Embed Size (px)
Citation preview

International Urology and Nephrology 14 (1), pp. 23--28 (1982)
Fibrin Pyelotomy for the Removal of Multiple Renal Calculi
Z. NAG:C, D. FRANG, F. GSTZ, J. HOBLER
Department of Urology, University Medical School, P6cs, Hungary
(Received November 28, 1980)
The method of fibrin pyelotomy used in the surgery for multiple renal calculi is described. The indications, field of application and the results of the method are discussed. Its use on a larger scale is advocated. It is pointed out that complete re- moval o f the stones in case of multiple calculi is facilitated by this procedure.
Every surgeon undertaking an extraction of calculi from the renal pelvis will know the relief at having been able to wash out the small calculus in question in a fibrin-embedded state. The method developed by J. E. Dees in 1943 for the removal of multiple calculi puts this favourable constellation into practice [I ]. It basically consists in the production of an elastic fibrin polymer by intrapelvic interaction of fibrinogen and thrombin. The material thus obtained is plastic, but at the same time elastic, attaching the calculi of various sizes and uneven surfaces very firmly. The method escaped attention at first, but it has been repeatedly employed from the 'sixties onward [2, 3].
Method
The technique requires two components (a, b). Component a: 60 ml blood is withdrawn under aseptic conditions, and 30 ml
platelet-rich plasma obtained by centrifugation is brought together at room temperature with 1 g human fibrinogen dispensed in this dose. By gentle agita- tion of the flask, dissolution of the fibrinogen in the plasma is accelerated. From the material thus prepared 10 to 15 ml are used.
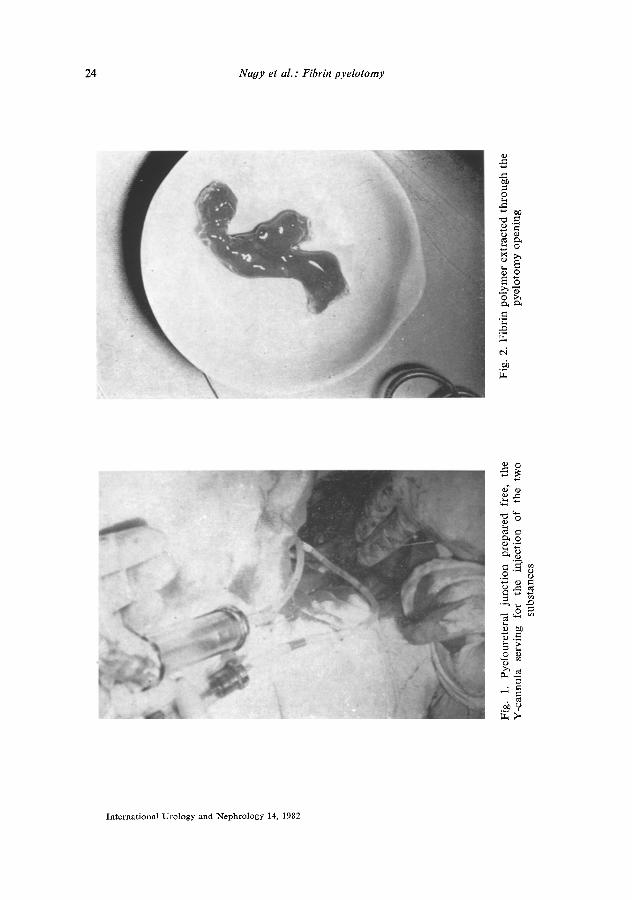
Component b: 30 NIH thrombin in 5 ml/40 M CaC12. After exposure of the pyeloureteral junction and soft clamping of the ureter
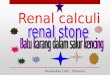
(Fig. 1) the renal pelvis is punctured and the urine is sucked off from the pelvic system. Subsequently, the two components are injected simultaneously into the pelvis. Allowing 5 minutes for the formation of the fibrin polymer, pyelotomy is performed through which the calculi embedded in the elastic polymer thus formed are removed (Fig. 2).
International Urology and Nephrology 14, 1982
24 Nagy et al. : Fibrin pyelotomy
o
0
o 0
0 >~
ei
+~
0 o
~.~
2 ~
In terna t ional Uro logy and Nephrology 14, 1982
Nagy et al. : Fibrin pyelotomy 25
0 . . ,
o : - ~
..~ 0 ~ Z
o
0
.~ '~0
a=
0 5 ~ o - ~
~ o~ o~
~ o
.~
International Urology and Nephrology 14, 1982

