Embed Size (px)
Citation preview
Final report
Cancer Plan – Action 24
2009-2011
Authors:
- UZ Brussel: Lore Decoster, Katrien Van Puyvelde, Godelieve Conings
- UZ Leuven: Hans Wildiers, Koen Milisen, Johan Flamaing, Cindy Kenis
- UCL Saint Luc: Frank Cornelis, Pascale Cornette, Ramona Moor
The Cancer Plan - Action 24 with call:" Support to pilot projects in the clinical oncogeriatrics" was
launched in 2009.
The information and views set out in this report are those of the author(s) and do not necessarily
reflect the official opinion of the Minister of Public Health or the FPS Health.
The FPS Health does not guarantee the accuracy of the data included in this study.
Neither the FPS Health nor any person acting on the FPS Health’s behalf may be held
responsible for the use which may be made of the information contained therein.
1. Selected projects
Fifteen pilot projects were initially selected, one resigned within the first year (project n° 022) and
the other included only one patient due to staff problems (project n°004). Finally 13 projects
remained of which eight multi-centric and five mono-centric. Two out of 13 projects were
randomized trials, two qualitative and nine were observational.
The projects had different end points:
o 9 projects focused on the use of screening tools and / or (comprehensive) geriatric
assessment ((C)GA) in daily clinical practice;
o 1 project analyzed the relation between sarcopenia in older cancer patients and functional
outcome;
o 1 project focused on advanced care planning in palliative older cancer patients
o 1 project analyzed the experiences of older cancer patients and their families during cancer
therapy;
o 1 project examined the relation between screening and toxicity of chemotherapy in older
cancer patients.
2. Patient characteristics
- The number of included patients differed in the different projects, varying from 32 included
patients to 3518.
- Seven projects (005, 008, 010, 011, 013, 014 and 015) included patients from 70 year and above,
five included patients from 65 year and more (001, 016, 018, 021 and 024) and one (020)
included from 60 year and more.
- Most of the projects included various types of tumors except two projects:
o 1 project including head and neck tumors (018)
o 1 project including hematologic malignancies (001).
3. Screening tools and geriatric assessment used
- Three projects did not use a screening tool to detect frail older patients (001, 011 and 014).
- The other projects all used one or more screening tools to identify patients in need of further
evaluation by GA (see Table 1) . In total six different screening tools were assessed.
- Six studies performed comparative analysis of different screening tools: projects n° 005, 013,
015, 018, 020 and 021.
Table 1: projects using screening tools
Screening tool Project number
G8 005
015
016
018
021
VES-13 008
018
020
ISAR 013
015
020
GRP (= fTRST) 005
010
024
SEGA 013
020
GFI 021
- One project did not perform a GA, in the other projects the use of GA was very variable with the
use of different instruments within the GA and cut-off scores.
This wide variation illustrates the need for a standardized approach in Belgium, both regarding
screening tools and GA.
4. Results and conclusions
The results and conclusions of all projects are listed in table 2.
Three of the 13 projects did not report final results and/or conclusions in the final report: project n°
001, 014 and 016. Their analysis was still running at the moment of the final reporting.
4.1 Conclusions on screening tools
Four projects had as primary objective to validate the use of screening tools to detect vulnerable
patients in the oncogeriatric population.
1/ In project n° 018 the VES-13 and G8 were compared with GA in older patients with head
and neck cancer . In this study G8 was superior as a screening tool with the highest
sensitivity. A different cut off from the one initially validated for G8 (12 instead of 14) was
proposed in head and neck cancer patients, however due to the differences in CGA items and
cut off it is impossible to compare the study with the original validation of G8 (Bellera et al).
In addition a combination of both screening tool was proposed (VES-13+(17-G8)) resulting in
higher sensitivity and specificity than the G8 or VES-13 alone.
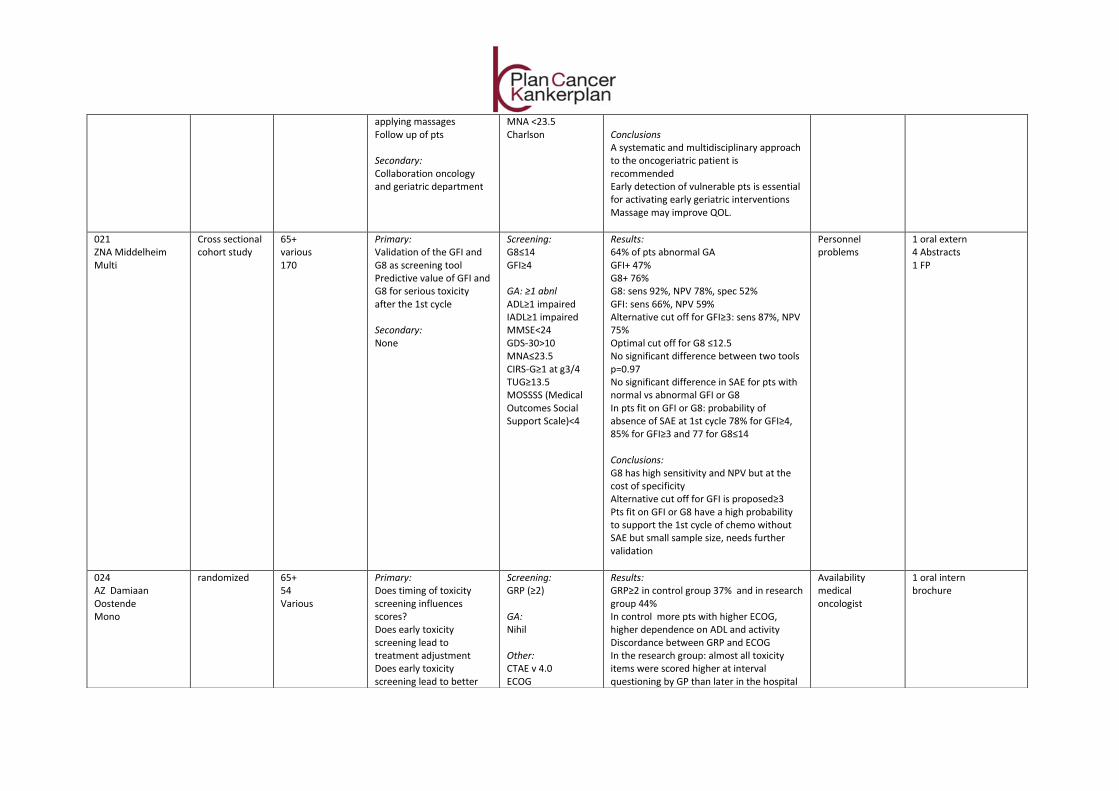
2/ GFI and G8 were compared with GA in project n°021. G8 demonstrated the best sensitivity
and negative predictive value (NPV) but at the cost of the specificity. Both tools were also
correlated with the occurrence of serious adverse events after the first cycle of
chemotherapy. Patients with a normal screening on G8 and GFI had the best probability to
support the chemotherapy without serious adverse effects.
3/ In project n° 015 the ISAR and G8 were compared with GA. This study concluded that
according to the ROC curves there was no significant difference between the ISAR and the G8
for sensitivity and specificity and they concluded that a high prevalence of geriatric
syndromes and comorbidities are associated with a positive ISAR and G8 but not with the
tumor stage. To note is that in this study a much lower sensitivity, specificity and NPV for the
G8 was observed compared to other studies and the confidence intervals. In addition we
have some statistical concerns regarding the results of this study (for example authors report
2 values for AUC ROC curves for ISAR and the confidence intervals for all AUC do not seem to
be correct).
4/ Finally in project n°020 the VES-13, ISAR and SEGA were used to detect vulnerable patient,
but no comparison was made with a GA, they only described the total number of patients
who screened positive, and no sensitivity or specificity of the tools were described.
