Embed Size (px)
Citation preview

Fellows Cases
Aaron Kirkpatrick Jaime Torres
Ashima Synghal Sahni Annise Georgette Wilson
Moderators: Alejandra C. Lastra
Madeleine Grigg-Damberger
The presenters have disclosed no conflict of interest

Learning Objectives
At the conclusion of this course participants will be able to:
1. Construct a diagnostic approach to circadian rhythm disorders and evaluate the role for actigraphy testing.
2. Recognize challenges in Narcolepsy treatment including side effects of certain medications.
3. Assess the pathophysiology, recognize causes and recommend treatment for cataplexy.
The presenters have disclosed no conflict of interest

Case
Aaron Kirkpatrick, MD

History of Present Illness (HPI)
30 year-old male with history of blindness presents for insomnia and excessive daytime sleepiness.

HPI
• Normal sleep schedule in high school (graduated 06)
• Sleep complaints began in 2009
• Mother reports that patient spends majority of the day in bed on the computer
• Bedtime is variable (anywhere from 10 pm – 4 am)
• Usually on computer before going to bed

HPI
Bedtime: Variable
• Takes 45 min – 60 min to fall asleep
• Awakens to loud noises or when hungry; takes 30-60 min to fall back asleep
Waketime: Variable
• Occasionally takes long naps

HPI
• Thinks about being taken advantage of when trying to go to sleep
• Does not use any sleep aids

Past Medical History
• Blindness in both eyes secondary to premature birth
• Psychosis (event in 2011)

Past Surgical History
• Colon surgery as infant due to perforated bowel
• Eye surgery secondary to detached retina at 2 years old

Family History
• Mother: Hypertension (HTN)
• Father: HTN and Diabetes Mellitus
• Uncle: Colon cancer

Social History
• Lives at home with parents
• Graduated High School; has attempted to participate in daytime activities but encountered barriers
• Tobacco: Never smoked
• Alcohol: Never drank
• No illicit drug use

Medications
No daily medications

Physical Exam
Vitals: Blood pressure 115/75; Pulse: 90; Oxymetry: 98% General: NAD, no accessory muscle use or conversational dyspnea
HEENT: Blind, anicteric, conjunctiva pink. Nares patent. Oral mucosa moist, no thrush. MMP 3, neck circumference of 15. Tonsils 2+ symmetric
Neck: Supple, no JVD, no stridor. No palpable LAD
Respiratory: Symmetric chest expansion. CTAB. No wheeze/rale/rhonchi
Cardiovascular: Normal S1 and S2, no audible pathologic murmurs/gallops/rubs
Gastrointestinal: Abdominal contour is normal. Abdomen soft, nontender, nondistended. + BS
Psychiatric: Speech is appropriate with regular rate and rhythm.
SKIN The skin has no visible rash, or ulcers noted

