Embed Size (px)
Citation preview

Fluid Therapy in SmallRuminants and Camelids
Meredyth Jones, DVM, MSa,*, Christine Navarre, DVM, MSb
KEYWORDS
� Fluid therapy � Sheep � Goat � Llama � Alpaca � Crystalloid � Colloid� Parenteral nutrition
KEY POINTS
� Animals estimated to be more than 8% dehydrated should receive intravenous resuscita-tion at least initially, and then may be maintained on intravenous or oral fluid therapy.
� Hypoglycemia, hyperkalemia, and acidosis are the most life-threatening abnormalities,and require most immediate correction.
� Crystalloid solutions should be used cautiously in animals with hypoproteinemia becauseof the risk of pulmonary edema. Synthetic or natural colloid solutions are preferred in thesepatients.
� Hypertonic solutions are useful for short-term improvement of cardiac output, drawingwater from the interstitium into the vasculature; they are contraindicated in hyperosmolarsyndromes such as carbohydrate overload.
� Dextrose-containing solutions are indicated for use in hypoglycemic animals or those withhepatic lipidosis syndromes, but must be administered judiciously to achieve energy sup-plementation without inducing glucose diuresis. Insulin may be indicated to improveglucose utilization.
� Parenteral nutrition is indicated in patients with anorexia, those with severe systemic dis-ease, and those with evidence of protein loss, and should be initiated early in the thera-peutic period to achieve maximum efficacy.
INTRODUCTION
Body water, electrolytes, and acid-base balance are important considerations in theevaluation and treatment of animals with any disease process, with restoration ofthese a priority as adjunctive therapy. The goals of fluid therapy should be to maintaincardiac output and tissue perfusion, and to correct acid-base and electrolyteabnormalities.
The authors have no disclosures.a Food Animal Field Services, Department of Large Animal Clinical Sciences, College of Veter-inary Medicine, Texas A&M University, 4475 TAMU, College Station, TX 77843, USA; b LSUAgCenter, 105 Francioni Hall–LSU, Baton Rouge, LA 70803-4210, USA* Corresponding author.E-mail address: [email protected]
Vet Clin Food Anim 30 (2014) 441–453http://dx.doi.org/10.1016/j.cvfa.2014.04.006 vetfood.theclinics.com0749-0720/14/$ – see front matter � 2014 Elsevier Inc. All rights reserved.

Jones & Navarre442
PATIENT EVALUATION
A thorough physical examination is an important component of the evaluation of anypatient, aiding in the diagnosis of the primary disease condition and the extent towhich fluid and electrolyte therapy is indicated.
Hydration Deficit
Hydration deficit is best determined by reduction in body weight from the normally hy-dratedstate, but thisbaselinebodyweight is infrequentlyavailablewhen thedehydratedpatient is evaluated. Mental state, skin turgor, color and texture of mucous membrane,temperature of the extremities, and recession of the globe are all used in combination toestimate hydration status, but these criteria have not been validated in ruminants orcamelids (Table 1). Alterations in packed cell volume (PCV) and total plasma protein(TPP) may also be used as indicators of hydration status, but are limited in their utility.The reference interval for PCV is fairly wide, making it an insensitive indicator of hydra-tion, and baseline values for an individual are rarely available. Moreover, owing to theprevalence of diseases in sheep, goats, and camelids that alter PCV and TPP (internalparasitism, failure of passive transfer, chronic inflammatory disease), these valuesmustbe interpreted in light of the history and physical examination findings.
Electrolyte and Acid-Base Alterations
Serum biochemistry and blood gas analysis are the most appropriate tools for assess-ment of electrolyte, glucose, and acid-base abnormalities. Results of this testing mayhelp prioritize fluid components for replacement. In general, hypoglycemia, hyperka-lemia, and acidosis represent abnormalities that are most life-threatening and requirethe most immediate correction.
