Embed Size (px)
Citation preview

today’s Veterinary Practice January/February 201444
Practical Dentistry PEER REVIEWED
An ulcer is a break in the skin or mucous membrane, with loss of surface tissue, disintegration, and necrosis of epithelial tissue. Oral ulceration occurs specifically
on the mucous membrane of the oral cavity; bacteria popu-late the exposed area, leading to inflammation and pain.
Several ulcerative diseases are seen in dogs and cats; this article will review the most common ones, including etiol-ogy, presentation, diagnosis, and treatment/management.
FELINE CAUDAL STOMATITISFeline caudal stomatitis (FCS)—a clinical diagnosis of inflammation and proliferation of the gingiva and oral mucosa—is a very frustrating and poorly understood dis-ease in cats.1 Specifically, inflammation associated with the mucosa of the caudal part of the mouth (mucositis)2 is the delineating factor between caudal stomatitis and peri-odontal disease.1,3
EtiologyThe etiology of this disease process is currently unknown.4 Multiple etiologies may exist that, either alone or com-bined, create the inflammation.4 Possible causative agents include an inflammatory response to plaque, viruses (par-ticularly upper respiratory), Bartonella henselae infec-tion, or altered immune status (feline immunodeficiency or leukemia viruses, FIV or FeLV).1,5-8 However, it appears to be an excessive, inflammatory immune response to a heretofore unknown agent.4,9
Clinical Features History. Owners often report a history of halitosis, dys-phagia, pawing at the mouth, anorexia, crying out in pain when eating or yawning, weight loss, unkempt appear-ance, and drooling.3,9-11
Oral Examination. Upon examination:• Affected gingiva and oral mucosa have varying amounts of
inflammation, proliferation, and ulceration (Figure 1).12 • The mucosa is typically bright red, with friable tissues
that bleed easily.9 • Inflammation is typically, but not always, bilaterally
symmetrical.12 The clinical sign that differentiates caudal stomati-
tis from periodontal disease is the presence of caudal inflammation (distal to the teeth) in cases of caudal stomatitis (Figure 2).1,3,12 This presentation was previously called faucitis, but is now known as caudal mucositis.12 In
contrast, in cases of typical periodontal disease, inflamma-tion is associated with the gingiva surrounding the teeth, and does not extend distally into the caudal oral mucosa to any significant extent.
DiagnosisCaudal stomatitis is a clinical syndrome, which does not indicate a specific etiology or diagnosis; therefore, diagno-sis is made by visual inspection of the oral cavity.1,12
Additional diagnostic tests to further evaluate the patient include:4,12 • Dental radiographs• Complete blood count and serum biochemical profile• Evaluation of FeLV/FIV status.
If inflammation is asymmetrical or otherwise atypical, or radiographic findings are suspicious for neoplasia, a biopsy should be submitted for histopathology.1,3
FELINE & CANINE ORAL ULCERATIVE DISEASEBrook A. Niemiec, DVM, FAVD, Diplomate AVDCSouthern California Veterinary Dental Specialties, San Diego, California
Figure 1. Significant inflammation of the gingiva and oral mucosa.
1
Figure 2. Severe caudal mucositis.
2

January/February 2014 today’s Veterinary Practice 45
Practical Dentistry |
Feli
ne
an
D c
an
ine
Or
al
Ulc
er
atiV
e D
ise
as
e
Therapeutic OptionsIdeally, the goal of therapy is total eradication of oral inflammation; however, reducing the amount of inflammation is sometimes the best degree of healing that can be achieved.3,9
Even intense efforts at plaque control and medical ther-apy rarely result in an acceptable response—in terms of decreased inflammation.13 Therefore, recommended treat-ment encompasses:11
• Extraction therapy is the preferred treatment for FCS and should be performed as soon as possible.
• Medical therapy should be reserved for those patients in which clients will not allow (or cannot afford) extrac-tion therapy.
• My approach to resistant cases—after retained roots are ruled out—is as follows: » Feline interferon » Cyclosporine » Corticosteroids.