4.2 Conclusions on GA
Five projects (project n° 005, 008, 013, and 020) had as mean objective to study the importance of a
geriatric assessment to detect unknown geriatric problems and/or the impact of the geriatric
assessment on therapy decision, quality of life and/or functionality.
1/ Project n° 005 was the largest project of the 13 selected. In this multi-centric GA detected new
problems in all geriatric domains in a large number of patients (51%) but the influence on
treatment decisions was limited and in a minority of patients this lead to directed interventions.
It was encouraging to observe a gradually increase in awareness in physicians treating cancer
patients of the implementation of GA in the management of older cancer patients.
2/ In project n°008 implementation of GA also led to identification of new health problems and
the need of geriatric interventions. The impact on functionality still needs to be validated and
further analysis is ongoing.
3/ Project n°020 concluded that early social interventions lead to shorter hospital stays.
4/ Finally the last study on GA (project n° 013) demonstrated the identification of geriatric
problems, and the need to reinforce geriatric interventions from paramedics.
To conclude, performance of GA detects new problems in a significant proportion of older cancer
patients. The impact of directed geriatric interventions in case of impairment on GA as well as follow-
up need further investigation. This is an important focus in the ongoing ‘Cancer Plan – Action 24’ and
the scientific committee has made it an important aim of the general database.
4.3 Conclusions on the relationship between screening/CGA and treatment related toxicity
One study (project n° 024) focused only on chemotherapy toxicity and concluded that the timing of
chemotherapy toxicity assessment influences the amount of G1 toxicity but that this did not lead to
an adaptation of the chemotherapy.
4.4 Conclusions regarding advanced care planning
One quantitative study (project n° 011) focused on palliative care and advanced care planning. It
demonstrated a risk of pseudo-participation of the patient in decisions about advanced care
planning, however the majority of older patients experienced positively the dialogue about advanced
care planning.
4.5 Conclusions regarding experiences of older cancer patients
The second qualitative study (project n° 010) analyzed the experience of elderly and their caregivers
during cancer therapy and concluded that active listening to their life stories and an individual
approach is very important.
5. Major problems encountered by different projects
Most of the projects had problems with the start because of a lack of personnel and problems with
recruitment of patients. Some projects report the problems of recruitments due to high refusal of the
patients probably due to the announcement of the cancer diagnosis. In addition a lack of geriatric
culture and resistance from other specialties was observed.
6. Conclusions
The ‘Cancer Plan – Action 24’ on pilot projects in clinical oncogeriatrics was launched in 2009 and
included 13 projects.
These projects were an important first step in the optimalisation of the care for older cancer
patients. Thanks to the projects thousands of older cancer patients underwent some form of geriatric
evaluation and support. The ‘Cancer Plan - Action 24’ brought up an interest in oncogeriatrics in
many oncologists, hematologists, geriatricians and nurses. We can now state that geriatric oncology
lives in Belgium and that Belgium became one of the pioneers in the multidisciplinary approach of
older cancer patients. This is in our belief one of the most important realizations of the ‘Cancer Plan -
Action 24’.
At present three projects have not reported final results and/or conclusions.
Different projects have clearly shown that the performance of GA results in detection of previously
unknown problems involving all domains of the GA. However so far, little is known on the effect of
directed interventions and follow-up on care for older cancer patients, including quality of life,
treatment decisions, treatment tolerance. Further evaluation of this aspect is warranted to formulate
formal recommendations. This is why this is a main focus of the scientific committee in the current
Action 24 of the Cancer Plan (2012-15).
Ideally all older cancer patients should benefit from GA. However this approach it resource-
consuming: both in terms of time and finances. In order to limit the number of fit patients that
undergo a full GA, research has focused on screening tools. This was also the case in the ‘Cancer Plan
– Action 24’. All three projects focusing on screening have validated the G8 as optimal screening tool.
Finally, advanced care planning with participation of older cancer patients as well as active listening
seems an important aspect in the management of older cancer patients.
To conclude, the first projects of the ‘Cancer Plan – Action 24’ have demonstrated the feasibility of
screening followed by geriatric assessment in older cancer patients. So far, G8 has demonstrated the
highest sensitivity as a screening tool. The performance of GA leads to detection of unknown
problems but the current projects of the ‘Cancer Plan – Action 24’ should give us more information
on the implementation of geriatric interventions and follow up. In the future, it seems important to
achieve a consensus on which screening tool to use as well as on a standardized GA and cut off value,
in order to get a standardized approach in Belgium.
7. Recommendations
Some points for improvement need to be taken into account for the future:
1. It was evident that several small projects had the same study design and the same objective.
However, since there is no standard geriatric assessment (for the number of items, tests
included for each item and cut off value for impairment) it is impossible to perform
interstudy comparisons. The fundamental questions raises whether the FPS should not do
more efforts to stimulate collaborations. In France for instance, the government wrote a
grant proposal, and only selected 1 project, while the other applicants were obliged to
collaborate in the selected project. This kind of selection unifies efforts in a better way
whereas in the ‘Cancer Plan – Action 24 2009-11', there were sometimes small single center
studies with limited yield, and 2 funded projects didn’t start. In ‘Cancer Plan – Action 24
2012-15’, there is already better collaboration and global structuring thanks to the
establishment by the FPS of a scientific committee that overviews all the ongoing projects.

But there were still 15 projects selected with often similar or overlapping goals, and we
recommend to use the ‘French’ model for the next phase of the Cancer Plan – Action 24, with
1 project selected on a competitive basis or designed by the present scientific committee,
where the other applicants are obliged to collaborate to this project.
2. This raises also the issue of project financing. For ‘Cancer Plan – Action 24 2009-11’, financing
varied per project, while for ‘Cancer Plan – Action 24 2012-15’, the same amount of money
was given for each project/center, independent of the size of the hospital or the patients
included in the study. This creates inequality, disadvantages for large centers, and does not
motivate to include many patients in studies. There are mechanisms to deal with this. For
instance, in project 5, there were 10 centers involved, and the money was distributed
according to an upfront defined distribution key for each inclusion. This study included by far
the largest number of patients. The FPS could use this financing mechanism also in future
studies.
3. Several centers received more than one financing through participation in different projects.
This is also a fundamental question whether this strategy should be maintained in the future,
since some centers received financing for 2 projects, while projects were sometimes (at least
partially) overlapping in terms of efforts and organization, even if the objectives of the 2
selected projects where different. It should be acknowledged that the choice of sometimes
small single centers has not changed in the second call for projects of the ‘Cancer Plan –
Action 24 2012-15’. The FPS should reflect on future organizing and financing projects of this
kind.
4. It should also be acknowledged that care for older individuals is not specific for oncology.
Future projects should focus much more on interaction with the Belgian geriatric care
program including internal liaison for older hospitalized patients. And there is also a great
need for transmural transfer of geriatric assessment data, between general practitioners,
nursing homes and hospitals. There are currently projects in Belgium in geriatric care, like the
BELRAI project, but there is currently no interaction with the geriatric oncology actions. In
the future, these domains should be integrated as much as possible. The health authorities
should take this integration into account in the development of future projects in both
geriatrics and oncology.
Future calls for the next step of ‘Cancer Plan – Action 24’ should be well streamlined with the
future national development of the geriatric care program including internal liaison. There is
a need of a larger vision of geriatrics, with more coordination between the different
specialties and programs.
5. Finally, a consensus should be made on a uniform use of a screening tool and geriatric
assessment in order to achieve a clear overview of the management of older cancer patients.
In addition the importance of interventions and follow up is necessary.

