Embed Size (px)
Citation preview

Document 1.4
Firefighter Prehospital Care Program Module 5
Firefighter Prehospital Care Program Firefighter Prehospital Care Program Module 5Module 5
Airway Management & O2 Delivery

Objectives• Review airway anatomy and
physiology of breathing• Understand principles of
airway management• Recognize and manage an
obstructed airway• Use basic and advanced
airway procedures and adjuncts to maintain airway
• Effectively ventilate or assist ventilations
• Deliver supplemental oxygen using a variety of devices

Physiology of Breathing• Respiration brings oxygen for metabolism into
the alveoli, where it is picked up by red blood cells
• Waste carbon dioxide is carried in the blood into the alveoli, where it is removed through respiration
• Breathing depends on: – An intact airway– Lungs with an adequate surface area for gas exchange– Muscles which provide the force for air movement

Anatomy of the Airway•Can be obstructed by tongue and foreign materials•Protected by reflexes (coughing/gagging) that are impaired in the unconscious and semiconscious patients

Assessing Airway Patency• A speaking patient means airway is open and the
patient is breathing• Hoarseness can be a sign of airway burns or
disease that will threaten the airway• Noisy inhalations (stridor) suggests partial airway
obstruction• Assume airway needs to be kept open in the
unconscious patient

Basic Airway Management
hCheck for patencyh Is the patient able to
speak?hHead tilt/chin lifthModified jaw thrust (if
c-spine precautions are needed)
h If not breathing: give 2 breaths

Obstructed Airway• The majority of obstructions are the result of the
tongue and improve with head tilt or jaw thrust• If two breaths do not cause visible chest rise,
reposition the head/jaw• If still obstructed:
– Check mouth for foreign material (food, vomit, blood)– Finger sweep– Suction– Chest compressions

Finger Sweeps •Use body fluid precautions (gown, glove, mask, face shield, bunker gear)•Used to remove visible foreign material•Do not perform blind finger sweeps (may cause bleeding or push objects deeper)•Perform tongue jaw lift•Visualize foreign material•Insert finger in patient’s mouth•Hook finger and remove obstruction

Suction•A patient needs to be suctioned when gurgling is heard during breathing or ventilation, or visible vomit, fluid or blood is seen in the mouth
•Purpose is to remove blood, liquids, food particles from the airway
Portable Electric Suction
Hand-operated Suction
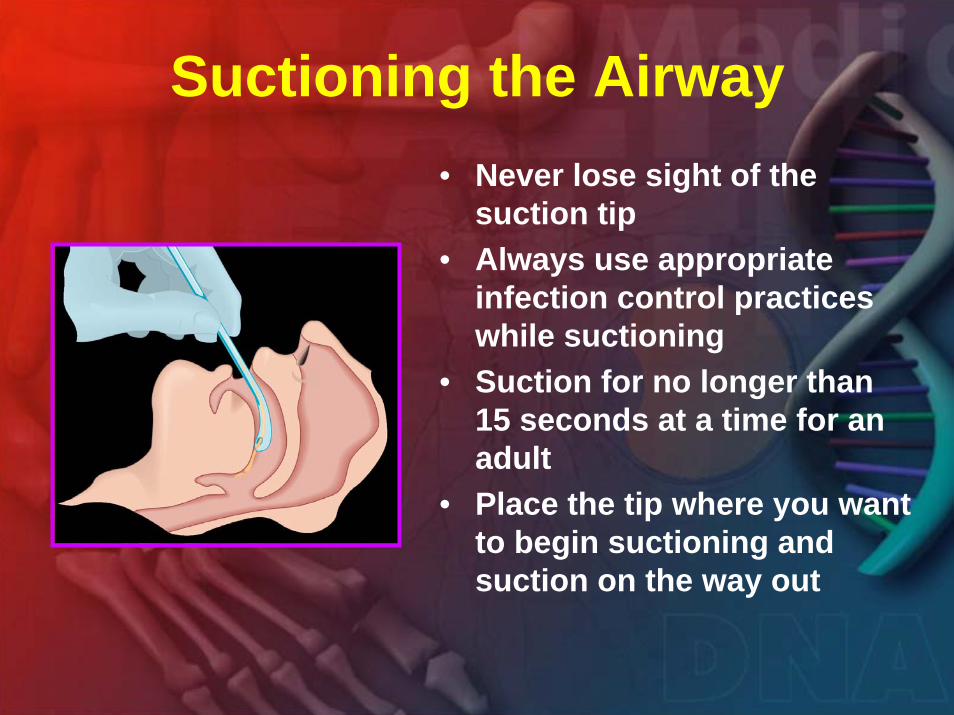
Suctioning the Airway• Never lose sight of the
suction tip• Always use appropriate
infection control practices while suctioning
• Suction for no longer than 15 seconds at a time for an adult
• Place the tip where you want to begin suctioning and suction on the way out