Surgical TherapyBecause inflammation control is the key to improvement of FCS, any tooth involved with inflammation due to any cause (ie, periodontal/endodontic disease, tooth resorp-tion) should be extracted.4 Remaining teeth must receive strict home care and routine professional cleanings to pre-vent further inflammation.11
However, since the majority of patients have widespread inflammation, which makes home care challenging, the most successful long-term treatment for FCS is extrac-tion of all premolars and molars and careful smooth-ing of the alveolar bone.1,12 Extraction of the rostral teeth is indicated when inflammation includes their gingiva.3,13 Therefore, I will typically perform full-mouth extractions when significant oral inflammation is present, while some veterinary dentists prefer to leave the canines and incisors intact, if possible.3,11
The vast majority of cats have an excellent response to this treatment, requiring no additional therapy (Figure 3).3,12,14
• If extraction therapy is not effective, it is usually due to the presence of retained roots (Figure 4).3,12 Postopera-tive dental radiographs must be exposed to document complete extraction of all tooth roots.3,12,13
• Some cats have only partial improvement and require long-term medical management, generally, though, at much lower doses than required for FCS that has not been treated surgically.
• The patients who have the least response to extraction therapy are typically those that have had long-standing, chronic inflammation that has been treated with repeat-ed high doses of glucocorticoids.3,12
It is important to note that, in my experience, the earlier teeth are extracted, the better the outcome.3,11 Therefore, make sure clients understand that delaying extraction therapy often results in a decreased response to this therapy.
Laser TherapyOne recent case report revealed improvement of inflam-mation after surgical laser therapy. However, despite sev-eral laser treatments, resolution occurred only after full-mouth extractions were performed.15 Therefore, laser ther-apy alone did not provide an obvious benefit. In addition, I have treated numerous patients in which laser therapy has been performed, but no response to this therapy is evi-dent. Consequently, this is not currently a recommended initial form of therapy.11
Medical Therapy When owners are reluctant to have multiple extractions performed, medical management may be attempted, but has several disadvantages: • Many products used are oral medications, which require
daily to twice daily administration. • Medical therapy is almost invariably a life-long process,
and many products have significant side effects. • No medical protocols have been shown to be completely
effective; they only reduce the clinical signs temporarily.11,13
Figure 4A. Recheck of patient that received “extraction” of the premolars and molars elsewhere. Note the severe inflammation.
4A 4B3
Figure 3. One month recheck of patient after full-mouth extractions for severe caudal stomatitis. Note the complete lack of inflammation.
Figure 4B. Dental radiograph of patient in 4A revealing the retained roots.

| Practical Dentistry
today’s Veterinary Practice January/February 201446
Antibiotics. Systemic antibiotics may decrease some oral inflammation. However, this is generally temporary at best, and most patients will relapse, even during the course of antibiotic therapy.3,13
Corticosteroids. Corticosteroids are, by far, the most commonly used and effective drugs for immune modu-lation, resulting in clinical improvement far more often than antibiotic therapy.3 However, long-term use may have detrimental effects, such as induction of diabetes mellitus and opportunistic infections.13,16 Chronic cor-ticosteroid therapy should only be used as a last resort—if an owner will not allow extractions.4
Immunosuppressive Treatment. Cyclosporine A has been proposed as an immunosuppressive drug for cats with caudal stomatitis,3 and some have promoted it as an alter-native to extractions in order to avoid glucocorticoid use.
While there is no published information that supports the use of cyclosporine A prior to extractions, it has been shown to be effective in cases refractory to extraction therapy,16 and may provide an alternative to long-term steroid therapy. Therefore, I prefer to use cyclospo-rine only in patients in which medical management is necessary post extraction.11
Cyclosporine A must be used with caution in cats with hepatic or renal disease, and there are reports of fatal opportunistic infections associated with its use.17-19
The bioavailability of the 3 available forms of cyclo-sporine is quite variable, and dosing depends on which form is used.13 A veterinary product is available for feline atopy (Atopica, novartis.com), which may be useful for this condition.
Interferon. Feline interferon (Vibragen, virbac.com) is reported to provide both antiviral and immunomod-ulatory effects, restoring the normal local immune response.20 Several studies have shown efficacy in resis-tant cases20-22 but, as of yet, no available evidence dem-onstrates its efficacy as a primary treatment. While this product is not currently available in the U.S., it can be imported by completing paperwork through the U.S. Food and Drug Administration.
