding, this is audit is now run on a continuous basis. Another NCA lead attributed a 97% compliance to their audit being given mandatory status.

Page 44
KEY LEARNINGS:
It’s helpful to be seen on the side of audit teams – appreciate that they are very busy and speak their language. Be encouraging at the beginning – “go easy on the stick”.
Have good clinical representation and ownership at trust level and NCA level – these people will be driving the audit forward.
Engage patient reps/managers/clinicians who will be able to implement change.
How an NCA considers outliers determines how staff engage with the audit
Ensure that trusts own their audit data regardless of who collects and submits the data.
AUDIT METHODOLOGY (DATA COLLECTION, SUBMISSION AND
QUALITY):
Three of the five NCA teams interviewed described their audit methodologies; one was a snapshot audit conducted on 15-20% of in-patients admitted with diabetes, while the other two followed the full patient pathway of all patients admitted for stroke and emergency laparotomy. Information about data collection, submission and quality was collected for four out of the five audits.
Audit data is submitted electronically by four of the five NCA teams consulted, using a CSV file or a bespoke web-tool. Where a web-tool is used directly, access is determined at the local level. Some clinics print off the web-tool fields, complete paper records and then enter the data into the web-tool at a later stage. The emphasis for data collection is on validity of data collected as well as compliance and completeness of data fields. A first stage of data validation (logic checks) is built into most web-tool such that clear inconsistencies in data are flagged for review before submission. An example of this is an error flag being raised when the total number of patients discharged exceeds the total number of patients admitted.
The NCA teams noted that a significant amount of time was needed for setting up administrative and information governance processes which support data collection. NCAs also commented on the length of time taken to follow-up with local audit teams and support them in collecting new data fields; they suggest this time should be considered when developing schedules for the audit.
KEY LEARNINGS:
Use a prospective electronic data entry tool, with in-built logic and consistency checks to increase the quality of data submitted and reduce burden for clinics.
Keep the dataset as lean as possible, ensuring a firm threshold on questions are included in the audit. This can be aided by reviewing the dataset annually and removing any questions which are not providing the required information or where the standard has been achieved over several audit cycles.
Avoid or minimise the use of patient identifiable data to limit information governance challenges.
The piloting phase is important for ensuring everything is understood and works as it should at clinic level.
Page 45
DATA ANALYSIS AND REPORTING:
Four of the five NCAs interviewed shared information about data analysis, and reporting. A standard set of analyses is performed on all audit data relating to the specific outcomes under review. Where relevant, the team perform risk-adjustments for mortality data, and make use of HES and ONS data to interpret their findings. In the case of three NCAs, data analysis is subcontracted to specialist teams, namely at NHS Digital, Bristol University and Oxford University.
The frequency of reporting differs between NCAs, though quarterly reporting is seen as the ideal balance between data processing time and timely actionable feedback for local clinics. Each clinic receives their own data ahead of any comparative data, which some NCA teams also highlight at an annual sector conference (or similar event) - before they are published online.
Audit results are presented in a range of styles for different audiences, including run charts and funnel plots which are then included in bespoke slide-decks and reports. Individual clinics’ performance is benchmarked against others in their region, and national comparisons are also made in reports. Comparative data sharing was common among all the NCAs reviewed. One NCA also provides peer-to-peer comparisons for consultants in the field and another is looking to develop this in the future. All audits focussed on sharing performance results relating to key indicators and measures of improvement.
Some NCAs reported that they also provide information in lay formats making it more accessible for the public online, as well as for professionals seeking a summary or easy-view option.
In addition to written reports, some audits also provide live or real-time comparable data online, for example in the form of run charts. These data are dynamic and clinics can choose to view their own data alongside previous years data or alongside other clinics.
KEY LEARNINGS:
Data should be shared with units as quickly as possible. One audit noted that their results were not shared with clinics for the first four to five years of the audit. Compliance at the beginning was around 20% - although it has increased steadily each year. The NCA attributes this to the time lag between data collection and sharing of audit results.
Where possible, data should include regional and national comparisons.
