Upload
dreamyiris
View
133
Download
3
Tags:
Embed Size (px)
Citation preview
Medical Officer Handbook for Neurosurgery
Department of Neurosurgery, Singapore General Hospital National Neuroscience Institute, Outram Campus Draft 2010
SY Lee S K Dinesh J Thomas June Goh1
TK TanContents 1. Department Guidelines 1.1.1. Teaching programme 1.1.2. Weekly schedule 1. Neurophysiology 2. Neuroanatomy 2.1. Brain anatomy 2.2. Ventricular system2.3.
Cerebral vasculature
3. Neuroradiology 3.1. CT, MRI , Angiography3.2.
Neuroradiology scans
4. Neurological Examination 4.1. Mini Mental State examination 5. Relevant Neurology 5.1. Headache5.2. 5.3. 5.4. 5.5. 5.6.
Hydrocepahalus Normal pressure hydrocephalus Status Epilepticus Herniations Brain death
6. Infections of the CNS 7. Spine7.1. 7.2. 7.3. 7.4. 8.
Low back pain Treatment options Tethered cord syndrome Asia spinal association chart
Tumors
2
8.1. 8.2. 8.3. 9. 10.
Primary tumors Cerebral metastases Radiation therapy
Neurophthalamology Surgical procedures and Operations 10.1. Admission guidelines (Elective cases) 10.2. Craniotomy 10.3. Frameless Stereotactic surgery 10.4. External Ventricular Drain(EVD) 10.5. Ventriculo-peritoneal shunt(V-P shunt) 10.6. Omaya reservoir 10.7. Lumbar puncture 10.8. Lumbar drain 10.9. Transsphenoidal Pituitary Clinical Pathway 10.10. Stereotactic Radiosurgery Neurosurgical Trauma Management 11.1.1. Protocol for Management of Severe Head Injuries 11.1.2. Severe Head Injury protocol checklist 11.1.3. Barbiturate coma protocol 11.1.4. Commonly asked questions in head injury 11.1.5. Guidelines for the management of head injuries sustained after a fall by inpatients in SGH.
11.
12. SAH and aneurysms 12.1. Definition and grading of SAH 12.2. Management of Cerebral aneurysms 12.3. NICU SAH protocol 12.4. NICU SAH checklist13.
Artriovenous malformations
14. Intracranial haemorrhage 15. Endocrinology15.1.1. 15.1.2. 15.1.3. 15.2.
SIADH Cerebral salt wasting DI Fluids and Electrolytes
16. General ICU Care 16.1. Change of Tracheostomy 16.2. Central Line insertion 16.3. Inotropes3
16.4. 16.5. 16.6. 16.8. 16.9. 16.10.
Anaphylaxis Sedation Blood sugar control Oxygen therapy Eye Care Guidelines Deep Vein Thrombosis
16.7. Surgical Nutrition
16.11. Pulmonary Embolism 16.12. Advanced Monitoring 16.12.1. Cardio Q 16.12.2. Cerebral State Monitor 17. Neuropharmacology 17.1.1. Analgesia 17.1.2. Sedation 17.1.3. Antiepileptics 17.1.4. Antibiotics 17.1.5. Common Neurosurgery drugs 17.2. 17.3. Glossary Abbreviations
4
Department Guidelines Core curriculum for Medical Officers [Duration: 6 months] GENERAL OBJECTIVES: 1. To introduce the scope of neurosurgery to the medical officer by a combination of clinical exposure to neurologic disease, structured teaching, operating theatre experience, and academic/research projects. 2. To train the medical officer so that at the end of 6 months, he/she has achieved a certain level of competence and confidence in managing neurosurgical conditions. SPECIFIC OBJECTIVES: A. Clinical Skills 1. To be able to perform a competent neurological evaluation including pertinent details in history and neurological examination. 2. To understand and recognize the fundamentals of X-ray/CT/MRI/DSA imaging of the brain and spine, including normal appearances and common pathological lesions. B. Treatment / Management Abilities 1. Head trauma To diagnose and initiate management of the spectrum of mild, moderate and severe head injury. 2. Cerebrovascular disease To recognize and manage subarachnoid haemorrhage, intracerebral haematomas, and occlusive cerebrovascular disease, including investigations required, surgical decisions, treatment options and postoperative complications. 3. Neuro-oncology To understand the clinical features of primary and secondary CNS tumours, as well as treatment principles including types of investigations, indications for biopsy or resection, surgical techniques, and adjuvant therapy. 4. Spinal disease To evaluate, diagnose and manage acute spinal trauma, acute cord compression, degenerative spinal disease, neoplastic conditions of the spine and spinal dysraphism, including complications secondary to these conditions. 5. CNS infections To understand, recognize and manage brain abscesses, subdural empyema, shunt infections and wound infections. 6. Neuro-intensive care To manage a comatose neurosurgical patient in terms of ventilator support, ICP/CCP manipulation, fluid and caloric requirements, and infection control. C. Surgical Skills (to be taught and supervised) 1. Shunt tap / externalization For shunt infections or malfunction 2. Lumbar drain For CerebroSpinal Fluid (CSF) leak or control of ICP 3. Lumbar puncture 4. Central Venous Catheter insertion 5. Arterial line insertion
5
TEACHING PROGRAM Clinical / Surgical Experience Each medical officer will have exposure for 1 month in the following areas: 1. ICU 2. OT Structured Teaching 1. Weekly Journal Club presentations (Friday) Presentation of selected papers (classic and current).2.
Weekly Morbidity & Mortality Round (Friday) Presentation and discussion on surgical morbidities and mortalities for audit, ensure good surgical practice, for learning and the prevention of mistakes from recurring. Weekly Rehab Rounds (Tuesday) Combined round with Neurosurgeon, physio/speech/occupational therapy, medical social worker, dietician and nurses, etc.
3.
4. Weekly NICU/Infectious Disease Rounds (Wednesday) Presentation and discussion with anesthetist and the ID physicians. 5. Weekly Neuro-Radiology Rounds (Friday) Combined conference with Neurologists and Radiologists on interesting clinical cases for management decisions.6.
Weekly Grand Surgical Ward Rounds (Wednesday) Teaching rounds to review all in-house neurosurgical patients. Monthly Combined Neuro-Radiology / Neuro-Pathology Conference (Thursday) Combined conference with Neurologists, Radiologists and Pathologists on tumors, muscle and nerve biopsies.
7.
Academics / Research Projects Every medical officer will be encouraged to participate in a research project in one of the above 6 areas under the supervision of the various program directors. At the end of 6 months, the aim is for at least one of the following: Presentation of an abstract at a local / regional meeting Publication of a case report / study in a local / international journal
6
WEEKLY SCHEDULE Monday: Tuesday: Wednesday Morning (0800hrs-0900hrs): Weekly Rehab Rounds Morning (0800hrs-0930hrs): NICU surgical Grand Ward Round Afternoon (1300hrs-1400hrs):SICU/ NICU/Infectious Disease Round Thursday Afternoon(1700hrs-1800hrs):Neuro-Radiology/Neuropathology Rounds Morning(0900-1000hrs): Weekly Neuro-Radiology Rounds Afternoon(1400-1700hrs): Weekly Journal Club presentations Weekly Morbidity & Mortality Round
Friday:
Grand Ward Round: All neurosurgical patients are presented for review and discussion especially the cases in Neuro ICU (NICU) and Neuro ICA (NICA). It is an important learning opportunity for the junior staff. The GWR stamps should be stamped in the case notes and the decision made during GWR should be documented down inside the case notes. Mortality and Morbidity Round: The list for the mortality round is found in the Medical Officers (MOs) room. The purpose is to present and discuss surgical morbidities and mortalities for audit, ensure good surgical practice, for learning and the prevention of mistakes from recurring. It is an excellent learning opportunity for the junior staff. If in doubt of the management, please consult the neurosurgeon in charge of the case before the presentation. Present the relevant information. Tick the result of the discussion e.g. expected or unavoidable. Rectify any amendments in the template before submitting to the department secretary. Journal Clubs: The list of journals to be presented will be released the month before. If not, consult the consultant regarding the journals to be presented. MOs should start to prepare their presentation the week before their turn. Read up around the tropic itself to get a good grasp of the paper. Provide a summary of the paper including the relevant tables and charts. Do not present large amount of confusing data. Rehabilitation Round: Tuesday (0830hrs-0930hrs) This is a combined round with the neurosurgeon, physio/speech/occupational therapy, medical social worker, dietician and nurses etc. MOs will present a short history followed by discussion on the patients rehab issues, home plans, discharge plans etc. Neuro-radiology/Neuropathology Conference: Friday (0900hrs-1000hrs) Interesting cases are identified by the neurosurgeon during the course of the week for discussion during the X-ray conference. Cases to be identified and communicated to neuroradiologist by every Wednesday. Once a month, on the last Friday, there will be a7
combined neuroradiology/neuropathology round. Pathology cases to be identified and communicated to the pathologist one week prior to meeting. NICU/Infectious Disease Round: Wednesday (1300hrs-1400hrs) NICU cases will be presented for discussion with the anesthetist and the ID physicians. MOs can consult the ID physician individually if there are any issues in the ward after the round. Ward Coverage 1. 2. 3. 4. 5. A. B. NICU NICA Ward 52B Room 1, 2, 3, 4, 5 Over flow patients Operating Theatre Medical Officer (OT MO) (MO should have a roster among themselves to be inside OT) NICU will be covered by a different anesthetist on call in NICU every week. If in doubt always consult the NICU anesthetist on any procedures. NICU and NICA MOs cross cover each other for post call. NICU and NICA MOs should be aware and may need to manage the ICU and ICA beds requirement. There are 8 beds in the NICU (NES is sharing with Neuro Medicine). NICU MOs will need to notify Neuro Medical Registrar if NES needs to take over their beds. An afternoon round is usually done around 1600hrs in the NICU with the NICU MO, anesthetist and the on call MO to take over. C. Weekends, 3 MOs are requested to be present to do the rounds and to finish the changes before leaving. (Sat: at 1230hrs, Sun: after all changes are done).
D. One MO should be in the Ward at all times to cover the NICU patients. Procedures 1. All procedures (arterial line, lumbar puncture, central line, lumbar drain etc.) should be documented. Signed consent is required (except in cases of emergency when patient unconscious/ incompetent and no N.O.K. availabledocument your attempt to contact them). 2. CXR should be ordered after all ICU nasogastric tube insertions to document the tip is inside the gastric fundus. 3. If you have not performed a procedure before, please make sure you log 3 supervised procedures before getting clearance from the HOD to perform the procedures without supervision.
