Embed Size (px)
Citation preview

. . . . . . . . Chapter 1. . . . . . . . Chapter 1. . . . . . . . Chapter 1. . . . . . . . Chapter 1

IntroductionIntroductionIntroductionIntroduction

1
1. Introduction
The eye is a unique organ, both anatomically and physiologically, containing several
widely varied structures with independent physiological functions that render the organ
highly impervious to foreign substances. The cornea and crystalline lens are the only
tissues in the body besides cartilage that have no blood supply. The inner and outer
blood-retinal barriers which have no cellular components, separate the retina and the
vitreous body from the systemic circulation therefore reduce the diffusion of molecules.
This complexity of the eye imposes challenges in front of the pharmaceutical scientist to
circumvent the protective barriers of the eye without causing any permanent tissue
damage [1].
1.1 Anatomy of Eye [2]
The human eye is an anatomically and physiology unique and a sensitive organ. It offers
many barriers to the entry of any foreign material. The eyes are protected by the blinking
eyelids at the anterior and at the posterior are housed in a protective bony cavity, the
orbit. The eyeball is ablate spheroid in shape.
Fig. 1.1. Anatomy of eyeball
The eyeball is composed of three layers:
i. Outer fibrous layer (Sclera and Cornea),
ii. Middle vascular layer, the uveal tract (Choroid, Ciliary body & Iris) and

iii. The innermost nervous layer (Retina).
i. Outer fibrous layer
The outer fibrous cornea
anterior and the sclera at the posterior segment. The white and opaque sclera a matrix
composed of proteoglycans and collagen fibres, at the anterior portion is extended to a
clear transparent mucosal surface, the conjunctiva. The most an
part of the eye is the transparent, dome
refractive medium of the eye offering resistance to the passage of most drugs.
The cornea is composed of five layers:
a. Stratified squamous epithelium,
b. Bowman’s membrane,
c. Thick, elastic network of connective tissue, the stroma (Substantia propria),
d. The fibrous collagen rich Descemet’s membrane, and
e. Endothelium (posterior epithelium).
Fig. 1.2. The cornea
hydrophilic barriers
The Bowman’s membrane ends at the cornea sclera junction, the limbus. In the limbus is
present the Canal of Schlemm that drains aqueous humor (secreted in the chamber
The innermost nervous layer (Retina).
Outer fibrous layer
The outer fibrous cornea-sclera layer comprises of the cornea and c
anterior and the sclera at the posterior segment. The white and opaque sclera a matrix
composed of proteoglycans and collagen fibres, at the anterior portion is extended to a
clear transparent mucosal surface, the conjunctiva. The most anterior portion of the outer
part of the eye is the transparent, dome-shaped window, the cornea. It forms the strongest
refractive medium of the eye offering resistance to the passage of most drugs.
The cornea is composed of five layers:
Stratified squamous epithelium,
Bowman’s membrane,
Thick, elastic network of connective tissue, the stroma (Substantia propria),
The fibrous collagen rich Descemet’s membrane, and
Endothelium (posterior epithelium).
The corneal structure showing the sequential hydrophobic and
hydrophilic barriers
The Bowman’s membrane ends at the cornea sclera junction, the limbus. In the limbus is
present the Canal of Schlemm that drains aqueous humor (secreted in the chamber
2
sclera layer comprises of the cornea and conjunctiva at the
anterior and the sclera at the posterior segment. The white and opaque sclera a matrix
composed of proteoglycans and collagen fibres, at the anterior portion is extended to a
terior portion of the outer
shaped window, the cornea. It forms the strongest
refractive medium of the eye offering resistance to the passage of most drugs.
Thick, elastic network of connective tissue, the stroma (Substantia propria),
phobic and
The Bowman’s membrane ends at the cornea sclera junction, the limbus. In the limbus is
present the Canal of Schlemm that drains aqueous humor (secreted in the chamber

3
between the lens and cornea) from the eye into veins of the sclera therefore, preventing
the rise of intraocular pressure. The hydrophobic epithelium and the hydrophilic stroma
prevent the entry of the hydrophilic and hydrophobic molecules respectively making
cornea the rate limiting membrane for the absorption of drugs.Conjunctiva is the thin,
transparent mucous membrane extending from the lateral margin of the cornea, across the
sclera, covering the internal surface of the eyelids. It is composed of a stratified
squamous columnar epithelium which contains many goblet cells, that rests on a lamina
propria of loose connective tissue.
ii. The uveal tract
The uveal tract also known as the vascular tunic consists of the choroid, ciliary body and
iris. The choroid forms the posterior five-sixths of the vascular tunic. It is the brown
coloured membrane pigmented by the melanocytes which prevents scattering of light rays
within the eye. The ciliary body is composed of ciliary muscles, thickened ring of tissue
which functions for the visual accommodation by controlling the extension of lens. Iris is
the circular, muscular, lightly pigmented diaphragm with a pupil in the center. The
contraction and expansion of the muscles of the iris adjusts the size of the pupil in
response to the light entering the eyeball.
iii. The innermost nervous layer
It is the retina consisting of the photoreceptor cells, bipolar neurons, ganglions and the
pigment cells. The retina is also known as tunica nervosa due to the presence of the
neurons. It is composed of two layers the pigmented layer which is a single layer of
melanocytes and a neural layer which is a sheet of nervous tissue. It contains three main
types of neurons: photoreceptor cells, bipolar cells and the ganglion cells. There are two
types of photoreceptor cells; rod cells responsible for coloured vision and cone cells to
impart vision in bright light. The ganglion cells function to process the electrochemical
information transmitted from the photoreceptors.
The lens is a transparent, avascular, biconvex structure, suspended by the suspensory
ligaments of the lens. It has three components:
i. The lens capsule, produced by anterior lens cells.

4
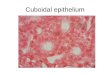
ii. A sub capsular epithelium, a cuboidal layer of cells that is only present on the
anterior surface of the lens.
iii. Lens fibres, derived from the sub capsular epithelial cells, which lose their nuclei
and organelles to become filled with proteins called crystallins.
A semi solid substance called the vitreous humor fills the posterior chamber of the
eyeball behind the lens in direct contact with the retina. It is responsible for the
transmission of light, provides support to the posterior surface of the lens and helps to
maintain the intraocular pressure.
1.2 The Nasolacrimal Apparatus
It is responsible for the production of tears which lubricates the cornea and conjunctiva.
The apparatus consists:
i. Meibomian glands (also known as sebaceous tarsal palpebral glands) secrete
anterior layer composed of lipids, which retard the evaporation of the underlying
water layers, serve to stabilize the film by increasing the surface tension and
lubricate the eyelids.
ii. Lacrimal gland and the accessory lacrimal glands (Krause and Wolfring glands)
secrete the middle aqueous layer which provides oxygen to the corneal
epithelium, and
iii. The goblet cells of the conjunctiva secrete the posterior layer which is a mixture
of mucins (glycoproteins) for hydrating the cornea. The stability of the tear film
depends on the integrity of mucin. In the absence of mucin, the cornea becomes
non wettable and the tear film becomes unstable and is subjected to breaking, with
the formation of dry areas.
The secreted tears flow through the superior and inferior punctum lachrimal followed by
their passage into the superior punctum canaliculus, lachrimal sac. The eyeball can
accommodate approximately 7 µL of fluid. Instillation of more than 10 µL leads to reflex
blinking of the eyelids. The reflex blinking of the eyes in response to the entry of any

5
foreign matter like the topically administered formulation leads to tear secretion and
drainage through the nasolacrimal duct to the nasal cavities.
Fig. 1.3. Anatomy of nasolacrimal apparatus
Through the highly vascular mucosa of the nasal epithelium, it is absorbed into the
systemic circulation. Tears dilute the drug remaining in the cul-de-sac, which reduces the
transcorneal flux of the drug.
1.3 Mechanisms and route of transport of drug molecules
The membrane, whether it is plasma membrane or a membrane encompassing cellular
organelles, imposes a barrier to the free movement of molecules. There are two general
processes of drug absorption across barrier membranes. The first type is called "the
transcellular transport process," where drug molecules have to go through the barrier cells
to reach the circulation. Transcellular transport is typically a two step process, starting
with drug uptake into the cells, and ending with drug efflux out of the cells. The second
type is called “the paracellular transport process," where the drug molecules travel
between the cells (or in the gaps) to reach the circulation.