Fluid Administration
RouteThe first decision to be made when initiating fluid therapy is whether fluids should beadministered parenterally or enterally. In ruminants and camelids, large volumes offluids may be administered into the rumen or first compartment, allowing for effectivetreatment of mild to moderate dehydration. In camelids specifically, the benefit ofrepeated oral fluid therapy should be weighed against the risks. Oral intubation isstressful in camelids and may induce cortisol-mediated lipolysis, particularly ifrepeated.1 Therefore, the authors rarely use oral fluid therapy in camelids. In general,the animals most likely to benefit from oral fluid therapy are those that are mentallyalert, have good gastrointestinal motility, and are less than 8% dehydrated. Animals
Table 1Physical examination parameters for estimation of hydration deficit in ruminants andcamelids
Mild, 4%–6% Moderate, 7%–9% Severe, >10%
Cervical skin tent 4–5 s 5–7 s >7 s
Globe recession 2–3 mm 3–4 mm 6–8 mm
Oral mucosa Moist, warm, pink Tacky, warm, pale Dry, cool, pale
Extremities Warm Cool Cold
Demeanor Standing, bright Sternal, slow Lateral, depressed
Adapted fromConstable PD,Walker PG,MorinDE, et al. Clinical and laboratory assessmentof hydra-tion status of neonatal calves with diarrhea. J Am Vet Med Assoc 1998;212:991–6; and Roussel AJ.Fluid therapy in mature cattle. Vet Clin N Am Food Anim Pract 1990;6(1):111–23.

Fluid Therapy in Small Ruminants and Camelids 443
not meeting these criteria are best managed with at least initial parenteral fluid resus-citation and correction of acid-base and electrolyte abnormalities.In small ruminants, jugular catheterization is the most practical means of admin-
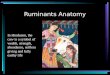
istering intravenous fluid therapy. In sheep and goats, over-the-needle cathetersare typically used and placed with relative ease. In camelids, placement of jugularcatheters can be more challenging and, although over-the-needle catheters areacceptable, peel-away catheters (Fig. 1) or J-wire catheters may result in easierand more reliable placement. A stab incision made with a #15 scalpel blade helpsfacilitate the placement of over-the-needle catheters in these species, particularlycamelids. Recommended catheter sizes for jugular catheterization are summarizedin Table 2.
Volume and rateWhen determining appropriate fluid volume and rate to be administered, one mustconsider:
� Replacement of hydration deficit� Maintenance fluid needs� Replacement of ongoing losses� Plasma protein concentration
Replacement of hydration deficit The volume required for hydration replacement iscalculated using the following formula:
(estimated%dehydration)� (bodyweight in kg)5 litersof fluidneeded to replacedeficit
As a general rule, hydration replacement should occur over approximately 4 hours,with maintenance and ongoing losses administered over the remaining hours in theday. In animals with low total protein and in camelids, hydration replacement mayneed to be slower, with half of the volume replaced in 4 to 6 hours and the remaindergiven over 12 to 24 hours.
Maintenance fluid requirement Maintenance fluid requirements account for normalwater losses attributable to urination, defecation, respiration, sweat, and other
Fig. 1. Placement of a peel-away catheter. A sheath is placed into the jugular vein, as in anover-the-needle catheter setup, and the needle is removed. The long, soft catheter is fedinto the sheath, which is then peeled into two halves and out of the vein, leaving the cath-eter in place.

