Embed Size (px)
Citation preview

FIRST-LINE THERAPY FOR ADVANCED NSCLC
Rogerio C. Lilenbaum, MD
Clinical Associate Professor of Medicine
University of Miami School of Medicine
Director, Thoracic Oncology Program
The Mount Sinai Comprehensive Cancer Center
Miami Beach, FL
QUESTIONS FOR DISCUSSION
• What are the options for 1st line therapy?
• What is the optimal management of the elderly and the PS 2 patients?
• What is the role of the non-platinum regimens?
• What is the role of the molecular targeted agents in 1st line therapy?

Cis/Vin and Cis/Gem vs. Cisplatin : Overall Survival
100%
80%
60%
40%
20%
0%0 12 24 36 48 60
J Clin Oncol 2000, 18:122-30.
P=.004
Su
rviv
al P
rob
abili
ty
1.0
0.90.80.70.6
0.50.40.30.20.10.0
0 5 10 15 20 25
Gem/Cis 260 9.0 39% 15%Cis 262 7.6 28% 8%
N MS 1YS 2YS N MS 1YS 2YSVin/Cis 206 8 36% 12%Cis 209 6 21% 7%
Cis/Vin vs Cisplatin
J Clin Oncol 1998, 16:2459-64.
Cis/Gem vs Cisplatin

MedianSurvival Survival
N Deaths (Months) 1-Year 2-Year1CBDCA+Pac 208 159 8 38% 15% CDDP+Vin 202 156 8 36% 16%
0 6 12 18 24 30Months
100%
80%
60%
40%
20%
0%
Cis-Vinorelbine vs Carbo-Paclitaxel SWOG 9509
1J Clin Oncol. 2001;19:3210-3218.

A Phase III Four-Arm Trial in Advanced NSCLC
Paclitaxel 135 mg/m2 over 24 hours, day 1Cisplatin 75 mg/m2, day 2
Gemcitabine 1000 mg/m2 days 1, 8, and 15Cisplatin 100 mg/m2 day 1
Docetaxel 75 mg/m2 day 1Cisplatin 75 md/m2 day 1
Paclitaxel 225 mg/m2 over 3 hours, day 1Carboplatin AUC=6 day 1
RANDOMIZED
Stratification
PS 0-2
WT Loss
Stage - IIIB, IV
Brain mets (+/-)
Schiller, NEJM 2002:92-98

A Phase III Four-Arm Trial in Advanced NSCLC
Regimen RR (%)
MST (mo.)
TTP
(mo.)
1-yr Survival
(%)
Cis/Paclitaxel 21.3 7.8 3.5 31
Cis/Gemcitabine 21.0 8.1 4.5* 36
Cis/Docetaxel 17.3 7.4 3.6 31
Carbo/Paclitaxel 15.3 8.2 3.3 35
*P = .002 by log rank test

A Phase III Four-Arm Trial in Advanced NSCLC
CIS-PAC CIS-GEM CIS-DOC CARBO-PAC
N = 282 N = 273 N = 278 N = 272
GR 4 ANC 55 37 49 42
Gr 4 thrombocytopenia 2 26* 1 2
Gr 3 nausea 25 36 23 8*
Gr 3 neuropathy 4 8 5 8
Gr 3-4 febrile neutropenia 16 4* 10 3*
Gr 3-5 renal 3 9* 3 1
Worst Gr 4-5 89 70 86 57*
*P < 0.05 vs. Arm A

Tax 326: Randomized Phase III Trialfor Advanced NSCLC
RANDOMIZE
Stratification Factors:
Stage of DiseaseIIIB vs. IV
Region
US/Canada
Latin America
Europe/LebanonIsrael
South Africa/AustraliaNew Zealand
Response assessment every 2 cycles
Docetaxel 75mg/m2 IV
Carboplatin AUC 6 IV Q 3 wks
Vinorelbine 25mg/m2 IV D 1, 8, 15 & 22Cisplatin 100mg/m2 IV D 1Q 4 wks
Docetaxel 75mg/m2 IVCisplatin 75mg/m2 IV Q 3 wks
vs.

