Embed Size (px)
Citation preview

Develop. Med. Child Neiirol. 1970,12,758-766
Fisher Syndrome in Childhood William Bell Maurice Van Allen James Blackman
AN acutely acquired neurologic disorder manifesting ophthalmoplegia, ataxia and areflexia was described by Fisher in 1956. The clinical course of the illness, plus the elevation of spinal fluid protein in one case suggested to him that this condition was a variant of the Guillain-Barr~-Strohl (G.B.S.) syndrome. Several subsequent reports have appeared (Smith and Walsh 1957, Neubert 1958, Darcourt and Cossa 1959, Arnould et a/. 1960, Hynes 1961, Lugaresi and Tassinari 1963, Goodwin and Poser 1963, Van Allen and MacQueen 1964, Patel et a/. 1966), although its recognition in children has remained infrequent (Van Allen and MacQueen 1964, Patel et al. 1966). The three cases described here occurred in the pediatric age group and illustrate certain variations in the symptomatology. In Cases 1 and 2, evidence of facial paresis and skeletal muscle weakness co-existed with other manifestations of the illness.
Case Reports Case 1
This 5-year-old boy was admitted to the University Hospitals for evaluation of diplopia, lethargy and leg pain. Because of intractable asthma, he had been taking 2.5 mg of prednisone per day which was prescribed 6 months prior to admission. Fifteen days before admission he experi- enced an upper respiratory infection, at
which time prednisone was discontinued. Thereafter, he had intermittent aching pain in both lower extremities. Six days prior to admission he developed diplopia. lethargy and left internal strabismus. He was hospitalized in his local community where a lumbar puncture was reported to be normal.
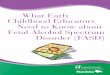
Physical examination revealed a lethar- gic child with a blood pressure of 120/84 mmHg and pulse rate of 80 per minute. There was mild cervical rigidity with pain on forward flexion of the neck. The pupils were dilated and did nct react to light. Ptosis and marked lateral rectus weakness was present bilaterally (Fig. 1). Vertical conjugate gaze was intact, and optic discs were normal. Mild bilateral facial paresis was noted. No sensory abnormalities were found. Stretch reflexes were dimini- shed in all four limbs. There was no Babinski sign. The child walked with a wide-based gait and appeared ataxic on turning. The results of routine laboratory studies are shown in the Table.
Because of lethargy and bilateral sixth nerve paresis, the initial diagnosis was pseudotumor cerebri secondary to steroid withdrawal. Intravenous dexamethasone was given for 24 hours but with no im- provement.
After recovery from an air study, weakness of the neck and both lower extremities appeared. By 8 days after admission, mild improvement of ataxia
Departments of Pediatrics and Neurology, and the Neurosensory Center, University of Iowa, College of Medicine, Iowa City, Iowa 52240, U.S.A.
758

WILLIAM BELL MAURICE VAN ALLEN JAMES BLACKMAN
Fig. 1. (Case 1.) Upper left: bilateral ptosis. Upper right: dilated pupil with absent response to light. Lower frames reveal lateral rectus paralysis bilaterally on attempted horizontal gaze.
and muscle weakness was apparent. Four weeks following hospital admission, ptosis was less marked and ocular move- ments and leg strength were improved. Examination 6 weeks after admission revealed absence of ptosis with continued improvemefit of ocular muscle function, facial paresis and ataxia. The muscle stretch reflexes remained absent. Pupils remained dilated with absence of light rcactions.
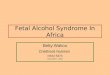
Repeated examination throughout the ensuing year revealed gradual disappear- ance of ataxia and improvement in muscle strength and reflex activity with persistence of an alternating internal strabismus
(Fig. 2). The pupils had returned to a normal size but light reactions remained sluggish.
Case 2* This 12-year-old girl was admitted to
University Hospitals with diplopia, head- ache, external ophthalmoplegia and ataxia beginning 4 days before. She had been in good health until one week previously when she developed a cough and nasal congestion. Bilateral ptosis and diplopia appeared 4 days prior to admission. Two days later, she developed severe frontal
*Previously described by Van Allen and Mac- Queen (1964).