6
Fig. 1.4. Transcellular and paracellular pathways for drug transport across
membrane
The transport of most of the molecules is contributed by both pathways. Lipophilic
molecules and molecules with specialized transport processes prefer the transcellular
route; whereas hydrophilic molecules lacking membrane transport processes prefer the
paracellular route. The mechanism of transcellular transport includes simple diffusion,
facilitated diffusion, active transport, endocytosis and exocytosis. Simple or passive
diffusion is a process that does not require cellular energy, but requires a chemical
gradient for the molecule to be transported. Facilitated diffusion is similar to simple
diffusion not requiring energy and follows chemical gradient, but it requires a membrane
transporter or carrier to facilitate the transport; two primary mode of facilitated
transport have been recognized in the biological system [3,4].
The paracellular pathway is an aqueous route involving diffusion of the molecule
between adjacent cells restricted by the presence of a series of junctional strands known
as tight junction, gap junction & desmosomes.
Mechanism of Ocular (Topical) Drug Absorption
Drugs administered by instillation must penetrate the eye and do so primarily through the
cornea and followed by the non-corneal routes. These non-corneal routes involve drug

7
diffusion across the conjunctiva and sclera and appear to be particularly important for
drugs that are poorly absorbed across the cornea.
Corneal permeation: The penetration of drugs across the corneal membrane occurs from
the pre-corneal space. Thus, the mixing and kinetic behaviour of drug disposition in tears
has a direct bearing on efficiency of drug absorption into the inner eye. The productive
absorption of most ophthalmic drugs results from diffusional process across the corneal
membrane. The efficiency of absorption process is a function of rate and extent at which
the transport processes occur. The flux of any drug molecule across a biological
membrane depends on the physicochemical properties of the permeating molecule and its
interaction with the membrane. The extent to which the transport or absorption process
occurs is also a function of physiological mechanism of pre-corneal fluid drainage or
turnover.
Factors affecting corneal transport:
Three factors are considered responsible for determining the transport efficiency
of a particular drug species across the corneal membrane.
1) The physiochemical properties of drug substance (e.g., ionization constant,
aqueous solubility, oil/water partition coefficient).
2) The formulation in which drug is prepared (e.g., pH of solution, types and
concentration of buffers, viscosity inducing agents and stabilizers).
3) The corneal structure and integrity.
Non-corneal permeation: Primary mechanism of drug permeation in the sclera is likely to
be diffusion across the intercellular aqueous media as in the case of structurally similar
corneal stroma. Therefore the possibility of partitioning mechanism cannot be eliminated.
Although, like cornea, the conjunctiva is composed of an epithelial layer covering an
underlying stroma, the conjunctival epithelium offers substantially less resistance than
does the corneal epithelium [5, 6].

8
Fig. 1.5. Mechanism and routes of drug transportation
1.4 Approaches to ocular drug delivery
Topical administration is more direct, but conventional preparations of ophthalmic drugs,
such as solutions or suspensions are relatively inefficient as therapeutic systems. A large
proportion of the topically applied drug is immediately diluted in the tear film and excess
fluid spills over the lid margin and the remainder is rapidly drained into the nasolacrimal
duct. A portion of the drug is not available for therapeutic action since it binds to the
surrounding extra orbital tissues. In view of these losses frequent topical administration is
necessary to maintain adequate drug levels. This results in transient periods of over and
under-dosing. Three factors have to be considered when drug delivery to the eye is
attempted.
Firstly, how to cross the cornea (external to ocular) to reach the site of action; secondly,
how to localize the pharmacodynamic action at the eye and minimize drug action on
other tissues and finally, how to prolong the duration of drug action such that the
frequency of drug administration can be reduced [7].
Initial attempts to overcome the poor bioavailability of topically instilled drugs (in
solution forms) typically involved the use of ointments based on mixtures of white
petrolatum and mineral oil. Ointment ensures good drug bioavailability by increasing the

9
contact time with the eye, minimizing the dilution of tears, and resisting nasolachrymal
drainage. But these vehicles has major disadvantage of providing blurred vision, they are
nowadays mainly used for either night time administration or for treatment on the outside
edges of the eyelids [8].
Now use of suspensions ophthalmic delivery system relies on the assumption that
particles may persist in conjuctival sac. The efficiency of suspension has shown high
variability, which occurred as a result of inadequate dosing, probably mainly due to the
lack of patient’s compliance in adequately shaking the suspension before administration
[9]. These disadvantages led to other formulation approaches being investigated or
simply into the development of dosage formulation that are divided into the ones that can
affect the precorneal parameters, and those that provide controlled and continuous
delivery to the pre and intraocular tissues.
The system discussed involves:
a) The newer system involved include, phase transition hydrogel systems, use of
cyclodextrins to increase solubility of various drug, vesicular systems, particulate
system, and chemical delivery systems such as the prodrugs.
b) The developed and under-developed controlled /continuous drug delivery systems
including ocular inserts, collagen shields, ocular fits, disposable intraocular lenses,
other new ophthalmic drug delivery systems, and
c) The newer trends directed towards the combination of drug delivery technologies
for improving the therapeutic response of a non-efficacious drug.
1.4.1 Conventional ocular delivery system
Eye drops/lotion - Eye drops may be solutions (aqueous and oily) are comparatively
convenient, safe, immediately active and acceptable to patients. Depending on the disease
condition, eye drops may contain steroids, prostaglandins, anesthetics, antihistamines,
sympathomimetics, parasympatholytics, β-receptor blockers, parasympathomimetics, and
non-steroidal anti-inflammatory drugs (NSAID). Eye drops also contain various inactive
ingredients such as viscosity enhancers (hydroxypropyl methylcellulose (HPMC),
carboxy methylcellulose (CMC), polyvinyl alcohol (PVA), and carbopol), preservatives

10
(benzalkonium chloride and chlorobutanol), demulcents (polyethylene glycol 400 and
polypropylene glycol), buffers (disodium phosphate, sodium borate, sodium citrate) and
tonicity adjusting agents (sodium chloride).
Fortunately, many therapeutic agents used in eye products are water-soluble compounds
or can be formulated as water-soluble salts, and a sufficiently high solution concentration
can be achieved in the administered dose. In comparison with more sophisticated
multiphase systems, solution products are preferred because they are generally easier to
manufacture and potentially provide better dose uniformity and ocular bioavailability.
The absorption of drugs from the eye is dependent upon the complex interplay of
physiological, physiochemical and formulation factors. Formulation of an optimal
ophthalmic dosage form requires a balancing act between the ocular irritation, corneal
permeation and stability. In this context, effect of formulation factors on corneal
permeation from aqueous drops and oily drops have been investigated earlier for different
NSAIDs like diclofenac [10,11], ketorolac [12,13] and flurbiprofen [14] and
fluoroquinolones like gatifloxacin [15], moxifloxacin [16,17].
Aqueous or oily suspension eye-drop formulations may be considered for drugs that are
poorly water soluble, or because of poor aqueous drug stability. The drug particle size
must be reduced to less than 10 µm levels to avoid irritation of the eye surface, leading to
blinking and excessive lachrymation. Suspensions may also be used to overcome
chemical instability of the drug, but at the same time may pose physical instability
problems. For example, there may be an increase in particle size with time (Ostwald
ripening), or difficulties in resuspension after periods of storage. The latter may result in
problems with homogeneity and dose uniformity. Although eye drops in the solution and
suspension forms have been the most common formulation approach for the treatment of
anterior segment diseases yet they have several drawbacks.
In a study it was reported that a large number of patients found it difficult to instill the
drop [18]. The secretion and drainage of tears at the rate of 1µL/min leads to tear
turnover at the rate of 16% which dilutes the drug solution and eventually increases its
drainage [19, 20]. The rates of drainage increases with increase in volume of the solution

11
instilled in the eye resulting in reduced bioavailability of the drug [21]. The amount of
drug absorbed cannot be estimated due to the limited volume holding capacity of the cul-
de-sac. The most widely used preservative benzalkonium chloride causes peeling of the
corneal epithelium cells at their borders, inhibits the growth of the cells and enlarges the
intercellular spaces in the superficial cells of the cornea [22-24]. Corneal calcification can
occur due to the phosphate buffer present in the eye drops [25, 26].
Eye ointments are sterile semi-solid preparations intended for application to the
conjunctiva. They are attractive because of their increased contact time and better
bioavailability compared to solutions but their use is limited as they interfere with vision
and are not suitable for use during the day time [27-29].
1.4.2 Hydrogel
Aqueous gel (hydrogels) consists of high molecular weight, cross linked polymers that
form a three dimensional network in water. Hydrogels are based on the addition of
hydrocolloids to aqueous drug solutions. Currently, two groups of hydrogels are
distinguished, namely preformed and in situ forming gels.
Preformed hydrogels can be defined as simple viscous solutions which do not undergo
any modifications after administration. Preformed hydrogels for topical administration in
the eye can be based on natural, synthetic, or semisynthetic polymers (like cellulose
derivatives, polyvinyl alcohol, carbomer, hyaluronic acid).
The use of preformed hydrogels still has drawbacks that can limit their interest for
ophthalmic drug delivery or as tear substitutes. They do not allow accurate and
reproducible administration of quantities of drugs and, after administration; they often
produce blurred vision, crusting of eyelids, and lachrymation. A new approach is to try to
combine advantages of both solutions and gels, such as accuracy and facility of
administration of the former and prolonged residence time of the latter. Thus, in situ
hydrogels can be instilled as eye drops and undergo an immediate gelation when in
contact with the eye [30].