FELINE JUVENILE (PUBERTY) GINGIVITIS/PERIODONTITISDefinitionJuvenile periodontal disease develops when inflam-mation occurs shortly after permanent tooth erup-tion.9,23
EtiologyThe cause of this condition is unknown, but an infectious etiology is theorized. In humans, a simi-lar condition occurs due to a suspected temporary decrease in immune status during the pubertal peri-od.23,24 A genetic predisposition toward feline juve-nile periodontitis has been reported in Siamese, Somali, and Maine Coon cats.9
Clinical FeaturesHyperplastic gingivitis appears as significant gin-gival enlargement and inflammation (Figure 5).11
This disease is often mistaken for caudal stomatitis; apart from the age of onset, the distinguishing clinical sign is lack of caudal inflammation in cats with hyperplastic gingivitis.11 • If left untreated, this disease typically progresses to peri-
odontal disease, possibly resulting in early tooth loss.23
• As the patient matures, the inflammation may subside at approximately 2 years of age,9 following the same pattern as the human disease.24 If hyperplastic gingivitis is treated aggressively early
on, the patient may have normal periodontal health in the future.11
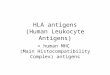
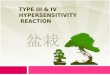
Juvenile periodontitis does not involve enlargement of the gingiva, and typically leads to rapid proliferation of plaque, calculus, and periodontal inflammation (Figure 6, page 48).12 This, in turn, results in early bone loss, periodon-tal pocket formation, and furcation exposure.9 Bone loss is generally most severe around the mandibular first molars (Figure 7, page 48).
Diagnosis11,23
• Histopathology should be considered in order to rule out other causes of gingival inflammation.
• Dental radiographs should be performed to evaluate the quality of the alveolar bone and early tooth resorption.
• Culture and sensitivity testing is generally unrewarding.
Therapeutic OptionsEarly (9 months of age) and frequent professional den-tal cleaning (every 6–9 months), along with strict home care is critical to decrease inflammation.11,23
• Ideally, home care consists of daily brushing; alterna-tives and/or complementary home care therapies include chlorhexidine rinses (CET Oral Hygiene Rinse, virbac.com), plaque control diets (t/d Canine and Feline Dental Health Diets, hillsvet.com), and treats (Greenies, greenies.com).
• If gingival hyperplasia is present, gingivectomy is recom-mended to remove pseudopockets, decrease inflamma-tion, and facilitate plaque control.9
• Extraction of any significantly diseased teeth is warranted.23
Figure 5. Significant hyperplastic gingivitis in a 10-month-old cat. This pet was referred for “stomatitis.” However, note the complete lack of caudal mucositis. The patient has juvenile periodontitis, not caudal stomatitis.
5
| Practical Dentistry
today’s Veterinary Practice January/February 201448
CHRONIC ULCERATIVE PARADENTAL STOMATITIS (KISSING LESIONS)DefinitionChronic ulcerative paradental stomatitis (CUPS) is an ulcerative, immune-mediated reaction of the oral tissues, typically the buccal mucosa but also the tongue.25
EtiologyCUPS is believed to represent an inflammatory rath-er than infectious etiology. A hypersensitivity reaction is most likely triggered by gram negative bacteria (and their inflammatory antigens) associated with the periodontal disease trigger.25,26
Clinical FeaturesCUPS is most common in small dogs, especially white breeds; however, this condition can occur in any breed. Onset is typically during middle age.25 Presenting signs include intense oral pain, halitosis, and partial to com-plete anorexia:25,27
Oral examination typically reveals:25 • Significant dental plaque and calculus, with gingivitis
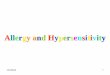
and gingival recession• The classic sign of severe buccal ulceration, in areas of con-
tact between the mucosa and affected teeth (Figure 8)• Lesions are typically most severe over the maxillary
canine and carnassial teeth and in areas of gingival recession.
• Occasionally there can be involvement of the entire buc-cal mucosa and the lateral edges of the tongue.
Diagnosis• Clinical signs are classic; however, histopathology
should be performed. • Dental radiographs should be exposed to evaluate peri-
odontal status. • Response to therapy (complete dental prophylaxis), with
early relapse, is confirmatory.Therapeutic OptionsThe key to managing this disease process is compre-hensive plaque control, which is achieved by a com-
bination of strict home care, regular dental cleanings, and selective to full-mouth extractions.25-27
Home Care. Tooth brushing and chlorhexidine rinses are the most effective means of plaque control at home. Dental diets or treats can be used in addition to or, in place of, brushing or rinsing. Finally, a barrier sealant (OraVet, merial.com) has shown some benefit in patients when used consistently.
An important point to consider is that, in the majority of cases:25 • Only partial recovery will occur even with the strictest
home care. • Without strict home care, conservative therapy will fail.