759

DEVELOPMENTAL MEDICINE AND CHILD NEUROLOGY. 1970, 12
TABLE Results of Some Investigations on 3 cases of Fisher Syndrome
Investigation Case 1 Case 2
Urinalysis Hemoglobin (gm/100 ml) White cells (per cu mm) Sedimentation rate (mmihr) BUN (mg/100 ml) Serum calcium (mg/ 100 ml) Serum phosphorus (mg/IOO ml) Blood sugar (mg/IOO ml) Brain scan EEG
Nerve conduction velocities X-ray: Skull
Chest Serologic test for syphilis Brucellosis agglutination test Histoolasmosis
N N (N') 14 13.6
11,000 16,000* (N' 28 12 12
12
9 . 4 4 .2
N
12 12 9.4 4.2
12 N N N
N N N N N N
N Tubeiculin test N Lumbar puncture mm.jwater 90 160 (1 30', 1 802) CSF glucose mg/IOO ml 60 62 (54%) CSF protein mg/100 ml 222 125 ( I S 1 , 130') CSF culture N Pneumoencephalogram N
__ Case 3
N 12
8,400 17
___
some excess post. slow activity
N N N
N 50 31
* = On day of admission; = investigations at previous admission; = 16 days after admission.
headaches and on the following day, vomiting occurred along with dizziness, stiffness of the neck, and a staggering gait.
Previous Episode: At age 6 years, she had been admitted to University Hospitals for diplopia and external ophthalmoplegia. A mild upper respiratory infection had preceded the development of diplopia by 2 weeks. Physical examination at that time revealed slight ptosis of the left lid with only minimal horizontal ocular motion and essentially no vertical motion of either eye. The pupils were equal but reacted sluggishly to light. Bell's pheno- menon was present and the fundi were normal, as was the remainder of the neurological examination. A Prostigmin test was performed without improvement of eye muscle function, and there was no change with hypnosis. See Table for results of other tests.
Ophthalmoplegia disappeared one month later.
Present Episode: Physical examination on the second admission at age 12 years included blood pressure of 120/80 mmHg and pulse rate 90 per minute. The tympanic membranes were reddened and the nasal mucosa congested. The general examination was otherwise unremarkable. Mild bilateral ptosis was present but the lids could be elevated by voluntary effort. There was complete external ophthalmo- plegia (Fig. 3). Bell's phenomenon was absent. Opticokinetic nystagmus could not be induced. The pupils were slightly irregular and reacted only minimally to light. The fundi were normal. There was bilateral facial paresis but function of the other cranial nerves was intact. Moderate weakness of the proximal musculature of the upper and lower extremities was noted. Sensory examination was normal and the tendon stretch reflexes were absent. There was no Babinski sign. The Romberg test was positive, and the gait was broad-based
760

WILLIAM BELL MAURICE VAN ALLEN JAMES BLACKMAN
Fig. 2. (Case I .) Findings 7 months after onset of illness. Ptosis now absent. Upper left frame shows persistent left internal strabismus but extraocular movements otherwise virtually normal.
and ataxic. The finger-to-nose and heel-to- after admission showed improvement of shin tests were dyssynergic on both sides. the facial weakness but no change in the The results of routine tests on the day of ophthalmoplegia or ptosis. Slight weak- admission are shown in the Table. ness in elevation of the shoulders was
Electromyogram of the lateral and noted, and the gait remained somewhat medial recti of the right eye revealed only ataxic. She could now squat and rise and short, low-voltage bursts appearing at was able to walk on heels and toes. long intervals. Electromyography of Lumbar puncture was repeated and the facial musculature revealed fibrillation results are shown in the Table. potentials. Examination 9 weeks after discharge
revealed marked improvement of extra- Examination prior to discharge I6 days
76 1

DEVELOPMENTAL MEDICINE AND CHILD NEUROLOGY. 1970, 12
ocular muscle function. Vertical gaze was normal, as was horizontal gaze to the right. Gaze to the left showed persistent left lateral rectus paresis. Her ataxia was less and facial paresis had improved. Three months after discharge, extraocular muscle function was normal (Fig. 4). Cerebrospinal fluid was normal 5 months after discharge. She was entirely well except for diminished stretch reflexes 2 years after the onset of the illness.
