Embed Size (px)
Citation preview

Fine-Needle Aspiration Biopsy of the Mediastinum
JAMES LINDER, M.D.
Omaha, Nebraska
GREGG A. OLSEN, M.D. WILLIAM W. JOHNSTON, M.D., F.I.A.C.
Durham, North Carolina
From the Division of Cytopathology, Department of Pathology, Duke University Medical Center, Durham, North Carolina, the Department of Pa- thology and Microbiology, University of Nebras- ka Medical Center, Omaha, Nebraska, and the Division of Hematology-Oncology, Department of Internal Medicine, Duke University Medical Center, Durham, North Carolina. Requests for reprints should be addressed to Dr. James Linder, Department of Pathology and Microbiolo- gy, University of Nebraska Medical Center, 42nd and Dewey Avenue, Omaha, Nebraska 68105. Manuscript submitted December 11, 1985, and accepted January 13, 1986.
Fine-needle aspiration is a useful technique to identify neoplasms of many sites, such as breast, thyroid, and lung. Thirty-two mediastinum aspirates from 29 patients were reviewed. Five aspirates yielded insufficient material. Five aspirates were of benign lesions. Four aspi- rates were suggestive of. but not diagnostic of malignancy. Eighteen aspirates contained malignant cells; in 13 of these, a definite cell type was identified, which usually was metastatic lung carcinoma; in five instances, the cell type could not be unequivocally identified. Compli- cations were minimal, two instances of pneumothorax (6.3 percent) and two of hemoptysis (6.3 percent). No deaths or hemorrhage oc- curred. In 16 of the 29 patients [55 percent), thoracotomy was avoided because of fine-needle aspiration biopsy. It is concluded that fine-needle aspiration biopsy of the mediastinum is a safe, useful diagnostic tool. This procedure may obviate the need for thoracotomy in persons with inoperable cancer, thus lowering medical costs and length of hospital stay.
Fine-needle aspiration biopsy, widely used in Europe, has become popu- lar in the United States as pressure for cost-containment intensifies. Significant cost savings have been proved in fine-needle aspiration biopsy evaluation of breast and thyroid neoplasms [ 1,2]. The application of fine-needle aspiration biopsy to mediastinal lesions poses unique considerations, because of the diversity of mediastinal neoplasms and the proximity of the heart and great vessels. Despite this, isolated reports have described the cytopathology of mediastinal aspirates [3-51. In this report, we describe our experience in mediastinal fine-needle aspiration biopsy, emphasizing the diagnostic accuracy and safety of this proce- dure.
PATIENTS AND METHODS