406 396 401
10.9 10.0 9.1
46 41 38
21 14 16
Tax 326: Randomized Phase III Trialfor Advanced NSCLC
Docetaxel/ Navelbine/ Docetaxel/
Cisplatin CisplatinCarboplatinN
Median survival (mo)
1-Yr survival (%)
2-Yr survival (%)
Belani et al. 2001
P=.044, Adjusted Log-Rank
2y Survival 21 vs 14%, p=.035
P=.66, Adjusted Log-Rank
2 y Survival 18 vs 14%
Cis/Tax vs. Cis/Nav Carbo/Tax vs Cis/Nav

ASCO 2002
Clinical Trials of 2-Drugs vs 1
Study Therapy MST 1-Yr Surv
CALGB1Paclitaxel
P + Carbo
6.7 m
8.8 m
33%
37%
SLUSG2Gemcitabine
G + Carbo
9.0 m
11.0 m
32%
44%
GCGLC3Docetaxel
D + Cispl
8.0 m
10.1 m
42%
48%
1Proc ASCO 21:1a (A #2), 2002; 2Proc ASCO 21:291a (A #1162), 2002; 3Proc ASCO 21:291a (A #1163), 2002
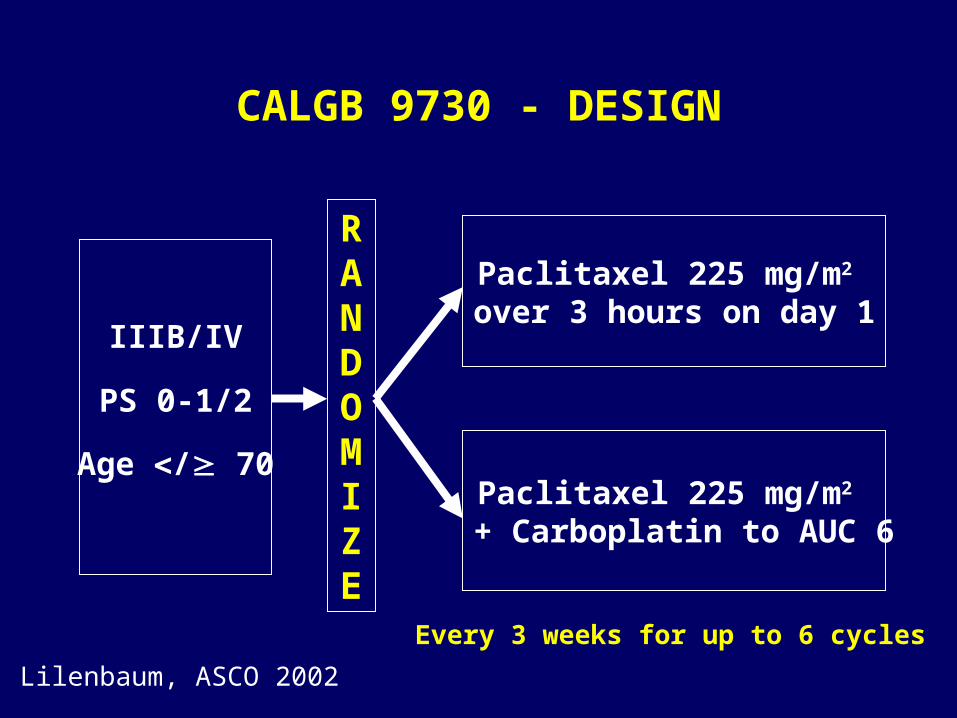
CALGB 9730 - DESIGN
RANDOMIZE
Paclitaxel 225 mg/m2 over 3 hours on day 1
Paclitaxel 225 mg/m2 + Carboplatin to AUC 6
Every 3 weeks for up to 6 cycles
IIIB/IV
PS 0-1/2
Age / 70
Lilenbaum, ASCO 2002
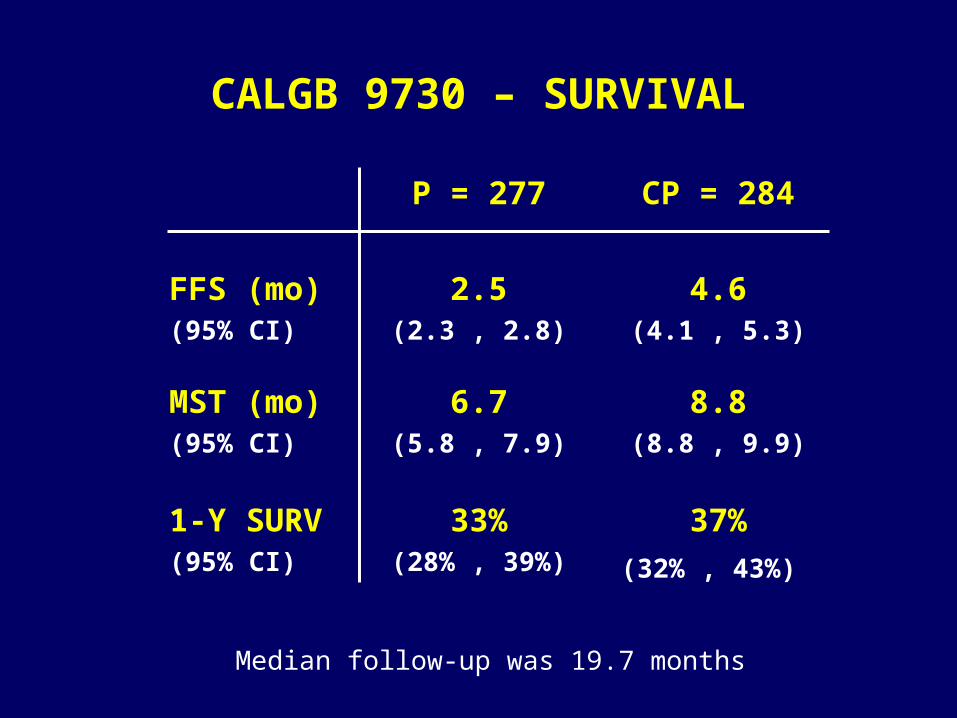
CALGB 9730 – SURVIVAL
P = 277 CP = 284
FFS (mo)(95% CI)
2.5(2.3 , 2.8)
4.6(4.1 , 5.3)
MST (mo)(95% CI)
6.7(5.8 , 7.9)
8.8(8.8 , 9.9)
1-Y SURV(95% CI)
33%(28% , 39%)
37%
(32% , 43%)
Median follow-up was 19.7 months