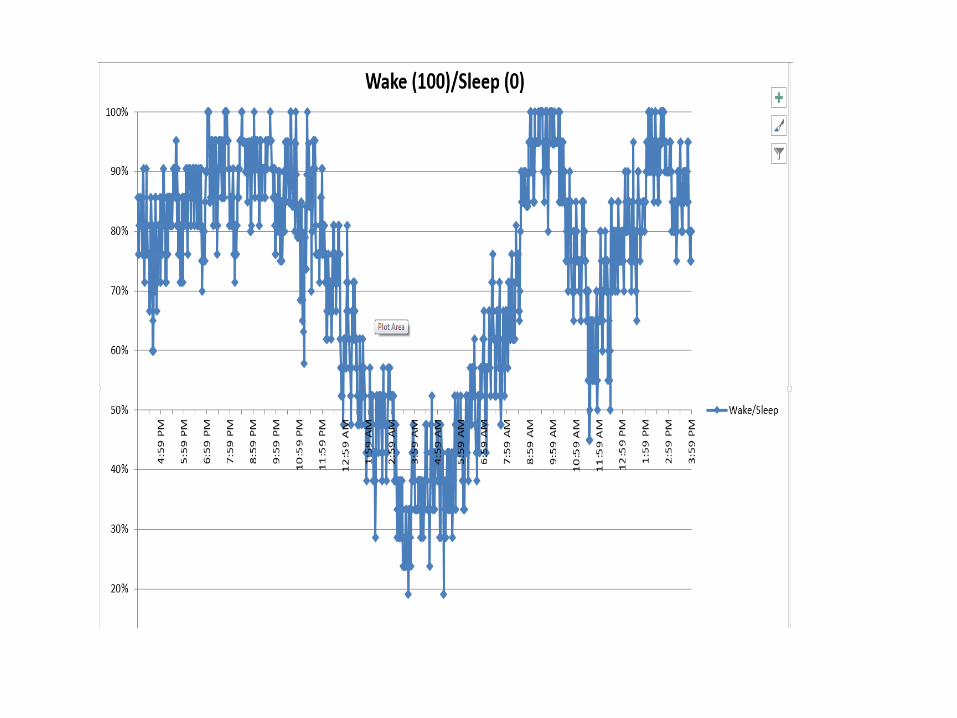
Summary
• 30 year-old male with blindness since birth with abnormal sleep schedule
• Goes to bed anywhere from 10 pm – 4 am
• Spends most of the day in his room on the computer
• Normal sleep schedule while in high school
• Occasionally takes long naps during the day





Recommendations
• Nightly melatonin (2 mg) at 11:30 pm
• Bedtime between 1-1:30 am
• Waketime around 8:30 am

Teaching Points
Delayed Sleep-Wake Phase Disorder
• Circadian rhythm promotes wakefulness until late evening
• Results in delayed sleep onset (midnight or later)
• Usually has a consistent bedtime
• Circadian system is actively driving sleep later than conventional wake-up times
Non 24 Hour Sleep Wake Disorder
• Free running circadian system
• Usually longer than 24 hours
• Inconsistent bedtime; will eventually align with normal bedtime for a brief period

Sleep Disorders in the Blind
• All disorders have been linked to abnormally timed melatonin production
• Related to light perception
• Irrespective of degree of vision loss

Case
Jaime Torres, MD

History of Present Illness (HPI)
24 year old female presents for evaluation of excessive daytime sleepiness (EDS). - On presentation she reported EDS, unrefreshing
sleep, dry mouth, frequent nocturnal arousals, and morning headaches
- Consistent sleep wake cycles, 10PM to 8AM - Managed EDS with mid day 1 hour nap and
caffeine - +cataplexy?, sleep paralysis and hypnogogic
hallucinations

Past Medical History
ADHD
Hashimoto’s thyroiditis
Depression
Obstructive Sleep apnea
Narcolepsy without cataplexy
Parasomnia- Sleep walking

PSG/MSLT (3/1/15)
• TST: 500 minutes
• SOL: 12 minutes
• REM latency: 1h 24 min
• AHI 5.87, REM AHI 10, Supine 7, O2 nadir 94%
• MSLT: mean sleep onset latency of 3.4 minutes with 3 SOREM

Medications
• Sodium oxybate 2.25g nightly
• Dextroamphetamine 40mg BID
• Bupropion 150mg
• Fluoxetine 20mg
• Flonase
• Levothyroxine 50mg
• Cetirizine
• Mirena IUD

Social history
• Prior use of THC
• Denied EtOH or tobacco
• Completed a college degree
• Not sexually active with men

Physical exam
• Vitals: BP 139/89, HR 109, RR 16 99% on RA
• BMI 19.6
• Gen: WD/WN, NAD
• HEENT: MMP 3, Tonsils: absent
• Card: RRR, s1/s2
• Pulm: CTAB, no wheezing
• GI: soft abdomen, +BS
• Neuro: normal tone, no deficits


Treatment plan
• Adjust sodium oxybate dosing
• Repeat PSG on sodium oxybate
• Continuation of stimulants
• Consistent sleep-wake cycle with a scheduled mid-day nap