Table 2Recommended catheter sizes for jugular catheterization
Patient Adult Sheep, Goat Kid, Lamb Adult Llama, Alpaca Cria
Catheter size 16 gauge 18 gauge 14–16 gauge 16–18 gauge3.2500 (8.3 cm) 200 (5.1 cm) 3.25–5.500 (8.3–14 cm) 2–3.500 (5.1–8.9 cm)
Jones & Navarre444
evaporation, and differ based on physiologic status (lactation, pregnancy) and age.Neonates have higher total body water volume than adults, and require a higher main-tenance fluid volume.Maintenance fluid needs can be estimated using the following general guidelines:
� Adults: 50 mL/kg/24 hours or 1 mL/lb/h� Neonates: 70 to 80 mL/kg/24 h or 2 mL/lb/h
These numbers are typically used in all species and are supported by establishedwater requirements of goats, which range from 30 to 66.6 mL/kg/d with a mean of44.8 mL/kg/d.2 Neonates are typically assigned a higher maintenance volume, with70 mL/kg found to be acceptable in calves.3
If fluid rates are difficult to control or are in animals likely to disrupt the fluid line,replacement fluids may be divided and administered every 3 hours by calculatingthe total volume needed for a 3-hour period and providing this as a single bolus.This approach is not appropriate with solutions that contain greater than 2% dextroseor with parenteral nutrition (PN) solutions.
Ongoing losses Ongoing losses include fluid, protein, and electrolytes, which are lostas a result of a continuing disease process, such as diarrhea or internal or external lossof fluid. Quantifying ongoing losses can be challenging and, in the absence of the abil-ity to measure these directly, parameters such as PCV, TPP, serum electrolyte panel,and body weight may be used to monitor the success of fluid therapy to sustain bodyfluid, protein, and electrolyte balance.
FLUID TYPE
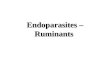
The 4 basic types of solutions used in clinical practice, which vary in composition,cost, and usefulness depending on the pathologic processes, are crystalloid solu-tions, colloid solutions, PN, and blood products. The article by Balcomb and Fosterelsewhere in this issue addresses the use of whole blood and blood products. A sum-mary algorithm to assist in fluid selection is provided in Fig. 2.
Crystalloid Solutions
Crystalloid solutions represent the most common fluids used in veterinary practice,and contain water, electrolytes (particularly sodium), and/or dextrose. Crystalloidsmay be classified as balanced, resembling the composition of the extracellular fluid,or unbalanced, designed to replace specific components.Examples of crystalloid solutions used in veterinary practice include:
� Isotonic solutions
� Balanced solutions- Polyionic solutions (Ringer’s solutions; Normosol [Hospira, Lake Forest, IL];Plasma-Lyte [Baxter, Deerfield, IL])
� Unbalanced solutions- 0.9% NaCl solution

Fig. 2. Suggested fluid compositions for various clinical and metabolic conditions in small ruminants and camelids.
Fluid
Therapyin
SmallRuminants
andCamelid
s445

Jones & Navarre446
- 1.3% NaHCO3 solution- 5% dextrose solution
The isotonic crystalloids have an osmolality similar to that of plasma and equilibraterapidly with the interstitial fluid. Only 20% to 25% of the infused volume of the admin-istered solution remains in the intravascular space 1 hour after infusion. For thisreason, crystalloids are well suited for rehydration of body tissues and restoration ofelectrolyte and acid-base abnormalities, but are not ideal for long-term maintenanceof cardiac output. This characteristic of crystalloid solutions must also be consideredwhen treating patients with hypoproteinemia, a common condition in small ruminantsand camelids. Proteins serve to retain fluid within the vasculature, and the use of crys-talloids in hypoproteinemic patients is associated with the development of edema and,of particular concern, pulmonary edema.
Hypertonic Solutions
Hypertonic solutions have a higher osmolality relative to plasma, the most common ofwhich is hypertonic saline (7.2%NaCl), which has been used successfully in the resus-citation of sheep after hemorrhage.4 These solutions are contraindicated in hyperos-molar conditions, which may occur in ill camelids and with camelids with grainoverload. Hypertonic solutions are reviewed in the article by Smith and Berchtold else-where in this issue.
Hypotonic Solutions
Hypotonic solutions are rarely used in veterinary medicine. Although there are somespecific conditions for which they have value, these are not common, and rapidadministration of solutions that are hypotonic relative to a patient’s serum can causedevelopment of cerebral edema and lysis of brain cells.