Data should be presented in a range of styles.
Make the audit aspirational but with clear steps and phases to sites can see their progress. This means using measures that are discriminatory enough to show progress.
QUALITY IMPROVEMENT:
To support and drive quality improvement, the NCAs used a range of strategies. One NCA has a dedicated quality improvement lead among their project team who produces and publishes quality improvement animations while another has a dedicated ‘Quality Improvement and Peer-Review Project Manager’ who has been appointed by their Royal College to support trusts for 12 months. In contrast, another audit directly links participation in audits to staff appraisals.
Other methods used to drive quality improvement included:
Annual events focused on quality improvement
Page 46
Identifying outliers and providing support in the following forms:
o Creating an outlier policy and disseminating this to sites
o Signposting clinics who present as outliers to professional associations who offer detailed on-site inspections
o Notifying the CQC through a routine data flow and an annual letter to the CQC Medical Director
o Directed visits with underperforming sites
Deep analysis and case notes tools
A peer review scheme (not funded through HQIP)
Regional improvement workshops
Publications
Conference presentations
NCA sponsored quality improvement awards which showcase studies of clinics’ use of local data
Facilitating shared learning between trusts
KEY LEARNINGS:
A range of approaches can be adopted to drive quality improvement. These include providing support in the form of tools and direct assistance to clinics.
Offering opportunities to share good practice and discuss challenges among peers can be helpful.
COMMUNICATION:
The NCA teams interviewed reported several methods used to communicate with their stakeholders, including online, direct and face-to-face approaches:
Mass online communication: Each NCA has an open-access website which acts as a hub for information about their audit and includes audit results These websites are updated regularly. One NCA also described its use of the social media platform, Twitter.
Direct online communication: In most cases, all communication begins with one or two representatives from each trust, who are nominated by the trust’s Chief Executive Officer and/or Medical Director. These leads are a direct point of contact and responsible for signing-off the completed data. Each NCA produces a newsletter which is either available following subscription or sent directly to nominated audit leads. Any further information is then cascaded to relevant local stakeholders via this nominated lead. One NCA reported that they circulate annual audit reports directly to all clinicians involved in their audit. Another NCA also displays posters in clinics to help inform local teams about the audit.

Page 47
Face-to-face communication: Each NCA varied their communication depending on their resources and the needs of the local audit teams. One NCA reported that they visit sites who may struggle with the audit to offer appropriate support. Another NCA hosts regular events focused on quality improvement which are well attended, however as the cost of delivering this event exceeds available resources, the frequency of the events has been reduced from quarterly to annually.
KEY LEARNINGS:
The audit set up phase would include time to identify and engage senior strategic and operational stakeholders and design appropriate communication methods and events to help build ownership and buy-in among local teams.
Direct and indirect communication methods may prove useful at different points in the audit.
PATIENT INVOLVEMENT:
All five NCAs recognised the importance of patient involvement throughout the audit cycle. Each NCA sought patient feedback in different ways including:
Patient representation on their steering and/or clinical reference groups
Patient experience questionnaires conducted in collaboration with a sector charity and professional institute,
National PROMS programme.
A combination of ad hoc and regular patient groups and events convened to explore specific topics, such as formatting and content of audit reports.
One audit noted the lack of a patient representation on their immediate project team as a gap and they are currently exploring this.
KEY LEARNINGS:
Patients should be invited to join all formal groups involved in the set-up, implementation and communication of the audit data.
Although beyond the scope of the feasibility study, a future NCA of VTE prevention continue to explore ways to obtain robust patient experience data, for example in collaboration with the sector charity, Thrombosis UK.