Narcolepsy management
• Behavioral – Consistent sleep-wake cycles
– Patient and family education
– Scheduled naps
– Safety precautions
– Avoidance of depressants
• Pharmacologic – Sodium oxybate
– Stimulants
– Anti-depressants (TCA, SSRI)

Sodium oxybate dosing

Sodium oxybate side effects
• Nausea (20%), dizziness (15%), emesis (11%), enuresis (7%)
• Behavioral: confusion, anxiety, hallucinations, aggression
• Parasomnias (6%)
• Pregnancy category C
– Excreted in breast milk
• Dependence
• Bradycardia

Patient follow up
• Up-titrated to 9gm sodium oxybate nightly
• Finding food crumps on bed
• PSG (on Xyrem): AHI 7.1, Supine 18
• Mild ongoing EDS in spite of multiple stimulants

Teaching points
• Management of narcolepsy requires both behavioral and pharmacologic approaches
• Sodium oxybate doing should begin at 2.25g twice a night and up-titrated weekly to a treatment dose of 6-9g nightly
• Sleep related eating disorder and other parasomnias could be induced by Sodium Oxybate. Patients should be counseled to avoid risks of injury
Case
Ashima Sahni, MD
and
Annise Wilson, MD

Case Presentation
23 year old female presented to the clinic with childhood complaints of events associated with:
– Sudden loss of muscle tone of the whole body
– Happens with hard laughter
– Lasts for 1-2 minutes
– Not associated with loss of consciousness and/or no post-ictal confusion
– No lightheadedness/prodrome prior to the episode
– Frequency = 2 -3 times/year but now 3 – 6 times/year
•Age of onset = 8 to 10 years old
•Denies any history of childhood trauma or perinatal insult
•Doesn’t recall any hospitalization or illness around the onset of the symptoms.
•Doesn’t recall receiving any vaccination around that time.

Thoughts?

Differential Diagnosis
• Cataplexy
• Syncope – Loss of consciousness during hearty laughter.
• Hyperekplexia – Exaggerated startle responses to acoustic, tactile or visual stimuli provokes
facial grimace, shoulder abduction, flexion neck, trunk, elbows and knees, and fall.
• Epilepsy - Rare case reports: gelastic-atonic; focal seizures with asymmetric loss of tone causing
fall;cluster of myoclonic jerks causing fall in juvenile myoclonic epilepsy;ictal syncope in temporal lobe epilepsy.Ictal activity on EEG.
• Hypo and hyperkalemic periodic paralysis- Episodic limb weakness affecting
eyes and trunk with preserved consciousness; begin before breakfast, last 15-60 minutes; emotional stress can trigger
• Pseudocataplexy – negative emotions, more often have global weakness,
longer duration, comorbid with depression, normal DTRs during the attack

Additional History
Review of systems –
No fever, no weight loss, no depression/anxiety, no cough, no palpitation,
PMH –
h/o migraines (Age of onset: 12, Both sides, Frequency: Every few months, Lasts for several hours to 1 day, Visual Aura are present,
Other Triggers: Light and red wine)
PSH – negative
Social history - negative for use of tobacco, alcohol, or illicit drugs
Family history :
Mother –migraines, paternal grandmother – breast cancer, maternal grandmother - lymphoma
Medications – Excedrin as needed
Allergies- NKDA
Occupational History: forensic accountant

Sleeping Habits
• Estimated number of hours of sleep/night: 6-7 hours
• Bedtime : 11 pm
• Sleep onset latency: 10-15 minutes
• Wake time: 7 am
• WASO: none
• Naps: no
• Caffeinated beverages consumed/day: 1 cup/day mostly in the morning

Epworth Sleepiness Scale
• 2 - Sitting and reading
• 1 - Watching TV
• 0 - Sitting inactive in a public place (eg a theater or a meeting)
• 2 - As a passenger in a car for an hour without a break
• 3 - Lying down to rest in the afternoon when circumstances permit
• 0 - Sitting and talking to someone
• 0 - Sitting quietly after a lunch without alcohol
• 0 - In a car, while stopped for a few minutes in traffic
8/24 = normal
• 0 = no chance of dozing
• 1 = slight chance of dozing
• 2 = moderate chance of dozing
• 3 = high chance of dozing