Patient Selection. All percutaneous transthoracic cases of fine-needle aspiration biopsy at Duke University Medical Center from January 1979 to December 1983 (six years) were reviewed. For this study, we defined the mediastinum as the region bounded laterally by the pleural cavities, superi- orly by the thoracic inlet and inferiorly by the diaphragm [6]. Lesions lying within the hila of the lungs, cephalad to the manubrium, or within boney structures of the thorax were excluded. During our study, 32 mediastinal aspirates were obtained in 29 patients. The patients, who ranged from j6 to 82 years of age, all had radiologic suggestion of a mediastinal mass (Table I). Fine-needle aspiration biopsy was performed by vascular radiologists, with fluoroscopic or computed tomographic guidance, using 22-gauge needles. Cytopathologic Analysis. Immediately after the aspiration, biopsy speci-
December 1986 The American Journal of Medicine Volume 81 1005
MEDIASTINAL FINE-NEEDLE ASPIRATION BIOPSY-LINDER ET AL
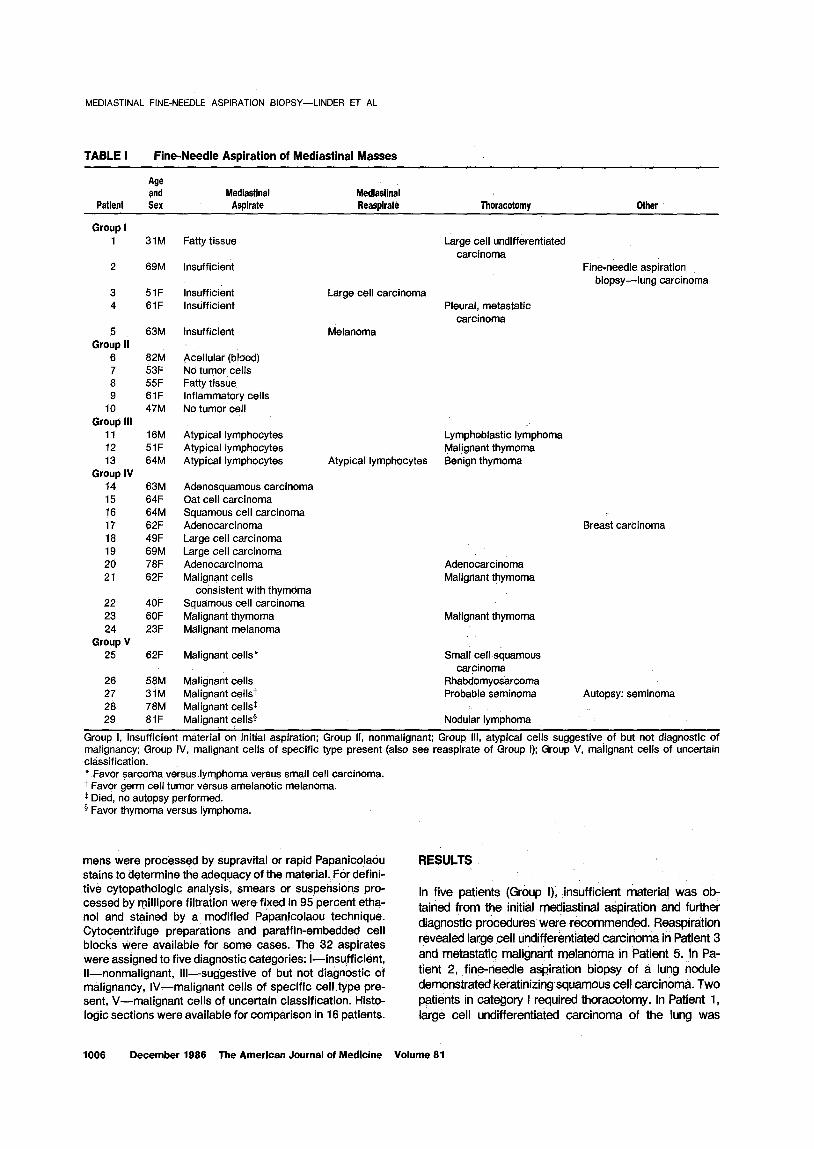
TABLE I Fine-Needle Aspiration of Mediastinai Masses
Patient
Age and Sex
Mediastinal Aspirate
Medtastinal Reaspirate Thoracotomy Other
Group I 1 31M
2 69M
3 51F 4 61F
5 63M Group II
6 82M 7 53F 8 55F 9 61F
10 47M Group III
11 16M 12 51F 13 64M
Group IV 14 63M 15 64F 16 64M 17 62F 18 49F 19 69M 20 78F 21 62F
22 40F 23 6OF 24 23F
Group V 25 62F
26 58M 27 31M 28 78M 29 81F
Fatty tissue
Insufficient
Insufficient Insufficient
Large cell carcinoma
Insufficient Melanoma
Acellular (blood) No tumor cells Fatty tissue inflammatory cells No tumor cell
Atypical lymphocytes Atypical lymphocytes Atypical lymphocytes Atypical lymphocytes
Adenosquamous carcinoma Oat cell carcinoma Squamous cell carcinoma Adenocarcinoma Large cell carcinoma Large cell carcinoma Adenocarcinoma Malignant cells
consistent with thymoma Squamous cell carcinoma Malignant thymoma Malignant melanoma
Malignant cells*
Malignant cells Malignant cellst Malignant cellsx Malignant cell&
Large cell undifferentiated carcinoma
Fine-needle aspiration biopsy-lung carcinoma
Pleural, metastatic carcinoma
Lymphoblastic lymphoma Malignant thymoma Benign thymoma
Breast carcinoma
Adenocarcinoma Malignant thymoma
Malignant thymoma
Small cellsquamous carcinoma
Rhabdomyosarcoma Probable seminoma Autopsy: seminoma
Nodular lymphoma
Group I, insufficient material on initial aspiration; Group II, nonmalignant; Group Ill, atypical cells suggestive of but not diagnostic of malignancy; Group IV, malignant cells of specific type present (also see reaspirate of Group I); Group V, malignant cells of uncertain classification. * Favor sarcoma versus lymphoma versus small cell carcinoma. 7 Favor germ cell tumor versus amelanotic melanoma. t Died, no autopsy performed. * Favor thymoma versus lymphoma.
