Embed Size (px)
Citation preview

Fetal programming of metabolic disease
A stimulus or insult at a critical period of early life, often when rates of growth are maximal, leads to irreversible changes in structure and function of target organs.
– Pancreas Late onset diabetes
– Kidney? Hypertension
– Heart Coronary artery disease
– Blood vessels Hypertension, atherosclerosis, stroke
Barker, DJ & Clark, PM. (1997) Reviews of Reproduction, 2: 105-112.

Sheffield Ward

-2.5 -3 -3.4 -3.9 >3.980
100
120
140
160
180 Systolic (p = 0.0005)Diastolic (p = 0.0001)
Birth Weight [kg]
Blo
od
Pre
ssu
re[m
mH
g]
Relationship between fetal growth retardation and blood pressure in
middle age

Aorta (p = 0.01)
7
8
9
10
11
12
13
14
PWV [ms-1]
-2.5 -3 -3.4 >3.4
Birth Weight [kg]
Relationship between fetal growth retardation and arterial stiffness in
middle age
Martyn CN et al. British Heart Journal, (1995). 73: 116-121.
Leg (p = 0.03)

Babies
With thanks to Chris Martyn

What is the mechanism linking reduced birth weight and increased blood pressure in adult life?

Hypothesis• With age, progressive fragmentation and loss of
elastin (which cannot be resynthesised) and replacement by collagen --> increased arterial stiffness --> increased pulse pressure.
• In growth retarded infants elastin synthesis is reduced in utero, arteries are stiffer than normal from an early age and never fully recover.
Martyn CN and Greenwald SE. Lancet. 1997; 350: 953-955.

Berry CL, et al. (1972) Journal of Pathology. 108: 265-274.
0
10
20
30
40
50
ElastinCollagen
Gestational age (weeks) Months after birth
40200 2 864 1210
Birth
Protein (% dry weight)
Human aortic elastin & collagen in early life

aorta
common iliac
external iliac
umbilical arteries
internal iliac
Normal SUA

Histology
UI present
UI absent
Berry CL et al. (1976) British Heart Journal, 38: 310-315.
Meyer WW and Lind J. (1974) Archives of Disease in Childhood,. 49: 671-679.
Compliance
0
2
4
6
8
NORMAL SUA (+) SUA (-)
Co
mp
lian
ce
[%
/10
mm
Hg
]

Twin to Twin Transfusion Syndrome (TTTS)
A natural model of the effects of volume loading on fetal vascular
development.

TTTS occurs in identical twins
• Most identical twins share a common placenta (monochorionic).
• Of these, 10-15% develop TTTS wherein blood is unevenly distributed between them.
• Thought to be due to the presence of deep arteriovenous anastomoses within the placenta.
• Recipient:– Hypervolaemia, polyuria, polyhydramnios, LV hypertrophy, systemic
hypertension(?), cardiac malformations.
• Donor:– Hypovolaemia, poor renal perfusion, oliguria, oligohydramnios.

Prognosis & treatment
• Perinatal mortality in 80 to 100% of untreated cases• Amnioreduction (symptomatic)
– to reduce amniotic fluid volume and pressure– 60 to 70% survival
• Laser ablation of anastomoses– to prevent inter-twin transfusion and establish separate circulations– Better than 70% survival

Hypothesis
• Previously shown that donor twin has 2x increase in brachial artery PWV in infancy
• Is this due to chronic hypovolaemia and or abnormal pressure during uterine life?
• If so, laser treatment, by restoring normal pressure and flow, should prevent vascular remodelling and reduce inter-twin PWV differences?

Subjects
• 50 twin pairs (London & Hamburg)
• PWV measured in brachioradial artery
• Median corrected postnatal age 11.1 months
• Range 1 week to 64 months
• Ethical approval in both centres

TTTSSymptomatically
treated (n = 14)
TTTSlaser treated
(n = 13)
No TTTS(n = 12)
No TTTSNon identical
(n= 11)
Identical(monochorionic)
Non-identicaldichorionic
4 groups

Variables measured
• Brachial artery PWV
• Birthweight
• Gestational age
• BP differences between twins
• Age at diagnosis
• Mean age at PWV measurement

PWV [ms-1]
1
3
5
7
9
11
L H
Symp Laser Non TTTS Non I
L HD RD R
identical
TTTS No TTTS
PWV donor recipient pairs

PWV differences
-2
-1
0
1
2
Heavier - Lighter [ms-1]
Symp Laser No TTTS Non I
identical
TTTS No TTTS

Limitations
• Milder manifestation of TTTS in conservatively treated group
• Variable onset and duration of TTTS before treatment
• Radial artery compliance may not reflect that of central arteries and LV load
• Cross sectional measurements at different (young) ages, no idea yet of long term effects

Conclusions
• Vascular programming seen in identical twins with TTTS
• PWV discordancy altered but not abolished by intrauterine laser treatment, to resemble that seen in fraternal twins with separate uterine circulations

Hypothesis• With age, progressive fragmentation and loss of elastin
(which cannot be resynthesised) and replacement by collagen --> increased arterial stiffness --> increased pulse pressure.
• In growth retarded infants elastin synthesis is reduced in utero, arteries are stiffer than normal from an early age and never fully recover.
Martyn CN and Greenwald SE. Lancet. 1997; 350: 953-955.