Acidifying Solutions
Saline and Ringer’s solution are acidifying solutions that are appropriate as a solesolution or as a base solution for animals presenting with metabolic alkalosis, asmay occur with gastrointestinal obstruction or stasis and anorexia. Because of itshigh sodium content, saline is also useful for correcting hyponatremia, as occurswith obstructive urolithiasis and ruptured urinary bladder. Alkalotic ruminants arefrequently anorexic, resulting in hypokalemia, and supplementation of these basesolutions with 10 to 40 mEq/L of potassium chloride is frequently indicated.
Alkalinizing Solutions
Metabolic acidosis is encountered in patients with carbohydrate overload, diarrheafrom enteritis, pregnancy toxemia, and a few other conditions. Isotonic sodium bicar-bonate (1.3% NaHCO3) and hypertonic sodium bicarbonate (5% or 8.4% NaHCO3)may be used alone or be added to other solutions to directly correct metabolicacidosis. To determine the bicarbonate replacement needed for a patient, thefollowing equations may be used:
Neonates: mEq bicarbonate needed 5 base deficit � body weight in kg � 0.6
Adults: mEq bicarbonate needed 5 base deficit � body weight in kg � 0.3
For these formulas, the base deficit may be directly obtained from a blood gas anal-ysis, or estimated by subtracting the patient’s serum total CO2 (or plasma bicarbonate)

Fluid Therapy in Small Ruminants and Camelids 447
from the normal serum total CO2 value of 24 mEq/mL. The constants 0.6 and 0.3represent the approximate proportion of extracellular fluid volume relative to totalbody weight, which is different for neonates compared with mature animals. Fromthis formula, the total milliequivalents of bicarbonate needed to completely correctthe acidosis can be calculated. Intravenous administration of 1.3% NaHCO3 isfrequently used for this replacement, and contains approximately 156 mEq bicarbon-ate/L. The hypertonic 5.0% NaHCO3 contains 0.6 mEq/mL of sodium bicarbonate,whereas 8.4% NaHCO3 contains 1 mEq/mL. Isotonic 1.3% NaHCO3 solution maybe formulated by beginning with 260 mL of 5% NaHCO3 or 156 mL of 8.4% NaHCO3
and adding a sufficient quantity of sterile water to make 1 L. Hypertonic NaHCO3 so-lutions should be used with caution until proved to be safe for camelids. Recently, hy-pertonic NaHCO3 solutions have been shown to be effective in treating D-lactateacidosis in calves.5
In some cases, such as neonatal diarrhea and severe grain overload, the entirecalculated deficit of bicarbonate may need to be administered to correct the acidosis,but in most cases partial correction by administration of about half of the deficit over 2to 4 hours will be followed by complete correction, after fluid resuscitation allows thenormal physiologic compensatory mechanisms to function in the treated animal.Solutions including lactated Ringer’s, Normosol-R (Hospira), and Plasma-Lyte A
(Baxter) are also considered alkalinizing fluids, owing to the presence of themetaboliz-able bases lactate, acetate, or gluconate. These bases are metabolized by various tis-sues, depending on the metabolizable base, resulting in a net increase in the strongion difference that corrects the metabolic acidosis. However, the alkalinizing effectwill be delayed relative to the administration of NaHCO3 solution, owing to the timerequired for metabolism. When using a product containing lactate, it is important toremember that only the L-lactate isomer is metabolized to bicarbonate even thoughthe solution contains equal parts of the D- and L-isomers. When perfusion of the liveris altered, the D-isomer will not be metabolized efficiently and may exacerbate lacticacidosis. Combined with the delayed alkalization potential of the metabolizable basesrelative to bicarbonate, this makes these solutions less desirable for resuscitation of amoderate to severe metabolic acidosis.A D-lactic acidosis syndrome of lambs has been described, resulting in severe meta-
bolic acidosis6 believed to result from increased substrate presentation to the large in-testine. A similar syndrome has been described in goat kids.7 These syndromes havebeen successfully corrected through the oral administration of 50 mmol HCO3 admin-istered as 50 mL 8.4%NaHCO3 solution,
