Embed Size (px)
Citation preview
Fluid and Electrolytes: Navigating the Chem-7
Jeffrey H. William, MD Assistant Professor of Medicine, HMS
Associate Program Director, BIDMC Renal Fellowship Co-Firm Chief, Tullis Firm, BIDMC Internal Medicine Residency
Primary Care Internal Medicine 2019
October 21, 2019
Disclosures
• None
Logging into Nearpod
Step 1. Go to this website: https://nearpod.com. Scroll down until you see a white text box with “For Students: Enter CODE” Step 2. Click in this white box and enter DVUNB into the box on the webpage. Then click on the arrow to the right of the typed CODE. Step 3. Type in a fun nickname. Don’t worry, your answers will still be anonymous.
Simplistic view of the kidneys • Kidneys help maintain homeostasis:
– Sensing and regulation of total circulating volume (Na+ content)
– Maintenance of serum osmolality to prevent brain swelling or shrinking (Na+ concentration / water)
– Control of serum electrolyte concentrations within small ranges (i.e. potassium, bicarbonate, calcium, magnesium, phosphorus)
– Elimination of toxins/nitrogenous by-products of protein catabolism (i.e. BUN)
https://www.pinterest.com/pin/120963939967022898/
The Chem-7 tells us so much about our patients!
• Na+ = WATER balance • K+ = medication effect,
dietary intake, renal function
• HCO3- = acid-base balance
• BUN and Cr = renal function • Glucose = diabetes mellitus
Na+
K+
Cl-
HCO3-
BUN
Cr Glucose
Today’s Case A 34-year-old woman presents to the clinic with diffuse abdominal pain and dysuria. She has a history of obesity, bipolar disorder, and hypertension. She is very thirsty. She has had some medication adherence issues in the past, but states that she has been better about remembering lately. Medications: hydrochlorothiazide 12.5mg daily, olmesartan 20mg daily, and oxcarbazepine (Trileptal)
Physical Exam
Vitals: T100.1°F, BP 80/40 mmHg, HR 120 bpm, RR 38 breaths/minute, BMI 37 kg/m2
General: Uncomfortable, breathing rapidly. HEENT: Mucous membranes were dry. CV: Tachycardic, normal S1 and S2, no murmurs, no S3/S4 Resp: Lungs are clear to auscultation and percussion. Abdomen: Distended and diffusely tender. Extremities: Trace lower extremity edema. Neuro: Somewhat inattentive, but conversant. No focal deficits

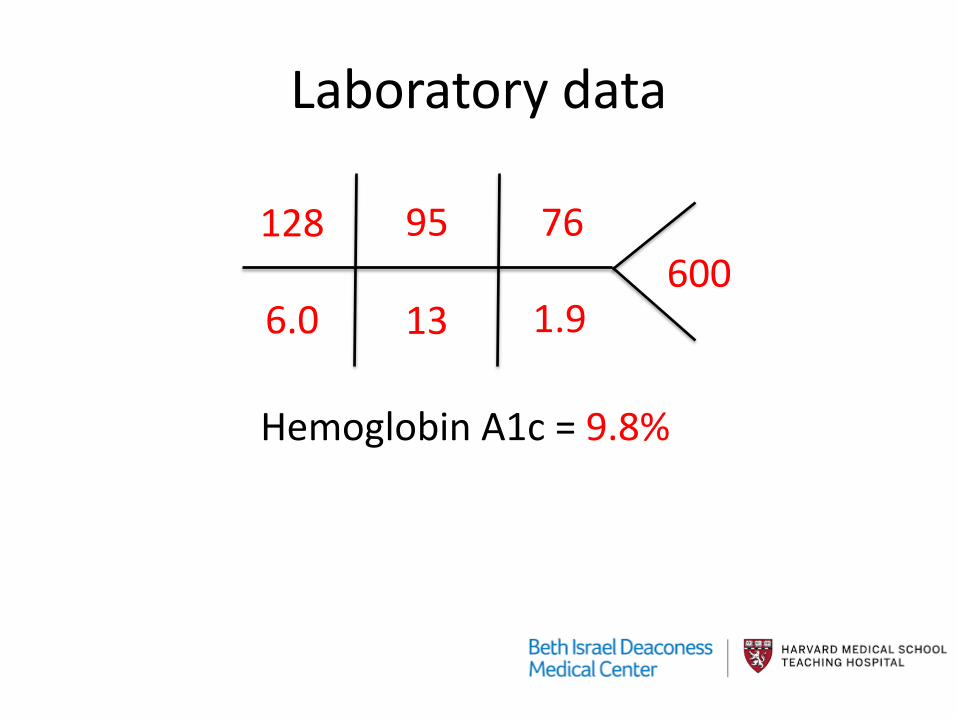
Laboratory data
128
6.0
95
13
76
1.9 600
Hemoglobin A1c = 9.8%

Where do you even start??
128
6.0
95
13
76
1.9 600
Hemoglobin A1c = 9.8%
Hyponatremia
Hyperkalemia
Low bicarbonate/?acidosis
Elevated BUN and creatinine
Hyperglycemia
Prioritizing your approach
Which electrolyte abnormality will you address first? a) Hyponatremia b) Hyperkalemia c) Low bicarbonate (presumed acidosis) d) Azotemia (high BUN and creatinine) e) Hyperglycemia
HYPERKALEMIA
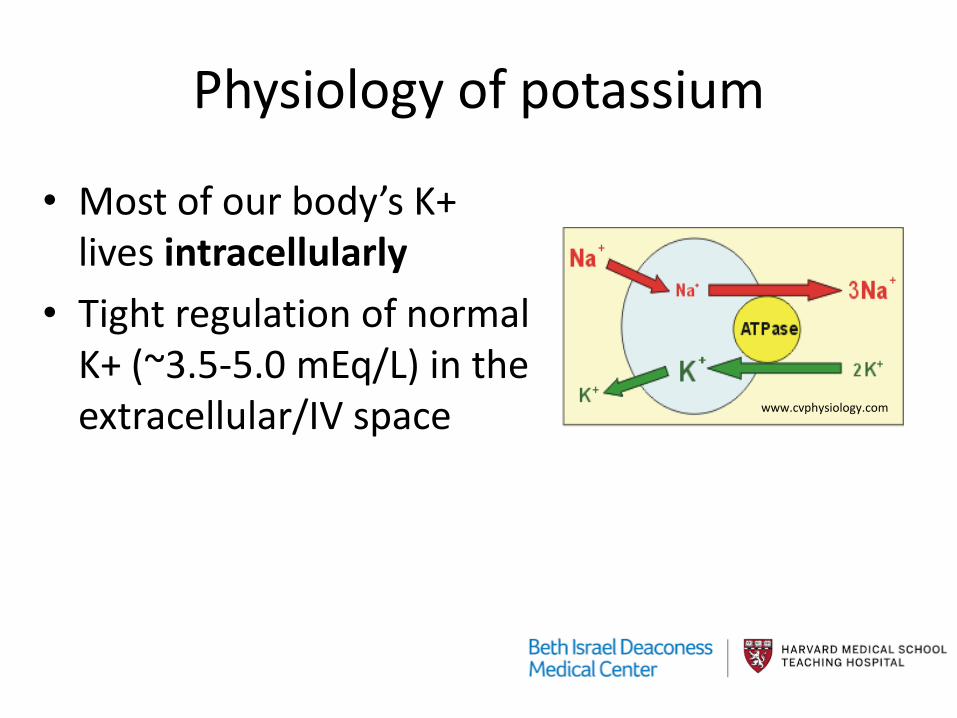
Physiology of potassium
• Most of our body’s K+ lives intracellularly
• Tight regulation of normal K+ (~3.5-5.0 mEq/L) in the extracellular/IV space www.cvphysiology.com

When do we detect excess K+ in the blood (via phlebotomy)?
• Cellular redistribution • Intake > excretion
• Requires impairment in renal excretion • Cell lysis
– Tumor lysis syndrome/cell death (in vivo) – Pseudohyperkalemia (in vitro)
• Tourniquet use • Clot formation in EDTA-based collection tubes
Therapy for hyperkalemia harnesses K+ physiology
• Limit K+ intake • Discontinue medications that may alter K+
excretion • Promote intracellular shift • Improve K+ excretion/removal

Limit K+ intake: K+ = 39.1 mg =1mmol or 1mEq
• Banana = 1 mEq/inch • OJ has 12 mEq/cup • Nu salt™ - 530 mg per 1/6 tsp =13 mEq • Tomato sauce 811 mg/1cup= 20mEq • 1 cup of raisins = 28 mEq • Baked potato = 22 mEq • 8 ounce Steak = 30 mEq
www.kidney.org