8
Neurophysiology Monro Kellie Model In a non-expansile, non-contractable (fixed), freely communicating space the pressure of the fluid contents is everywhere equal and directly proportional to the fluid volume. Intracranial pressure results from contributions from intracranial fluid compartments: 1. brain tissue (more than 80% fluid) 2. intra-arterial blood 3. cerebrospinal fluid (CSF). In the Monro-Kellie model total intracranial pressure is divided into a contribution from each of the 3 intracranial volumes: brain parenchyma, cerebrospinal fluid CSF, and cerebral arteries. The contribution of each compartment to the pressure is equal to the ratio of each compartment to the whole intracranial volume. As long as total intracranial volume stays the same the intracranial pressure remains the same. If the volume of one compartment increases or decreases the volume of one or both other compartment must decrease or increase in order for the total volume (and therefore, ICP) to remain the same. If the volume of any compartment is decreased while that of the other two volumes remains the same the total intracranial pressure must go down. The Monro Kellie model is the conceptual basis for current physical intracranial pressure management strategies and protocols. Cerebral perfusion pressure (CPP) The pressure the blood is under as it enters the cerebral arteries. This pressure is necessary to keep oxygenated blood from reaching the brain cells.Cerebral perfusion pressure (CPP) = MAP [1/3(systolic pressure+2xdiastolic pressure)] ICP
Two major concepts underlie CPP/ICP resuscitation: the first is that elevated intracranial pressure decreases cerebral perfusion according to the equation CPP = MAP - ICP where "CPP" is "cerebral perfusion pressure", "MAP" = mean arterial pressure, ICP = intracranial pressure). Second, that there is a normal range for cerebral perfusion pressure and a threshold pressure at which cerebral perfusion is so low that cellular injury results. In management of increased intracranial pressure, an effort is made to maintain the ICP below 20 mmHg and the CPP above 60mmHg. Diuresis to decrease ICP should be avoided if there is any circulatory compromise either hypo or hyper-dynamic.
9
Intracranial Pressure The Monro Kellie hypothesis is the basis for reducing ICP by reducing the volume of: 1. brain and soft tissue, 2. intracranial circulating blood, 3. cerebrospinal fluid (CSF), or any combination of these. Soft tissue volume can be reduced by removal of tissue water with diuretics. Intravascular blood volume decreases when intracerebral blood vessels constrict in response to hyperventilation with alkalinization of the blood and CSF. The volume of the CSF compartment can be decreased directly by shunting and drainage. Monro Kellie Hypothesis (intracranial volume compartments)Compartment Parenchyma Blood Cerebrospinal fluid % 70 5 25 Volume reduction technique Diuresis Hyperventilation Drainage
Management of Raised Intracranial Pressure 1. Head position around 30 degrees: Simple head elevation can promote venous return from the head and reduce ICP. It should be noted that head elevated does lower the mean arterial pressure supplying the brain, but the 30 degrees angulation has been shown to offer the best compromise. Hyperventilation: Though very effective in reducing ICP through its cerebral vasoconstrictive effect, hyperventilation causes reduced cerebral blood flow (CBF). Only mild to moderate degree of hyperventilation is recommended. (pCO2 > 30mmHg). Hyperosmolar agents: Mannitol can be used to draw water out of the brain tissue by osmotic forces. This reduces brain tissue volume and ICP. These agents should generally be "weaned off" to prevent rebound cerebral edema Sedation and pain relief. Agitation and muscle tremors/spasms can artificially elevate ICP. CSF drainage with an external ventricular drain can lower the ICP. Evacuate the causative intracranial mass lesion, including hematoma or neoplasm.
2.
3.
4.
5. 6.
10
11
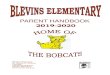
Ventricular System12
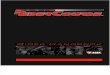
Circle of Willis (left) 1. Vertebral 2. Anterior Inferior Cerebellar 3. Basilar 4. Superior Cerebellar 5. Posterior Cerebral 6. Posterior Communicating 7. Middle Cerebral 8. Internal Carotid 9. Ophthalmic 10. Anterior Cerebral 11. Communicating 12. Hypothalamic 13. Anterior Choroidal
13
Neuroradiology Computed Tomography(CT) CT scan looks at the intracranial tissues with a display greyscale (degrees of black and white) based on the density characteristics of the tissue volume.14
Plain x-rays and CT scans are images resulting from differential penetration of xrays through tissues of different densities. As on a plain x-ray, denser objects on CT are lighter, and less dense objects darker. On a cranial CT, bone is white, air is black, and brain tissue is intermediate shades of gray. The Hounsfield unit (named after one of the inventors of CT) quantifies the gradations from black to white on a density gray scale. Individual tissue types, such as gray matter, white matter, and fat, each have their characteristic Hounsfield value, which can be used to determine density (and, therefore, type) of tissue. Fat is very low density, even less than CSF: on CT it is closest in density of all tissues to air. Within the parenchyma, the darker areas are less dense, thus the gray matter of gross specimens appear lighter on CT than the corresponding gross white matter. We can use the Hounsfield unit measurement on our computer screen to determine the tissue types. CT is fast and cheap and good for bony definition but exposures pts to radiation and thus not suitable for pregnant women but is less sensitive for soft tissue differentiation.
Magnetic Resonance Imaging (MRI) MRI is more sensitive than CT for detection of lesions affecting the CNS, particularly those of the spinal cord, cranial nerves and posterior fossa structures Diffusion MR a sequence that detects reduction of microscopic motion of water, is the most sensitive technique for detecting acute ischemic stroke, useful in encephalitis, abscesses and prion diseases. Guidelines for neuroimaging Condition Haemorrhage Acute parenchymal Subacute/Chronic SAH Aneurysm Ischemic Infarction Haemorrhagic infarct Carotid/Vertebral Dissection Vertebral basilar insufficiency Carotid stenosis Suspected mass lesion e.g. tumors, abscess Vascular malformation White matter disorders, dementia Demyelinating disease Condition Cranial neuropathy, meningeal disease Infection, abscesses Immunosuppression with focal findings Seizures 1st time Partial complex/ refractory Trauma acute Shear injury/Chronic haemorrhage Spine stenosis15
Recommended technique CT>MRI MRI CT/CTA, LPAngio Angio>CTA,MRA CT MRI>CT MRI/MRA CTA, MRI/MRA CTA>Doppler U/S,MRA MRI + contrast MRI +/- Angiography MRI MRI +/- contrast Recommended technique MRI + contrast CT as screen MRI with coronal T2W imaging CT non-contrast MRI CT,MRI
Low Back pain without neurodeficits With deficits Cervical spondylosis Infection, myelopathy AVM
CT, MRI after 4 weeks of conservative Mx MRI>CT MRI or CT myelography MRI + contrast MRI, myelography, angiography
Conventional Angiography Invasive procedure, only reserved for pts in whom small vessel detail is essential for diagnosis and for whom interventional therapies are planned
Neuroradiology scans
16
Extradural hematoma: lucid interval
Subdural hematoma: right hyperdense lesion, effacement of brain cortex (loss of gyri and sulci), left midline shift, compression of the ventricle
Acute hydrocephalus: CSF is produced continuously at a rate of approx 0.3ml/min, 20 ml/hr, 500 ml/day. Intraventricular volume CSF around 40ml. Total CSF volume at one time: 150 ml. Suddural Hygroma: preservation of the cerebral sulci and gyri. No need for treatment.
17
Subarachnoid Hemorrhage (SAH): blood in the basal cisterna
Right chronic subdural Hematoma (SDH): right hyperdense acute on chronic SDH, with fluid level, midline shift towards the left, compression of the right lateral ventricle and effacement of sulci and gyri.
18
Left Basal Ganglia Hematoma: mild midline shift to the right
Left thalamic bleed with intraventricular extension
Cerebellar hematoma
Angiogram: aneurysm in the left vertebral artery and spasm of basilar artery
19
Towne Carotid 1. Internal Carotid 2. External Carotid 3. Anterior Cerebral 4. Middle Cerebral
Lateral Carotid 1. Internal Carotid 2. External Carotid 3. Anterior Choroidal 4. Anterior Cerebral
Towne Vertebral 1. Vertebral 2. Posterior Inferior Cerebellar 3. Anterior Inferior Cerebellar 4. Basilar 5. Posterior Cerebral
20
Lateral Vertebral 1. Vertebral 2. Posterior Inferior Cerebellar 3. Basilar 4. Superior Cerebellar 5. Posterior Cerebral 6. Occipital 7. Posterior Temporal
Basic Neurological Examination Initial evaluation in the emergency setting. This is the basic information you will need before picking up the phone to consult the neurosurgical consultant. GCS initial, current (if different from initial). Time over which change occurred. Pupils symmetry/asymmetry, any change from initial findings. Limbs symmetry/asymmetry in GCS motor score, any change from initial findings. o If patient is obeying commands grade the power according to MRC grade BP, PR look for changes suggestive of a Cushings response (BP, HR). Complete Neurological Examination For all elective cases and as appropriate for urgent/ emergency admissions. The complete exam should be aimed for at least once, when the patient recovers sufficiently, during inpatient stay (if it was not done at admission). Cranial nerves I XII bilaterally 1. Olfactory occlude each nostril and ask the pt to gently sniff and correct identify a mild test stimulus. E.g. soap, toothpaste, coffee 2. Optic check visual acuity with or w/o correction with a Snellen chart. Map visual fields by confrontation in each quadrant in each eye, using a small white object moving form the peripheral towards the centre. Pts VF should be mapped against examiners. Formal perimetry and tangent screen exam may be necessary to document small defects. Refer Ophthalmologist if in doubt. Fundoscopy to view optic disc and note ratio. 3. 4, 6. Oculomotor, Abducens and - Direct and consensual papillary reaction to lightand convergence. Lid lag, droop, retraction. Range of movement of each eye. Left to right and then up and down. Document nystagmus if present. 5. Trigeminal Feel the masseter and temporalis when pt bites down and test jaw opening, protusion. Test sensation over entire face and document which division(Ophthalmic,VI- forehead; Maxillary,V2- cheek; Mandibular,V3-lower lip). Test Cornea(V1) with a small wisp of cotton for sensation. Test jaw jerk. 7. Facial Asymmetry of face at rest. Test eyebrow elevation, forehead wrinkling, eye closure, smiling, frowning, puffing of cheeks, whistle. Check if forehead is spared (in UMN lesions). Test for taste in anterior 2/3 of tongue( cotton bud soaked in 50% glucose). Test tear production from lacrimal glands (Schirmer test) . 8. Vestibulocochlear- Ability to hear tuning fork, finger rub, watch tick. Rinnes test(516Hz tuning fork on mastoid process{BC} then in front of ear{AC}, ask which is louder) and Webers test(516Hz tuning fork on vertex of head, ask which ear is louder). Otoscopy to examine tympanic membrane. Rinne test in deaf ear Webers test Conductive dearness Bone Conduction,BC>AC Deaf ear louder Sensorineural deafness Air Conduction,AC>BC Good ear- louder
21
9. 10. Glossopharyngeal and Vagus -Palate-uvula elevation with ahhh sensation in posterior pharynx, tonsils and posterior 1/3 taste sensation in tongue. Gag reflex on each side. Direct examination of vocal cords by laryngoscopy by ENT if necessary 11. Accessory check shoulder shrug(trapezius) and head rotation(SCM) to each side 12. Hypoglossal check bulk and power of tingue. Look for deviation form midline on protusion, fasciculations and atrophy. Tone, power, reflexes (deep tendon + plantar), sensation in all limbs Medical research council(MRC) scale 5 normal,4-submaximal power against resistance, 3 antigravity movement, 2- movement with gravity eliminated, 1- flicker of movement, 0- none Tone normal, decreased, increased spastic, lead pipe, cogwheel Reflexes C5-Biceps; C6-Supinator; C7-triceps,C8-finger;L3/4-knee;S1-ankle Sensation- light touch, pain, and temperature should be tested separately. Refer to Asia spine association chart and anatomy diagram for dermatomes (page) Cerebellar function assessment Rapid alternating movements (Dysdiadochokinesia) tapping one hand on the back of the other quickly; demonstrate to pt 1st. Finger nose test- look for past pointing (dysmetria), intention tremor Heel-shin test joint position sense, movements are worse when repeated with eyes closed Gait Rombergs, veering to side of lesion(cerebellar ataxia) Speech- slurring, disjointed rhythm with scanning speech Nystagmus multidirectional gaze-evoked in cerebellar lesions- nystagmus in the direction of gaze, occurring in more than one direction In patients with skull base fracture: assess for CSF leak (if not initially obvious, reassess when patient is able to sit up in temporal bone fracture assess hearing + facial nerve function. In trauma cases assess cervical spine clinically + radiologically. CT/MRI C-spine if necessary.