8 or intravenous administration of 5% sodiumbicarbonate, along with oral supplementation, based on measured base deficit.7
Dextrose Solutions
Dextrose-containing solutions without electrolytes have a relatively narrow spectrumof utility because of the rapid metabolism of the dextrose component, leaving free wa-ter to dilute other blood components. These solutions are useful in the treatment of hy-poglycemia in neonates, particularly if hypothermic, and in animals with pregnancytoxemia. Fifty percent dextrose is commercially available and may be administeredundiluted at 1 mL/10 lb (4.5 kg) body weight during hypoglycemic crisis, or addedto sterile water to make 10% dextrose (200 mL/L) and 5% isotonic dextrose(100 mL/L), which may be used alone or in combination with other fluids. Fifty percentdextrose may also be added to polyionic solutions to make 1% to 2.5% solutions (20–50 mL/L) to provide a source of energy.Pregnancy toxemia is a common indication for the use of dextrose-containing solu-
tions over a period of time. In sheep and goats, a variety of metabolic derangements

Jones & Navarre448
have been documented as part of the pregnancy toxemia, including hyperketonemia,ketonuria, metabolic acidosis, hypocalcemia, hypoglycemia, and decreased liverfunction from hepatic lipidosis.9 Hypoglycemia is an inconsistent finding in cases ofpregnancy toxemia, and a finding of euglycemia or hyperglycemia should notdissuade one from considering pregnancy toxemia as a differential diagnosis.Oral fluid therapy may be used to prevent the progression of very early pregnancy
toxemia, and is frequently initiated by producers at the farm. In cases where the animalis recumbent or prefers to be recumbent, oral therapy should not be expected to haltor reverse the progression of pregnancy toxemia. Intravenous therapy is nearly alwaysindicated in these cases, and should not be postponed.Polyionic, balanced solutions containing dextrose are typically used as the basis for
therapy for pregnancy toxemia; however, additional components such as calcium glu-conate 23% (20–50 mL/L), NaHCO3 (calculated from base deficit), and potassium (20–40 mEq/L) may be added to the base solution. Solutions should not be formulated tocontain both calcium and bicarbonate ions because these 2 ions may form an insol-uble precipitate. Glucose is usually provided to small ruminants and camelids as2.5% dextrose in a polyionic solution or 5% dextrose in polyionic solution or water.The rate and concentration of dextrose should be adjusted in response to changesin the concentrations of glucose and ketones in the urine. The goal is to provideenough energy to reduce or eliminate ketone production yet not exceed the renalthreshold for glucose, which will result in diuresis. Although the goal of negative resultsfor both urine glucose and ketones is seldom achieved, monitoring urinary ketonesand glucose is a sensitive and inexpensive method by which to evaluate the successof energy supplementation in these cases.A major goal of therapy is to reestablish the appetite of the patient. Dextrose-
containing fluids are not a replacement for enteral nutrition, as 5% dextrose given atmaintenance rate provides only 25% of maintenance energy requirement whilemeeting none of the protein or other nutritional requirements of a late-gestation ani-mal. At least partial PN (PPN) is indicated for many animals with pregnancy toxemia.Prolonged or repeated administration of dextrose-containing solutions may be asso-ciated with hypophosphatemia and subsequent recumbency, especially in anorexicanimals.10
Dextrose-containing solutions should be used with caution in camelid species.Camelids have been shown to produce less insulin and to have decreased insulinsensitivity in comparison with other species.11 When dextrose-containing fluids areused, the dextrose concentration should be low (usually 2.5% or lower) and bloodglucose should be monitored, and exogenous insulin administration may be requiredduring therapy. An exception to this is animals that are anorexic or experiencing he-patic lipidosis. In these cases, dextrose therapy and PN are indicated to reduce theprogression of lipolysis, which leads to further depression of appetite and worseningof the condition. Insulin therapy is indicated for blood glucose concentrationsexceeding 350 to 400 mg/dL, and the following doses are provided as starting pointsfor subcutaneous therapy: regular insulin 0.25 U/kg, Ultralente 0.2 to 0.4 U/kg, Lente0.25 to 0.5 U/kg.A hyperosmolar syndrome has been described in ill neonatal camelids,12,13 charac-