CALGB 9730 – OVERALL SURVIVAL
0 10 20 30 40
Months
0.0
0.2
0.4
0.6
0.8
1.0
Pro
ba
bil
ity
PaclitaxelPaclitaxel and Carboplatin
Log-rank = 0.2022
Wilcoxon = 0.0125

Gemcitabine/Carboplatin versus MIC
Gemcitabine 1200 mg/m2d 1, 8
Carboplatin AUC = 5 d 1 q.21 days
Mitomycin 6 mg/m2
Ifosfamide 3 g/m2
Cisplatin 50 mg/m2
Day1 q.21 days
Stage IIIb/IV NSCLCPS 0-3
Rudd, ASCO 2002:A1164

LLCG: GC vs MIP in Advanced NSCLCSurvival
0 3 6 9 12 15 18 21 24 27 30 33 36
0
.2
.4
.6
.8
1
GC
MIP
Pro
po
rtio
n S
urv
ivin
g P
ts.
Med 1-Y
GC 10.2m 38%MIP 6 .9m 28%
Months

What are the options for 1st line therapy?
• Patients with advanced NSCLC and good PS should be treated with a platinum-based doublet.
• Platinum-based doublets are better than an old single agent (Cis) and a new single agent (Paclit)
• All platinum-based doublets have comparable efficacy, but vary in cost and toxicity
• Three-drug regimens are more toxic and no better than doublets
• The preferred platinum analog remains controversial
CISPLATIN
CARBOPLATIN
PACLITAXELDOCETAXEL
VINORELBINEGEMCITABINE
+

QUESTIONS FOR DISCUSSION
• What are the options for 1st line therapy?
• What is the optimal management of the elderly and the PS 2 patients?
• What is the role of the non-platinum regimens?
• What is the role of the molecular targeted agents in 1st line therapy?
Non-Platinum Regimens
• Deliver comparable survival with less toxicity better therapeutic index
• Represent alternative regimens to patients who are not optimal candidates for platinum-based therapy