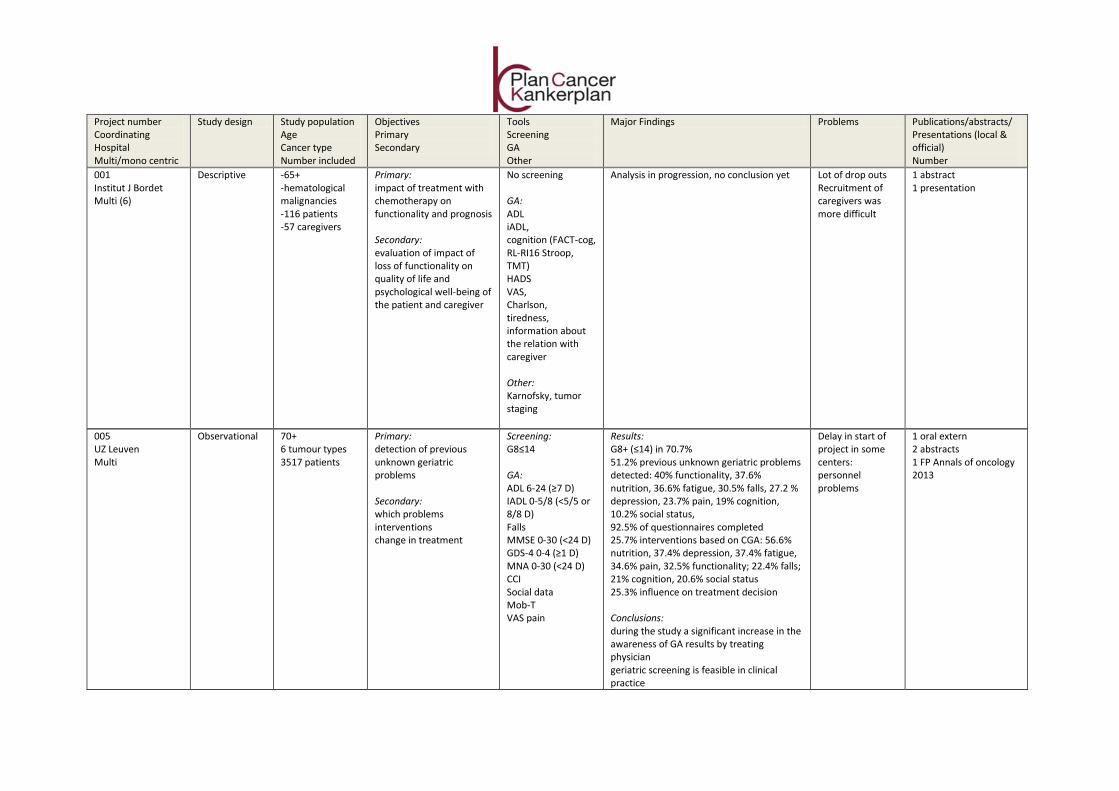
001 Institut J Bordet Multi (6)
Descriptive -65+ -hematological malignancies -116 patients -57 caregivers
Primary: impact of treatment with chemotherapy on functionality and prognosis Secondary: evaluation of impact of loss of functionality on quality of life and psychological well-being of the patient and caregiver
No screening GA: ADL iADL, cognition (FACT-cog, RL-RI16 Stroop, TMT) HADS VAS, Charlson, tiredness, information about the relation with caregiver Other: Karnofsky, tumor staging
Analysis in progression, no conclusion yet Lot of drop outs Recruitment of caregivers was more difficult
1 abstract 1 presentation
Project number Coordinating Hospital Multi/mono centric
Study design Study population Age Cancer type Number included
Objectives Primary Secondary
Tools Screening GA Other
Major Findings Problems Publications/abstracts/ Presentations (local & official) Number
005 UZ Leuven Multi
Observational
70+ 6 tumour types 3517 patients
Primary: detection of previous unknown geriatric problems Secondary: which problems interventions change in treatment
Screening: G8≤14 GA: ADL 6-24 (≥7 D) IADL 0-5/8 (<5/5 or 8/8 D) Falls MMSE 0-30 (<24 D) GDS-4 0-4 (≥1 D) MNA 0-30 (<24 D) CCI Social data Mob-T VAS pain
Results: G8+ (≤14) in 70.7% 51.2% previous unknown geriatric problems detected: 40% functionality, 37.6% nutrition, 36.6% fatigue, 30.5% falls, 27.2 % depression, 23.7% pain, 19% cognition, 10.2% social status, 92.5% of questionnaires completed 25.7% interventions based on CGA: 56.6% nutrition, 37.4% depression, 37.4% fatigue, 34.6% pain, 32.5% functionality; 22.4% falls; 21% cognition, 20.6% social status 25.3% influence on treatment decision Conclusions: during the study a significant increase in the awareness of GA results by treating physician geriatric screening is feasible in clinical practice
Delay in start of project in some centers: personnel problems
1 oral extern 2 abstracts 1 FP Annals of oncology 2013
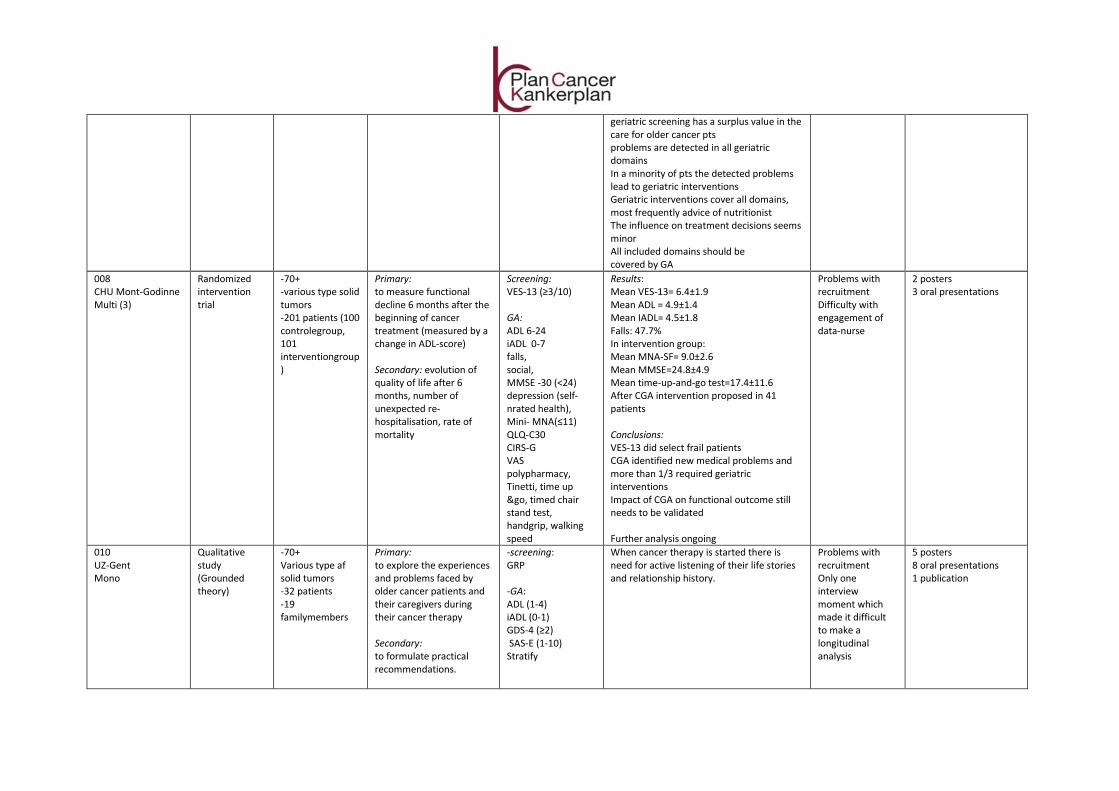
008 CHU Mont-Godinne Multi (3)
Randomized intervention trial
-70+ -various type solid tumors -201 patients (100 controlegroup, 101 interventiongroup)
Primary: to measure functional decline 6 months after the beginning of cancer treatment (measured by a change in ADL-score) Secondary: evolution of quality of life after 6 months, number of unexpected re-hospitalisation, rate of mortality
Screening: VES-13 (≥3/10) GA: ADL 6-24 iADL 0-7 falls, social, MMSE -30 (<24) depression (self-nrated health), Mini- MNA(≤11) QLQ-C30 CIRS-G VAS polypharmacy, Tinetti, time up &go, timed chair stand test, handgrip, walking speed
Results: Mean VES-13= 6.4±1.9 Mean ADL = 4.9±1.4 Mean IADL= 4.5±1.8 Falls: 47.7% In intervention group: Mean MNA-SF= 9.0±2.6 Mean MMSE=24.8±4.9 Mean time-up-and-go test=17.4±11.6 After CGA intervention proposed in 41 patients Conclusions: VES-13 did select frail patients CGA identified new medical problems and more than 1/3 required geriatric interventions Impact of CGA on functional outcome still needs to be validated Further analysis ongoing
Problems with recruitment Difficulty with engagement of data-nurse
2 posters 3 oral presentations
010 UZ-Gent Mono
Qualitative study (Grounded theory)
-70+ Various type af solid tumors -32 patients -19 familymembers
Primary: to explore the experiences and problems faced by older cancer patients and their caregivers during their cancer therapy Secondary: to formulate practical recommendations.
