Embed Size (px)
DESCRIPTION
shock
Citation preview

Fluid management inpediatric shock
Rismala Dewi
Emergency and Pediatric Intensive Care DivisionFMUI-CMH

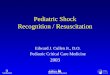
Pediatric Assessment Triangle
Circulation

Hemodynamics
MyocardialContractility
Stroke Volume Preload
Cardiac Output Afterload
Blood Pressure Heart Rate
Systemic Vascular Resistance
pediatric

Understanding some of physiologicaldifferences will help when working with a
critically ill child

Hypotension is a late
and premorbid sign

StrokeVolume
Afterload
Contractility
Preload
Heart Rate
Cardiac Output

A state in which there is inadequate
tissue perfusion to meet metabolic
demands
It is not LOW BLOOD PRESSURE !!!It is HYPOPERFUSION…..

Hypotension is a late
and premorbid sign

Stages of ShockCOMPENSATED
vital organ function is maintained, BP remainsnormal, tachycardia
UNCOMPENSATEDmicrovascular perfusion is compromised; significantreductions in effective circulating volume
IRREVERSIBLEinadequate perfusion of vital organs; irreparabledamage; death cannot be prevented
“Whatever the cause, the body responds in similar way”

The questions must be answered:
Does the child require emergent therapy?
What kind of fluid should be given?
How much fluid and what rate should fluid begiven initially and then in follow-up?

Management

Volumereplacement
Fluidreplacement
Fluidreplacement

Interstitial
Plasma
Transcellular
14% 5% 1%
Extracellular water20% body weight
Intracellular water40% body weight
Total body water = 60% body weightO
smol
ality
–m
Osm
/L
300
200
100
0
SHOCK

Fluid balance paradigm

Normal heart rate
Normal pulses
Capillary refill time < 2 seconds
Normal blood pressure
Warm extremities
Normal mental status
Urine output >1 mL/kg/hr

Whichfluid?

Cristalloid Colloid
Advantages
Extracellular space expanders
Lactare buffer
Limited plasma volume expansion
Maintain urinee output
Reduced plasma oncotic pressure
Cheap
Advantages
Good intravascular persistence
Reduced resuscicitation time
Moderate volume required
Enhancing microvascular flow
Minor risk of tissue oedem
Moderation of SIRS
Disadvantages
Poor plasma volume support
Reduce plasma COP
Large quantities needed
Risk of overhydration
Risk of hyponatremia
Disadvantages
Risk of volume overload
Adverse effect on haemostasis
Tissue accumulation
Adverse effect on renal function
Risk of anaphylaxis
More expensive

Initial fluid resuscitation with crystalloidminimal 20 mL/Kg in children
Consider addition of albumin in patientrequiring substantial amounts of crystalloid
to maintain adequate MAP
Goaldirected
(targeted)


Don’t give too much Fluid!!
Hepatomegaly
Rales
Increased WOB
↑Jugular venous pressure
Chest X-ray
USCOM
Echocardiography
Fluid responsiveness

Problem to be concern
Metabolicacidosis
Volumeoverload
Electrolyteimbalance
CoagulopathyFluid shiftand raised
ICP

Maintenance fluid

Choong, K et al. Arch Dis Child 2006;91:828-835
Meta- analysis iv fluids in children:-hypotonic vs. isotonic-
Isotonic solutions Hyponatremia

Stablehemodynamic?
Volumeresponsive?
Continue volumereplacement
Cold extremities?
Y
N
NYMonitor
INOTROPIC VASOPRESSOR

Conclusion
Recognize compensated shock quickly-havea high index of suspicion, remembertachycardia is first sign and hypotension islate and ominousAssessment , management of fluid balanceand prescription of appropriate fluidconstitute some of challenges for clinician





![[PPT]Pediatric Shock - School of Medicine - LSU Health New …medschool.lsuhsc.edu/emergency_medicine/docs/Shock States... · Web viewPediatric Shock Recognition, Classification and](https://img.pdfslide.net/doc/110x75/5af6b2147f8b9a8d1c8f3686/pptpediatric-shock-school-of-medicine-lsu-health-new-statesweb-viewpediatric.jpg)