-
8/8/2019 Final Immunology 6
1/20
Immunopathology
Diseases of immunity
The immune system is a defensive system whose primaryfunctions
are to protect against infectious organisms such as
bacteria, viruses, fungi and parasites and development of
cancer.
Immunity is the results of nonspecific or nature (innate or
native)
and acquired (adaptive or specific).
I-Innate or natural immunity (Nonspecific immunity)
It considers the first line of defense mechanisms; are not
specific to antigen and lack memory.
It depends on individual species variation in susceptibility
to
infection, for example horse and equine are resistant to
infection
with canine distemper virus, a highly pathogenic agent to the
dog.
Moreover, neutrophils and macrophages beside skin, mucous
membranes, and mucus covers respiratory epithelium, saliva
and
gastric acid play an immportant role in nature immunity.
Natural
antibodies, interferons and complement system are involved also
in
the natural immunity.
II-Acquired immunity (Specific immunity)
Adaptive immunity in general consists of cell mediate
immunity (mediated by T lymphocytes) against intracellular
pathogens and humoral immunity (mediated by B lymphocytes)
against extracellular pathogens and toxin. The acquired
immunity
characterized by; (1) previous exposure to the antigen, (2)
highly
specific for certain antigens, (3) and memory.
109
-
8/8/2019 Final Immunology 6
2/20
Immunopathology
Cells involved in acquired immunity
1-Antigen-presenting cells (APCs)
Macrophages, Langerhans cells of skin and follicular dendritic
cells
found in the germinal centers of lymph nodes and spleen are
considered antigen presenting cell. The APCs phagocylize the
antigens and degrade into antigenic peptides. The APCs then
connected the antigenic peptides to major histocompatibility
complex (MHC) and present the complex on the surface of the
cell
in a form that can be recognized by other cells.
2-T-lymphocytes are another important class of cells
involved
in the acquired immune response.
The most important subset of T-lymphocytes is the helper T
cells, which characterized by presence of CD4 molecules on
their
surface. Those cells secrete a number of chemical substances,
known
as cytokines that regulate the function of the immune
system.
Another subset of T-cells are the cytolytic (cytotoxic) T
lymphocytes which have CD8 molecules on their surface,
cytotoxic
cells are responsible for killing virus infected cells and
cells
expressing foreign antigens on their surfaces.
Suppressor T cells are another subset that secretes
cytokines
suppresses the activity of B lymphocytes and cytotoxic T
cells.
Adhesion molecules involved in the immune system
Adhesion molecules are membrane-bound proteins that allow
one
cell to interact with another. Adhesion molecules play an
important role
110
-
8/8/2019 Final Immunology 6
3/20
Immunopathology
in directed of the immune cells to a particular site to perform
some
function. Three groups of adhesion molecules are recognized;
(1)
immunoglobulin superfamily, (2) integrin and (3) selectin
family
Acquired immunity classified to
1-Humoral immunity
The humoral immunity, is mediated by B lymphocytes against
intracellular pathogens, involves circulating antibodies and can
passively
transfer with serum. Antibodies are glycoprotein substance
present in the
body fluid that combat diseases and formed as a result of
exposure to
foreign antigens. Antigens are substances that are foreign to
the host.
Haptens are simple chemicals that can induce antibodies when
coupled to
carrier protein.
2-Cell-mediated immunity
It is a form of acquired immunity, mediated by T
lymphocytesagainst extracellular pathogens and toxin, requires a
stimulus, highly
specific and has a memory. It depends on immune cells not
antibodies, so it cannot be transferred by serum. Cell
mediated
immunity responsible for resistance and reaction associated
with
granulomatous diseases, simple bacteria, some protozoa and
metazoan parasites. Also it involved in the mechanism of
graft
rejection, certain viral diseases and destruction of
neoplasm.
The cell mediated immune response resulted from interaction
of
T lymphocytes and antigen presenting cells (APCs) as
macrophages.
Antigens is processed by APCs and presented to T lymphocytes
by
macrophages. Sensitize T lymphocytes release chemokines
which
111
-
8/8/2019 Final Immunology 6
4/20
Immunopathology
call additional macrophages (principle effector cells) that
accumulate
at reaction site.
Microscopically, the delayed reaction of cell mediates
immunity is characterized by:
1. Proliferation of large lymphocytes in the paracortical
regions
of lymph nodes. The lymphocytes may release chemokines to
attract
macrophages or destroying the antigens with lysis of cells
through
release of cytoplasmic granules or enhance apoptosis (cytotoxic
or
cytolytic cells).
