Embed Size (px)
Citation preview

“A Study To Correlate Feeding Practices Of Mothers And Nutritional Status Of
Their Children In A Selected Area, Bangalore”
By
ROSAMMA K. J.
Dissertation submitted to the
Rajiv Gandhi University of Health Sciences, Karnataka, Bangalore
In partial fulfillment
of the requirements for the degree of
Master of Science
In
Paediatric Nursing
Under the guidance of
PROF. J. LOVERA GRACE LILLY RANI
Department of Paediatric Nursing
Sarvodaya College of Nursing
Agrahara Dasarahalli,
Bangalore – 560 079
November 2007

RAJIV GANDHI UNIVERSITY OF HEALTH SCIENCE, KARNATAKA
DECLARATION BY THE CANDIDATE
I, Rosamma K.J. hereby declare that this dissertation / thesis entitled
“A Study To Correlate Feeding Practices Of Mothers And Nutritional Status Of
Their Children In A Selected Area, Bangalore” is a bonafide and genuine research
work carried out by me under the guidance of Mrs. J. Lovera Grace Lilly Rani,
Professor, Department of Pediatric Nursing, Sarvodaya College of Nursing.
Signature of the Candidate Date : Place : Bangalore ROSAMMA K.J.
ii
CERTIFICATE BY THE GUIDE
This is to certify that this dissertation entitled “A Study To Correlate
Feeding Practices Of Mothers And Nutritional Status Of Their Children In A
Selected Area, Bangalore” is a bonafide research work done by Rosamma K.J in
partial fulfillment of the requirements for the award of degree of Master of Science
in Pediatric Nursing.
Signature of the Guide MRS. J. LOVERA GRACE LILLY RANI
Professor
Date: Department of Paediatric Nursing
Place : Bangalore Sarvodaya College of Nursing
Bangalore
iii
ENDORSEMENT BY THE HOD, PRINCIPAL/HEAD OF THE INSTITUTION
This is to certify that this dissertation / thesis entitled “A Study To Correlate
Feeding Practices Of Mothers And Nutritional Status Of Their Children In A
Selected Area, Bangalore” is a bonafide research work done by Rosamma K. J in
partial fulfillment of the requirements for the award degree of Master of Science in
Pediatric Nursing.
Seal & Signature of HOD Seal & Signature of Principal PROF. J. LOVERA GRACE LILLY RANI PROF.T. BHEEMAPPA Date: Date: Place: Bangalore Place: Bangalore
iv
COPY RIGHT
DECLARATION BY THE CANDIDATE
I hereby declare that the Rajiv Gandhi University of Health Sciences,
Karnataka, Bangalore, shall have the rights to preserve, use and disseminate this
dissertation in print or electronic format for academic / research purpose.
Signature of the Candidate Date: Place : Bangalore ROSAMMA K.J
© Rajiv Gandhi University of Health Sciences, Karnataka, Bangalore
v
ACKNOWLEDGEMENT
“Praise the Lord for He is good;
Sing to our God for He is loving;
To Him our praise is due.” (Ps.146:1)
“Gratitude is the attitude of mind and heart.” I raise my heart in gratitude to
God Almighty, who has been my inspiration and guiding force behind all my efforts.
I wish to express my sincere thanks to all who have helped me in
accomplishing this task successfully.
I express my thanks to Mr. V. Narayan Swamy, Chairman, Sarvodaya
Group Of Institutions, Bangalore for his encouragement, support and deep
inspiration to conduct this PG programme in his esteemed institution.
The present study has been completed under the inspiring guidance and
supervision of my guide Prof. J. Lovera Grace Lilly Rani, M.Sc. (N), Head Of The
Department, Paediatric Nursing, Sarvodaya College Of Nursing I express my
deep sense of gratitude for her valuable suggestions, encouragement and keen interest
in the planning and execution of the study. I consider it a great honour and privilege
to complete this study under her supervision.
I express my heartfelt gratitude to Prof. T. Bheemappa, Principal and HOD
of Psychiatric Nursing, Sarvodaya College of Nursing for his valuable advice and
timely support during the study period.
I owe deep gratitude to my Prof. Victorial Selva Kumari M.Sc. (N), Vice
Principal, Sarvodaya College of Nursing, for her encouragement, suggestions,
vi

timely assistance, guidance, genuine interest and moral support at every stage of this
study.
It is my great pleasure and privilege to take up this study under the extensive
support and meticulous corrections of Prof. Hemalatha Ravi MSc (N) Paediatric
Nursing in the initial stages of this study.
I express my sincere gratitude to Mrs. Satya Lawrence M.Sc. (N)
Asst. Professor, Dept of Child Health Nursing for her guidance, support and
encouragement during the course of this study.
I acknowledge my gratitude to Mrs. Maria Gladys M. Sc. (N), Lecturer,
Dept of Child Health Nursing, Sarvodaya College of Nursing for her cooperation,
guidance and support during the study.
I wish to place my sincere thanks to all the members of Dissertation
committee of Sarvodaya College of Nursing for their suitable suggestions, genuine
interest and timely encouragement which contributed towards the completion of the
study.
I would like to extend my thanks to Dr. Gangaboraiah, Bio-Statistician,
KIMS for his timely assistance and valuable suggestions and directions in the
statistical analysis and presentation of data.
I extend my thanks to Librarians of Sarvodaya College of Nursing for the
computer assistance.
The investigators would like to extend her gratitude to all the experts who
have contributed their times and effort towards validating the tool.
vii

I wish to acknowledge my gratitude to V.S Communications and
Mr. Suraj Shetty, Netcom Technologies who helped me to bring this dissertation to
its final shape.
My thanks goes to Mrs. Nirmala Sridhar, M.A. Psychology, M.A. English
Literature, M.A. M.Phil. P.G. Diploma in Guidance and counselling for editing
this manuscript. My gratitude goes to Mrs. A.B. Jayasree, M.A. Kannada for
translating my tool in Kannada.
I extend my thanks to all my friends especially Mrs. Ceeba Francis,
Mrs. Geeta Das, Miss. Lavanya, Miss. Rajini and Mrs. Rosmin for their
supportive and positive interaction during the study.
My special thanks to all the participants who helped me to complete my
study.
I am immensely thankful to my Provincial Sr. Damian and all my
community sisters for their constant prayers, encouragement and moral support
which sustained me throughout the study.
I am grateful to my beloved parents, brothers and sisters for their valuable
support and encouragement.
My sincere gratitude to all those names have not mentioned but who have
directly or indirectly helped me for the successful completion of the study.
Signature of the candidate
Date:
Place : Bangalore ROSAMMA K.J
viii

LIST OF ABBREVIATIONS USED
1. BF : Breast Feed
2. CF : Complimentary Feeding
3 . χ2 : Chi – Square
4. DHS : Demographic and Health Survey
5. df : degree of freedom
6. HAZ : Height for age Z-scores
7. IAP : Indian Association of Paediatrics
8. NNMB : National Nutrition Monitoring Bureau
9. NCAER : National Council for Applied Economics Research
10. NM : Nutritional marasmus
11. PEM : Protein energy malnutrition
12 SD : Standard Deviation
13. Σ : Summation
14. TCFP : Traditional Complimentary Feeding Practice
15. UNICEF : United Nations International Children’s Emergency Fund
ix

TABLE OF CONTENTS
SL.NO. CONTENTS PAGE NO
1. Introduction 1 - 15
2. Objectives 16
3. Review Of Literature 17 – 35
4. Methodology 36 – 44
5. Results 45 – 64
6. Discussions 65 – 68
7. Conclusion 69 – 72
8. Summary 73 – 76
9. Bibliography 77 – 82
10. Annexure 83 – 110
x

LIST OF TABLES
Sl. No. Title of the Table Page No.
1 Area wise analysis of mean and standard deviation of feeding
practices of mothers
59
2 Area wise classification of respondents on feeding practices 60
3 Correlation between feeding practice of mothers and selected
nutritional parameters of their children
61
4 Association between feeding practices and demographic
variables of mothers
62
5 Association between feeding practices and selected variables of
children
64
xi
LIST OF FIGURES
Sl.No. Title of the Figure Page No
1 Conceptual frame work 15
2 Schematic representation of research design 38
3 Frequency and percentage distribution of mothers by age 47
4 Frequency and percentage distribution of mothers by religion 48
5 Frequency and percentage distribution of respondents by type of
family 49
6 Frequency and percentage distribution of mothers according to
their educational status 50
7 Frequency and percentage distribution of mothers by occupation 51
8 Frequency and percentage distribution of mothers by family
income 52
9 Frequency and percentage distribution of mothers by duration of
married life 53
10 Frequency and percentage distribution of no of under five
children 54
11 Frequency and percentage distribution of respondents by source
of information 55
12 Frequency and percentage distribution of birth order of children 56
13 Frequency and percentage distribution of children by age 57
14 Frequency and percentage distribution of children by gender 58
xii

ABSTRACT
Statement Of The Problem
“A Study To Correlate Feeding Practices Of Mothers And Nutritional
Status Of Their Children In A Selected Area, Bangalore.”
Background
Malnutrition is an important health problem in many developing countries
including India. It is mainly due to faulty dietary habits. It is known that in addition to
illness and infection in early childhood, inadequate food intake will contributes to
stunting and underweight in most of the children in India.
The objectives of the study were
1. To assess the feeding practices of mothers.
2. To assess the nutritional status of children.
3. To find out the correlation between the feeding practices of mothers and the
nutritional status of their children.
4. To find out the association between feeding practices of mothers and their children
with selected variables.
Hypothesis
H1: There is a correlation between feeding practices of mothers and nutritional status
of their children.
xiii
Method
The study was conducted in Chikkabasti and Doddabasti after obtaining
permission from the Medical Officer, Primary Health Centre, K. Gollahalli. Survey
approach and descriptive correlative design was adopted for the present study. The
sample of the study consisted of 100 mothers and their children. The tool used for the
study was structured questionnaire and the technique adopted for the study was
structured interview schedule. The obtained data was analysed by using descriptive
and inferential statistics and interpreted in terms of objectives of the study.
Results
The findings of the study revealed that most of the respondents were in the age
group between 18 – 23 years. Education wise, majority of them were education upto
high school. Occupation wise, 82 percent of them were housewives. Religion wise,
majority of them (62 percent) of them were Muslims. Most of them belonged to
nuclear families. 73 percent of them had income below Rs.5000. 60 percent of
mothers had only one child and 50 percent of them had duration of 5 – 9 years of
married life. Most of them had TV / radio as source of information.
With regard to children 48 percent were between 2 – 3 years of age among
which females were 55 percent and male 45 percent. 48 percent of them belonged to
second in birth order.
Among the total respondents, 5 percent of the respondents practiced not
satisfactory feeding practices, 81 percent of them practiced moderately satisfactory
feeding practices and only 14 percent of them practiced satisfactory feeding practiced.
xiv
Interpretation and conclusion
The study showed that there were significant association between feeding
practices and mothers’ demographic variables such as education, occupation and
religion of mothers. Whereas there was no-significant association between feeding
practices and mothers’ demographic variables such as age, number of under five
children, years of married life, income, type of family, birth order, age of the child,
gender and sources of information.
However, there was positive correlation between feeding practices and
selected nutritional parameters like present weight, height, mid arm circumference
and chest circumference.
Key Words
Feeding practices, Nutritional status, mothers, children.
xv
1. INTRODUCTION
“Look to your health and if you have it, praise God and value it next to
conscience; for health is the second blessing that we mortals are capable of, a
blessing money can’t buy”.
- Izaak Walton
Children are the first call agenda of human resource development – not only
because young children are the most vulnerable, but because the foundation for life-
long learning and human development is laid in these crucial early years. It is now
globally acknowledged that investment in human resources development is a pre-
requisite for economic development of any nation. Early childhood constitutes the
most crucial period in life, when the foundations are laid for cognitive, social,
emotional, physical, motor development and cumulative life-long learning.1
India is the home to the largest child population in the world. “The
development of children is the first priority on the country’s development agenda, not
because they are the most vulnerable, but because they are our supreme assets and
also the future human resources of the country”. In these words, our Tenth Five Year
Plan (2002-07) underlines the fact that the future of India lies in the future of Indian
children. 1
There is a saying that, ‘if we have good health we would have achieved
most of the things in life’. Every child has the right to possess good health. Life
would have been uncomplicated or simple, if we could attain all that we need
automatically or without an effort. But then God has placed us in a world where we
1
have all that are needed for a healthy living and we on our part has to make use of
these things in an effective manner.
It is recognized that the period from birth to two years of age is a “critical
window” for the promotion of optimal growth, health and cognitive development.2
Nutrition plays an important role in the physical, mental and emotional development
of a child. Infants and pre-school children are the most vulnerable group. UNICEF
has pointed out that malnutrition is the biggest and single cause of infant and child
mortality. Malnutrition is largely by product of poverty, ignorance, insufficient
education and large family size. These factors influence most directly the quality of
life and are the true determinants of malnutrition in society.
A child’s early years have long been recognised as particularly critical time for
developing good dietary habits. It also is an important time for taking in nutrients
amounts required not only for optimal growth and development but for influencing
mental development as well.3 It is very important that parents provide regular
information about an infant’s or toddler’s nutritional needs, eating habits, cultural and
religious preferences about food and health. It is well known that inadequate food
intake in addition to illness and infection in the first two years of life contributes to
stunting and underweight in millions of children in India and around the world.4 Poor
breast feeding patterns, low nutrient density and poor quality of complementary feed
accounts for much of the nutrient deficiency.
Mother’s knowledge related to feeding of babies also reflects the nutritional
status of the child. Children completely depend on mothers for their nutrition.
2

Breast-feeding, and other dietary practices adapted by her reflect the nutritional status
of the child. Breast-fed infants and children grow normally during the first six months
of their life, and show slow growth during the transitional period of weaning because
they do not get enough nutritious foods.
Exclusive breast feeding for the first six months of life could save at least 1.3
million lives a year that’s about 3500 children each day according to UNICEF. The
Indian Academy of Paediatrics supports exclusive breast feeding for six months and
points out that breast feeding provides invaluable immunological protection from a
whole host of diseases.5
Gosh had argued that the high rates of malnutrition in India are not primarily
caused by poverty; rather the behaviours of delayed initiation of breast feeding, early
introduction of water and liquids and delay in complementary feeding result in a
period of perpetual hunger for the child.6
Many researchers agree that socio-economic and environmental conditions,
together with feeding practices, are important determinants of nutritional status in
developing countries. Inadequate quantity and poor quality of food result in growth
faltering, which is exacerbated by the high prevalence of fever and diarrhoeal
diseases. Inappropriate feeding patterns may also contribute to child malnutrition. The
World Health Organization recommends that children under the age of four months
should be exclusively breastfed.7 Appropriate complementary feeding promotes
growth and prevents stunting among children between 6-24 months. The period of
complementary feeding is when other foods or liquids are provided along with breast
3

milk. Rates of malnutrition usually peak at this time with consequences that persist
throughout life. Stunting is seldom reversed in later childhood and adolescence.
Weaning is not a sudden withdrawal of child from the Breast. It is a gradual
process starting around the age of 4-5 months.8 because breast milk alone is not
sufficient to sustain growth and development for an infant of this age.9 It is also said
that introduction of food other than breast milk at an early period (before 4 months)
decreases the frequency of breast feeding leading to malnutrition.10 Weaning food
should be rich in protein and other nutrients. Weaning can be traumatic experiences
for the infant because it looses the oral gratification from sucking.11
It is well established that nutritional status is major determinant of the health
and well being among children and there is no doubt regarding the importance of the
study of child’s nutritional status according to spatial and temporal dimension.
Developing country like India, accounts for about 40 percent of under nourished
children in the world and it is largely due to the result of dietary inadequacy in
relation to their needs. In the light of the above, the assessment of nutritional status of
an individual or population, anthropometry is widely recognized as one of the useful
techniques, because it is highly sensitive to detect undernutrition.12
Reliable community based data generated by the National Nutrition
Monitoring Bureau (NNMB) from eight central and southern states. (Andhra Pradesh,
Gujarat, Karnataka, Kerala, Madhya Pradesh, Maharashtra, Orissa and Tamil Nadu)
also confirm a decline in clinical deficiency signs in pre-school children from 1975-79
to 1988-90 in rural areas. The overall prevalence of marasmus decreased from 1.3 to
4
0.6 per cent and kwashiorkor from 0.4 to 0.1 per cent. Among the 12,000 children
evaluated in the ‘repeat surveys’. Gujarat showed the highest prevalence of both
forms, while in the other states their prevalence was below 1 per cent. In the NNMB
and the National Council for Applied Economics Research (NCAER) linked survey
conducted in 1994 among 1828 pre-school children in the same eight states but in
different sampled areas, the overall prevalence of kwashiorkor and marasmus as 0.2
and 0.4 per cent. Fortunately, a similar declining trend was documented in the under-
privileged urban slums of these six states. The overall prevalence of marasmus has
diminished from 3.7 per cent in 1975-79 to 0.2 per cent in 1993-94. No cases of
kwashiorkor were observed.13
In India nearly 75 percent of the populations reside in the village, of the total
rural population 50 percent is still under the poverty lines. Majority of children in
India are not in a position to get adequate nourishment because of very low per capita
income of their families. As per 2001 census, India has around 157.85 million
children, constituting 15.42 percent of India’s population, who are below the age of 6
years. Of these 157.86 million children, 75.95 million children are girls and remaining
81.91 million children are boys. The sex ratio among children as per Census 2001 is
927 i.e. 927 females per 1000 males. A significant proportion of these children lives
in economic and social environment which impedes the child’s physical and mental
development. These conditions includes poverty, poor environmental sanitation,
disease, infection, inadequate access to primary health care, inappropriate child caring
and feeding practices.1 This present study is an effort to analyze the feeding practices
of mothers and the nutritional status of their children in a selected community.
5

Need for the study
The child is the center of attraction in a family. The first important way the
young children feel part of the family is through a schedule that is like that of the
other family members. Being able to eat with the family goes a long way toward
making children feel that they are now truly family members.
Children are the future of any nation. In India about three – fourth of the infant
population lives in villages. It is imperative to preserve this wealth and to promote
their well being through exercising utmost care in order to make them healthy and to
protect them from deadly diseases. Care of children had always traditionally been the
forte of mothers’ irrespective of education, income and social class differences.14
Malnutrition is increasingly recognized as a prevalent and important health
problem in many developing countries. This problem has serious long term
consequences for the child and adversely influences their development.15 Poor
nutrition or malnutrition is caused by not getting the proper nutrients needed for
normal growth and development. Undernourished children do grow to their full
potential of physical and mental abilities. Malnutrition makes the child more
susceptible to infection and recovery is slower and mortality is higher.8
Over the past two decades, there has been a substantial and progressive
decline in infant and child mortality rates in India. There has also been a significant
reduction in the prevalence nutritional deficiency disorders. It is therefore important
that increasing attention is now paid to the nutritional status of the survivors. The
alarming reports of some international agencies which have placed India at about the
6
bottom-rung of an arbitrary world development scale, have raised apprehensions that
the nutritional status of women and children in India shows no signs of
improvement.13
“Children’s health is tomorrow’s wealth”. The professional who work with
the children must have the knowledge of existing feeding practices among mothers
and the nutritional status of their children. She must be able to identify the various
feeding practices and taboos that exists and which in turn affect the nutritional status
of children, should share her skill and knowledge to prevent malnutrition.
According to the National Family Health Survey, malnutrition affects children
the most during 6–12 months of age and one of the major determinants is poor
feeding practices during first year of life. Breast feeding is extremely important
during illness, as children like to be with the mothers and continue to be breast fed.4
Appropriate complementary feeding involves a combination of practices to maintain
breast milk intake and, at the same time, improve the quantity and quality of foods
children consume.
The 6-11 month period is an especially vulnerable time because infants are
just learning to eat and must be fed soft foods frequently and patiently. Care must be
taken to ensure that these foods complement rather than replace breast milk. Energy
intake can be increased by increasing breastfeeding frequency, increasing food
portion size, feeding children more frequently, and providing more energy-dense
foods. Micronutrient intake can be increased by diversifying the diet to include fruits,
vegetables, and animal products; using fortified foods; giving supplements.10 During
7