Non-Platinum, Taxane-Based Doublets
• Paclitaxel + gemcitabine• Docetaxel + gemcitabine• Paclitaxel + vinorelbine• Docetaxel + vinorelbine
Non-Platinum, Non-Taxane Doublets
• Vinorelbine + Gemcitabine• Gemcitabine + Irinotecan• Vinorelbine + Ifosfamide

A EORTC Randomized Phase III Trial of Three Chemotherapy Regimens In Advanced Non-Small Cell
Lung Cancer
NSCLC
PS 0-2
Stage IIIB or IV
Paclitaxel 175 mg/m2 d 1
Cisplatin 80 mg/m2 d 1
every 21 days
Gemcitabine 1250 mg/m2 d 1, 8
Cisplatin 80 mg/m2 d 1
every 21 days
Gemcitabine 1250 mg/m2 d 1, 8
Paclitaxel 175 mg/m2 d 1
every 21 days
Van Meerbeeck et al, Proc Am Soc Clin Oncol, 20: #1228, 2001
RANDOMIZED
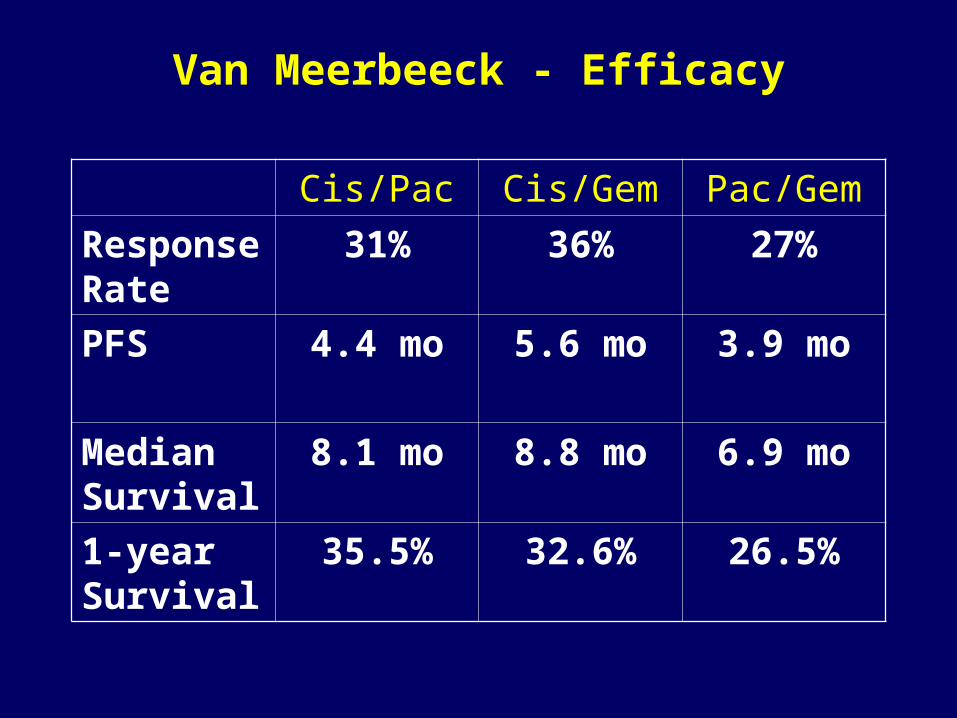
Van Meerbeeck - Efficacy
Cis/Pac Cis/Gem Pac/Gem
Response Rate
31% 36% 27%
PFS 4.4 mo 5.6 mo 3.9 mo
Median Survival
8.1 mo 8.8 mo 6.9 mo
1-year Survival
35.5% 32.6% 26.5%

Van Meerbeeck - Toxicity
Toxicity (% of pts) Cis/Pac Cis/Gem Pac/Gem
Gr. 3/4 ANC 33 43 30
Neutropenic Fever 1 3 2
Gr. 3/4 Thrombocytopenia 1 36 6
Gr. 3/4 Bleeding 1 0 1
Gr. 3/4 Anemia 3 11 4
Gr. 3/4 Nausea 8 13 6
Gr. 3/4 Vomiting 8 13 5
Gr. 3/4 Sensory Neurotoxicity
3 2 1
Gr. 3/4 Motor Neuropathy 3 1 3
Gr. 3/4 Lethargy 9 11 11
Gr. 3/4 Dyspnea 8 10 12
Toxic deaths 3 1 4