-screening: GRP -GA: ADL (1-4) iADL (0-1) GDS-4 (≥2) SAS-E (1-10) Stratify
When cancer therapy is started there is need for active listening of their life stories and relationship history.
Problems with recruitment Only one interview moment which made it difficult to make a longitudinal analysis
5 posters 8 oral presentations 1 publication
geriatric screening has a surplus value in the care for older cancer pts problems are detected in all geriatric domains In a minority of pts the detected problems lead to geriatric interventions Geriatric interventions cover all domains, most frequently advice of nutritionist The influence on treatment decisions seems minor All included domains should be covered by GA
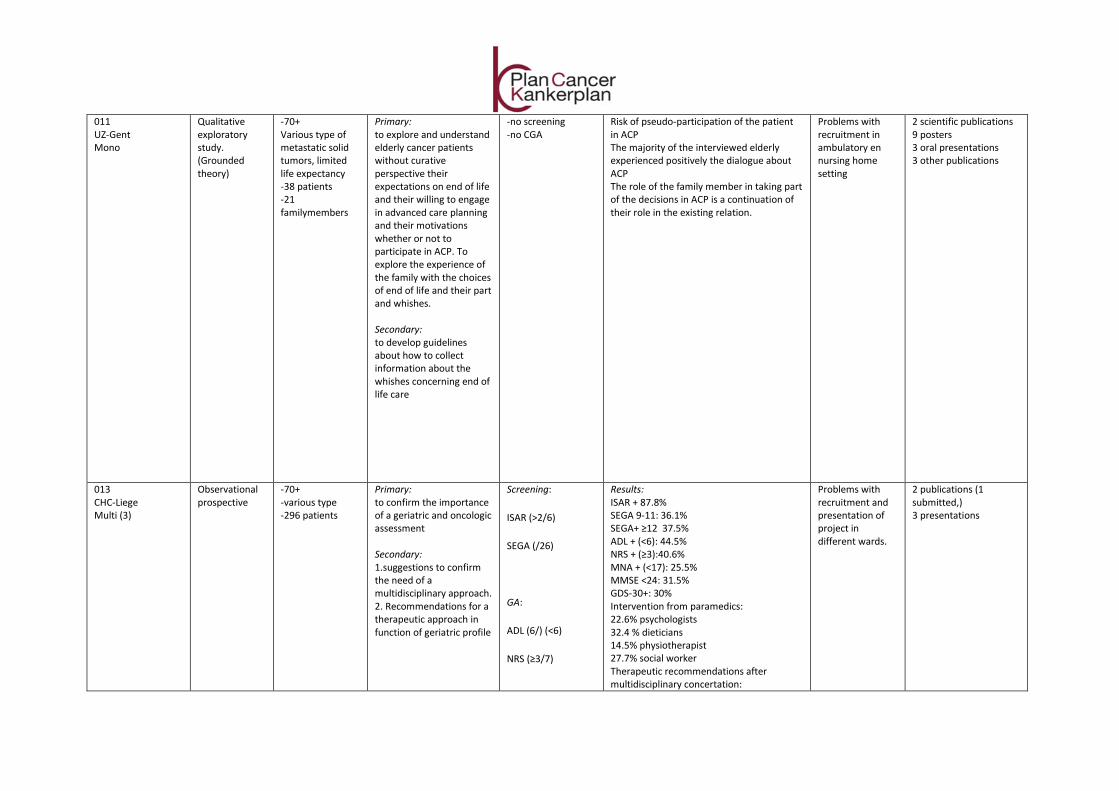
011 UZ-Gent Mono
Qualitative exploratory study. (Grounded theory)
-70+ Various type of metastatic solid tumors, limited life expectancy -38 patients -21 familymembers
Primary: to explore and understand elderly cancer patients without curative perspective their expectations on end of life and their willing to engage in advanced care planning and their motivations whether or not to participate in ACP. To explore the experience of the family with the choices of end of life and their part and whishes. Secondary: to develop guidelines about how to collect information about the whishes concerning end of life care
-no screening -no CGA
Risk of pseudo-participation of the patient in ACP The majority of the interviewed elderly experienced positively the dialogue about ACP The role of the family member in taking part of the decisions in ACP is a continuation of their role in the existing relation.
Problems with recruitment in ambulatory en nursing home setting
2 scientific publications 9 posters 3 oral presentations 3 other publications
013 CHC-Liege Multi (3)
Observational prospective
-70+ -various type -296 patients
Primary: to confirm the importance of a geriatric and oncologic assessment Secondary: 1.suggestions to confirm the need of a multidisciplinary approach. 2. Recommendations for a therapeutic approach in function of geriatric profile
Screening:
ISAR (>2/6)
SEGA (/26)
GA:
ADL (6/) (<6)
NRS (≥3/7)
Results: ISAR + 87.8% SEGA 9-11: 36.1% SEGA+ ≥12 37.5% ADL + (<6): 44.5% NRS + (≥3):40.6% MNA + (<17): 25.5% MMSE <24: 31.5% GDS-30+: 30% Intervention from paramedics: 22.6% psychologists 32.4 % dieticians 14.5% physiotherapist 27.7% social worker Therapeutic recommendations after multidisciplinary concertation:
Problems with recruitment and presentation of project in different wards.