Resolution of clinical signs may occur due to the stoic nature of dogs, but there is generally some degree of con-tinued inflammation (and pain). Typically, these patients can only achieve complete resolution with partial to full-mouth extractions.
Surgical Therapy. During the first anesthetic event: • A complete dental prophylaxis should be performed. • Dental radiography should be performed.• All periodontally diseased teeth (especially those with
gingival recession) should be extracted. • Histopathology should be obtained and submitted to a
reference laboratory.Medical Therapy. Medical therapy is generally unre-
warding, but can be added to strict plaque control mea-sures in nonresponsive patients in which the owners are particularly resistant to extractions.25
A combination of antibiotic and anti-inflammatory medi-cations is typically used. It is important to note that patients often only have a partial response to this medical therapy, and only a transient (weeks to months) recovery follow-ing thorough dental prophylaxis.25 With either conserva-tive modality, relapse is usually imminent and generally complete.
Prior to initiation of therapy, and at regular intervals through the course of treatment, clients must be informed about the side effects and long-term complications that may result from antibiotic and anti-inflammatory medica-tions. Regular blood and urine testing must be performed
6 7
Figure 6. Severe hyperplastic oral inflammation in a 2 year old cat.
Figure 7. Dental radiograph of patient in figure 6. Note the signifi-cant alveolar bone loss, blue arrows.
8
Figure 8. Classic contact ulcer on the buccal mucosa over the maxil-lary right canine.

January/February 2014 today’s Veterinary Practice 49
Practical Dentistry |
Feli
ne
an
D c
an
ine
Or
al
Ulc
er
atiV
e D
ise
as
e
to ensure that untoward effects are not occurring. These factors, and the involved costs, need to be weighed
against surgical therapy.Follow-Up. After the diagnosis is confirmed, remind
the owner of the long-term and consistent commitment required for treating this disease process. • In addition to home care, regular dental cleanings (sev-
eral times a year) are necessary to control clinical signs in most patients.
• If this is a concern, or home care is impossible, extrac-tion of the maxillary canine and carnassial teeth (as well as any other teeth involved) should be performed.25
• Consequently, full-mouth extractions are not unusual in these cases. This therapy, while extreme, is curative in the vast majority of cases.25 When full-mouth extractions are performed, it is not
uncommon for clients to report that their dogs are “acting like a puppy again.”
EOSINOPHILIC GRANULOMA COMPLEX EtiologyEtiology of this condition is unknown. However, a local accumulation of eosinophils is thought to initiate inflam-mation and necrosis,28 which may result from local (food) or systemic allergies, although, these lesions have been seen in patients in which allergic disease has been ruled out.29,30 Additional causes include a response to irritation, such as chronic grooming or traumatic malocclusion,25,31 or a genetic predisposition.32
While these lesions have been reported in dogs,33 they are much more common in cats. Therefore, the discussion in this section will relate to cats, although, the disease pro-cess is similar in both species.34
Clinical Features• Indolent ulcers are the most common oral manifesta-
tion, and present as brownish-red lesions on the upper lip or around the maxillary canine teeth (Figure 9).35
• Linear granulomas can be single or multiple; the most commonly affected sites are the lips, gingiva, palate, and tongue (Figure 10).25 They are generally nonpainful, but may develop secondary infections.
• The typical presentation is a raised, lobulated yellow-pink mass; however, it can also appear ulcerative. These lesions may lead to severe periodontal loss, pathologic fractures, or oronasal fistulas.34,36,37
Diagnosis• Histopathology should be performed to confirm the
diagnosis.36 • Following diagnosis confirmation, a thorough allergy
evaluation should be conducted, including food trial, flea treatment, +/- allergy testing.25
Therapeutic OptionsThe acute disease process is best treated with system-ic corticosteroids, and a typical initial protocol is pred-nisone, 2 mg/kg Q 12 H for 3 to 4 weeks.28,38 Additional options include intralesional triamcinolone (3 mg/week) or methylprednisolone injections.39
Antibiotic therapy is occasionally required to induce remission and/or treat secondary infection. There are also some patients that appear to respond to antibiotic therapy alone.40 Therefore, we initially treat mild cases with antibiotics alone and more severe cases with a combi-nation of antibiotics and corticosteroids.
