Embed Size (px)
Citation preview
First trimester determination of adverse pregnancy outcome
Prof. Gordon C S Smith, MD, PhD
Department of Obstetrics & Gynaecology,Cambridge University
“In the first half of pregnancy, genetic control is dominant and gives rise to relatively narrow limits of variability of patterns of fetal growth”
Gluckman PD & Liggins GC. In Fetal Physiology and Medicine. 1984.
Early model of human fetal growth
• Genetically programmed early on• Variability greatest in third trimester• Bulk of weight gain in third trimester• Implied a key role for maternal nutrition in
the last third of pregnancy• Led to multiple trials of dietary
supplementation in late pregnancy
Low birth weight anomaly
• Women with poor diet are at increased risk of a low birth weight baby
• Dietary supplementation during the presumed phase of maximum fetal growth has a minimal effect on birth weight, except in conditions of starvation
Susser, Am J Clin Nutr 1991;53:1384-1396
Hypothesis
• The intra-uterine conditions in early pregnancy determine, at least in part, the eventual birth weight
Prediction
• Measurements of fetal growth or placental function in early pregnancy may be predictive of eventual outcome
QMH cohort study
• All women attending for antenatal care at The Queen Mother’s Hospital Glasgow 1985-1995
• Included women had a scan in the first 12 weeks – actual size
• Excluded women who had used oral contraception in last 3 months, irregular or non-28 day menstrual cycle and not certain of date of LMP – expected size
• Study group of 4229
Outcomes studied
• Examined both absolute birth weights, relative weights and gestational age
• Low birth weight (<2500g)• Low birth weight at term (<2500g at or after 37
weeks gestation)• Birth weight <5th percentile for gestational age• Preterm birth
– Extreme (24-32 weeks)– Moderate (33-36 weeks)
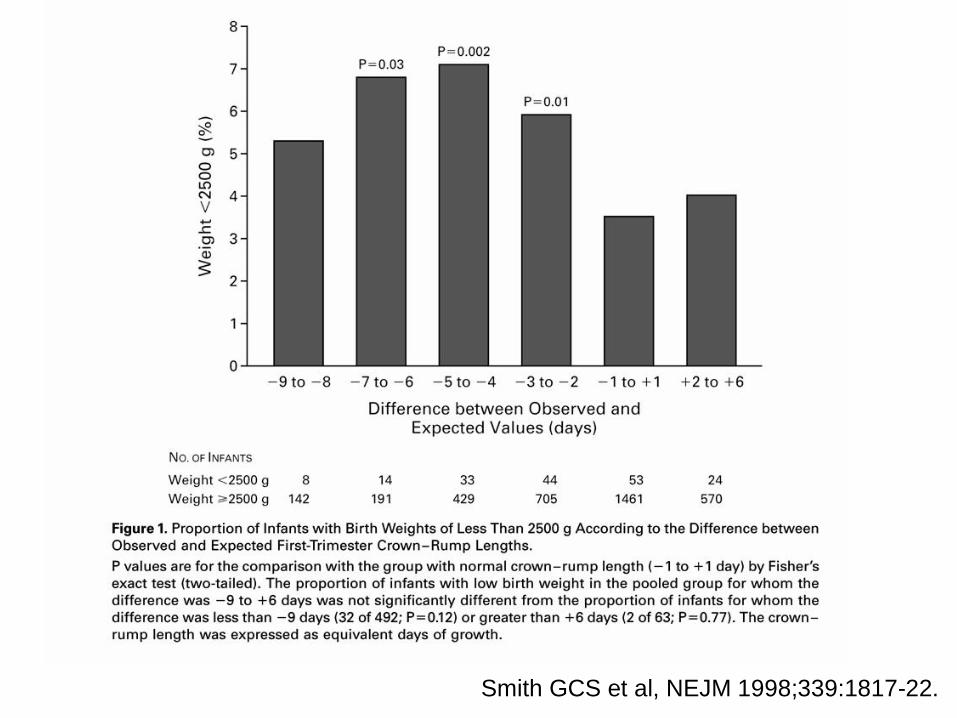
Smith GCS et al, NEJM 1998;339:1817-22.