Animal model of fetal growth retardation
• Pregnant rats divided into two groups– Low protein (LP) group given 9% protein diet
– Control group (C) given 18% protein diet, isocaloric
– Offspring weaned at 4 weeks onto normal diet
– Animals killed at 4, 8 and12 weeks
• Measure – BP or Left ventricular dimensions
– Aortic elasticity & chemical compositionUnpublished data

Left ventricle
0.4
0.5
0.6
0.7
LV thickness/ext rad.
4 8 12 16
Age [weeks]
*
*
0
50
100
150
Caudal artery systolic BP [mmHg]
4 8Age [weeks]
Control
Low Protein

Animal weights
0
2
4
6
8
Birthweight [g]
4 8 12 16
Age [weeks]
* * *
0
0.25
0.5
0.75
1
Weight at death [kg]
4 8 12 16
Age [weeks]
*
Control
Low Protein

Aortic Dimensions
0.0
0.5
1.0
1.5
2.0
4 8 12 16
Age [weeks]
*
*
Wall
cross
sect
ional are
a [
mm
2]
Control
Low Protein

Aortic stiffness
0
250
500
750
1000
4 8 12 16
Age [weeks]
Ein
c at
= 1
.3 [k
Pa
]
*
*
Control
Low Protein

Aortic elastin & collagen
0
20
40
60
80
Collagen [%DW]
4 8 12 16
Age [weeks]
0
20
40
60
80
Elastin [% DW]
4 8 12 16
Age [weeks]
**
Control
Low Protein

Conclusions
• Reduced body weight, aortic dimensions, elastin content and increased BP or LV hypertrophy in 4 & 12 week LP animals is consistent with the hypothesis that protein deprivation in utero leads changes in vessel structure and composition.
• The elasticity differences in 4 and 12 week animals were consistent with the hypothesis. However the results from the 8 week animals are not.

Limitations
• Preliminary study, limited age range
• Lack of in vivo central pressure measurements.
• Applicability of rat model to human in utero growth retardation?

ProblemIs the reduction in aortic elastin content a cause or a consequence of hypertension?

2.5
3.0
3.5
4.0
4.5
5.0
Aortic stiffness (arbitrary units)
0.4 0.5 0.6 0.7 0.8 0.9 1
Max stretch (mm)
P<0.01
Skin stretch for 500 mbar. 60 children aged 10 -11y

Fingerprints and hypertension

Palmar angle: abc
a
c
b
Palmar angle

3 basic types of fingerprint pattern
From: Holt S. Quantitative genetics of fingerprint patterns. Br. Med. Bull. 1961; 17:247

0 1-2 3-5135
140
145
150
No. of whorls on right hand
>43
ATD angle (°)
Sy
sto
lic B
P
Fingerprint results
40-42
≤ 39

Godfrey et al. BMJ 307, 405-409 (1993)
Fingerprint Summary
• Blood pressure in middle age is strongly correlated with number of finger whorls
• Inversely correlated with palmar angle

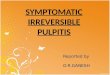
Case Sex Age Occupation Findings
1 F 101 Laundress Cardiac hypertrophy and degeneration. Severe generalized arteriosclerosis
2 F 101 University professor
Bronchopneumonia, influenza, cardiac hypertrophy, coronary sclerosis
3 M 102 Rabbi Cardiac hypertrophy, fibrosis, generalized arteriosclerosis
4 M 102 Restaurant owner
Cardiac hypertrophy, fibrosis, coronary–valvular sclerosis
5 M 106 Shepherd Bronchopneumonia, cardiac hypertrophy, fibrosis, fibrinous pericarditis, coronary sclerosis
Death By Old Age
Robert L. Exp Gerontol 1999, 34:491-501.
2 F 101 University professor
Bronchopneumonia, influenza, cardiac hypertrophy, coronary sclerosis
3 M 102 Rabbi Cardiac hypertrophy, fibrosis, generalized arteriosclerosis
4 M 102 Restaurant owner
Cardiac hypertrophy, fibrosis, coronary–valvular sclerosis