22
Mini mental examination Mental status exam is an important diagnostic tool used to evaluate a patient's orientation, concentration and memory (i.e. cognition). Although it is not imperative to perform a mini mental exam each time you evaluate a patient neurologically, a baseline score should be established when a patient is first examined. Serial exams may be performed if deficits in cognition are noted at a later date or discovered upon the initial examination. More in-depth neurocognitive tests may be necessary if deficits are discovered. The mini mental exam is scored out of a total of 30 points. A score of 24 or higher is considered within normal range, although specific deficits may be noted and investigated further. A score of below 24 is indicative of dementia. Performance of the mini mental examination.
Orientation. Date: Ask the patient to state the date. The patient achieves one point for each correct answer of the following: year, month, day, season and numerical date (a total of five points). Location: Ask the patient to state where they are. The patient achieves one point for address, town, country, hospital and ward (a total of five points) Registration. Ask the patient if you can test their memory. State the name of three unrelated items (dog, pencil, ball) and then ask the patient to repeat the three items. The patient gets one point for each item repeated, i.e. registered (a total of three points). Ask the patient to remember these items, because you will ask for the patient to repeat them again later in the examination. Attention and Calculation. Ask the patient to begin with 100 and count backwards by subtracting 7's. The patient receives 1 point for each correct answer with a maximum of five points. If the patient is unable to subtract, have them spell the word WORLD in reverse, getting 1 point for each correct letter. Recall. Ask the patient to repeat the three words that they were asked to remember.Score 0-3. Language. Naming: Show the patient a watch and then ask them to name the object shown to them. Repeat this question showing the patient a pen. Score 0-2. Repetition: Ask the patient to repeat the following sentence: "No ifs, ands, or buts." Score 0-1.
23
Three step command: Hand the patient a piece of paper and state the following command: "hold this piece of paper, fold the paper in half, place the paper on the table". One point for each correct movement, maximum of 3. Reading: On a blank sheet of paper write clearly the following: CLOSE YOUR EYES. Show this paper to the patient and ask them to read it to themselves and do what it says. Score 0-1. Writing: Give the patient a piece of paper and pen and ask the patient to write any sentence they would like. The sentence must contain a noun and a verb, yet correct punctuation is not required. Score 0-1. Copying: On a sheet of paper draw two intersecting pentagons and then ask the patient to copy these objects. Score 0-1. All ten angles must be present with appropriate intersection points. Ignore tremor. Consciousness. Estimate the patient's level of consciousness: alert, lethargic, obtunded, stuporous, or comatose. An alert patient is vigilantly attentive and keen. A lethargic patient is dull, sluggish and appears half asleep. An obtunded patient opens their eyes, responds slowly to questions, is somewhat confused, and has a decreased interest in their environment. A stuporous patient is near unconscious with apparent mental inactivity and reduced ability to respond to stimulation. Comatose patients are unconscious and unresponsive.
Add the up the total score and note the level of consciousness.
24
Relevant Neurology Headache Chronic recurring headache Vascular type : migraine Muscular : tension headache Headache due to pathology Intracranial pathology: Subarachnoid haemorrhage sudden onset severe headache, worst head of my life with vomiting and focal neurological deficits Increased ICP from any cause Tumor causing mass effect or hydrocephalus Irritation or Inflammation of the meninges : meningitis Local pathology Eye pain , frontal sinusitis, giant cell arteritis Head trauma post concussive syndrome Following craniotomy Any new severe headaches or a change in pattern of a long-standing, recurrent headache warrants a CT or MRI brain especially when accompanied with symptoms of nausea and vomiting and or a abnormal neurological exam. Post LP headache A.k.a spinal headache. Follows procedures like lumbar puncture/drain or dural opening. Occurs when patient is erect and relieved when recumbent. May be associated with nausea, vomiting, visual disturbances and dizziness Pathophysiology It is thought to be due to CSF leakage due to dura puncture which reduces the CSP cushioning effect on the brain, accompanied with gravity pull on the brain when erect, tension and traction on the dura blood vessels and tethering of the brain to the pain sensitive dura. Occurs in about 20% after LP. Treatment Lie flat in bed for at least 6 hrs Maintain good hydration, PO or IV Analgesia e.g. paracetamol 1g QDS/PRN Abdominal binder High dose sterioids : PO dexamethasone 20mg/day and tail down the dose gradually Epidural blood patch : Access the epidural space, separate sterile venepuncture site to withdraw 10mls of patients own blood and inject it into the epidural space. Ensure that one is in the epidural space and ensure that CSF cannot be aspirated prior injection. Lie for 30mins supine. Effective in one application in 90%, may be repeated if ineffective. Risks : infection, cauda equine compression.
25
Hydrocephalus Hydrocephalus is a condition in which excess CSF builds up within the ventricles of the brain and may increase pressure within the head. CSF has three crucial functions: 1) it acts as a "shock absorber" for the brain and spinal cord; 2) it acts as a vehicle for delivering nutrients to the brain and removing waste; and 3) it flows between the cranium and spine to regulate changes in pressure within the brain. The average adult produces about 300mls of CSF daily. When an injury or illness alters the circulation of CSF, one or more of the ventricles becomes enlarged as CSF accumulates. In an adult, the skull is rigid and cannot expand, so the pressure in the brain may increase profoundly. Hydrocephalus is a chronic condition. It can be controlled, but usually not cured. With appropriate early treatment, however, many people with hydrocephalus lead normal lives with few limitations. Hydrocephalus can occur at any age, but is most common in infants and adults age 60 and older. It affects adult males and females, as well as people of different races about equally. Experts believe that normal pressure hydrocephalus accounts for 5 to 6 percent of all cases of dementia. Hydrocephalus Ex-Vacuo Hydrocephalus ex-vacuo occurs when a stroke or injury damages the brain and brain matter actually shrinks. The brain may shrink in older patients or those with Alzheimer's disease, and CSF volume increases to fill the extra space. In these instances, the ventricles are enlarged, but the pressure is usually normal. Symptoms of Adult-Onset Hydrocephalus Headaches Nausea Difficulty focusing the eyes Unsteady walk or gait Leg weakness Sudden falls Irritability Drowsiness Personality changes Seizures
Diagnosing Hydrocephalus Review pts medical history, and perform a complete neurological examination including diagnostic testing if needed Ask specific questions to determine if symptoms are caused by hydrocephalus
26
The neurological examination will also help to determine the severity of your condition. There are a wide variety of diagnostic tests that can help pinpoint the cause and severity of hydrocephalus. These include Computed tomography scan (CT scan),Magnetic resonance imaging (MRI), Isotopic cisternography, Lumbar puncture , Intracranial pressure monitoring
Surgery Hydrocephalus can be treated in a variety of ways. The problem area may be treated directly (by removing the cause of CSF obstruction), or indirectly (by diverting the fluid to somewhere else e.g. V-P,V-A shunt). Indirect treatment is performed by implanting a shunt to divert the excess CSF away from the brain. The body cavity in which the CSF is diverted is usually the peritoneal cavity In some cases, two procedures are performed, one to divert the CSF, and another at a later stage to remove the cause of obstruction (e.g., a brain tumor). Once inserted, the shunt system usually remains in place for the duration of a patient's life (although additional operations to revise the shunt system are sometimes needed). The shunt system continuously performs its function of diverting the CSF away from the brain, thereby keeping the intracranial pressure within normal limits. An alternative operation called endoscopic third ventriculostomy may be recommended. In this operation, a tiny burr hole is made in the skull and a neuroendoscope is utilized to enter the brain. The neurosurgeon will then make a small hole in the floor of the third ventricle, creating a new pathway through which CSF can flow. Prognosis The prognosis for hydrocephalus depends on the cause, the extent of symptoms, and the timeliness of diagnosis and treatment. Some patients show a dramatic improvement with treatment while others do not. In some instances of NPH, dementia can be reversed by shunt placement. Other symptoms such as headaches may disappear almost immediately if the symptoms are related to elevated pressure. If the cause of NPH is known, the rate of shunting success can be as high as 80 %. In cases in which the cause is unknown, the success rate varies from 25-74%. In general, the earlier hydrocephalus is diagnosed, the better the chance for successful treatment. The longer the symptoms have been present, the less likely it is that treatment will be successful. There is no way to accurately predict how successful surgery will be for each individual. Some patients will improve dramatically while others will reach a plateau or decline after a few months. Shunt malfunction or failure may occur. The valve can become clogged or the pressure in the shunt may not match the needs of the patient, requiring additional surgery. In the event of an infection, antibiotic therapy may be needed. A shunt malfunction may be indicated by headaches, vision problems, irritability, fatigue, personality change, loss of coordination, difficulty in waking up or staying awake, a return of walking difficulties, mild dementia or incontinence.