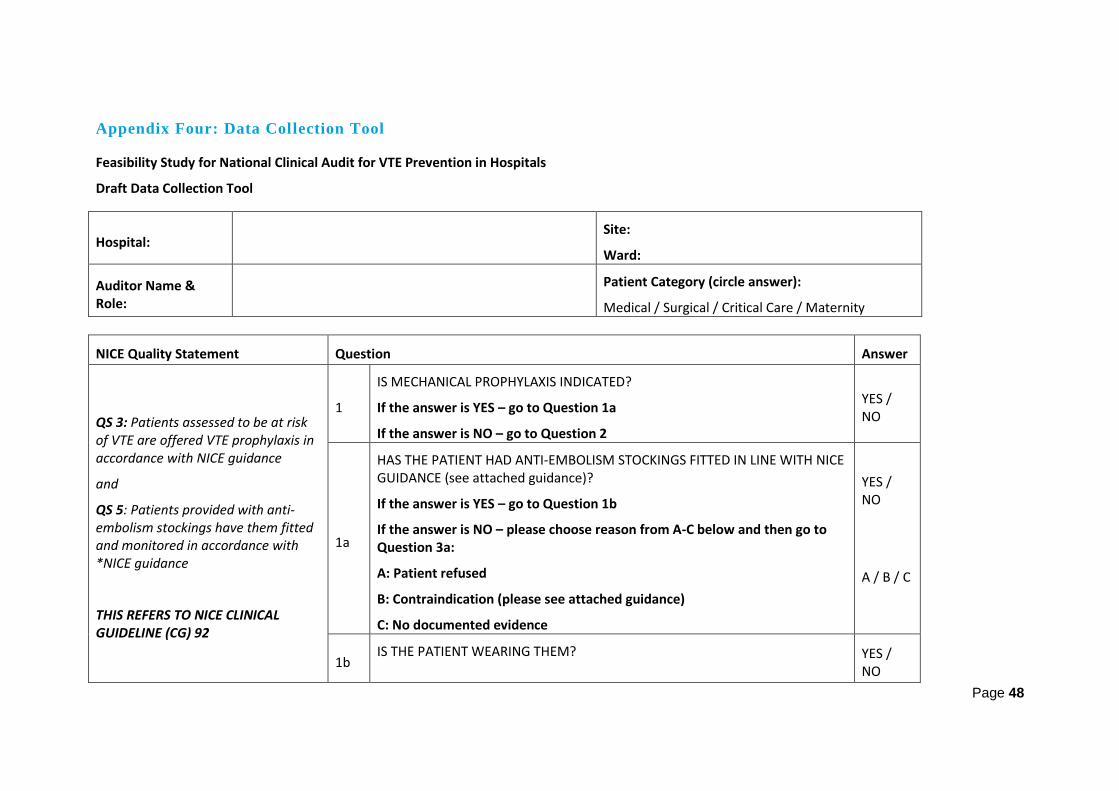
Page 48
Appendix Four: Data Collection Tool
Feasibility Study for National Clinical Audit for VTE Prevention in Hospitals
Draft Data Collection Tool
Hospital: Site:
Ward:
Auditor Name & Role:
Patient Category (circle answer):
Medical / Surgical / Critical Care / Maternity
NICE Quality Statement Question Answer
QS 3: Patients assessed to be at risk of VTE are offered VTE prophylaxis in accordance with NICE guidance
and
QS 5: Patients provided with anti-embolism stockings have them fitted and monitored in accordance with *NICE guidance
THIS REFERS TO NICE CLINICAL GUIDELINE (CG) 92
1
IS MECHANICAL PROPHYLAXIS INDICATED?
If the answer is YES – go to Question 1a
If the answer is NO – go to Question 2
YES / NO
1a
HAS THE PATIENT HAD ANTI-EMBOLISM STOCKINGS FITTED IN LINE WITH NICE GUIDANCE (see attached guidance)?
If the answer is YES – go to Question 1b
If the answer is NO – please choose reason from A-C below and then go to Question 3a:
A: Patient refused
B: Contraindication (please see attached guidance)
C: No documented evidence
YES / NO
A / B / C
1b IS THE PATIENT WEARING THEM? YES /
NO

Page 49
If the answer is YES – go to Question 1c
If the answer is NO – please provide details as to why and then go to Question 1c:
A: Patient refused
B: Contraindication (please see attached guidance)
C: Unable to determine
A / B / C
1c
ARE THEY BEING MONITORED IN LINE WITH NICE GUIDANCE (see attached guidance)?