26 Naqy et al. : Fibrin pyelotomy
FieM of indication
1. Multiple calculi in the pelvic system. 2. A solitary "migrating" calculus in the dilated pelvic system.
Correct indication is essential, since in case of a narrow calyceal neck, when the calculus or calculi occupying the dilated calyx exceed the diameter of the neck in size, the procedure is doomed to failure. Accurate localization of the calculi requires preoperative radiograms in the necessary oblique positions.
Material
The technique was applied in 8 cases. Complete removal of the calculi was achieved in 6 cases. In two cases, with a calyceal calculus in each, nephrotomy had to be performed for the extraction of the calculus, owing to narrowness of the calyceal neck.
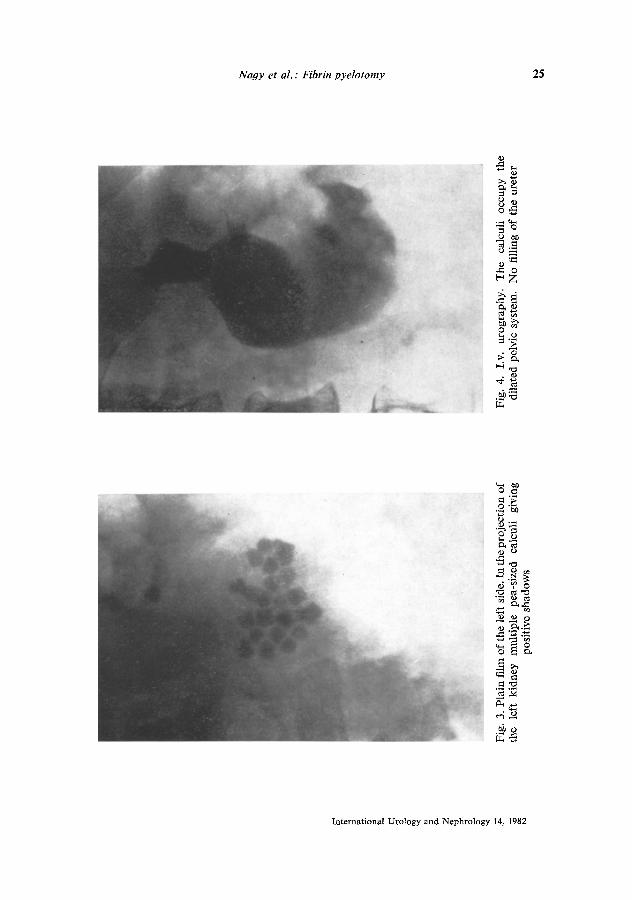
An illustrative case history is presented below. In Sz. J., a male aged 61, the presence of numerous pea-sized renal calculi
was confirmed by radiography (performed on 29 April 1978) which, on the evi- dence of i.v. urography, occupied the dilated pelvic system (Figs 3 and 4). Fibrino- pyelotomy and pelvic repair according to Hynes-Anderson were performed. The postoperative plain film showed no positive shadow indicative of calculi (Fig. 5). The changes revealed by i.v. urography in the projection of the kidney were con- sistent with the results of the previous reconstructive surgery. Ureteral passage was free (Fig. 6).
Discussion
Complete removal of calculi is the precondition for the prevention of cal- culous recurrences. This is, however, difficult if the calculi are in a dilated pelvic system. Though the image-amplifying tube and other supplementary optic instru- ments are of invaluable aid, they leave us in numerous cases with unsolved tasks. Residual calculi, in association with urinary infection, set the stage for the forma- tion of staghorn calculi, necessitating reoperation in many cases. The present technique proposed by us at the Meeting of the Association of Hungarian Urol- ogists, June 1980, may greatly contribute to a complete elimination of the cal- culi, if the indications are properly observed. Our observations since this meeting have shown that the method may be used also in marginal or marginopolar sur- gery for staghorn calculi if also a calculous matrix or a core for the accretion of further calculous masses is found in individual dilated calyces. In that case the material used molds the matrix or the minute calculi into a single mass and per- mits total extraction.
International Urology and Ncphrology 14, 1982

Nagy et al. : Fibrin pyelotomy 27
; ; o ~ . _ o
" " 0 " ~
.~- ~
O Z
~ . ~
._~ ~ ~7
~ ' ~ �9 o
International Urology and Ncphrology 14, 1982

28 Nagy et al. : Fibrin pyelotomy
References
1. Dees, J. E.: J. UroL, 36, 167 (1943); cit.: Burchardt, P., Reinecke, F.: Method and clini- cal use of fibrin pyelotomy. International Symposium on Urolithiasis Research, Davos, Switzerland, March 29=April 1, 1976. Urolithiasis Research. Plenum Press, New York 1976, p. 541.
2. Burchardt, P., Klosterhalfen, H. : Klinische Erfahrungen mit der Fibrinpyelotomie. Uro- loge A, 11, 221 (1972).
3. Cranidis, A., Terhorst, B.: 4th Congress of the European Association of Urology, Athens, 28-31 May 1980. Abstracts, p. 145.
4. Nagy, Z., Frang, D., G~Stz, F., Htibler, J.: Meeting of the Hungarian Association of Urology, Budapest, 16 June 1980.
International Urology and l'qephrology 14, 1982