12
In situ gels
In situ gels are the low viscosity solutions that undergo phase transition in the
conjunctival cul-de-sac to form viscoelastic gels due to conformational changes of
polymers in response to the physiological environment change (pH, ion activated or
temperature). The viscous gels reduce the drainage and improve the contact time than the
conventional eye drops. Gellan gum, Gelrite®
, xanthan gum, chitosan, sodium alginate,
carbopol, pluronic, poloxamers and pluronic copolymers are reported to exhibit the sol-
gel transition [31-35].
1.4.3 Ocular inserts
Solid erodible (soluble) or non-erodible (insoluble) inserts have been commercially
available for some time as a means of prolonging the release of drugs in to the eye. The
Ocusert™ (nonerodible system developed by Alza Corporation) and SODI™ (Soluble
Ophthalmic Drug Insert - erodible system) are commercially available formulations.
Ocular inserts are the solid ophthalmic devices usually of 8 mm diameter with drug
dispersed in the polymer reservoir or matrix system intended to increase the precorneal
contact time, increase bioavailability and maintain a therapeutic drug concentration in the
target tissues. The release rate and the mechanism can be controlled by the use of
different natural and synthetic polymers like sodium alginate, collagen, gelatin, Eudragit
RS-100 and RL-100, p-HEMA, polyethylene oxide, cellulose acetate phthalate and
hydroxypropylmethyl cellulose (HPMC) [36-41].
To improve the intraocular retention of inserts, mucoadhesive thiolated ocular inserts
comprising of polyacrylic acid-cysteine conjugate as polymeric matrix, containing either
diclofenac sodium or diclofenac-tris (hydroxymethyl)-amino methane were prepared and
evaluated. In-vitro release studies conducted using simulated lachrymal fluid revealed a
significantly lesser release of drug from diclofenac-tris inserts compared with diclofenac
sodium inserts. The inserts were successful in providing a controlled drug release with
release rate approximating zero order release kinetics [42].
In another study reservoir type ocular inserts of ketorolac were formulated using HPMC
or methylcellulose and povidone as polymeric films, and ethylcellulose film as rate

13
controlling membrane [43]. The ocular inserts casted using HPMC (4%) and ethyl
cellulose (3%) was found to sustain ketorolac tromethamine release by zero order kinetics
for 22 h.
Ocular inserts of indomethacin were fabricated using a combination of low and high
molecular weight polyvinyl alcohol. The ex-vivo permeation of drug from ocular inserts
was evaluated through excised goat cornea, and it was observed that physical cross
linking of inserts by freeze-thaw cycling and increase in the proportion of low molecular
weight polyvinyl alcohol decreased the apparent corneal permeability of indomethacin
[44].
In another study, ocular inserts/films of aceclofenac were prepared using glycero-gelatin
polymer and evaluated for physicochemical parameters and drug release profiles. Ocular
irritation of the developed formulation was also checked by HET-CAM test and efficacy
of the developed formulation against prostaglandin-induced ocular inflammation in rabbit
eye was determined. The results of the study showed that the cross-linked ocular insert
proved to be significantly better in various evaluating parameters such as tensile strength,
swelling potential, drug release and pharmacodynamic activity [45].
1.4.4 Contact lenses
Use of soft contact lenses as a carrier for drug delivery is gaining attention. Sedlacek, in
the year 1965 described [46] the use of contact lenses to increase the residence time
(typically days) of the drug in the eye, patient comfort and to limit the drug loss by
drainage, lacrimation or conjunctival absorption [47]. Medicated soft contact lenses can
be used to treat ocular diseases in addition to the correction of refractive deficiencies.
Contact lenses loaded by soaking technique [48] are not therapeutically effective due to a
very low uptake of drug by the lens and a rapid release might lead to low residence time.
The other limitations like the limited drug incorporation in lens matrix, incompetent to
offer slow and extended drug release, wastage of large fraction of drug during loading
procedure have limited its use in ODDS. The uptake and release of the drug depends on
the material of the lens (as a function of ionicity, water and silicone content), loading
solution, time during which is placed in the loading solution and molecular weight of the

14
drug incorporated [49]. Novel techniques molecular imprinting and supercritical solvent
impregnations have surmounted all these issues. Molecular imprinting produces synthetic
macromolecular networks template-medicated polymerization mechanisms with specific
affinity, capacity and selectivity for the diffusion of drug molecules. A therapeutically
relevant amount of drug can be loaded and released over an extended period of time and
this technique is applicable to daily-wear and extended-wear contact lenses. In the
supercritical fluid impregnation technique, drug is impregnated and dispersed in a
polymer matrix by dissolving in compressed high volatile fluids (like carbon dioxide) at
temperatures and pressures near or above their critical temperatures and pressures and
bringing the resultant mixture in contact with polymer matrix [50-52].
A method for preparation of soft contact lenses of poly (hydroxyethyl methacrylate)
(PHEMA) using molecular imprinting technique for norfloxacin delivery has been
described [51]. PHEMA hydrogels are used as soft contact lenses. Hydrogel is a
polymeric material which swells in water and retain large quantity of water within its
structure but does not dissolve. Due to high water content hydrogel is soft and rubbery
and offers low frictional irritation to the body tissue. PHEMA hydrogels on immersion in
drug solution takes up the drug which can be applied to eye. PHEMA is synthesized by
polymerization. If HEMA is polymerized with a functional monomer like acrylic acid
which can interact with cationic drug by non-covalent interaction, the affinity of the lens
for drug could be increased. However, if the lens is synthesized by conventional
polymerization method, a random distribution of functional monomer is obtained. In the
molecular imprinting technology, the drug is polymerized with the monomers, so that the
functional monomers arrange themselves around the drug molecule, according to their
interaction capacity. The polymerization and cross-linking fix the spatial sequence and
after removal of the template molecule, recognition cavities complementary in shape and
functionality of the drug are obtained. In the said study, acrylic acid and ethyleneglycol
dimethacrylate (cross-linker) were dissolved in 2- hydroxyethyl methacrylate (HEMA).
Norfloxacin was added to the solution and 2-2'-azo-bis (isobutyronitrle) was added as a
polymerization initiator. The solution was put in a mould and exposed to 50°C for 12h

15
and 70°C for 24h. After polymerization, the gel was immersed in boiling water for 15
min to remove unreacted monomers and treated with HCL and water to remove
norfloxacin and subsequently the polymer was dried. Similarly, a non-imprinted polymer
was made without addition of norfloxacin.The imprinted polymer when immersed in
norfloxacin solution loaded greater amounts of norfloxacin than the non-imprinted ones.
Imprinted polymeric hydrogel, synthesized with norfloxacin: acrylic acid in 1:3 and 1:4
molar ratios, showed greatest ability to control the release process sustained for >24h.
1.4.5 Collagen Shield
Collagen is the most abundant primary fibrous protein present in the animal tissues. The
fibrils of the connective tissue in skin, bones, eyes, tendons and ligaments mainly
comprise of collagen. Stroma, which forms 90% of the cornea, and the Bowman’s layer
are lamellas of collagen, which imparts mechanical strength to the eyeball [53, 54].
Collagen derived from porcine sclera and molded into clear thin pliable sheets was
fabricated as a potential vehicle to promote the healing of the de epithelialized corneal
conditions, to eliminate the painful use of contact lenses and to achieve a sustained
delivery of drugs [55, 56]. Bio-Cor® marketed by Bausch and Lomb was the first
commercially available porcine collagen shield. Glucan/collagen therapeutic eye shields
were the patented products of Biosource Genetics Corporation used to deliver glucan
through the collagen shields [57]. A pre-soaked collagen shield of ofloxacin applied
before surgery appeared safe and provided higher concentration of ofloxacin in aqueous
humor (0.96 µg/mL) of the human eye compared to 0.3% w/v ofloxacin aqueous
drop(0.29 µg/mL) [58].
1.4.6 Microspheres
Microspheres are monolithic particles possessing a porous or solid polymer matrix,
whereas microcapsules consist of a polymeric membrane surrounding a solid or a liquid
drug reservoir. The application of such systems in the ophthalmic field has been
extensively reviewed by Kreuter and colleagues [59-60]. Upon topical instillation of a
particulate suspension in the cul-de-sac, the drug is slowly released in the lachrymal pool
by dissolution and mixing, diffusion, or mechanical disintegration or erosion of the