Palmer, B. F. NEJM 2004;351:585-592
Impaired release of renin: NSAIDS, beta blockers, diabetes, advanced age, tacrolimus
ACE inhibitors
Angiotensin receptor blockers
Impaired aldosterone metabolism: adrenal disease, heparin, ketoconazole
Aldosterone receptor blockers (spironolactone and eplerenone)
Medications and RAAS
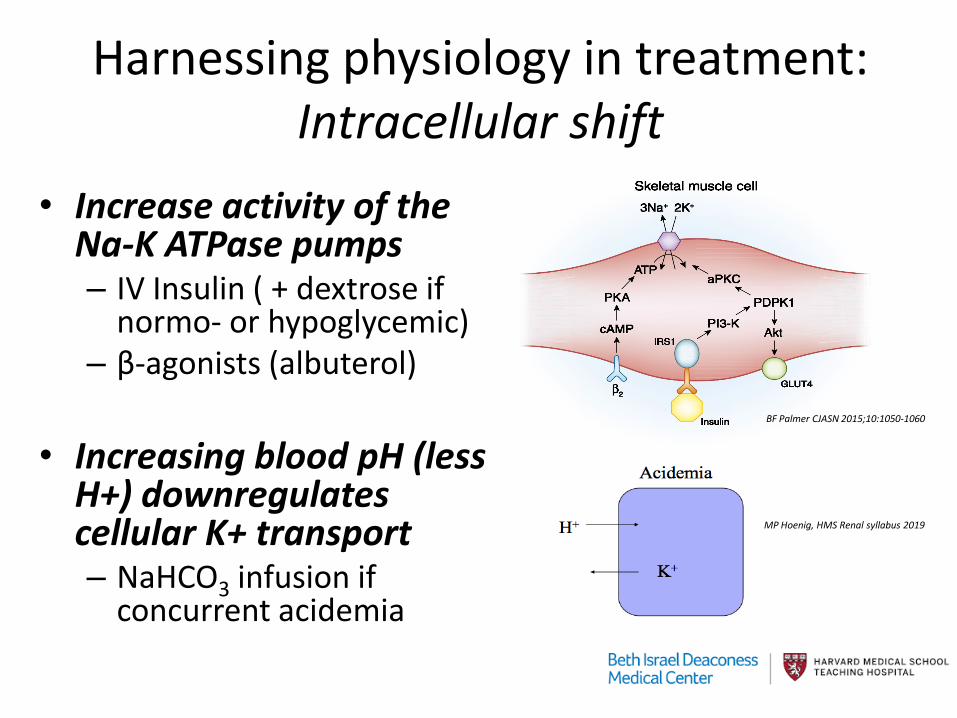
Harnessing physiology in treatment: Intracellular shift
• Increase activity of the Na-K ATPase pumps – IV Insulin ( + dextrose if
normo- or hypoglycemic) – β-agonists (albuterol)
• Increasing blood pH (less
H+) downregulates cellular K+ transport – NaHCO3 infusion if
concurrent acidemia
BF Palmer CJASN 2015;10:1050-1060
MP Hoenig, HMS Renal syllabus 2019
Ankita Roy et al. CJASN 2015;10:305-324
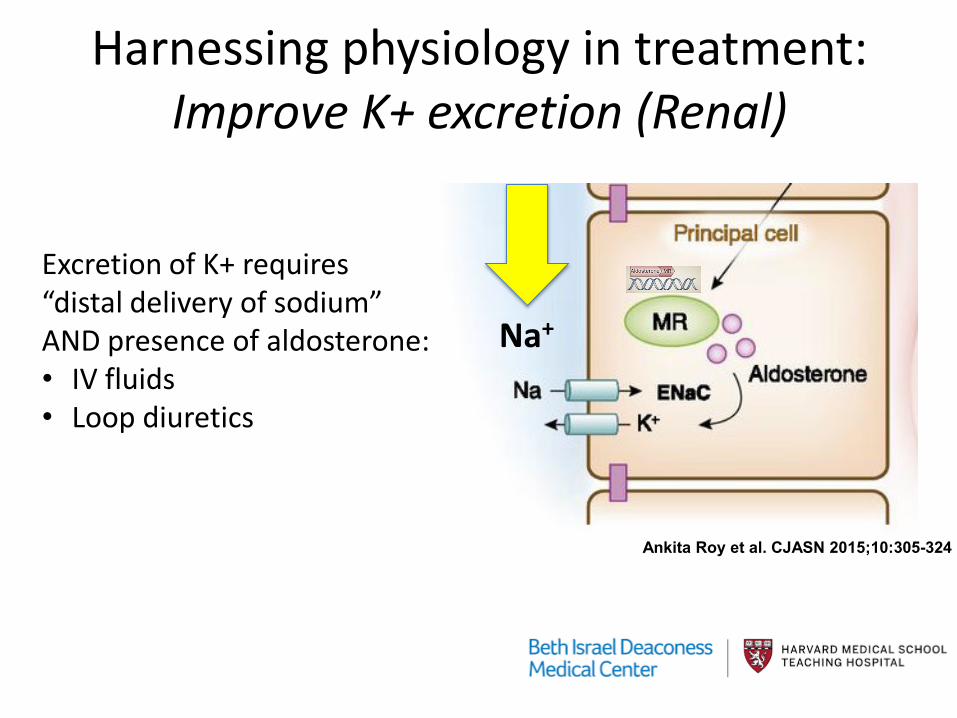
Na+
Harnessing physiology in treatment: Improve K+ excretion (Renal)
Excretion of K+ requires “distal delivery of sodium” AND presence of aldosterone: • IV fluids • Loop diuretics
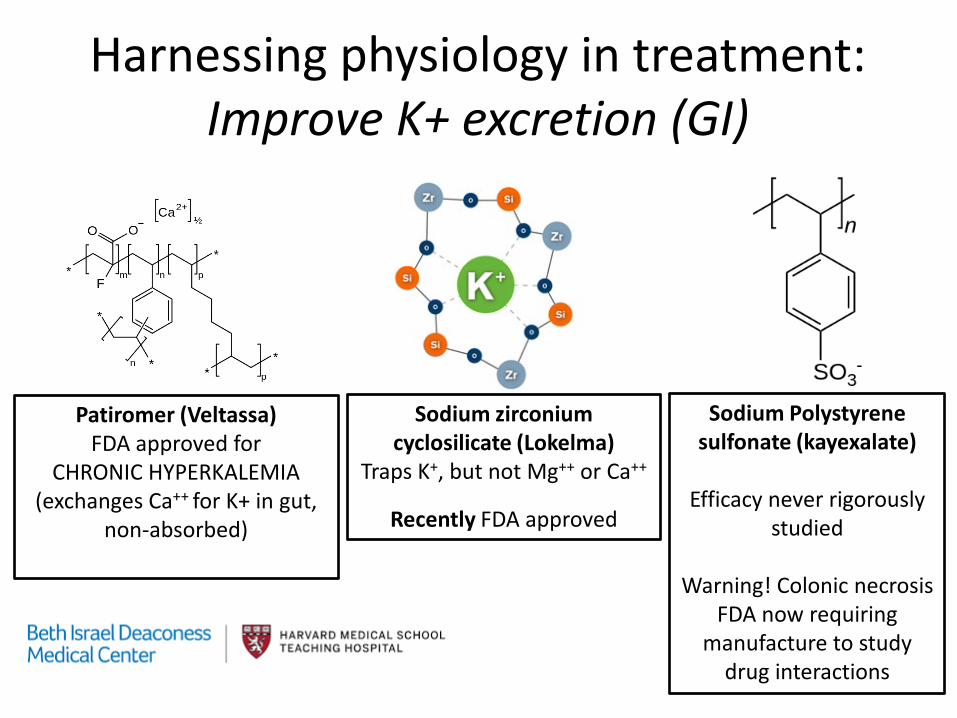
Patiromer (Veltassa) FDA approved for
CHRONIC HYPERKALEMIA (exchanges Ca++ for K+ in gut,
non-absorbed)
Sodium zirconium cyclosilicate (Lokelma)
Traps K+, but not Mg++ or Ca++
Recently FDA approved
Sodium Polystyrene sulfonate (kayexalate)
Efficacy never rigorously
studied
Warning! Colonic necrosis FDA now requiring
manufacture to study drug interactions
Harnessing physiology in treatment: Improve K+ excretion (GI)
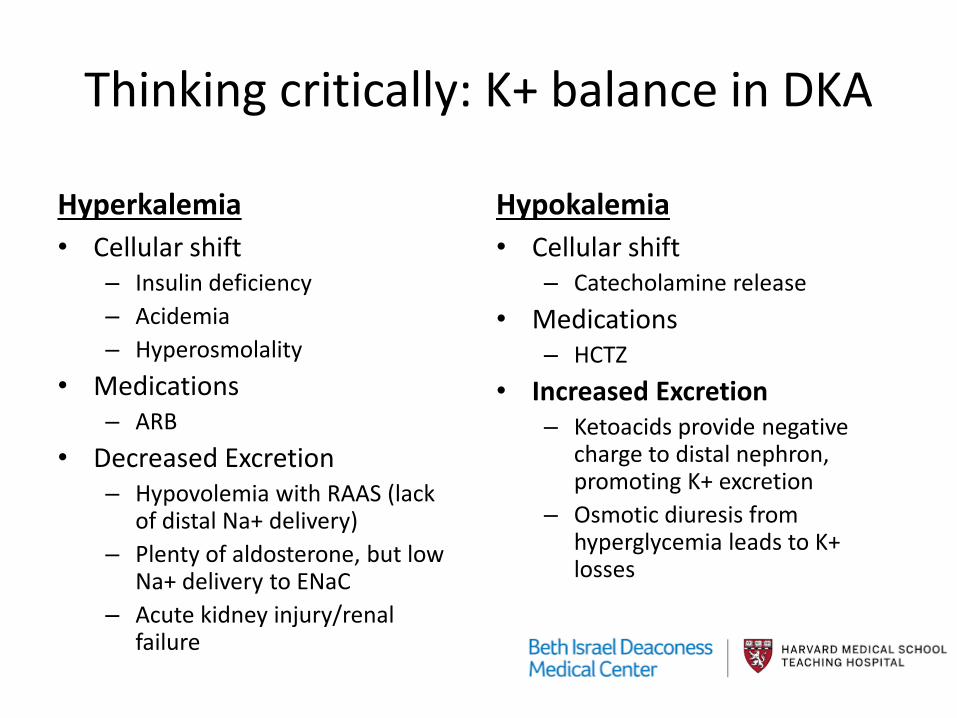
Thinking critically: K+ balance in DKA
Hyperkalemia • Cellular shift
– Insulin deficiency – Acidemia – Hyperosmolality
• Medications – ARB
• Decreased Excretion – Hypovolemia with RAAS (lack
of distal Na+ delivery) – Plenty of aldosterone, but low
Na+ delivery to ENaC – Acute kidney injury/renal
failure
Hypokalemia • Cellular shift
– Catecholamine release • Medications
– HCTZ • Increased Excretion
– Ketoacids provide negative charge to distal nephron, promoting K+ excretion
– Osmotic diuresis from hyperglycemia leads to K+ losses
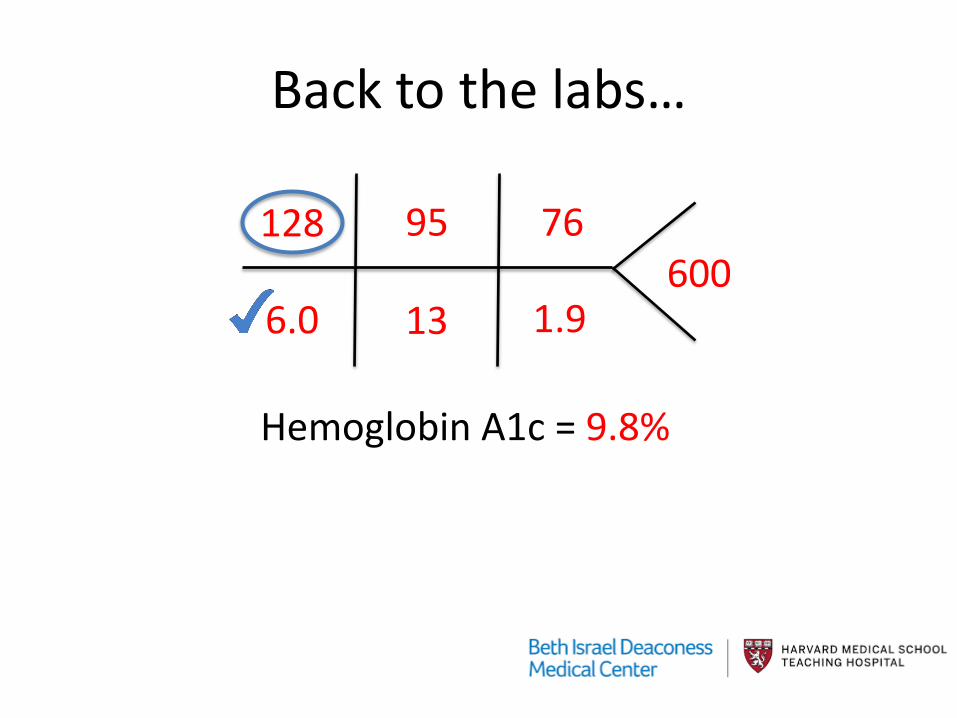
Back to the labs…
128
6.0
95
13
76
1.9 600
Hemoglobin A1c = 9.8%
HYPONATREMIA
Hyponatremia is a WATER problem!
