Embed Size (px)
Citation preview

DERMATOLOGIC SURGERY
Flammability of topical preparations and surgicaldressings in cutaneous and laser surgery: A controlled
simulation study
Katharine Arefiev, MD,a Melanie Warycha, MD,b Dennis Whiting, PA-C,b and Murad Alam, MD, MSCIb,c,d
Redwood City, California, and Chicago, Illinois
From
of
gy
ic
Supp
U
Conf
Acce
700
Background: Surgical fires are a rare, but serious complication of dermatologic procedures involvingelectrosurgical and laser devices. Given the lack of data regarding basic fire safety principles, manydermatologists remain unaware of this potential risk.
Objective: We evaluated the flammability of topical preparations and surgical drapes commonlyencountered in the immediate operative field during cutaneous and laser surgery.
Methods: Surgical dressings, drapes, and pork belly skin were examined for fire risk upon exposure toisopropyl alcohol, chlorhexidine gluconate, and aluminum chloride under dry, saturated, and dampconditions. Both electrosurgery and a carbon-dioxide laser were used as ignition sources.
Results: At least some char was observed in 86 of 126 simulated conditions (68%). Flames occurred in 2test conditions: dry underpad drapes and cotton balls exposed to the carbon-dioxide laser. In general,drapes and dressings dampened or saturated with isopropyl alcohol failed to ignite with electrofulgurationor electrodessication, although sparks and moderate char developed on pork belly skin and the underpaddrape. Materials dampened or saturated with chlorhexidine gluconate, which contains isopropyl alcohol,generated less smoke and char compared with materials exposed to aluminum chloride, which does notcontain alcohol.
Limitations: Future studies may assess the flammability of materials in the setting of oxygensupplementation.
Conclusion: In common cutaneous surgical environments, electrosurgery or ablative laser may lead tochar and rarely to fire. Char may be seen in up to two thirds of simulated conditions, and in a minuteproportion of conditions, fire is observed. ( J Am Acad Dermatol 2012;67:700-5.)
Key words: carbon-dioxide laser; electrosurgery; fire; patient safety; skin preparation; surgical fires.
Although often overlooked, surgical fires are apotential hazard of both cutaneous and lasersurgery. According to the Emergency Care
Research Institute, approximately 50-100 surgicalfires occur in the United States each year, themajorityof which involve electrosurgical or laser devices.1
Dermatologists routinely use electrodesiccation, yetmay be unfamiliar with the inherent flammability of
the Department of Dermatology, Stanford University School
Medicine, Redwood Citya; and Departments of Dermatolo-
,b Otolaryngology,c and Surgery,d Feinberg School of Med-
ine, Northwestern University, Chicago.
orted by the Department of Dermatology, Northwestern
niversity.
licts of interest: None declared.
pted for publication April 22, 2012.
commonly encountered topical preparations andsurgical dressings. Carbon-dioxide laser resurfacingalso carries a potential fire risk, especially if per-formed in an oxygen-enriched environment.2
To our knowledge, controlled studies have notbeen performed to evaluate topical preparations,such as disinfectants and/or hemostatic agents, asa fuel source in the setting of electrosurgery or
Reprint requests: Murad Alam, MD, MSCI, Department of
Dermatology, Northwestern University, 676 N St Clair St, Suite
1600, Chicago, IL 60611. E-mail: [email protected].
Published online May 28, 2012.
0190-9622/$36.00
� 2012 by the American Academy of Dermatology, Inc.
doi:10.1016/j.jaad.2012.04.026

J AM ACAD DERMATOL
VOLUME 67, NUMBER 4Arefiev et al 701
carbon-dioxide laser surgery. In fact, fire risk andprevention techniques are inadequately addressedin the dermatologic literature, with much of the dataon fire safety related to surgical procedures conduct-ed under general anesthesia rather than ambulatorycutaneous and laser surgery. In this study, weconducted live simulations to evaluate the flamma-
CAPSULE SUMMARY
d Electrosurgical and laser devicescontribute to more than 90% of surgicalfires.
d Exposure of dry materials to carbon-dioxide laser can generate flames. Whenexposed to electrosurgery and carbon-dioxide laser, materials soaked withaluminum chloride produce more smokeand char than those soaked withisopropyl alcohol.
d Dermatologists should be aware offlammable materials within the surgicalfield and educate staff regarding firesafety practices.
bility of commonly used top-ical preparations and surgicaldressings/drapes in the set-ting of electrosurgery andcarbon-dioxide laser use.