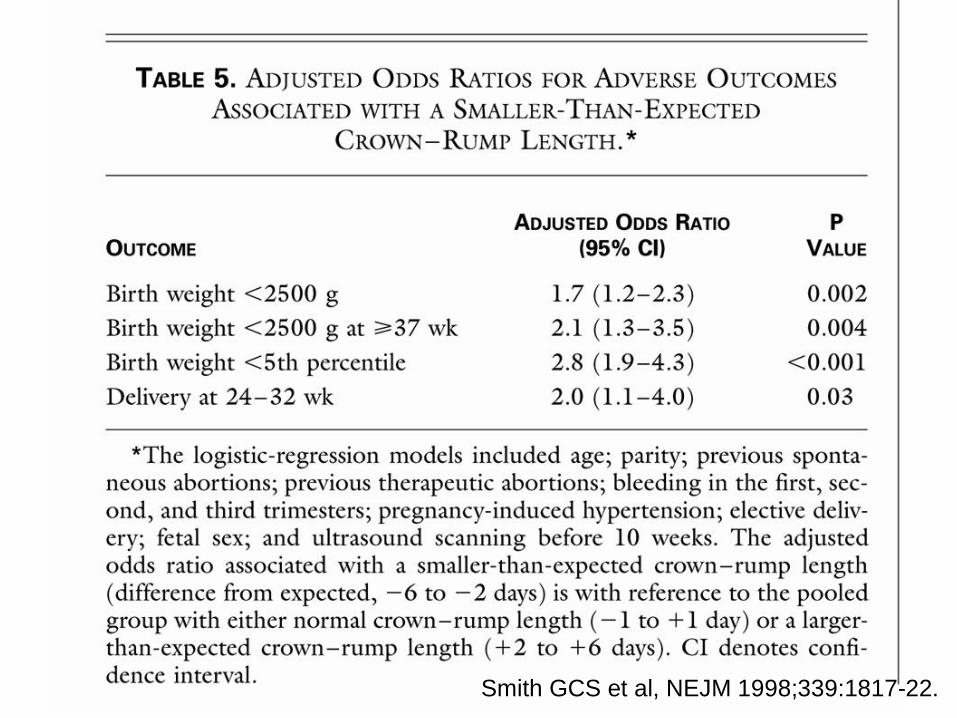
Smith GCS et al, NEJM 1998;339:1817-22.
Interpretation of results
• Poor growth of the fetus in the first trimester associated with increased risk of adverse outcome
• Could also indicate over-estimation of the age of the fetus– i.e. ovulation occurred later than assumed– Unlikely given restriction of women to those
with a regular 28 day cycle
Alternative hypothesis
• Could be due to delayed ovulation• Prolonged menstruation to conception
interval associated with adverse outcome• Based on second trimester US
measurements• Expected size of fetus based on LMP
alone, no information on cycle duration, certainty of recall or hormonal contraception
Gardosi & Francis, BJOG. 2000;107:228-37
Follow-up study
• Data from FASTER trial• Large scale, multi-center, prospective
cohort study of Down syndrome screening• >30,000 women, 976 eligible women
conceived using assisted reproductive technology method – known date of conception with CRL measurement
• Repeated analysis and replicated result
Bukowski, et al for FASTER consortium, Unpublished data
Smith GCS et al, NEJM 1998;339:1817-22.