Today’s Case A 34-year-old woman presents to the clinic with diffuse abdominal pain and dysuria. She has a history of obesity, bipolar disorder, and hypertension. She is very thirsty. She has had some medication adherence issues in the past, but states that she has been better about remembering lately. Medications: hydrochlorothiazide 12.5mg daily, olmesartan 20mg daily, and oxcarbazepine (Trileptal)
Laboratory data
128
6.0
95
13
76
1.9 600
Hemoglobin A1c = 9.8%
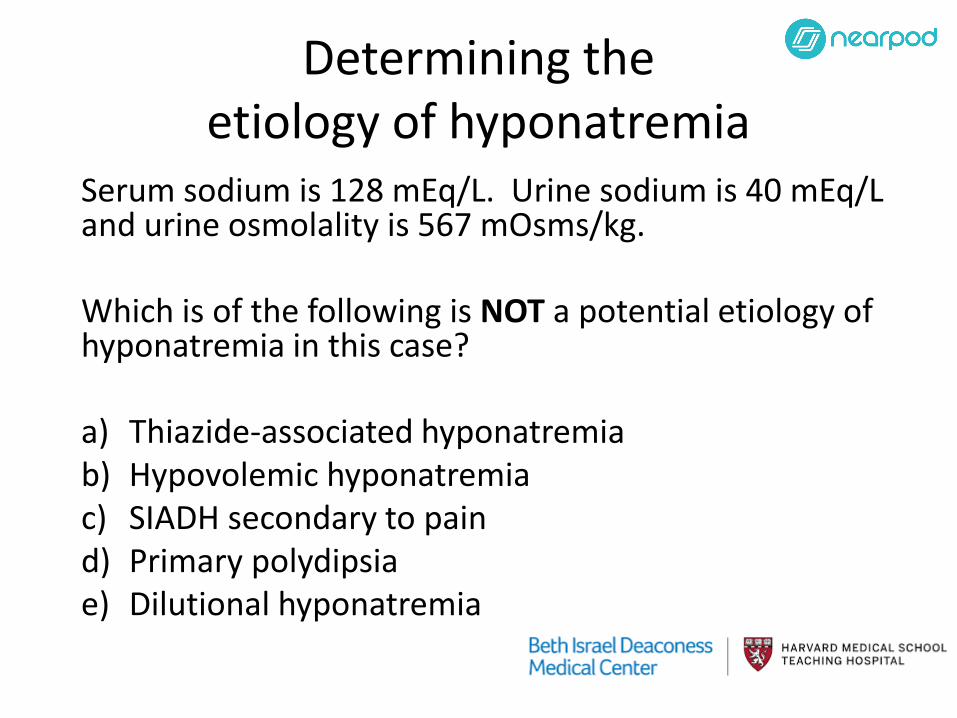
Determining the etiology of hyponatremia
Serum sodium is 128 mEq/L. Urine sodium is 40 mEq/L and urine osmolality is 567 mOsms/kg. Which is of the following is NOT a potential etiology of hyponatremia in this case? a) Thiazide-associated hyponatremia b) Hypovolemic hyponatremia c) SIADH secondary to pain d) Primary polydipsia e) Dilutional hyponatremia
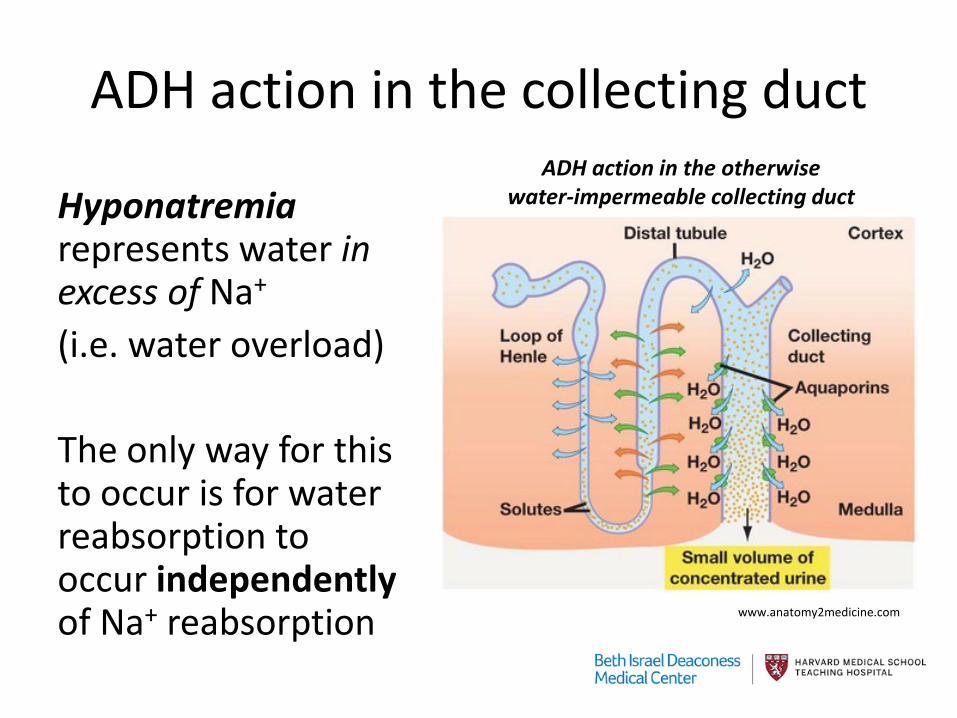
ADH action in the collecting duct
Hyponatremia represents water in excess of Na+
(i.e. water overload) The only way for this to occur is for water reabsorption to occur independently of Na+ reabsorption
ADH action in the otherwise water-impermeable collecting duct
www.anatomy2medicine.com
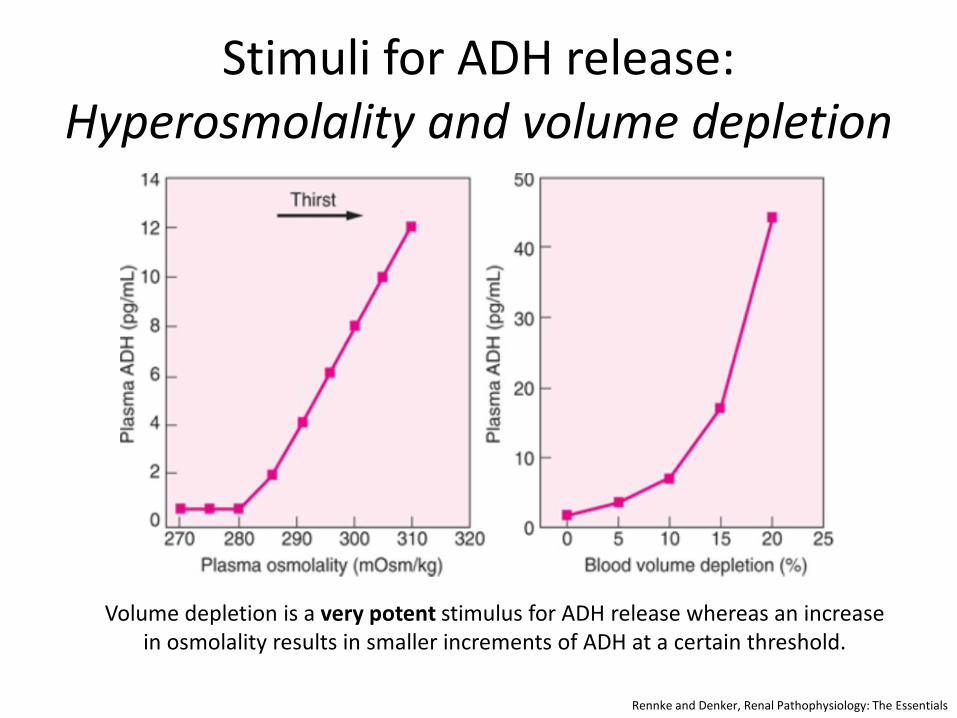
Stimuli for ADH release: Hyperosmolality and volume depletion
Rennke and Denker, Renal Pathophysiology: The Essentials
Volume depletion is a very potent stimulus for ADH release whereas an increase in osmolality results in smaller increments of ADH at a certain threshold.
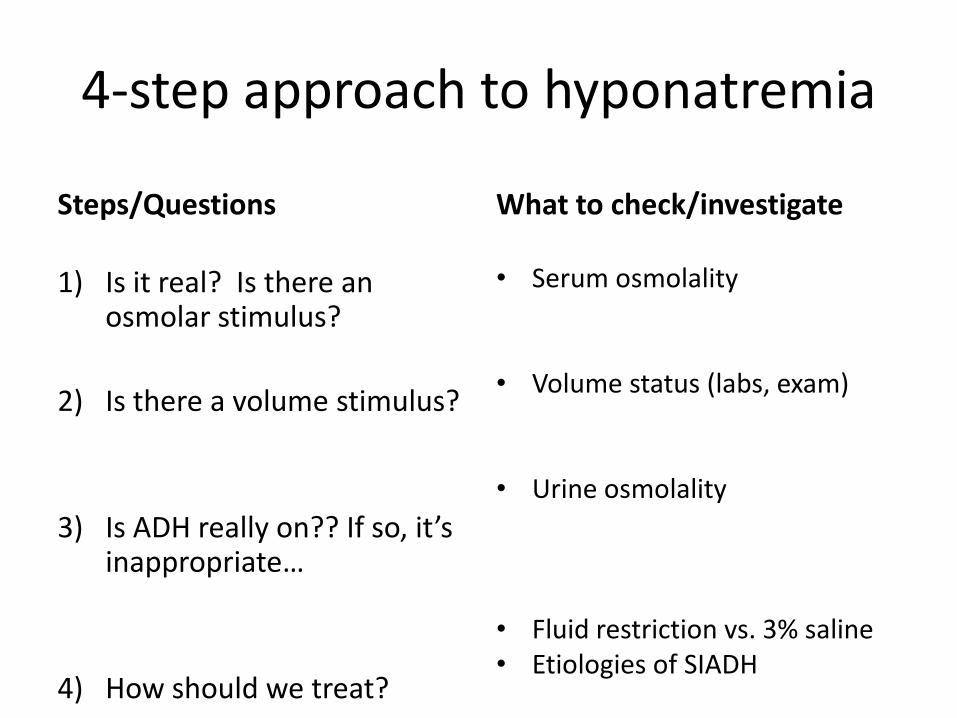
4-step approach to hyponatremia
Steps/Questions
1) Is it real? Is there an osmolar stimulus?
2) Is there a volume stimulus?
3) Is ADH really on?? If so, it’s inappropriate…
4) How should we treat?
What to check/investigate
• Serum osmolality
• Volume status (labs, exam)
• Urine osmolality
• Fluid restriction vs. 3% saline • Etiologies of SIADH
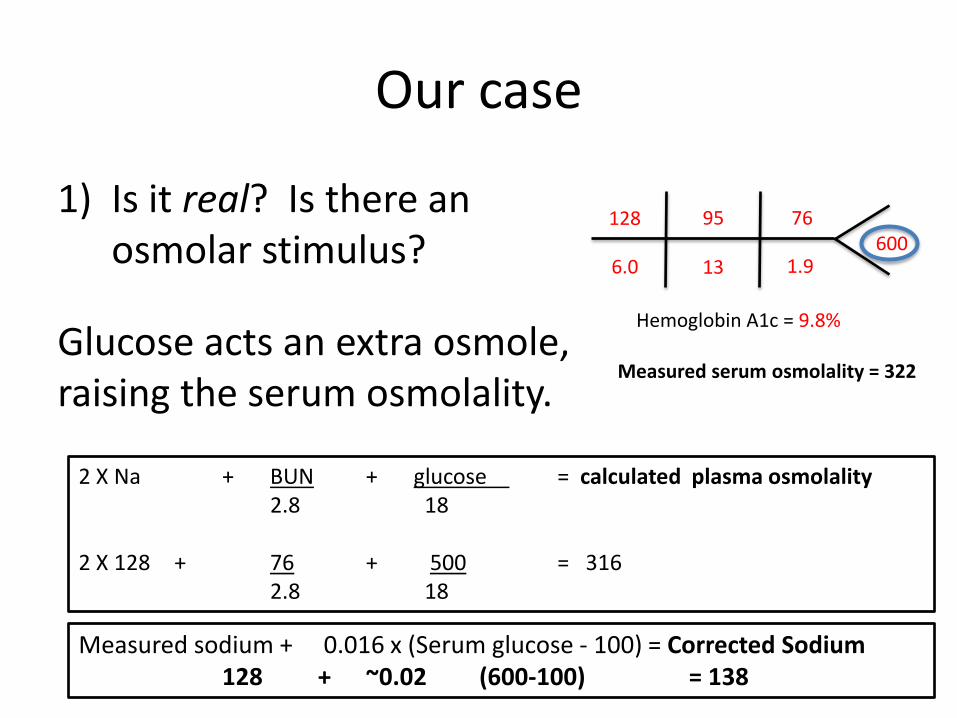
Our case
1) Is it real? Is there an osmolar stimulus?
Glucose acts an extra osmole, raising the serum osmolality.
128
6.0
95
13
76
1.9 600
Hemoglobin A1c = 9.8%
Measured serum osmolality = 322
2 X Na + BUN + glucose = calculated plasma osmolality 2.8 18 2 X 128 + 76 + 500 = 316 2.8 18
Measured sodium + 0.016 x (Serum glucose - 100) = Corrected Sodium 128 + ~0.02 (600-100) = 138