METHODSDry fuel sources
Surgical dressings anddrapes were selected basedon their frequency of usein procedural dermatol-ogy, and included: gauze(Kendall Curity, 12-ply4-in 3 4-in United StatesPharmacopeial Conventiontype VII gauze sponge); cot-ton surgical towel; surgicaldrape (Graham professio-nal poly-lined towel/drape);
cotton balls; and absorbent underpad drape(Tendersorb Underpads, Tyco HealthcareeKendall).In addition, fresh pork belly skin was also chosen tosimulate human skin.Liquid fuel sourcesTopical fluid preparations were selected based on
their widespread use in dermatologic surgery andknown potential for flammability, and included:isopropyl alcohol 70% (Hydrox Laboratories);chlorhexidine gluconate 4.0% wt/vol (Hibiclens,M€olnlycke Health Care); and aluminum chloride35% (Delasco Dermatologic Lab and Supply Inc).
Ignition sourcesThe ignition sources were also selected based on
their frequency of use in procedural dermatology,and included electrofulguration, electrodesiccation,and carbon-dioxide laser. The energy levels werebased on commonly used parameters.Electrofulguration (Hyfrecator 2000, ConMed Corp,Utica, NY) was set at 18Wusing the high output port,with the tip advanced toward the surface of thematerial until an arc was maintained for 5 seconds.Electrodesiccation (Hyfrecator 2000, ConMed Corp)was also set at 18 W using the high output port, withthe tip gently pressed onto the surface of the materialfor 5 seconds. As we limited the study conditions
to those most commonly used in dermatology prac-tices, we did not study electrocoagulation. Thecarbon-dioxide laser (UltraPulse Active FX,Lumenis Inc, Santa Clara, CA) was set at 12.5 mJand 150 Hz, with a 7-mm square scan size anddensity setting at 3. One full scan size of the carbon-dioxide laser was performed on each material.
Given that povidone io-dine has a short duration ofaction, is inactivated in thepresence of blood, and isnow uncommonly used bydermatologic surgeons, whotend to favor chlorhexidine,we chose not to include po-vidone iodine as a treatmentarm. Significantly, povidoneiodine does not include analcohol base, and so may beexpected to be less flamma-ble than the other solutionsthat were tested.
Experimental procedureAll surgical dressings and
drapes, and pork belly skin,were examined for fire risk
upon exposure to each of the 3 ignition sourcesunder dry, saturated, and damp conditions, with thelatter 2 conditions using each of the 3 liquid fuelsources. The amount of dry material tested allowedfor absorption of 15 mL of fluid, which was used asthe definition of ‘‘saturated.’’ Damp conditions wereattained by squeezing excess fluid out of the materialand then pressing it between 2 pieces of paper towel.With regard to the pork belly skin, saturated condi-tions were characterized by a thin layer of fluid onthe surface of the tissue, and damp conditions weremet when enough fluid was wiped off to leave only amoist sheen on the surface.
Outcome definitions‘‘Spark’’ was recorded if electrofulguration pro-
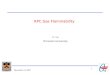
duced sparks from the tip of the electrode to thetested material, or if electrodesiccation producedsparks from the edges of the electrode tip while incontact with the tested material. The presence of avisible plume was recorded as ‘‘smoke.’’ If fireoccurred, this was recorded either as ‘‘focal flame’’if limited to the test area, or ‘‘spreading flame’’ if thefire spread beyond the tested site. If no flamewas observed, but charring was visible, thiswas graded as mild, moderate, or severe char(Fig 1). All outcomes were rated based on forcedagreement between 2 dermatologists trained in

Fig 1. Char on graded scale: mild (left), moderate (mid-dle), and severe (right).
J AM ACAD DERMATOL
OCTOBER 2012702 Arefiev et al
procedural dermatology, and 1 dermatology physi-cian assistant.
RESULTSTable I outlines the response to electrofulgura-
tion, electrodesiccation, and carbon-dioxide lasertreatment performed on surgical dressings, surgicaldrapes, and pork belly skin under dry, saturated, anddamp conditions.
ElectrofulgurationOf the dry materials, only the pork belly skin
developed a spark with associated char. Whenexposed to isopropyl alcohol under saturated anddamp conditions, none of the tested materials pro-duced sparks, char, or smoke with electrofulgura-tion. Based on our unexpected failure to ignitealcohol-soaked materials, we also applied electro-fulguration to gauze dampened with isopropyl alco-hol and water, and to gauze only partially dampenedwith isopropyl alcohol. These 2 additional condi-tions were added to see if the dissociation of alcoholin water, or the proximity of dry gauze to gauzesoaked with alcohol, respectively, would bettersimulate true surgical conditions and be more likelyto result in ignition. However, despite these modifi-cations, still no reaction was observed. Conversely,all materials tested with chlorhexidine gluconateunder saturated and damp conditions produced aspark and associated mild to moderate char. Therewas no difference in the degree of reaction seen withchlorhexidine gluconate under both saturated anddamp conditions except for the drape under dampconditions, which did not elicit spark or char. Damppork belly skin also resulted in a greater accumula-tion of char compared with saturated pork belly skin.All materials tested with aluminum chloride solutiondeveloped a spark under saturated conditions, ex-cept for the underpad. Under damp conditions, the
gauze, drape, and pork belly skin developed morechar in comparison with saturated conditions withaluminum chloride.