mens were processed by supravital or rapid Papanicolaou stains to determine the adequacy of the material. For defini- tive cytopathologic analysis, smears or suspehsions pro- cessed by rniliipore filtration were fi,xed in 95 percent etha- nol and stained by a modified Papanicolaou technique. Cytocentrifuge preparations and paraffin-embedded cell blocks Were available for some cases. The 32 aspirates were assigned to five diagnostic categories: l-insufficient, ll-nonmalignant, Ill-suggestive of but not diagnostic of malignancy, IV-malignant cells of specific cell type pre- sent, V-malignant cells of uncertain classification. Histo- logic sections were available for comparison in 16 patients.
RESULTS
In five patients (Group I); insufficient material was ob- tained from the initial m$iastinal aspiration and further diagnostic procedures were recommended. Reaspiration revealed large ceil undifferentiated carcinoma in Patient 3 and metastatic malignant melanoma in Patient 5. in Pa- tient 2, ,fine-needle aspiration biopsy of a lung nodule demonstrated keratinizingsquamous ceil carcinoma. Two patients in category I required thoracotomy. in Patient 1, large ceil undifferentiated carcinoma of the lung was
1006 December 1966 The American Journal of Medicine Volume 61

MEDIASTINAL FINE-NEEDLE ASPIRATION BIOPSY-LINDER ET AL
diagnosed; however, no tumor was found in the mediasti- num. In Patient 4, widely me&static lung carcinoma was identified.
In five patients (Group II), nonmalignant diagnoses were rendered. Three of these patients were without known malignancy, but had mediastinal enlargement on chest radiography. Aspirates of Patients .6 and 7 yielded only blood! .and simultaneous fluoroscopic examination sug- gested the mediastinal prominence represented promi- nent pulmonary vasculature. No complication occurred from the aspiration of these bland vessels; however, both patients died approximately seven months later of myo- cardial infarction and brain .stem stroke, respectively. Patient 8 had an..enlarged~ left scalene lymph node, and mediastinal prominence ,on chest radiography. Histologi- cally, the lymph node was’ replaced by fati extensive sampling of the mediastinum by. fine-needle aspiration biopsy revealed only fatty tissue. The patient is well after 18 months of follow-up. Patients 9 and 10 had cutaneous malignant-melanoma. Chest radkgraphy in each suggest- ed a viidened mediastinum; however; fine-needle aspira- tion biopsy yielded no ,malignant cells. After one year, neither patient had evidence of mediastinal tumor.’
In four aspirates (Group Ill), cells suggestive of but not diagnostic of malignancy were seen. In Patient 1 l., the fine-needle aspiration.biopsy specimen consisted of small lymphocytes with scant cytoplasm and contoured nuclei with indistinct nucleoli; tissue obtained from thoracotomy was a lymphoblastic lymphoma, T cell type. In Patient i 2, rare epitheiioid cells were intermixed with numerous small lymphocytes. Tissue biopsy demonstrated a malig- nant. thymoma invading the pleura. Initial, and repeated fine-needle aspiration biopsy in Patient 13 revealed small lymphocytes and an occasional epithelioid cell. Tissue biopsy demonstrated a benign, encapsulated thymoma.