2. Macrophages, epithelioid cells, multi-nucleated giant
cells,
and small numbers of neutrophils.
Disorders of the immune system
The diseases of immune system are broadly classified into
1- Autoimmune diseases
2-Immunodeficiency diseases
3- Hypersensitivity
4- Possible immune disorders classical example of this group
being amyloidosis.
1-Autoimmune diseases
It is defined as a specific immune response to self
antigens. Autoimmune diseases are occurs due to loss of
immunologic tolerance to self tissues or cellular antigens
and
112
-
8/8/2019 Final Immunology 6
5/20
Immunopathology
characterized by abnormal or excessive activity of self
reactive
immune effector cells.
The etiology of most autoimmune diseases is still elusive
as they are often multifactorial and have a genetic and
environmental component.
Autoimmune diseases can be organ specific, localized or
systemic.
Several autoimmune diseases are recorded in animals such
as Lupus erythematosus, rheumatoid arthritis
2-Immunodeficiency syndromes
Immunodeficiency disease occurs when there is a failure of
the
immune system to protect the host from infectious organisms
or
cancer.
They consider a number of genetic and congenital acquired
defects in innate and acquired immune system render
individuals
more susceptible to infectious agents and neoplasm.
An immunodeficiency syndrome that results of a congenital or
genetic defect in a component of the immune system is called
a
primary immunodeficiency, but the one result from complication
of
infections, malnutrition, or aging or a side effect of
immunosuppressant, irradiation or chemotherapy of cancer is
called
secondary immunodeficiency diseases.
I-Primary immunodeficiency
113
-
8/8/2019 Final Immunology 6
6/20
Immunopathology
1. Neutrophils disorders
A-Canine cyclic neutropenia: it is characterized by cyclic
neutropenia every 8-12 days due to defect in bon marrow stem
cell
maturation. The animals are more susceptible to bacterial
infection
of digestive and respiratory system.
B-Chediak-Higashi disease (CHD)
It is characterized by partial albinism and increase
susceptibility
to bacterial infection and a tendency to hemorrhage. The
disorders is
characterized by presence of large granules in the cytoplasm
of
neutrophils, macrophages, NK cells and melanocytes.
2. Adhesion molecules deficiencies
Leukocyte adhesion deficiency syndromes are characterized by
recurrent bacterial and fungal infections.
3. Complement deficiencies
Animal with C3 and C5 deficiencies is unable to opsonize and
destroy bacterial organisms.
4. B-lymphocytes deficiencies
Agammagloblinemia and hypogammaglobulinemia may resultfrom
defective synthesis, increase catabolism or excessive loss of
immunoglobulines.
5. T-lymphocytes deficiencies
114
-
8/8/2019 Final Immunology 6
7/20
Immunopathology
Deficiencies of T-lymphocytes generally result in more
serious
susceptibility to infection than defects involving B-cells,
owing to
the essential contribution of T cells to normal B-cell
function.
II. Secondary immunodeficiency disorders
1-Failure of passive transfer of maternal immunoglobulin
It is the one of the most common acquired forms of
immunodeficiency in veterinary medicine due to failure of animal
to
consume colostrum.
2-Virus induced immunosuppression
The virus induce suppression through direct effect on the cell
of
immune system especially macrophages and lymphocytes.
Immunosuppression usually accompanies diseases as canine
distemper,
hog cholera, bovine virus diarrhea and others.
III-Hypersensitivity (Allergy)
Definition:
A hypersensitivity is defined as the altered reactivity to a
specific antigen that results in pathologic reaction when
exposure toof a sensitized host to that specific antigen. Also
hypersensitivity is
defined as an abnormal, exaggerated immune reaction to a
foreign
agent (antigen), with resulting injury to host tissues.
115
-
8/8/2019 Final Immunology 6
8/20
Immunopathology
Antigens which produce such a harmful effect
calledallergens.
They may be bacterial, nonbacterial or even simple chemical
substance.
There are four different mechanisms of hypersensitivity
(TypeI,
II, III and IV). All forms, except type IV, are mediated by
antibodies. Type IV is mediated by T lymphocytes and
macrophages. All forms need initial exposure (sensitizing or
preparatory dose) followed by second dose of the same antigen
after
1 or more weeks (challenge or eliciting dose). An immediate
violent
response may be seen within few seconds or minutes
(immediate
hypersensitivity). On the other hand, the reaction to the
challenge
dose may appear several hours or days or even months later
(delayed
hypersensitivity).