16
polymeric matrix (60). The upper size limit for microparticles for ophthalmic
administration is about 5-10 µm. The ophthalmic administration of particles of higher
size can result in an itching sensation and can induce lachrymation, with the possible
consequence of reducing drug bioavailability. Modification with the use of mucoadhesive
and viscous polymers can be used to improve the corneal retention and bioavailability of
the formulation [61].
1.4.7 Nanoparticles
Nanoparticles are polymeric colloidal particles ranging in size from 10 to 1000 nm.
Depending on the method of the preparation, nanospheres or nanocapsules can be
obtained. Nanospheres have a matrix-like structure, wherein active compounds can be
firmly adsorbed onto their surface, entrapped, or dissolved in the matrix. Nanocapsules
have a polymeric shell and an inner core. In this case the active substances are not only
dissolved in the core but may also be adsorbed onto the nanocapsule surface. Colloidal
systems in the sub-micron range can be incorporated in the eye drops as an alternative to
the conventional dosage forms [62, 63].
Pignatello et al formulated nanoparticles with Eudragit RL and RS using a modified
quasi- emulsion solvent diffusion technique and solvent evaporation method [64]. Upon
administration of these nanoparticles in rabbits, sustained release and increased
absorption of the incorporated NSAIDs (ibuprofen and flurbiprofen) were observed.
Furthermore, no signs of inflammation or discomfort were detected in the rabbits' eyes,
suggesting a local bio tolerance of these nanoparticles [65, 66].
To increase the ocular availability, ketorolac was entrapped in N-isopropylacrylamide,
vinyl pyrrolidone and acrylic acid based copolymeric nanoparticles. The particles were
spherical and had a size of 35 nm. In-vitro permeation studies through excised cornea
revealed twofold higher permeation of drug from nanoparticle formulation, compared
with an aqueous suspension of the drug. Pharmacodynamic evaluation of nanoparticle
formulation in PGE2-induced ocular inflammation in rabbits showed a significantly
higher ocular anti-inflammatory activity for 5 h compared with the aqueous suspension,

17
which has been attributed to the small size of the particles and mucoadhesiveness. The
nanoparticle formulation did not show any corneal damage during in-vitro study [67].
Adibkia et al also studied a NSAID-loaded Eudragit nanoparticle formulation. The
piroxicam based Eudragit RS100 nanoparticles were prepared by solvent
evaporation/extraction technique. These nanoparticles were used to control inflammatory
symptoms in rabbits with endotoxin-induced uveitis, where a microsuspension of
piroxicam was used as control. The in-vivo examinations revealed that the inflammation
could be inhibited by the nanoparticle formulation more significantly than the pure
piroxicam microsuspension, improving ocular delivery for local inhibition of
inflammation [68].
In another study with PLGA, Vega et al applied an experimental design to optimize a
formulation of flurbiprofen-loaded nanoparticles. The particle surface was coated with
Poloxamer 188 (BASF SE, Ludwigshafen, Germany), resulting in zeta potential values of
approximately -25 mV and a particle size of 230 nm. Drug entrapment efficiencies of
over 90% were obtained, and in-vitro release studies showed a burst release, followed by
a slower release, completed after 90 min. In-vivo studies performed in rabbits
demonstrated that the formulations did not induce toxicity or irritation. Nanoparticle
formulations were compared with the commercial eye drops (Ocoflur Allergan, Belgium)
after induction of inflammation by instillation of sodium arachidonate. The results
indicated a very good anti-inflammatory efficacy for flurbiprofen-loaded PLGA
nanoparticles providing controlled and continuous drug delivery [69].
1.4.8 Solid lipid nanoparticles
SLNs were first patented by Muller and Lucks (1996). Since then they have attracted
scientists as a widely used, stable, non-toxic, and reliable particulate drug delivery
vehicle. Lipid nanoparticles consist of solid lipid spheres, with average diameters
between 50 and 1000 nm, dispersed in aqueous medium [70-72]. These particles are
similar to those described as polymeric nanoparticles, being in this case composed of a
solid lipid core matrix, stabilized by surfactants. As such, these lipid nanoparticles will
have high encapsulation efficiency and loading capacity for lipophilic molecules.

18
Surfactants used for their production include biological membrane lipids (lecithin, pure
phospholipids), bile salts (e.g., sodium taurocholate), biocompatible nonionic molecules
(e.g., ethylene oxide/propylene oxide copolymers, sorbitan esters, and fatty acid
ethoxylates). When optimized, lipid nanoparticles show high physical stability, protection
of incorporated labile drugs against degradation and excellent in-vivo tolerability.
However, these systems generally exhibit a low drug payload and have the tendency to
expulsion of drug during storage due to the transition of highly ordered lipid particles
[73, 74].These disadvantages can be alleviated by using structured lipid matrices in SLN
formulations and surface modification of the particles [75]. The sodium diclofenac loaded
lipid nanoparticles were prepared by Attama et al using the combination of homolipid
from goat (goat fat) and a phospholipid, applying the hot high-pressure homogenization
method [76]. Administration of this formulation in bioengineered human cornea showed
a sustained release of the drug. Furthermore, permeation of sodium diclofenac through
the cornea construct was improved by surfacing nanoparticles with phospholipid, which
showed the better performance of this formulation for ocular application.
1.4.9 Liposomes
Liposomes are membrane-like vesicles consisting of one or more concentric bilayers,
produced from natural nontoxic phospholipids and cholesterol, alternating aqueous and
lipophilic compartments. Because of their size, amphiphilic properties, and
biocompatibility, liposomes are promising systems for drug delivery. They can be
classified according to structural features as multilamellar vesicles, small unilamellar
vesicles, and large unilamellar vesicles, depending on their size and the number of lipid
bilayers. With respect to their electrical charge, liposomes can have a positive, negative,
or neutral surface charge, depending on their chemical composition (type of
phospholipids, drug substances, and other lipid molecules). They can accommodate both
hydrophilic and lipophilic drugs, respectively, into the aqueous compartment or the lipid
bilayer [77].
The use of phospholipid vesicles to increase the precorneal residence time and as carriers
for water soluble and lipid soluble drugs has been reported [78, 79]. Positively charged

19
liposomes showed a higher binding affinity to the anionic corneal and conjunctival
mucoglycoproteins and better entrapment efficiency than the neutral and negatively
charged vesicles [80]. Mixed brain gangliosides were incorporated into the membranes of
phosphatidylcholine liposomes to provide receptor sites for wheat germ agglutinin, a
lectin that binds strongly to corneal epithelium, led to enhanced topical drug flux [81].
Collasomes, liposomes coupled to collagen matrices and PAMAM (Polyamido amine)
dendrimers-coated puerarin liposomes were prepared to increase the adhesion capacity
and penetration of liposomes [82, 83]. In another study, pre-corneal retention of
diclofenac sodium has also been reported to be increased by use of liposomes. The
cationic liposomes of diclofenac sodium prepared by reverse phase evaporation were
observed to provide a 211% increase in aqueous humor concentration of drug compared
with conventional aqueous eye drop formulation [84]. Niosomes were found to be better
vesicle system to deliver hydrophilic and lipophilic drugs to eyes due to their better
stability than the liposomes [85, 86]. Large disc shaped vesicles, discomes were derived
from niosomes by the addition of a non-ionic surfactant Solulan C24 [87]. The large size
of discomes fit in cul-de-sac thereby preventing its drainage into the systemic pool as
well as disc shape [88].
1.4.10 Ocular minitablets
These are the bioerodible tablets weighing about 6 mg and 8 mm (4×2mm) in diameter.
Minitablets with matrix system were prepared by direct compression of the powdered
blend of drug, polymer and other excipients. The drug release occurs due to swelling of
the polymer followed by dissolution in the tear fluid. High drug concentration can be
maintained in tear fluid using minitablets for a prolonged time period. On insertion, the
tablet absorbs the tear fluid and sustains the drug release on being hydrated [89, 90].
1.4.12 Ocular iontophoresis
It is an advanced non-invasive technique to avoid the complications associated with
administration of frequent, high dose sub-conjunctival injections or eye drops which
require hospitalization of the patient [91-93]. Direct current (DC) of low intensity 0.2 mA
to 4 mA for 10-20 min is applied that drives charged molecules across the cornea, sclera