the third trimester of pregnancy through the early childhood years malnutrition
interferes with the development of the brain. This in turn affects the child’s ability to
learn. As a result children will never be as bright as nature had meant them to be.
Knowledge of weaning foods and practice is an important aspect of preventive
and social pediatrics. Programs to improve complementary feeding must conduct
local assessments. Local studies should identify local diets and current good practices
to be supported, test options for improving the traditional diet and related feeding
practices, and identify target audiences and effective strategies for reaching them.10
A study of Dietary Pattern, Household food Security and Nutritional Profile of
Under-five Children of a Community of West Bengal conducted by Sandip Kumar
Ray, Akshil Bandhu Biswas, Sathi Kumar, concluded that : the overall prevalence
of malnutrition based on IAP classification, among the under-five, was found to be
80.90 percentage and that of severe grades of malnutrition (grades III and IV) was
9.26 percentage Prevalence of both overall malnutrition as well as severe grades of
malnutrition was highest in 12 to less than 24 months age group being 85.7
percentage and 18.2 percentage respectively while lowest prevalence was observed
amongst the infants.
The prevalence of malnutrition including its severe grades was observed to be
higher in females as compared to their male counterparts, amongst the families where
number of children were 2 or more as well as amongst the families where mothers
were working as compared to those who were not.16
8
Breast milk is the ideal food for the infant. But after six months production of
breast milk which is the source of nourishment is reduced. So complementary feeds
should be in children’s diet.
Kumar D and Goel conducted a study on “Influence on infant feeding
practices and nutritional status of under-five children”. This study included 217
under-five children.
Initiation of Breast Feed: They found that 55.8 per cent were breast fed within
six hours of birth of whom 30.6 per cent under weight, 49.6 per cent stunting and 12.4
per cent were wasting. Whereas 42.2 per cent were breast fed after 6 hours. Among
them 43.7 per cent were under weight, 64.6 per cent stunting and 8.3 per cent wasting.
Colostrum Feeding: 42.2 per cent had colostrum feeding; among whom 27.5
per cent under weight, 42.1 per cent stunting, 10.5 per cent wasting. 54.8 per cent who
didn’t have colostrum feeding of whom 43.7 per cent suffered under weight, 59.0 per
cent stunting and 10.6 per cent wasting.
Exclusive Breast Feeding: 23.5 per cent had exclusive breast feeding among
whom 27.4 percent under weight, 49.0 percent stunting and 5.6 percent wasting were
found. And 76.5 percent who did not have exclusive breast feed also suffered from
under weight, stunting and wasting i.e. 43.7 percent, 52.4 percent and 12.0 percent
respectively.
9
Proper Complimentary Feeding: 38.7 percent had proper complimentary
feeding of whom 28.6 percent under weight, 44.0 percent stunting and 8.3 percent
wasting. Also 61.3 percent who did not have proper complimentary feeding suffered
from underweight, stunting and wasting i.e. 41.3 percent, 56.4 percent and 12.0
percent respectively.17
The Institute for Research in Medical Statistics, New Delhi undertook a study
to assess the nutritional status of the population residing in Bihar. Among children,
nutritional deficiency was observed inspite of higher intake of energy. Therefore, to
examine the role of dietary and other related factors on nutritional status of children, a
detailed analysis was done for the data collected in the study.
The survey covered all the 50 districts including all 704 blocks, 1418 villages,
236 urban ward, 28360 households and about 11,000 children of Bihar. For selection
of village and households, an appropriate sampling methodology was used.
Information was collected on households characteristics, demographic profile,
anthropometry etc. Children under five years of age were categorized using Gomez
classification as severe, moderate, mild and normal.
This analysis indicates that the malnutrition among children depends on both
better sanitary conditions and on dietary intake. The severe and moderate level of
malnutrition among children was much higher among those with poor housing and
sanitary conditions even with the same level of dietary intake whereas inspite of lower
dietary intake, the level of malnutrition was much lower for those living in better
sanitary conditions. Thus to reduce the problem of malnutrition among children, there
10
should be dual focus on dietary intake as well as providing safe drinking water, better
sanitation and housing condition for improving their general standard of living.18
Since mothers are solely responsible for the breast feed, weaning and
preparing various type of diet for children, they should have sufficient knowledge
regarding feeding to prevent malnutrition and promote optimum health for their
children. Malnutrition in children is a complex problem and must be viewed within a
broad frame work of child care including feeding practices. A good understanding of
the nutritious situation of an area is necessary for improved planning of development
of its people. So that nurses could assist mothers to improve or modify their feeding
practices wherever necessary to improve their children’s health status. Therefore this
study aimed at assessing the feeding practices of mothers and nutritional status of
their children in a selected area, Bangalore.
Statement of the problem
“A Study To Correlate Feeding Practices of Mothers And Nutritional
Status Of Their Children In A Selected Area, Bangalore.”
Operational Definitions
1. Feeding practices: Refers to the pattern of feeding that are commonly
practiced by mothers include breastfeed, type of food stuffs, quality and
quantity, feeding techniques, number of feeds per day that mothers use for
their children.
2. Nutritional status: It refers to assessment of selected nutritional parameters
like present weight, height, and mid arm circumference and chest
circumference.
11
3. Children: Refers to individuals between 6 months to 3 years of age.
4. Mothers: Refers to women between the age of 15 to 45 years and having
children in the age group of 6 months to 3 years.
Hypothesis
H1: There is positive correlation between feeding practices of mothers and
nutritional status of their children.
Inclusion criteria
1. Mothers of children who were willing to participate in the study.
2. Both male and female children.
Exclusion criteria
1. Mothers who have physically and mentally challenged children.
2. Mothers who did not have the children along with them at the time data
collection.
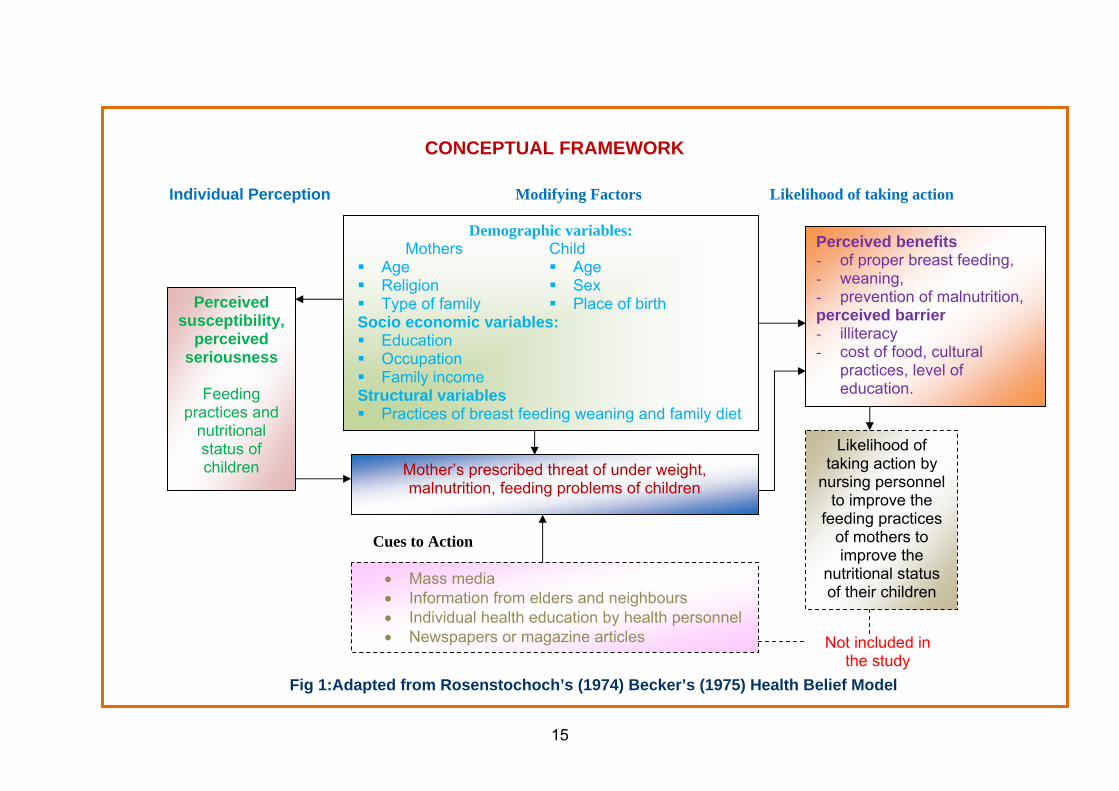
Conceptual Framework
The Conceptual Framework for the study is based on health belief model.
Health beliefs are person’s ideas convictions and attitudes about health and illness.
They may be based on factual information or misinformation. The health behaviour
usually results from health beliefs.
The Health Belief Model (HBM) was one of the first models that adapted
theory from the behavioural sciences to health problems, and it remains one of the
12
most widely recognized conceptual frameworks of health behaviour. Rosenstoch
(1974) and Becker’s and Maiman’s (1975) model, address the relationship between
the persons beliefs and behaviours. It is a way of understanding and predicting how
clients will behave in relation to their health and how they will comply with health
care therapies. Use of the model is based on a persons perceptions of susceptibility to
an illness and the seriousness of the illness.19
This model helps, nurse to understand various behaviours including mothers
perception, beliefs and various behaviour in order to plan the most effective care.
The investigator felt that Becker’s model is suitable as conceptual framework
for this study. Mothers feeding practices regarding breast feeding, weaning and family
diet can be modified by health education and information by health personnel.
Mothers can apply this knowledge in taking care of their children.
The model describes about 3 variables
1. Mothers Perception
Mothers perceived knowledge regarding breast feeding, weaning and family
diet. Foods according to the age, feeding technique and problems during each
stage.
2. Modifying Factors
Mother’s perception is influenced and modified by demographic variables like
mothers age, religion, type of family, child’s age and sex, socio economic
variables like education occupation and family income and structural variables
13

14
like feeding practices. The mother’s perception is also influenced by cues to
action like mass media, information from elders and neighbours and information
getting from health personnel.
3. Likelihood of Taking Action
This part indicates that mothers may try to take action to assess nutritional need of
their children and initiating proper feeding practices to prevent malnutrition,
underweight and feeding problems. Thus to improve the nutritional status of their
children. Perceived barriers like illiteracy, poor socio economic status and lack of
knowledge of mothers may lead to unhealthy practices.
Projected Outcome
Study will provide an insight into satisfactory feeding practices of mothers and
the nutritional status of their children, thereby help the nurses to sow the seeds
towards correct feeding practices.
15
Cues to Action
Fig 1:Adapted from Rosenstochoch’s (1974) Becker’s (1975) Health Belief Model
Demographic variables: Mothers Child Age Age Religion Sex Type of family Place of birth
Socio economic variables: Education Occupation Family income
Structural variables Practices of breast feeding weaning and family diet
Mother’s prescribed threat of under weight, malnutrition, feeding problems of children
Perceived benefits - of proper breast feeding, - weaning, - prevention of malnutrition, perceived barrier - illiteracy - cost of food, cultural
practices, level of education.
Not included in the study
Likelihood of taking action by
nursing personnel to improve the
feeding practices of mothers to improve the
nutritional status of their children
• Mass media • Information from elders and neighbours • Individual health education by health personnel • Newspapers or magazine articles
Perceived susceptibility,
perceived seriousness
Feeding
practices and nutritional status of children
Likelihood of taking action Modifying Factors Individual Perception
CONCEPTUAL FRAMEWORK

2. OBJECTIVES
Statement of the problem
“A Study To Correlate Feeding Practices of Mothers And Nutritional
Status Of Their Children In A Selected Area Bangalore.”
Objectives of the study
1. To assess the feeding practices of mothers.
2. To assess the nutritional status of children.
3. To find out the correlation between the feeding practices of mothers and the
nutritional status of their children.
4. To find out the association between feeding practices of mothers and their
children with selected variables.
16
3. REVIEW OF LITERATURE
Review of literature is a key step in research process. Review of literature
refers to an extensive, exhaustive and systematic examination of publications relevant
to the research project.9 The review of related literature is valuable guide to define the
problem, recognising its significance, suggesting promoting data gathering devices,
appropriate study design and source of data.
Review of literature for the present study has been organised under the
following headings
1. Literature related to the prevalence of malnutrition and its relation with
feeding practices.
2. Literature related to the feeding practices of mothers and nutritional status of
their children.
3. Literature related to the influence of weaning practices on nutritional status of
children
4. Literature related to the maternal nutritional knowledge and child nutritional
status.
1. Literature related to the Prevalence of malnutrition and its relation to feeding
practices
Chirumulay D, Nisal R has done a study on prevalence of malnutrition and
its relation with feeding practices in 605 tribal under five children. There was a
significant relation of nutritional status of preschool children to feeding practices.
Exclusive breast- feeding was beneficial only up to 6 months age. After this age, it
lost its advantage. Children above one-year age exclusively fed on breast had a high
17
prevalence of malnutrition. No other factor, like sex of the child, parental literacy,
past history of illnesses had any significant effect. Health education messages should
stress on importance of timely weaning with introduction of solid foods by 6 to 9
months of age; to address the widespread problem of malnutrition in under five
children.24
Abdul Sayed ZT has done the study on the determinants of nutritional
marasmus (NM) and kwashiorkor (K) using Sudanese children aged 6-36 months.
Subjects consisted of 55 children with NM and 55 with K, admitted to the children’s
Emergency Hospital in Khartoum. Mothers were interviewed in hospital, and
information on duration of breastfeeding, age at introduction of supplementary foods,
and weaning foods was obtained. Observations were made in 20 percent of homes of
study children. The results suggest a positive association between prolonged
breastfeeding without introduction of supplementary feeding between the ages of 6
and 24 months, and NM. Using multivariate analysis the data show that late
introduction of supplementary foods produces an increase of 1.4 fold odds of
developing nutritional marasmus, rather than kwashiorkor. In contrast the odds ratio is
1.9 for the two conditions in terms of age of cessation of breastfeeding, the
kwashiorkor children breastfeeding for fewer months. Results suggest strategies to
reduce the prevalence of NM and moderate PEM.25
Srivastava N, Sandhu A did a study on Index for measuring child feeding
practices. The investigation was undertaken with the objective of creating an infant
and child feeding index (ICFI) from a set of complementary feeding (CF) practices
and to determine its association with growth of infants and young children (6-23
18

months). A semi-structured interview schedule was used to collect information for
204 children from one large slum and two private paediatric clinics of urban
Vadodara. Results revealed that about half (5.05 percent) of the children were stunted
Height for Age Z score, nearly one-fourth (25.5 percent) were underweight, but
wasting was low (3 percent). It is concluded that the composite index in its present
form can reflect the CF practices more holistically than just one or few behaviour
studied separately. More research is needed in the direction of consulting of
composite index which can then be used for research, monitoring, evaluation and
much needed advocacy for complimentary feeding.2
Hossain I M, Yasmin R, Kabir I did a study on Nutritional and
immunisation status, weaning practices and socio-economic conditions of under five
children in three villages of Bangladesh. A total of 479 children aged 6-60 months
were studied during 1991 to 1992. According to Gomez classification, 96 percent of
children had varying degrees of protein energy malnutrition. According to Waterlow
classification 84 percent were stunted (36 percent mild, 33 percent moderate and 15
percent severe) and 67 percent were wasted (47 percent mild, 18 percent moderate
and 2 percent severe). Of all children 368 received BCG and 439 received partial or
full dose of DPT and Polio vaccines. Among children aged 13-60 months 75 percent
received Measles vaccine. Weaning food was started at 8.4 months. Low household
income, parental illiteracy, small family size, early or late weaning and absence of
BCG vaccination were significantly associated with severe PEM. Timely weaning,
education and promotion of essential vaccination may reduce childhood malnutrition
especially severe PEM.26
19
Excler JL, Nicolas E, Mojon M conducted a study on Protein-energy
malnutrition in an urban African milieu, etiologic factors in kwashiorkor and
marasmus-kwashiorkor. The etiologic factors of protein-energy malnutrition have
been studied in 59 children with kwashiorkor (KWK) or marasmus-kwashiorkor
(MKWK) and living in an African urban area. The decline of breast feeding leads to
an earlier PEM, mainly MKWK. This decline is linked to urbanization, mother's
activities, dislocation of traditional structures and use of artificial formulas.
Essentially based on cereals, the diet is responsible of the post-weaning P.E.M.
Poverty, ignorance and food taboos are related to a lack in weaning food varieties. A
small number of infants with KWK had a rich protein diet putting back the cause of
an hypoproteic diet on the KWK onset. Infections play a determinant role in the onset
of KWK and of some MKWK, after 2 years of age. Diarrhoea, measles,
bronchopulmonary and parasitic diseases are the most prevalent infections. Among
socio-cultural factors, conjugal disorders are predominating with child-mother break-
up and father's bonding failure. At the opposite of rural areas, the family size is
reduced. The three first birth ranges are specially concerned with young inexperienced
mothers.27
2. Literature related to Feeding practices of mothers and nutritional status of
their children.
Dinesh N.K, Goel, Poonam C, Mittal did a study to determine the nutritional
status of under-five children and to assess infant feeding practices and the association
with the under nutrition in Anganwari area of urban Allahabad. Among all under five
children surveyed, 36.4 percent were under weight, 51.6 percent had stunted growth
and 10.6 percent had wasted proportions of underweight and stunting were found
20

maximum among children aged 13-24 months. Wasting was more prevalent among
children aged 37-48 months. Initiation of breast feeding after six hours of birth,
deprivation from colostrum and improper complementary feeding were found
significant risk factors for underweight. Wasting was not significantly associated
with any infant feeding practices studied. They conclude that delayed initiation of
breast feeding, deprivation from colostrum and improper weaning are significant risk
factors for under nutrition among under fives. There is a need for promotion and
protection of optimal infant feeding practices for improving nutritional status of
children.17
Hannan A, Hassan M, Fazlur Rahman AKM, Rahman A conducted a
study on Infant feeding practices from birth to two years of age and nutritional status
of children and mothers in Bangladesh. Six nationwide cross-sectional surveys on
infant feeding practices and child and maternal nutritional status were conducted
every six months from July 1998 to February 2001. One district from each division of
the country and two upazilas from each selected district were randomly selected.
Anthropometric measurements of children included measurement of weight and
height / length. The nutritional status of mothers were assessed by taking height and
weight and expressing as body mass index. Information on breast feeding practices,
complementary feeding and anthropometric measurements were collected using two
sets of pre-tested questionnaire. The prevalence of continuation of breast feeding at
one year in most surveys was more than 96 percent and at 2 years more than 85
percent. Despite national efforts to improve breast feeding and nutritional status of
children and mothers in Bangladesh, the indicators have yet to reach an optional level.
21
These feelings can help policy – planners understand the need for intensifying future
programmes.20
Nyaruhucha CNM, Msuya JM, Mamiro PS and Kerengi AJ conducted a
study on Nutritional status and feeding practices of under-five children in Simanjiro
District, Tanzania. The study showed that 31 percent of the children were
undernourished, some of them severely. Children 2 - 3 years old were the most
affected. Breastfeeding duration of more than one year was common among the
mothers. Fifty-four percent of the mothers weaned their children as early as two
months after birth. The most common type of weaning food was maize porridge
(gruel) mixed with cow's milk Generally, 87 percent of households were facing some
degree of food insecurity where some of them either experienced food shortage for
3-4 months reported of eating less than three meals per day. An educated mother was
less likely to have an undernourished child, while a child from a teenage mother was
more likely to be undernourished. Small size of a household was in favour of nutrition
status. There is a great need to undertake interventions through community education
to rescue the situation in Simanjiro district. Efforts should also be undertaken to
mobilize the community members to adopt practices that favour good nutrition of
children.15
Kamau-Thuita F, Omwega AM, Muita JW conducted a study on Child care
practices and nutritional status of children aged 0 to 2 years in Thika, Kenya. Cross
sectional descriptive survey using a structured questionnaire and taking of
anthropometric measurements to determine the nutritional status of children aged 0 to
2 years. In addition, two day observations were conducted in a subsample of
22
households to assess time allocation for the main child care activities. The findings
revealed that mother’s knowledge about child care influences the amount and type of
care that is given to children. Time taken to perform various activities was also found
to vary with the mother's education level, her occupation, number of children less than
five years in the house and the child's age and birth order. Comparatively, children
who were malnourished had less time devoted to them for breastfeeding, food
preparation and feeding. Although mothers were the primary caregivers, the
responsibility of care giving was shared with other household members as well as
with neighbours. The amount and type of care that a child receives is determined to a
large extent by the mother and caregivers knowledge.21
Ruel MT, Menon P affirmed that Child feeding practices are associated with
child nutritional status in Latin America. Data from the Demographic and Health
Surveys (DHS) for 5 Latin American countries, were used to explore the feasibility of
creating a composite feeding index and to examine the association between feeding
practices and child height-for-age Z-scores (HAZ). The variables used for the index
were as follows: current breast-feeding, use of complementary foods and liquids in
the past 24 hrs, frequency of use over the past week and feeding frequency. The index
was made age specific for 6 to 9, 9 to 12 and 12 to 36 mo-old age groups, and age-
specific feeding practices were created. Bivariate analyses showed that feeding
practices were strongly and significantly associated with child HAZ in all 7 data sets,
especially after 12 mo of age. Differences in HAZ between child feeding practices
remained significant after controlling for potentially confounding influences, for all
countries except Bolivia. Among children whose mothers had primary schooling
compared with mothers with no schooling, or mothers with higher than primary
23

school level. The data available in DHS data sets can thus be used effectively to create
a composite child feeding index and to identify vulnerable groups that could be
targeted by nutrition education and behaviour change interventions.22
Alvarado BE, Tabares RE, Delisle H, Zunzunegui MV conducted a study
on Maternal beliefs, feeding practices and nutritional status in Afro-Colombian
infants. They combined ethnographic and epidemiological data. They collected
information using a food frequency questionnaire. Nine focus groups and 5 deep
interviews to mothers of children less than 2 years of age were performed. Their data
showed a prevalence of wasting of 2.6 percent and prevalence of stunting of 9.8
percent. These practices are characterized by a universal onset of breast feeding, that
lasted 10 months in average, and an early introduction of complementary food.
Breastfeeding is a cultural norm. Weaning is related to new pregnancy, to low milk
production and to negative effects of breast process on mothers’ health. Early
complementary feeding and bottle-feeding are highly valued due to their positive
effect on nutritional status and adaptation of children to adult-type diets. The
introduction of complementary food after 4 months, the quality of the first food
introduced and the diversity of complementary food predicted better nutritional status.
They conclude that nutritional illiteracy and mothers' erroneous beliefs result in 50
percent of the mothers having inadequate feeding practices.23
3.Literature related to the influence of weaning practices on nutritional status of
children
Hasan J, Ray J, Khan Z conducted a study on influences of weaning practices on
nutritional status in a cohort of 200 infants over a period of one year in the rural area of
24
Aligarh. Weaning was late in most of the infants under study. The nutritional status of
infants up to 6 months was significantly better than that of infants more than 6 months
of age. Most of them used the family- food as weaning food.28
Osuhor PC had prepared a standardized questionnaire and administered to 65
mothers attending the Nutrition Clinic of the Ahmadu Bellow University Teaching
Hospital, Kaduna, Northern Nigeria, over the October-December 1978 period to
determine at what age the 1st supplementary diet was introduced, the age the child
was weaned, and the weaning practices. The questionnaire dealt with various aspects
of weaning knowledge, attitudes, and practices. The mothers were referred to the
Nutrition Clinic because their babies already were suffering from protein energy
malnutrition, had failed to thrive, or had severe infections, e.g., measles,
gastroenteritis, or respiratory diseases. 58 of the families were of low socioeconomic
status. 36 mothers introduced supplementary feeds when their ch8ildren were between
7-9 months. All the mothers used corn, or millet gruel. A decision to wean a child
may be made if the child can crawl, walk, or has a good set of erupted milk teeth,
even if the child has not reached the traditional weaning age of 20-24 months. The
mean age of weaning was 17 months in this study. 78.5 percentage of the mothers
responded to the question about weaning food taboos, prohibitions, and their reasons
during the weaning period. Even when protein is available, a child may be denied the
protein because of socioeconomic factors. The use of carbohydrate gruels among
these low socioeconomic facilities coupled with sociocultural factors compounded the
feeding problem, and, consequently, protein energy malnutrition was common during
the weaning period.29
25
Puri RK, Sachdeva R had done a study on supplementary foods suited for
weaning and feeding of infants were developed, using locally available foods in
Punjab. Methods of cooking employed were those used commonly by low and
middle-income families, Cereal –pulse combinations along with some sesame seed
and groundnuts were used to enhance the protein quality. The ratio used was such that
the preparation did not deviate much from the accepted tastes of the population.,
Fresh green vegetables were also used. Fifteen recipes were standardized and
acceptability trials carried out with mothers and infants or the different socio-
economic groups. The preparations were highly accepted by all. Analysis of these
were done for protein, calories, vitamin C and iron to see their contribution to the
diet. The cost per serving a very low cost a substantial amount of the above nutrients
could be given to in making these recipes will go a long way towards popularizing
such formulations.30
Jansen AA had done a study to assess Mild protein- calorie malnutrition in
Western Samoa. Severe protein-caloric malnutrition is also an important cause of
death in infants and toddlers and anaemia in frequently found in small children. Data
on infant and toddler feeding practices were collected from 90 mothers from the town
of Apia and 38 mothers from island in Sava. Most belonged to the low income group.
In Apia, weaning foods consisted of milk, meat, and other protein- rich foods; in
Sava, taro, orange leaf tea and rice, were the main weaning foods. Generally, semi-
solids were nor introduced before the child was more than 6 months of age. Some
mothers in Sava appeared to give their children monotonous diet. A number of
cultural taboos appear to affect the children’s diet as well as that of pregnant and
lactating mothers.31
26
Malla S and Shrestha SM conducted a study on Complementary Feeding
Practices and its Impact on nutritional status of under two old children in urban areas
of the Kathmandu, Nepal. Magnitude of the malnutrition was very high in Nepal.
Child nutrition problem due to faulty child feeding practice was widely observed in
many parts of the country including Kathmandu valley. Complementary feeding
practice among the young children has been found very critical in urban areas of
Kathmandu valley. The study was based on primary data collected by applying the 30
cluster sampling method. Target population of the study were young children aged 0-
24 months. A set of questionnaire was used to interview mothers of 150 households.
Finding of the study indicated that about 92 percent households were found practicing
Traditional Complementary Feeding Practices and 8 percent households were found
practicing Commercial Complementary Feeding Practices. Traditional
complementary foods given to the children were found lacking in macronutrient
carbohydrate and protein severely, therefore, not fulfilling the nutritional requirement
of the children. Among traditional complementary food fed children, 63 percent of
children were found suffering from mild to severe form of malnutrition where as
among commercial food fed, only 41 percent of children were found suffering from
such form of malnutrition. About 33 percent of the children suffering from severe
malnutrition, parents were employed. Nutritional status of children from Kathmandu
district found better compared to young children from other district. Children from
Lalitpur district were found more severely malnourished. Surprisingly baby boys
found more severely malnourished compared to baby girls. Traditional foods fed
children were found more severely malnourished compared to commercial
complementary food fed.32
27
Heath AL, Tuttle CR, Simons MS, Cleghorn CL, Parnell WR undertook a
study regarding breastfeeding and weaning practices during the first year of life in
Dunedin, New Zealand. To investigate infant feeding practices during the first year of
life in a group of white infants in Dunedin, New Zealand. Statistical analyses
Regression analyses were performed to determine factors associated with successful
breastfeeding initiation and duration. Among mothers, 88 percent initiated breast
feeding, 42 percent were exclusively breastfed till 3 months, and 34 percent were
partially breastfed till 12 months. Intention to breast feed increased the likelihood of
successful breastfeeding initiation. Mothers who reported that they did not have
enough breast milk tended to exclusively breastfeed for a shorter period of time.
Tertiary education and exclusively breastfeeding at 1 month were associated with a
longer duration of breastfeeding. Perception of breastfeeding in public as
embarrassing was associated with a shorter duration of breastfeeding. Among infants,
45 percent were given non milk foods before 4 months of age, and 69 percent were
given unmodified cow's milk as a beverage before 12 months.33
Hussain AM, Rariquzzaman M had undertaken a study to determine the
weaning age in rural Bangladesh. Weaning beliefs and practices in two representative
rural villages in Bangladesh by interviews with 180 mothers with infants between 1
and 12 months of age. Maternal parity and family size were not found to be related to
weaning age. Family income and maternal education were consistently related to
appropriate weaning. Bi-variate controlled analysis showed that a mismatch between
mothers' responses and actual weaning behaviour toward infants 4-6 months old could
be attributed to family poverty.34
28