Predictions from hypothesis
• Trophoblast function in the first trimester of pregnancy will differ comparing babies ultimately born of low birth weight with those of normal birth weight
• Potential for testing the hypothesis as maternal blood contains many trophoblast derived proteins which are minimally produced by other maternal tissues
CUBS Study
• Non-interventional, prospective cohort study designed to evaluate predictors of Down’s syndrome
• Measured PAPP-A and free subunit of human chorionic gonadotrophin at 10-14 weeks using the Kryptor immunoassay analyzer
• Total cohort of approximately 13,000 women• Study group of 8839 women with outcome data
Aims of analysis
• To relate risk of subsequent adverse obstetric outcomes to levels of PAPP-A and FhCG at 10-14 weeks
Methods
• PAPP-A and FhCG expressed as multiples of median (MOM) for gestation
• MOMs adjusted for maternal weight and smoking
• Outcomes related to deciles of PAPP-A and FhCG to establish trend
• Strength of association between lowest 5th
percentile and adverse outcomes
Statistics
• Outcome across deciles of PAPP-A and FhCG tested by chi squared test for trend
• Univariate and multivariate analysis of lowest 5th percentile by logistic regression
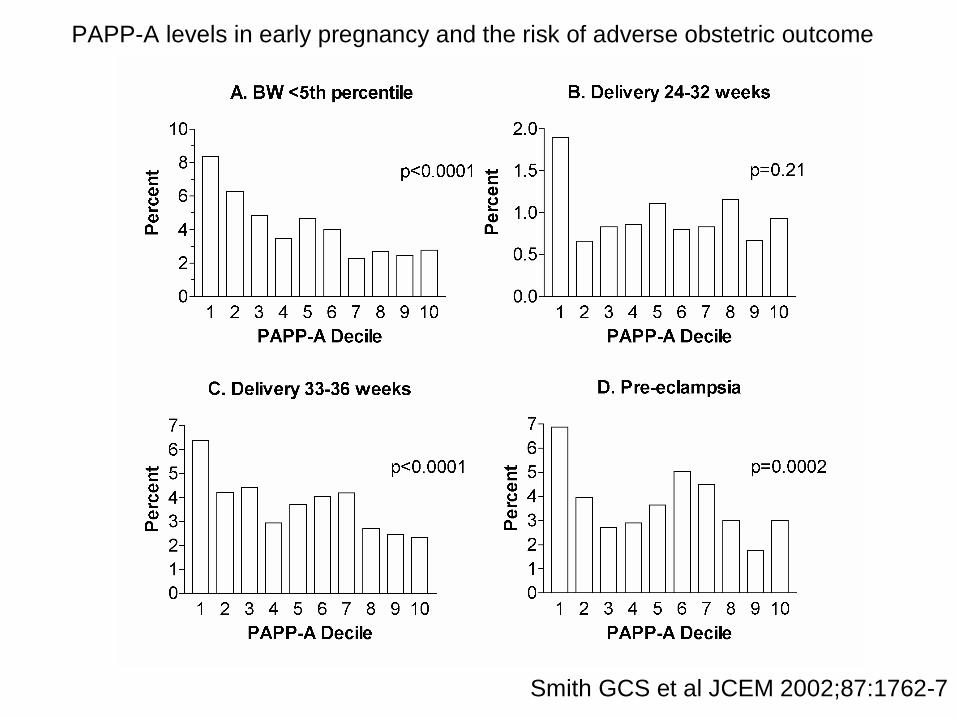
Smith GCS et al JCEM 2002;87:1762-7
PAPP-A levels in early pregnancy and the risk of adverse obstetric outcome
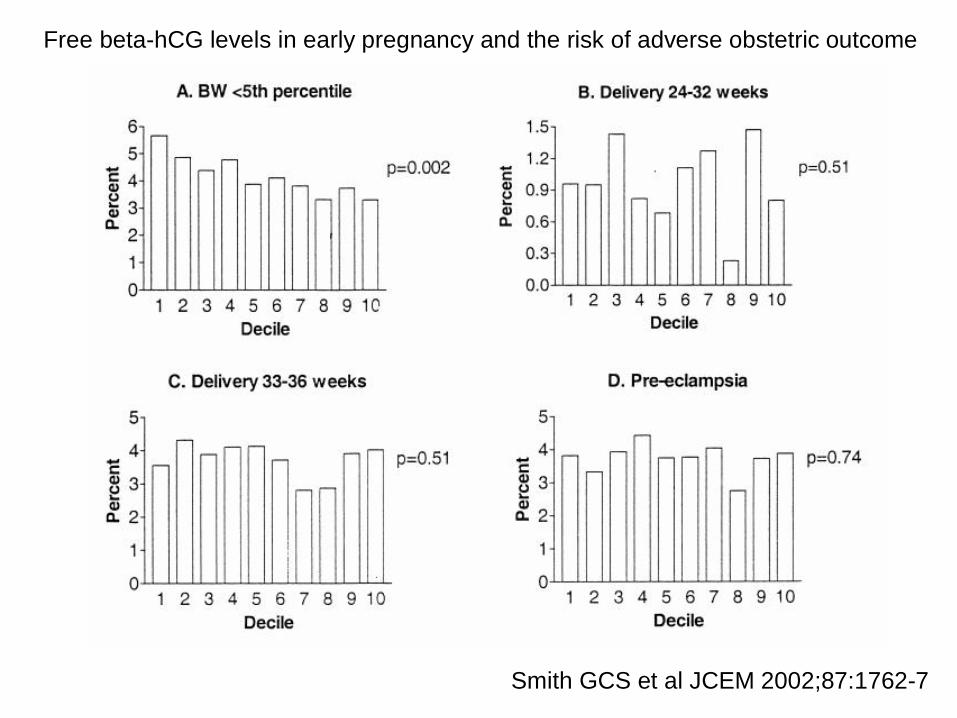
Free beta-hCG levels in early pregnancy and the risk of adverse obstetric outcome
Smith GCS et al JCEM 2002;87:1762-7
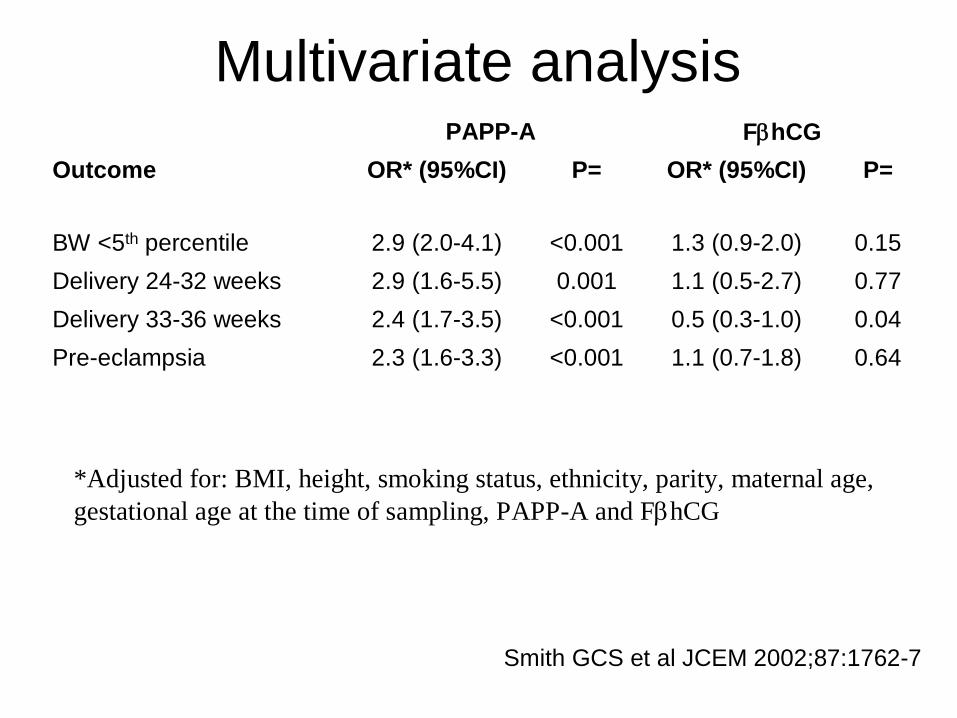
Multivariate analysis
0.641.1 (0.7-1.8)<0.0012.3 (1.6-3.3)Pre-eclampsia0.040.5 (0.3-1.0)<0.0012.4 (1.7-3.5)Delivery 33-36 weeks0.771.1 (0.5-2.7)0.0012.9 (1.6-5.5)Delivery 24-32 weeks0.151.3 (0.9-2.0)<0.0012.9 (2.0-4.1)BW <5th percentile
P=OR* (95%CI)P=OR* (95%CI)OutcomeFhCGPAPP-A
*Adjusted for: BMI, height, smoking status, ethnicity, parity, maternal age, gestational age at the time of sampling, PAPP-A and FhCG