Dilutional hyponatremia (in vivo) • Low serum sodium, but high serum osmolality! • Extra osmoles draw water from inside the cells into the
extracellular space (i.e., hyperglycemia, mannitol, and glycine)

Pseudohyponatremia (in vitro) “Solid phase” of plasma increased by paraproteins and triglycerides dilution effect drops [Na+]
Turchin A, Seifter JL, Seely EW. Clinical Problem Solving: Mind the Gap. New Engl J Med 349;15:1465-9
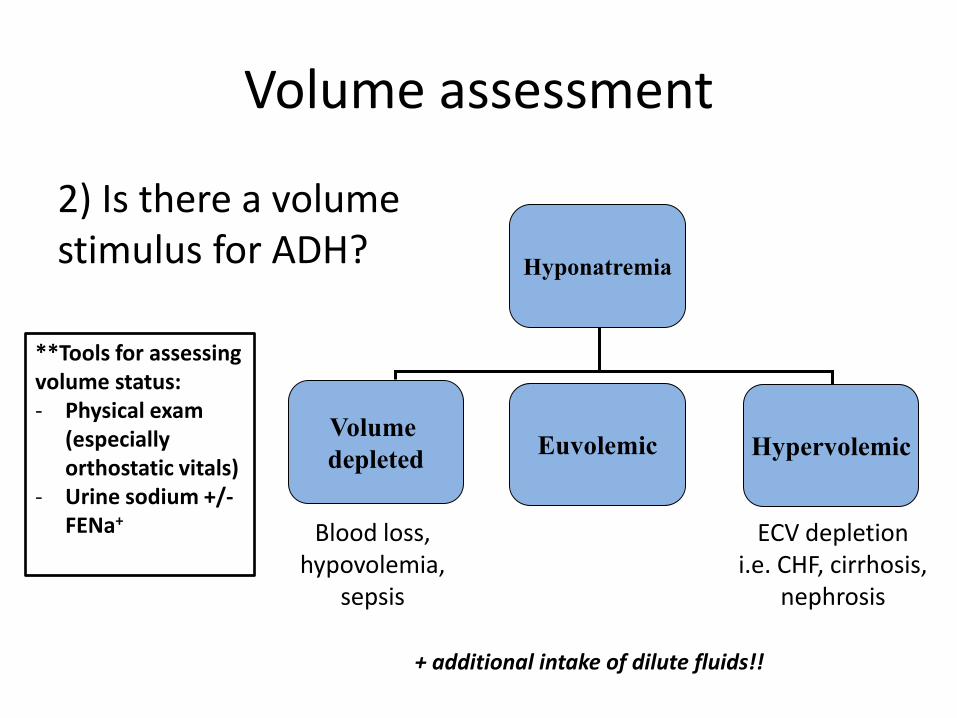
Volume assessment
2) Is there a volume stimulus for ADH?
Hyponatremia
Volume depleted Euvolemic Hypervolemic
Blood loss, hypovolemia,
sepsis
ECV depletion i.e. CHF, cirrhosis,
nephrosis
**Tools for assessing volume status: - Physical exam
(especially orthostatic vitals)
- Urine sodium +/- FENa+
+ additional intake of dilute fluids!!
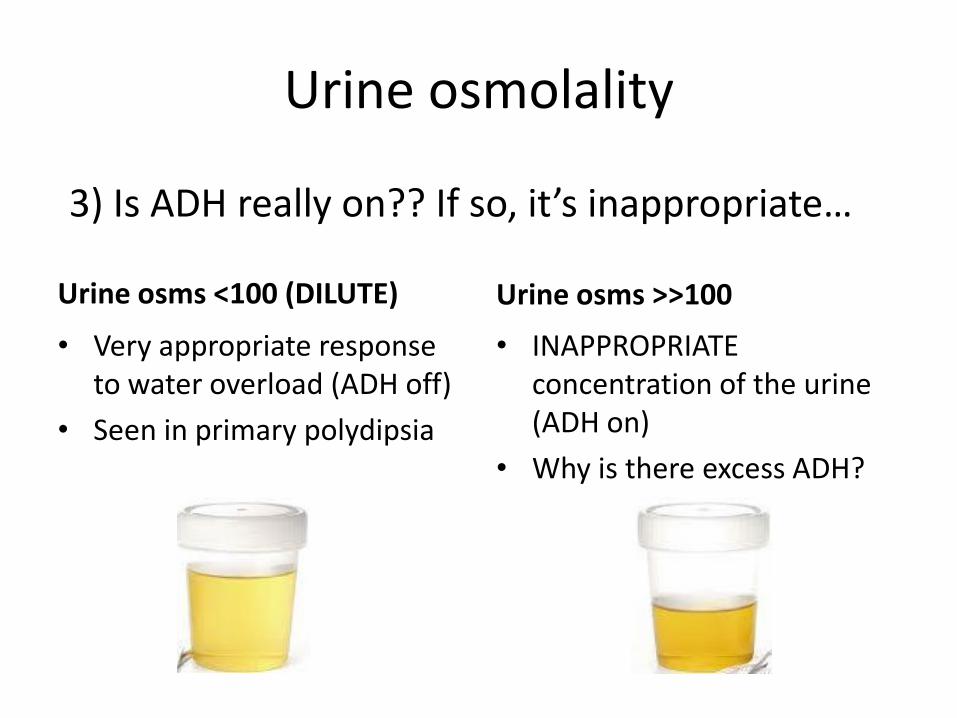
Urine osmolality
Urine osms <100 (DILUTE)
• Very appropriate response to water overload (ADH off)
• Seen in primary polydipsia
Urine osms >>100
• INAPPROPRIATE concentration of the urine (ADH on)
• Why is there excess ADH?
3) Is ADH really on?? If so, it’s inappropriate…
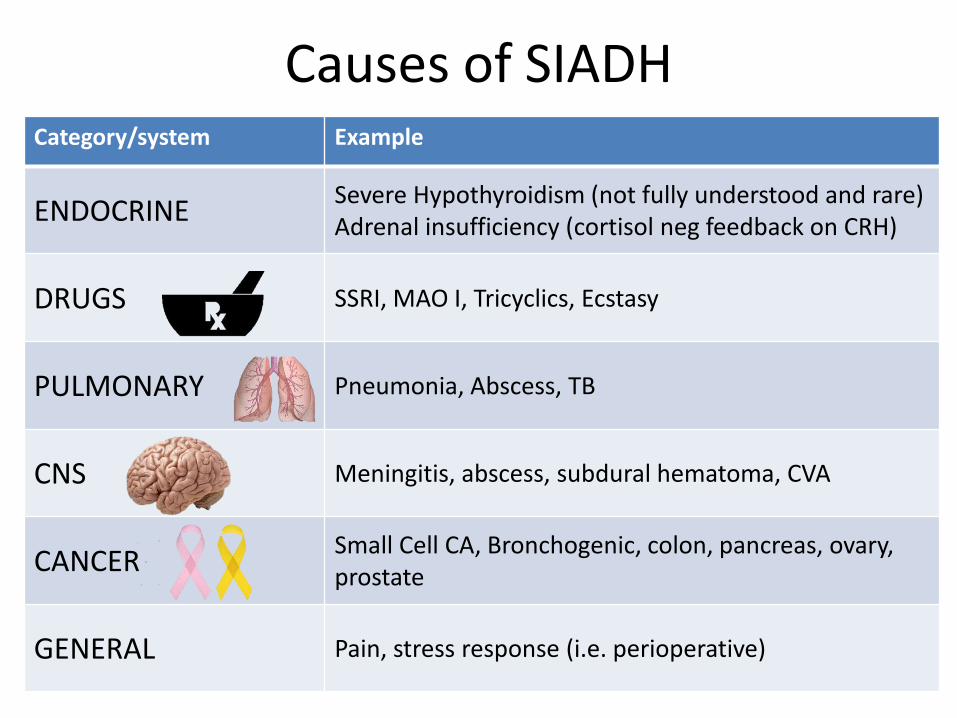
Causes of SIADH Category/system Example
ENDOCRINE Severe Hypothyroidism (not fully understood and rare) Adrenal insufficiency (cortisol neg feedback on CRH)
DRUGS SSRI, MAO I, Tricyclics, Ecstasy
PULMONARY Pneumonia, Abscess, TB
CNS Meningitis, abscess, subdural hematoma, CVA
CANCER Small Cell CA, Bronchogenic, colon, pancreas, ovary, prostate
GENERAL Pain, stress response (i.e. perioperative)
Considerations for treating SIADH
4) How should we treat? • Chronicity (acute vs. “chronic”) • Symptoms (neurologic) • Correction of no more than 6-8 mEq/24 hours • Address underlying etiology!