Moussa WA, Tadros MD, Mekhael KG, Darwish AE, Shakir AR
undertook a study on some simple methods of home processing and their implication
with weaning foods. One of the most practical solutions to combat Protein Energy
Malnutrition in low income groups is the intelligent mixing of cereals and legume
make available low cost weaning food of high nutritional quality. One of the main
obstacles to increase energy and-nutrient density of weaning foods of cereals and
legumes is the bulk factor. In this study some simple methods of home processing to
improve the nutritional quality of the home prepared weaning foods were tested and
the processed weaning foods were chemically and biologically evaluated.
Biochemical evaluation revealed that the germination of wheat raised its protein and
fat and reduced carbohydrate, while there was almost no change on lentils. Comparing
germination with a special chapati process, protein and fat content were higher in the
formula processed by the former method, while minerals were higher in the same
formula but processed by the latter method. Although further research is needed,
germination of ingredients of weaning foods of vegetable origin seems to be a good
option of the simple home processing technique.35
4. Literature related to maternal nutritional knowledge and child nutritional status
Sharma S, Nagar S did a study to determine the impact of educational intervention
on knowledge of mothers regarding childcare and nutrition in Himachal Pradesh. The
study aimed at providing educational interventions to mothers regarding knowledge
on children and nutrition. A total sample of 150 mothers were selected from two
villages, one of which served as experimental group and the other acted as control
group. The tool consisted of a self structured questionnaire schedule covering aspects
of childcare and nutrition. All mothers were first pre tested regarding their knowledge
29
on nursing, neonatal and infant care, health, child’s growth, behaviour and nutritional
aspects. Intervention consisted of educating mothers in the experimental group for a
period of one and a half years. All the mothers were then post-tested on the above
aspects. Significant differences were seen in all the aspects of childcare and nutrition
between experimental and control group mothers during post-testing.14
Appoh LY, Krekling S undertook a study on Maternal nutritional knowledge
and child nutritional status in the Volta region of Ghana. The data was collected in
Ghana on 55 well nourished and 55 malnourished mother-child pairs. Data on
mother's demographic and socio-economic characteristics as well as child
anthropometric data were also collected. Bi-variate analysis gave significant
associations between child nutritional status and the following variables: time of
initiating of breastfeeding, mother's knowledge of importance of colostrum and
whether colostrum was given to child, age of introduction of supplementary food, and
mother's knowledge about causes of kwashiorkor. Maternal formal education, and
marital status were also found to be associated with child nutritional status in bi-
variate analyses. Further analysis with Logistic regression revealed that maternal
nutrition knowledge was independently associated with nutritional status after the
effects of other significant variables were controlled for. Maternal education on the
other hand was not found to be independently associated with nutritional status. These
results imply that mother's practical knowledge about nutrition may be more
important than formal maternal education for child nutrition outcome.36
Tada Y, Keiwkarnka B, Pancharuniti N, Chamroonsawasdi K had
conducted a study on Nutritional status of the preschool children of the Klong Toey
30
Slum, Thailand. Cross-sectional study to examine the nutritional status of children
aged 1-5 years who live in the Klong Toey slum, Bangkok; the factors related to
nutritional status were also determined. Anthropometric measurements were made for
232 children; socioeconomic background information was obtained by interviewing
their mothers using a structured questionnaire. The prevalence of malnutrition among
the study sample was 25.4 percent by weight for age, 18.1 percent by height for age,
and 6.9percent by weight for height; the prevalence among pre-school children in
Thailand and in the Bangkok metropolitan area by weight-for-age was reported to be
8.73 percent and 5.25 percent respectively. Multiple logistic regression analysis was
used to identify the association with the nutritional status of children by height-for-
age. The results showed that family income, maternal housewifery or unemployment,
food practice, and a maternal educational level lower than primary school were
associated with the nutritional status of children. This finding implies that although
malnutrition is no longer considered to be a major health problem in Thailand, it
remains a threat to the health of the urban poor in Bangkok. This finding should not
be overlooked and countermeasures are indicated.37
Waihenya EW, Kogi-Makau W, Muita JW conducted a study on Maternal
nutritional knowledge and the nutritional status of preschool children in a Nairobi
slum. Nutritional status of 363 children aged six to 24 months was measured and
nutritional knowledge of their mothers assessed. Makina village was randomly
selected as the study site and all consenting households were involved in the study.
The study established that most mothers (97.5 percent) have access to nutrition
education. Prevalence of stunting (86.2 percent) and underweight (58.4 percent) was
high but that of wasting (1.9 percent) was low. There was no significant relationship
between the nutritional status of children and overall nutritional knowledge.
31
Unexpectedly, a negative relationship was found between nutritional status and
mothers' ability to recognize clinical signs of malnutrition, knowledge in the weaning
process and dietary management during sickness. Knowledge on frequency of feeding
was, however, positively related to nutritional states. In conclusion, nutritional
knowledge alone is inadequate in ensuring young children's nutrition security and,
hence, for nutritional education programmes to have a positive impact, facilitation
strategies must be incorporated.38
Chit TM, Kyi H, Thwin A had done a study on Mothers' beliefs and attitudes
towards child weight, child feeding and related practices in Myanmar. They identified
mother's attitude and concern regarding child weight and feeding practices and also to
explore the importance of growth monitoring activity in preventing Protein Energy
Malnutrition. Trained interviewers from the respective State/Division nutrition team
interviewed ninety mothers from different areas and Divisions. Mothers were
categorized into three groups of thirty; those with a well-nourished child, a
malnourished child or a child who had died of infectious disease. 90 percent of
well-nourished children were weighed at birth and 100 percent of them had received
regular weighing. 89 percent of their mothers could identify their child birth weight as
normal and all of them know the negative health consequences of Low Birth Weight.
Regarding attitude towards feeding during illness, most mothers of a well-nourished
child believe that feeding during illness is better for recovery. That proportion is high
as twice as of the remaining groups. Data regarding child feeding practices show
mothers of a well nourished child have timely and appropriate starting of these
practices. It is inferred from the recent finding that mothers who had received growth
monitoring program since delivery have better preventive behaviour for PEM and the
role of basic health staff in these activity is also acknowledged.39
32
Das DK, Ahmed S had conducted a study on knowledge and attitude of the
Bangladeshi rural mothers regarding breast feeding and weaning. Two hundred and
forty two mothers in 7 villages of Narayanganj district, Bangladesh were interviewed
to assess their knowledge and attitude regarding breastfeeding and weaning using
pretested questionnaires, though 83.5 percent mothers knew that colostrums is good
for the child, less than 8 percent of them gave it as the first food to their babies. Most
mothers did not have the correct knowledge about exclusive breastfeeding and the
appropriate time for introduction of weaning foods; and only 3 percent of them knew
how to prepare proper weaning foods.40
Pant I, Chothia K had undertaken a study to assess maternal knowledge
regarding breast feeding and weaning practices. The knowledge of mothers of the
high income group of urban Baroda, related to breast feeding and weaning. Forty
mothers with children aged 4 to 18 months were studied. Knowledge and practices
regarding breast feeding and weaning were assessed using pre-tested questionnaires.
Results indicated that only half the mothers breast fed their babies on the first day.
Breast feeding was stopped when the child was 3-6 months; top feeding and solid
supplements were initiated at 4-6 months. Mainly commercial baby foods were used
for weaning. Most mothers avoided 'dals' for the child because these were believed to
be difficult to digest and produced gas in the child's stomach. Fifty percent of mothers
were not in favour of feeding the sick child with small frequent meals.41
Bhat lA, Shah GN, Dhar GM, Mehnaz S conducted a study on the impact of
maternal knowledge and practice on the nutritional status of infants. They interviewed
123 mothers of infants attending the child health clinic of the S.K. Institute of Medical
Sciences in Srinagar to determine whether maternal knowledge and practice were
33

associated with the nutritional status of the infants. 28 children were considered to be
well nourished, while the remaining 95 children were determined to be in various
degrees of malnutrition. Mothers whose infants were well nourished had a higher
level of breast feeding knowledge than did those whose infants were moderate to
severely malnourished. None of the mothers of malnourished infants had an excellent
score on breast feeding practices. Little difference in infant nutritional status existed
between mothers who scored fair and those who scored poor, but among mothers of
well nourished infants, those who scored well were more likely to have infants of
good nutritional status than those who did not score well. These findings show a
decreasing trend between awareness and practice of breast feeding/infant weaning;
suggesting that further improvement of health education is needed to reduce the lag
between breast feeding awareness and practice.42
Bekle A, Berhane Y conducted a study on weaning in Butajira, South Ethopia
regarding mothers’ knowledge and practices. A descriptive cross sectional study on
mothers' knowledge and practice related to weaning was conducted in Butajira in
1994. A total of 1,543 mother-child pair were included in the study, of which
1.052 children were on weaning diet and 491 were exclusively breast feeding. Among
children who were already weaned, 40 percent were reported to have been started on
weaning food at the age of 4-6 months. Of the children who were reported to be
exclusively breast feeding, 34 percent were beyond the age of 7 months. The most
commonly used weaning food were cow's milk, adult food, sorghum water and cereal
gruel in descending order and the most important reasons for mothers to start weaning
were reduction of the amount of breast milk and mothers' belief that the child is at the
right age to start weaning food. The majority of the mothers used "swallow or
34

suffocate" method in feeding their children, though cups and bottles were also
mentioned as important feeding methods. The study demonstrated the presence of
inappropriate weaning practice in the area which needs appropriate intervention.43
35
4. METHODOLOGY
Research methodology is a way to solve systematically the research problem.
The methodology enables the researcher to project a blue print of the details, data,
approach, analysis and findings of research undertaken. The methodology of research
indicates the general pattern of an organized procedure for gathering valid and reliable
data for the purpose of investigations.
This chapter includes the description of research approach, research design,
variable setting, population, sample and sample size, sampling techniques, sampling
criteria, development of tool, description of the tool, pilot study, data collection
procedure, plan of data analysis. This study was done to assess the correlation
between the feeding practices of mothers and nutritional status of their children in a
selected area Bangalore.
Research approach
A research approach tells the researcher what data to collect and how to
analyze it. It also suggests possible conclusions to be drawn from the data. In view of
the nature of the problem selected for the study and objectives to be accomplished, a
descriptive survey approach was considered as appropriate for the present study.
Research Design
A research design is a blueprint for conducting a study that maximizes control
over factors that could interfere with the validity of the findings. It is the plan and
structure and strategy of investigation of answering the research question. It helps the
36

researcher in defining the attribute, selection of population and type of statistical
analysis to interpret the data.
The investigative design selected for this study is descriptive correlative
design. The purpose of a descriptive co-relational design is to describe variables and
examine relationships among these variables.
37
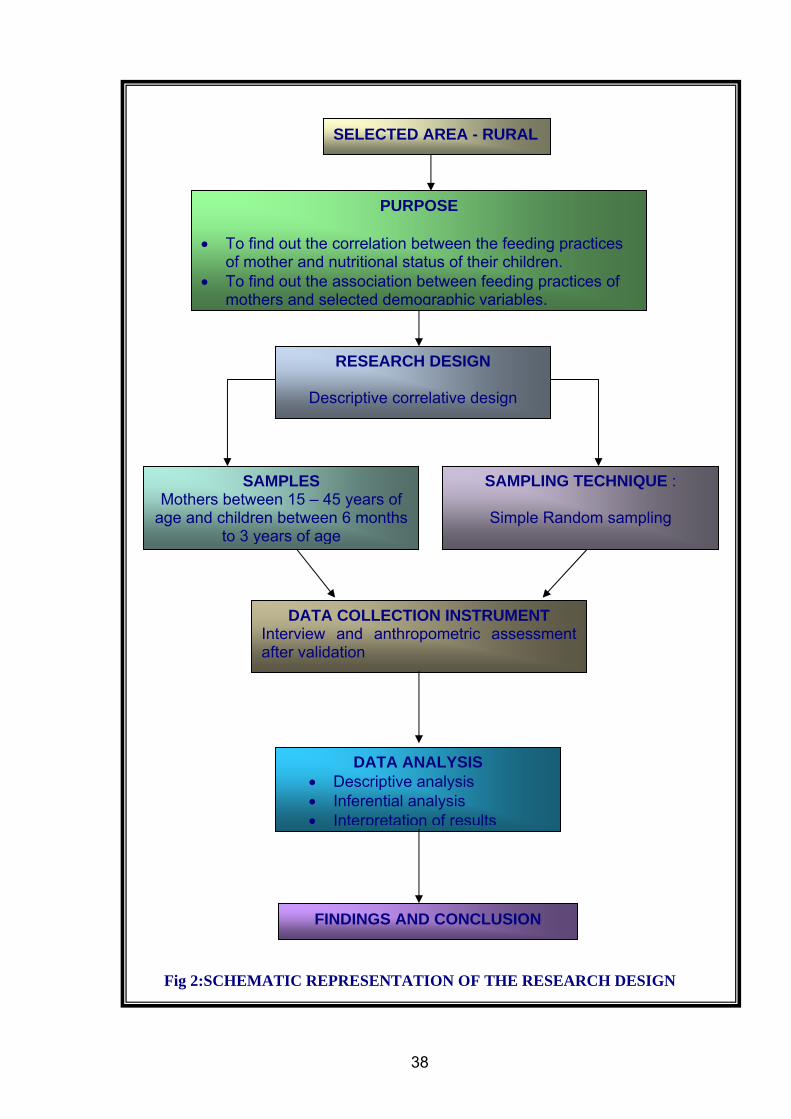
SELECTED AREA - RURAL
PURPOSE
• To find out the correlation between the feeding practices of mother and nutritional status of their children.
• To find out the association between feeding practices of mothers and selected demographic variables.
RESEARCH DESIGN
Descriptive correlative design
SAMPLES Mothers between 15 – 45 years of
age and children between 6 months to 3 years of age
SAMPLING TECHNIQUE :
Simple Random sampling
DATA COLLECTION INSTRUMENT Interview and anthropometric assessment after validation
DATA ANALYSIS • Descriptive analysis • Inferential analysis • Interpretation of results
FINDINGS AND CONCLUSION
Fig 2:SCHEMATIC REPRESENTATION OF THE RESEARCH DESIGN
38
Setting of the Study
Research setting is the specific place where data collection occurs. The
selection of setting was done on the basis of feasibility of conducting the study,
availability of the subject and co-operation from the authorities. The study was
conducted at Doddabasthi and Chikkabasthi villages under K. Gollahalli PHC.
Variables
Burns and Grove explained that research variables or concepts are the
qualities, properties or characteristics identified in the research purpose and objectives
or questions that are observed or measured in a study.
In the present study research variables are:
• Feeding practices – breast feeding, weaning and family diet.
• Nutritional status – Anthropometry measurements
Demographic variables of mothers include
• Age
• Education
• No of under five children
• Occupation,
• Duration of married life
• Family income and type of family.
Demographic variables of children
• Age
• Gender
• Birth weight
39

Population
The term population refers to the target population which represents the entire
set of individuals who meet the sampling criteria.
The total number of the houses in Chikkabasti - 275 and female population
805 and in Doddabasti, total houses 96 and female population only 230. The sample is
selected randomly. The target population for the present study comprises of all the
mother of reproductive age group and having children between 6 months to 3 years of
age and the same children residing at Chikkabasthi, Doddabasti Villages.
Sample
Sample refers to the subject of a population that is selected to participate in a
particular study.44 It is the portion of the population which represents the entire
population. In the present study samples consist of 100 mothers of reproductive age
group and 100 children of same mothers at Chikkabasthi and Doddabasthi, Bangalore.
Sampling Technique
Sampling theory point of view each individual in the population should have
an opportunity to be selected for the sample. One method of providing this
opportunity is referred to as random sampling. Hence, simple random sampling
technique was found to be apt for the study.
Sampling Criteria
Inclusion criteria
1. Mothers of children who were willing to participate in the study.
2. Both male and female children.
40

Exclusion Criteria
1. Mothers who have physically and mentally challenged children.
2. Mothers who did not have the children along with them at the time of data
collection.
Instrument
The information necessary for the study was obtained by the investigator.
Treece and Treece explained that the instrument selected in the research should be as
far as possible the vehicle that would provide data for drawing conclusions to the
study and the same time add to the body of knowledge in the discipline.45 The
instrument used for the present study is structured interview schedule.
Development of the Instrument
Instrument was developed based on
1. Review of literature
2. Consultation with guides
3. Subject experts in paediatrics and investigators
4. Consultation with statistician for data analysis
5. Spearman Brown’s formula was used for reliability.
Preparation of the blue print
A blue print was prepared prior to the construction of the questionnaire based
on which the items were developed. It depicted the distribution of items according to
the content areas. (Annexure H)
41
Description of the Tool
The instrument used in this study was structured interview schedule which
comprises of 3 sections.
Section I
Demographic Data
The first part of the tool consists of 14 items of which first 9 are related to
mothers background such as age, number of children, religion, education, occupation,
duration of married life, family income, type of family, source of information
regarding feeding practices and next five items are related to child’s age, gender, birth
weight, birth order and presence of other problem.
Section II
Check list consist of 30 items to assess the feeding practices of mothers i.e. breast
feeding, weaning and family diet. Total score is 30.
Section III
Anthropometry
Maximum Score – 30
Minimum Score – 0
Each correct item was given 1 score and wrong item was given 0 score
Content Validity
Validity refer to the degree to which an instrument measures what it is
supposed to measure. Content validity refers to the degree to which the items in an
instrument adequately represent the universe of content.
42

The prepared instrument along with the objectives, operational definitions,
blueprint, scoring key and criteria checklist for validation were submitted to 7 experts
which included 5 nurse educators, 1 paediatrician and 1 statistician to establish
content validity.
Reliability of the tool
Reliability of an instrument is the degree of consistency with which it
measures the attributes that it is supposed to measure. It refers to the extent to which
the same results are obtained on repeated administration of the instrument.
In order to establish the reliability of the tool, split half technique was used.
The tool was administered to 10 subjects and the reliability was tested by using
Spearman Brown’s prophecy formula.
Reliability of the tool was 0.9340 so the tool was found to be highly reliable
for data collection.
Pilot Study
Pilot study is a trial run study conducted before the actual study in a different
population with similar characteristics. Pilot study was conducted on 10 subjects in
Maruthinagar under K. Gollahalli, PHC, Bangalore from 7th August to 13th August.
The permission to conduct pilot study was obtained from the Medical Officer
K. Gollahalli PHC. Subjects were chosen by random sampling technique. The purpose
of the study was explained and informed consent was obtained from the samples. The
analysis was done by using descriptive and inferential statistics.
43

Data Collection Process
The data collection was from 3rd September to 3rd October 2007. Permission
was obtained from the Medical Officer, Primary Health centre, K. Gollahalli. The
investigator administered the tool to 100 mothers who were selected by using random
sampling technique after introducing and explaining the purpose of the study. Then
anthropometric measurements of their children were taken and recorded.
However, there few difficulties arose during the data collection period. Some
houses mothers had gone for work leaving their children with relatives. In certain
house mothers were there but children were with grand parents or gone to
Anganawadi. So the investigator had to exclude those families and go to the next and
get the 100 samples.
Plan for data analysis
Data was collected from 100 mothers and their children (100) from
Chikkabasthi – Doddabasthi, K.Gollahalli. The collected data was conveniently
summarized and tabulated by applying descriptive statistics such as mean, percentage,
and standard deviation.
Diagrams were used for depicting the authentic nature of at the data collected
on demographic variables and the practice aspects. Association between the selected
demographic variables and feeding practices will be analyzed by using χ2 and
presented through diagrams and tables. Correlation for the present study was
computed by using Spearman’s Rank Correlation.
44

5. RESULTS
This chapter deals with the analysis and interpretation of the data gathered to
correlate the feeding practices of mothers and nutritional status of their children.
Ordinarily the amount of data collected in a study is too extensive to be
reliably described by mere pursuit. In order to answer meaningfully the research
questions, the data must be processed and analyzed systematically and testing of
research hypothesis using those data.46
Objectives
1. To assess the feeding practices of mothers.
2. To assess the nutritional status of children.
3. To find out the correlation between the feeding practices of mothers and
the nutritional status of their children.
4. To find out the association between feeding practices and selected
variables of mothers and their children.
Organization and presentation of data
The obtained data were organized and presented under the following sections.
Section I
Describes the frequency distribution and percentage of demographic variables of
mothers and their children.
Section II
In this section mean and standard deviation of feeding practices are described.
45