GEMVIN – Study designGEMVIN – Study design
RANDOM
Cisplatin 80 mg/ /m², d 1 Vinorelbine 30 mg/m², d 1&8
or (at random)
Cisplatin 80 mg/ /m², d 1 Gemcitabine 1200 mg/m², d 1&8
Gemcitabine 1000 mg/m², d 1&8
Vinorelbine 25 mg/m², dd 1&8
Every 3 weeks, for a maximum of 6 cyclesGridelli, ASCO 2002
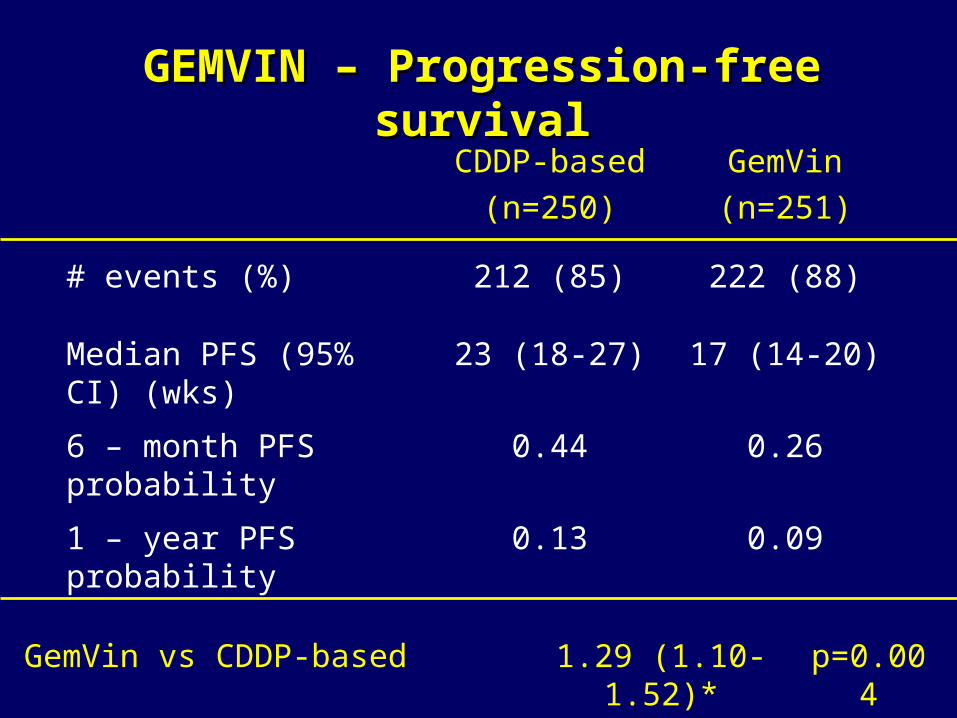
GEMVIN – Progression-free survivalGEMVIN – Progression-free survival
CDDP-based
(n=250)
GemVin
(n=251)
# events (%) 212 (85) 222 (88)
Median PFS (95% CI) (wks)
23 (18-27) 17 (14-20)
6 – month PFS probability
0.44 0.26
1 – year PFS probability 0.13 0.09
GemVin vs CDDP-based 1.29 (1.10-1.52)* p=0.004

GEMVIN – Overall survivalGEMVIN – Overall survival
CDDP-bsed
(n=250)
GemVin
(n=251)
# events (%) 175 (70) 180 (72)
Median OAS (95% CI) (wks)
38 (35-45) 32 (30-39)
6 – month OAS probability 0.66 0.62
1 – year OAS probability 0.37 0.31
GemVin vs CDDP-based 1.15 (0.96-1.37)* p=0.08

Phase II Study of Vinorelbine-Gemcitabine vs Paclitaxel-Carboplatin
Stratification • Stage IIIB/IV• PS 0−1/2
RANDOMIZ A T I O N
Vinorelbine 25 mg/m2 days 1, 8Gemcitabine 1,000 mg/m2 days 1, 8
Paclitaxel 200 mg/m2 day1Carboplatin (AUC=6) day 1
Every 3 weeks, for a maximum of 6 Cycles
Primary endpoint:QoL analysis (LCSS)

What is the role of the non-platinum regimens?
• Taxane-based regimens appear to offer comparable efficacy to platinum-based combinations
• Toxicity, however, is not significantly reduced and ca be substantial, especially in patients with less than optimal performance status
• The non-platinum, non-taxane based regimens are less toxic, but questions about equivalent efficacy remain. They are a viable option for patients unable to tolerate platinum-based therapy
QUESTIONS FOR DISCUSSION
• What are the options for 1st line therapy?
• What is the optimal management of the elderly and the PS 2 patients?
• What is the role of the non-platinum regimens?
• What is the role of the molecular targeted agents in 1st line therapy?