If the answer is YES – go to Question 2
If the answer is NO – please provide details as to why and then go to Question 3a:
A: Patient refused
B: Contraindication (please see attached guidance)
C: No documented evidence
YES / NO
A / B / C
QS 3: Patients assessed to be at risk of VTE are offered VTE prophylaxis in accordance with *NICE guidance
THIS REFERS TO NICE CLINICAL GUIDELINE (CG) 92
2
HAS THE PATIENT BEEN IDENTIFIED AS AT HIGH RISK OF BLEEDING?
If the answer is YES – go to Question 3
If the answer is NO – go to Question 2a
YES / NO
2a
IS PHARMACOLOGICAL THROMBOPROPHYLAXIS PRESCRIBED IN LINE WITH NICE GUIDANCE, OR AS PER THE LOCAL HOSPITAL’S GUIDANCE?
If the answer is YES – go to Question 2b
If the answer is NO – please provide details as to why and then go to Question 3a:
A: Contraindication (see NICE guidance)
B: No documented evidence
YES / NO
A / B

Page 50
2b
DID THE PATIENT RECEIVE OR IS THE PATIENT DUE TO RECEIVE PHARMACOLOGICAL THROMBOPROPHYLAXIS WITHIN THE FIRST 24 HOURS OF ADMISSION?
If the answer is YES – go to Question 3a
If the answer is NO – please provide details as to why and then go to Question 3a:
A: No documented evidence
B: Contraindication
YES / NO
A / B
QS 2: Patients/carers are offered verbal and written information on VTE prevention as part of the admission process
3a
HAS THE PATIENT (OR THEIR CARER) BEEN PROVIDED WITH WRITTEN INFORMATION ON VTE PREVENTION?
If the answer is YES – please choose either A or B below and then go to Question 3b:
A: Physical evidence (patient information is with the patient)
B: Documented evidence found
If the answer is NO – go to Question 3b
YES / NO
A / B
3b
HAS THE PATIENT (OR THEIR CARER) BEEN PROVIDED WITH VERBAL INFORMATION ON VTE PREVENTION?
A: YES – Documented evidence found
B: NO – No documented evidence
YES / NO
Any other comments:
Health Innovation Network (HIN), October 2017

Page 51
Appendix Five - VTE Exemplar Centre Criteria
Checklist for organisations considering making an application to become a
VTE Exemplar Centre
Tick 1. VTE STRATEGY
a. Chief Executive endorsement
b. Thrombosis committee/VTE Implementation group (or equivalent) established
Cross organisation and multidisciplinary representation (evidence to include relevant organisational chart)
c. VTE Guidance in place for
Clinicians (medicine & surgery)
Maternity
Extended prophylaxis
Tick 2. COMPLIANCE & PROCESSES
a. Risk assessment
Risk assessment system(s) in place
Risk assessment tools utilised