Smith GCS et al JCEM 2002;87:1762-7
Summary of results
• No independent predictive effect of FhCG• PAPP-A associated with all adverse
outcomes• FhCG was significantly associated with
some outcomes but not independently of PAPP-A
• Different patterns of association between PAPP-A and different outcomes
PAPP-A and normal pregnancy
• Further analysis of cases where sampling wholly within first trimester
• Excluded all complicated pregnancies and confined analysis to term births
• Regression analysis (linear, logistic and proportional hazards) to determine associations between absolute birth weight, low birth weight and onset of labour
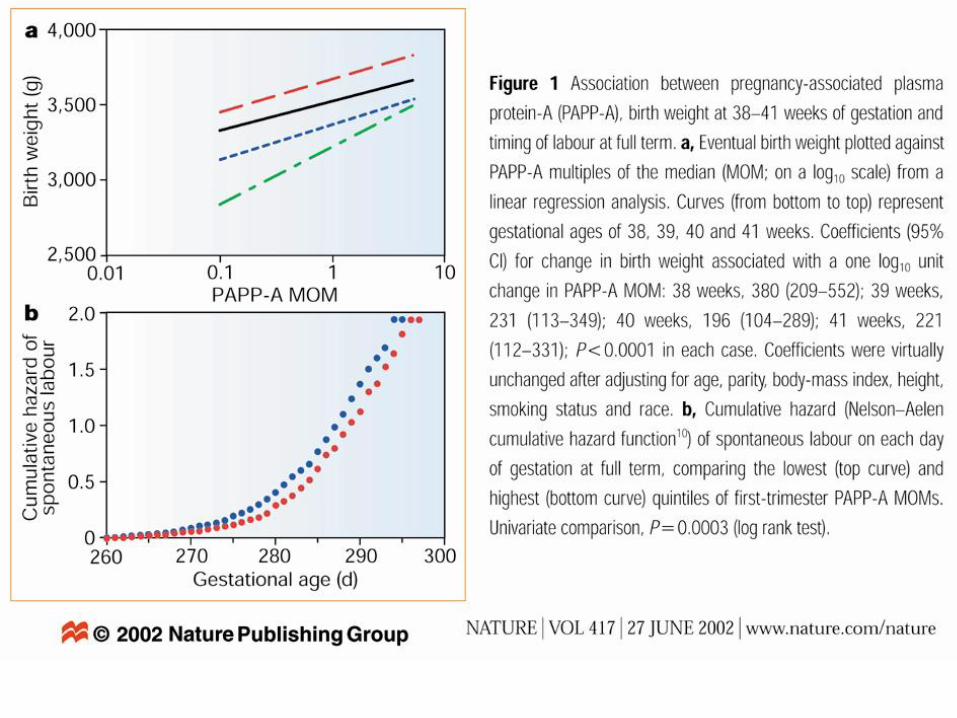
Risk of low birth weight at term
• Risk of a low birth weight baby at term explored using PAPP-A as a continuous variable (logistic regression)
• Odds ratio 0.2 (95% CI 0.1-0.6)• Indicates that across the range of PAPP-A
from the 1st - 99th percentile, risk of a low birth weight baby decreases by 80%
Smith GCS et al, Nature 2002; 417:916.