27
Normal Pressure Hydrocephalus (NPH) First described in 1965, A.k.a Hakim-Adams syndrome. Occurs in > 60 years old, more in males. Key features 1. Classic triad of Dementia, Gait disturbances and urinary incontinence 2. Communicating hydrocephalus on imaging, CT/MRI 3. Normal pressure on LP 4. Symptoms relieved after CSF shunting Etiology 1. Post SAH/ Post-trauma 2. Post-meningitis 3. After posterior fossa surgery 4. Tumors 5. Associated with Alzheimers disease (15%) 6. Deficiency of arachnoid granulations 7. Overlooked aqueductal stenosis 8. Idiopathic Diagnosis 1. LP pressure < 18cm H20; Response to a single/serial LP may be predictive 2. Trial of Lumbar drain (5 days, Mean improvement time 3 days) 3. Communication hydrocephalus on imaging 4. Others : EEG, CBF measurements( not specific), radionuclide cisternography Management 1. Dementia work-up should be completed 2. VP shunt is the treatment of choice( See page ..) 3. Medium pressure(65-90mmHg) valves should be used to prevent risk of SDH 4. Post-op, gradually sit the patient up slowly over a period of days. 5. If no improvement, assess for shunt malfunction. 6. Follow-up clinically and with CT/MRI 6-12 monthly Complications 1. SDH, hygroma, higher risk with low-pressure valves 2. Shunt infection 3. Shunt malfunction/migration 4. Intraparenchymal haemorrhage 5. Seizures Outcome 1. Urinary incontinence is the most likely to response to shunt, followed by gait disturbance and lastly dementia
28
2. 3.
Prognosis is better when symptoms are present for a short period Some do not improve and continue to deteriorate, it is important to exclude shuntrelated problems before attributing it to the natural course of disease.
Status Epilepticus Definition Defined as continuous seizure activity of more than 30 mins or 2 or more seizures without restoration of conciousness in between. If the seizure duration has exceeded 4 mins, then steps must be taken to abort the seizure. Aetiology CNS infection, trauma, tumour, CVA, anoxia etc Investigations 1. CT scan or MRI head in patients with new onset status and those with focal seizures 2. Lumbar puncture when an infectious etiology or SAH not seen on CT scan is being suspected 3. EEG: useful in determining whether the patient has a generalized or focal epileptiform abnormality and in helping to diagnose a non-convulsive status 4. Metabolic and toxicology screen and anticonvulsant levels Immediate management ABCs: Protect airway (roll patient on side, insert oral/nasal airway if possible, with supplemental O2; breathing and circulation) 2) Cardiac monitoring, SpO2 monitoring, ECG 3) IV access and sent bloods for FBC, U/E/Cr, Ca2+, Mg+, PO4-, Hypocount stat 4) Toxicology, ABG and therapeutic drug levels if indicated 5) Protocol to abort fit a) Give I/V diazepam 10mg bolus, max 20mg. PR Diazepam 10 mg if no IV access i) Give 5mg at a time, If there is any evidence of respiratory depression, stop infusion and transfer patient to ICU. b) DO NOT GIVE IF THE SEIZURE HAS ALREADY STOPPED. c) Diazepam should usually be followed by phenytoin loading. d) If not previously on phenytoin. Load with IV phenytoin 15mg/kg up to 1000mg in N/S not dextrose solution (to prevent precipitation) infuse at max rate of 50mg/min (1gm over 20 mins) with ECG monitoring. Stop/slow the infusion rate if there is any arrthymias i.e. QRS widening or hypotension. If the patient is on phenytoin and the level is not known, give IV phenytoin 500mg at 50mg/min. If patient is allergic to phenytoin use valproate. e) If seizures were to continue, transfer patient to ICA/ICU. f) Give additional dose of phenytoin at 5mg/hr up to 30mg/kg g) If seizure still persistent, inform the intensivist. h) Start phenobarbitone 10mg/kg at < 100mg/min up to 20mg/kg. Reduce the infusion rate if the BP falls.1)
29
i) If the seizures are still persistent, the patient may need a general anesthetic and/or barbiturate coma. This rare situation is to be co-managed with the intensivist and the neurologist. Note: In alcoholics and patients in whom hypoglycemia is identified as a cause, IV thiamine 50-100mg should precede the glucose bolus. 6) Treat the precipitating cause Anticonvulsants in prophylaxis and treatment of Seizures Phenytoin Loading dose: oral: 300 mg tds for 1 day. IV : 1g (up to 15 mg/kg) neat solution diluted to 20ml in N/S given over 20 minutes (i.e. rate not exceeding 50mg per minute) at the bedside by the M.O. with concurrent ECG monitoring. Maintenance doses of about 100mg should be given thereafter at intervals of every 68 hours, monitored by measurement of plasma concentrations; rate and dose reduced according to weight Watch for hypotension or arrythmias. Stop/slow down infusion rate if this is observed. To avoid local venous irritation each injection or infusion should be preceded and followed by an injection of sterile physiological saline through the same needle or catheter by intravenous injection via caval catheter, 3.55 mg/kg at a rate not exceeding 50 mg/minute, with blood pressure and ECG monitoring; repeat once if necessary By intramuscular injection, not recommended Sodium valproate Contraindications liver dysfunction, pancreatitis, porphyria, blood disorders. Dilute in Normal saline 0.9% Loading dose: i.v. 400-800mg slow I.V. (up to 10 mg/kg) Infuse over 3-5 minutes. Followed by iv infusion @ 1-2mg/kg/hr up to 2.5g/day Monitor liver function before and after initiation of therapy. For both drugs moderate dosage in patients who are hypoalbuminemic (common after severe illness). Consult the pharmacist about this.
30
Herniations Brain herniation represents mechanical displacement of normal brain relative to another anatomic region secondary to mass effect from traumatic, neoplastic, ischemic, or infectious etiologies. Herniations of the brain are divided in 5 major categories: (1) transtentorial, (2) subfalcine/cingulate, (3) foramen magnum/tonsillar, (4) sphenoid/alar, and (5) extracranial. Each category of herniation is associated with a specific neurologic syndrome. Transtentorial herniation Transtentorial herniation is a downward or an upward displacement of the brain through the tentorium at the level of the incisura. A descending transtentorial herniation occurs when the supratentorial brain herniates downward through the incisura. An ascending transtentorial herniation occurs when the infratentorial brain herniates upward through the incisura. Descending transtentorial herniation occurs more often than ascending herniations and includes the subcategory of uncal herniation. Ascending transtentorial herniation usually results from a posterior fossa tumor with mass effect. This results in the distortion of the midbrain, flattening of the posterior quadrigeminal plate and narrowing of the bilateral ambient cisterns. Extra-axial or intra-axial hematomas of the posterior fossa is a less common cause. Descending transtentorial herniation can cause various symptoms. Compression of the ipsilateral cranial nerve III may lead to ipsilateral dilatation of the pupil and abnormal extraocular movements. Compression of the ipsilateral corticospinal tracts in the brainstem may cause contralateral hemiparesis because these tracts decussate at the level of the medulla. Ipsilateral hemiparesis can also occur if there is sufficient mass effect causes the contralateral cerebral peduncle (Kernohan notch) to be compressed against the adjacent incisura. Other complications include unilateral or bilateral occipital lobe infarction from compression of the posterior cerebral artery. Brainstem hemorrhages are other complications caused by compression or kinking of pontine perforating vessels. Compression on the midbrain may cause hydrocephalus. Ascending transtentorial herniation causing brainstem compression can cause nausea and vomiting, which may progress rapidly to coma if rapid changes occur in the intracranial anatomy. A slow-growing mass in the posterior fossa results in slow changes in the intracranial anatomy; these do not often present as an acute emergency. Subfalcine/cingulate herniation
31
Subfalcine herniation occurs when the supratentorial brain is displaced underneath the falx secondary to mass effect. Subfalcine herniation does not necessarily indicate severe clinical symptoms. This type of herniation may lead to the clinical findings of headache, and symptoms may progress to contralateral leg weakness or ipsilateral frontal lobe infarction secondary to compression of the anterior cerebral artery. Foramen magnum/tonsillar herniation Foramen magnum herniation occurs when the infratentorial brain is displaced through the foramen magnum secondary to mass effect. Acute compression of the brainstem may result in obtundation and death. However, patients with Chiari I malformation may present with a paucity of symptoms, or they may present with dysesthesia in the extremities with cervical flexion. This is referred to as Lhermitte phenomenon Sphenoid/alar herniation Sphenoid/alar herniation results from the supratentorial brain sliding either anteriorly or posteriorly over the wing of the sphenoid bone. An anterior herniation occurs when the temporal lobe herniates anteriorly and superiorly over the sphenoid bone. Conversely, a posterior herniation occurs when the frontal lobe herniates posteriorly and inferiorly over the sphenoid bone. Associated clinical symptoms are usually minimal, though sphenoid herniations are often associated with other types of herniations. Extracranial herniation Extracranial herniation occurs with displacement of brain through a cranial defect. This finding usually results from a traumatic or surgical cause. The herniated region of the brain may become ischemic, leading to infarction. Invesitgations: For transtentorial herniation, CT or MRI is useful for evaluation. MRI can provide axial as well as sagittal and coronal views. Intervention Medical Treatment to decrease intracranial pressure. E.g. mannitol, hyperventilation, steroids etc. Surgical intervention in the treatment for increased intracranial pressure is dependent on cause. Neoplasms causing brain herniation may be resected if possible, to reduce mass effect. Patients with a large parenchymal and extra-axial hemorrhage may benefit from a standard craniotomy or craniectomy with duraplasty followed by clot evacuation. In cases of descending transtentorial herniation of the brain caused by a large subdural hematoma, emergency surgical decompression is required to prevent irreversible injury to the brainstem, as well as other areas of the brain.