A. Immediate hypersensitivity
It is characterized by an allergic reaction that occurs
immediately following contact with the antigen (challenge
dose).
Histamine is a mediator in immediate hypersensitivity for
the
following reasons.
1-Histamine injection reproduces the clinical manifestation
of
immediate hypersensitivity.
2-Histamine is higher in tissue severely affected in
hypersensitivity as liver in dog.
3-Antihistamine injection decreases the intensity of the
anaphylactic shock.
116
-
8/8/2019 Final Immunology 6
9/20
Immunopathology
4-Histamine can be demonstrated in blood during shock except
in rabbit because its platelets adhere to endothelium and
disappear
from the circulation during shock.
1. Type I (Cytotropic anaphylactic)
It is an inflammatory reaction results from IgE mediated
immune response directs against environmental antigen
(allergens)
and parasite antigen. The basic pathogenesis
includessensitization
phase and an effector phase.The sensitization phase develops
when IgE become fixed on specific Fce receptors on surface of
mast
cells and basophils. The host is now sensitized, and either
through a
second exposure or prolonged exposure, combination of antigen
with
fixed antibodies to mast cells and basophils, leading to release
of
vasoactive (Histamine, leukotriene and prostaglandine D2),
chemotactic(Eosinophil chemotactic factor and inflammatory
factor
of anaphylaxis) and spasmogenic substances (Histamine and
prostaglandins) that act on vessels and smooth muscle, results
in
effector phase. Complement is not necessary.
Cytotropic anaphylactic may be localized or systemic
(anaphylactic shock).
A. Systemic or Anaphylactic shock
Anaphylaxis refers to an acute systemic hypersensitivity
reaction to an antigen that is mediated by IgE and involves mast
cell
activation, resulting in a shock like state often involving
multiple
organs. Release of vasoactive amine into the circulation
causes
smooth muscle contraction, generalized vasodilation, and
increase
117
-
8/8/2019 Final Immunology 6
10/20
Immunopathology
permeability.The clinical signs and pathology are varying by
species. This variation reflects differences in distribution of
the mast
cells.The primary target tissues are blood vessels and
smooth
muscle. It can be demonstrated experimentally in guinea pig,
rabbit,
dog and cattle, these species react differently as follows.
1- Guinea pig: It dies within 10 minutes due to spasm of
bronchial muscles (Mast cells concentrated around bronchioles
in
guinea pig).
2- Dog shows epileptiform fits, coma and death within 1-2
hours of restlessness, diarrhea and vomiting due to pooling of
blood
in the liver and mesenteries due to contraction of venous
passages,
especially the hepatic vein.
3- Cattle show cutaneous edema, particularly around the
eyes,
valva and dyspnea.
4- Rabbit shows constriction of pulmonary artery and
dilatation
of the right heart.
5- Rat shows increase vascular permeability and intestinal
hemorrhage.
The lesions of anaphylactic shock can be summarized as
Spasm of the smooth muscles of blood vessels and
bronchioles.
Damaged endothelium of blood vessels with increase
permeability.
Damaged connective tissue fibers
118
-
8/8/2019 Final Immunology 6
11/20
Immunopathology
B- Local anaphylaxis or Atopy
In local types the clinical signs and pathological lesions
are
restricted to a specific tissue or organ. Atopy means
genetically
controlled predisposition to develop localized anaphylactic
reaction
to inhaled or ingested allergens. Specific diseases include
urticaria
and hay fever.Before we closed the discussion of type 1
hypersensitivity, it should be noticed that there are several
beneficial
function for type I as antigen elimination and play a role
in
resistance to parasites
2. Type II Hypersensitivity (Cytotoxic)
119
-
8/8/2019 Final Immunology 6
12/20
Immunopathology
In the original Gill and Combs classification, the type II
hypersensitivity was define as antibody mediated cytotoxic
hypersensitivity. It is characterized by an antigen-antibody
reaction
on the surface of a host cell that causes the destruction of
such cell.
The antigen involved may be endogenous (normal cell or
tissue
protein) to the cell or exogenous (drugs or microbial protein)
and
attached to the cell surface. Specific antibody, commonly IgG
and
IgM, is produced against the antigen and interact with it on the
cell
surface. This cell interaction causes cell damage in several
ways.