Section III
Area wise classification of respondents on feeding practices is analyzed.
Section IV
Correlation between feeding practices of mothers and selected nutritional
parameters of their children.
Section V
Association between feeding practices and demographic variables of mothers
Section VI
Association between feeding practices and selected variables of children.
46
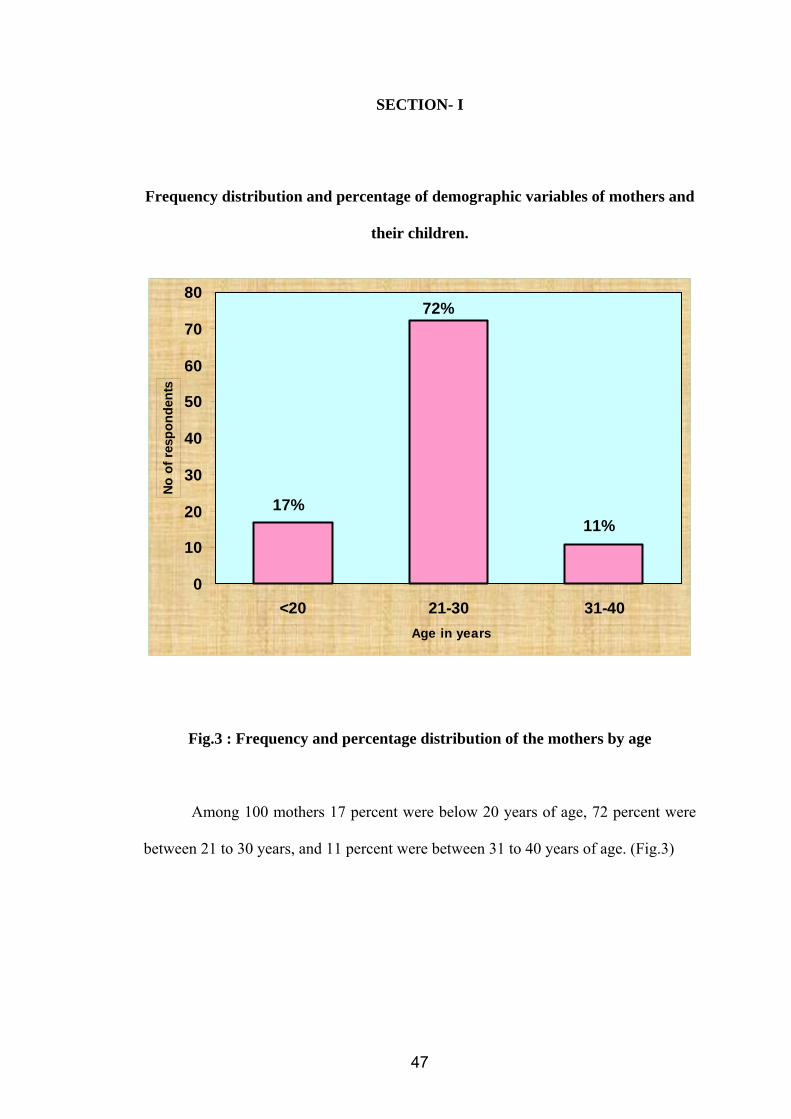
SECTION- I
Frequency distribution and percentage of demographic variables of mothers and
their children.
17%11%
72%
0
10
20
30
40
50
60
70
80
<20 21-30 31-40 Age in years
No o
f res
pond
ents
Fig.3 : Frequency and percentage distribution of the mothers by age
Among 100 mothers 17 percent were below 20 years of age, 72 percent were
between 21 to 30 years, and 11 percent were between 31 to 40 years of age. (Fig.3)
47
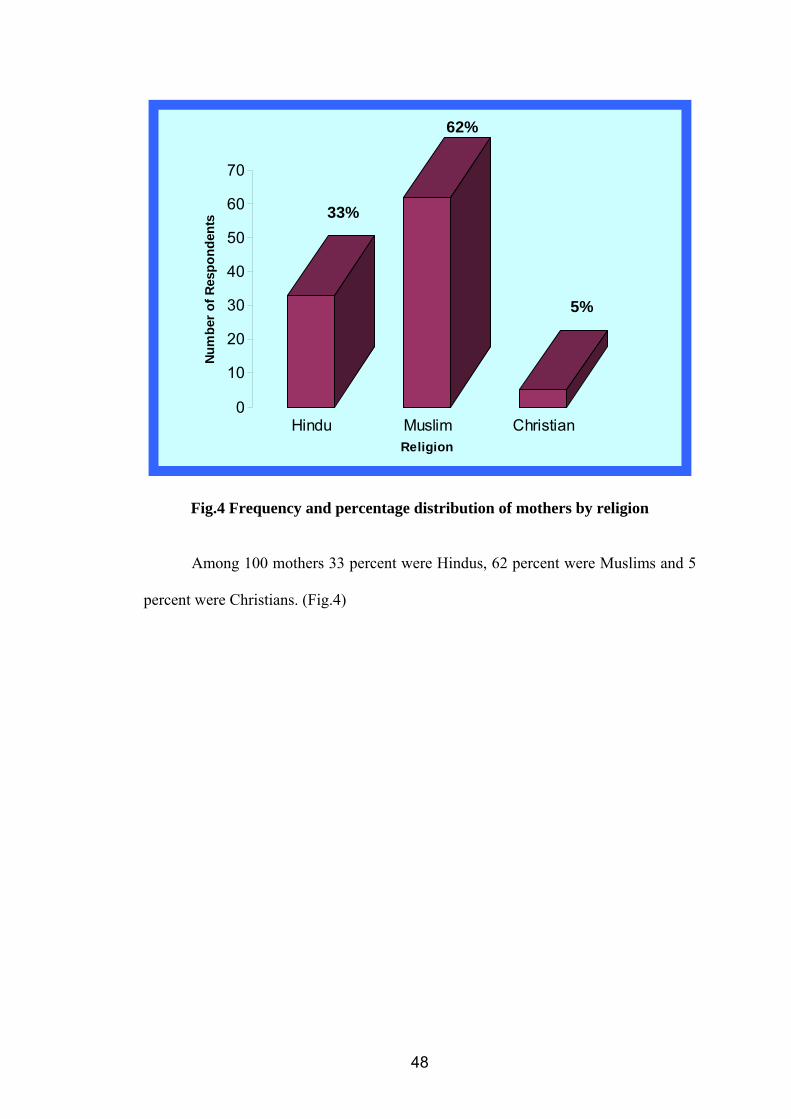
33%
62%
5%
0
10
20
30
40
50
60
70
Num
ber o
f Res
pond
ents
Hindu Muslim ChristianReligion
Fig.4 Frequency and percentage distribution of mothers by religion Among 100 mothers 33 percent were Hindus, 62 percent were Muslims and 5
percent were Christians. (Fig.4)
48
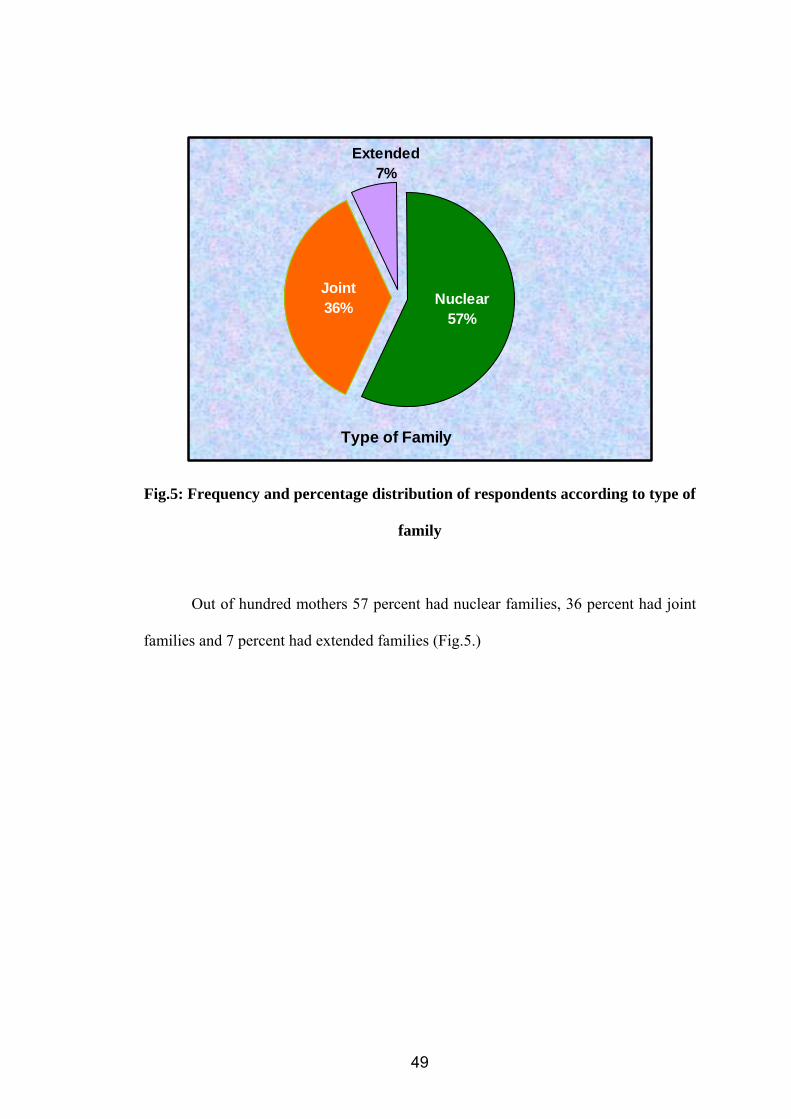
Type of Family
Extended7%
Nuclear57%
Joint36%
Fig.5: Frequency and percentage distribution of respondents according to type of
family
Out of hundred mothers 57 percent had nuclear families, 36 percent had joint
families and 7 percent had extended families (Fig.5.)
49
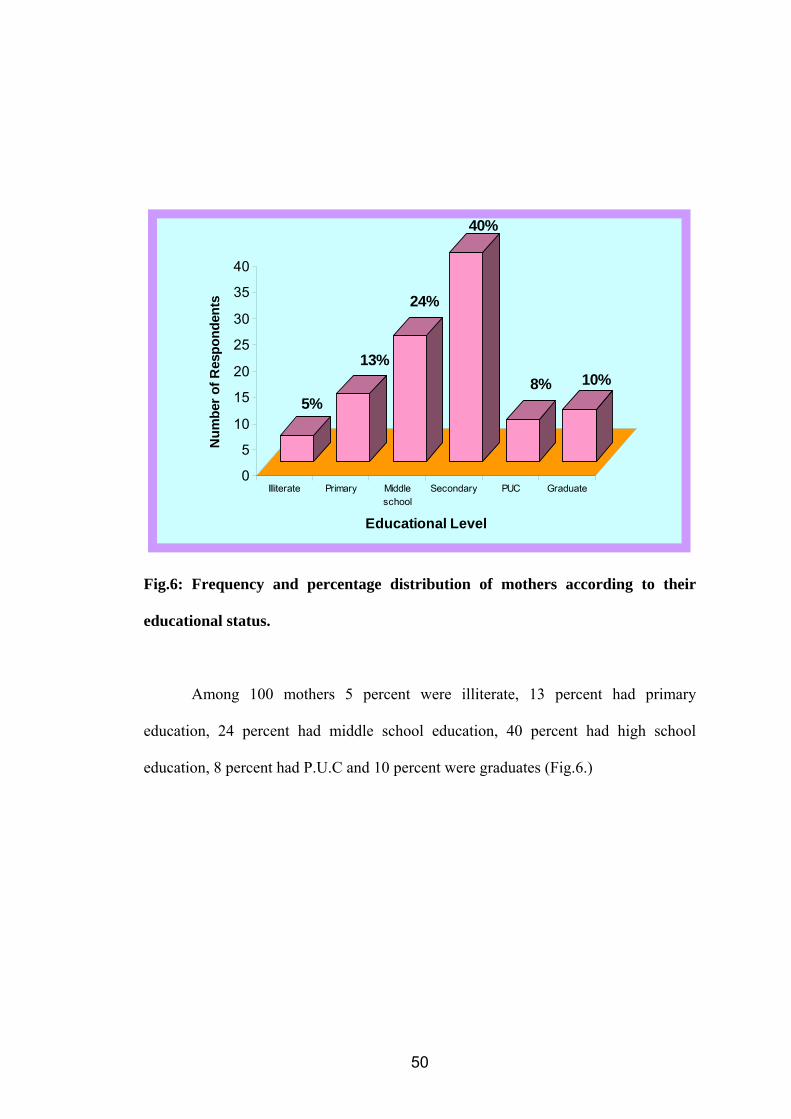
5%
13%
24%
40%
8% 10%
0
5
10
15
20
25
30
35
40
Num
ber o
f Res
pond
ents
Illiterate Primary Middleschool
Secondary PUC Graduate
Educational Level
Fig.6: Frequency and percentage distribution of mothers according to their
educational status.
Among 100 mothers 5 percent were illiterate, 13 percent had primary
education, 24 percent had middle school education, 40 percent had high school
education, 8 percent had P.U.C and 10 percent were graduates (Fig.6.)
50
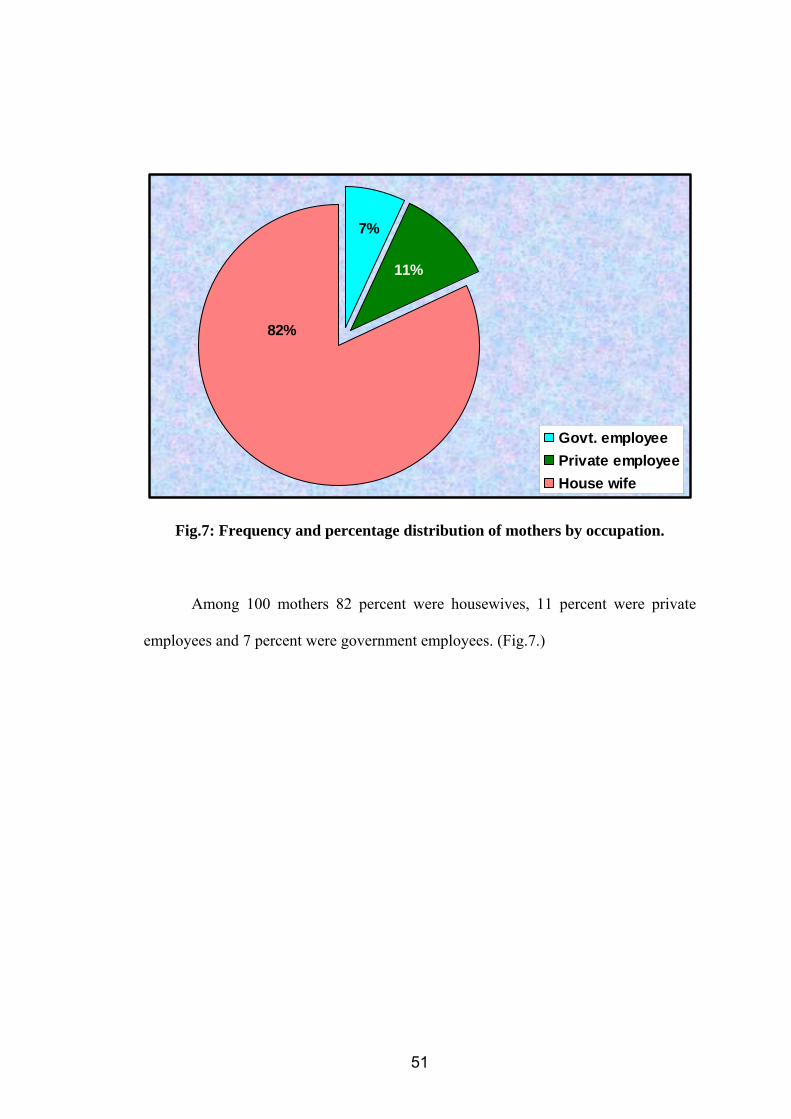
82%
7%
11%
Govt. employeePrivate employeeHouse wife
Fig.7: Frequency and percentage distribution of mothers by occupation.
Among 100 mothers 82 percent were housewives, 11 percent were private
employees and 7 percent were government employees. (Fig.7.)
51

79%
12% 9%
0
10
20
30
40
50
60
70
80
90
<5000 5001-10,000 >10,000
Family Income
Num
ber o
f Res
pond
ents
Fig.8: Frequency and percentage distribution of mothers by family income
Among 100 mothers 79 percent had family income below Rs.5,000, 12 percent
had family income between 5,001 to 10,000 and 9 percent had above Rs.10,000.
52
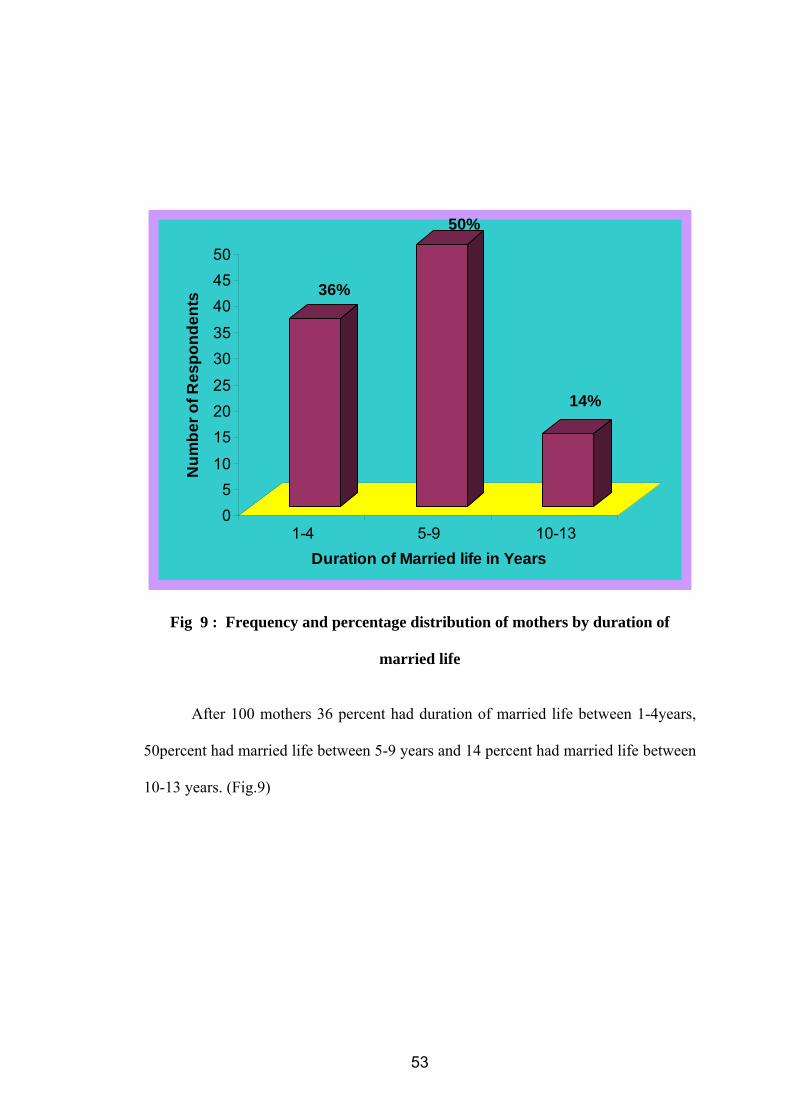
36%
50%
14%
05
10
152025
3035
404550
Num
ber o
f Res
pond
ents
1-4 5-9 10-13Duration of Married life in Years
Fig 9 : Frequency and percentage distribution of mothers by duration of
married life After 100 mothers 36 percent had duration of married life between 1-4years,
50percent had married life between 5-9 years and 14 percent had married life between
10-13 years. (Fig.9)
53

60%
40%
0
10
20
30
40
50
60
Num
ber o
f Res
pond
ents
1 2
No. of under five children
Fig 10 : Frequency and percentage distribution of no of under five children
Among 100 mothers 60 percent had only one childe below five years and 40
percent had 2 children below 5 years of age. (Fig 10)
54

43% 44%
13%
0
5
10
15
20
25
30
35
40
45
Num
ber o
f Res
pond
ents
Familymembers/relatives/friends
Radio/TV Books/Journals
Sources of Information
Fig.11 : Frequency and percentage distribution of respondents by source of
information
Among 100 mothers 43 percent had family members / relatives / friends as
source of information, 44 percent had radio / T.V and 13 percent had books / journals
as source of information (Fig.9)
55
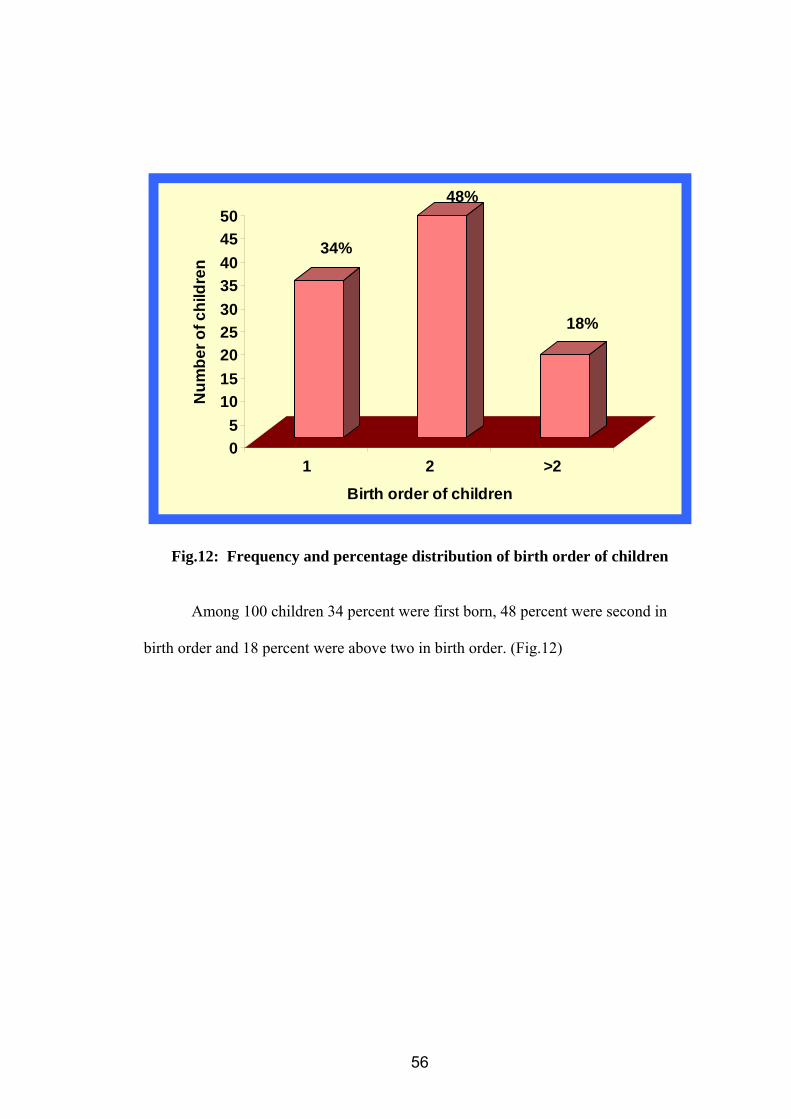
34%
48%
18%
05
101520253035404550
Num
ber o
f chi
ldre
n
1 2 >2
Birth order of children
Fig.12: Frequency and percentage distribution of birth order of children
Among 100 children 34 percent were first born, 48 percent were second in
birth order and 18 percent were above two in birth order. (Fig.12)
56
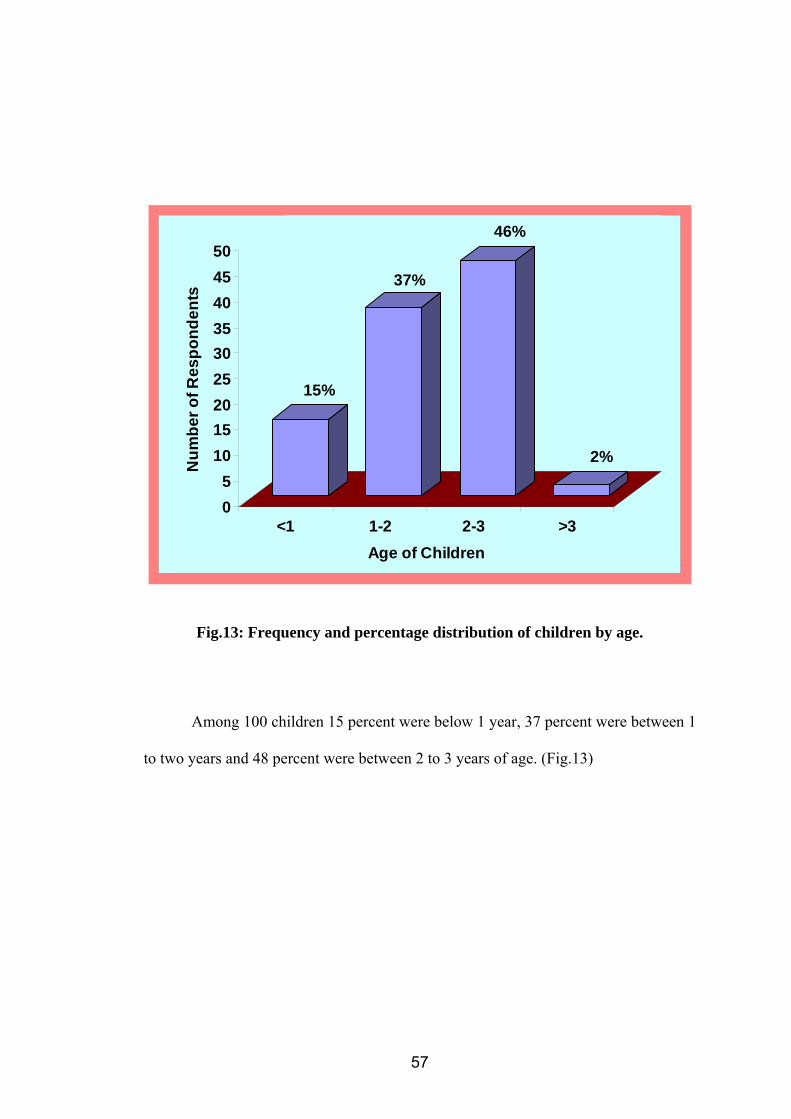
15%
37%
46%
2%
05
101520253035404550
Num
ber o
f Res
pond
ents
<1 1-2 2-3 >3Age of Children
Fig.13: Frequency and percentage distribution of children by age.
Among 100 children 15 percent were below 1 year, 37 percent were between 1
to two years and 48 percent were between 2 to 3 years of age. (Fig.13)
57