32
Brain Death Brain death refers to the total and irreversible cessation of all functions of the brain. A person who is brain dead has no spontaneous respiration and will need to be supported on a ventilator. Brain death is accepted as a legal definition of death in Singapore and in other advanced countries. It is determined based on a well-defined standard set of clinical criteria. The seven clinical criteria for determining irreversible cessation of all functions of the brain are as follows:1. 2. 3. 4. 5. 6. 7. the pupils are fixed and non-reactive to strong light there is no corneal reflex; there is no spontaneous motor response to painful stimulus, excluding spinal reflexes, there is no oculeocephalic reflex; there is no gag reflex or reflex response to tracheobronchial stimulation; there is no vestibule-ocular response on instillation of 50 cubic centimetres of ice-cold water into each ear; and there is no spontaneous respiration even with carbon dioxide tension at 50 millimetres or more or mercury.
These tests are to assess whether there is any response to various physical stimuli such as light, touch and pain. Brain death can only be certified if all seven clinical criteria are met. The clinical criteria for brain death as specified in the Interpretation Act must be observed to be present in the patient separately by two doctors before brain death can be certified. Both doctors must be experienced with specialist qualifications. Should the two doctors have differing opinions, brain death would not be certified. The two doctors who examine the patient must:
not have been involved in the care or treatment of the patient being certified not belong to the team of medical practitioners who will remove the organ from the body not have been involved in the selection of the proposed recipient of the organ not be involved in the care or treatment of the proposed recipient of the organ during his hospitalisation for the transplant
The following supplementary tests are allowed to be used for brain death certification. 1. Cerebal angiography to confirm that there is no intracranial blood flow. 2. Radionuclide scan to confirm that there is no intracranial profusion. The supplementary tests are to complement the clinical tests. They are not a substitute for the clinical criteria. If six of the seven clinical tests can be performed, the criteria for these six tests must be fully met, that is 6 upon 6, before the doctor proceeds to carry out an ancillary test.
33
Infections of the CNS
34
Acute infections include bacterial meningitis, viral meningitis, encephalitis, focal infections e.g. abscess, subdural empyema. Medical emergency, treatment should commence once suspected. Key goals 1. Identify and distinguish between the different conditions 2. Identify the pathogen 3. Initiate appropriate antimicrobial therapy and institute surgical treatment if necessary Clinical Presentation 1. Acute Rapid onset(48 hr onset with gradual worsening symptoms, with no or gradual impairment of higher functions. Commonly viral or granulomatous in origin. History 1. Risk factors prior infection e.g. otitis, sinusitis, pneumomia, endocarditis, asplenia, sickle cell, multiple myeloma, alcoholism, cirrhosis, head trauma with CSF leak, immunocompromised state e.g. AIDS, transplant pts, chronic steroid therapy 2. Listeria monocytogenes is a important consideration in pregnant women 3. Previous invasive neurosurgical procedure, think of S. aures, coagulase-negactive staphylococcus. 4. Rash of meningococcemia begins as a maculpaplular rash developing into a petechial rash on trunk, lower extremities, mucous membranes, palms, soles Principles of Management 1. Initiate empirical therapy once bacterial meningitis is suspected. Antibiotics should be started w/i 30mins. IV Ceftriaxone 2g stat, continue with 2g bd x 7-10 days. Consider adding amikacin if there is risk of CSF leak. Chloramphenicol if allergy to penicillin. Consult ID if in doubt. 2. Perform septic work-up including LP. If focal neurology or papilledema or signs of raised ICP, obtain CT head first. CSF for FEME, C/S, AFB smear and gram stain, viral serology/PCR if suspected .Bloods for FBC, U/E/Cr, PT/PTT, GXM , ESR, CRP. CXR, Urine C/S and UFEME. 3. If suspect viral encephalitis, give IV acyclovir(10mg/kg 8hrly for 14 days) for presumptive herpes simplex.( Obtain MRI +/- EEG). HSV affects temporal lobes mainly. 4. CLC, Hrly parameters, admit to ICU/ICA, Intubate if GCS < 8. obtain ID consult early. 5. Treat seizures with Phenytoin . 6. Treat TB Meningitis with isoniazid(15mg/kg/day), rifampicin(15mg/kg/day), and pyrazinamide(1.5-2g/day) CSF findings in Meningitis Cause/CSF Appearance WBC/mm3 Type of wbc Protein Glucose
35
Normal Viral Bacterial TB
Clear Clear Cloudy Clear
0.1
mmol/L > 2.2 >2.2 False localizing CN 6 palsy Look for intracranial lesion Ischemic risk factors
InvestigationsPapilloedema and/or bilateral CN 6 palsies neuroimaging BP, bld glucose
ManagementCover affected eye to relieve diplopia Refer ENT Conservatie mx if ischmemic To assess for possible underlying NPC Resolution in 3mth
Facial nerve (seventh) palsy HistoryFacial asymmetry Inability to close eyes
Physical examinationLoss of forehead creases Unable to close eye Loss of nasolabial fold Drooping of angle of mouth Other CN involvement UMN lesion Neurological exam brainstem, cortical lesion LMN lesion: try to identify site Cerebellopontine angle Temporal bone Ear Parotid gland Bellss palsy LMN lesion (if preserved - UMN lesion) Risk of exposure keratopathy potentially sight threatening esp. if infected
CVA (isch/ haem), tumour CN 6,7,8 +/- 5 Fracture (hx of trauma, Battles sign, CSF otorrhoea) Otitis media, Ramsey-Hunt Tumour, trauma Diagnosis of exclusion
47
Investigations ManagementProtect the cornea tape lid shut at night, copious lubricants*, lateral tarsorraphy if exposure is severe Refer ENT
Neuroimaging Refer eye to assess exposure keratopathy Ear lesions
* Lubricants Eyedrops: Gutt hypromellose Q3H (cheap, easily available, single bottle but preservatives bad for corneal epithelium in long term) Gutt tears naturale free/ Refresh plus Q2H (preservative free, comes in disposable tubes better for eye in longer term, but more costly) Ointments: longer-lasting occ solcoseryl/ Duratears/ Vidisic TDS or QDS (B) Multiple cranial nerve palsies Cavernous sinus syndrome (CN 3,4,5,6) History, Physical Exam: Combination of the above-mentioned CN palsies Etiology: Vascular o aneurysm: intracavernous sinus carotid aneurysm, posterior cerebral artery aneurysm o cavernous sinus thrombosis Inflammatory o meningitis o bacterial: syphilis, TB o viral: herpes zoster o Tolusa Hunt Tumour o primary: pituitary adenoma, meningioma, cranipharyngioma o secondary: NPC, lymphoma, mets Trauma o Carotid-cavernous sinus fistula Cerebellopontine angle syndrome (CN 5,6,7,8) Etiology: Tumour o Acoustic neuroma o NPC o Clivus meningioma Trauma o Basal skull fracture
o Pontine glioma o V CN neuroma
48
Lateral medullary syndrome (5,8,9,10) Etiology: Stroke Multiple sclerosis Clinical features: CN 5 and spinothalamic tract crossed hemihypoalgesia CN 8 nystagmus CN 9, 10 dysarthria, dysphagia Sympathetic Horners (ptosis, miosis, anhydrosis, enophthalmos) Cerebellum nystagmus, disdiadokinesia, intention tremor Traumatic Eye Injuries Blowout fracture Fracture of the orbital walls. Medial and inferior walls most commonly involved HistoryMechanism of injury Diplopia, pain with ocular movement Physical Exam Enophthalmos Periorbital swelling Orbital rim tenderness, crepitus, step Blunt injury object larger than orbit
Signs suggestive of blowout fracture # of orbital wall. Maxillary haemoantrum
InvestigationsXR orbits CT orbits
ManagementRefer to plastics/ eye (oculoplastics) Pt to avoid blowing nose Oral antibiotic prophylaxis
Traumatic optic neuropathyDamage to optic nerve: transaction, impingement by bony fragments, or compression by haemorrhage Blurring of vision after trauma History
ExaminationRAPD Visual acuity Usually very poor but can be normal Bony impingement, transaction of optic n, retrobulbar haemorrhage Refer eye, KIV IV steroids
InvestigationsCT orbits (fine cuts)
Management
Open globe injuries Can result from blunt trauma, (high velocity) foreign body entry. Pain and decreased vision may be elicited in history. Severe subconjunctival haemorrhage and limited extraocular motility are features that may be present grossly. Refer to eye specialist for assessment and primary repair. Hyphaema
49
Blood in the anterior chamber of the eye. Layer of blood may be visible on general inspection. Ususally resolves spontaneously but may be complicated by increased intra-ocular pressure causing pain. Refer to eye specialist for assessment. Useful numbers SGH neuro-radiology reporting room 6326 6062 SNEC mainline 62277255 Neuro-ophthalmology consultants (SNEC): Prof Barry Cullen, Dr Sharon Tow
50
Surgical procedures and operations Elective Neurosurgical admissions (Guidelines only) Most elective admissions will be for Brain Tumour patients as well as Spinal cases. CRANIOTOMY 1. History and examination 2. Check Relevant pre-op investigations are done, if not then order: FBC, U/E/Cr, PT/ PTT, GXM 2 to 4 units (aneurysm surgery will need at least 4 units). Trace all old notes. CXR / ECG as clinically appropriate If patient has been to Pre-admission Clinic then check all blood inv and CXR / ECG are with the case notes 3. Make sure CT / MRI +/- angiogram is present with the notes. Some patient will require specific MRI sequences called STEALTH. For these patients stereotactic markers will need to be placed on them(ALWAYS CHECK WITH REGISTRAR WITH REGARD TO POSITION IF IN DOUBT) if MRI needs to be done, call Radiologist or MRI counter and fax the request form with the urgent form to the MRI counter. Write on form for STEALTH MRI Brain. Please exclude Contraindications to MRI ! Place the markers, insert IV cannula and then send the patient down. If the markers are to come off then they need to be replaced at the exact spot. MRI will burn a disc for STEALTH patients. This must accompany the patient to theatre .Check consent has been signed and side specified; Write and dispatch OT chit. 4. All patients will require an IV drip when NBM. 5. Consultants may request specific orders on the admission form check that these have been done or ordered. Aspirin should have been ceased for 1 week prior to surgery.