‘Cells meeting cytologic criteria for malignancy were present in 18 aspirates, representing 56 percent of the study. In 13 instances, a definite cell type was identified (Group IV). Eight of the 13 were metastases from an occult lung carcinoma, three of these were large cell undifferentiated carcinoma, two were squamous cell car- cinoma, and one each was adenocarcinoma, adenosqua- mous carcinoma, and small cell anaplastic carcinoma, on the basis of previously described cytologic criteria [7]. Patient 17 exhibited clusters of uniform cells with a high nuclear-to-cytoplasmic ratio and hyperchromatic nuclei. A history of breast carcinoma was elicited, and the fine- needle aspiration biopsy specimen was morphologically similar to the breast primary. Patient 21 had biphasic cytomorphologic features with one component of cohe- sive, pleomorphic epithelial cells, and another of small lymphocytes. Thoracotomy demonstrated a thymoma re- placing the mediastinum and invading the innominate vein.
Five patients (Patients 25 to 29) had cytologic features of malignancy, but insufficient features to identify a cell
type with absolute certainty (Group V). A differential diag- nosis including thymoma, small cell anaplastic carcino- ma, lymphoma; or germ cell tumor was suggested. Four patients in this group underwent. thoracotomy. Light and electron microscopy showed a small cell squamous car- cinoma in Patient 25, and an embryonal rhabdomyosar- coma in Patient 26. A biopsy specimen from Patient 27 was suspected to represent an anaplastio seminoma, but this diagnosis was not established until autopsy. Histologic study and immunologic cell surface markers showed Pa- tient 29 to have a B cell lymphoma, poorly differentiated lymphocytic type. One patient, Patient 28, refused thora- cotomy and died shortly thereafter. Autopsy was not permitted.
COiilMENTS Fine-needle aspiration biopsy is a well-established diag- nostic tool, readily applied to most body sites with low risk to the patient ,and high probability for diagnostic yield. Several excellent monographs describe the range and utility of the technique [8-lo]. Fine-needle, aspiration biopsy is a particularly attractive method to evaluate the mediastinum. This small body site. contains organs that can give rise to diverse primary neoplasms, and lymph nodes that frequently harbor metastatic carcinoma [6]. The shielding of the mediastinum.by,the sternum, plus the proximity of the heart and great vessels, complicates the diagnosis of mediastinal lesions. Thoracotomy and me- diastinoscopy may yield mediastinal, tissue, ,but are more complicated than fine-needle aspiration biopsy. Medias- tinoscopy, furthermore, does not permit full examination of the posterior mediastinum, subcarinal region, and sub- a&tic region [ 111. Mediastinal fine-needle aspiration biop- sy can be guided by fluoroscope or computed tomograph- ic scanner, with the latter offering more precise place- ment of the biopsy needle [ 12,131: Both 20-gauge and 22-gauge thin-wall needles have been used successfully. The former enables aspiration of larger amounts of mate- rial, and the latter theoretically offers a greater margin of safety if the aorta, superior vena cava, and pulmonary vessels are punctured.
The efficiency of mediastinal fine-needle aspiration biopsy is well illustrated by our study; with repeated aspiration, suitable material was obtained in 26 of 29 patients (89.7 percent). In the Ikerature, 72 percent to 82 percent of mediastinal asp/rates have yielded diagnostic material [4,13,14]. Metastatic carcinoma was found in 64 percent of our patients. Similar findings were reported by Jereb and Us-Krasovec [4] (62 percent) and by Rosen- berger [ 141 (55.6 percent). Me&stases are usually de- rived from occult lung carcinoma, although our series included metastatic melanoma and breast carcinoma. Some mediastinal tumors may be difficult to precisely identify by the aspiration technique [ 141. In our series, distinguishing lymphoma from thymoma and seminoma with complete certainty was difficult. Since we always
December 1988 The American Journal of Medicine Volume 81 1007

MEDIASTINAL FINE-NEEDLE ASPIRATION BIOPSY-LINDER ET AL
endeavored to provide a diagnosis suitable to initiate treatment, we reported five cases as “malignant cells of uncertain classification” and recommended thoracotomy to obtain tissue for histologic examination. We also found difficulty in cytologically distinguishing “benign” and “ma- lignant” thymomas. In many.instances, this distinction can only be made by gross evidence of thymoma invading mediastinal structures. There were no false-positive re- sults in our cases. Five of the initial aspirates did not yield sufficient material. In these cases, the clinical suspicion of neoplasia prompted reaspiration or thoracotomy for diagnosis.