The most dangerous part of managing Na+ problems is the CORRECTION
• If you did not witness the initial Na+ change or you aren’t sure, consider the hyponatremia to be chronic
• Dysnatremias represent changes in serum osmolality and, in turn, neuronal cell size
Danziger and Zeidel CJASN 2015
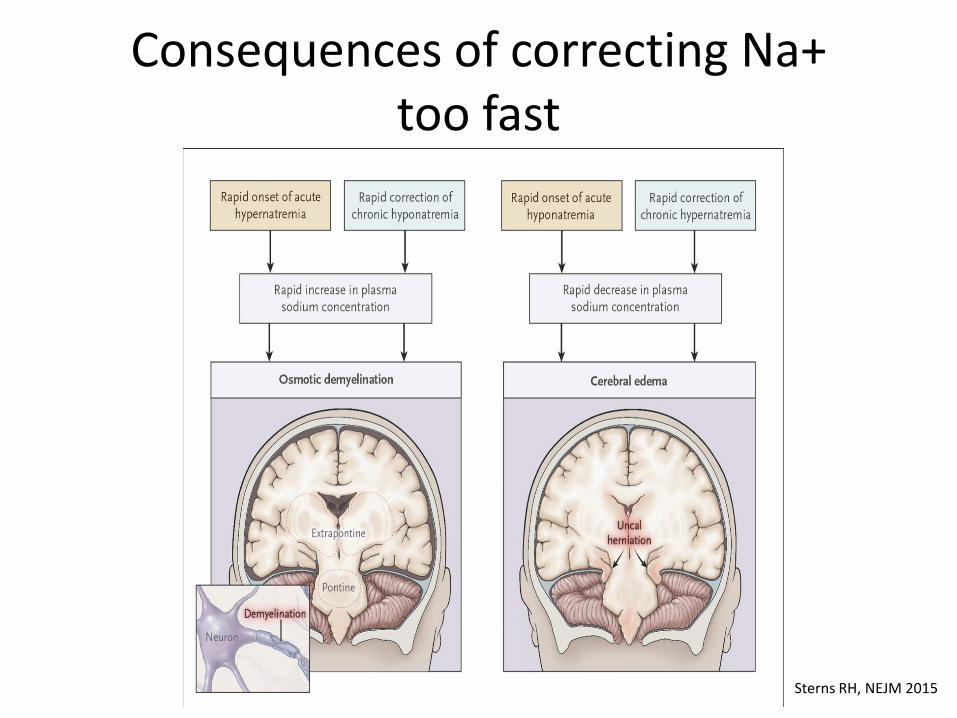
Consequences of correcting Na+ too fast
Sterns RH, NEJM 2015

Tips for treating severe, acute hyponatremia
• 3% (hypertonic) saline if severely altered mental status or concerning neurologic findings – Consider addition of loop diuretics if evidence of
volume overload • Watch for overcorrection
– Correction may occur rapidly once volume replete and stimulus to ADH release suppressed
– Closely follow [Na+] during correction, q1-2 hours • Discontinue offending medications • Do NOT give isotonic fluids if suspicion for SIADH
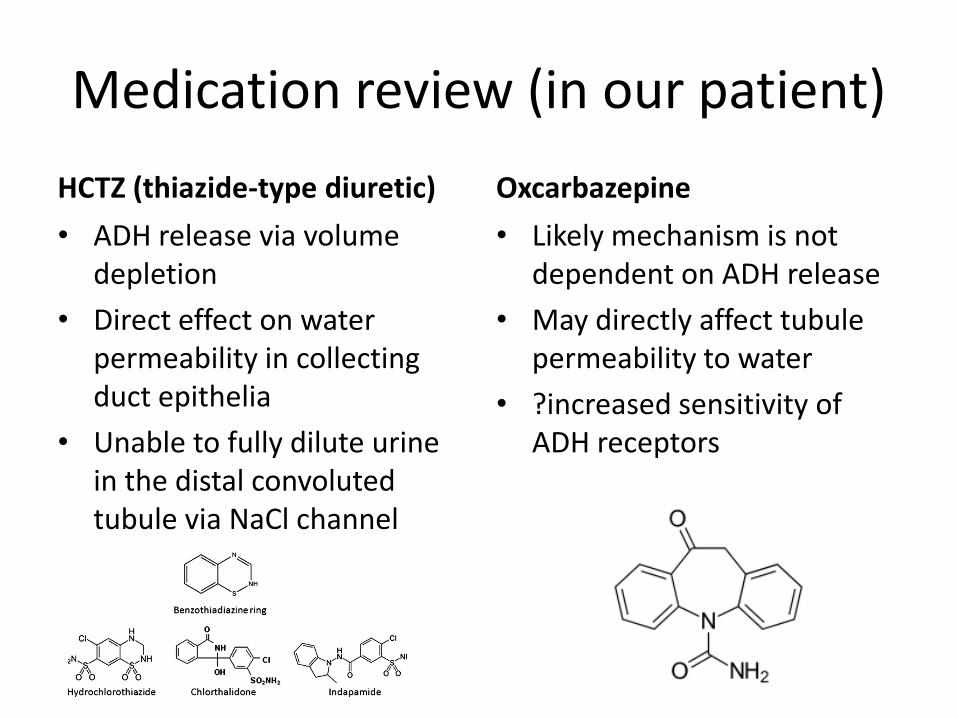
Medication review (in our patient) HCTZ (thiazide-type diuretic) • ADH release via volume
depletion • Direct effect on water
permeability in collecting duct epithelia
• Unable to fully dilute urine in the distal convoluted tubule via NaCl channel
Oxcarbazepine • Likely mechanism is not
dependent on ADH release • May directly affect tubule
permeability to water • ?increased sensitivity of
ADH receptors