Case 3* This 7-year-old girl was admitted to
University Hospitals for evaluation of diplopia, ataxia and ophthalmoplegia of 4 days duration. She had been in good health until 9 days prior to admission when she developed nausea and recurrent vomiting. Improvement followed but on awakening 4 days before admission, she noted diplopia and later developed headache and abdominal pain. She became progressively more irritable, drowsy and unsteady. Her past medical and family histories were unrevealing.
On admission, the child was irritable and drowsy. Blood pressure was 104/60 mmHg. There was mild ptosis of the left upper lid with marked limitation of all eye movements. The pupils were dilated and nonreactive to light. The rest of the cranial nerves were intact. Muscle strength was normal in all limbs and sensation was intact. The gait was ataxic and the stretch reflexes were diminished. The plantar responses were flexion bi- laterally. The results of routine tests are shown in the Table.
On examination 6 weeks after ad- mission, marked improvement was noted with only slight impairment of conjugate gaze. Ataxia had disappeared and the pupillary light reactions were normal, but
*Previously described by Van Allen and Mac- Queen (1964).
she remained areflexic. Three years after the illness, her recovery was found to be complete.
Discussion In 2 of our 3 cases the syndrome
developed following an upper respiratory infection. All 3 recovered from their illness, although in the first case mild extraocular muscle weakness persisted. Two of the cases had significant limb weakness in a pattern consistent with that seen in the Guillain-Barr~-Strohl syn- drome. Case 2 described above is unique in that the syndrome was recurrent, at least in part. Her first episode occurred 54 years before the second, and consisted primarily of external ophthalmoplegia following a respiratory infection.
Lethargy and irritability occurred in 2 of the 3 patients and was not explained by fever or identified metabolic abnormalities. Lethargy in these cases in the initial stages of the illness suggests at least some component of central nervous system involvement, possibly brain stem in loca- tion in view of the other associated signs. Drowsiness was described by Fisher (1956) early in the course of the illness in his Case 2. He also suggested that the occurrence of total external ophthalmo- piegia with relative sparing of the levator palpebrae function (as in our Cases 2 and 3) provoked suspicion of dysfunction within the central nervous system. Marked ataxia in the absence of weakness or proprioceptive sensory loss has also been used as evidence of brain stem or cere- bellar dysfunction. Pathologic confirmation of the site of disease in this syndrome has not been available but clinical evidence in a number of cases described is suggestive of dysfunction within the central nervous system, perhaps in conjunction with involvement peripherally.
Previously described cases in childhood with findings similar to ours include Case
762

WILLIAM BELL MAURICE V A N ALLEN JAMES BLACKMAN
Fig. 3. (Case 2.) Central insert shows gaze directly ahead with ptosis volun- tarily overcome. Nearly complete paraly- sis of ocular gaze in all directions. White dot indicates direction ofattempted gaze.
Fig. 4. (Case 2) 34 months after onset, extraocular muscle function and facial muscle strength appear normal.