If an allergy component is identified, it should be addressed (eg, flea control, hyposensitization, food trial).41 However, many cases remain idiopathic, requiring lifelong therapy. Cyclosporine has been shown to be effective in treating this condition, with fewer side effects demon-strated compared to steroids.42,43 �
cUPs = chronic ulcerative paradental stomatitis; Fcs = feline caudal stomatitis; FelV = feline leukemia virus; FiV = feline immunodeficiency virus
To view the references for this article, go to todays veterinarypractice.com/resources.asp#resources.
Brook A. Niemiec, DVM, FAVD, Diplomate AVDC, is chief of staff of Southern California Veterinary Dental Specialties, with offices in San Diego and Murrieta, California, and Las Vegas, Nevada.
Figure 9. Large eosinophilic granuloma (indolent ulcer) on the nose of a cat.
9
Figure 10. Eosinophilic granuloma sublingual in a cat.
10

| Practical Dentistry
today’s Veterinary Practice January/February 201450
References1. Lyon KF. Gingivostomatitis. Vet Clin N Am Small Anim Pract 2005;
35(4):891-911.2. AVDC accepted nomenclature; available at avdc.org. 3. Debowes LJ. Problems with the gingiva. In Niemiec BA (ed): Small
Animal Dental, Oral and Maxillofacial disease: A Color Handbook. London: Manson, 2010, pp 159-181.
4. Camy G, Fahrenkrug P, Gracis M, et al. Proposed guidelines on the management of feline chronic gingivostomatitis (FCGS) syndrome: A consensus statement, September 2010.
5. Lommer MJ, Verstraete FJM. Concurrent oral shedding of feline calicivirus and feline herpesvirus 1 in cats with chronic gingivostomatitis. Oral Microbiol Immunol 2013; 18:131-134.
6. Hardy WD, Zuckerman E, Corbishley J. Serological evidence that Bartonella cause gingivitis and stomatitis in cats. Annual Vet Dental Forum Proc 2002; pp 79-82.
7. Thompson RR, Wilcox GE, Clark WT, Jansen KL. Association of calicivirus infection with chronic gingivitis and pharyngitis in cats. J Small Anim Pract 1984; 25(4):207-210.
8. Dowers KL, Hawley JR, Brewer MM, et al. Association of Bartonella species, feline calicivirus, and feline herpesvirus 1 infection with gingivostomatitis in cats. J Feline Med Surg 2010; 12(4):314-321.
9. Wiggs RB, Lobprise HB. Domestic feline oral and dental disease. Veterinary Dentistry, Principals and Practice. Philadelphia: Lippincott, 1997, pp 482-517.
10. Niemiec BA. Ptalysim. In Ettinger SJ, Feldman EC (ed): Textbook of Veterinary Internal Medicine. Philadelphia: Saunders, 2010.
11. Niemiec BA. Unusual forms of periodontal disease. In Niemiec BA (ed): Veterinary Periodontology. Ames, IA: Wiley-Blackwell, 2012, pp 91-104.
12. Niemiec BA. Oral pathology. Top Companion Anim Med 2008; 23(2):59-71.
13. Bellows J. Treatment of oropharyngeal inflammation. Feline Dentistry: Oral Assessment, Treatment, and Preventative Care. Ames, Iowa: Wiley-Blackwell, 2010, pp 242-268.
14. Hennet P. Chronic gingiva-stomatitis in cats: Long term follow up on 30 cases treated by dental extractions. J Vet Dent 1997; 14(1):15-21.
15. Lewis JR, Tsugawa AJ, Reiter AM. Use of CO2 laser as an adjunctive treatment for caudal stomatitis in a cat. J Vet Dent 2007; 24(4):240-249.
16. Lommer MJ. Efficacy of cyclosporine for chronic, refractory stomatitis in cats: A randomized, placebo-controlled, double-blinded clinical study. J Vet Dent 2013; 30(1):8-17.
17. Last RD, Suzuki Y, Manning T, et al. A case of fatal systemic toxoplasmosis in a cat being treated with cyclosporine A for feline atopy. Vet Dermatol 2004; 15(3):194-198.
18. Beatty J, Barra V. Acute toxoplasmosis in two cats on cyclosporine therapy. Aust Vet J 2003; 81(6):339.
19. Davis E. Systemic cyclosporine administration and life threatening infections. An emerging problem in veterinary medicine. Am Vet Dental Forum Proc 2007.
20. Southerden P, Gorrel C. Treatment of a case of refractory feline chronic gingivostomatitis with recombinant interferon omega. J Small Anim Pract 2007; 48(2):104-106.