Gender of Children
Male 48% Female
52%
Fig.14: Frequency and percentage distribution of children by gender.
Among 100 children 52 percent were females and 48 percent were males.
58

SECTION II
TABLE 1
Area wise analysis of mean and standard deviation of feeding practices of
mothers
n =100
Sl. No Area wise analysis Max. score Range Mean SD Mean
% 1 Breast feed 9 5-9 6.98 0.84 77.56 2 Weaning 10 4-10 7.11 1.08 71.10 3 Family diet 11 1-11 5.28 1.96 48.00
Total 30 13-15 19.37 2.51 64.57
The total score 30. The total mean feeding practices was 19.37 with a standard
deviation of 2.51 while total mean percentage was 64.57. (Table 1).
59
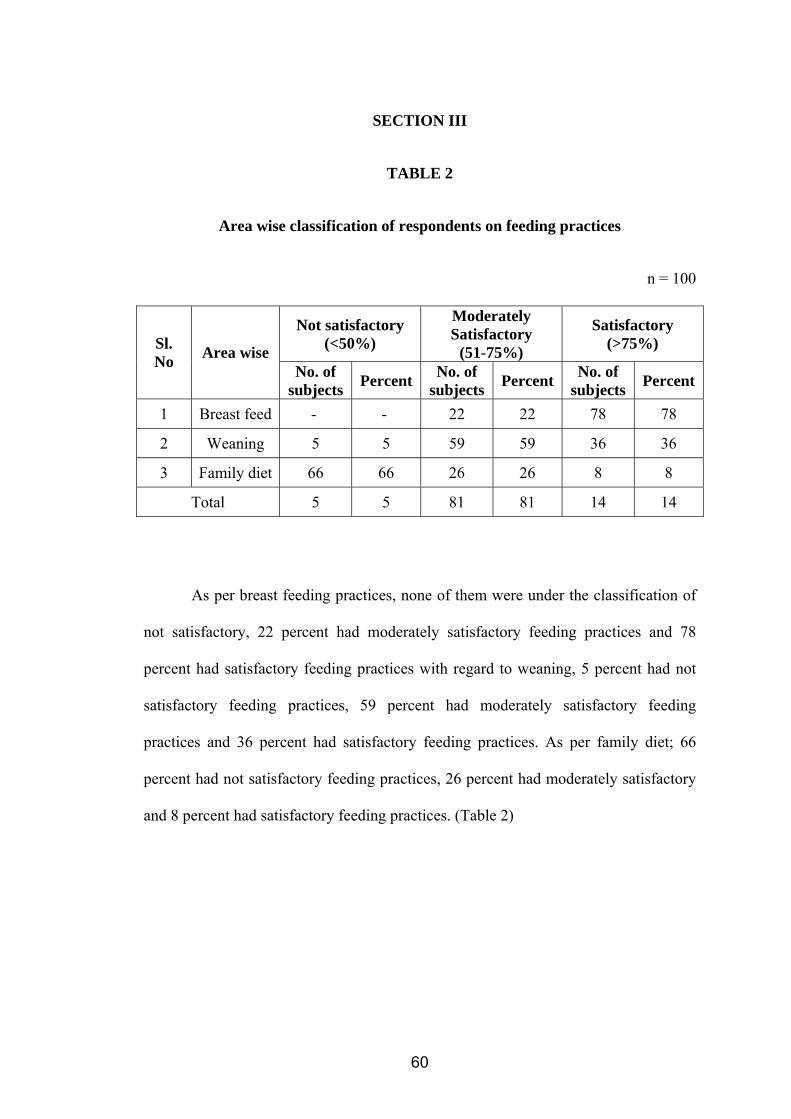
SECTION III
TABLE 2
Area wise classification of respondents on feeding practices
n = 100
Not satisfactory (<50%)
Moderately Satisfactory
(51-75%)
Satisfactory (>75%) Sl.
No Area wise No. of
subjects Percent No. of subjects Percent No. of
subjects Percent
1 Breast feed - - 22 22 78 78
2 Weaning 5 5 59 59 36 36
3 Family diet 66 66 26 26 8 8
Total 5 5 81 81 14 14
As per breast feeding practices, none of them were under the classification of
not satisfactory, 22 percent had moderately satisfactory feeding practices and 78
percent had satisfactory feeding practices with regard to weaning, 5 percent had not
satisfactory feeding practices, 59 percent had moderately satisfactory feeding
practices and 36 percent had satisfactory feeding practices. As per family diet; 66
percent had not satisfactory feeding practices, 26 percent had moderately satisfactory
and 8 percent had satisfactory feeding practices. (Table 2)
60
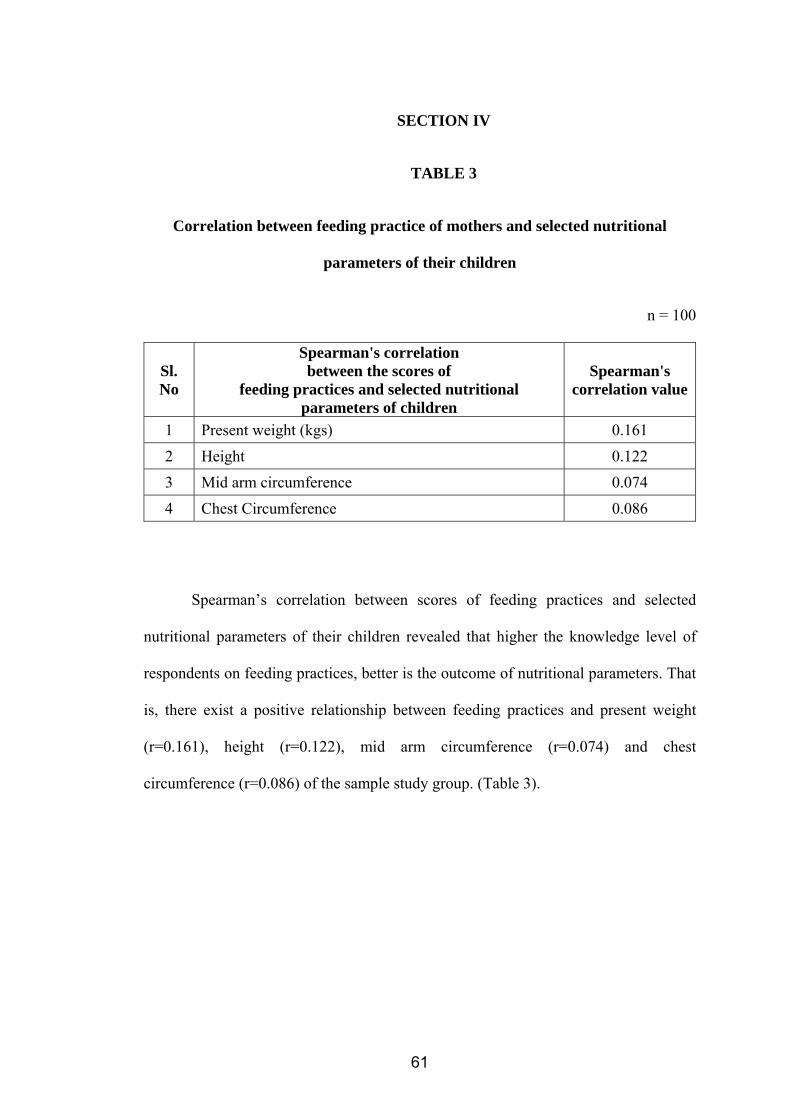
SECTION IV
TABLE 3
Correlation between feeding practice of mothers and selected nutritional
parameters of their children
n = 100
Sl. No
Spearman's correlation between the scores of
feeding practices and selected nutritional parameters of children
Spearman's correlation value
1 Present weight (kgs) 0.161 2 Height 0.122 3 Mid arm circumference 0.074 4 Chest Circumference 0.086
Spearman’s correlation between scores of feeding practices and selected
nutritional parameters of their children revealed that higher the knowledge level of
respondents on feeding practices, better is the outcome of nutritional parameters. That
is, there exist a positive relationship between feeding practices and present weight
(r=0.161), height (r=0.122), mid arm circumference (r=0.074) and chest
circumference (r=0.086) of the sample study group. (Table 3).
61
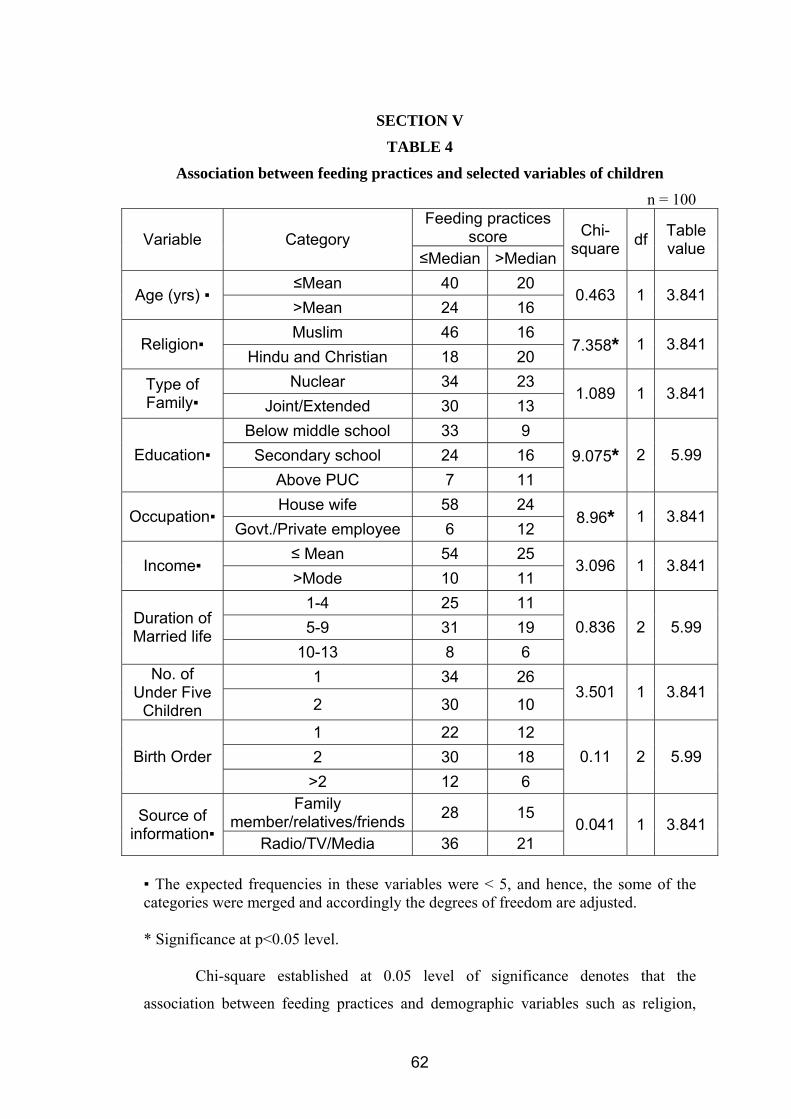
SECTION V
TABLE 4
Association between feeding practices and selected variables of children n = 100
Feeding practices score Variable Category
≤Median >Median
Chi-square df Table
value
≤Mean 40 20 Age (yrs) ▪
>Mean 24 16 0.463 1 3.841
Muslim 46 16 Religion▪
Hindu and Christian 18 20 7.358* 1 3.841
Nuclear 34 23 Type of Family▪ Joint/Extended 30 13
1.089 1 3.841
Below middle school 33 9 Secondary school 24 16 Education▪
Above PUC 7 11 9.075* 2 5.99
House wife 58 24 Occupation▪
Govt./Private employee 6 12 8.96* 1 3.841
≤ Mean 54 25 Income▪
>Mode 10 11 3.096 1 3.841
1-4 25 11 5-9 31 19 Duration of
Married life 10-13 8 6
0.836 2 5.99
1 34 26 No. of Under Five
Children 2 30 10 3.501 1 3.841
1 22 12 2 30 18 Birth Order
>2 12 6 0.11 2 5.99
Family member/relatives/friends 28 15 Source of
information▪ Radio/TV/Media 36 21 0.041 1 3.841
▪ The expected frequencies in these variables were < 5, and hence, the some of the categories were merged and accordingly the degrees of freedom are adjusted. * Significance at p<0.05 level.
Chi-square established at 0.05 level of significance denotes that the
association between feeding practices and demographic variables such as religion,
62
education and occupation were statistically significant. However the Chi-square value
established at 0.05 level of significance denotes that the association between feeding
practices and demographic variables like age, type of family, income, duration of
married life, number of under five children, birth order and source of information
were not statistically significant. (Table 4).
63
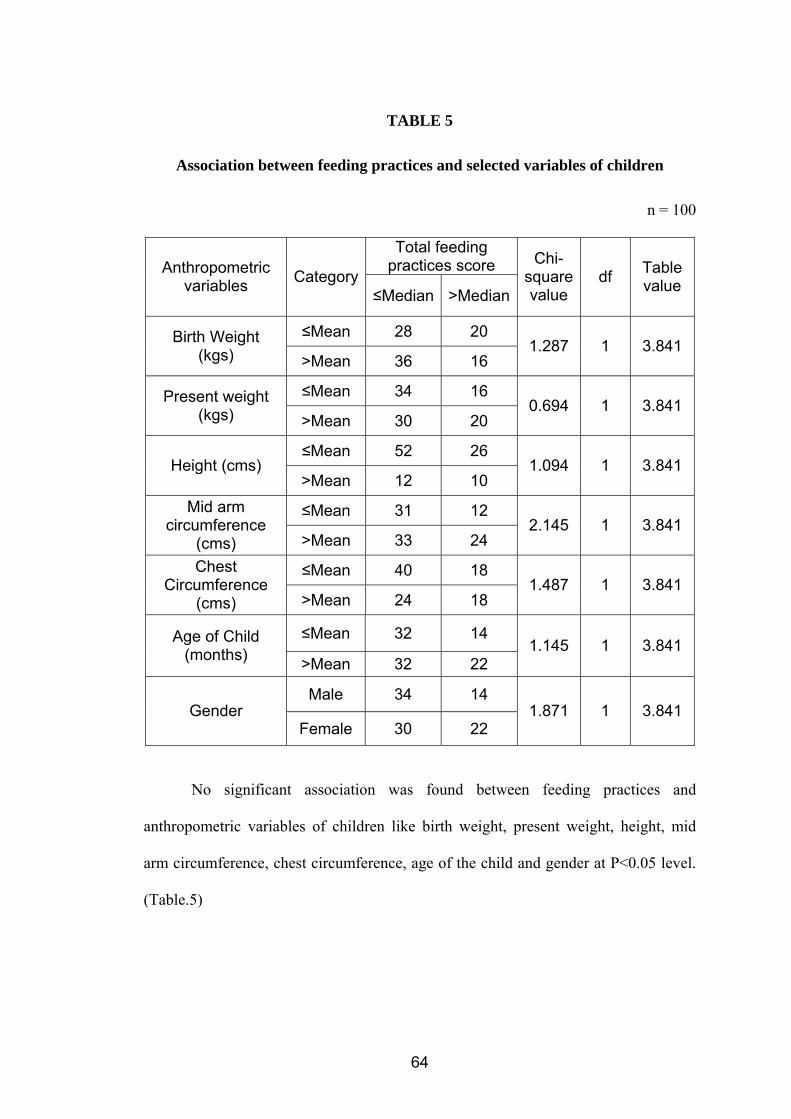
TABLE 5
Association between feeding practices and selected variables of children
n = 100
Total feeding practices score Anthropometric
variables Category≤Median >Median
Chi-square value
df Table value
≤Mean 28 20 Birth Weight (kgs) >Mean 36 16
1.287 1 3.841
≤Mean 34 16 Present weight (kgs) >Mean 30 20
0.694 1 3.841
≤Mean 52 26 Height (cms)
>Mean 12 10 1.094 1 3.841
≤Mean 31 12 Mid arm circumference
(cms) >Mean 33 24 2.145 1 3.841
≤Mean 40 18 Chest Circumference
(cms) >Mean 24 18 1.487 1 3.841
≤Mean 32 14 Age of Child (months) >Mean 32 22
1.145 1 3.841
Male 34 14 Gender
Female 30 22 1.871 1 3.841
No significant association was found between feeding practices and
anthropometric variables of children like birth weight, present weight, height, mid
arm circumference, chest circumference, age of the child and gender at P<0.05 level.
(Table.5)
64
6. DISCUSSION
The present study was aimed to correlate the feeding practices of mothers and
nutritional status of their children. The correlation was done by making association
between the demographic variables and feeding practices and correlation coefficient
between feeding practices and parameters.
The study was conducted in Chikkabasthi and Doddhabasthi among
reproductive age group of mothers who have children between the age of 6 months
and 3 years.
A structured interview schedule was used to assess the feeding practices
among mothers. The research design adopted for the study was descriptive correlative
design. Random sampling technique was used to select 100 mothers and their children
between the age group of 6 months to 3 years from rural communities.
Main findings of the study were discussed under the following sections.
Section – 1
Findings related to the demographic characteristics of respondents
Among 100 mothers, 17 percent of them were below 20 years of age, 72
percent of them were between 21 – 30 years and 11 percent were between 31 – 40
years of age. 3 percent among the total respondents were Hindus, 62 percent of them
were Muslims and 5 percent of them were Christians. 57 percent of them belonged to
nuclear families, 36 percent of them lived in joint families and 7 percent of them lived
in extended families. Education wise, only 5 of them were illiterate, 13 percent had
primary education, 24 had middle school education, 40 percent had high school
65
education, 8 percent were educated upto PUC and 10 percent of them were graduates.
Occupation wise, 82 percent of them were housewives, 11 percent of them were
private employees and 7 percent were government employees. Family income wise,
79 percent of them had an income of below Rs. 5000, 12 percent of them had an
income between Rs.5001 and Rs.10000 and 9 percent of them had a family income of
above Rs. 10000. Among the total mother respondents 36 percent had a duration of
1 – 4 years of married life, 50 percent had a duration of 5 – 9 years of married life and
14 percent had a duration of 10 – 13 years of married life.
Among the 100 subjects, 60 percent had only 1 child below 5 years and 40 percent
of them had 2 children below 5 years of age.43 percent of the respondents attributed
family members/ relatives/ friends as the source of information on feeding practices, 4
percent attributed the same to radios/ television and 13 percent of them attributed it to
books and journals. Among 100 children 34 percent were first born, 48 percent were
2 nd in birth order and 18 percent of them held an ordinal position of >2. 15 percent
of the children were below 1 year, 37 percent were between 1 – 2 years of age and 48
percent were 2 to 3 years of age. Among the total children subjects 52 percent of them
were females and 48 percent of them were males.
The first objective was to assess the feeding practices of mothers
Breast feeding aspect maximum score was 9 and response on feeding practice
mean 6.98, mean percentage 77.56 and SD 0.84. Weaning aspect maximum score 10
and response on feeding practice mean 7.11, mean percentage 71.10 and SD 1.08.
Family diet – maximum score 11, mean 5.28, mean percentage 48.00 and SD 1.96.
66

The second objective was to assess the nutritional status of children
As per breast feeding practices, none of them were under the classification of
not satisfactory, 22 percent had moderately satisfactory feeding practices and 78
percent had satisfactory feeding practices with regard to weaning, 5 percent had not
satisfactory feeding practices, 59 percent had moderately satisfactory feeding
practices and 36 percent had satisfactory feeding practices. As per family diet; 66
percent had not satisfactory feeding practices, 26 percent had moderately satisfactory
and 8 percent had satisfactory feeding practices.
The third objective was to find out correlation between the feeding practices of
mothers and the nutritional status of their children.
Spearman’s correlation between scores of feeding practices and selected nutritional
parameters of their children revealed that higher the knowledge level of respondents on
feeding practices, better is the outcome of nutritional parameters. That is, there exist a
positive relationship between feeding practices and present weight (r=0.161), height
(r=0.122), mid arm circumference (r=0.074) and chest circumference (r=0.086) of the sample
study group.
The fourth objective was to find out the association between feeding practices of
mothers and their children with selected variables.
Chi-square established at 0.05 level of significance denotes that there is
statistically significant association between feeding practices and demographic
variables of mothers such as religion, education and occupation. The remaining
variables are found non-significant.
67

No significant association was found between feeding practices and
anthropometric variables of children like age, gender, birth weight, present weight,
height, mid arm circumference and chest circumference at p<0.05 level.
Testing of hypothesis
H1: There is correlation between feeding practices of mothers and nutritional status of
their children.
Since there exist a positive relationship between feeding practices and present weight
(r=0.161), height (r=0.122), mid arm circumference (r=0.074) and chest circumference
(r=0.086), the researcher concluded that there is positive correlation between feeding
practices of mothers and nutritional parameters of their children. Hence the score is positive
the hypothesis is accepted.
68
7. CONCULSION
The present study was aimed to correlate the feeding practices of mothers and
nutritional status of their children. The correlation was done by making association
between the demographic variables and feeding practices and correlation coefficient
between feeding practices and parameters.
The study was conducted in Chikkabasthi and Doddhabasthi among
reproductive age group of mothers who have children between the age of 6 months
and 3 years.
A structured interview schedule was used to assess the feeding practices
among mothers. The research design adopted for the study was descriptive correlative
design. Random sampling technique was used to select 100 mothers and their children
between the age group of 6 months to 3 years from rural communities.
The following conclusions are made from the study
• The participants included in the study were between the age group of 18 – 40
years.
• There is non significant association between age of the mothers and feeding
practices.
• As per educators 5 percent illiterate, 8 percent PUC, 10 percent graduates and 13
percent primary school, 24 percent middleclass school and 40 percent high school.
• There was significant association between education and feeding practice.
• With regard to under five children most of them had only one child and others 2.
• But there was not significant association between no of under five children and
feeding practices.
69
• Occupation wise most of them were housewives 82 percent, 7 percent government
employees and 11 percent private employees respectively.
• There was significant association between occupation and feeding practices.
• As per family income, most of them had below Rs.5000, 12 percent had between
5,001 to 10,000 and 9 percent had above Rs.10,000 as family income.
• With regard to duration of married life – up to 1 to 4 years 36 percent, 5-9 years
50 percent above 10 years 13 years 14 percent were there. But there was no
association between duration of married life and feeding practice of mothers.
• As per source of information TV / radio was used by 44 percent, family members /
relatives 43 percent and book/journal was used by 13 percent.
• Correlation between feeding practices and nutrition parameter; present weight r =
0.161, height r = 0.122, mid arm circumference r = 0.074 and chest circumference
r = 0.086 were positively correlated.
So findings of the study reveal that there is a positive correlation between
feeding practices of mothers and nutritional status of their children’s parameters.
Implications of the study
The findings of the study have implications in various fields of nursing. They
are:
• Nursing education
• Nursing practices
• Nursing administration
• Nursing research
70