2 publications (1 submitted,) 3 presentations
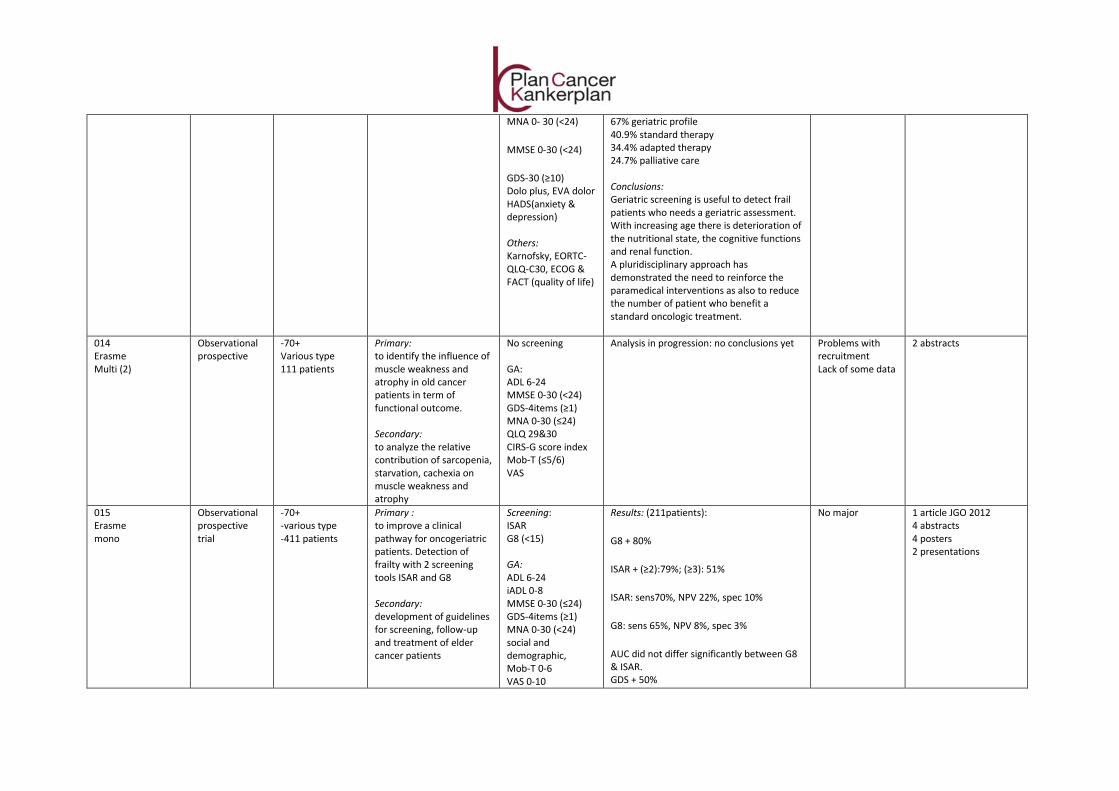
MNA 0- 30 (<24)
MMSE 0-30 (<24)
GDS-30 (≥10) Dolo plus, EVA dolor HADS(anxiety & depression) Others: Karnofsky, EORTC- QLQ-C30, ECOG & FACT (quality of life)
67% geriatric profile 40.9% standard therapy 34.4% adapted therapy 24.7% palliative care Conclusions: Geriatric screening is useful to detect frail patients who needs a geriatric assessment. With increasing age there is deterioration of the nutritional state, the cognitive functions and renal function. A pluridisciplinary approach has demonstrated the need to reinforce the paramedical interventions as also to reduce the number of patient who benefit a standard oncologic treatment.
014 Erasme Multi (2)
Observational prospective
-70+ Various type 111 patients
Primary: to identify the influence of muscle weakness and atrophy in old cancer patients in term of functional outcome. Secondary: to analyze the relative contribution of sarcopenia, starvation, cachexia on muscle weakness and atrophy
No screening GA: ADL 6-24 MMSE 0-30 (<24) GDS-4items (≥1) MNA 0-30 (≤24) QLQ 29&30 CIRS-G score index Mob-T (≤5/6) VAS
Analysis in progression: no conclusions yet Problems with recruitment Lack of some data
2 abstracts
015 Erasme mono
Observational prospective trial
-70+ -various type -411 patients
Primary : to improve a clinical pathway for oncogeriatric patients. Detection of frailty with 2 screening tools ISAR and G8 Secondary: development of guidelines for screening, follow-up and treatment of elder cancer patients
Screening: ISAR G8 (<15) GA: ADL 6-24 iADL 0-8 MMSE 0-30 (≤24) GDS-4items (≥1) MNA 0-30 (<24) social and demographic, Mob-T 0-6 VAS 0-10
Results: (211patients):
G8 + 80%
ISAR + (≥2):79%; (≥3): 51%
ISAR: sens70%, NPV 22%, spec 10%
G8: sens 65%, NPV 8%, spec 3%
AUC did not differ significantly between G8 & ISAR. GDS + 50%
No major 1 article JGO 2012 4 abstracts 4 posters 2 presentations
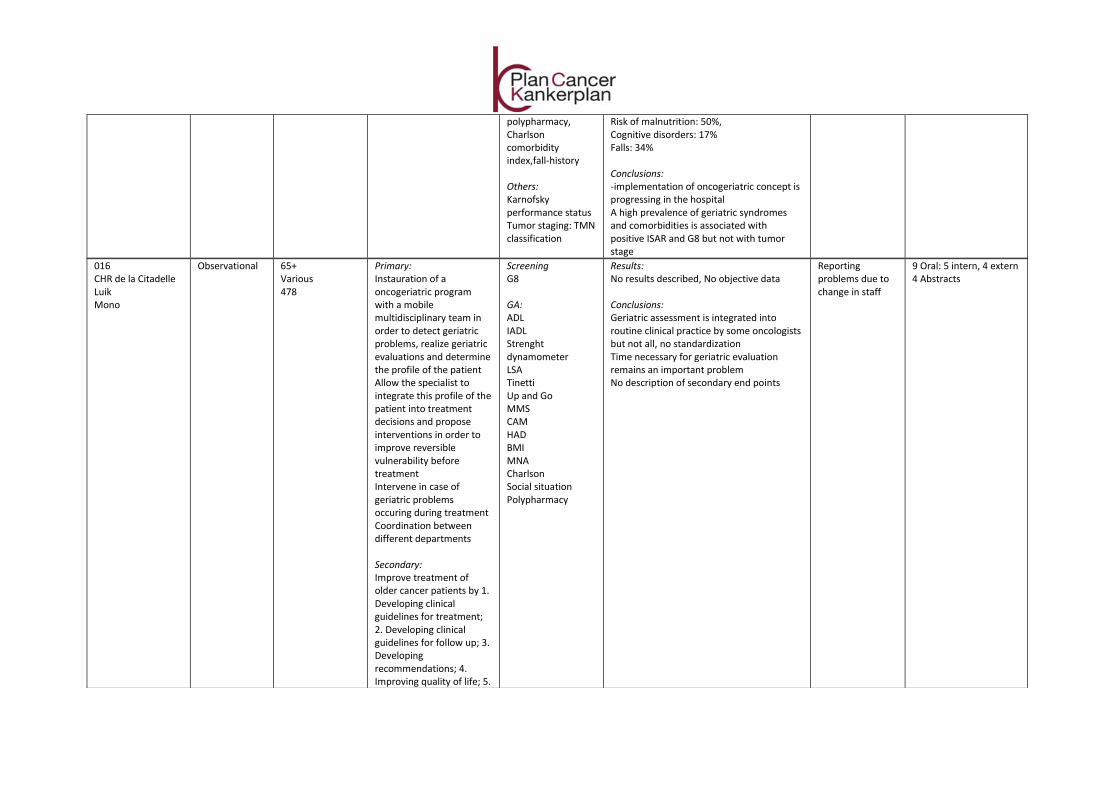
polypharmacy, Charlson comorbidity index,fall-history Others: Karnofsky performance status Tumor staging: TMN classification
Risk of malnutrition: 50%, Cognitive disorders: 17% Falls: 34% Conclusions: -implementation of oncogeriatric concept is progressing in the hospital A high prevalence of geriatric syndromes and comorbidities is associated with positive ISAR and G8 but not with tumor stage
016 CHR de la Citadelle Luik Mono
Observational 65+ Various 478
Primary: Instauration of a oncogeriatric program with a mobile multidisciplinary team in order to detect geriatric problems, realize geriatric evaluations and determine the profile of the patient Allow the specialist to integrate this profile of the patient into treatment decisions and propose interventions in order to improve reversible vulnerability before treatment Intervene in case of geriatric problems occuring during treatment Coordination between different departments Secondary: Improve treatment of older cancer patients by 1. Developing clinical guidelines for treatment; 2. Developing clinical guidelines for follow up; 3. Developing recommendations; 4. Improving quality of life; 5.