-
-
-
SPINAL CASES 1. History and examination check for pain, document pre-op neurological deficits 2. Pre-op investigations: FBC, U/E/Cr, PT/PTT, GXM 1 unit; CXR / ECG as clinically appropriate 3. Check CT / MRI / SPINAL x-rays available pre-op 4. Consent signed and levels specified; Write and dispatch OT chit 5. Special orders: Some patients will require C- collars to go with patient to surgery. Some consultants prefer pre-op skin markers (paper clips stuck to skin by micropore tape) to be placed at the relevant spinal levels and X-rays to be done with the skin markers. This is to facilitate intraop planning. CAROTID ENDARTERECTOMY 1. History and examination
51
-
Blood pressure control is imperative pre-op. If patient is markedly hypertensive then inform registrar ASAP as medications may need to be altered. 2. Pre-op Investigations: FBC, U/E/Cr, PT/PTT, GXM at least 4 units CXR / ECG as clinically appropriate 3. Check Carotid angiogram is done, if not then see if it has been organised . 4. Check consultants specific orders aspirin does not need to be stopped pre-operatively but check with consultant / registrar if not sure. 5. If patient is on continuous heparin infusion then check with your consultant when to cease preop. There is a protocol in the wards for the management of heparin infusion please read it before starting heparin for anyone. 6. Check consent signed and side specified. 7. Write and dispatch OT chit 8. NBM at midnight with IV drip order TRANSPHENOIDAL PITUITARY SURGERY( see Clinical Pathway for details) 1. History and examination Document visual fields and visual acuity with Snellen chart if no pre-op eye review requested Make sure no signs or symptoms of sinusitis (if present then contact registrar) 2. Pre-op investigations FBC, U/E/Cr, PT/PTT, GXM 2 units ECG / CXR as clinically appropriate Make sure pituitary hormone work up results is in case notes. 3. Check CT / MRI films are present 4. Pre-op consults: See if pre-op consult for ophthalmology or endocrine required. If unsure then check admission notes, clinic notes or with consultant in charge. 5. Medications may need to be charted pre-op as requested by consultant or endocrinology, check for these in the notes and order them as necessary 6. Check consent signed 7. Write and dispatch OT chit 8. NBM at 12 midnight with IV drip order
-
EMBOLISATION / ANGIOGRAM 1. History and examination 2. Pre-op Investigation: Angiogram: requires FBC, PT / PTT, Urea and Cr Embolisation (done under GA): FBC, U/E/Cr, PT/PTT, GXM 2 units, CXR and ECG as appropriate 3. Consent for angiogram to be taken by MO in charge see attached sheet on consent. Consent for Embolisation will be taken by neuroradiologist and will be with the request form usually in angio suite already. 4. NBM at midnight with IV drip for all patients.
52
Craniotomy and its complications Craniotomy is an operation where a window is cut into the skull bone to allow the surgeon to operate on the brain. The purpose of the operation may be to remove a blood clot, tumour, or blood vessel disorder among others. Modern advances have made brain surgery safer. However, as with all surgical procedures, complications can occur. Some of these risks and complications are inherent in any operative procedure, especially when general anaesthesia is administered. In addition, some of the possible complications specifically following Craniotomy are: Cerebral haemorrhage This may occur at the site of operation usually some time after the operation is completed. If haemorrhage is suspected, it can be confirmed by CT brain scan. If the haemorrhage is large, further surgical procedures may be required to treat it. It may result in irreversible paralysis, coma or even death. Post-operative brain swelling This can result from manipulation of the brain. It may require the original bone window to be left out when the skin incision is closed (this will require a second operation to replace the bone window at a later time). Further surgery may be required to treat the swelling. Post-operative infection This is a potentially very serious complication that occurs despite the routine surgical prophylaxis against infection. Treatment of infection can involve multiple surgical procedures and prolonged hospital stay for antibiotic treatment. Post-operative brain water circulation disorder This is due to disturbance of the brain water circulation pathways that sometimes develops after surgery. Its treatment may require further surgery to allow diversion of the brain water to another body cavity. This can sometimes have permanent effects (neurologic deficit) Post-operative brain malfunction (neurologic deficit) The likelihood of this complication varies from one operation to another. It may be a temporary condition or it may be permanent. It may be the end-result of other complications (eg. haemorrhage, swelling, infection). The patient may experience the loss of vision, hearing, speech/ language ability, sensation, paralysis of limbs, loss of coordination of limbs or cognition (thinking ability), specific cranial nerve dysfunction, coma or even death. Seizures This develops in some patients after surgery. The patient may be required to take anti-convulsant medication for life.
53
Frameless Stereotactic Neurosurgery The first part of the procedure involves CT or MRI performed with fiducial markers which are taped to the scalp before the brain is imaged. Frameless systems can also use bony landmarks e.g. mastoid process. The second part utilizes a set of guides orientated to the same coordinate system registered in the computer containing the brain images. Once registration is completed, the computer can show the relationship of our surgical instruments to the imaged brain. Frameless or image guided surgery is very helpful for the accurate approach and removal of large brain tumors Indications: 1. Biopsy deeply structures esp. in near eloquent brain, brainstem lesions, small lesions, pts unable to tolerate GA for open biopsy. 2. Catheter placement drainage of deep lesions, EVD, indwelling catheter for intratumoral chemo, radioactive implantation. 3. Electrodes placement Deep Brain stimulation electrodes, epilepsy electrodes 4. Evacuation of ICH using adjunctive urokinase 5. Localising lesion for open craniotomy 6. Stereostatic radiosurgery Steps: 1. MRI/CT Scan is done usually the day before the operation. 2. Place fiducial markers on the patients to act as reference points. 3. Some small areas of shaving may be needed for the markers to stick. 4. Use permanent marker pen to mark the location. 5.Place at least 8 fiducials, with 1-2 on contralateral side, on the bony attachment of the head which are not movable e.g. mastoid process. Some markers should be higher, lower and at the level of the brain tumour. A wide area needs to be covered. But the location of the fiducial markers should be accessible by the surgeon during the actual positioning of the patient intraop (if the patient is supine, it will be useless to have markers on the occipital protuberance as it is not accessible intra-op) 6. If unsure of the location of the markers, consult the registrar or neurosurgeon for the exact placement if in doubt before scan. 7. Advise pt and nurses not to wash hair and try to keep the fiducial markers in place till operation External Ventricular Drain(EVD) These drains are catheters placed for several different reasons including acute obstructive hydrocephalus (eg. from a blood clot in the fourth ventricle), tumor obstructing the aqueduct or for communicating hydrocephalus such as after a SAH or meningitis. They are also placed temporarily after removing an infected VP shunt while the infection is treated with antibiotics prior to replacing another VP shunt. The nurse will be checking the drain and taking measurements. A sample of CSF may be taken. There will be CSF in the drainage system. The fluid may be clear, yellowish, or bloody.
54
The patients GCS level should be monitored closely after any adjustment to the height of the EVD, clamping, removal etc. EVD Removal 1. To be done under aseptic condition 2. The stitch holding the drain will be removed. The drain is removed. 3. ALL EVD drain tips should be sent for culture. (All EVD drain culture results should be traced before sending the patient home) 4. A stitch will be used to close the drain exit site. 5. A small dressing will be placed over the area. The Neurosurgeon in charge will decide on the duration of EVD drainage before weaning, change of EVD or conversion to a VP shunt. In general, EVD catheters are changed after 7 days or earlier if there is signs of infection. These drains are subject to 3 main problems: 1. Infection2. Dislocation (usually during a turn or when pulled by a patient)
3.
Blockage (usually due to blood clots)
In general the EVD drainage is regulated by gravity. The EVD drip chamber is usually set at 510cm above the external auditory meatus (= level of foramen of Monroe) and left to free drainage. This height can be adjusted to achieve more drainage (by lowering it) or less (by raising it) according to the clinical situation. Physiological Facts 1) Average daily CSF production = 300ml/day 2) Average Lateral Ventricle volume = 20ml CSF 3) Average Total CSF volume = 150ml
55
1. 2. 3. 4.
Management of a Blocked CSF drain. Note the clinical situation. If there is no neurologic deterioration or change, then discuss with the neurosurgeon regarding flushing. He may opt to observe the patient. If CSF drainage is mandatory an attempt to flush the catheter will be ordered. Use aseptic technique and wear a sterile gown Dead space of EVD catheter = 2ml established can repeat up to 2 more attempts. If there is still no flow, inform the neurosurgeon. He may decide to replace the catheter.