Nursing Education
Nursing education emphasizes on preparing dedicated nurse to impart health
education both in community settings and clinical areas by using various methods of
educational technology to improve the feeding practices.
Nursing Practice
“When love and skill work together expect a master piece”.
– John Ruskin
Nurse plays an important role in the feeding of children. It starts even before a
mother is pregnant. Through health education demonstration of preparation of feed
and feeding, nurse can help to improve the feeding practices of mothers wherever it is
needed. Not only during infancy, but also till adolescence this teaching has to be
continued. Planned health teaching programme can be made ongoing process both in
clinical setting as well as in community setting is mandatory.
Nursing Administration
Nursing administration should have proper vision and mission while making
and implementing the policy with regard to health care of the children. Since children
are the dependable and vulnerable population, mothers should be taken into
consideration for the improvement of children’s nutritional status.
Nursing Research
We can bring about a tremendous improvement in the health status of children
through research. Though the present correlative study is like a drop in an ocean, can
prepare the path for future quantitative and qualitative research to improve the feeding
practices of mothers to establish a better nutritional status for their children.
71
Limitations
• Only certain parameters were used to assess the nutritional status of children.
• Interview technique does not collect the accurate data regard to feeding practices.
• The tool used by the investigator needs a broad and comprehensive validation.
Recommendations
• Study can be replicated in different community setting
• Structured teaching program can be arranged for mother as part of experimental
study to improve their feeding techniques.
• A comparative study can be conducted between rural and urban settings.
72
8. SUMMARY
The main purpose of the study was to correlate the feeding practice of mothers
and nutritional status of their children.
Objectives of the study were
1. To assess the feeding practices of mothers
2. To assess the nutritional status of children
3. To find out the correlation between the feeding practices of mother and the
nutritional status of their children.
4. To find out the association between feeding practices of mothers and their
children with selected variables.
The conceptual frame work adopted for this study was based on Rosenstoch’s
and Becker’s health belief model.
The review of related literature and non research literature helped the
investigator to develop the conceptual frame work, structured interview schedule and
plan for data analysis.
The study was conducted in Doddabasthi and Chikkabasthi from 3rd
September to 3rd October 2007. The study adopted descriptive survey approach with
random sampling technique.
Sample of the study consisted of 100 rural mothers and their children. The tool
used for data collection was structured interview schedule.
73

It consists of the following sections
Section I
Deals with demographic variables which include age of the mothers. Number
of under five children, religion, education, occupation duration of married life, family
income, type of family, source of information regarding feeding practices.
Also children’s demographic variables such as age, gender, birth weight, birth
order and presence of other problems.
Section II
It consists of 30 items with regard to practices of mothers concerning breast
feeding, weaning and family diet. Total score was 30.
The steps involved in the development of instruments were preparation of blue
print, construction of items, content validity and preparation of the final copy of the
tool.
After obtaining formal permission from Medical officer of K. Gollahalli, PHC,
the tool was used for data collection. Then the collected data were analyzed using
descriptive and inferential statistics and interpreted in terms of objectives.
Section III
Deals with the anthropometry of the children
74
Major findings of the study
1. Findings regarding the demographic characteristics of the respondents
Participants included in the study were mothers between 18 to 40 years of age.
Majority of them (72 percent) were between 21 to 30 years. Most of them (62 percent)
were Muslims. There were 33 percent Hindus and only 5 percent Christians. Majority
(57 percent) had nuclear families, 36 percent had joint families and only 7 percent had
extended families.
With regard to education ; majority (40 percent) had high school education,
only 5 percent illiterates and 10 percent graduates were there as per occupation 82
percent were housewives. 11 percent private employees and only 7 percent
Government employees. As per family income 79 percent had below Rs.5,000, 12
percent had between 5,001 to 10,000 and only 9 percent had above Rs.10,000 as their
income. Half (50 percent) of them had married life between 5 to 9 years, 36 percent
between 1 to 4 years and only 14 percent between 10 to 13 years. Among them 60
percent had only 1 child below five years and 40 percent had 2 children below five
years.
As source of information 44 percent had TV/Radio, 43 percent had family
members/relatives/friends and only 30 percent used mass media.
With regard to children 48 percent were between 2 to 3 years of age, 37
percent between 1 to 2 years and only 15 percent below 1 year. Among them 52
percent females and 48 percent males were there.
75

2. Findings pertaining to area wise classification of feeding practices
Breast feeding: 78 percent adequate, 22 percent satisfactory and none of them had
not satisfactory feeding practices.
Weaning : 5 percent not satisfactory, 59 percent satisfactory and 36 percent had
adequate feeding practices.
Family diet: 66 percent not satisfactory, 26 percent satisfactory and 8 percent had
adequate feeding practices. Overall 5 percent not satisfactory, 81 percent satisfactory
and 14 percent had adequate feeding practices.
3. Correlation between feeding practices and selected nutritional parameters.
Finally, it is found that there is a positive correlation between mothers feeding
practices and nutritional status of their children. Spearman’s Rank Correlation value
to correlate the feeding practices of mothers and selected nutritional parameters of
children is found to be r = +0.161 for the present weight (kgs), r = +0.122 for height,
r = +0.074 for mid arm circumference and r =+ 0.086.
4. Association between demographic variables and feeding practices.
There were significant association between demographic variables like
religion, education and occupation of mothers and feeding practices. However there
was no significant association between demographic variables such as age, type of
family, income, duration of married life, number of under 5 children, birth order, age
of the child, gender and source of information.
76
9. BIBLIOGRAPHY
1. Child development – An Introduction available from:
http://wcd.nic.in/cdintro.html [cited 2007 Sep 22].
2. Srivatsava N, Sandhu A. Index for Measuring Child Feeding Practices. Indian
J. Pediatr. 2007 April; vol. 74(4): 363-8.
3. David P. Nutrition Assessment of Infant and Toddlers. Healthy Child Care
2003 [online]. [cited 2007 May 6]; Available from:
http://www.frontiernet/~manage/ccni
4. Engle PL, Pelto G, Bentley. Care for Nutrition and Development. JIMA. 2000
Sep. vol. 98, No.9.
5. Breastfeeding and Family Foods Loving and Healthy [editorial] Pediatric
Companion April – June 2005.
6. Gosh S. Integrated Child Development Services Programme – Need for Re-
appraisal. Indian Pediatr. 1997; 34: 911-8.
7. Child Malnutrition and feeding practices in Malawi.
www.unu.edu/unupress/foodN182e/ch13.htm
8. Park k. Parks text book of preventive and social medicine. 18th ed. Jabalpur:
Banarsidas Bhanot; 2005. P 399
9. Dr. BT Basavanthappa. Nursing research. New Delhi : Jaypee Brothers; 2005.
P 113-23
77
10. Linkages. Facts for feeding. Academy for Educational development.1825
Connecticut, Ave, NW, Washington UK. www.linkagesproject.org
11. Redding A.B, Marlow RD. Text book of pediatric Nursing. 6th ed. New Delhi:
Elsevier; 2005. P 584-8
12. Mitra M, Kumar PV, Chakrabarty S, Bharath P. Nutritional Status of Kamar
Tribal children in Chhittisgarh. Indian J Peadtr. 2007 Apr; vol.74(4): 381-4
13. Sachdev HPS. Nutrition status of Children and Women in India, Recent
Trends. Nutrition foundation of India Events at NFI, 1997 Jul.
14. Sharma S, Nagar S. Impact of Educational Intervention on knowledge of
mothers regarding child care and nutrition in Himachal Pradesh. J. Soc. Sci;
12(2); 2006. 139-42.
15. Nyarucucha CN, Msuya JM, Mamira PS, Kerengi AJ. Nutritional status and
Feeding Practives of under five children in Simanjiro Dt. Tanzania. Tanzania
Health Research Bulletin, 2006. Vol.8. No.3 P162-7.
16. Ray SK, Biswas AB, Kumar S. A study of Dietary Pattern, Household Food
Security and Nutritional Profile of Under-five Children of a Community of
West Bengal. Vol. 98, No. 9, Culcatta : JIMA advertiser ; 2002 P 519.
17. Kumar D, Goel NK, Poonam Sing, Mittal. Influence of infant feeding
practices on nutritional status of under five children. Indian J. Pediatr. 2006
May; Vol.73(5): 417-21.
78

18. Yadav RJ, Singh P. Factors influencing Nutritional Status of Children in
Bihar, Available from : http//www.indianpediatrics.net/ictt2.html [cited 2007
Sep 23].
19. Potter PA, Perry AG. Fundamentals of Nursing. 6th Ed. New Delhi: Mosby;
2005. P 91-2.
20. Hannan A, Hassan MQ, Fazlur AK, Rahman A. Infant feeding practices from
birth to 2 years of age and nutritional status of children and mothers in
Bangladesh. 10th ASCON Abstract No: 133, Dhaka 1362, Bangladesh.
21. Kamau TF, O Mwega GM, Muita JW. Child care practices and nutritional
status of children aged 0-2 years in Thika, Kenya. East Afr Med J. 2002 Oct;
79(10): 524-9. Available PMID: 12635757.
22. Ruel MT, Menon P. Child feeding practices are associated with child
nutritional status in Latin America: innovative used of the demographic and
health surveys. J Nutr. 2002 Jun; 132(6): 1180-7. Available PMID: 1204231.
23. Alvarado BE, Tabarer RE, Delisle H, Zunzunegni MV. Maternal beliefs,
feeding practices and nutritional status in Afro – Colombian infants. Arch
Latinoam Nutr. 2005 Mar; 55(1): 55-63. Available PMID 16187679.
24. Chirmulay D, Nisal R. Nutritional status of tribal under five children in
Ahemadnagar District, Maharastra in relation to weaning/feeding practices.
Indian Pediatr. 1993 Feb; 30(2):215-22. Available from PMID: 8375884
79

25. Abdul Sayed ZT, Latham MC, Roe DA. Prolonged breast feeding without the
introduction of supplementary feeding. J Trap Pediatr. 1995 Feb;41(1):29-33.
Available PMID: 7723126.
26. Hossain IM, Yasmin R, Kabir I. Nutritional and immunization status, weaning
practices and socio economic conditions of under five children in three
villages of Bangladesh. Indian J Public Health. 1999 Jan – Mar; 43(1): 31-41.
Available PMID 11243087.
27. Excler JL, Nicolas E, Mojon M. Protein – energy malnutrition in an urban
African milieu Med Trop (Mars). 1985 Apr – Jun; 45(2): 155 – 61. Available
PMID: 3978552.
28. Hasan J, Ray J, Khan Z. Role of meaning in the nutritional status of infant-a
longitudinal study in the rural area of Aligarh. J. Indian med Assoc. 1996
May; 94(5):169,215. PMID:8855567
29. Osuhar PC. Weaning practices in Kaduna. Northern Nigeria. Indian J public
Health. 1986 Jul-Sep Indexed for MEDLINE(3):138-44 Available PMID:
3610298.
30. Puri RK, Suchdeva R. Development low cost supplementary foods for infants
and children from locally available food in Punjab Child care Health Dev.
1984 Jul-Aug;19 (4);227-36. Available PMID: 6434193.
31. Jansena A. Malnutrition and child feeding practices in western Samoa. J Trop
Pediatr Eniron child Health. 1977 Dec; 23(6): 293-306. Available PMID:
415150.
80

32. Malla S, Sherestha. Complementary feeding practices and its impact on
nutritional status of under two year old children in urban area of the
Kathmandu, Nepal. Journal of Nepal Health Research Council. 2004 Apr ;
Vol.2. No.1.
33. Heath AL, Tuttle CR, Simons MS, Cleghorn CL. A longitudinal study of
breast feeding and weaning practices during the first year of life in Dunedin,
New Zealand. J Am Diet Assoc. 2002 Jul; 102(7): 937-43. Available PMID:
12146555.
34. Hussain AM. Rafiquzzaman M. Determinants of weaning age in rural
Bangladesh. Soc Biol, 1994 Spring – Summer; 41(1-2): 78-82. Available
PMID 7973842.
35. Moussa WA, Tadros MD, Mekhael KA. Some simple methods of home
processing and their implications with weaning foods. Nahrung. 1992; 36(1):
26-33. Available PMID: 1579153.
36. Appah LY, Krehling S. Meternal Nutritional Knowledge and Child Nutritional
Status in Volta region of Ghana. Matern Child Nutr. 2005 April. [cited on
2007 June 1]; 1(2): 100-10. Available PMID: 16881885 [pubmed-indexed for
medline]
37. Tada Y, Keiwkarnka B, Pancharuriti N, Chamaroonsawasdi K. Nutritional
Status of preschool children of the Klong Toey slum Bangkok. Southern Asian
J Trop Med Public Health. 2002 Sept, 628-37. Available PMID: 12693602
38. Washenya EW, Kogi-Makan W, Muita JW. Maternal nutritional knowledge
and the nutritional status of preschool children in a Nairobi Slum. East Afr
Med J. 1996 Jul; 73(7): 417-8. Available PMID: 8918000.
81

39. Chit TM, Kyi H, Thuwin A. Mother’s beliefs and attitudes towards child
weight, child feeding and related practices in Myanmar. Nutr Health. 2003;
17(3) 231-54. Available PMID 14703156.
40. Das DK, Ahmed S. Knowledge of the Bangladeshi rural mothers regarding
breast feeding and weaning. Indian J Pediatr. 1995 Mar – Apr; 62(2) 213-7.
Available PMID 10829870
41. Pant I, Cholthia K. Maternal knowledge regarding breast feeding and weaning
practices. Indian J Pediatr. 1990 May – Jun; 57(3): 395-400. Available PMID
2228093.
42. Bhat IA, Shah GN, Dhar GM, Mehnaz S. A study on the impact of maternal
knowledge and practices on the nutritional status of infants. Indian J Matern
Child Health. 1992 Jan-Mar; 3(11): 12-5. Available PMID: 12318654.
43. Bekele A, Berthane Y. Weaning in Butajira, South Etiopia: A study on
mother’s knowledge and practices. Ethiop Med J. 1998 Jan; 36(1): 37-45.
Available PMID 10214446.
44. Burns N, Grove S.K. Understanding Nursing Research. 2nd ed. New Delhi:
Saunders; 2002 p185.
45. Treece EW, Treece JW. Element of Research in Nursing. St. Louis: Mosby;
1977 p349.
46. Polit FT, Beck JC. Nursing Research. Principles and Methods. 2nd ed.
Philadelphia: Lippincott Williams and Williams; 2004 p716.
82
10. LIST OF ANNEXURE
Sl.No. Annexure Page No
A Letter seeking permission to conduct pilot study 84
B Letter granting permission to conduct pilot study 85
C Letter seeking permission to conduct main study 86
D Letter granting permission to conduct main study 87
E Letter seeking expert opinion on content validity of the tool 88 – 89
F Criteria checklist for validating the tool 90 – 91
G Certificate of content validity 92
H Blue Print 93
I Tool used for the study (English) 94 – 98
J Tool used for the study (Kannada) 99 – 103
K Scoring Key 104
L Letter seeking consent of the participant (English) 105
M Letter seeking consent of the participant (Kannada) 106
N Certificate of analysis of data 107
O Certificate of Editing 108
P List of experts 109 - 110
83

ANNEXURE – A
LETTER SEEKING PERMISSION TO CONDUCT THE PILOT STUDY
From,
Rosamma K.J, II Year M.Sc. Nursing, Sarvodaya College of Nursing Bangalore
To,
The Medical Officer Primary Health Centre K. Gollahalli Bangalore South
Through,
The Principal Sarvodaya College of Nursing Bangalore
Respected sir,
Sub.: Seeking permission to conduct pilot study
I, Rosamma K.J am a bonafide PG Student of Sarvodaya College of Nursing
affiliated to Rajiv Gandhi University of Health Sciences, Bangalore with a
specialization in Pediatric Nursing.
I have to conduct a pilot study as a part of my main research for the purpose of
partial fulfillment of my course. My problem statement is “A Study To Correlate
Feeding Practices Of Mothers And Nutritional Status Of Their Children In A
Selected Area Bangalore”.
In this regard, I kindly request you to grant me permission for conducting pilot
study.
Thanking you,
Date: Yours faithfully,
Place: ROSAMMA K.J
84
ANNEXURE – B
LETTER GRANTING PERMISSION TO CONDUCT THE PILOT STUDY
From,
The Medical Officer,
Primary Health Centre,
K. Gollahalli,
Bangalore South.
To,
Rosamma K.J,
2nd Year M.Sc. Nursing,
Sarvodaya College of Nursing,
Bangalore.
Dear Student,
As per your request forward through the Principal, Sarvodaya College of
Nursing you are permitted to do the pilot study in K. Gollahalli, Bangalore as
mentioned in your letter.
Date:
Place :
85

ANNEXURE – C
LETTER SEEKING PERMISSION FOR CONDUCTING THE MAIN STUDY
From,
Rosamma K.J. 2nd Year M.Sc. Nursing, Sarvodaya College of Nursing Bangalore
To,
The Medical Officer of Health, PHC K. Gollahalli, Bangalore South, Bangalore
Through, The Principal Sarvodaya College of Nursing Bangalore
Sub: Seeking permission to conduct main study
Respected sir,
I, Rosamma K.J is a bonafide PG Student of Sarvodaya College of Nursing
affiliated to Rajiv Gandhi University of Health Sciences, Bangalore with a
specialization in Pediatric Nursing.
I have to conduct a main study as a part of my main research for the purpose
of partial fulfillment of my course. My problem statement is “A Study To Correlate
Feeding Practices Of Mothers And Nutritional Status Of Their Children In A
Selected Area, Bangalore”.
In this regard, I kindly request you to grant me permission for conducting
main study.
Thanking you,
Date: Yours faithfully,
Place: ROSAMMA K.J
86
ANNEXURE – D
LETTER GRANTING PERMISSION TO CONDUCT THE MAIN STUDY
From,
The Medical Officer of Health,
PHC K. Gollahalli,
Bangalore South,
Bangalore.
To,
Rosamma K.J,
2nd Year M.Sc. Nursing,
Sarvodaya College of Nursing
Bangalore
Dear Student,
As per your request forward through the principal Sarvodaya College of
Nursing you are permitted to do the main study in K. Gollahalli PHC in Bangalore as
mentioned in your letter.
Date:
Place:
87
ANNEXURE – E
LETTER SEEKING EXPERTS OPINION AND SUGGESTIONS FOR THE
CONTENT VALIDITY OF THE TOOL.
From,
Rosamma K.J,
II Year M.Sc. Nursing,
Sarvodaya College of Nursing,
Bangalore.
To,
Through,
The Principal,
Sarvodaya College of Nursing,
Bangalore.
Dear Madam / Sir,
Sub.: Request for opinion and suggestions of experts for establishing
content validity of research tool.
I, Rosamma K.J II Year Student of Master of Science in Nursing
(Pediatric Nursing), student of Sarvodaya College of Nursing, Bangalore, have
selected the following topic for my research project, to be submitted to Rajiv Gandhi
University of Health Sciences, Karnataka, Bangalore, in partial fulfillment university
requirement for the award of Master of Nursing degree.
TITLE OF THE TOPIC
“A Study To Correlate Feeding Practices Of Mothers And Nutritional
Status Of Their Children In A Selected Area Bangalore”.
88
The objectives of the study are
1. To assess feeding practices of mothers.
2. To assess the nutritional status of children.
3. To find out the correlation between the feeding practices of mothers and the
nutritional status of their children.
4. To find out the association between feeding practices of mothers and the
selected demographic variables.
With regard to this may I request you to validate my tool (Structured Interview
Schedule) for its appropriateness and relevancy. I would be highly obliged and remain
thankful for your great help if you could validate the tool and give your valuable
opinion and suggestions wherever required.
Herewith I am enclosing a copy of
a) Questionnaire
b) Correct response and scoring key
c) Evaluation criteria
d) Content validity certificate
Thanking you,
Date: Yours faithfully,
Place: Bangalore ROSAMMA K.J.
89

ANNEXURE – F
Evaluation Criteria for validation of tool
Instruction
A tool has been constructed for data collection. It consist of four parts.
Section : I Deals with demographic data.
Section : II Deals with practices of mothers regarding breast feeding, weaning and
family diet.
Section : III Deals with Anthropometry
Areas Item No.
Relevant Relevant to
Certain Extent
Not Relevant
Suggestions
1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13.
Section I Demographic data
14. 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12.
Section II Checklist
13.
90