Physical Exam
BP 130/70 mmHg | Pulse 68 | Resp 18 | BMI 25.85 kg/m2 | SpO2 97% HEENT: NCAT, neck supple and non-tender, oral mucosa pink and moist; nasal mucosal
RESP: Clear to auscultation; No audible wheezes noted CVS: RRR Abdomen: Soft, non-tender EXTREMITIES: No clubbing, no cyanosis. No LE edema noted

Neurological Exam
MS: Alert, speech fluent and appropriate, language intact.
CN: PERRL. EOMI. Smooth pursuits w/ no nystagmus noted. Smile symmetric. Uvula midline with symmetric palatal elevation. Head turns b/l. Tongue midline.
MOTOR: Normal bulk and tone. No adventitious movements or bradykinesia. UE strength- 5/5 throughout
LE strength- 5/5 throughout
Deep tendon reflexes:3 plus and symmetric
Absent Babinski signs bilaterally
SENSORY: Intact to light touch
COORDINATION: No dysmetria or ataxia.
GAIT: Steady, able to tandem, negative Romberg sign

Next Steps?

Work-up
• CBC, BMP, LFTs – normal
• TSH/T4- normal
• EKG – normal sinus rhythm
• MRI brain ordered


MRI Brain WWO
6 mm focus of hyperintense FLAIR signal in the right ventral aspect of the periaqueductal gray
This MRI brain was followed up by baseline tumor protocol including a 3D flair sequence
7 mm, nonenhancing area of hyperintense T2/FLAIR signal within the right dorsal, medial midbrain, along the periaqueductal gray matter

Diagnosis
Patient only had symptoms suggestive of cataplexy without sleep paralysis, hallucinations, and sleep attacks
Autoimmune panel - negative

Repeat MRI Brain- 6 months
Repeat MRI Brain- 6 months
A 7 mm, nonenhancing area of hyperintense T2/FLAIR signal within the right dorsomedial midbrain, along the periaqueductal gray matter, is unchanged since the previous MRI

Cataplexy • The term cataplexy is derived from the Latin word cataplessa
(to strike down with fear or the like) and Greek kataplexis (down-stroke).
• It was coined by Henneberg in 1916
• True prevalence of isolated cataplexy is unknown
• Prevalence with excessive daytime sleepiness (EDS) in young adults is 29%
• Familial cases have been reported with or without EDS
• It persists throughout life, although the frequency of attacks might decrease with age.
• Men often experience a higher number of cataplectic attacks than women

Clinical Features
• Triggered by emotions mostly positive
• Preserved consciousness
• Difficulty to evoke in unfamiliar and often uncomfortable locations
• Lack of pre-syncopal symptoms
• Affects all skeletal muscles – Forward drop of the head (nuchal weakness)
– Sagging of the jaw (hypotonia of the facial muscles)
– Buckling of the knees
• Abolished DTRs during the event
• Respiratory muscles and ocular muscles are not involved
• Mostly bilateral
• Most patients report a consistent pattern of muscle involvement
• Mostly abrupt onset ( 10 sec to 2 mins)
• Surface EMG on the myohyoid may show “waxing and waning” tone with bouts of rapid eye movements with irregularities on both breathing and heart rate.

N Engl J Med 2015;373:2654-62.

Pathophysiology
Cataplexy may be considered a transition from wakefulness directly to an atonic state as seen in REM sleep, triggered by emotional stimulus.
This theory is supported by therapeutic improvement with the use of medications that have REM suppressing action.

J. Neurosci., September 5, 2012 • 32(36):12305–12311
vIPAG- ventrolateral periaqueductal gray LPT- lateral pontine tegmentum SLD - sublaterodorsal nucleus
Ach GABA AND GLYCINE
Raphe nucleus – 5HT
Loc cerelus – NE
Solid pathways are active;
Dashed pathways are inactive.
Green pathways are excitatory;
red pathways are inhibitory.