Recovery Position
•Gravity keeps the airway clear of tongue and foreign material•Useful in patients who are breathing well and not injured (never use if suspected spinal injury)•Monitor patients’ breathing and pulse while in this position until paramedic arrival•Not used if patient is not breathing or needs active treatment

Oropharyngeal Airways (OPA)
• A curved plastic device to keep the tongue from obstructing the airway
• Variety of sizes• OPA flange rests against
the patient’s lips• Will stimulate gagging in a
conscious or semiconscious patient

Sizing an Oropharyngeal Airway
Measure from the corner of the mouth to the ear lobe

Insert Airway Upside Down

Rotate Airway 180o

Child Oropharyngeal Airway

Nasopharyngeal Airways•Same purpose as oropharyngeal airways
•Better tolerated in patients with gag reflex
•May cause nosebleeds
•Size airway from the tip of the patient’s nose to the ear lobe
•Lubricate before use

•Insert airway with bevel towards the septum
•Slowly rotate airway while inserting
•STOP! If resistance is met when advancing

Assessing Breathing
Adult
Child
Infant
Neonate
12 - 20 breaths per minute
15 - 30 breaths per minute
25 - 40 breaths per minute
Up to 50 breaths per minute
Look for adequate chest rise and fall and adequate rate of breathing
Assessing Adequate Respirations
ADULTS At least 8 breaths per minute, visible chest rise
Children& Infants
Newborns
At least 10 breaths per minute
At least 20 breaths per minute
Prepare to assist ventilations if respiratory rate is too slow or too shallow

Artificial Respiration
•Inhaled air has 21% O2
•Exhaled air still has 16% O2
•Mouth to mouth can sustain life
•Other devices can provide barriers to infection or increase oxygen delivery
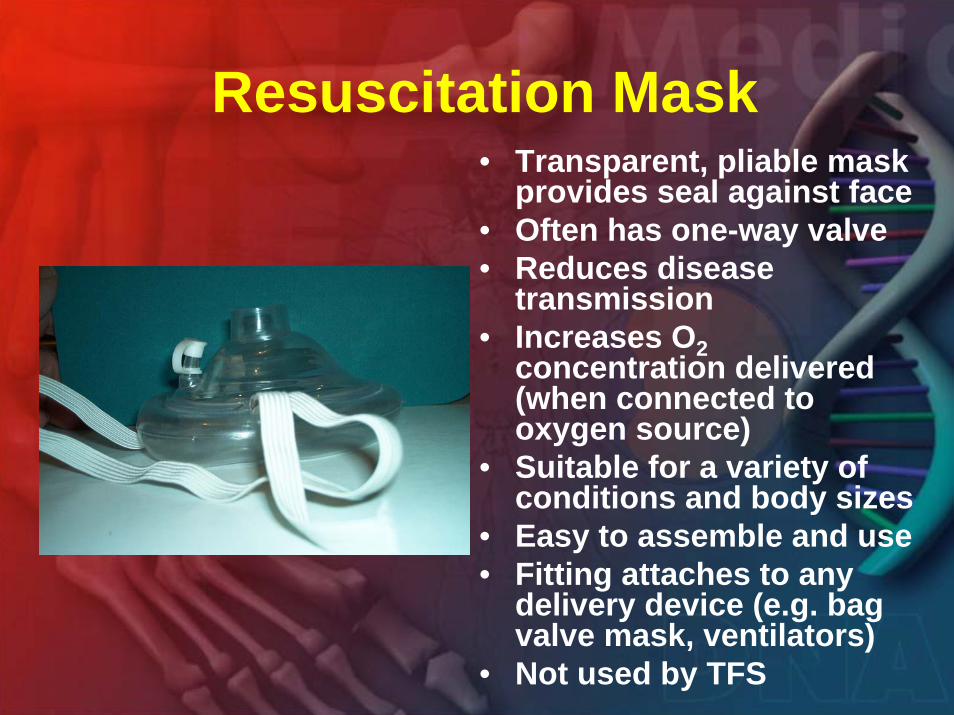
Resuscitation Mask• Transparent, pliable mask
provides seal against face• Often has one-way valve• Reduces disease
transmission• Increases O2
concentration delivered (when connected to oxygen source)
• Suitable for a variety of conditions and body sizes
• Easy to assemble and use• Fitting attaches to any
delivery device (e.g. bag valve mask, ventilators)
• Not used by TFS

Bag Valve Mask (BVM)
• Delivers nearly 100% O2 when hooked up to oxygen supply
• More effective when used by 2 rescuers
• Provides feedback as to airway resistance
• Reduces disease transmission

Bag Valve Mask (BVM )• Open airway (head tilt/chin lift or jaw thrust)• Check breathing• Insert airway• Place mask (one rescuer to provide seal if possible)• Squeeze bag (second rescuer using only one hand,
watch for visible chest rise)Disadvantages:• Difficult to master for one rescuer• Requires regular practice to stay proficient• Causes gastric distension with air• May take longer to assemble• Not readily available in some settings