Areas Item No.
Relevant Relevant to
Certain Extent
Not Relevant
Suggestions
14. 15. 16. 17. 18. 19. 20.
21. 22. 23. 24. 25. 26. 27. 28. 29. 30.
91
ANNEXURE – G
CERTIFICATE OF CONTENT VALIDITY
This is to certify that the tool developed by Rosamma K.J., M.Sc. Nursing
Student of Sarvodaya College of Nursing, Bangalore (Affiliated to Rajiv Gandhi
University of Health Sciences), has been validated by the undersigned and can
proceed with this tool and conduct the main study for dissertation entitled “A Study
To Correlate Feeding Practices Of Mothers And Nutritional Status Of Their
Children In A Selected Area, Bangalore”.
Signature :
Name :
Designation :
Date :
Seal :
92
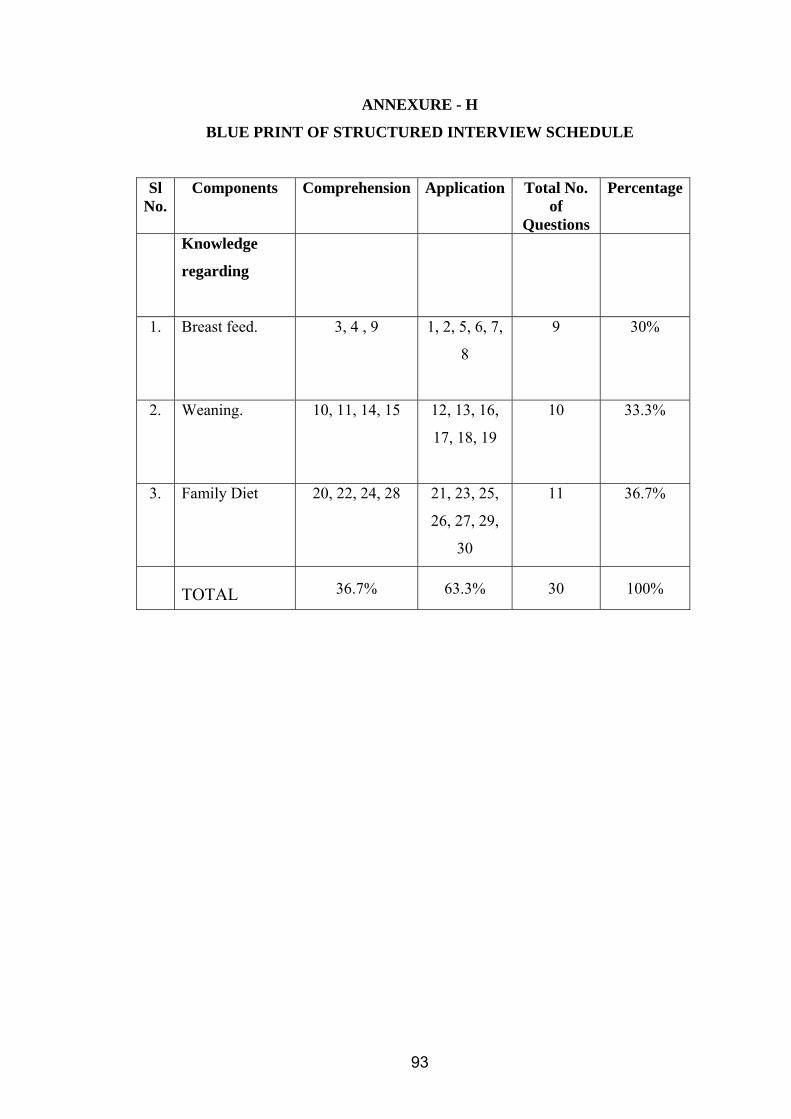
ANNEXURE - H
BLUE PRINT OF STRUCTURED INTERVIEW SCHEDULE
Sl No.
Components Comprehension Application Total No. of
Questions
Percentage
Knowledge
regarding
1. Breast feed.
3, 4 , 9 1, 2, 5, 6, 7,
8
9 30%
2. Weaning.
10, 11, 14, 15 12, 13, 16,
17, 18, 19
10 33.3%
3. Family Diet
20, 22, 24, 28 21, 23, 25,
26, 27, 29,
30
11 36.7%
TOTAL 36.7% 63.3% 30 100%
93
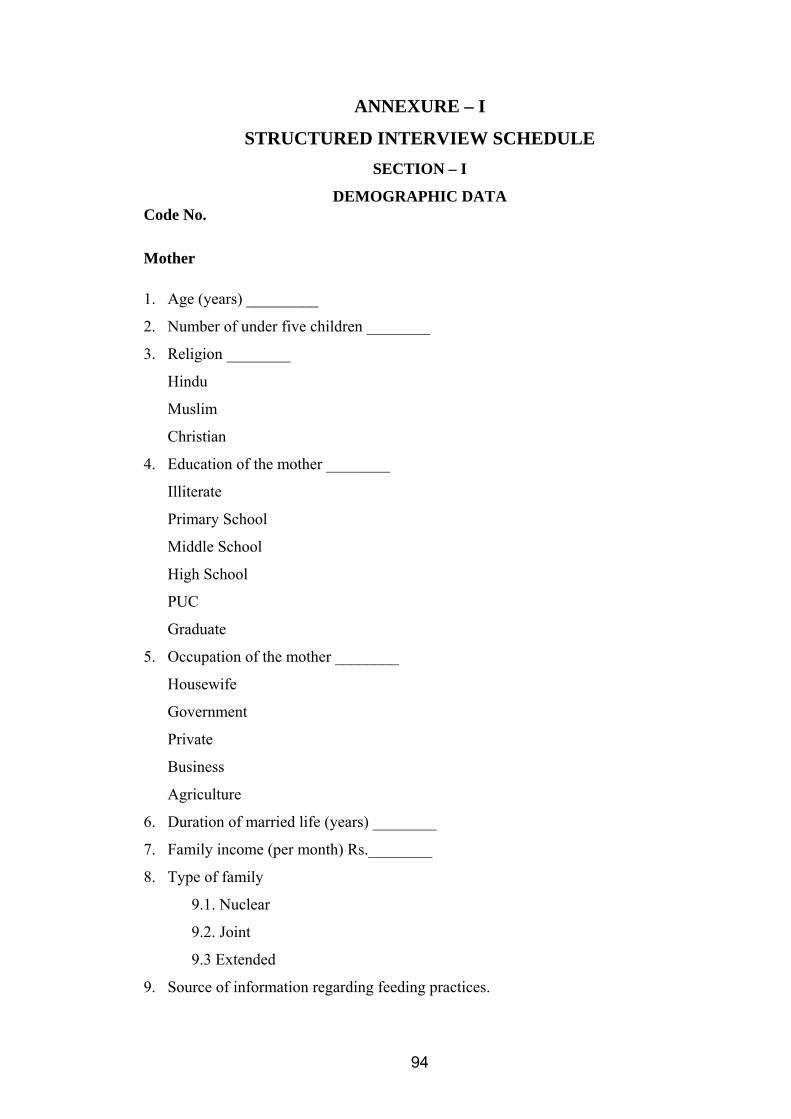
ANNEXURE – I
STRUCTURED INTERVIEW SCHEDULE SECTION – I
DEMOGRAPHIC DATA Code No.
Mother 1. Age (years) _________
2. Number of under five children ________
3. Religion ________
Hindu
Muslim
Christian
4. Education of the mother ________
Illiterate
Primary School
Middle School
High School
PUC
Graduate
5. Occupation of the mother ________
Housewife
Government
Private
Business
Agriculture
6. Duration of married life (years) ________
7. Family income (per month) Rs.________
8. Type of family
9.1. Nuclear
9.2. Joint
9.3 Extended
9. Source of information regarding feeding practices.
94
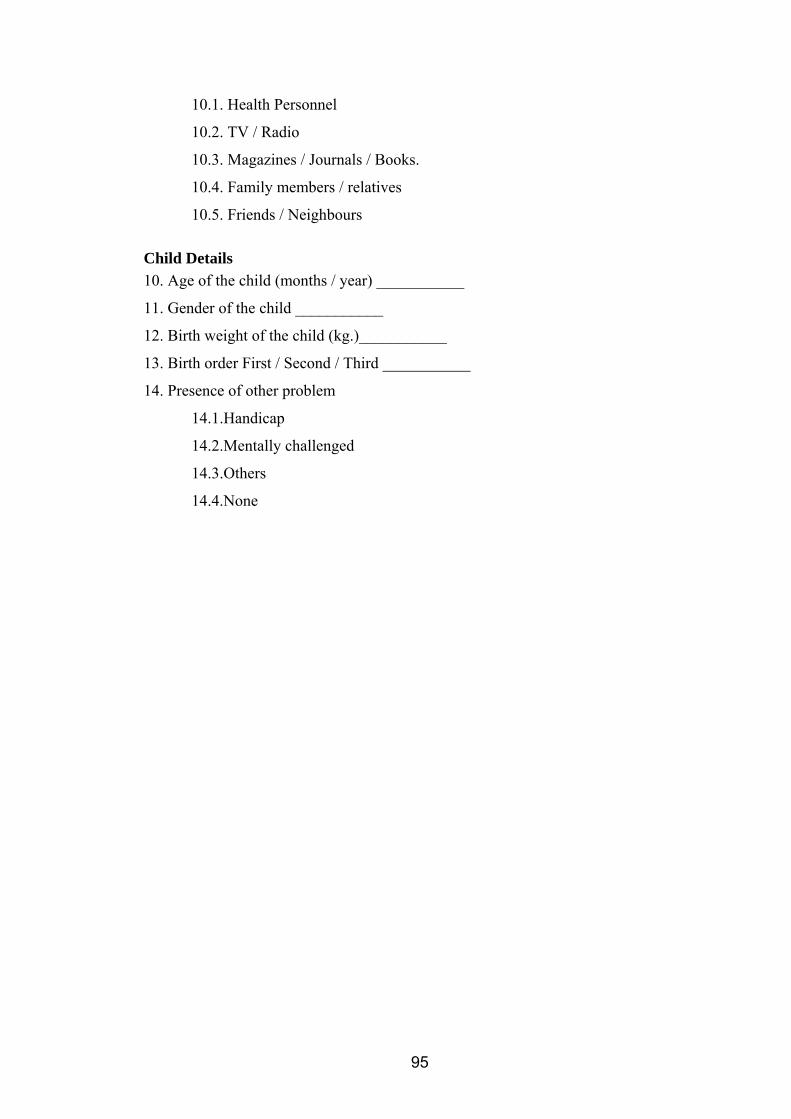
10.1. Health Personnel
10.2. TV / Radio
10.3. Magazines / Journals / Books.
10.4. Family members / relatives
10.5. Friends / Neighbours
Child Details 10. Age of the child (months / year) ___________
11. Gender of the child ___________
12. Birth weight of the child (kg.)___________
13. Birth order First / Second / Third ___________
14. Presence of other problem
14.1.Handicap
14.2.Mentally challenged
14.3.Others
14.4.None
95
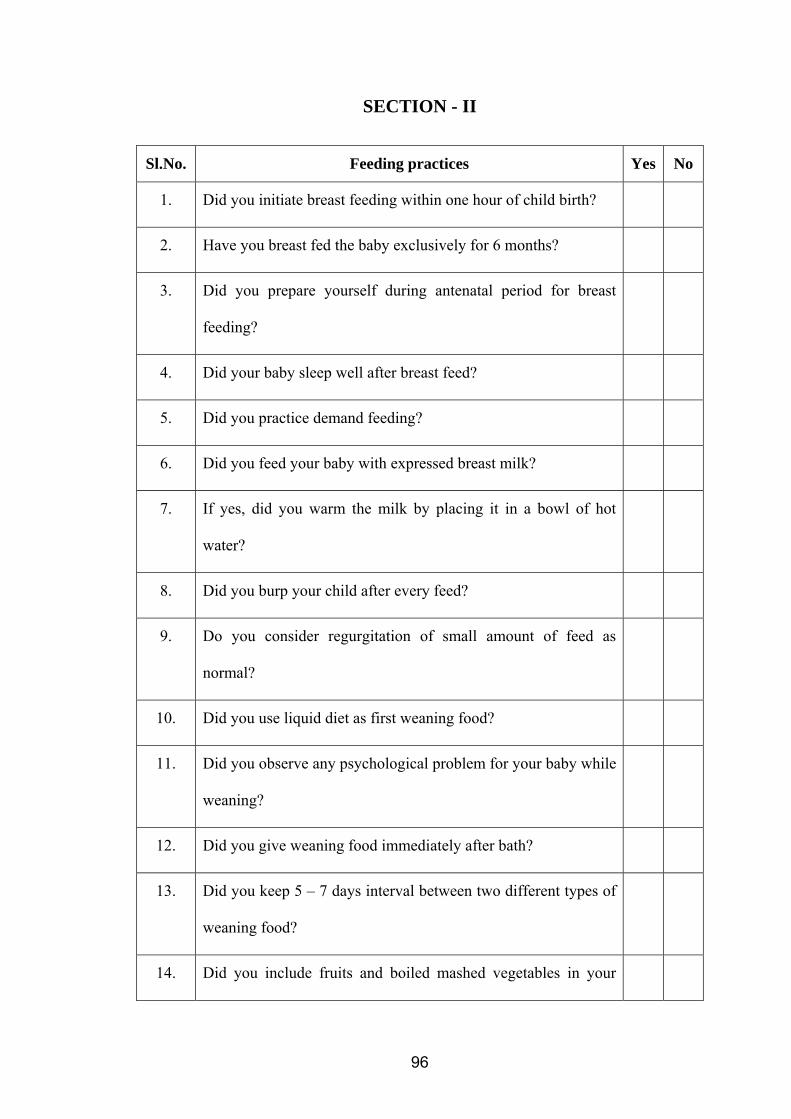
SECTION - II
Sl.No. Feeding practices Yes No
1. Did you initiate breast feeding within one hour of child birth?
2. Have you breast fed the baby exclusively for 6 months?
3. Did you prepare yourself during antenatal period for breast
feeding?
4. Did your baby sleep well after breast feed?
5. Did you practice demand feeding?
6. Did you feed your baby with expressed breast milk?
7. If yes, did you warm the milk by placing it in a bowl of hot
water?
8. Did you burp your child after every feed?
9. Do you consider regurgitation of small amount of feed as
normal?
10. Did you use liquid diet as first weaning food?
11. Did you observe any psychological problem for your baby while
weaning?
12. Did you give weaning food immediately after bath?
13. Did you keep 5 – 7 days interval between two different types of
weaning food?
14. Did you include fruits and boiled mashed vegetables in your
96
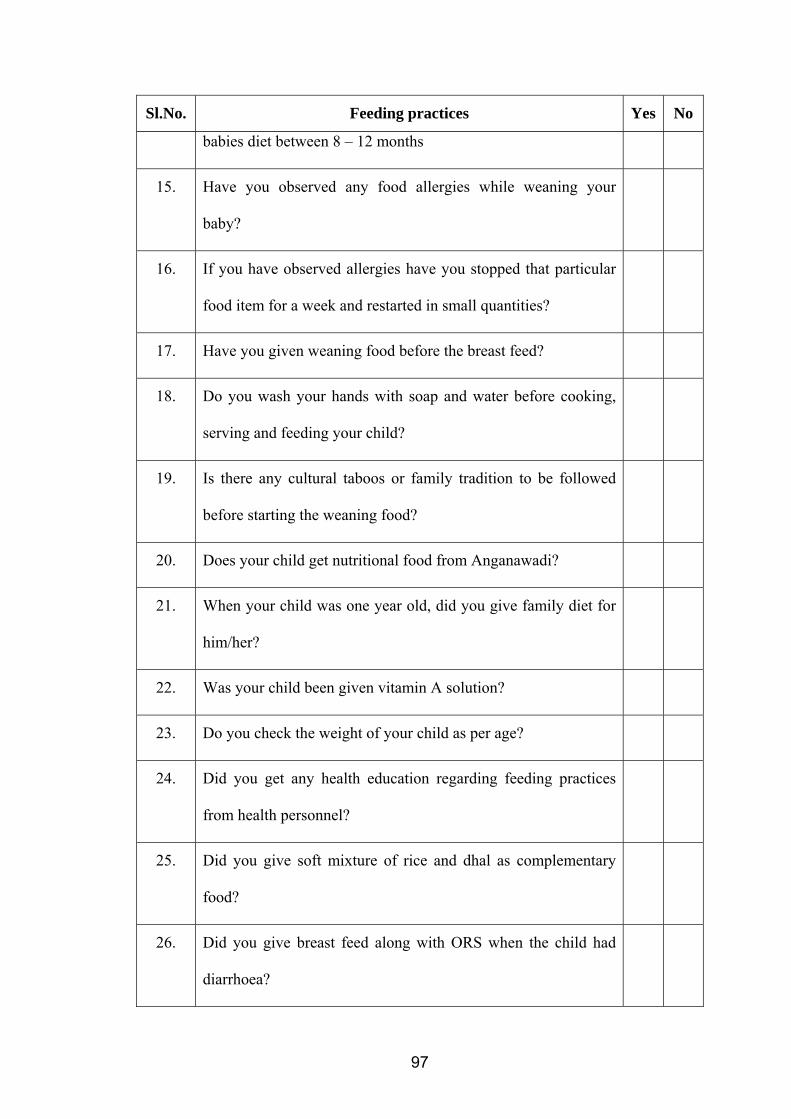
Sl.No. Feeding practices Yes No
babies diet between 8 – 12 months
15. Have you observed any food allergies while weaning your
baby?
16. If you have observed allergies have you stopped that particular
food item for a week and restarted in small quantities?
17. Have you given weaning food before the breast feed?
18. Do you wash your hands with soap and water before cooking,
serving and feeding your child?
19. Is there any cultural taboos or family tradition to be followed
before starting the weaning food?
20. Does your child get nutritional food from Anganawadi?
21. When your child was one year old, did you give family diet for
him/her?
22. Was your child been given vitamin A solution?
23. Do you check the weight of your child as per age?
24. Did you get any health education regarding feeding practices
from health personnel?
25. Did you give soft mixture of rice and dhal as complementary
food?
26. Did you give breast feed along with ORS when the child had
diarrhoea?
97
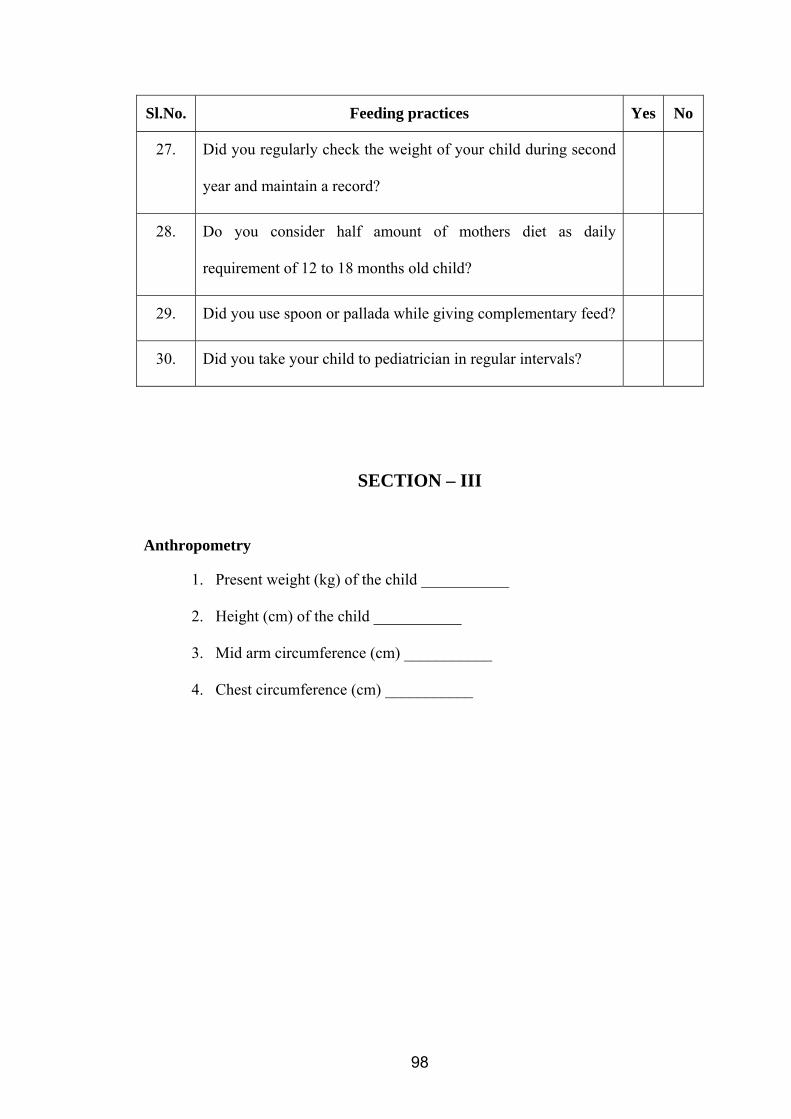
Sl.No. Feeding practices Yes No
27. Did you regularly check the weight of your child during second
year and maintain a record?
28. Do you consider half amount of mothers diet as daily
requirement of 12 to 18 months old child?
29. Did you use spoon or pallada while giving complementary feed?
30. Did you take your child to pediatrician in regular intervals?
SECTION – III
Anthropometry
1. Present weight (kg) of the child ___________
2. Height (cm) of the child ___________
3. Mid arm circumference (cm) ___________
4. Chest circumference (cm) ___________
98
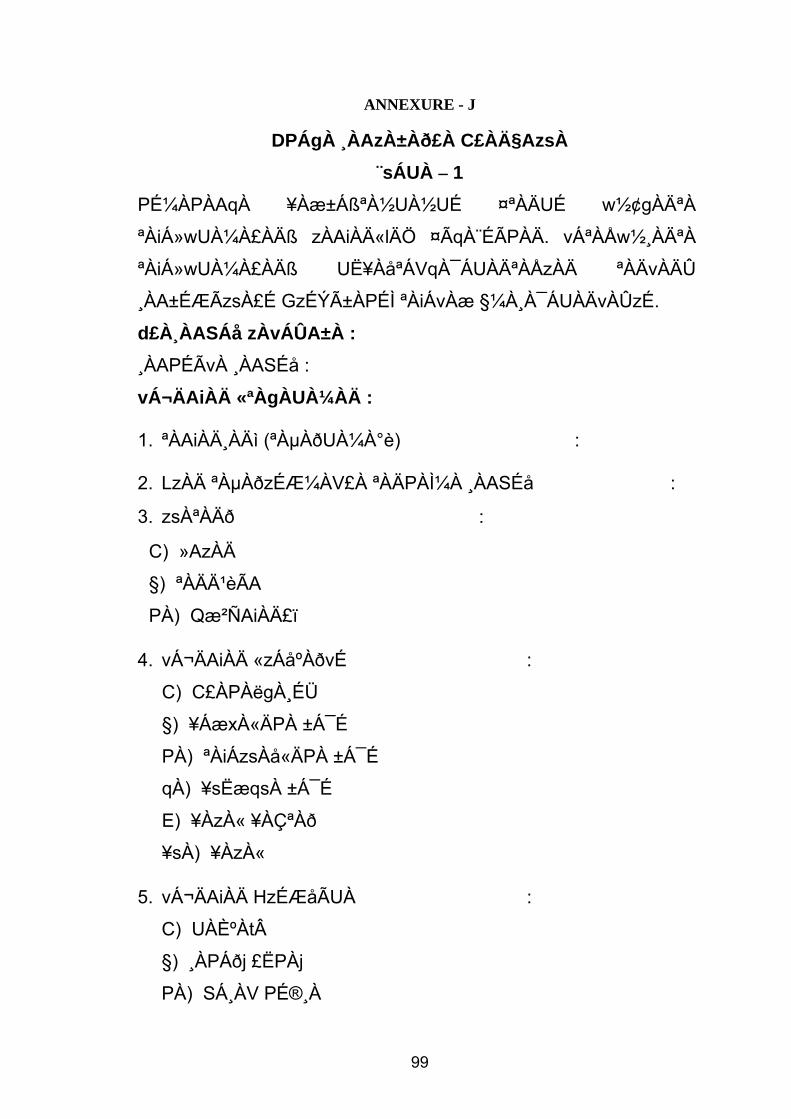
ANNEXURE - J
DPÁgÀ ¸ÀAzÀ±Àð£À C£ÀħAzsÀ
¨sÁUÀ – 1 PɼÀPÀAqÀ ¥Àæ±ÁߪÀ½UÀ½UÉ ¤ªÀÄUÉ w½¢gÀĪÀ
ªÀiÁ»wUÀ¼À£ÀÄß zÀAiÀÄ«lÄÖ ¤ÃqÀ¨ÉÃPÀÄ. vÁªÀÅw½¸ÀĪÀ
ªÀiÁ»wUÀ¼À£ÀÄß UË¥ÀåªÁVqÀ¯ÁUÀĪÀÅzÀÄ ªÀÄvÀÄÛ
¸ÀA±ÉÆÃzsÀ£É GzÉÝñÀPÉÌ ªÀiÁvÀæ §¼À¸À¯ÁUÀÄvÀÛzÉ.
d£À¸ÀASÁå zÀvÁÛA±À : ¸ÀAPÉÃvÀ ¸ÀASÉå :
vÁ¬ÄAiÀÄ «ªÀgÀUÀ¼ÀÄ :
1. ªÀAiÀĸÀÄì (ªÀµÀðUÀ¼À°è) :
2. LzÀÄ ªÀµÀðzÉƼÀV£À ªÀÄPÀ̼À ¸ÀASÉå :
3. zsÀªÀÄð :
C) »AzÀÄ
§) ªÀÄĹèÃA
PÀ) Qæ²ÑAiÀÄ£ï
4. vÁ¬ÄAiÀÄ «zÁåºÀðvÉ :
C) C£ÀPÀëgÀ¸ÉÜ
§) ¥ÁæxÀ«ÄPÀ ±Á¯É
PÀ) ªÀiÁzsÀå«ÄPÀ ±Á¯É
qÀ) ¥sËæqsÀ ±Á¯É
E) ¥ÀzÀ« ¥ÀǪÀð
¥sÀ) ¥ÀzÀ«
5. vÁ¬ÄAiÀÄ HzÉÆåÃUÀ :
C) UÀȺÀtÂ
§) ¸ÀPÁðj £ËPÀj
PÀ) SÁ¸ÀV PÉ®¸À
99

qÀ) ªÁå¥ÀgÀ
E) ªÀåªÀ¸ÁAiÀÄ
6. ªÉʪÁ»PÀ fêÀ£À (ªÀµÀðUÀ¼À°è) :
7. PÀÄlÄA§zÀ ªÀgÀªÀÄ£À (wAUÀ½UÉ gÀÆ.UÀ¼À°è) :
8. PÀÄlÄA§zÀ «zsÀ :
C) «¨sÀPÀÛ PÀÄvÀÄA§
§) C«¨sÀPÀÛ PÀÄlÄA§
PÀ) «¸ÀÛgÀuÁ PÀÄlÄA§
9. ºÁ®Æt¸ÀĪÀ C¨sÁå¸ÀzÀ §UÉÎ ¥ÀqÉ¢gÀĪÀ ªÀiÁ»wUÀ¼À
ªÀÄÆ® :
C) DgÉÆÃUÀå ¹§âA¢
§) zÀÆgÀzÀ±Àð£À / DPÁ±ÀªÁtÂ
PÀ) ¥ÀĸÀÛPÀ / ¤AiÀÄvÀPÁ°PÉUÀ¼ÀÄ / ¸ÀªÀiÁZÁgÀ
¥ÀwæPÉUÀ¼ÀÄ
qÀ) PÀÄlÄA§zÀªÀgÀÄ / §AzsÀÄUÀ¼ÀÄ
E) UɼÉAiÀÄgÀÄ / CPÀÌ¥ÀPÀÌzÀªÀgÀÄ
ªÀÄUÀÄ«£À «ªÀgÀUÀ¼ÀÄ : 10. ªÀÄUÀÄ«£À ªÀAiÀĸÀÄì
:
11. ªÀÄUÀÄ«£À °AUÀ :
12. ºÀÄnÖzÁUÀ ªÀÄUÀÄ«£À vÀÆPÀ (Q.UÁæA) :
13. ºÀÄnÖ£À PÀæªÀÄUÀ¼ÀÄ ªÉÆzÀ®£É / JgÀqÀ£Éà / ªÀÄÆgÀ£Éà :
14. EvÀgÉ vÉÆAzÀgÉUÀ¼ÀÄ
:
C) CAUÀ«PÀ®
§) ªÀiÁ£À¹PÀ C¸Àé¸ÀÜvÉ
100