Why is NS in SIADH a bad idea?
With a fixed urine osmolality of 600mOsm/L, 1L of NS actually ADDED more water into the body, further worsening the hyponatremia!
= + = 100 mOsm
= fluid
0.9% saline (300mOsm in 1L)
Urine (300mOsms in 0.5L)
0.5L of free water
NS ~ 300mOsm/L Urine osms = 600mOsm/L

Strategies in the treatment for outpatient hyponatremia in setting of SIADH
Small volume of concentrated urine
ADH IS PRESENT • Fluid intake (oral and IV) – Limit fluid intake
• Increase solute intake – Salt tabs (though these make patients thirsty) – High protein diet
• Medications Goal: Limit kidneys’ ability to make concentrated urine loop diuretics limit gradient V2 receptor blocker block ADH effect

Hays R. N Engl J Med 2006;355:2146-2148
Oral Vasopressin-Receptor Antagonists
VAPRISOL Conivaptan (IV)
SAMSCA Tolvaptan (oral)
• FDA approved for hyponatremia in setting of euvolemia (SIADH) and volume overload (CHF and cirrhosis) with serum Na <125
• response variable so start in hospital setting and $$$ • do not prescribe if hypodipsia or difficulty accessing water!
Chronic hyponatremia?
Am J Med. 2006;119:71.e1-71.e8.
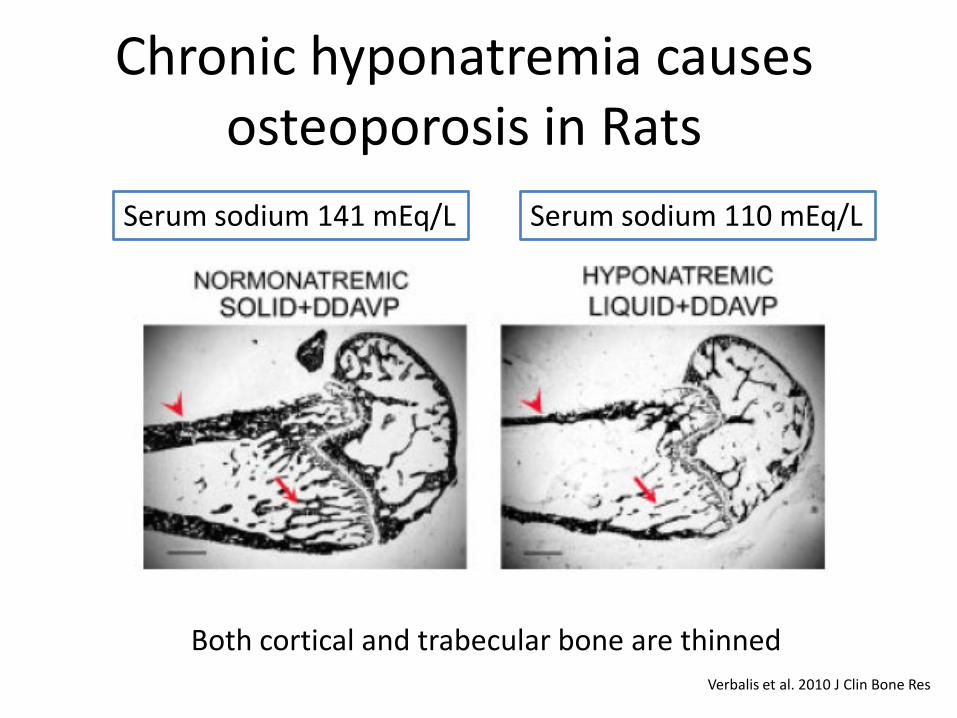
Chronic hyponatremia causes osteoporosis in Rats
Serum sodium 141 mEq/L Serum sodium 110 mEq/L
Both cortical and trabecular bone are thinned Verbalis et al. 2010 J Clin Bone Res
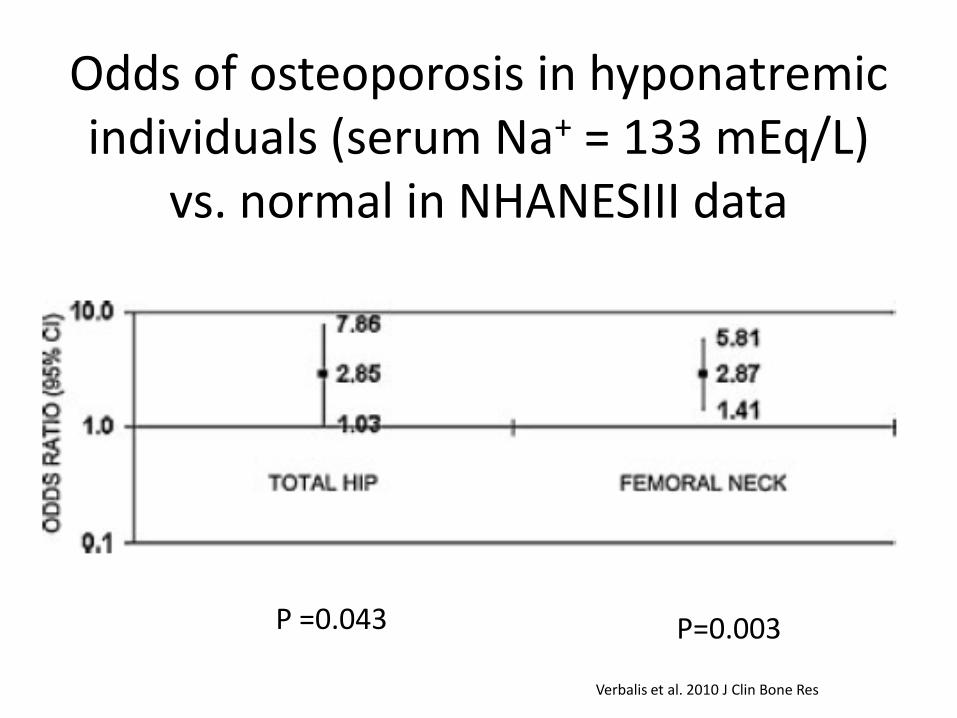
Odds of osteoporosis in hyponatremic individuals (serum Na+ = 133 mEq/L)
vs. normal in NHANESIII data
Verbalis et al. 2010 J Clin Bone Res
P =0.043 P=0.003

Chronic hyponatremia (Na <135 mEq/L)
CNS impairment • Unsteady gait • Confusion
Osteoporosis • Decrease bone mineralization • Increased osteoclast activity
Fall Fragile bones
FRACTURE From: Verbalis 2010
Back to the labs…again…
128
6.0
95
13
76
1.9 600
Hemoglobin A1c = 9.8%
ACID-BASE ABNORMALITIES
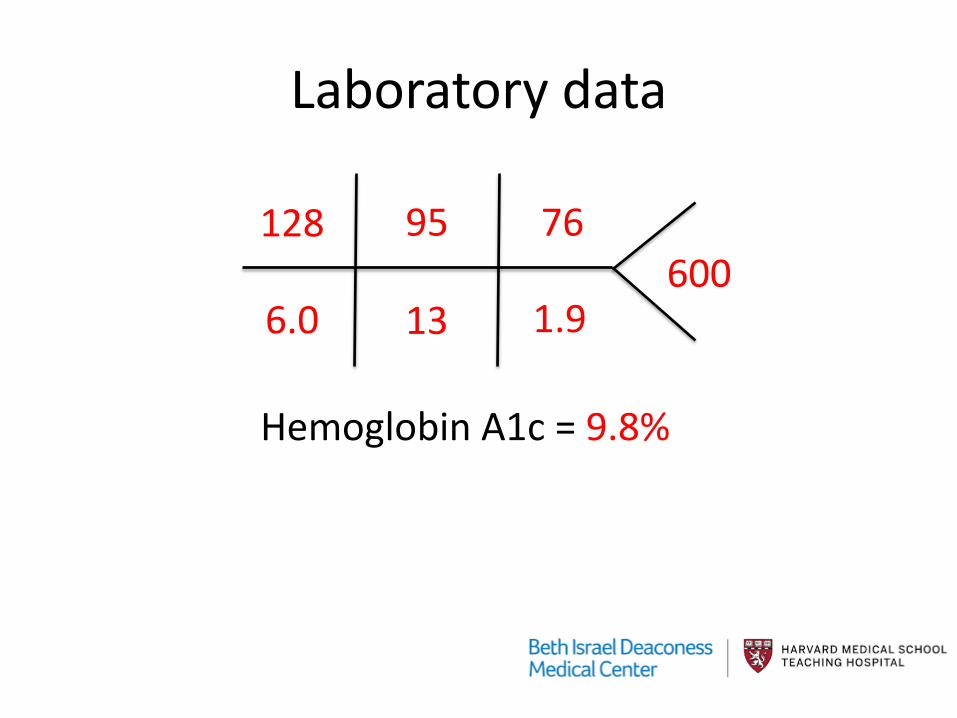
Laboratory data
128
6.0
95
13
76
1.9 600
Hemoglobin A1c = 9.8%