Supplemental Oxygen Delivery• Used in patients who are
breathing spontaneously• Nasal cannula used with
patients who need only 24 - 44% oxygen (e.g. chronic lung disease)
• Simple face mask delivers 35 - 55% oxygen
• Non-rebreather mask delivers 80 - 90% oxygen; first choice in emergency setting

Medical Oxygen• Atmospheric oxygen is 21%• Medical oxygen is 99.995%• Cylinders come in various
sizes• At high flow rates:
→ D = 21 minutes (found in most EMS/Fire oxygen bags)
→ E = 37 minutes→ M = 181 minutes
(installed in most ambulances)

Oxygen Cylinder
• Distinctive white top• 3 pin neck – only connects to oxygen
regulators• Yellow diamond marking that says
‘Oxidizer’• Made of steel or an alloy• D cylinder holds 350 litres of oxygen
Cylinder Safety• Cylinder has an internal
pressure of approximately 2000 pounds per square inch (PSI)
• The oxygen cylinder must always be in a secure state

Oxygen Regulator and Flowmeter• Reduces O2 pressure
from 2000 PSI to 70 PSI• Gauge indicates
pressure in the cylinder • Largest pin has a
gasket• Flow valve adjusts flow
between 1 and 15 litresper minute
Pressure Regulator
Pressure gaugeFlow valve
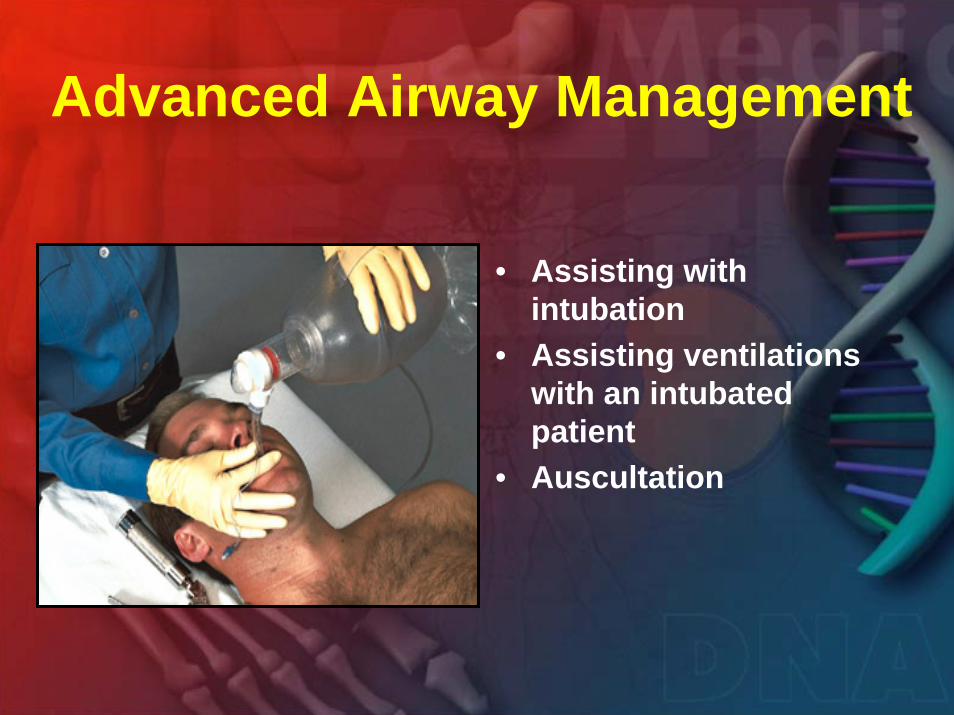
Advanced Airway Management
• Assisting with intubation
• Assisting ventilations with an intubated patient
• Auscultation

Endotracheal Tube
15 mm adapter (connects to
BVM)
Inflation port
Cuff
Murphy Eye

Assisting with Intubation
Cricothyroidmembrane
Thyroidcartilage
CricoidCartilage Esophagus
Trachea
•“BURP” maneuver
•Helps paramedic see airway/vocal cords
•Cricoid Pressure
•Helps reduce gastric distension

Ventilating the Intubated Patient• An OPA can be used to
protect the tube from patient’s teeth
• Hold the tube with 2 fingers
• Never push or pull on the tube
• Squeeze BVM with one hand; watch for chest rise
• Resistance to squeezing is an alert to possible problems

Auscultation
Listen in 4 areas
• Listen to upper chest and lower chest
• Normal breath sounds are quiet
• Compare left and right
• Sounds should be similar on both sides
• Less breath sounds on one side suggests disease, injury, or a dislodged endotracheal tube
• Include findings in report to paramedics

Summary
– Airway anatomy and the physiology of breathing & the principles of airway management
– Recognition and management an obstructed airway
– Basic and advanced airway procedures and adjuncts to maintain an airway
– How to effectively ventilate or assist ventilations
– How to deliver supplemental oxygen using a variety of devices
In this module we have discussed and/or practiced:
Any Questions ?