PÀ) EvÀgÉ
R) AiÀiÁªÀÅzÀÆ E®è
¨sÁUÀ – 2
PÀæ. ¸ÀA.
ºËzÀÄ E®è
1. ªÀÄUÀÄ ºÀÄnÖzÀ MAzÀÄ
UÀAmÉAiÉƼÀUÉ ¤ÃªÀÅ JzÉ
ºÁ®£ÀÄß PÀÄr¹gÀÄ«gÁ?
2. DgÀÄ wAUÀ¼ÀªÀgÉUÉ ªÀÄUÀÄ«UÉ §jÃ
JzÉ ºÁ®£ÀÄß ªÀiÁvÀæ PÀÄr¹gÀÄ«gÁ?
3. ¥Àæ¸ÀªÀ ¥ÀǪÀðzÀ°èAiÉÄ ¤ÃªÀÅ JzÉ
ºÁ®£ÀÄß ªÀÄUÀÄ«UÉ PÀÄr¸À®Ä
vÀAiÀiÁj £Àqɹ¢ÝÃgÀ?
4. JzÉ ºÁ®Ä PÀÄr¹zÀ £ÀAvÀgÀ ªÀÄUÀÄ
ZÉ£ÁßV ¤zÉæ ªÀiÁqÀÄvÀÛzÉAiÉÄÃ?
5. DºÁgÀ ¸ÉêÀ£É ªÀÄUÀÄ«£À ºÀPÀÄÌ
JA§AvÉ C¨sÁå¸À ªÀiÁr¢ÝÃgÁ?
6. JzɬÄAzÀ »ArvÉUÉzÀ ºÁ®£ÀÄß
ªÀÄUÀÄ«UÉ PÀÄr¹¢ÝÃgÁ?
7. ºËzÁzÀgÉ, ºÁ®£ÀÄß ©¹¤Ãj£À°èlÄÖ
¨ÉZÀÑUÉ ªÀiÁr ¤Ãr¢ÝÃgÁ?
8. ºÁ®Ä PÀÄr¹zÀ £ÀAvÀgÀ
ªÀÄUÀĪÀ£ÀÄß vÉÃUÀĪÀAvÉ
ªÀiÁr¢ÝÃgÁ?
9. QrzÀ ºÁ®Ä ¸Àé®à ¥ÀæªÀiÁtzÀ°è
ºÉÆgÀ§gÀÄvÀÛzÉ. EzÀ£ÀÄß
¸ÁªÀiÁ£ÀåªÉAzÀÄ ¥ÀjUÀt¹¢ÝÃgÁ?
10. zÀæªÀ ¥ÀzÁxÀðªÀ£ÀÄß ªÉÆzÀ®
101

¥ÀÆgÀPÀ DºÁgÀªÉAzÀÄ
¥ÀjUÀt¹¢ÝÃgÁ?
11. ¥ÀÇgÀPÀ DºÁgÀªÀ£ÀÄß
¥ÁægÀA©ü¹zÁUÀ ªÀÄUÀÄ«£À
ªÀiÁ£À¹PÀ ¹ÜwUÀwAiÀÄ£ÀÄß
UÀªÀĤ¹¢ÝÃgÁ?
12. ¸ÁߣÀ ªÀiÁrzÀ vÀPÀët ¥ÀÇgÀPÀ
DºÁgÀªÀ£ÀÄß ¤ÃqÀÄwÛÃgÁ?
13. JgÀqÀÄ «zsÀzÀ ¥ÀÇgÀPÀ
DºÁgÀªÀ£ÀÄß ¤ÃqÀĪÁUÀ £ÀqÀÄªÉ 5–
7 ¢£ÀUÀ¼À CAvÀgÀzÀ°è
ªÀiÁqÀÄwÛÃgÁ?
14. 8 – 12 wAUÀ¼À°è ªÀÄUÀÄ«UÉ ¤ÃqÀĪÀ DºÁgÀzÀ°è ºÀtÄÚUÀ¼ÀÄ, §qsÀ¬Ä¹zÀ ªÀÄvÀÄÛ ZÉ£ÁßV QªÀÅazÀ vÀgÀPÁjUÀ¼À£ÀÄß ¤ÃqÀÄ«gÁ?
15. ¥ÀÇgÀPÀ DºÁgÀ ¤ÃqÀĪÀ
¸ÀªÀÄAiÀÄzÀ°è DºÀgÀ¢AzÀ SÁ¬Ä¯É
§j¸À§ºÀÄzÁzÀ AiÀiÁªÀÅzÀPÀÆÌ
¸ÀÆPÀëöä ¸ÀAªÉâAiÀiÁVgÀĪÀ
¥ÀgÀ¸ÀÜwAiÀÄ£ÀÄß JzÀÄj¹¢ÃgÀ?
16. ºÁUÁVzÀÝ°è CAvÀºÀ DºÁgÀªÀ£ÀÄß
MAzÀÄ ªÁgÀ ¤°è¹ £ÀAvÀgÀ C®à
¥ÀæªÀiÁtzÀ°è ¥ÀÅ£ÀB ¤ÃqÀÄ«gÁ?
17. JzÉ ºÁ®£ÀÄß ¤ÃqÀĪÀ ªÀÄÄ£Àß
¥ÀÇgÀPÀ DºÁgÀªÀ£ÀÄß ¤ÃqÀÄ«gÁ?
18. CqÀÄUÉ ªÀiÁqÀĪÀ ªÀÄÄ£Àß §r¸ÀĪÀ
ªÀÄvÀÄÛ G¤¸ÀĪÀ ªÀÄÄ£Àß ¤ªÀÄä
PÉÊUÀ¼À£ÀÄß ¸Á§Æ£ÀÄ ªÀÄvÀÄÛ
102
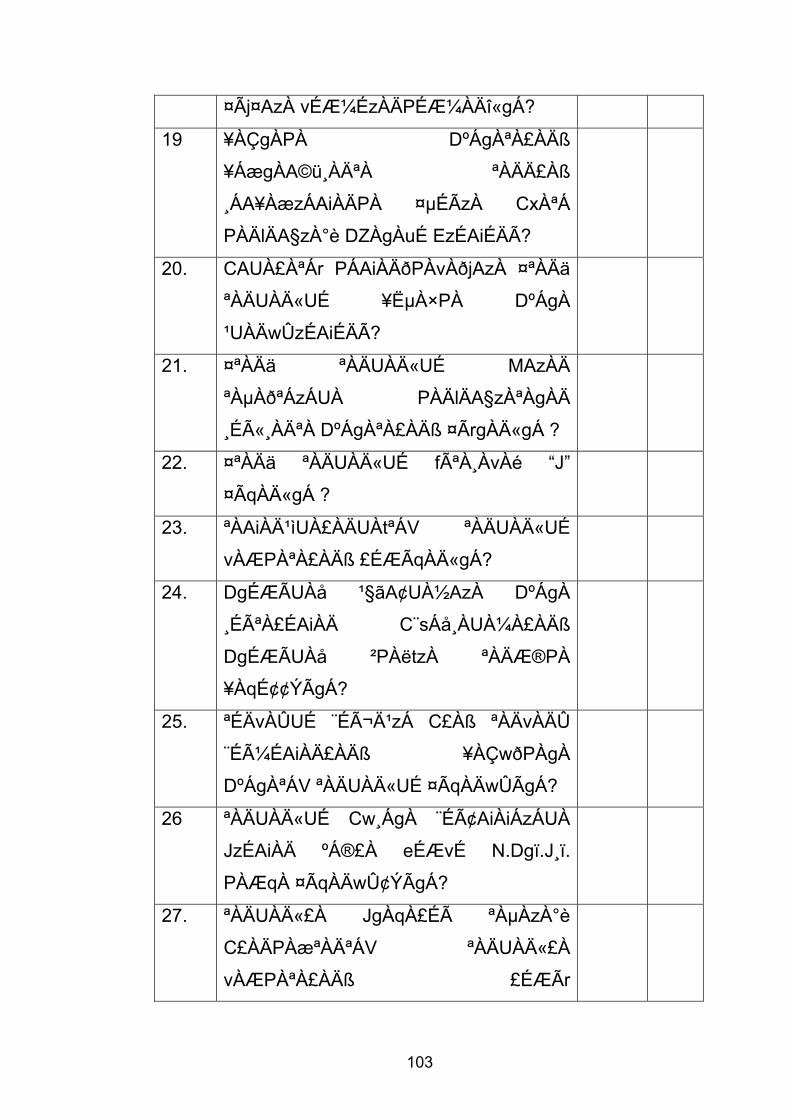
¤Ãj¤AzÀ vÉƼÉzÀÄPÉƼÀÄî«gÁ?
19 ¥ÀÇgÀPÀ DºÁgÀªÀ£ÀÄß
¥ÁægÀA©ü¸ÀĪÀ ªÀÄÄ£Àß
¸ÁA¥ÀæzÁAiÀÄPÀ ¤µÉÃzÀ CxÀªÁ
PÀÄlÄA§zÀ°è DZÀgÀuÉ EzÉAiÉÄÃ?
20. CAUÀ£ÀªÁr PÁAiÀÄðPÀvÀðjAzÀ ¤ªÀÄä
ªÀÄUÀÄ«UÉ ¥ËµÀ×PÀ DºÁgÀ
¹UÀÄwÛzÉAiÉÄÃ?
21. ¤ªÀÄä ªÀÄUÀÄ«UÉ MAzÀÄ
ªÀµÀðªÁzÁUÀ PÀÄlÄA§zÀªÀgÀÄ
¸Éë¸ÀĪÀ DºÁgÀªÀ£ÀÄß ¤ÃrgÀÄ«gÁ ?
22. ¤ªÀÄä ªÀÄUÀÄ«UÉ fêÀ¸ÀvÀé “J”
¤ÃqÀÄ«gÁ ?
23. ªÀAiÀĹìUÀ£ÀÄUÀtªÁV ªÀÄUÀÄ«UÉ
vÀÆPÀªÀ£ÀÄß £ÉÆÃqÀÄ«gÁ?
24. DgÉÆÃUÀå ¹§ãA¢UÀ½AzÀ DºÁgÀ
¸ÉêÀ£ÉAiÀÄ C¨sÁå¸ÀUÀ¼À£ÀÄß
DgÉÆÃUÀå ²PÀëtzÀ ªÀÄÆ®PÀ
¥ÀqÉ¢¢ÝÃgÁ?
25. ªÉÄvÀÛUÉ ¨ÉìĹzÁ C£Àß ªÀÄvÀÄÛ
¨ÉüÉAiÀÄ£ÀÄß ¥ÀÇwðPÀgÀ
DºÁgÀªÁV ªÀÄUÀÄ«UÉ ¤ÃqÀÄwÛÃgÁ?
26 ªÀÄUÀÄ«UÉ Cw¸ÁgÀ ¨ÉâAiÀiÁzÁUÀ
JzÉAiÀÄ ºÁ®£À eÉÆvÉ N.Dgï.J¸ï.
PÀÆqÀ ¤ÃqÀÄwÛ¢ÝÃgÁ?
27. ªÀÄUÀÄ«£À JgÀqÀ£Éà ªÀµÀzÀ°è
C£ÀÄPÀæªÀĪÁV ªÀÄUÀÄ«£À
vÀÆPÀªÀ£ÀÄß £ÉÆÃr
103
zÁR°¸ÀÄwÛ¢ÝÃgÁ?
28. vÁ¬ÄAiÀÄÄ ¢£Á®Ä ¸Éë¸ÀĪÀ DºÁgÀ
¥ÀæªÀiÁtzÀ CzsÀðzÀµÀÄÖ 12 – 18
wAUÀ¼À ªÀÄUÀÄ«£À
DºÁgÀªÁVgÀÄvÀÛzÉ JAzÀÄ
£ÀA§ÄwÛÃgÁ?
29. M¼À®qÀ CxÀªÁ ZÀªÀÄZÉAiÀÄ£ÀÄß
¥ÀÇwðPÀgÀ DºÁgÀ ¤ÃqÀĪÁUÀ
G¥ÀAiÉÆÃV¹¢ÝÃgÁ?
30. PÀæªÀħzÀÞªÁV ²±ÀÄvÀdÕjAzÀ
ªÀÄUÀĪÀ£ÀÄß vÀ¥Á¸ÀuÉUÉ
M¼À¥Àr¸ÀÄwÛ¢ÝÃgÁ?
¨sÁUÀ – 3 ªÀÄ£ÀĵÀå£À zÉúÀ ªÀiÁ¥sÀ£ÀPÉÌ ¸ÀA§A¢ü¹zÀ «ªÀgÀUÀ¼ÀÄ :
1. ªÀÄUÀÄ«£À
FV£À vÀÆPÀ
(Q.UÁæA.
UÀ¼À°è)
: ………………………………………………
2. ªÀÄUÀÄ«£À
JvÀÛgÀ (¸ÉA.
«ÄÃlgï UÀ¼À°è)
: ………………………………………………
3. ªÉÄïÁãUÀzÀ
PÉÊAiÀÄ
ªÀÄzsÀåzÀ°è£À
¸ÀÄvÀÛ¼ÀvÉÀ
¥Àj¢ü
(¸ÉA. «ÄÃlgï
: ………………………………………………
104
UÀ¼À°è)
4. JzÉAiÀÄ
¸ÀÄvÀÛ¼ÀvÉ
(¸ÉA. «ÄÃlgï
UÀ¼À°è)
: ………………………………………………
105
ANNEXURE – K
SCORING KEY
Q. No. Correct Option Score
1. Yes 1
2. Yes 1
3. Yes 1
4. Yes 1
5. Yes 1
6. Yes 1
7. Yes 1
8. Yes 1
9. Yes 1
10. Yes 1
11. Yes 1
12. Yes 1
13. Yes 1
14. Yes 1
15. Yes 1
16. Yes 1
17. Yes 1
18. Yes 1
19. Yes 1
20. Yes 1
21. Yes 1
22. Yes 1
23. Yes 1
24. Yes 1
25. Yes 1
26. Yes 1
27. Yes 1
28. Yes 1
29. Yes 1
30. Yes 1
106
ANNEXURE – L
CONSENT FORM FOR THE RESPONDENTS
Dear Participant,
I, Rosamma K.J., 2nd year Nursing student of Sarvodaya College of Nursing
as part of the partial fulfilment of the course, have to conduct a study and the problem
selected is “A Study To Correlate Feeding Practices Of Mothers And Nutritional
Status Of Their Children In A Selected Area, Bangalore”.
I request you to participate in the study and respond to the questions asked.
The information provided by you will be strictly confidential and will be used
only for the study purpose. This is for your information and kind participation.
Thanking you,
Yours sincerely
Signature of the investigator
(Rosamma K.J)
I am willing to participate in the study and aware that the information provided by me
will be kept confidential and used for the study purpose.
Place: Bangalore
Date: Signature of the Participant
107
ANNEXURE – M
GvÀÛgÀ PÉüÀĪÀªÀgÀ ¸ÀªÀÄäw £ÀªÀÄÆ£É
F PÁAiÀÄðPÀæªÀÄzÀ°è ¨sÁUÀªÀ»¸ÀĪÀªÀgÉÃ,
¸ÀªÉÇÃðzÀAiÀÄ PÁ¯ÉÃeï D¥sï £À¹ðAUï£À JA. J¸ï. ¹.
¢éwÃAiÀÄ ªÀµÀðzÀ «zÁåy𤠹¸ÀÖgï. gÉÆøÀªÀÄä eÉÆøÀ¥sï
DzÀ £Á£ÀÄ vÀªÀÄä°è «£ÀAw¹PÉƼÀÄîªÀÅzÉãÉAzÀgÉ £À£Àß
CzsÀåAiÀÄ£ÀzÀ CAUÀªÁV ¤ªÀÄä°è PÉ®ªÀÅ ªÀiÁ»wUÀ¼À£ÀÄß
¸ÀAUÀ滸À®Ä EaÒ¸ÀÄvÉÛãÉ. £À£Àß CzsÀåAiÀÄ£ÀzÀ
«µÀAiÀĪÉãÉAzÀgÉ ‘¨ÉAUÀ¼ÀÆj£À ¤UÀ¢vÀ ¥ÀæzÉñÀzÀ°è
vÁAiÀÄA¢gÀÄ vÀªÀÄä ªÀÄPÀ̽UÉ ºÁ®Ær¸ÀĪÀ PÀæªÀÄ
ªÀÄvÀÄÛ ªÀÄPÀ̼À ¥ËµÀ×PÁA±ÀzÀ ¨É¼ÀªÀtÂUÉUÉ EgÀĪÀ
¸ÀA¨sÀAzsÀ’ ªÀ£ÀÄß PÀÄjvÀÄ.
DzÀÝjAzÀ vÁªÀÅ zÀAiÀÄ«lÄÖ £Á£ÀÄ PÀ¼ÀĪÀ
¥Àæ±ÉßUÀ½UÉ GvÀÛj¸À¨ÉÃPÉAzÀÄ ºÁH F
PÁAiÀÄðPÀæªÀÄzÀ°è ¸ÀQæAiÀĪÁV ¥Á¯ÉÆμÀî¨ÉÃPÉAzÀÄ
«£ÀAw¸ÀÄvÉÛãÉ. ¤ÃªÀÅ MzÀV¸ÀĪÀ ªÀiÁ»wAiÀÄÄ PÉêÀ®
«zÁå¨sÁå¸ÀzÀ zÀȵÀ׬ÄAzÀ ªÀiÁvÀæ §¼À¸À®UÀĪÀÅzÀÄ
ºÁUÀÆ CzÀ£ÀÄß UÉÆÃ¥ÀåªÁV EqÀ¯ÁUÀĪÀÅzÀÄ.
ªÀAzÀ£ÉUÀ¼ÉÆA¢UÉ, vÀªÀÄä «±Áé¹,
«ZÁj¸ÀĪÀªÀgÀ ¸À»
108
£Á£ÀÄ MzÀV¸ÀĪÀ F ªÀiÁ»wAiÀÄÄ CzsÀåAiÀÄ£ÀPÁÌV
§¼À¸À¯ÁUÀÄvÀÛzÉ ºÀUÀÆ CzÀ£ÀÄß UÉÆÃ¥ÀåªÁV
EqÀ¯ÁUÀÄvÀÛzÉ JA§ÄzÀ£ÀÄß w½zÀÄ £Á£ÀÄ F
PÁAiÀÄðPÀæªÀÄzÀ°è ¸ÀQæAiÀĪÁV ¨sÁUÀªÀ»¸À®Ä
EaÒ¸ÀÄvÉÛãÉ.
¸ÀܼÀ : ¨ÉAUÀ¼ÀÆgÀÄ ¢£ÁAPÀ : ¨sÁUÀªÀ»¸ÀĪÀªÀgÀ ¸À»
109
ANNEXURE – N
CERTIFICATE OF ANALYSIS OF DATA
This is to certify that data analysis done by Rosamma K.J., Second Year
M.Sc. Nursing, Sarvodaya College of Nursing, Bangalore, in her study titled “A
Study To Correlate Feeding Practices Of Mothers And Nutritional Status Of
Their Children In A Selected Area, Bangalore” has been verified by me.
Date : Signature
Place : Bangalore Seal
110
ANNEXURE – O
CERTIFICATE OF EDITING
This is to certify that data analysis done by Rosamma K.J., Second Year
M.Sc. Nursing, Sarvodaya College of Nursing, Bangalore, in her study titled “A
Study To Correlate Feeding Practices Of Mothers And Nutritional Status Of
Their Children In A Selected Area, Bangalore” has been edited by me.
Date : Signature of the Editor
Place : Bangalore Mrs. Nirmala Sridhar,
M.A English, M.A Psychology,
PG Diploma in Guidance &
Counselling
111
ANNEXURE - P
LIST OF EXPERTS
1. Dr. G. Kasthuri, Ph.D Prof. and HOD, Dept. of Pediatric Nursing Oxford College of Nursing Bangalore
2. Mrs. Hemalatha Ravi, M.Sc. (N)
Prof. and HOD, Dept. of Pediatric Nursing Maruthi College of Nursing Bangalore
3. Mrs. J. Lovera Grace Lilly Rani, M.Sc. (N)
Prof. and HOD, Dept. of Pediatric Nursing Sarvodaya College of Nursing Bangalore
4. Mrs. Satya Lawrence, M.Sc. (N)
Asso. Professor, Dept. of Pediatric Nursing Sarvodaya College of Nursing Bangalore
5. Mrs. Renuka N, M.Sc. (N)
Lecturer Dept. of Pediatric Nursing, Govt. of College of Nursing Fort, Bangalore
6. Mr. G.R. Chamnalkar, M.Sc. (N)
Prof. Pediatric Nursing, Dept. of Pediatric Nursing Oriental College of Nursing Bangalore
7. Dr. Jayaprakash Rai, MD
Pediatrician, Sarvodaya Hospital Bangalore
112
8. Dr. H.S. Surendra, Asso. Professor in Bio-Statistics, GKVK Agriculture College, Yellahanka, Bangalore
9. Miss. Jesly, M.Sc.
Dietitian Dept. of Nutrition St. John’s Medical College, Bangalore.
113