Significance of fetal growth
• Poor fetal growth is a risk factor for antepartum stillbirth
• Poor fetal growth may be predictive of disease in later life
Antepartum stillbirth
• Most common cause of perinatal death• Majority have no direct cause, but are
associated with impaired growth• Associations with second trimester
biophysical measurements– msAFP and uterine artery Doppler
• Postulated may be due to impaired ‘second wave’ of trophoblast invasion
Methods 1• Record linked CUBS study database with
Scottish Morbidity Record 2 (SMR2, national database maternity hospital discharge data) and the Scottish Stillbirth & Infant Death Enquiry (national register of perinatal deaths)
• Limited to women assayed in first 10 weeks post-conception
• Linked database contained first trimester biochemistry and eventual outcome for 7934 singleton births between 24-43 weeks gestation
• Independent ascertainment of exposures and events
Smith GCS et al, JAMA. 2004;292:2249-2254
Methods 2
• PAPP-A and FhCG, expressed as MoMs• Low defined as ≤5th percentile (<0.4 MoM
for PAPP-A)
Smith GCS et al, JAMA. 2004;292:2249-2254
Results 1
• No association between low PAPP-A (≤5th
percentile) and a range of maternal characteristics– Age, marital status, socio-economic
deprivation, ethnicity, smoking, parity, previous abortions, height and BMI (all P>0.05)
Smith GCS et al, JAMA. 2004;292:2249-2254
Smith GCS et al, JAMA. 2004;292:2249-2254