20
and the adjacent tissues [94-98]. It is limited to drug molecules which can ionize and
have low molecular weight. Singh et al., proposed a new efficient technique
MacroesisTM (patent filed by Buckeye Pharmaceuticals, Beachwood, OH, U.S.) which
uses alternating current instead of direct current. Therapeutic concentrations were
achieved in the ocular tissues in less time period and it is possible to deliver the drug to
the posterior segment of the eyeball [99].
1.5 Ophthalmic inflammatory disorders and treatment
The most common disease affecting the eye is inflammation. Inflammatory conditions of
the eye are designated according to the tissue affected. Conjunctiva and cornea are
constantly exposed to various types of physical, chemical, microbial (bacteria, fungi,
viruses), and allergic agents and hence prone to develop acute, sub-acute, and chronic
inflammations. Conjunctivitis, keratitis, retinitis, uveitis, endophthalmitis, dacryocystitis,
dacryoadenitis and iritis are the inflammatory disorders of the eye parts. The disease
ranges in severity from mild forms, which can still interfere significantly with quality of-
life, to severe cases characterized by potential impairment of visual function. Ocular
inflammation is also a common result of cataract surgery, producing pain and
photophobia in many patients and potentially leading to serious complications including
increased intraocular pressure, posterior-capsule opacification, cystoid macular edema,
and decreased visual acuity.
Inflammation is manifested as a cellular and vascular response to the injury, infection,
ischemia and excessive or inappropriate operation of immune mechanism. The response
is amplified by activation of inflammatory cells and production of chemical mediators
like acidic lipids e.g. prostaglandins, thromboxanes, leukotrienes, vasoactive amines,
cytokines etc. The acidic lipids are produced through arachidonic acid metabolism.
Arachidonic acid is released from the phospholipids component of cell membrane by the
action of phospholipase A2. The arachidonic acid is fed into the cyclooxygenase and
lipoxygenase pathways, resulting in production of pro-inflammatory prostaglandins and
leukotrienes [100].

21
Ocular actions of PGs are manifested in three ways [101]. Firstly, they act on intraocular
pressure (IOP). PGE1 & E2 increase the IOP by local vasodilation and increased
permeability of blood aqueous barrier. On the other hand PGF2α lowers the IOP which is
attributed to increased uveoscleral out flow. Secondly they act on iris smooth muscle to
cause miosis. Thirdly, PGs cause vasodilation and increase the vascular permeability
resulting in increased aqueous humor protein concentration.
The pharmacological approach of management of inflammation involves administration
of anti-inflammatory agents. Topical administration of drugs is the most preferred route
for management of ocular inflammations as it provides higher ocular drug concentrations,
avoiding the systemic side effects associated with the oral administration. However due
to the physiologic constraints of the eye only few of the anti-inflammatory agents which
possess certain physicochemical properties can be formulated into a suitable dosage form
effective for the management of ocular inflammations. Corticosteroids used to be the
mainstay of topical therapy in the management of ocular inflammations [102], but their
anti-inflammatory effect was outweighed by serious adverse effects like elevation of
intraocular pressure, progression of cataracts, increased risk of infection and worsening
of stromal melting [103]. Corticosteroids, the potent anti-inflammatory agents elicit their
action by blocking the enzyme phospholipase A2 to inhibit arachidonic acid production,
thereby preventing the synthesis of all the PGs, thromboxanes and eicosanoids. On the
other hand non-steroidal anti-inflammatory drugs (NSAIDs) exert their anti-inflammatory
action by inhibiting the enzymes cyclooxygenase (COX 1 & COX 2).
As a class, NSAIDs have proven to be a safe and effective alternative to corticosteroids in
the topical management of ocular inflammations [104]. Currently these drugs are used
topically very widely in inhibition of intra-operative miosis, management of post-
operative inflammation, treatment of seasonal allergic conjunctivitis, prevention and
treatment of cystoid macular edema and in the control of pain after photo refractive
keratectomy [105]. NSAIDs have also been found to be useful in decreasing bacterial
colonization of contact lenses and prevent bacterial adhesion to human corneal epithelial
cells [106].

22
NSAIDs comprise of several chemically heterogeneous class of drugs which possess
potent cyclooxygenase inhibitory activity. However, the topical use of NSAIDs in
ophthalmology is limited to relatively water soluble salicylic acid, indole acetic acid, aryl
acetic acid, aryl propionic acid and enolic acid derivatives. Most of the NSAIDs are
weakly acidic drugs, which ionize at the pH of the lachrymal fluid and therefore have
limited permeability through the anionic cornea which has an isoelectric point (pI) of 3.2
[107]. Reducing the pH of the formulation increases the unionized fraction of the drug
which enhances permeation. Being acidic, NSAIDs are inherently irritant and reducing
the pH of formulation further increases their irritation potential, as well as decreasing
their aqueous solubility. In addition, the anionic nature of NSAIDs lends to the formation
of insoluble complexes with cationic quaternary ammonium preservatives, such as
benzalkonium chloride [10, 14]. Thus; it has proved difficult to formulate topical NSAID
formulations that are comfortable when applied topically to the eye.
There are four NSAIDs currently approved by the US Food and Drug Administration for
the treatment of postoperative inflammation after cataract surgery, namely kerotolac,
bromfenac, diclofenac and nepafenac.
Aceclofenac, 2-[[2-[2- [(2, 6-dichloro phenyl) amino] phenyl] acetyl] oxy] acetic acid, is
a NSAID of the phenyl acetic acid group which is structurally related to diclofenac. It
possesses good anti-inflammatory and analgesic activities, while maintaining better
gastric tolerance in comparison with other NSAIDs such as indomethacin and diclofenac.
Aceclofenac acts as such by inhibiting the secretion of tumor necrosis factor (TNF-α) and
interleukin-1 along with preferential selective cyclooxygenase-2 (COX-2) inhibition after
conversion into active metabolite [108-110]. The present study gives an insight into
various approaches used in topical ocular delivery of aceclofenac.

23
Drug profile [110-112]
Aceclofenac
Chemical Structure
Drug Category : Anti-inflammatory
Chemical Name : 2-[(2, 6-Dichlorophenylamino) phenyl]acetoxy acetic acid
Molecular Formula : C16H13Cl2NO4
Molecular Weight : 354.2
Melting Point : 149° to 150 °C
Description : A white to almost white crystalline powder.
Solubility : It is practically insoluble in water; soluble in alcohol and
methyl alcohol; freely soluble in acetone and
dimethylformamide.
Partition Coefficient : 2.9
Elimination Half Life : 4 h
Dissociation Constant : 4.7 [pKa]

24
Pharmacokinetics
Absorption : Aceclofenac is well absorbed after oral administration.
Metabolites : It is metabolised in hepatocytes and microsomes to 4-
hydroxyaceclofenac, which can undergo further
conjugation. Other metabolites also identified include
diclofenac and 4-hydroxydiclofenac, and their
hydroxylated derivatives.
Distribution : Aceclofenac penetrates into synovial fluid and
concentrations here reach approximately 57% of those
in plasma.
Volume of distribution : Apparent volume of distribution is approx. 25 L
Protein binding : >99% plasma protein bound.
Clearance : 70% of an administered dose is excreted in urine as
glucuronides of aceclofenac and diclofenac
Mechanism of action : Preferential selective cyclooxygenase-2 (COX-2)
inhibition after conversion into active metabolite,
aceclofenac acts as such by inhibiting the secretion of
tissue necrosis factor (TNF-α) and interleukin-1.
Dosage : A usual dose of 100 mg twice daily is administered with
a reduction to 100 mg daily for patients with hepatic
impairment.
Adverse Effects : Dizziness, vertigo, puritus, rash and dermatitis
Drug Interactions : Interaction with anticoalulants, cyclosporins, diuretics,
quinolones,digoxin,methotrexate and lithium
Usage and adminisrations : It is used in the management of osteoarthritis,
rheumatoid arthritis, and ankylosing spondylitis, in
usual oral doses of 100 mg twice daily. Reduced doses
should be used in patients with hepatic impairment.
Proprietary names : Airtal; Barcan; Biofenac; Difucrem; Falcol; Gerbin.

25
polymer profile [113]
Eudragit RL 100 / Eudragit RS 100
Nonproprietary Name
"Ammonio Methacrylate Copolymer Type A“Ph. Eur.
"Ammonio Methacrylate Copolymer Type B“Ph. Eur.
"Ammonio Methacrylate Copolymer, Type A and B" USP/NF
"Aminoalkylmethacrylate Copolymer RS" JPE
Commercial form
Solid substances Eudragit RL 100 (Type A) and Eudragit RS 100 (Type B)
Chemical structure
Eudragit RL 100- Poly (ethyl acrylate, methyl methacrylate,
trimethylammonioethyl methacrylate chloride) 1 : 2 : 0.2.
Eudragit RS 100- Poly(ethyl acrylate, methyl methacrylate,
trimethylammonioethyl methacrylate chloride) 1 : 2 : 0.1.
Eudragit RL 100 and Eudragit RS 100 are copolymers of acrylic and methacrylic acid
esters with a low content in quaternary ammonium groups. The ammonium groups are
present as salts and make the polymers permeable. The average molecular weight is
approx. 150,000.