2 of Pate1 et al. (1966). This 6-year-old and Barnes (1965) was a 5-year-old boy girl exhibited trunkal and limb ataxia, who developed complete external ophthal- nearly complete external ophthalmoplegia moplegia, ataxia, areflexia, but without and weakness of the lower extremities. limb weakness. Within five weeks of onset, Complete recovery occurred by two recovery was complete except for persisting months after the onset except for dimini- areflexia. Both of these children had shed stretch reflexes. Case I of Munsat normal pupillary findings, in contrast to
163

DEVELOPMENTAL MEDICINE AND CHILD NEUROLOGY. 1970, 12
two of our cases, in whom the pupils were abnormally dilated and light reactions were absent. In the third of our cases, the pupillary response to light was present but diminished. Pupillary abnormalities also were noted in the adult patient described by Hynes (1961), and in the cases of Fisher (1956). Thus, it is evident that internal ophthalmoplegia may accom- pany extraocular muscle paresis or paraly- sis in this disorder.
There seems little doubt that a disorder exists which is manifested by ophthalmo- plegia, ataxia, areflexia, at times with limb weakness and bilateral facial paresis, often with an elevated spinal fluid protein, and with a benign course. The cause is unestablished and its relationship to the G.B.S. syndrome remains debatable. Mun- sat and Barnes (1965) discussed the possible widespread neurologic involve- ment compatible with a diagnosis of G.B.S. syndrome and believed that another eponym for those cases with cranial nerve involvement and ataxia is unwar- ranted.
The obvious problem in relating the Fisher syndrome to the G.B.S. syndrome is that the pathogenesis of the latter is unknown and even its definition remains a matter of dispute and debate. Some have preferred to restrict the term ‘Guillain- Barr6 syndrome’ to those cases with acute or subacute onset of radicular or peripheral and cranial nerve involvement in which the etiology remains undetermined. Others have accepted evidence of CNS involve- ment as compatible with this diagnosis. A ‘cerebral’ form has been described (Baker 1943) as well as an ‘ataxic’ form with degeneration of Clarke’s columns and of Flechsig’s middle root zone in the spinal cord (Richter 1962).
The addition of fcrms, types and varia- ions of the G.B.S. syndrome has created confusion as to where limits should be in regard to criteria acceptable for this
diagnosis. Perhaps the term would have more meaning were it restricted to cases with peripheral nervous system involve- ment of undetermined etiology, usually with an elevated spinal fluid protein and generally with a favorable outcome. This appears to have been the intention of Guillain, Bard and Strohl (1916) in their original paper. That retrograde degenera- tive anterior horn cell changes might occur as described by Haymaker and Kernohan (1949) would not be surprising. The diag- nostic criteria outlined by Marshall (1963) are compatible with those presented here. He suggested that an effort be made to ascertain the cause in every case with acute polyneuropathy. Cases due to infectious mononucleosis or porphyria should be designated as such. Those following a clearly recognized infectious illness such as measles or chicken pox should be labelled as post-infectious polyneuro- pathy. For the remaining cases of acute polyneuropathy in which the cause cannot be found, ‘the time-honoured term Landry- Guillain-Barre syndrome will serve well, and avoids the assumption of knowledge we do not possess.’
In view of the limited number of ways that neural tissue may respond to adverse stimuli, it is probable that a number of factors; infectious, toxic or allergic, may result in the same clinical picture. That an agent, such as a virus, might result in a syndrome with radicular dysfunction in one person and produce spinal cord and radicular signs in another is also quite reasonable. As the inciting agents are commonly not identified, the former might best be identified as one with G.B.S. syndrome and the latter as having myelo-radiculitis of undetermined origin. The eponym of ‘Fisher’ would thus seem justified for the syndrome under discus- sion, since the cause remains unestablished and the support for CNS dysfunction is rather strong. While the agents that cause
764

WILLIAM BELL MAURICE V A N ALLEN JAMES BLACKMAN
this syndrome and the G.B.S. syndrome may be the same, the recognition of the two as nosologically different would seem reasonable. Although the two disorders may represent a continuum of neurologic disease due to common causative factors, retaining eponyms in the context of their original description is advisable to avoid confusion of meaning.