Use 2ml of sterile N/S to flush the catheter from the 3-way tap point. If no flow
56
Ventriculo-peritoneal shunt The Operation After a general anesthetic is administered, the patient is positioned on his back, with his head turned to one side. The hair over the scalp incision area is shaved. Usually two incisions are made: a small incision in the abdomen and a curved incision in the scalp. The scalp flap is then turned back to expose the skull, into which a small burr hole is drilled. This uncovers the dura, the brain's covering, over the enlarged ventricles. The shunt is inserted first into the abdominal incision and is brought beneath the skin over the abdomen, chest, and neck, into the scalp opening. After the tubing and reservoir are in place, a small cut is made in the dura and a ventricular tube is inserted into the brain's right ventricle. The reservoir is then attached to the ventricular tube and is fitted into the opening in the patient's skull. Signs of a shunt infection 1. A fever that is equal to or higher than 38.5 C 2. Redness and tenderness along the path of the VP shunt 3. Swelling along the path of the VP shunt 4. Meningitis and Kernigs sign 5. Change in mental state
Ommaya Reservior Cerebrospinal fluid (CSF) surrounds the brain and spinal cord. Sometimes, medications need to be given into the CSF because intravenous medications will not reach that area. Medications can be given into the CSF when an ommaya reservoir is inserted. The ommaya reservoir, or port, is a dome like device that is placed surgically under the scalp. It is used for: 1. Give medications directly into the CSF 2. Measure the pressure of the CSF 3. Take samples of CSF to be tested 4. Inserted into cysts for intermittent decompression SAMPLING AND DRUG ADMINISTRATION Consistent guidelines for access, injection of medications, and withdrawing CSF from the Ommaya reservoir will prevent infection or adverse outcomes. 1. All medications will be preservative-free. No alcohol or alcohol containing products should ever be used for site preparation of an Ommaya Reservoir. Maintaining sterile technique, prepare skin over Ommaya reservoir. Swab to cleanse skin over reservoir with povidone-iodine using a circular motion from inner to out. Repeat with two additional swabs. Allow to dry two minutes, then remove excess povidone-iodine with dry sterile gauze. 2. Insert needle (Need to use fine bore butterfly needle) through middle of dome, at an angle perpendicular to the dome. Gently advance needle until the tip of the needle meets the backstop of the reservoir. (Alternate insertion sites in dome.) 3. If lab studies on CSF needed, withdraw 2 ml CSF, clamp tubing, and discard CSF. Then withdraw 1-4 ml. 4. Inject medication slowly (3-5 minutes) into reservoir 5. Remove scalp vein needle from reservoir. 6. Place sterile 2 x 2 dressing over reservoir. 7. Maintain pressure at injection site 3-5 minutes. 8. If need for multiple aspirations use the 4 quadrant technique. 9. Observe patient throughout the procedure. Stop the aspiration if patient complains of headache, giddiness, nausea, vomiting or new neurological findings. 10. When instilling medications use isovolumetric technique. E.g. aspirate 2ml, instill 1ml medication, flush with 1ml normal saline/aspirate. (Dead space of ommaya reservoir =1ml)
Lumbar Puncture Indications: 1. To obtain CSF sample to check for meningitis / cytology / immune markers / xanthochromia in subarachnoid haemorrhage 2. To measure opening and closing pressures via manometer especially in deciding for surgery in normal pressure hydrocephalus (NPH) 3. Therapeutic removal of CSF to assess for benefit of Ventriculo-peritoneal shunt in NPH. Contra-indications: 1. Raised intracranial pressure e.g. if non-communicating hydrocephalus, papilledema on ophthalmoscopy. All patients will require CT head prior to LP to reduce risk of coning is suspicion of increased pressure. 2. Cardiorespiratory unstable patients 3. Infection at the site of Lumbar puncture e.g. pressure ulcer 4. Coagulopathy Materials (will be prepared by nurses) Lumbar Puncture set with sterile gloves. Wear a mask and protective gown as well! Spinal Needle use a 20 / 22-gauge always if possible Manometer to measure pressure Sterile drapes Local Anaesthetic usually 5mls is sufficient Material for skin sterilization iodine and alcohol usually Adhesive pressure dressing Technique 1. Place the patient in the lateral decubitus position lying on the edge of the bed and facing away from operator. Place the patient in a knee-chest position with the neck flexed. The patient's head should rest on a pillow, so that the entire cranio-spinal axis is parallel to the bed. Sitting position is the second choice because there may be a greater risk of herniation and CSF pressure cannot be measured 2. Find the posterior iliac crest and palpate the L4 spinous process, and mark the spot with a fingernail. Prepare the skin by starting at the puncture site and working outward in concentric circles. Put on sterile gloves. Drape the patient. 3. Anaesthetize the skin and then insert in the midline with the needle parallel to the floor and the point directed toward the patient's umbilicus to anaesthetize between the spinous processes. 4. Next use the Spinal 22 G needle and advance slowly, in the same direction, about 2 cm or until a give is felt (piercing the membrane of the dura and entry into subarachnoid space). Then withdraw the stylet in every 2- to 3-mm advance of the needle to check for CSF return. If the needle meets the bone or if blood returns (hitting the venous plexus anterior to the spinal canal), withdraw to the skin and redirect the needle. If CSF return cannot be obtained, try one disc space up. 5. When cerebrospinal fluid begins to flow from the needle, discard the first few drops. Never aspirate CSF!!! 6. Measure the opening pressure with a manometer; allow the patient to relax, and check for good respiratory variation of the fluid level in the manometer to ensure that the needle is properly positioned.
7.
8. 9.
Remove the manometer and allow 1 to 2 cc of CSF to flow into each of the three sterile tubes. Send the first for glucose and protein, the second for Gram stain and culture and sensitivity (C&S), and the third for cell count and differential. A fourth tube, when indicated, is collected for viral titre or cultures, India ink preparation, Cryptococcus antigen, VDRL, or cytology (if needed). In subarachnoid haemorrhage, 3 tubes need to be collected to measure the differential cell count from bottle 1 to 3 as well as for xanthochromia. Measure the closing pressure obtaining CSF for investigations. Withdraw the needle without replacing the stylet. Dress the puncture site with a pressure bandage. Have the patient lie in bed for at least 6 hours and monitor parameters hourly for 6 hours. Document the procedure in the case notes.
Complications 1. Post-lumbar puncture headache: 2. Occurs in 10% to 30% of patients within 1 to 3 days and lasts 2 to 7 days. Lying flat relieves the pain. Treatment consists of bed rest and fluid with simple analgesics. 3. Can be reduced by using the most practical size needle that is 22 G. 4. Keep bevel of needle facing upward i.e. in the direction of the dural fibres.
Lumbar Drain These drains are catheters placed at the bedside into the lumbar subarachnoid space to remove CSF. Indications of Lumbar drain 1. Non-obstructive hydrocephalus (e.g. following SAH) 2. To treat CSF leaks resulting from cranial surgery or trauma The lumbar drain is a small plastic catheter used to remove CSF. It is inserted using the same technique as a lumbar puncture except in this case a Tuohy needle is used. The usual orders are to remove 100mls CSF per nursing shift. (300mls/day). Please check with the neurosurgeon in charge. The nurse will also be checking the drainage system frequently. The fluid may be clear or coloured. The head of the bed may be elevated. However, if the patient is going to sit up or assume the upright posture the drain must be clamped to prevent sudden over drainage and possible subdural hematoma. The risks of a lumbar drain are: - Meningitis - Hematoma - Bleeding - Leakage of cerebrospinal fluid (CSF) - Paralysis - Infection Lumbar drains are removed after about 1 week in this center. (Please check with the neurosurgeon in charge of the patient before removing the drains) Procedure 1. A standard LP is performed (See Steps 1-8 on Lumbar Puncture) 2. When CSF is encountered, the curve of the needle is directed superiorly, the stylet is removed, and the catheter is advanced into the subarachnoid space at least 20 cm (Fig. A). The catheter (17- or 18-gauge) is then slowly advanced with one hand, and the needle is simultaneously removed. 3. A local anesthetic agent is injected subcutaneously along the desired path of tunneling for the length of the needle. The free Tuohy needle(Fig. B) is passed from this direct lateral position and brought out through the initial LP site, with care being taken not to cut the catheter with the tip of the needle
Transsphenoidal Pituitary Clinical Pathway Pre-Op/Day of admission 1. Blds : FBC,U/E/CR, PT/PTT, Hep B, GXM 1 unit 2. Pituitary Hormonal profile if not done previously a. Synacthen test, fT4,TSH,GH,IGF1, FSH,LH,Testosterone,E2 3. ECG,CXR if more than 40 yrs or otherwise indicated 4. Diet of choice or Specific Diet( e.g. low salt, low fat, DM); NBM 12MN 5. Pre-op assessment by Endocrinologist, Ophthalmologists, Anesthetists if already not done before; Inform Endocrinologist of patient admission. 6. Order in IMR IV Cefazolin 2g and IV Metronidazole 500mg on call to OT; if pt allergic to beta-lactams, order IV clindamycin 600mg and IV gentamicin 1.5mg/Kg 7. IV hydrocortisone 100mg on call to OT. Day of Surgery/ 0 POD / Post-Op 1. CLC and parameters hrly, Hrly urine output and I/O charting; Visual charting 2. IF Diabetes insipidus/ Urine output >200mls/hr for 2 hrs a. Repeat Na+ and serum osmolality; Hypocount 6hrly 3. Assess for CSF leak and bleeding from nose a. Document total no. of nasal bolsters change requireed b. inform Neurosurgeon if excessive 4. IV hydrocortisone 100mg 8H unless Cushings a. If Cushings/Apoplexy/ Pre-existing Hypocortisolism i. continue IV hydrocortisone 100mg 6H b. If Pre-existing DI- administer s/c DDVAP 4g bd, nasal DDVAP can be started once nasal packs removed 5. Rest in bed, head up 30 degrees. Keep Urine catheter 1st POD 1. CLC and parameters hrly, Hrly urine output and I/O charting; Visual charting 2. IF Diabetes insipidus/ Urine output >200mls/hr for 2 hrs a. Repeat Na+ and serum osmolality; Hypocount 6hrly 3. Assess for CSF leak and bleeding from nose a. Document total no. of nasal bolsters change requireed b. inform Neurosurgeon if excessive c. Remove nasal pack if no bleeding 4. IV hydrocortisone 50mg 8H unless Cushings(8am,2pm,8pm) a. If Cushings/Apoplexy/ Pre-existing Hypocortisolism i. continue IV hydrocortisone 100mg 6H till last dose on 2POD 8pm ii. Can covert to Oral on 2POD if taking diet well b. If Pre-existing DI- administer s/c DDVAP 4g bd, nasal DDVAP can be started once nasal packs removed 5. If DI suspected- Inform Endocrinologist a. monitor I/O, hrly urine output; replace urine loss with 5% Dextrose b. monitor hypocount 6H.
6. Feeds to Diet as tolerated; Ambulate as tolerated 2nd POD 1. Review CLC, Visual charting and Monitor I/O, H/C 2. Assess for signs of Cushings- anorexia, N+V, myaglia, low grade fever a. Call Endocrinologist if signs presents 3. Remove IV plug, except for pts with Cushings disease 4. Remove urinary catheter if no DI or as ordered 5. Pts with intact cortisol axis(i.e. peak synacthen response>550nmol/l and 2nd POD cortisol> 450nmol/l) a. Stop hydrocortisone replacement 6. Pts with possible hypocortisolism(2nd POD50nmol/l) a. Continue IV hydrocortisone 100mg 6H 8. If pre-existing hypocortisolism a. Start oral hydrocortisone 40mg OM, 20mg ON 9. If Apoplexy a. Give at least double physiological dose; consult Endocrinologist 10. If pre-existing DI a. Nasal ddavp may be restarted once nasal packs are removed 11. Diet as order and tolerated: ambulate as tolerated 3rd POD 1. If pt well, no DI/fever/bleeding consider discharge 2. Assess as mentioned in 1st and 2nd POD 12. Pts with intact cortisol axis(i.e. peak synacthen response>550nmol/l and 2nd ,3rd POD cortisol> 450nmol/l) a. Stop hydrocortisone replacement 13. Pts with possible hypocortisolism(2nd ,3rd POD cortisol 2x BP >200 mmHg Bradycardial 8, admitted to the NICU for close monitoring due to high risk for deterioration. 3. Post-craniotomy (for mass lesions) with brain swelling or potential for further brain swelling. 4. Intra-cranial mass lesions with potential for further swelling and deterioration.
Exclusion Criteria: 1. SHI with intractable hypotension despite maximal resuscitation and assessed to be unlikely to survive. 2. Patients with clinical and compatible CT evidence of brainstem death. 3. Presence of a terminal illness for which active management of the SHI is deemed futile.