26
Structural formula of Eudragit RS and Eudragit RL
Description
Eudragit RL 100 and Eudragit RS 100: colourless, clear to cloudy granules with a faint
amine-like odour. Eudragit RS and Eudragit RL are copolymers synthesized from acrylic
acid and methacrylic acid esters, with Eudragit RL (Type A) having 10% of functional
quaternary ammonium groups and Eudragit RS (Type B) having 5% of functional
quaternary ammonium groups. The ammonium groups are present as salts and give rise to
pH independent permeability of the polymers. Both polymers are water-insoluble, and
films prepared from Eudragit RL are freely permeable to water, whereas, films prepared
from Eudragit RS are only slightly permeable to water.
Solubility
1g of the substances dissolves in 7g aqueous methanol, ethanol and isopropyl alcohol
(containing approx. 3 % water), as well as in acetone, ethyl acetate and methylene
chloride to give clear to cloudy solutions. The substances are practically insoluble in
petroleum ether, 1 N sodium hydroxide and water.
Safety
Polymethacrylate copolymers are widely used as film-coating materials in oral
pharmaceutical formulations. They are also used in topical formulations and are generally
regarded as nontoxic and nonirritant materials. A daily intake of 2 mg/kg body-weight of

27
Eudragit (equivalent to approximately 150mg for an average adult) may be regarded as
essentially safe in humans.
Applications in Pharmaceutical Formulation or Technology
Eudragit RL 100 and Eudragit RS 100 are used to form water-insoluble film coats for
sustained-release products. Eudragit RL films are more permeable than those of Eudragit
RS, and films of varying permeability can be obtained by mixing the two types together.

28
References
1. Mitra AK, editor. Ophthalmic drug delivery systems. 2nd
edition. Marcel Dekker
Inc., New York, USA, 2003. p. 1-15.
2. Davson, H. (1969). In "The Eye" (H. Davson, ed.), Vol. 1, 2nd ed. Academic Press,
New York and London
3. Grass GM, Cooper ER, Robinson JR. Mechanisms of corneal drug penetration III:
Modeling of molecular transport. J Pharm Sci 2006; 77(1):24 - 6.
4. Grass GM, Robinson JR. Mechanism of corneal drug penetration I: In vivo and In-
vitro kinetics. J Pharm Sci 1988; 77(1):3-14.
5. Chastain JE, Precorneal, corneal and post corneal factors, in: A.K. Mitra (Ed.),
Ophthalmic Drug Delivery Systems, Marcel Dekker, New York, (2003) pp. 59–82
6. Maurice DM and Mishima S. Ocular pharmacokinetics, in: M.C. Sears (Ed.),
Handbook of Experimental Pharmacology, Pharmacology of the Eye, vol. 69,
Springer-Verlag, Berlin-Heidelberg (1984) pp. 19-116
7. Washington N, Washington C. and wilson,C.G. physiological pharmaceutics,
Barriers to drug absorbtion ,2nd edition, (2001) pp; 254-255
8. Lachman L, Liberman HA, ; The theory and practice of industrial pharmacy;
Verghees publishing house, Bombay , 3rd edition, (1991) pp 548
9. Hecht G, Roehrs RE, Cooper ER, Hiddemen JW, VanDuzee BF (1990) Design and
evaluation of ophthalmic pharmaceutical products. In: Banker GS, Rhodes CT
(ed.), Modern Pharmaceutics, Vol. 40, 2 nd ed., Marcel Dekker, New York, pp.
539-603.
10. Ahuja M, Dhake AS, and and Majumdar DK. Effect of formulation factors on In-
vitro permeation of diclofenac from experimental and marketed aqueous eye drops
through excised goat cornea. Yakugaku Zasshi 2006; 126:1369-1375.
11. Ahuja M, Sharma SK and Majumdar DK. In-vitro corneal permeation of diclofenac
from oil drops. Yakugaku Zasshi. 2007; 127(10):1739-1745.

29
12. Malhotra M, Majumdar DK. In-vitro transcorneal permeation of ketorolac
tromethamine from buffered and unbuffered aqueous ocular drops. Indian J Exp
Biol. 1997, 35:941Y947.
13. Malhotra M and Majumdar DK. In-vitro transcorneal permeation of ketorolac from
oil based ocular drops and ophthalmic ointment. Indian J. Exp. Biol. 1997;
35:1324-1330.
14. Gupta M and Majumdar DK. Effect of concentration, pH and preservatives on In-
vitro transcorneal permeation of ibuprofen and flurbiprofen from non-buffered
aqueous drops. Indian J. Exp. Biol. 1997;35:844-849.
15. Rathore MS, Majumdar DK. Effect of formulation factors on In-vitro transcorneal
permeation of gatifloxacin from aqueous drops. AAPS PharmSciTech 2006; 7:57.
16. Pawar PK, Majumdar DK. Effect of formulation factors on In-vitro permeation of
moxifloxacin from aqueous drops through excised goat, sheep, and buffalo corneas.
AAPS PharmSciTech 2006; 7:E13.
17. Pawar PK, Majumdar DK. In-vitro permeation characteristics of moxifloxacin from
oil drops through excised goat, sheep, buffalo and rabbit corneas. Pharmazie 2007;
62:853-7.
18. Winfield AJ, Jessiman D, Williams A, Esakowitz L. A study of the causes of non-
compliance by patients prescribed eyedrops. Br J Ophthalmol 1990; 74:477-80.
19. Mishima S, Gasset A, Klyce SD Jr, Baum JL. Determination of tear volume and
tear flow. Invest Ophthalmol 1966; 5:264-76.
20. Schoenwald RD, Boltralik JJ. A bioavailability comparison in rabbits of two
steroids formulated as high viscosity gels and reference aqueous preparations.
Invest Ophthalmol Vis Sci 1979; 18:61-6.
21. Benedetto DA, Shah DO, Kaufman HE. The instilled fluid dynamics and surface
chemistry of polymers in the pre ocular tear film. Invest Ophthalmol 1975; 14:887-
902.

30
22. Pfister RR, Burstein N. The effects of ophthalmic drugs, vehicles, and preservatives
on corneal epithelium: a scanning electron microscope study. Invest Ophthalmol
1976; 15:246-59.
23. Samples JR, Binder PS, Nayak S. The effect of epinephrine and benzalkonium
chloride on cultured corneal endothelial and trabecular meshwork cells. Exp Eye
Res 1989; 49:1-12.
24. Lidgate DM, Fu RC, Fleitman JS. Corneal permeability of ketorolac tromethamine
when formulated with tobramycin. Drug Dev Ind Pharm 1989; 15:1779-95.
25. Schrage NF, Schlossmacher B, Aschenbernner W, Langefeld S. Phosphate buffer in
alkali eye burns as an inducer of experimental corneal calcification. Burns 2001;
27:459-64.
26. Schrage NF, Frentz M, Reim M. Changing the composition of buffered eye-drops
prevents undesired side effects. Br J Ophthalmol 2010; 94:1519-22.
27. Hardberger R, Hanna C, Boyd CM. Effects of drug vehicles on ocular contact time.
Arch Ophthalmol 1975; 93:42-5.
28. Shchipanova AI, Maĭchuk IuF, Nikolaeva IS, Pershin GN. Pharmacokinetics and
antiviral activity of riodoksol in an ointment and in ophthalmic drug films in ocular
herpes. Farmakol Toksikol 1981; 44:439-42.
29. Greaves JL, Wilson CG, Birmingham AT. Assessment of the precorneal residence
of an ophthalmic ointment in healthy subjects. Br J Clin Pharmacol 1993; 35:188-
92.
30. Edith Mathiowitz. In: Encyclopedia of controlled drug delivery, A Wiley-
lnterscience Publication.
31. Srividya B, Cardoza RM, Amin PD. Sustained ophthalmic delivery of ofloxacin
from a pH triggered in situ gelling system. J Control Release 2001; 73:205-11.
32. Gupta H, Velpandian T, Jain S. Ion- and pH-activated novel in-situ gel system for
sustained ocular drug delivery. J Drug Target 2010; 18:499-505.
33. Balasubramaniam J, Pandit JK. Ion-activated in situ gelling systems for sustained
ophthalmic delivery of ciprofloxacin hydrochloride. Drug Deliv 2003; 10:185-91.