ElectrodesiccationAs with electrofulguration, only the pork belly
skin developed char (mild) under dry testing condi-tions. With the addition of isopropyl alcohol, sparksand moderate char developed on the damp under-pad, damp pork belly skin, and saturated pork bellyskin. A range of responses was seen when materialswere made damp or saturated by chlorhexidinegluconate. Variable degrees of sparks, smoke, andchar were noted under all conditions except satu-rated underpad. The pork belly skin again producedmore char with chlorhexidine gluconate under damprather than dry or saturated conditions. When ex-posed to aluminum chloride, sparks developed ondamp pork skin belly and underpad. Smoke withoutassociated sparks was seen with damp gauze.
Carbon-dioxide laserAll dry materials tested with the laser produced
variable degrees of smoke and char, with the under-pad developing focal flame and cotton balls spread-ing flame. Smoke and/or char was also elicited underthe remaining 6 test conditions, with severe charnoted on drapes dampened and saturated withaluminum chloride, and cotton dampened withaluminum chloride.
DISCUSSIONIn recreating test conditions frequently encoun-
tered in procedural dermatology, we were able todemonstrate the potential fire hazard posed byelectrodesiccation, electrofulguration, and carbon-dioxide laser surgery in contact with surgical drapesand topical preparations. Although overt flameswere evident after 1 pulse of the carbon-dioxidelaser to the dry underpad drape and cotton balls,smoke with variable degrees of charring waselicited in 86 of 126 simulated conditions (68%).Interestingly, surgical drapes and dressings satu-rated with isopropyl alcohol failed to ignite withelectrosurgery, although sparks and moderate chardeveloped on pork belly skin and the underpaddrape. Likewise, chlorhexidine gluconate, whichcontains isopropyl alcohol, generated less smokeand char in tested conditions compared with alu-minum chloride, which does not contain isopropylalcohol. Lastly, in 11 of 18 tested conditions, wefound that surgical dressings and drapes madedamp with aluminum chloride produced greaterdegrees of smoke and char when compared withmaterials saturated with aluminum chloride. In the

Table I. Flammability of surgical dressings, drapes, and pork belly skin, with and without topical preparations, in setting of electrofulguration,electrodesiccation, and carbon-dioxide laser use
Material (amounts
adjusted to approximate
equal volumes; except
skin) Ignition source Dry
Isopropyl alcohol 70% Chlorhexidine gluconate 4% Aluminum chloride 35%
Saturated Damp Saturated Damp Saturated Damp
Gauze (2 layers) Electrofulguration / / / Sparks,moderate char
Sparks,moderate char
Sparks, smoke Sparks, severechar
Electrodesiccation / / / Smoke,moderate char
Smoke, sparks,moderate char
/ Smoke,moderate char
CO2 Smoke, mild char Smoke Smoke Smoke Smoke Smoke, mild char Smoke,moderate char
Drape (4 layers) Electrofulguration / / / Sparks,moderate char
/ Sparks, smoke Sparks, severechar
Electrodesiccation / / / Sparks, smoke,moderate char
Mild char Mild char Severe char
CO2 Smoke,moderate char
Smoke, mild char Smoke, mild char Smoke, mild char Smoke, mild char Smoke, severechar
Smoke, severechar
Towel (2 layers) Electrofulguration / / / Sparks, mild char Sparks, mild char Sparks, smoke,moderate char
Sparks, smoke,moderate char
Electrodesiccation / / / Mild char, smoke Sparks, smoke,mild char
Moderate char Moderate char
CO2 Smoke,moderate char
Smoke, mild char Smoke, mild char Smoke, mild char Smoke, mild char Smoke,moderate char
Smoke,moderate char
Underpad (1 layer) Electrofulguration / / / Sparks, smoke,moderate char
Sparks, smoke,moderate char
/ /
Electrodesiccation / / Spark,moderate char
/ Sparks, smoke,moderate char
/ Sparks, smoke,moderate char
CO2 Focal flame Mild char Mild char Smoke Smoke Mild char, smoke Moderate char,smoke
Cotton(8 balls flattened)
Electrofulguration / / / Sparks,moderate char
Sparks,moderate char
Sparks, mild char Sparks,moderate char
Electrodesiccation / / / Sparks, mild char Sparks, mild char Mild char Mild charCO2 Spreading flame Smoke Smoke, mild char Smoke Smoke Smoke, mild char Smoke, severe
charSkin (pork belly) Electrofulguration Sparks,
moderate char/ / Sparks, mild char Sparks,
moderate charSparks, mild char Sparks,
moderate charElectrodesiccation Mild char Sparks,
moderate charSparks,moderate char
Mild char Moderate char / Sparks,moderate char
CO2 Mild char Mild char Mild char Mild char Mild char Moderate char Moderate char
CO2, Carbon-dioxide laser.