Acid-base balance
Which of the following is the most likely acid-base disturbance in this case? a) Anion-gap metabolic acidosis (AGMA) b) AGMA + respiratory alkalosis c) Non-anion gap metabolic acidosis d) Respiratory alkalosis with appropriate
metabolic compensation e) Not enough information; I need a blood gas
Acid-Base disturbances provide a physiologic basis for clinical events
• Asthmatic patient appears tired? Intubation? • Is the diarrhea significant enough to lead to
acidosis? • Why does my patient appear short of breath?
Is it due to normal compensation or abnormal physiology?
• Why is the anion gap so high? Intoxication or ingestion?
Determination of acid-base status requires a blood gas!
• Our patient’s ABG: – pH 7.22 – pCO2 21 – pO2 96
• HCO3
- 13

4-step approach to acid-base abnormalities
1) Acidemia or alkalemia (pH)? 2) What is the primary process – metabolic or
respiratory (pCO2)? 3) Is there a secondary process – appropriate or
inappropriate compensation (HCO3-)?
4) Calculate the anion gap. If there is one, is there another underlying metabolic process (the “Δ/Δ”)?

Practice makes better!
• Our patient’s ABG: – pH 7.22 – pCO2 21 – pO2 96
• Na+ 128, Cl- 95 • HCO3
- 13
Your findings:
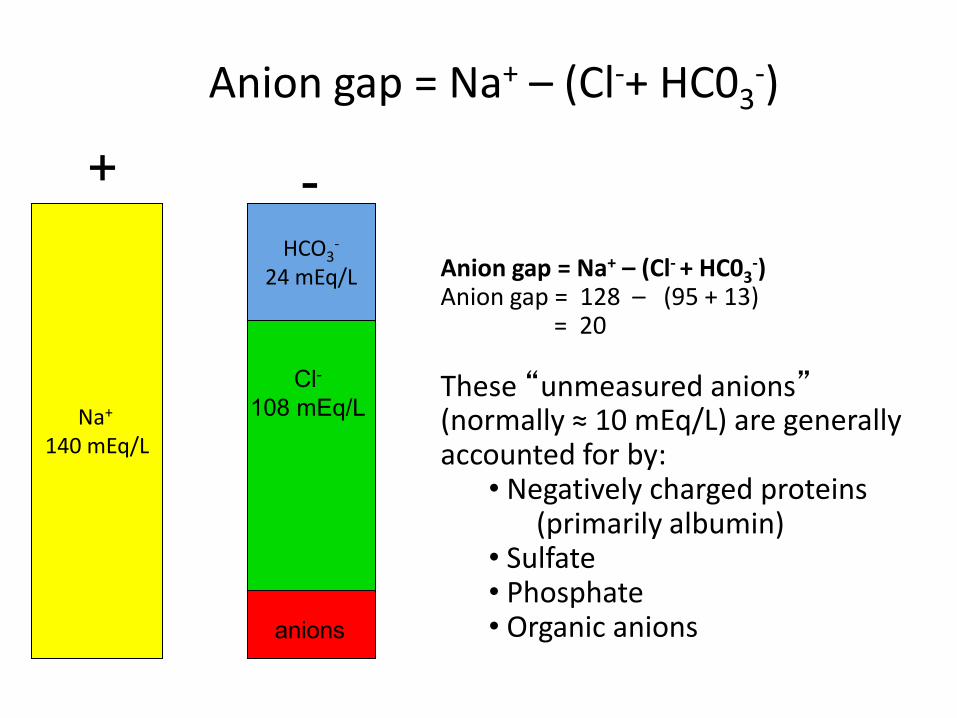
Anion gap = Na+ – (Cl-+ HC03-)
+ -
Na+
140 mEq/L
HCO3-
24 mEq/L
anions
Anion gap = Na+ – (Cl- + HC03
-) Anion gap = 128 – (95 + 13) = 20 These “unmeasured anions” (normally ≈ 10 mEq/L) are generally accounted for by:
• Negatively charged proteins (primarily albumin) • Sulfate • Phosphate • Organic anions
Cl- 108 mEq/L

Na+
Cl–
HCO3–
AG
Non gap (or normal gap or “hyperchloremic”) Metabolic Acidosis
Na+
Cl–
HCO3–
Anion Gap Metabolic Acidosis
Na+
Cl–
HCO3–
Classify metabolic acidosis by the presence or absence of an anion gap
Normal
Anion Gap acidoses
1. Ketoacidosis (starvation or diabetic) 2. Lactic Acidosis 3. Ingestion of toxins
– Methanol (windshield wiper fluid) – Ethylene glycol (antifreeze) – Salicylates (aspirin)
4. Severely reduced renal function