Solid pathways are
active;
Dashed pathways are
inactive.
Green pathways are
excitatory;
red pathways are
inhibitory.
GABA AND glycine
vIPAG- ventrolateral periaqueductal gray LPT- lateral pontine tegmentum SLD - sublaterodorsal nucleus
Basal forebrain - Ach

Causes of Cataplexy
• Pathognomonic for Narcolepsy 1 (idiopathic)
• Secondary causes:
– Hereditary
– Acquired

Secondary Hereditary Causes of Cataplexy
• Niemann-Pick type C
• Prader-Willi Syndrome
• Norrie Disease
• Moebius Syndrome
• Angelman Syndrome
• Autosomal Dominant Cerebellar Ataxia, Deafness and Narcolepsy (ADCA-DN)

Secondary Cataplexy in Acquired Disorders
• Injury to hypothalamus and pontomedullary region
• Tumors in hypothalamus
• Hypoxic ischemic injuries in pontine region
• Paraneoplastic syndrome
• Limbic encephalitis
• Rapid onset obesity with hypothalamic dysfunction, hypoventilation and autonomic dysregulation (ROHHAD)

Journal of Clinical Sleep Medicine, Vol. 7, No. 2, 2011
• 67 year old presented with cataplexy symptoms
• Had started when he was admitted to the hospital for transient neurological symptoms
• Hypothalamus is intact therefore no narcolepsy symptoms
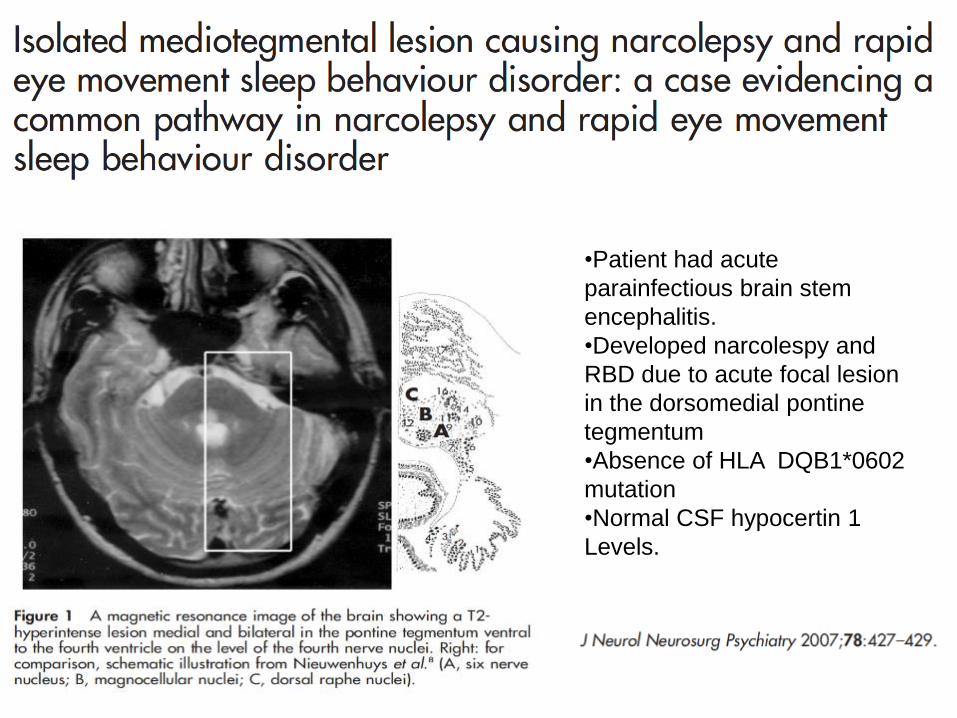
•Patient had acute
parainfectious brain stem
encephalitis.
•Developed narcolespy and
RBD due to acute focal lesion
in the dorsomedial pontine
tegmentum
•Absence of HLA DQB1*0602
mutation
•Normal CSF hypocertin 1
Levels.