Screening G8 GA: ADL IADL Strenght dynamometer LSA Tinetti Up and Go MMS CAM HAD BMI MNA Charlson Social situation Polypharmacy
Results: No results described, No objective data Conclusions: Geriatric assessment is integrated into routine clinical practice by some oncologists but not all, no standardization Time necessary for geriatric evaluation remains an important problem No description of secondary end points
Reporting problems due to change in staff
9 Oral: 5 intern, 4 extern 4 Abstracts
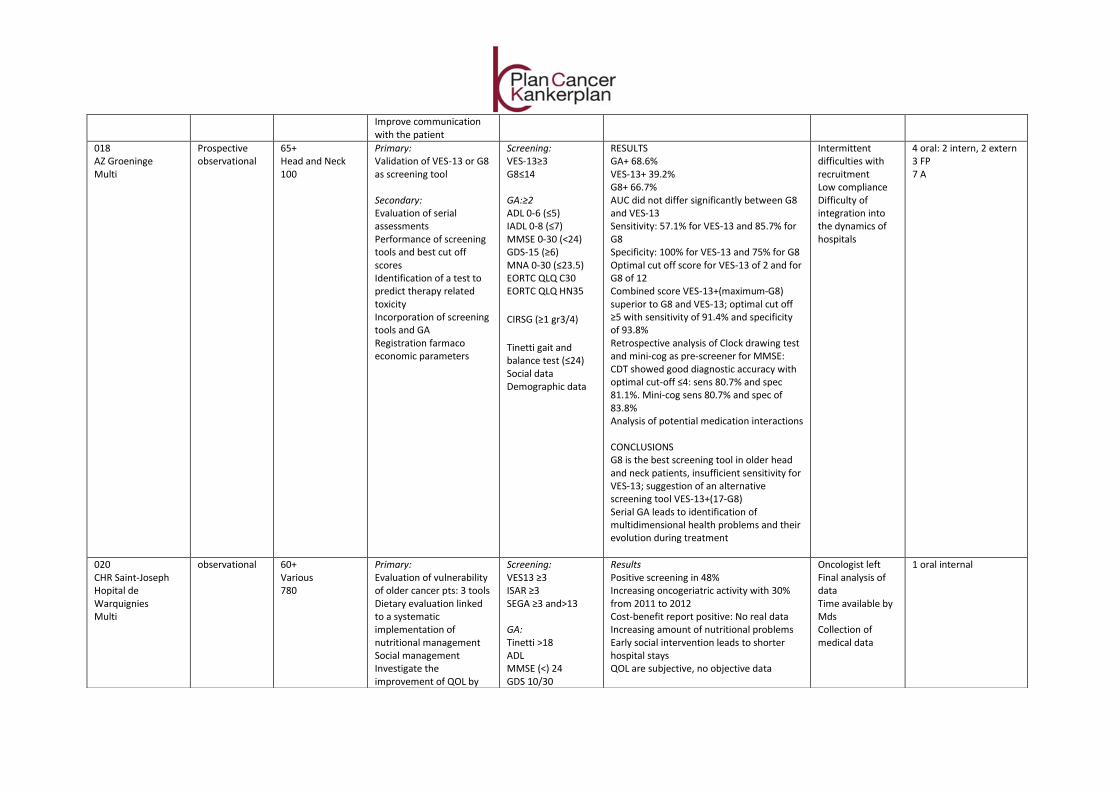
Improve communication with the patient
018 AZ Groeninge Multi
Prospective observational
65+ Head and Neck 100
Primary: Validation of VES-13 or G8 as screening tool Secondary: Evaluation of serial assessments Performance of screening tools and best cut off scores Identification of a test to predict therapy related toxicity Incorporation of screening tools and GA Registration farmaco economic parameters
Screening: VES-13≥3 G8≤14 GA:≥2 ADL 0-6 (≤5) IADL 0-8 (≤7) MMSE 0-30 (<24) GDS-15 (≥6) MNA 0-30 (≤23.5) EORTC QLQ C30 EORTC QLQ HN35
CIRSG (≥1 gr3/4)
Tinetti gait and balance test (≤24) Social data Demographic data
RESULTS GA+ 68.6% VES-13+ 39.2% G8+ 66.7% AUC did not differ significantly between G8 and VES-13 Sensitivity: 57.1% for VES-13 and 85.7% for G8 Specificity: 100% for VES-13 and 75% for G8 Optimal cut off score for VES-13 of 2 and for G8 of 12 Combined score VES-13+(maximum-G8) superior to G8 and VES-13; optimal cut off ≥5 with sensitivity of 91.4% and specificity of 93.8% Retrospective analysis of Clock drawing test and mini-cog as pre-screener for MMSE: CDT showed good diagnostic accuracy with optimal cut-off ≤4: sens 80.7% and spec 81.1%. Mini-cog sens 80.7% and spec of 83.8% Analysis of potential medication interactions CONCLUSIONS G8 is the best screening tool in older head and neck patients, insufficient sensitivity for VES-13; suggestion of an alternative screening tool VES-13+(17-G8) Serial GA leads to identification of multidimensional health problems and their evolution during treatment
Intermittent difficulties with recruitment Low compliance Difficulty of integration into the dynamics of hospitals
4 oral: 2 intern, 2 extern 3 FP 7 A
020 CHR Saint-Joseph Hopital de Warquignies Multi
observational 60+ Various 780
Primary: Evaluation of vulnerability of older cancer pts: 3 tools Dietary evaluation linked to a systematic implementation of nutritional management Social management Investigate the improvement of QOL by
Screening: VES13 ≥3 ISAR ≥3 SEGA ≥3 and>13 GA: Tinetti >18 ADL MMSE (<) 24 GDS 10/30
Results Positive screening in 48% Increasing oncogeriatric activity with 30% from 2011 to 2012 Cost-benefit report positive: No real data Increasing amount of nutritional problems Early social intervention leads to shorter hospital stays QOL are subjective, no objective data
Oncologist left Final analysis of data Time available by Mds Collection of medical data
1 oral internal
applying massages Follow up of pts Secondary: Collaboration oncology and geriatric department
MNA <23.5 Charlson
Conclusions A systematic and multidisciplinary approach to the oncogeriatric patient is recommended Early detection of vulnerable pts is essential for activating early geriatric interventions Massage may improve QOL.