That several neurologic disorders may be suggested by the constellation of symptoms and signs comprising this syndrome is of the greatest importance. In our Case 1, the history of steroid intake plus bilateral sixth nerve paresis and lethargy raised the possibility of pseudo- tumor cerebri. The absence of papilledema and the normal spinal fluid pressure removed this diagnosis from further consideration. Brain stem glioma was also entertained, despite the absence of hyperreflexia. Myasthenia gravis may be suspected because of ptosis and ophthal-
moplegia. A cavernous sinus inflammatory process referred to as ‘painful ophthalmo- plegia’ (Hunt et al. 1961) shares certain features in common with the Fisher syndrome. Metastatic disease to the midbrain (Stevenson and Hoyt 1963) may also result in signs closely analogous to those characteristic of the Fisher syndrome. Ophthalmoplegia, ataxia and peripheral neuropathy occur in Wernicke’s encepha- lopathy and thus bears considerable similarity to the disorder under discussion. Mental changes tend to be more profound and the etiologic factors associated with the production of Wernicke’s syndrome are uncommon in children. Further con- siderations in differential diagnosis include diphtheritic neuritis, botulism and brain stem vascular insufficiency, all rare disorders in childhood, however.
Acknowledgernenr: The Neurosensory Center is supported by grant No. NS 03354 of the National Institute of Neurological Diseases and Stroke.
SUMMARY Three children are described with acute onset of ophthalmoplegia, ataxia and areflexia.
These cases closely resemble those described by Fisher and subsequently referred to as the Fisher syndrome. The eventual outcome was favorable with almost complete recovery in all three cases.
While the authors recognize this disorder and the Guillain-Bard syndrome as related conditions in a spectrum of neurologic disease, the rationale for maintaining them as nosologically separate is presented. There appears to be reasonably firm evidence for central nervous system involvement in those with the Fisher syndrome. The authors would prefer to restrict the term ‘Guillain-Barrt’ to those with peripheral nervous system disease from the clinical standpoint. The problems of differential diagnosis in this syndrome are reviewed.
RESUMG Les auteurs decrivent trois enfants ayant prdsentks une ophtalmoplegie, une ataxie et une
areflexie B debut brutal. Ces cas ressemblent a ceux qui ont CtC dCcrits par Fisher et dtnommes par la suite Syndrome de Fisher. L’tvolution a Ctt favorable avec recuperation pratiquement compltte dans les trois cas.
Les auteurs reconnaissent que ce trouble et le syndrome de ‘Guillain-BarrC-Strohl’ doivent &tre rapprochts au sein des maladies neurologiques mais ils indiquent les raisons qui leur paraissent justifier une separation nosologique. I1 semble en effet qu’il y a une participation de l’atteinte du systtme nerveux central dans le syndrome de Fisher.
Les auteurs prtfereraient restreindre le terme de syndrome de ‘Guillain-BarrC-Strohl’ aux troubles cliniques limit& au territoire du systkme nerveux pkriphtrique. Les problhmes du diagnostic differentiel de ce syndrome sont revus.
765

DEVELOPMENTAL MEDICINE AND CHILD NEUROLOGY. 1970, 12
ZUSAMMENFASSUNG Es werden drei Kinder mit akutem Beginn einer Ophthalmoplegie, Ataxie und Areflexie
beschrieben. Diese Falle gleichen den von Fisher beschriebenen und in der Folge als Fisher-Syndrom erwahnten sehr genau. Der Verlauf war letztlich gutartig, mit einer fast volligen Genesung in allen drei Fallen.
Die Autoren erkennen die nahe Verwandtschaft dieser Erkrankung mit dem Guillain- Barrt-Strohl-Syndrom im Hinblick auf die neurologische Stdrung, legen jedoch die Griinde dar, die fur eine nosologische Trennung sprechen. Es scheint ziemlich klare Anhaltspunkte zu geben, die fur eine Beteiligung des Zentralen Nervensystems beim Fisher-Syndrom sprechen.