Smith GCS et al, JAMA. 2004;292:2249-2254
Smith GCS et al, JAMA. 2004;292:2249-2254
Summary of results
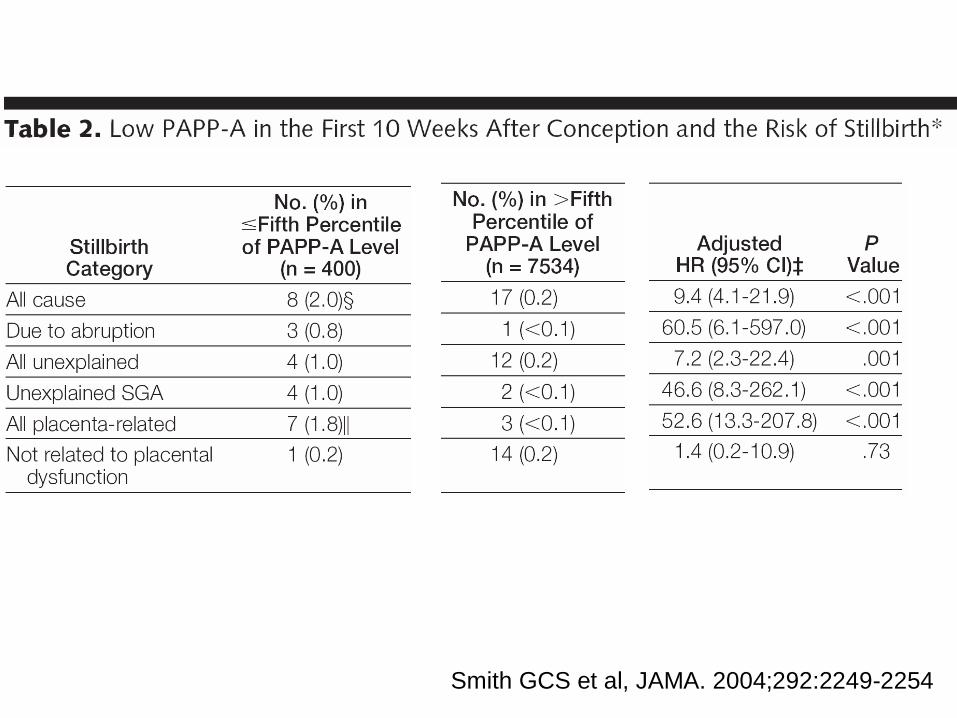
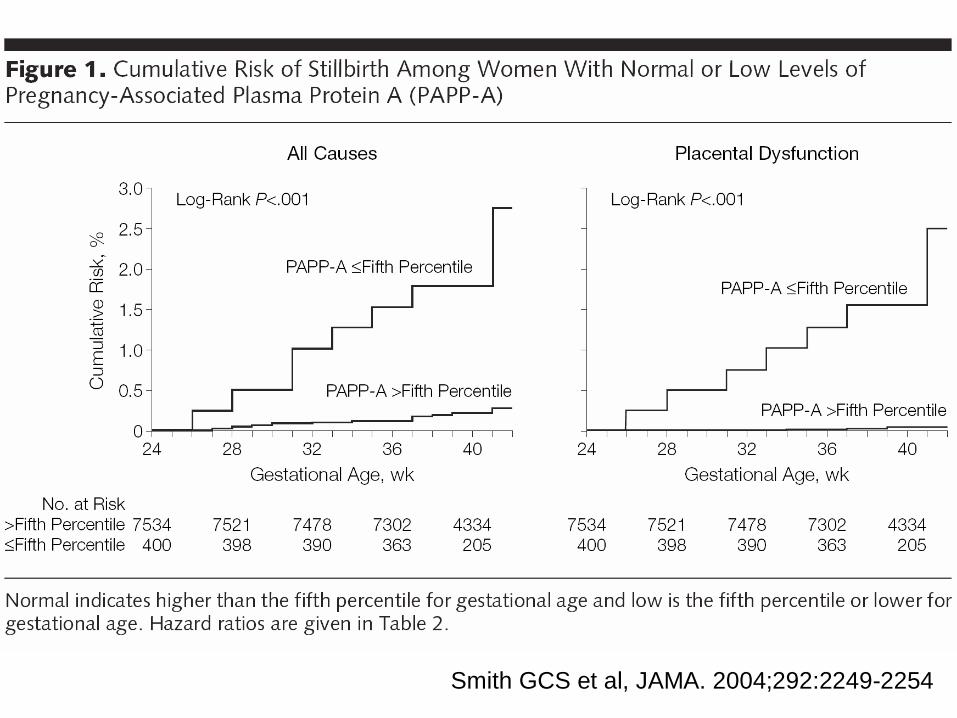
• Very strong relationship between low PAPP-A and subsequent risk of stillbirth
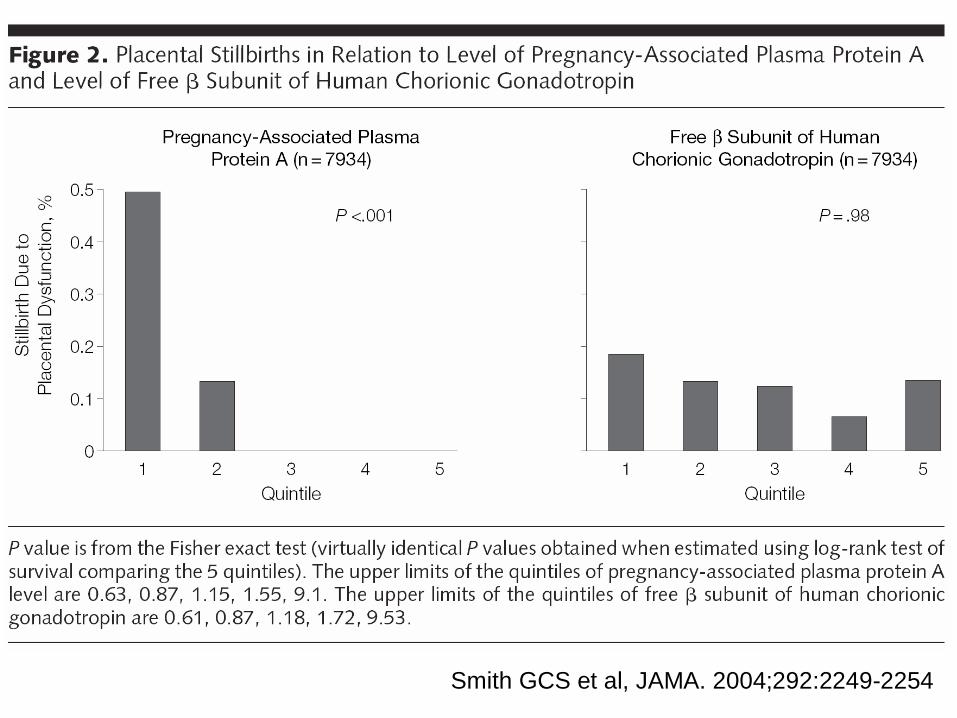
• Association due to stillbirth related to placental dysfunction
• No placental stillbirths in upper 60% of PAPP-A• Association specific
– Not due to maternal confounding– No relationship with FhCG– No relationship with other causes of stillbirth
Smith GCS et al, JAMA. 2004;292:2249-2254
PAPP-A
• Produced in syncytiotrophoblast• PAPP-A has protease activity on IGFBP-4• Low levels of PAPP-A lead to low levels of
IGFBP-4 and likely decrease placental effects of IGF-II which would adversely affect growth
• Role supported by studies in mice: PAPP-A null mutants exhibit severe early onset IUGR (Conover et al, Development 2004;131:1187-1194)
Further studies on 1st trimester trophoblast & obstetric outcome
• Follow-up studies using stored samples from cohort linked to Scottish maternity and perinatal death databases
• Nested-case control study of 1000 complicated pregnancies and 1000 controls
• Measured s-Flt1, PlGF, IGF-1, IGF-2, IGFBP-1, IGFBP-3, Leptin and MMP-9
Relationship between first and second trimester predictors
• Elevated AFP and hCG associated with increased risk of stillbirth
• How does this relate to association with PAPP-A?