021 ZNA Middelheim Multi
Cross sectional cohort study
65+ various 170
Primary: Validation of the GFI and G8 as screening tool Predictive value of GFI and G8 for serious toxicity after the 1st cycle Secondary: None
Screening: G8≤14 GFI≥4 GA: ≥1 abnl ADL≥1 impaired IADL≥1 impaired MMSE<24 GDS-30>10 MNA≤23.5 CIRS-G≥1 at g3/4 TUG≥13.5 MOSSSS (Medical Outcomes Social Support Scale)<4
Results: 64% of pts abnormal GA GFI+ 47% G8+ 76% G8: sens 92%, NPV 78%, spec 52% GFI: sens 66%, NPV 59% Alternative cut off for GFI≥3: sens 87%, NPV 75% Optimal cut off for G8 ≤12.5 No significant difference between two tools p=0.97 No significant difference in SAE for pts with normal vs abnormal GFI or G8 In pts fit on GFI or G8: probability of absence of SAE at 1st cycle 78% for GFI≥4, 85% for GFI≥3 and 77 for G8≤14 Conclusions: G8 has high sensitivity and NPV but at the cost of specificity Alternative cut off for GFI is proposed≥3 Pts fit on GFI or G8 have a high probability to support the 1st cycle of chemo without SAE but small sample size, needs further validation
Personnel problems
1 oral extern 4 Abstracts 1 FP
024 AZ Damiaan Oostende Mono
randomized 65+ 54 Various
Primary: Does timing of toxicity screening influences scores? Does early toxicity screening lead to treatment adjustment Does early toxicity screening lead to better
Screening: GRP (≥2) GA: Nihil Other: CTAE v 4.0 ECOG
Results: GRP≥2 in control group 37% and in research group 44% In control more pts with higher ECOG, higher dependence on ADL and activity Discordance between GRP and ECOG In the research group: almost all toxicity items were scored higher at interval questioning by GP than later in the hospital
Availability medical oncologist
1 oral intern brochure
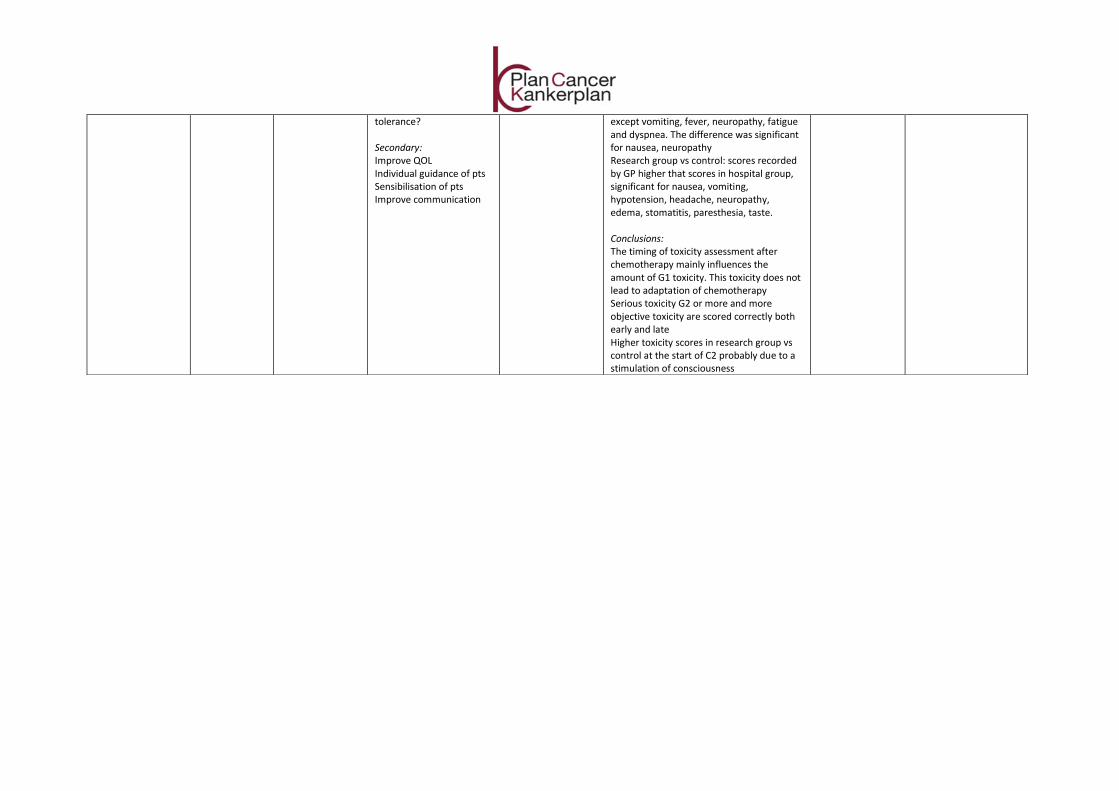
tolerance? Secondary: Improve QOL Individual guidance of pts Sensibilisation of pts Improve communication
except vomiting, fever, neuropathy, fatigue and dyspnea. The difference was significant for nausea, neuropathy Research group vs control: scores recorded by GP higher that scores in hospital group, significant for nausea, vomiting, hypotension, headache, neuropathy, edema, stomatitis, paresthesia, taste. Conclusions: The timing of toxicity assessment after chemotherapy mainly influences the amount of G1 toxicity. This toxicity does not lead to adaptation of chemotherapy Serious toxicity G2 or more and more objective toxicity are scored correctly both early and late Higher toxicity scores in research group vs control at the start of C2 probably due to a stimulation of consciousness
KPC_24_B_026
Cancerplan – Action 24
Projects 2009-2011
Summary in Dutch and French
The information and views set out in this report are those of the author(s) and do not
necessarily reflect the official opinion of the Minister of Public Health or the FPS Health.
The FPS Health does not guarantee the accuracy of the data included in this study.
Neither the FPS Health nor any person acting on the FPS Health’s behalf may be held
responsible for the use which may be made of the information contained therein.
KPC_24_B_026
Kankerplan – Actie 24
Projecten 2009-2011 (samenvatting)
Auteurs:
- UZ Brussel: Lore Decoster, Katrien Van Puyvelde, Godelieve Conings
- UZ Leuven: Hans Wildiers, Koen Milisen, Johan Flamaing, Cindy Kenis
- UCL Saint Luc: Frank Cornelis, Pascale Cornette, Ramona Moor
'Kankerplan - Actie 24' werd gelanceerd in 2009 met als doel de ondersteuning van
pilootprojecten in de klinische oncogeriatrie.
1. Geselecteerde projecten
In totaal werden dertien projecten geselecteerd waarvan acht multicentrisch en vijf
monocentrisch.
Deze projecten hadden zeer verschillende eindpunten, met name:
- het gebruik van screeningsinstrumenten en/of geriatrische evaluatie in de
dagdagelijkse praktijk (9 projecten)
- de relatie tussen sarcopenie in oudere patiënten met kanker en functionele status (1
project)
- ‘advanced care planning’ in oudere patiënten met kanker (1 project)
- de ervaringen van oudere patiënten met kanker en hun familie tijdens de kanker
behandeling (1 project)
- de relatie tussen screening en toxiciteit in oudere patiënten met kanker (1 project)
Het aantal patiënten geïncludeerd in de verschillende projecten varieert van 32 tot 3518. In
7/13 projecten werden patiënten vanaf 70 jaar geïncludeerd, in 5/13 vanaf 65 jaar of en in 1
vanaf 60 jaar. Elf projecten includeerden verschillende types tumoren, terwijl twee projecten
zich beperkten tot één tumor type.
2. Resultaten van de geselecteerde projecten
Van drie projecten werden er geen eindresultaten verkregen.
2.1 Screeningsinstrumenten
Vier projecten onderzochten het gebruik van screeningsinstrumenten om fragiele
patiënten te identificeren in de oudere kankerpopulatie.
Verschillende screeningsinstrumenten werden gebruikt met name G8, GFI, VES-13, ISAR
en SEGA. In twee projecten blijkt vertoont de G8 de beste sensitiviteit in vergelijking met
respectievelijk de VES-13 en de GFI. In een derde project zijn G8 en ISAR gelijkwaardig.
2.2 Geriatrische evaluatie
In vijf projecten was het primair objectief het beschrijven van de impact van een
geriatrische evaluatie in de detectie van onbekende geriatrische problemen en/of de
impact op therapiebeslissingen, levenskwaliteit en functionele status.
Al deze projecten toonden aan dat een geriatrische evaluatie nieuwe problemen
detecteert in een belangrijke proportie oudere patiënten met kanker.