Die Autoren neigen dam, die Bezeichnung ‘Guillain-BarrC-Strohl-Syndrom’ auf Falle rnit klinischer Erkrankung des peripheren Nervensystems zu beschranken. Die Probleme der Differentialdiagnose bei diesem Syndrom werden er8rtert.
REFERENCES Arnould, G.,Tridon, P., Schmitt, J., Guerci, 0. (1960) ‘Polyradiculoneurite aYgue curable a fornie ophtalmo-
plkgique.’ Rev. Oto-neuro-ophtal., 32,425. Baker, A. B. (1943) ‘Guillain-Barre’s disease (encephalo-myelo-radiculitis).’ J . Lancet, 63, 384. Darcourt, G., Cossa, P. (1959) ‘Syndrome de Guillain-Bard avec ophtalmoplegie extrinsique bilaterale et
ataxie algue.’ Rev. Oto-neuro-ophtal., 31,416. Fisher, M. (1956) ‘An unusual variant of acute idiopathic polyneuritis (syndrome of ophthalmoplegia, ataxia
and areflexia).’ New England J . Med., 255, 57. Goodwin, R. F., Poser, C. M. (1963) ‘Ophthalmoplegia, ataxia and areflexia (Fisher’s syndrome).’ J. Amer.
med. Ass., 186,258. Guillain, G., Barre, J.-A., Strohl, A. (1916) ‘Sur un syndrome de radiculonevrite avec hyperalbuminose du
liquide ctphalo-rachidien sans rbction cellulaires remarques sur les caracteres cliniques et graphiques des reflexes tendineux.’ Bull. SOC. Hbp. Paris, 40, 1462.
Haymaker, W., Kernohan, J. W. (1949) ‘Landry-Guillain-BarrC syndrome: clinico-pathologic report of 50 fatal cases and critique of literature.’ Medicine (Balt.), 28, 59.
Hunt, W. E., Meagher, J. N., LeFever, H. E., Zeman, W. (1961) ‘Painful ophthalmoplegia.’ Neuro1og.v (Minneap.), 11,56.
Hynes, E. A. (1961) ‘Syndrome of Fisher. Ophthalmoplegia, ataxia and areflexia.’ Amer. J. Ophthal., 51,701. Lugaresi, E., Tassinari, C. A. (1963) ‘La sindrome di Fisher: oftalmoplegia, atassia, areflessia.’ Riv. Oto-
neuro-ofral., 38, 423. Marshall, J. (1963) ‘The Landry-GuillainBarre syndrome.’ Brain, 86, 55. Munsat, T. L., Barnes, J. E. (1965) ‘Relation of multiple cranial nerve dysfunction to the Guillain-Barre
syndrome.’ J. Neurol. Neurosurg. Psychiat., 28, 115. Neubert, F. R. (1958) ‘Complete ophthalmoplegia in acute toxic polyneuritis.’ Brit. J . Ophthal.. 42, 632. Patel, A., Pearce, L., Hairston, R. (1966) ’Miller-Fisher syndrome (variant of Landry-Guillain-Barre-Strohl
syndrome) ophthalmoplegia, ataxia, areflexia.’ Sth. med. J., 59, 171. Richter, R. (1962) ‘The ataxic form of polyradiculoneuritis (Landry-Guillain-Barre syndrome).’J. Neuropath.
exD. Neurol.. 21. 171. Smiih, J. L., Walsh, F. B. (1957) ‘Syndrome of external ophthalmoplegia, ataxia and areflexia (Fisher).’
Stevenson. G. C., Hovt. W. F. (1963) ‘Metastasis to midbrain from mammarv carcinoma. Cause of bilateral Arch. Ophrhal. (Chic.), 58, 109.
ptosis and ophthalmoplegia.’J. Aker. med. Ass., 186, 514. Van Allen, M. W., MacQueen, J. C. (1964) ‘Ophthalmoplegia, ataxia and the syndromeof Landry-Guillain-
Barre: a report of four cases with comment on the ophthalmoplegia.’ Trans. Amer. neurol. Ass., 89,98.
766