Data demonstrating meeting/exceeding National Quality Requirement of consistently achieving 95% threshold
b. Root cause analysis
Process and staff (flow chart demonstrating how RCA is undertaken, how findings drive improvement and how duty of candour is implemented)
c. Audit
Audit mechanisms in place and staff to support the process
% patients receiving appropriate thromboprophylaxis
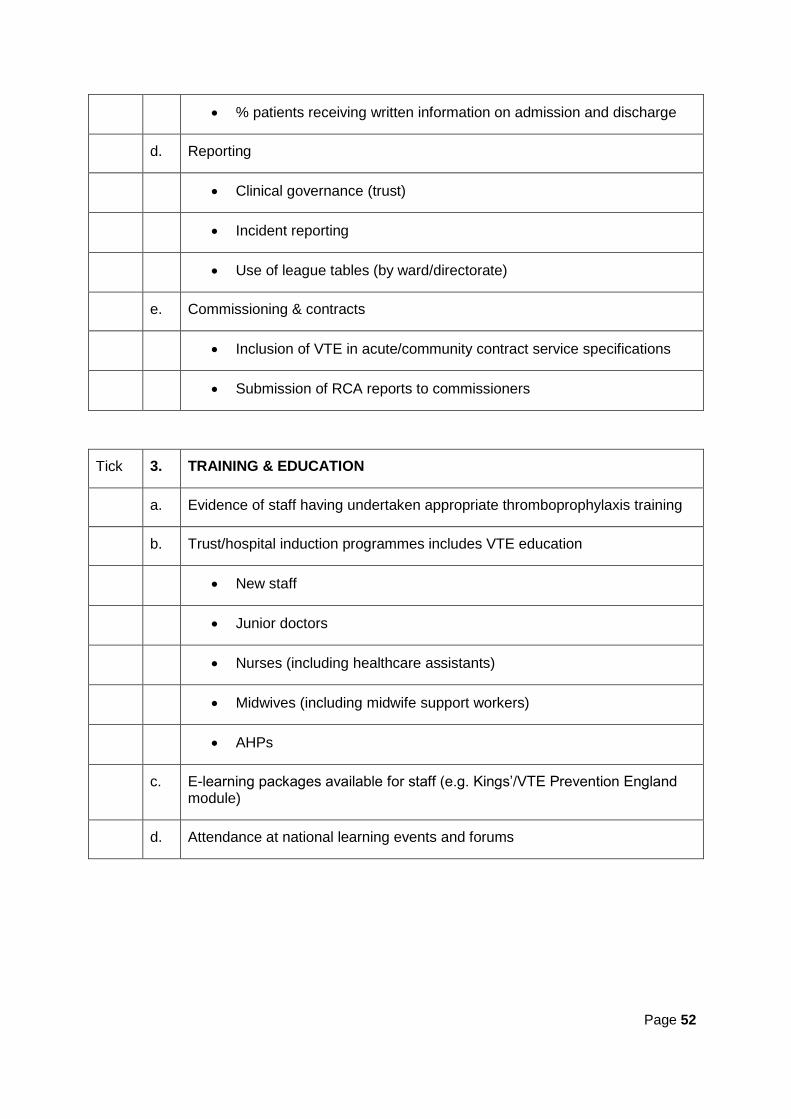
Page 52
% patients receiving written information on admission and discharge
d. Reporting
Clinical governance (trust)
Incident reporting
Use of league tables (by ward/directorate)
e. Commissioning & contracts
Inclusion of VTE in acute/community contract service specifications
Submission of RCA reports to commissioners
Tick 3. TRAINING & EDUCATION
a. Evidence of staff having undertaken appropriate thromboprophylaxis training
b. Trust/hospital induction programmes includes VTE education
New staff
Junior doctors
Nurses (including healthcare assistants)
Midwives (including midwife support workers)
AHPs
c. E-learning packages available for staff (e.g. Kings’/VTE Prevention England module)
d. Attendance at national learning events and forums
Page 53
Tick 4. COMMUNICATIONS
a. Staff
VTE Communications strategy in place
Evidence of communications undertaken (e.g. campaigns, internal communication such as newsletters, intranet, league tables, use of social media e.g. Twitter)
b. Patient (evidenced by audit)
Written information is offered – Patient Information Leaflet
VTE is explained verbally to patients by appropriate member of staff
c. Hospital patient group(s) are informed about VTE
Tick 5. IMPLEMENTATION
a. Establishment of VTE champions by ward/department/speciality
b. Roles and responsibilities of VTE champions
c. VTE process diagram (how implementation is applied across the trust, risk assessment, patient information, discharge, community transition)
Tick 6. PATIENT & COMMUNITY
a. Patient care plans
b. Education for self-injection
c. Transition to the community
Care pathways /protocols established for the transition of patients into community hospitals
Links with primary care (Re. extended prophylaxis, on-going management of VTE)
Page 54
The Health Innovation Network is the Academic Health Science Network for south London
and part of the national AHSN Network.
We are a founding partner of DigitalHealth.London building the global digital capital, together.
@HINSouthLondon
www.healthinnovationnetwork.com