A- Complement dependent reactions
There are two mechanisms by which antibody and complement
mediate type II hypersensitivity.
1-Antibody reacts with the antigen present on the surface of
the
cells causing activation of the complement system and resulting
in
formation of membrane attack complex, resulting cell lysis.
2- The cells become susceptible to phagocytosis
(opsonization)
by fixation of antibody or C3b fragment to the cell surface.
B- Antibody-dependent cell-mediated cytotoxicity
It does not involve fixation of the complement but instead
requires the cooperation of leukocytes. The target cell, coated
with
antibody, are killed by a variety of non-sensitized cells
(monocytes,
neutrophils, eosinophils and NK cells) that have Fc receptors,
the
later bind to the target by their receptors for the Fc fragment
of IgG
and cell lysis proceeds without phagocytosis.
120
-
8/8/2019 Final Immunology 6
13/20
Immunopathology
Clinically type II hypersensitivity occurs in the
transfusion
reaction, erythroblastosis fetalis, equine infectious
anemia,
autoimmune hemolytic anemia and certain drug reaction.
3-Type III hypersensitivity (Aggregate)
Type III hypersensitivity is designated as immune complex
hypersensitivity. Interaction of antigen and antibody may result
in
the formation of immune complexes, either locally or
systematically,
which deposit at various sites in the body and activate
complement
causing acute inflammation and injury. In type III
hypersensitivity,
the cells or tissues are destroyed not because the antibody
become
directed to that tissue, but rather because the immune
complexes
either stuck to that cells or are deposited in that tissue.
Pathogenesis
Immune complex are capable of producing a wide variety of
acute inflammation through:
1-Interact withcomplement system to generate C3a and C5a
which stimulate the release of vasoactive amines and
chemotactic
factors.
2-Stimulate macrophages to release cytokines that are very
important during inflammation.
Types of immune complex injury
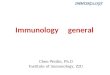
1- Arthus phenomenon (Local form)
121
-
8/8/2019 Final Immunology 6
14/20
Immunopathology
It is immediate hypersensitivity characterized by
vasculitis.
Pathogenesis: The
subcutaneously injected
antigen into
hyperimmunized animal
diffuses away from the site
of injection into the vessel
walls and formed immune
complex beneath the
endothelial cells, when this
complex activate the
complement system, C3a
and C5a are produced and
neutrophils are attracted to
the site of injection.
Lesions:
Massive aggregation of neutrophils within the blood vessels
and in their wall.
Fibrinoid necrosis in the wall of the blood vessel.
Hemorrhage and edema.
Thrombosis
Serofibrinous inflammation.
122
-
8/8/2019 Final Immunology 6
15/20
Immunopathology
2-Serum sickness (General type III immediate
hypersensitivity)
It may be acute or chronic
A-Acute serum sickness: It develops without previous
sensitization to the responsible antigen. Injection of a large
amount
of antigen into the blood stream, as horse serum allows a part
of
antigen to circulate in blood after development of the
specific
antibody, thus antigen bind with antibody and form
antigen-antibody
complex. The large complexes are removed from the blood by
phagocytic cells. The small complex is deposited in the vessels
with
the complement. Release chemotactic factors from complement
invite neutrohpilic infiltrations which lead to necrotizing
vasculitis.
Many vessels are affected but mostly the major arteries,
endocardium and renal glomeruli.
B-Chronic serum sickness: It results of repeated
interavenous
exposure to antigen which results in immune complex formation
in
blood. It is important in pathogenesis of many diseases-in man
and
animals. It results in deposition of immune complexes on the
epithelial side of basement membrane of glomeruli. It may or
may
not contain complement which leads to immune complex
glomerulonephritis(GBM-nephritis). Deposition of this complex
in
vessel walls leads to vasculitis (similar to arthus
phenomenon).
B. Delayed hypersensitivity
(Type IV hypersensitivity)
123
-
8/8/2019 Final Immunology 6
16/20
Immunopathology
Type IV hypersensitivity is also known as cell mediated
hypersensitivity because it is the results of interaction of
T
lymphocytes and the specific antigen to which they have been
sensitized. The resulting immune response is mediated either
by
direct cytotoxicity by CD8 T lymphocytes or by the release
of
soluble cytokines from CD4 lymphocytes, which act through
mediator cells (macrophages) to produce chronic inflammatory
reaction. Type IV hypersensitivity reaction take more than 12
hours
to develop (24-28 hours needed to develop because it depend
in
sensitized lymphocytes) and involve cell mediate immune
reaction
rather than humoral one, so it cannot be transferred by serum
but can
transferred by T cells- The best example for Type IV
hypersensitivity is tuberculin reaction.