2.3 Verband tussen screening/geriatrische evaluatie en behandelingsgerelateerde toxiciteit
Eén project richtte zich op chemotherapiegerelateerde toxiciteit in oudere patiënten met
kanker en concludeerde dat het tijdstip waarop deze toxiciteit werd nagevraagd een
invloed had op het aantal graad 1 neveneffecten maar niet op het vervolg van de
behandeling.
2.4 Advanced care planning
Eén studie richtte zich op de palliatieve zorgen en advanced care planning en concludeerde
dat de meerderheid van oudere patiënten met kanker de dialoog over advanced care
planning als positief ervaarden.
2.5 Ervaringen van oudere patiënten met kanker tijdens de behandeling
Eén studie onderzocht de ervaringen van ouderen en hun mantelzorgers tijdens de
kankerbehandeling en besloot dat actief luisteren en een individuele benadering
belangrijk is.
3. Algemeen besluit
Tussen 2009 en 2011 ondersteunde Kankerplan - Actie 24 in totaal 13 pilootprojecten in de
klinische oncogeriatrie.
Deze projecten werden een belangrijke eerste stap in de optimalisatie van de zorg voor een
steeds groeiende groep oudere patiënten met kanker. Met behulp van deze ondersteuning,
genoten duizenden oudere patiënten met kanker voor het eerst een vorm van geriatrische
evaluatie en bijhorende ondersteuning. Kankerplan - Actie 24 wekte bij vele artsen betrokken
in de behandeling van patiënten met kanker interesse op voor oncogeriatrie en bevorderde
de samenwerking met geriatrische diensten.
De verschillende projecten hebben duidelijk aangetoond dat het uitvoeren van een
geriatrische evaluatie problemen in de verschillende geriatrische domeinen kan identificeren.
Gezien een dergelijke evaluatie niet haalbaal lijkt in alle oudere patiënten met kanker (zowel
financieel als op gebied van tijd) lijkt een eerste selectie door gebruik te maken van een
screeningsinstrument aangewezen. Alle projecten met de focus op screening hebben de G8
geoordeeld als een goed screeningsinstrument.
Ten slotte lijken advanced care planning met participatie van de oudere patiënt alsook actief
luisteren een belangrijk onderdeel uit te maken in de zorg van oudere patiënten met kanker.
In conclusie hebben de eerste projecten van 'Kankerplan - Actie 24' de relevantie en
haalbaarheid aangetoond van het gebruik van een screeningsinstrument gevolgd door een
geriatrische evaluatie in oudere patiënten met kanker in de dagdagelijkse praktijk. Een
gestandaardiseerde aanpak in België lijkt aangewezen.
KPC_24_B_026
Plan Cancer – Action 24
Projets 2009-2011 (résumé)
Auteurs:
- UZ Brussel: Lore Decoster, Katrien Van Puyvelde, Godelieve Conings
- UZ Leuven: Hans Wildiers, Koen Milisen, Johan Flamaing, Cindy Kenis
- UCL Saint Luc: Frank Cornelis, Pascale Cornette, Ramona Moor
Le ‘Plan Cancer – Action 24’ a été lancé en 2009 et avait comme but de soutenir des projets
pilotes dans l’oncogériatrie.
1. Projets sélectionnés
Au total, treize projets avaient été sélectionnés dont huit multicentriques et cinq
monocentriques.
Ces projets avaient des objectifs très différents. C’est à dire :
- l’utilisation d’un instrument de dépistage et/ou d’une évaluation gériatrique dans la
pratique quotidienne (9 projets)
- la relation entre la sarcopénie chez le patient âgé atteint de cancer et l’évolution
fonctionnelle (1 projet)
- ‘Planification préalable des soins’ chez le patient âgé atteint de cancer (1 projet)
- les expériences des patients âgés atteint de cancer et leurs familles pendant le
traitement anti-cancéreux (1 projet)
- la relation entre le dépistage et la toxicité chez les patients âgés atteint de cancer (1
projet)
Le nombre des patients inclus dans les différents projets varie entre 32 et 3518. 7/13 projets
ont inclus des patients à partir de 70 ans, 5/13 à partir de 65 ans et 1 à partir de 60 ans. Onze
projets ont inclus différents types de tumeurs, alors que deux projets se sont limités à un type
de tumeur.
2. Résultats des projets sélectionnés
Pour trois projets nous ne disposons pas des résultats finaux.
2.1 Instruments de dépistage
Quatre projets ont étudié l’utilisation d’un ou plusieurs instruments de dépistage pour
identifier les patients fragiles dans une population oncologique âgée.
Des différents instruments de dépistage ont été utilisés, notamment G8, GFI, VES-13, ISAR
et SEGA. Dans deux projets, le G8 démontre la meilleure sensibilité comparativement avec
le VES-13 et le GFI. Dans un troisième projet, le G8 et l’ISAR étaient comparables.
2.2 Evaluation gériatrique
Cinq projets avaient comme objectif primaire l’utilité d’une évaluation gériatrique pour la
détection de problèmes gériatriques inconnus et/ou l’effet d’une telle évaluation sur les
décisions thérapeutiques, la qualité de vie et la fonctionnalité.
Tous ces projets ont démontré qu’une évaluation gériatrique détecte de nouveaux
problèmes dans une quantité importante de patients âgés atteints de cancer.
2.3 Relation entre dépistage/évaluation gériatrique et toxicité liée au traitement
Un projet a étudié la toxicité de la chimiothérapie chez les patients âgés atteints de cancer
et a conclu que le moment où le patient a été interrogé sur la toxicité avait une influence
sur le nombre d’effets secondaires de grade 1 mais pas sur la suite du traitement.
2.4 ‘Planification préalable des soins’
Une étude s’est concentrée sur les soins palliatifs et ‘la planification préalable des soins‘
et a conclu que la majorité des patients âgés ressent le dialogue sur la planification
préalable des soins comme positif.
2.5 Expériences de patients âgés atteints de cancer pendant le traitement
Une étude a examiné les expériences des patients âgés et leurs proches pendant le
traitement anticancéreux et a conclu que l’écoute active et une approche individuelle sont
importantes.
3. Conclusion générale
Entre 2009 et 2011, le Plan Cancer - Action 24 a supporté 13 projets pilotes dans
l’oncogériatrie.
Ces projets ont été un premier pas très important dans l’optimalisation des soins pour un
groupe croissant de patients âgés atteints de cancer. Avec ce support, des milliers de patients
âgés atteints de cancer ont bénéficié pour la première fois d’une évaluation et d’un support
gériatrique. Le Plan Cancer - Action 24 a ainsi éveillé chez beaucoup de médecins, impliqués
dans le traitement du cancer, un intérêt pour l’oncogériatrie et a stimulé la coopération avec
les services gériatriques.
Les différents projets ont démontré clairement que la performance d’une évaluation
gériatrique peut identifier des problèmes dans les différents domaines gériatriques. Vu qu’une
telle évaluation ne semble pas réalisable chez tous les patients âgés atteints d’un cancer (aussi
bien du point de vue financier ainsi du point de vue du temps disponible), une première
sélection par un instrument de dépistage est conseillée. Tous les projets se concentrant sur le
dépistage, ont identifié le G8 comme étant un bon instrument de dépistage.
Finalement des facteurs importants dans les soins de patients âgés atteints de cancer sont : la
‘planification préalable des soins’ avec participation du patient âgé ainsi que l’écoute active
du patient.
En conclusion, les premiers projets du Plan Cancer - Action 24 ont démontré la faisabilité de
l’utilisation des instruments de dépistage suivi par une évaluation gériatrique dans les patients
âgés atteints d’un cancer dans la pratique de tous les jours. Une approche standardisée en
Belgique est recommandée.





