The “compensatory” response
• Appropriate respiratory compensation for a severe metabolic acidosis is a respiratory alkalosis.
• This respiratory response is NORMAL and PHYSIOLOGIC, helping the body to eliminate acid, but needs to be monitored just the same
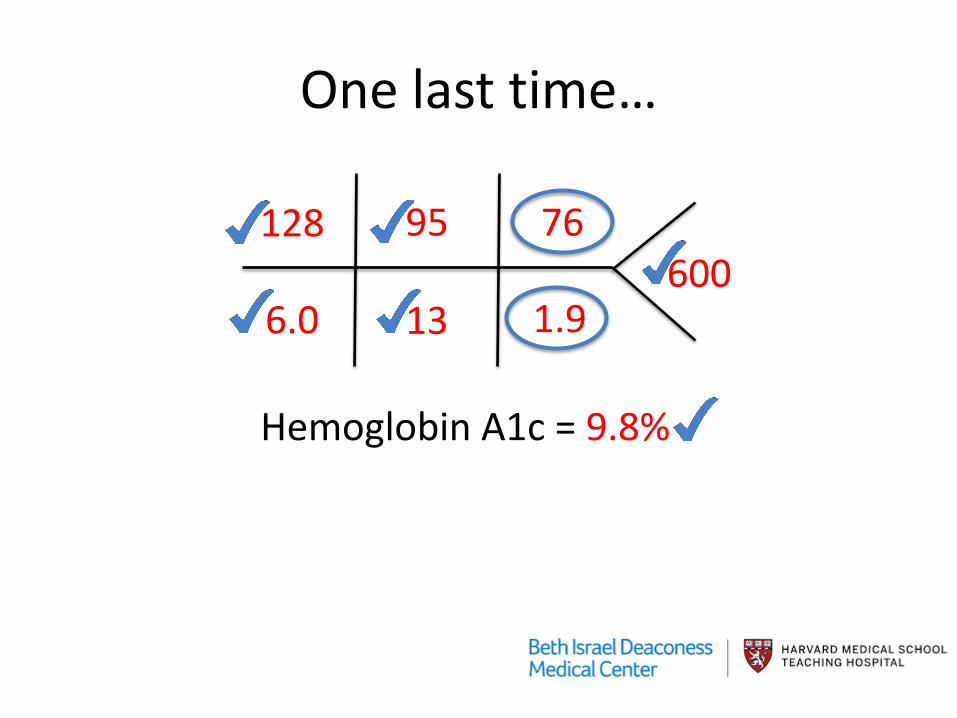
One last time…
128
6.0
95
13
76
1.9 600
Hemoglobin A1c = 9.8%
ACUTE KIDNEY INJURY
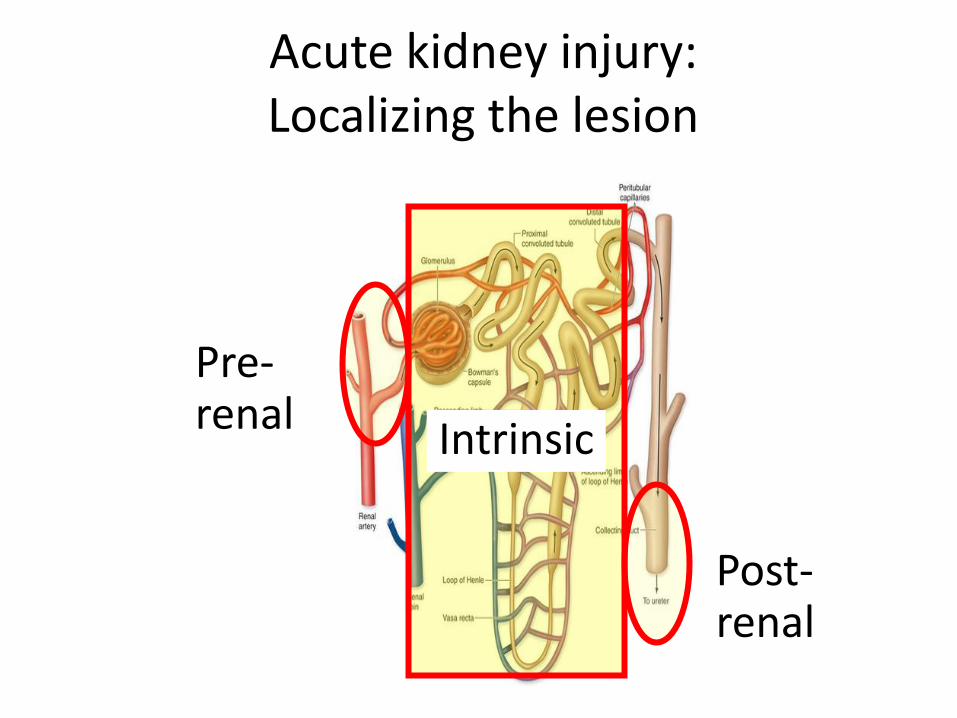
Pre-renal Intrinsic
Post-renal
Acute kidney injury: Localizing the lesion
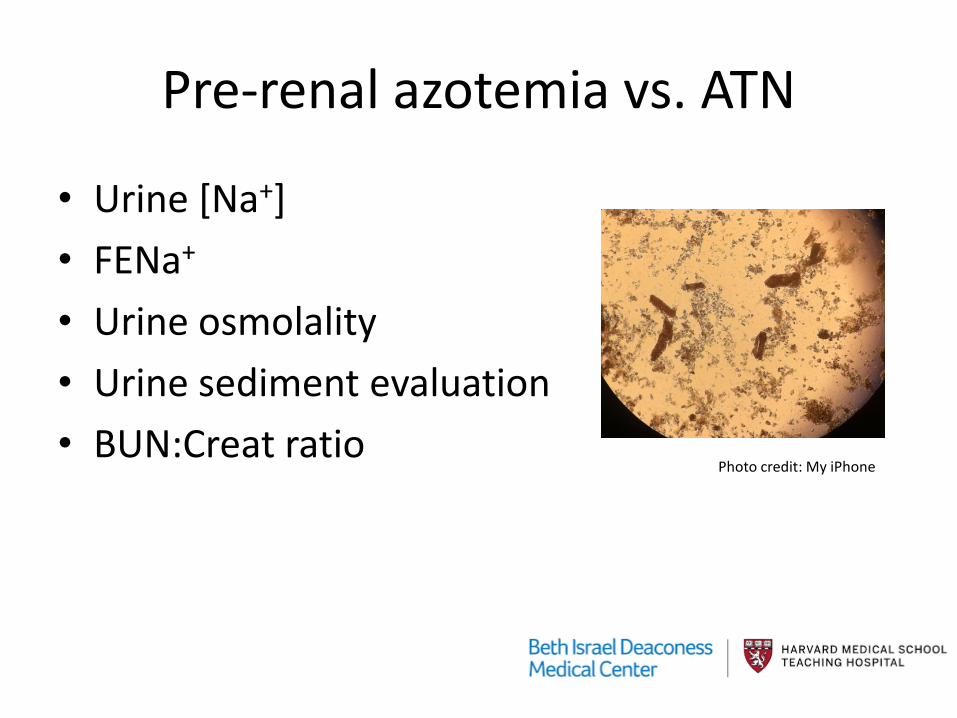
Pre-renal azotemia vs. ATN
• Urine [Na+] • FENa+ • Urine osmolality • Urine sediment evaluation • BUN:Creat ratio
Photo credit: My iPhone
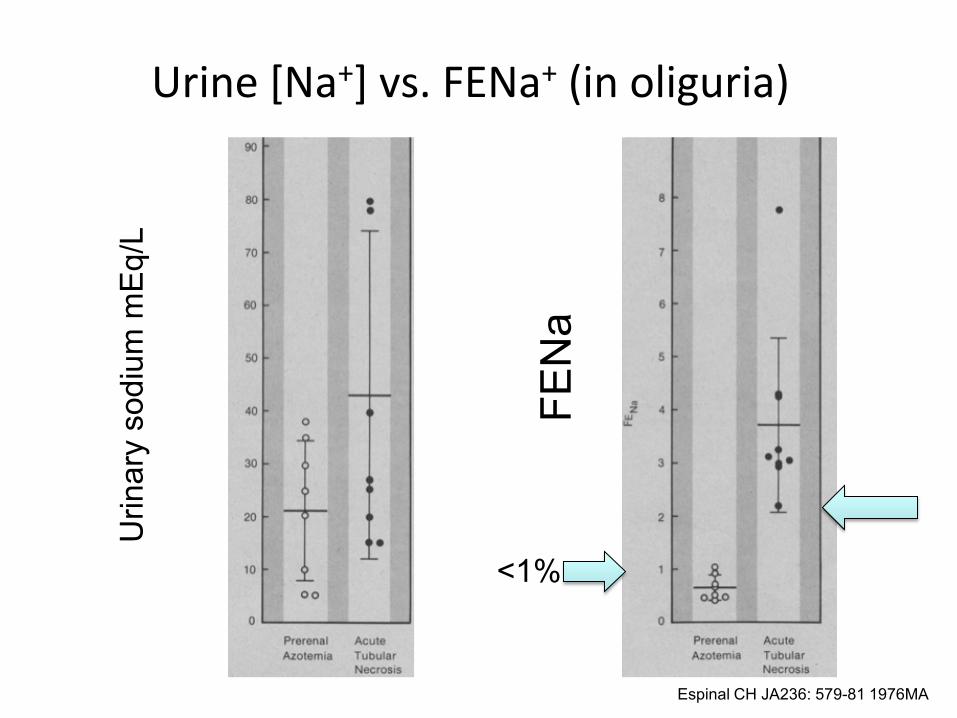
Espinal CH JA236: 579-81 1976MA
Urin
ary
sodi
um m
Eq/L
FEN
a <1%
Urine [Na+] vs. FENa+ (in oliguria)
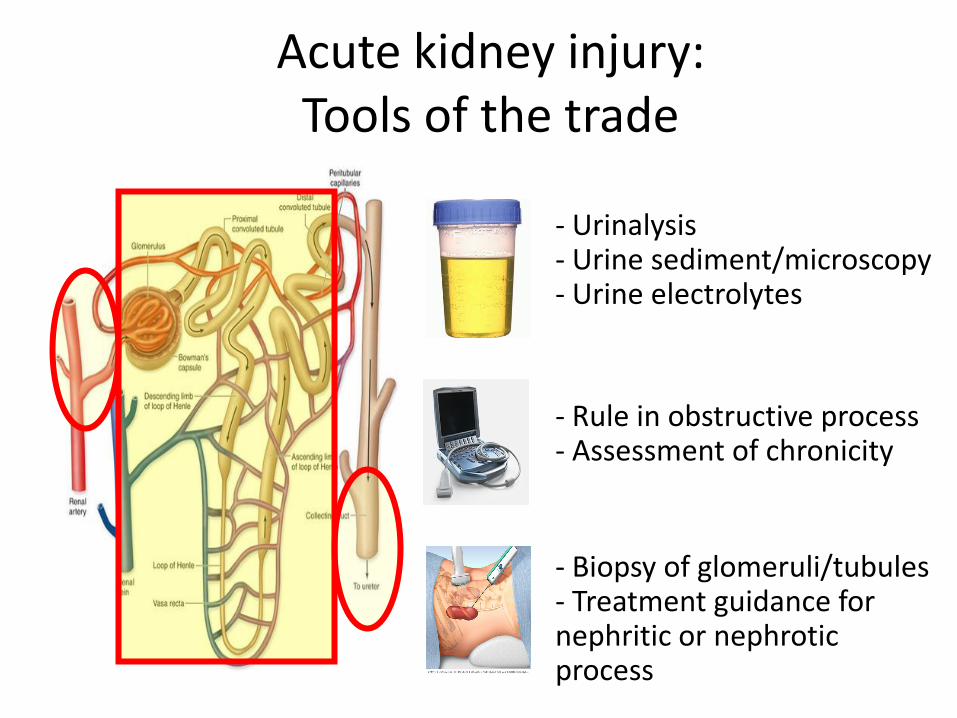
Acute kidney injury: Tools of the trade
- Urinalysis - Urine sediment/microscopy - Urine electrolytes
- Rule in obstructive process - Assessment of chronicity
- Biopsy of glomeruli/tubules - Treatment guidance for nephritic or nephrotic process

Today’s Case A 34-year-old woman presents to the clinic with diffuse abdominal and dysuria. She has a history of obesity, bipolar disorder, and hypertension. She is very thirsty. She has had some medication adherence issues in the past, but states that she has been better about remembering lately. Medications: hydrochlorothiazide 12.5mg daily, olmesartan 20mg daily, and oxcarbazepine (Trileptal)
128
6.0
95
13
76
1.9 600
Hemoglobin A1c = 9.8%
Vitals: T100.1°F, BP 80/40 mmHg, HR 120 bpm, RR 38 breaths/minute, BMI 37 kg/m2
General: Uncomfortable, breathing rapidly. HEENT: Mucous membranes were dry. CV: Tachycardic, normal S1 and S2, no murmurs, no S3/S4 Resp: Lungs are clear to auscultation and percussion. Abdomen: Distended and diffusely tender. Extremities: Trace lower extremity edema. Neuro: Somewhat inattentive, but conversant. No focal deficits
pH 7.22 pCO2 21 pO2 96
Key points – K+
• Potassium physiology dictates treatment – K+ intake – Cellular shift – Renal excretion: via distal Na+ delivery and
aldosterone – GI elimination: via non-reabsorbed binder
Key points – Na+
• Hyponatremia is a water (overload) problem! • Excess ADH can be physiologic (osmolar or
volume stimulus) or pathophysiologic (inappropriate release).
• Acute treatment may cause neurologic symptoms and requires close monitoring
• Chronic hyponatremia may contribute to falls and fractures.
• Management should address fluid and solute intake, as well as medications that affect concentrating ability.

Key points – Acid-Base
• Determination of acid-base disturbances informs clinical care
• Stepwise approach helps to uncover underlying processes
• Anion gap acidosis has a limited differential diagnosis – lactic acid, ketoacids, ingested acids, and severe renal failure

Key points – Acute kidney injury
• Localizing the “lesion” will guide treatment • The renal “tools of the trade”, including urine
evaluation, ultrasound, and biopsy, help us determine the site of injury
• Many objective, non-invasive tests can help us differentiate pre-renal etiologies from instrinic issues (i.e. ATN)

Next Best Steps
• Approach every electrolyte abnormality with physiology in mind to help guide your management.

Questions?