31
34. Lin HR, Sung KC. Carbopol/pluronic phase change solutions for ophthalmic drug
delivery. J Control Release 2000; 69:379-88.
35. Ma WD, Xu H, Nie SF, Pan WS. Temperature-responsive, Pluronic-g-poly(acrylic
acid) copolymers in situ gels for ophthalmic drug delivery: rheology, In-vitro drug
release, and in vivo resident property. Drug Dev Ind Pharm 2008; 34:258-66.
36. Bensinger R, Shin DH, Kass MA, Podos SM, Becker B.. Pilocarpine Ocular Inserts.
Invest Ophthalmol 1976; 15:1008-10.
37. Sultana Y, Aqil M, Ali A. Ocular inserts for controlled delivery of pefloxacin
mesylate: preparation and evaluation. Acta Pharm 2005; 55:305-14.
38. Hsiue GH, Guu JA, Cheng CC. Poly (2-hydroxyethyl methacrylate) film as a drug
delivery system for pilocarpine. Biomaterials 2001; 22:1763-9.
39. Charoo NA, Kohli K, Ali A, Anwer A. Ophthalmic delivery of ciprofloxacin
hydrochloride from different polymer formulations: In-vitro and in vivo studies.
Drug Dev Ind Pharm 2003; 29:215-21.
40. Di Colo G, Burgalassi S, Chetoni P, Fiaschi MP, Zambito Y, Saettone MF. Gel-
forming erodible inserts for ocular controlled delivery of ofloxacin. Int J Pharm
2001; 215:101-11.
41. Deshpande PB, Dandagi P, Udupa N, Gopal SV, Jain SS, Vasanth SG. Controlled
release polymeric ocular delivery of acyclovir. Pharm Dev Technol 2010; 15:369-
78.
42. Hornof M, Weyenberg W, Ludwig A and Bernkop- Schnurcha A. Mucoadhesive
ocular insert based on thiolated poly acrylic acid): development and in vivo
evaluation in humans. J. Control Rel. 2003;89:419-428.
43. Jayaprakash P S, James CC, Rajan N S M G, Saisivam S and Nagarajan M. Design
and evaluation of ketorolac tromethamine ocuserts. Indian J. Pharm. Sci. 2000;
62:334-338.
44. Pandit JK, Harikumar SL, Mishra D N and Balasubramaniam J. Effect of physical
cross-linking on In-vitro and ex vivo permeation of indomethacin from polyvinyl
alcohol ocular inserts. Indian J. Pharm. Sci. 2003; 65:146-151.

32
45. Manish Mathurm, and Ritu Mehra Gilhotra. Glycerogelatin-based ocular inserts of
aceclofenac: Physicochemical, drug release studies and efficacy against
prostaglandin E2-induced ocular inflammation. 2011; 18(1):54-64.
46. Sedlacek J. Possibility of application of eye drugs with the aid of gel-contact lenses.
Cesk Oftalmol 1965; 21: 509-12.
47. Singh K, Nair AB, Kumar A, Kumria R. Novel approaches in formulation and drug
delivery using contact lenses. J Basic Clin Pharm 2011;2:87-101.
48. Hillman JS. Management of acute glaucoma with Pilocarpine-soaked hydrophilic
lens. Br J Ophthalmol 1974; 58:674-9.
49. Karlgard CC, Wong NS, Jones LW, Moresoli C. In-vitro uptake and release studies
of ocular pharmaceutical agents by silicon-containing and p-HEMA hydrogel
contact lens materials. Int J Pharm 2003; 257:141-51.
50. Costa VP, Mara EM, Braga A, Duarte ARC, Duarte CMM, Leite EOB, Gil MH, de
Sousa HC. Development of therapeutic contact lenses using a supercritical solvent
impregnation method. J Supercrit Fluids 2010; 52:306-16.
51. Alvarez-Lorenzo C, Yañez F, Barreiro-Iglesias R, Concheiro A. Imprinted soft
contact lenses as norfloxacin delivery systems. J Control Release 2006; 113:236-
44.
52. Hiratani H, Fujiwara A, Tamiya Y, Mizutani Y, Alvarez-Lorenzo Cl. Ocular
release of timolol from molecularly imprinted soft contact lenses. Biomaterials
2005; 26:1293-8.
53. Baer E, Cassidy JJ, Hiltner A. Hierarchial structure of collagen composite system:
lessons from biology. Pure & Appl Chem 1991; 63:961-73.
54. Komai Y, Ushiki T. The three-dimensional organization of collagen fibrils in the
human cornea and sclera. Invest Ophthalmol Vis Sci 1991; 32:2244-58.
55. Shaker GJ, Ueda S, LoCascio JA, Aquavella JV. Effect of a Collagen Shield on Cat
Corneal Epithelial Wound Healing. Invest Ophthalmol Vis Sci 1989; 30:1565-8.
56. Palmer RM, McDonald MB. A corneal lens/shield system to promote postoperative
corneal epithelial healing. J Cataract Refract Surg 1995; 21:125-6.

33
57. Erwin LR. Glucan/collagen therapeutic eye shields. US4946450 (1990).
58. Taravella MJ, Balentine J, Young DA, Stepp P.Collagen shield delivery of
ofloxacin to the human eye. J Cataract Refract Surg1999; 25:562-5.
59. Zimmer AK, Zerbe H, Kreuter J. Evaluation of pilocarpine-loaded albumin
particles as drug delivery systems for controlled delivery in the eye I. In-vitro and
in vivo characterization. J Control Release 1994; 32:57-70.
60. Zimmer AK, Chetoni P, Saettone MF, Zerbe H , Kreuter J. Evaluation of
pilocarpine-loaded albumin particles as controlled drug delivery systems for the eye
II. Co-administration with bioadhesive and viscous polymers. J Control Release
1995; 33:31-46
61. Bin Choy Y, Park JH, Prausnitz MR. Mucoadhesive microparticles engineered for
ophthalmic drug delivery. J Phys Chem Solids 2008; 69:1533-36.
62. Calvo P, Vila-Jato JL, Alonso MJ. Comparative In-vitro evaluation of several
colloidal systems, nanoparticles, nanocapsules, and nanoemulsions, as ocular drug
carriers. J Pharm Sci 1996; 85:530-6.
63. Calvo P, Alonso MJ, Vila-Jato JL, Robinson JR. Improved ocular bioavailability of
indomethacin by novel ocular drug carriers. J Pharm Pharmacol 1996;48:1147-52.
64. Pignatello R, Bucolo C, Puglisi G. Ocular tolerability of Eudragit RS100 and
RL100 nanosuspensions as carriers for ophthalmic controlled drug delivery. J
Pharm Sci 2002; 91:2636-41.
65. Pignatello R, Bucolo C, Ferrara P, Maltese A, Puleo A, Puglisi G. Eudragit RS100
nanosuspensions for the ophthalmic controlled delivery of ibuprofen. Eur J Pharm
Sci 2002; 16:53-61.
66. Pignatello R, Bucolo C, Spedalieri G, Maltese A, Puglisi G. Flurbiprofen loaded
acrylate polymer nanosuspensions for ophthalmic application. Biomaterials 2002;
23:3247-55.
67. Gupta AK, Madan S, Majumdar DK, Maitra A. Ketorolac entrapped in polymeric
micelles: preparation, characterization and ocular anti-inflammatory studies. Int. J.
Pharm. 2000; 209:1-14.

34
68. Adibkia K, Siahi MR, Nokhodchi A, Javadzedeh AR, Barzegar-Jalali M, Barar J,
Mohammadi G, Omidi Y. Piroxicam nanoparticles for ocular delivery:
physicochemical characterization and implementation in endotoxin-induced uveitis.
J Drug Target, 2007; 15(6):407-16.
69. Vega E, Egea MA, Valls O, Espina M, Garcia ML. Flurbiprofen loaded
biodegradable nanoparticles for ophthalmic administration. J Pharm Sci 2006;
95:2393-405.
70. Muller RH, Mader K, Gohla S. Solid lipid nanoparticles (SLN) for controlled drug
delivery-a review of the state of the art. Eur J Pharm Biopharm 2000; 50:161-77.
71. Muller RH, Petersen RD, Hommoss A, Pardeike J. Nanostructured lipid carriers
(NLC) in cosmetic dermal products. Adv Drug Deliv Rev 2007; 59:522-30.
72. Muller RH, Radtke M, Wissing SA. Solid lipid nanoparticles (SLN) and
nanostructured lipid carriers (NLC) in cosmetic and dermatological preparations.
Adv Drug Deliv Rev 2002; 54 (Suppl 1):S131-55.
73. Souto EB, Mehnert W, Muller RH. Polymorphic behaviour of Compritol 888 ATO
as bulk lipid and as SLN and NLC. J Microencapsul 2006; 23: 417-33.
74. Souto EB, Muller RH. Investigation of the factors influencing the incorporation of
clotrimazole in SLN and NLC prepared by hot high pressure homogenization. J
Microencapsul 2006; 23:377-88.
75. Attama AA, Schicke BC, Muller-Goymann CC. Further characterization of
theobroma oil-beeswax admixtures as lipid matrices for improved drug delivery
systems. Eur J Pharm Biopharm 2006; 64:294-306.
76. Attama AA, Reichl S, Muller-Goymann CC. Diclofenac sodium delivery to the
eye: In-vitro evaluation of novel solid lipid nanoparticle formulation using human
cornea construct. Int J Pharm 2008; 355:307-13.
77. Niesman MR. The use of liposomes as drug carriers in ophthalmology. Crit Rev
Ther Drug Carrier Syst. 1992;9(1):1-38.
78. Smolin G, Okumoto M, Feiler S, Condon D. Idoxuridine-liposome therapy for
herpes simplex keratitis. Am J Ophthalmol 1981; 91:220-5.