21. Hennet P, Camay G. Comparative efficacy of a recombinent feline interferonomega in refractory cases of Calici-virus positive cats with caudal stomatitis: A randomized multicentric, controlled, double blind study in 39 cats. J Feline Med Surg 2011; 13(8):577-578.
22. Mihaljevic S. Feline gingivitis-stomatitis FORl complex: First clinical data on the use of interferon. BTP Congress Proc 2002.
23. Niemiec BA. Pathology in the pediatric patient. In Niemied BA (ed): Small Animal Dental, Oral and Maxillofacial Disease: A Color Handbook. London, Manson, 2010, pp 189-126.
24. Neville BW, Damm DD, Allen CM, Bouquot JE. Periodontal diseases. Oral and Maxillofacial Pathology, 2nd ed. Philadelphia: Saunders, 2002, pp 137-162.
25. Niemiec BA. Problems with the oral mucosa. In Niemiec BA (ed): Small Animal Dental, Oral and Maxillofacial Disease: A Color Handbook. London: Manson Publishing, 2010, pp 189-191.
26. Boutoille F, Hennet P. Maxillary osteomyelitis in two scottish terrier dogs with chronic ulcerative paradental stomatitis. J Vet Dent 2011; 28(2):96-100.
27. Lobprise HB. Oral ulceration and chronic ulcerative paradental stomatitis. Blackwell’s Five-Minute Veterinary Consult Clinical Companion—Small Animal Dentistry, 2nd ed. Ames, IA: Wiley-Blackwell, 2012, pp 243-247.
28. Leiferman KM. A current perspective on the role of eosinophils in dermatologic diseases. J Am Acad Derm 1991; 24:1101–1112.
29. Harvey RG, McKeever PJ. Ulcerative dermatoses. A Colour
Handbook of Skin Diseases of the Dog and Cat. London: Manson Publishing, 1998, p. 81–106.
30. Wilkenson GT, Bate MJ. A possible further manifestation of feline eosinophilic granuloma complex. JAAHA 1984; 20:519-526.
31. Garcia M, Pagerois X, Curco N, et al. Eosinophilic ulcer of the oral mucosa: 11 cases. Annales de Dermatologie et de Vénéréologie 2002; 129(6–7):871-873.
32. Leistra WH, van Oost BA, Willemse T. Nonpruritic granuloma in Norwegian forest cats. Vet Rec 2005; 156(18):575-577.
33. Bredal WP, Gunnes G, Vollset I, Ulstein TL. Oral eosinophilic granuloma in three Cavalier King Charles spaniels. J Sm Anim Prat 1996; 37:499-504.
34. Woodward TM. Greater palatine island axial pattern flap for repair of oronasal fistula related to eosinophilic granuloma. J Vet Dent 2006; 23(3):161-166.
35. Frost P, Williams CA. Feline dental disease. Vet Clin N Am Sm Anim Pract 1986; 16:851.
36. Silvestros SS, Mamalis AA, Sklavounou AD, et al. Eosinophilic granuloma masquerading as aggressive periodontitis. J Perio 2006; 77(5):917-921.
37. Holzhauer AM, Abdelsayed RA, Sutley SH. Eosinophilic granuloma: A case report with pathological fracture. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1999; 87(6):756-759.
38. Reedy LM. Results of allergy testing and hyposensitization in selected feline skin diseases. JAAHA 1982; 18:618-623.
39. Withrow ST, Norris AM, Dubielzig RR. Oropharyngeal neoplasms. In Harvey CE (ed): Veterinary Dentistry. Philadelphia: Saunders, 1985, pp 123-126.
40. Rosencrantz WS. Feline eosinophilic granuloma complex. In Griffin CE, Kwochka KW, MacDonald JM (eds): Current Veterinary Dermatology. St. Louis: Mosby, 1993, pp 319-324.
41. MacEwan EG, Hess PW. Evaluation of effect of immunomodulation of the feline eosinophilic granuloma complex. JAAHA 1987; 23:519-526.
42. Steffan J, Favrot C, Mueller R. A systematic review and meta-analysis of the efficacy and safety of cyclosporine for the treatment of atopic dermatitis in dogs. Vet Derm 2006; 17(1):3-16.
43. Vercelli A, Raviri G, Cornegliani L. The use of cyclosporine to treat feline dermatosis: A retrospective analysis of 23 cases. Vet Derm 2006; 17(3):201-206.