Partial cataplexy with bilateral
internuclear ophthalmoplegia
and vertical nystagmus.
Dx – GBM
The tumor extended into the
thalamus, hypothalamus, and
medial temporal lobes bilaterally
and involved the head of the
caudate on the right.
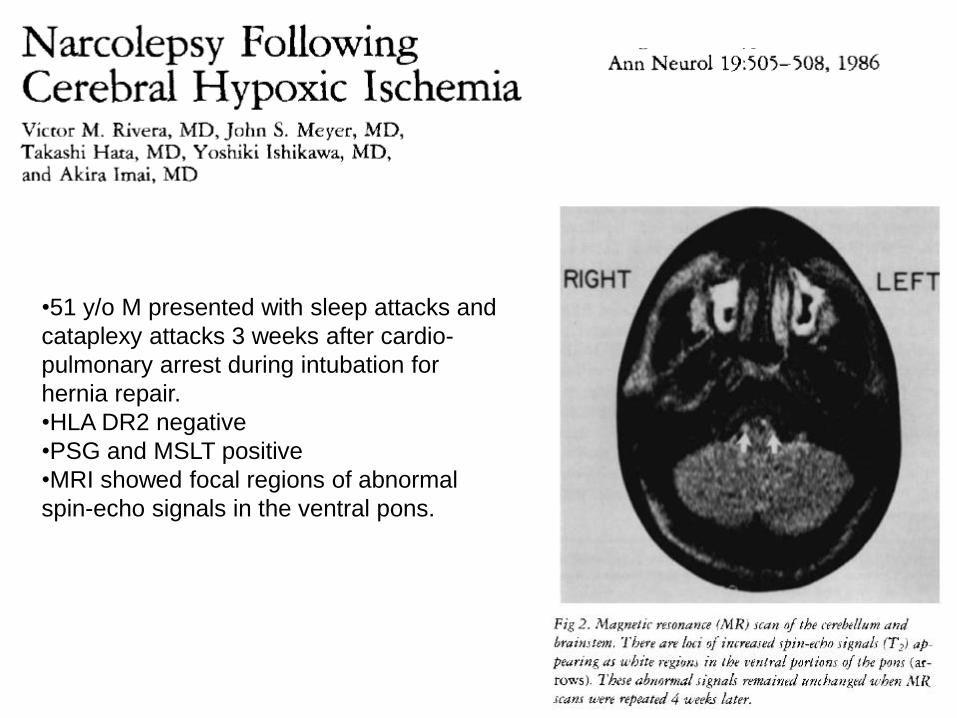
•51 y/o M presented with sleep attacks and
cataplexy attacks 3 weeks after cardio-
pulmonary arrest during intubation for
hernia repair.
•HLA DR2 negative
•PSG and MSLT positive
•MRI showed focal regions of abnormal
spin-echo signals in the ventral pons.
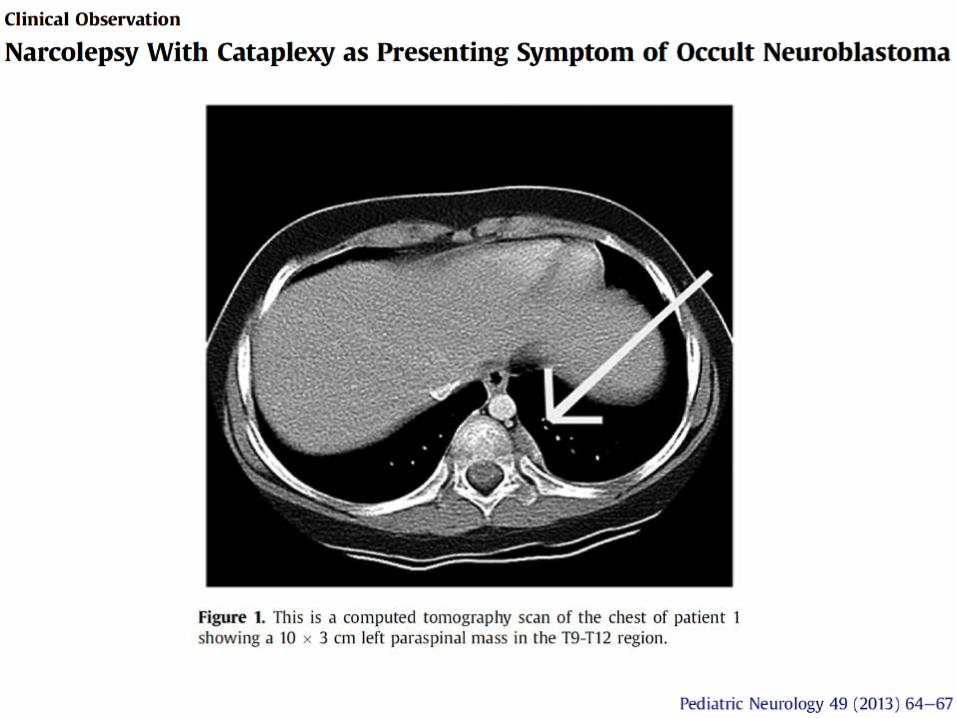
• Neuroblastoma associated with the paraneoplastic syndrome of opsoclonus-myoclonus.
• Presentation with narcolepsy-cataplexy is not well-documented
• Described 3 patients, each presenting in early childhood with complex neurological symptoms including narcolepsy with cataplexy that were subsequently found to have paraspinal neuroblastoma.
• In two of the cases, neurological symptoms resolved with treatment of the tumor and/or immunosuppression
• 1 case, the child persistently had a devastating course despite complete
resection of the tumor and aggressive immunosuppression.