35
79. Schaeffer HE, Krohn DL. Liposomes in topical drug delivery. Invest Ophthalmol
Vis Sci 1982; 22:220-7.
80. Taniguchi K, Itakura K, Yamazawa N, Morisaki K, Hayashi S, Yamada Y Morisaki
K, Hayashi S, Yamada Y Morisaki K, Hayashi S, Yamada Y Morisaki K, Hayashi
S, Yamada Y. Efficacy of a liposome preparation of anti-inflammatory steroid as an
ocular drug-delivery system. J Pharmacobiodyn 1988; 11:39-46.
81. Schaeffer HE, Breitfeller JM, Krohn DL. Lectin-mediated attachment of liposomes
to cornea: influence on transcorneal drug flux. Invest Ophthalmol Vis Sci 1982;
23:530-3.
82. Kaufman HE, Steinemann TL, Lehman E, Thompson HW, Varnell ED, Jacob-
LaBarre JT, Gebhardt BM. Collagen-based drug delivery and artificial tears. J Ocul
Pharmacol 1994; 10:17-27.
83. Liu Y, Sun K, Yao W, Liang N, Mu H, Liang R, Yao C. Corneal penetration of
PAMAM dendrimers-coated puerarin liposomes. Zhongguo Zhong Yao Za Zhi
2010; 35:30-4.
84. Sun KX, Wang AP, Huang LJ, Liang RC and Liu K. Preparation of diclofenac
sodium liposomes and its ocular pharmacokinetics. Yao Xue Xue Bao 2006;
41:1094-1098.
85. Aggarwal D, Garg A, Kaur IP. Development of a topical niosomal preparation of
acetazolamide: preparation and evaluation. J Pharm Pharmacol 2004; 56:1509-17.
86. Abdelbary G, El-Gendy N. Niosome-encapsulated gentamicin for ophthalmic
controlled delivery. AAPS PharmSciTech 2008; 9:740-7.
87. Vyas SP, Mysore N, Jaitely V, Venkatesan N. Discoidal niosome based controlled
ocular delivery of timolol maleate. Pharmazie 1998; 53:466-9.
88. Abdelkader H, Ismail S, Kamal A, Alany RG. Design and evaluation of controlled-
release niosomes and discomes for naltrexone hydrochloride ocular delivery. J
Pharm Sci 2011; 100:1833-46.

36
89. Weyenberg W, Vermeire A, Remon JP, Ludwig A. Characterization and in vivo
evaluation of ocular bioadhesive minitablets compressed at different forces. J
Control Release 2003; 89:329-40.
90. Weyenberg W, Bozdag S, Foreman P, Remon JP, Ludwig A. Characterization and
in vivo evaluation of ocular minitablets prepared with different bioadhesive
Carbopol-starch components. Eur J Pharm Biopharm 2006; 62:202-9.
91. Fishman PH, Jay WM, Rissing JP, Hill JM, Shockley RK. Iontophoresis of
gentamicin into aphakic rabbit eyes. Sustained vitreal levels. Invest Ophthalmol Vis
Sci 1984; 25:343-5.
92. Hobden JA, Rootman DS, O'Callaghan RJ, Hill JM. Iontophoretic application of
tobramycin to uninfected and Pseudomonas aeruginosa-infected rabbit corneas.
Antimicrob Agents Chemother 1988; 32:978-81.
93. Hobden JA, O'Callaghan RJ, Hill JM, Reidy JJ, Rootman DS, Thompson HW.
Tobramycin iontophoresis into corneas infected with drug-resistant Pseudomonas
aeruginosa. Curr Eye Res 1989; 8:1163-9.
94. Grossman RE, Chu DF, Lee DA. Regional ocular gentamicin levels after
transcorneal and transscleral iontophoresis. Invest Ophthalmol Vis Sci 1990;
31:909-16.
95. Hobden JA, Reidy JJ, O'Callaghan RJ, Insler MS, Hill JM. Ciprofloxacin
iontophoresis for aminoglycoside-resistant pseudomonal keratitis. Invest
Ophthalmol Vis Sci 1990; 31:1940-4.
96. Pescina S, Ferrari G, Govoni P, Macaluso C, Padula C, Santi P, Nicoli S. In-vitro
36permeation of bevacizumab through human sclera: effect of iontophoresis
application. J Pharm Pharmacol 2010; 62:1189-94.
97. Molokhia SA, Jeong EK, Higuchi WI, Li SK. Transscleral iontophoretic and
intravitreal delivery of a macromolecule: study of ocular distribution in-vivo and
postmortem with MRI. Exp Eye Res 2009; 88:418-25.
98. Vollmer DL, Szlek MA, Kolb K, Lloyd LB, Parkinson TM. In-vivo transscleral
iontophoresis of amikacin to rabbit eyes. J Ocul Pharmacol Ther 2002; 18:549-58.

37
99. Singh RP, Mathews ME, Kaufman M, Riga A. Transcleral delivery of
triamcinolone acetonide and ranibizumab to retinal tissues using macroesis. Br J
Ophthalmol 2010; 94:170-3.
100. Harry J and Mission G. Clinical Ophthalmic Pathology, Principles of Diseases of
the Eye and Associated Structures, Butterworth Heinemann, Oxford, UK, 2001.
101. Chang J H and Chung H. Non-steroidal anti-inflammatory drug and endotoxin
induced uveitis. Korean. J. Ophthalmol. 1993; 7:35-42.
102. Polansky J and Weinreb R. Steroids as anti-inflammatory agent. In M. Sears (ed.),
Pharmacology of the Eye, Springer, New York, 1984, pp. 460-583.
103. Raizman M. Corticosteroid therapy of eye diseases; fifty years later. Arch.
Ophthalmol. 1996; 114:1000-1001.
104. Waterbury L, Kunysz EA and Bewerman R. Effect of steroidal and non steroidal
anti-inflammatory agents on corneal wound healing. J. Ocul. Pharmacol. 1987;
3:43-54.
105. Schalnus R. Topical nonsteroidal anti-inflammatory therapy in ophthalmology.
Ophthalmologica 2003; 217:89-98.
106. Bandare BM, Sankaridurg PR and Willcox MD. Nonsteroidal anti-inflammatory
agents decrease bacterial colonization of contact lenses and prevent adhesion to
human corneal epithelial cells. Curr. Eye Res. 2004; 29:245-251.
107. Rojanasakul Y and Robinson JR. Transport mechanisms of the cornea:
characterization of barrier permselectivity. Int. J. Pharm. 1989; 55:237-246.
108. Grau M, Montero JL, Guasch J, Felipe A, Carrasco E, Julia S. The pharmacological
profile of aceclofenac, a new non steroidal anti-inflammatory and analgesic drug.
Agents Actions Suppl. 1991; 32: 125-129.
109. Hinz B, Auge D, Rau T, Rietbrock S, Brune K, Werner U. Simultaneous
determination of aceclofenac and three of its metabolites in human plasma by high
performance liquid chromatography. Biomed. Chromatogr. 2003; 17:268-275.
110. Dooley M, Spencer CM, Dunn CJ. Aceclofenac: a reappraisal of its use in the
management of pain and rheumatic disease. Drugs 2001; 61: 1351-78.

38
111. Neil M.J,editor. The Merck index: an Encyclopedia of chemicals, drugs and
biologicals. 14th ed. Whitehouse station, NJ, USA, Merck Research Laboratories
Division of Merk &Co., 2006, 582
112. Martindale. The Complete Drug Reference. 33th
edition, Pharmaceutical Press
2002.
113. Rowe RC, Sheskey PJ, Owen SC. Polymethacrylates In: Handbook of
Pharmaceutical Excipients, 5th
ed.,2009, 553-560