Five patients who underwent fine-needle aspiration biopsy because of the radiologic impression of a medias- tinal mass had no mediastinal tumor by this form of biopsy. These are believed to be true-negative results, since no patient has mediastinal tumor after one-year follow-up. Before any aspirate is interpreted as benign, however, the utmost care must be taken to insure thor- ough sampling.
No serious complication occurred in our patients, al- though two had small pneumothoraces and two had mild
1.
2.
3.
4.
hemoptysis (6.3 percent each). Previous reports of he- moptysis cdmplicating mediastinal fine-needle aspiration biopsy range from 3 percent to 10.4 percent, and pneu- mothorax from 14 percent to 2 1 percent [ 13-151. Our lower incidence of pneumothorax may reflect the small gauge needles used, compared with the 18- or 20-gauge needles used by others. Significant hemorrhagic compli- cations have not occurred in mediastinal fine-needle aspi- ration biopsy. The risk of transthoracic aspiration can be minimized by not performing mediastihal aspiration in patients receiving anticoagulants or with hemorrhagic di- athesis, arterial-venous malformation, pulmonary’ hyper- tension, severe emphysema, or pulmonary hydatid cyst [151.
Mediastinal fine-needle aspiration biopsy is less com- plicated thah thoracotomy and. mediastinoscopy: It is valu- able to confirm maiignancy when the lesion is inoperable, to distinguish metastatic from primary mediastinal tumors, and to identify infections via morphologic evaluation or culture. Fine-needle aspiration biopsy of the mediastinum is a safe and efficacious technique useful in cost-effective medical care.
REFERENCES
Kaminsky DB: Aspiration biopsy in the content.of the new Medicare fiscai policy. Acta Cytol 1984; 28: 333-336.
Hamberger B, Gharib H, Melton LJ, Goellner JR, Ztnsmeister AR: Fine-needle aspiration biopsy of thyroid nodules. Im- pact on thyroid practice and cost of care. Am J Med 1982; 73: 38 l-384.
Dahlgren SE, Ovenfors CO: Aspiration biopsy diagnosis of neurogenous mediastinal tumors. Acta Radio1 1970; 10: 289-298.
Jereb M, Us-Krasovec M: Transthoracic needle biopsy of mediastinal and hilar lesions. Cancer 1977; 40: 1354-1357.
Francis D, Hojgaard K: Transthoracic aspiration biopsy. Acta Pathol Microbial lmmunol Stand [A] 1977; 85: 889-896.
Silverman NA, Sabiston DC: Mediastinal masses. Surg Clin North Am 1980; 60: 757-777.
Johnson WW, Frable WJ: The cytopathology of the respira- tory tract. Am J Pathol 1976; 84: 372-424.
Dahlgren S, Nordenstrom B: Transthoracic needle biopsy. Chicago: Year Book Medical Publishers, 1966.
9. Frable WJ: Thin-needle aspiration biopsy. Philadelphia: Saunders, 1983.
10. Zajicek J: Aspiration biopsy cytofogy. Part I. Cytology of supradiaphragmatic organs. Monogr Clin Cytol 1974; 4: l-27.
11. Pearson FJ, Nelems JM, Henderson RD. et al: The role of mediastinoscopy in the selection of treatment for bron- chial carcinoma with involvement of superior mediastinal lymph nodes. J Thorac Cardiovasc Surg 1972; 64: 382-407.
12. Schechter DC, Acinapara AJ: Pulmonary diagnostic invasive procedures. NY State J Med 1980; 80: 1577-1589, 1702-1711.
13. Westcott JL: Percutaneous needle aspiration of hilar and mediastinal masses. Diagn Radio1 1981; 141: 232-239.
14. Rosenberger A, Adler OB: Fine-needle aspiration biopsv of mediastinal masses. Isr J Med Sci 198t; 17: 49-52. -
15. Sander DE, Thorn&on BW. Budden BJE: Percutaneous asoi- ration lung biopsy. Can’ Med Assoc J 1971; 104: 139- 142.
1008 December 1988 The American Journal of Medicine Volume 81





