• Patient presented with a clinical syndrome of limbic encephalitis, narcolepsy, and cataplexy.
• The anti-Ma2 antibody was positive.
• No mass on imaging but orchiectomy was performed and testicular carcinoma was found.
Neuro-Oncology 5, 214–216, 2003

Multiple sclerosis and cataplexy
• Symptoms of narcolepsy/cataplexy developed in a monozygotic twin at the age of 56 years, 25 years after the onset of multiple sclerosis.
• The diagnosis of narcolepsy/cataplexy was confirmed by polygraphic recordings.

Treatment
Mild and infrequent – patient may choose not to be treated
Non pharmacological –
– Sleep hygiene
– Actively informing friends and colleagues, with psychological support to aid in this process of acceptance of the diagnosis
– Driving precautions

Treatment
• Severity may change overtime
• Sodium oxybate and anti-depressants
• No head to head trials
• Not formally studied for cataplexy
Norepinephrine and serotonin suppress REM sleep, and by blocking reuptake of these neurotransmitters, antidepressants reduce REM sleep and substantially reduce cataplexy.

Curr Treat Options Neurol (2017) 19: 23

Back to our patient
• Patient had a lesion in the dorsomedial midbrain along the periaqueductal gray matter which is vital for maintaining tone during wakefulness.

Hypothalamus
vIPAG- ventrolateral periaqueductal gray LPT- lateral pontine tegmentum
SLD - sublaterodorsal nucleus
Medial medulla

Back to our patient
• EEG and autonomic testing - deferred
• Lumbar puncture - refused
• PSG/MSLT - refused
• SNRI was offered for the management of cataplexy but patient wanted to think about it
• Will get serial MRI brain
Take Home Points
• Isolated cataplexy is a rare but important consideration in the differential diagnosis of a patient with drop attacks without alteration of consciousness.
• Consider neuroimaging in patients with isolated cataplexy to r/o secondary causes including tumors/lesions in hypothalamus and brainstem
• Pathogenesis of cataplexy - SLD causes atonia in sleep and gets activated in the wakefulness due to loss of orexin/excitation of amygdala
• Orexin levels in the CSF could be normal.


Questions?

Special Thanks
• Dr. Hrayr Attarian
• Dr. Sabra Abbott

Thank you!