JAM
ACADD
ERM
ATOL
VOLU
ME67,N
UM
BER4
Arefi
evet
al
703

J AM ACAD DERMATOL
OCTOBER 2012704 Arefiev et al
remaining 7 test conditions, no difference wasobserved between damp and saturated dressingsand drapes. Thus, even small amounts of aluminumchloride can pose a fire risk and should be avoidedin the surgical field.
Several case reports identifying alcohol-basedskin preparations as a fuel source in surgical fireshave been published.3-5 Despite these data, we wereunable to demonstrate flammability of isopropylalcohol using electrofulguration and electrodesicca-tion. To further explore why isopropyl alcohol failedto ignite under tested conditions, we also evaluatedthe flammability of gauze dampened with isopropylalcohol and water, and gauze only partially damp-ened with isopropyl alcohol. However, we againfailed to elicit char or flames in the tested conditionswhen subjected to electrosurgery or carbon-dioxidelaser pulses. One of the limitations of our study wasthat it was performed at room temperature ratherthan physiologic skin temperature, thus it is possiblethat alcohol evaporation was not optimized to pro-vide concentrations sufficient for combustion.However, flammable vapor from isopropyl alcoholis generated at 538F and should theoretically ignitewhen combined with air, thus it is unclear why wecould not reproduce this reaction under tested con-ditions.6 It is possible that very specific conditionsare required for ignition of alcohol-soaked gauze;this may explain why only a few case reports exist ofalcohol ignition despite the fact that alcohol-soakedgauze is a common finding in surgical fields. Ourstudy suggests that the case report data may exag-gerate the likelihood of inadvertent ignition ofalcohol-impregnated gauze.
Another limitation of our study was the inability toevaluate oxygen supplementation as an indepen-dent factor in tested conditions. Given the inherentsafety concerns posed by the generation of heat inoxygen-enriched environments, we could not ex-pose research personnel to these high-risk scenarios.Nevertheless, it is important to be aware of theincreased likelihood of ignition when electrosurgicalor laser devices are used in high oxygen environ-ments. In fact, one report found that oxygen sup-plementation was a contributing factor in 74% of allsurgical fires, whether delivered through a nasalcannula, face mask, or endotracheal tube.7 Althoughthe fire risk posed by oxygen supplementation ismost relevant for surgeries conducted under generalanesthesia, dermatologists may face similar circum-stances as the population ages and portable oxygendevices become more accessible. To minimize firerisk, it has been suggested that oxygen not beallowed to accumulate under dressings and drapes.Bipolar electrosurgery has also been suggested for
coagulation by the Emergency Care ResearchInstitute as a means to prevent surgical fires insituations where oxygen supplementation is re-quired.8 Lastly, adjusting fraction of inspired oxygento less than 50% may decrease the risk of airway fireduring oropharyngeal surgery.4
In reviewing the literature, 2 previous studieshave examined the ignition potential of surgicaldrapes and dressings, although neither assessedfire risk when topical skin preparations were incor-porated. One study investigating the flammability ofsurgical drapes with continuous firing of a carbon-dioxide laser (15 W, 2-mm spot size) found that alltested drapes ignited in oxygen-enriched environ-ments (50% and 95% oxygen), with nonwovencellulose/polyester blend drapes, woven cotton/polyester blend drapes, and huck cotton toweldrapes igniting in room air at a mean time of 3seconds, 4 seconds, and 12 seconds, respectively.9
Although this study provides insight into the easewith which materials within an operative field can beignited, continuous firing of a carbon-dioxide laseroutside of the target tissue may not simulate routineuse of this laser during patient encounters. A secondstudy evaluating the effects of 2 carbon-dioxidelasers (Coherent Ultrapulse 5000 laser at 300 mJ/50W and 9-mm spot size; Silktouch at 18 W and 9-mmspot size) on surgical drapes and dressings reportedignition of dry blue sterile drapes and dry gauzewithin 1 pass of the Silktouch laser and 1 to 3 passesof the Coherent Ultrapulse 5000 laser. Of note, noflames were observed when these materials weremoistened with saline.10 In comparing our resultswith the latter study, we were able to elicit flameswith 1 pass of the carbon-dioxide laser to theunderpad drape and cotton balls, but not in testedconditions using dry sterile drapes. These divergentdata may be explained by the difference in lasersettings used in our study and that of Rohrich et al.10
Overall, our study evaluated many more conditionsthan either of these prior studies, and did so in amanner that more closely mimicked actual surgicalconditions.