Biological Agents for Solid TumorsSignal Transduction/Cell-Cycle
Inhibitors– Farnesyl transferase– Flavopiridol– Retinoids– UCN-101
Gene Therapy– GM-CSF– Wild-type p53– Antisense
– c-myc– PKC
Vaccines– Tumor cells– Peptides– Dendritic cells– Viral vaccines
Angiogenesis Inhibitors
– SU5416/SU6668
– Anti-VEGF antibodies
– Interferon-/– Marimastat
– ZD6474
– LY317615
– TNP-470
– Endostatin/angiostatin
Receptor-Targeted Therapy– Trastuzumab
– Anti-EGFR
– ZD1839
– C225
– OSI-774

Stage III/IV NSCLC N=1029/Trial
*Gemcitabine/cisplatin (trial 14)
*Paclitaxel/carboplatin (trial 17)
Randomize
Chemotherapy * x6 cycles + 250 mg ZD1839
Chemotherapy * x6 cycles + 500 mg ZD1839
Chemotherapy * x6 cycles + Placebo
Continue ZD1839 or placebo until disease progression
Primary endpoint: Survival
ZD1839 Randomized Trials With Chemotherapy in Advanced NSCLC


Bevacizumab (rhuMAb-VEGF) in NSCLC:ECOG4599 Schema
R
A
N
D
O
M
I
Z
E
R
A
N
D
O
M
I
Z
E
Eligibility:
• No prior Rx
• Stage IIIB or IV
• Non-SqCCa
• ECOG PS 0-1
Eligibility:
• No prior Rx
• Stage IIIB or IV
• Non-SqCCa
• ECOG PS 0-1
CBDCA: AUC = 6
Paclitaxel: 200 mg/m2
CBDCA: AUC = 6
Paclitaxel: 200 mg/m2
CBDCA: AUC = 6
Paclitaxel: 200 mg/m2
rhuMAb-VEGF: 15 mg/kg
CBDCA: AUC = 6
Paclitaxel: 200 mg/m2
rhuMAb-VEGF: 15 mg/kg
Upon PD crosssover to Anti-VEGF NOT ALLOWED

The Affinitac Phase III TrialThe Affinitac Phase III Trial
Eligible patientsrandomized to:
Eligible patientsrandomized to:
Restaging for response every 2 cyclesRestaging for response every 2 cycles
Treatment continues up to 6 cycles(more if patient is benefiting)
Treatment continues up to 6 cycles(more if patient is benefiting)
Post-Treatment follow-up•Survival•Tumor progression
Post-Treatment follow-up•Survival•Tumor progression
Day 0: Paclitaxel 175 mg/m2
Carboplatin AUC 6 21-day cycle
Day 0: Paclitaxel 175 mg/m2
Carboplatin AUC 6 21-day cycle
ARM AARM A ARM BARM B
Days 0-14: ISIS 3521, CIVDay 3: Paclitaxel 175mg/m2
Carboplatin AUC 6Days 15-21: Rest
Days 0-14: ISIS 3521, CIVDay 3: Paclitaxel 175mg/m2
Carboplatin AUC 6Days 15-21: Rest
Stratified for: Stage History of CNS Disease
Stratified for: Stage History of CNS Disease
Sample size = 600
What is the role of the molecular targeted agents in 1st line therapy?








![· Web viewTraditional Chinese medicine (TCM) has attained great popularity in the alternative and complementary treatment of advanced NSCLC [8]. Recent studies have indicated that](https://img.pdfslide.net/doc/110x75/5e24122970c7d52248376ed7/web-view-traditional-chinese-medicine-tcm-has-attained-great-popularity-in-the.jpg)