Types of delayed hypersensitivity
1-Infectious hypersensitivity
It is the prototypical types of delayed hypersensitivity as
occurs
in localized tuberculin response. Moreover, it occurs in
facultative
intracellular organisms, e.g. mycobacteria and fungi. It is the
most
important form of type IV hypersensitivity. The best example
is
Koch phenomenon.
Koch phenomenon is the reaction of the normal and
tuberculous guinea pigs to injected tubercle bacilli. The normal
one
develops hard nodules at the site of injection within 2 weeks.
The
nodule ulcerated and the animals die from generalized
tuberculosis.
124
-
8/8/2019 Final Immunology 6
17/20
Immunopathology
The tuberculous guinea pig develops inflammatory edema and
necrosis at the site of injection which heal later.
Microscopically, granulomatous reaction is seen
(Macrophages, lymphocytes and epithelioid cells)
2-Allergic contact dermatitis
Contact dermatitis is characterized by eczematous reaction
at
the point of contact with an allergen.
Cause:
Contact with agents such- as nickel, dichromate compounds,
dyes, formaldehyde and synthetic fibers. A contact dermatitis
has
two stages.
A-Sensitization: It takes 10-14 days and involved
presentation
of the antigen by Langerhans cells and producing a
populationofCD4 T cells.
B-Ellcitation: During this phase degranulation of mast cells
and cytokines release from other cells are potent inducer of
endothelial adhesion molecules and migration of mononuclear
cells
toward the antigen.
Microscopically, the dermis infiltrated with mononuclear
cells
beside hyperemia and edema of the dermis.
Table (4): Differences between immediate and delayed
hypersensitivities
125
-
8/8/2019 Final Immunology 6
18/20
Immunopathology
Immediate Delayed
-Immediate onset (up to 12 hours). -Delayed onset (after 12
hours).
-Circulating antibodies (humoral). -Cellular immunity (no
antibodies).
-Passive transfer by serum. -Passive transfer by cells.
-Affect smooth muscle, blood
vessels and collagen.
-Affect any tissue.
-Not affected by the rout of
administration.
- Almost through the skin.
-Types include: Type I,II and III. -Types include: Type IV.
3-Transplant rejection
The frequency of tissue transplantation has increased
dramatically since 1970. Immunologic reactivity against
transplanted
cells may be directed against many antigens on the surface
membrane of cells such as
1-Antigens on erythrocytes
2-Antigens on surface of nucleated cells as MHC class I, II and
III.
Mechanism of transplant rejection
1- Direct pathway of graft rejection is mediated by CD8
cytotoxic
T lymphocytes which cause cell injury and tissue damage
126
-
8/8/2019 Final Immunology 6
19/20
Immunopathology
2-Indirect pathway of graft rejection: It mediated by
recipient's T
lymphocytes that recognize antigen on the graft presented by
the antigen presenting cells of the recipient. It is depend on
the
activation of CD4 lymphocytes and elaboration of cytokines
and development of delayed hypersensitivity.
Table showing mechanisms of immunologic tissue injury
Type Mechanisms Examples
Type I
(Anaphylactic,
atopic)
Humoral Abs of IgE type resulted
in basophils/mast cell sensitize
and release of anaphylactic
Systemic anaphylaxis
Local anaphylaxis such as hay
fever, bronchial asthma
127
-
8/8/2019 Final Immunology 6
20/20
Immunopathology
mediators
Type II
Cytotoxic
i-Cytotoxic auto and iso-
antibodies to blood cells
ii-Cytotoxic Abs to tissue
components
iii-Ab dependent cell mediated
cytotoxicity (ADCC)
i. Autoimmune hemolytic
anemia, transfusion reaction
ii. Myasthenia gravis
iii. Tumor cells and parasites
Type III i. Local (|Arthus
reaction) Ag-Ab
complexes
ii. Systemic (circulating)
Ag-Ab complexes or
serum sickness
i. Injection of ATS
ii. Glomerulonephritis
Type IV
(Cell mediated)
i. Classical delayed hyper
sensitivity mediated by CD4 T
cell
ii. T cell mediated cytotoxicity by
CD8 T cells
i-Tuberculin reaction
ii-Virus infected cells,
transplant rejection
128