Beyond the specific high-risk conditions we un-covered, our study should be a general reminder ofthe need to identify and correct flammability risksbefore ignition occurs. Because 90% of surgical firesare caused by monopolar electrosurgical units andlaser devices, appropriate use of such equipment,and adequate staff training, is imperative.11 If der-matologic procedures are delegated to physicianassistants or other mid-level providers, fire safetytraining may be an adjunct to procedure-specificinstruction. In high-risk environments, checklists or atime-out performed before each procedure can lead

J AM ACAD DERMATOL
VOLUME 67, NUMBER 4Arefiev et al 705
to the identification and removal of potential fuelsources from the surgical field. Given the sporadicrisk of alcohol ignition, it may be most prudent tolet alcohol-based skin preparations dry completelybefore draping the patient.3 For longer procedures,positioning of the drapes may be modified so as notto allow flammable vapors to accumulate. Somehave suggested that hairs within the surgical fieldmay be clipped to prevent pooling of potentiallyflammable solutions.
In summary, our study confirms that fire is apotential complication of dermatologic proceduresusing electrosurgery and laser devices. More thantwo thirds of the 126 conditions we simulated led tochar, and we were able to elicit flames with inadver-tent exposure of dry underpad drapes and cottonballs to the carbon-dioxide laser. Surprisingly, sometopical preparations that are not routinely consideredvery flammable, namely aluminum chloride, werefound to increase risk. Our study should be helpfulfor future researchers, who may modify more exper-imental conditions, and seek to better understand thefactors leading to char and fire in some rare cases.
Fortunately, to the extent that dermatologic sur-gery rarely requires oxygen supplementation, firerisk during skin cancer and cutaneous laser surgeryunder local anesthesia is very low. In addition,hidden fires are less likely in dermatology as patientsare awake and able to communicate. Fire safetyresearch of the type we undertook shows the lowrisk of overt fire during cutaneous applications and
provides some useful information that may help usreduce this risk even further.
REFERENCES
1. Educational videos on surgical fires. Health Devices 2000;29:
274-80.
2. Daane SP, Toth BA. Fire in the operating room: principles and
prevention. Plast Reconstr Surg 2005;115:73e-5e.
3. Batra S, Gupta R. Alcohol based surgical prep solution and the
risk of fire in the operating room: a case report. Patient Saf
Surg 2008;2:10.
4. Roy S, Smith LP. What does it take to start an oropharyngeal
fire? Oxygen requirements to start fires in the operating room.
Int J Pediatr Otorhinolaryngol 2011;75:227-30.
5. Patel R, Chavda KD, Hukkeri S. Surgical field fire and skin burns
caused by alcohol-based skin preparation. J Emerg Trauma
Shock 2010;3:305.
6. US Department of Labor. Occupational safety and health
guidelines for isopropyl alcohol; Occupational Safety and
Health Administration. Available from: URL:http://www.osha.
gov/SLTC/healthguidelines/isopropylalcohol/recognition.html.
Accessed September 1, 2011.
7. A clinician’s guide to surgical fires: how they occur, how to
prevent them, how to put them out. Health Devices 2003;32:
5-24.
8. ECRI Institute. New clinical guide to surgical fire prevention:
patients can catch fireehere’s how to keep them safer. Health
Devices 2009;38:314-32.
9. Wolf GL, Sidebotham GW, Lazard JLP, Charchaflieh JG. Laser
ignition of surgical drape materials in air, 50% oxygen, and
95% oxygen. Anesthesiology 2004;100:1167-71.
10. Rohrich RJ, Gyimesi IM, Clark P, Burns AJ. CO2 laser safety
considerations in facial skin resurfacing. Plast Reconstr Surg
1997;100:1285-90.
11. Smith LP, Roy S. Operating room fires in otolaryngology:
risk factors and prevention. Am J Otolaryngol 2011;32:
109-14.