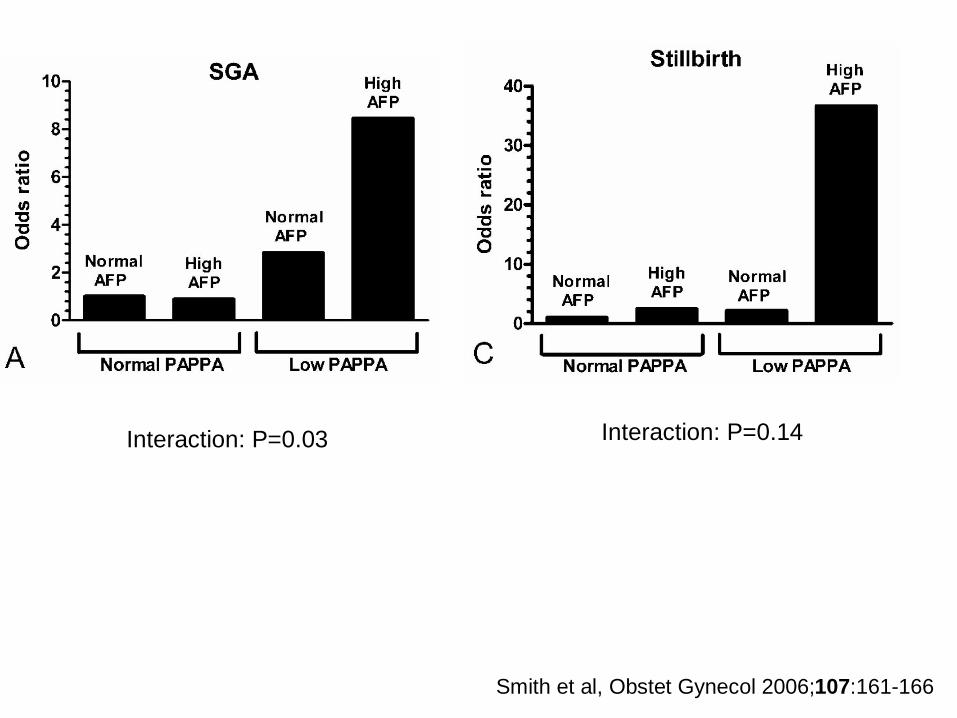
Interaction: P=0.03 Interaction: P=0.14
Smith et al, Obstet Gynecol 2006;107:161-166

Conclusions
• Fetal growth and risk of stillbirth determined in first trimester
• Synergistically predictive with second trimester markers
• Potential for sequential screening for stillbirth risk, comparable to Down’s syndrome screening
Acknowledgements• Dr Jill Pell, Consultant in Public Health, Greater
Glasgow Health Board• Information & Statistics Division of the NHS
Scotland (James Boyd, David Walsh, Richard Dobbie), SMR2 & SMR1 data.
• Dr Jenny Crossley & Dr David Aitken, Department of Medical Genetics, Yorkhill, Glasgow (CUBS study)
• Mr John Fleming & Dr Margaret McNay, Department of Ultrasound, The Queen Mother’s Hospital, Glasgow, Ultrasound database study