Admission and Transfer All patients admitted to NICU from the Emergency Department (ED), general ward (GW) or through inter-hospital transfer, must first be triaged and accepted by the neurosurgical registrar on call. The procedure for accepting of new cases from ED and the movement protocol from ED to the scan room and then to NICU is covered under a separate protocol.
Initial Assessment and Management Resuscitate aggressively and promptly to correct any hypotension and/or hypoxemia, which are important causes of secondary brain injuries. The AIRWAY, BREATHING and CIRCULATION must be assessed IMMEDIATELY upon admission. All SHI with GCS 8 should be intubated, if not already intubated in the ED, to protect the
airway and assure effective ventilation and oxygenation. Patients for transfer to the NICU from GW should be intubated first prior to transfer. Aim to keep MAP 80 mmHg and SpO2 >95%. Patients with isolated closed head injuries should NEVER be hypotensive, unless already brain dead. If hypotensive, always SUSPECT AND LOOK FOR other causes e.g. intra-abdominal bleeding, scalp wounds, base of skull fractures, thoracic injuries or pelvic fractures. ALL SHI patients should have a cervical collar to protect the cervical spine till the neurosurgeon-in-charge has cleared the neck after reviewing the cervical spine x-rays CT scan. In patients expected to require the cervical collar for 40 yrs, unilat or bilat motor posturing or SBP 20 mmHg Maintain normo-volemia and normo-tension o Order maintenance fluids: normal saline at 80-120 ml/hr (depending on size of patient). Add 10-15 ml of 7.45% KCl to each 500 ml unit if renal function normal and serum K is not raised. Avoid hypotonic fluids. o Keep MAP >80 mmHg, CVP 6-10 mmHg and urine output > 0.5-1.0 ml/kg/hr o Look for and treat causes of hypotension or hypovolemia. o Treat hypotension aggressively with fluid boluses (isotonic saline, colloids or blood).
o Start inotropes early (noradrenaline infusion: 4 mg in 100 ml D5% at 1-10 ml/hr titrated to MAP and/or CPP) to maintain perfusion pressures while catching up with volume replacement. Secure and protect the airway and decompress stomach o All intubations must be performed by an anaesthetic trainee, registrar or consultant. During office hours, page the consultant in NICU. After office hours, page the ICU registrar (Mon-Fri) or the OT anesthesia registrar (Sat, Sun and PH). For emergency cases, activate the airway pager for assistance. o Patients should be intubated via rapid sequence induction using a sedative (etomidate or midazolam) and a neuromuscular blocking agent (succinylcholine). o Confirm tube placement with auscultation. Use the capnometer when in doubt. o A CXR must be ordered to check the tube position after intubation. o Insert NG tube to decompress stomach, preferably orogastric. Ensure optimal ventilation and oxygenation. Avoid routine hyperventilaton. o Aim for normocapnia (PaCO2 35-40 mmHg) with SIMV or CMV o Keep PaO2 >100 mmHg and SpO2 >95% with appropriate FiO2 o Patients should NOT be hyperventilated routinely or prophylactically as this can further compromise already low cerebral blood flow, especially during the first 24 hrs following HI. o Hyperventilation may be used for brief periods during acute neurological deteriorations, to control intra-cranial hypertension, pending evacuation of mass lesions in the OT. Ensure adequate sedation and analgesia o Patient agitation and restlessness can lead to self extubation, dislodgement of invasive lines or excessive hypertension and worsen brain edema. o Start with a narcotic (IV morphine infusion: bolus 2-4 mg followed by 1-5 mg/hr or IV fentanyl: 25-50 g followed by 5-50 g/hr) o Add IV propofol 10-100 mg/hr (1-10 ml/hr) if patient still restless. Bolus 10-30 mg (13 ml)
o Avoid benzodiazepines as far as possible. o Reduce coughing and bucking on the ETT during tracheal suctioning by adding lignocaine (2-4% 1-2 ml) into the ETT before suctioning. Ensure neck is kept in a neutral position with the head elevated 20-30o Avoid hyperthermia. Keep rectal temperature twice a day) o LFT (weekly) o CXR (weekly if intubated or when clinically indicated)
SEVERE HEAD INJURY MANAGEMENT PROTOCOL CHECKLIST
Inclusion Criteria:
o SHI with post-resuscitation GCS 8 o Mod HI with GCS >8, admitted for close monitoring due to high risk for deterioration. o Post-craniotomy with brain swelling or potential for further brain swelling.Exclusion Criteria:
o SHI with poor hemodynamics despite maximal resuscitation and unlikely to survive. o Patients with clinical and compatible CT evidence of brainstem death. o Patients with a terminal illness for which active management of the SHI is deemed futile.INITIAL ASSESSMENT AND MANAGEMENT
o Check and stabilize ABCs. Keep MAP 80 mmHg and SpO2 >95% o Intubate ALL patients with GCS 8, if not already intubated in the ED or GW. o If patient with isolated closed HI is hypotensive, look for OTHER CAUSES of hypotension o Put cervical collar in all SHI patients until CS cleared by NS after reviewing CS x-rays o Insert ryles tube to decompress stomachMONITORING
o Hemodynamic monitors for ALL patients: Continuous ECG, pulse oximetry, rectal temp, hourly UOP NIBP (cycle q 30 min; if no IA line inserted, cycle q10-15 min) IA and CVP lines o Neurological monitoring for ALL patients: Hrly GCS, eye signs, limb power and ICP monitorSURGICAL MANAGEMENT: evacuate mass lesions ASAP NEUROLOGICAL MANAGEMENT
o Primary aims: Keep CPP 60-70 mmHg and ICP 55% and PbtO2 > 20 mmHg o Maintain normo-volemia and normo-tension with CVP 6-10 mmHg and UOP 0.5-1.0 ml/kg/hr o If hypotensive, replace aggressively with normal saline, colloids and blood. o May need to start inotropes (norad) to maintain MAP while catching up with blood loss. o Aim for normocapnia (PaCO2 35-40 mmHg) and PaO2 >100 mmHg and SpO2 >95% o Ensure adequate sedation and analgesia o Keep neck neutral and head elevated at 20-30o o Keep Hb 10g/dl and Na+ 140-145 mmol/L o Order NS at 80-120 ml/hr. Add 10-15 ml of 7.45% KCl to each 500 ml unit o Avoid hyperthermia o Order anti-gastritis prophylaxis: IV ranitidine or omeprazole o Order BS control protocol (Keep BSL 4-8 mmol/L) o Order seizure prophylaxis o Nutrition: Start enteral nutrition EARLY (within 24-48 hrs) o DVT prophylaxis: TED stockings sequential calf compression deviceIf ICP >25 mmHg despite the above, consider the first-tier options:
o Consider repeating CT o Order mannitol therapy (0.5-1 g/kg bolus followed by 100 ml q 4-8 hrly) o Drain CSF if EVD in situ o Hypertonic saline therapy (target Na+ at 145-150 mmol/L).If ICP >25 mmHg despite the first-tier options, consider second-tier options:
o Decompressive craniectomy (in consultation with NS) o Barbiturate coma (refer Appendix B: Barbiturate coma protocol) o Hypothermia therapy (active cooling to 33-34oC with cooling blanket + NM blockade)
o Optimized hyperventilation (PaCO2 25-30 mmHg). With SjvO2
Standard hemodynamic monitoring for ALL SHI patients: and/or PbtO2 monitoring. Continuous ECG, pulse oximetry, core temperature (rectal). Hourly urine output and I/O fluid balance All patients with or at risk of intracranial hypertension must have invasive arterial monitoring, CVP line and ICP monitor at admission to NICU. Check whether the patient is in or may be a candidate for research protocols Interventions in stage II to be targeted to clinical picture and multimodality monitoring Guidelines may be modified at the discretion of the consultant in charge Treatment grades III and IV only after approval by NICU consultant
I
10-15 head up, no venous obstruction CPP 60 (CVP 6-10;PAC) SpO295%; PaO2100mmHg, PaCO235-40mmHg Temp37 Blood sugar 4-7 mmol/L C; Propofol 2-5/mg/kg/hr (midazolam 0.1mg/kg/hr Morphine 0-3mg/hr or fentanyl 0.5-2mcg/kg/hr; atracurium Yes
Yes
II
ICP60
No
-Recent CT - low risk of surgical lesion
Start at 0.25-1.0 g/kg bolus followed by 100 ml 20% mannitol q 4-12 hrly CardioQ/PAC, volume, vasoactivates to increase MAP (CPP 90-100) Reduce PaCO2 to 35-40mmHg CPP 25 (Check probe, ? re-CT) No CT No
III
Trial bolus IV anaesthetic ( CSF if EVD propofol 50-200mg) Temp 33-34 , Drain egvasoactive agentsin situ Maintain CPP with fluids and If favourable effect on ICP and CPP start Barbiturate coma (refer Appendix B: Barbiturate coma protocol) Active cooling to 33-34oC with cooling blanket for 24-72 CPP 25 hrs. (refer Hypothermia blanket protocol) (Check probe, ? re-CT)
IV concurrent neuromuscular blockade to prevent shivering V
Surgical lesion? CSF drainage? Role for surgical decompression?
Optimized hyperventilation (PaCO2 25-30 mmHg). Should only be carried out with SjvO2 and/or PbtO2 monitoring to avoid cerebral ischemia caused by the hyperventilation
Surgery Yes
Barbiturate Coma Protocol Indications: High dose barbiturate infusion(thiopentone) for: 1. Haemodynamically stable and 2. Salvageable severe head injury(GCS20-25 mm Hg) 4. refractory to maximal medical and surgical intra-cranial pressure(ICP) lowering therapies. Barbiturate coma lowers ICP by reducing cerebral metabolic demands, cerebral blood flow and cerebral blood volume. 2nd tier option in reducing ICP if ICP remains >20-25 mm Hg despite adding 1 st tier options which include: 1. 2. 3. 4. Repeating CT scan to exclude new or expanding mass lesions Osmotherapy with IV mannitol or hypertonic saline External ventricular drain insertion Mild hyperventilation
Patients who are more likely to respond: 1. Metabolic autoregulation to CO2 still intact(test by noting fall in ICP when patient is transiently hyperventilated at bedside) 2. High frequency waves still present on EEG monitoring(hence preferentially EEG monitor should be present) Prior to initiation of Barbiturate coma: 1. Order and ensure that an inotrope, preferably noradrenaline, is diluted and ready for infusion before starting thiopentone to avoid falls in MAP and CPP. 2. EEG monitoring is recommended during barbiturate coma. Initiation of Barbiturate coma: a. Dilute the thiopentone to 25mg/ml by adding 20 ml of sterile water for inj