terized by hyperglycemia, hypernatremia, and hyperosmolarity, which manifests as afine head tremor, ataxia, and base-wide stance. Insulin resistance and glucosediuresis are believed to be among the contributors to this syndrome; therefore, solu-tions containing high concentrations of sodium and dextrose are typically avoided inneonatal camelids. Insulin therapy is indicated for this syndrome, with constant-rateregular insulin infusion advocated at an initial rate 0.02 U/kg/h.13

Fluid Therapy in Small Ruminants and Camelids 449
Colloidal Solutions
Colloidal solutions contain high molecular weight compounds that are retained in theintravascular space and serve to maintain or increase intravascular volume in animalswith hypoproteinemia. These molecules act similarly to albumin by maintaining os-motic pressure within the vascular system. In fact, on a weight to weight basis, 6%dextran 70 is actually 2.5 times more osmotically active than albumin.4
Colloidal solutions may be divided into natural and synthetic compounds.
� Natural colloid solutions
� Whole blood� Plasma� Synthetic colloid solutions� Hetastarch� Dextrans� Modified gelatin solutions
Despite their higher cost, colloids are more appropriate than crystalloids for use inhypoproteinemic patients and those requiring longer-term stabilization of cardiacoutput. In one study of induced hemorrhage and resuscitation in sheep, the additionof 6% dextran 70 to 7.2% NaCl resulted in maintenance of a significantly higher car-diac output in comparison with other hypertonic solutions by redistribution of intersti-tial fluid into the vasculature.4
The use of hetastarch has been evaluated in healthy llamas.14 Administration of50 mL/kg hetastarch over 60 minutes to healthy llamas resulted in hemodilution, asindicated by significant decreases in hematocrit, hemoglobin, total serum protein,and albumin concentrations, indicating the ability of hetastarch to expand plasma vol-ume. These effects were greater than those observed after administration of lactatedRinger’s solution. Hetastarch also significantly increased plasma colloid osmotic pres-sure for 96 hours after infusion.
Orally Administered Solutions
Oral fluid therapy represents an economical and effective means for replacing mild tomoderate fluid and electrolyte deficits. In addition, oral therapy is indicated in cases ofsevere hypokalemia and hypophosphatemia, where intravenous administrationcarries a greater risk for complications and is frequently less effective than oraltherapy.To achieve effective absorption of water, oral fluids must contain sufficient sodium
to facilitate transport across the intestinal mucosa. Ideally oral solutions shouldcontain at least 90 mmol/L of sodium. Ruminants with anorexia and gastrointestinalstasis frequently have low concentrations of plasma potassium and chloride, makingit important that oral replacement solutions contain extraphysiologic concentrations ofthese electrolytes.
� Oral electrolyte solution for adult ruminants (per liter of water)
� 7 g NaCl� 1.5 g KCl� 1 g CaCl2Table 3 lists common conversions for salts used in oral fluids.Severe hypophosphatemia may be encountered in animals with prolonged anorexia
or parasitism. Phosphate is the bioactive form of phosphorus, making phosphite saltforms found in commercially available intravenous solutions inadequate for

Table 3Conversion of grams of listed feed-grade salt per teaspoon (g/t)
Salt g/t
NaCl 6.1
KCl 6
NaHCO3 5
CaCl2 4
Jones & Navarre450
phosphorus replacement. Phosphate salts may be found in commercially availablephosphate enemas, but must be carefully diluted for intravenous use, and intravenousadministration is associated with an inadequate duration of the increase in serumphosphorus in cattle.15 Oral supplementation of phosphorus is preferable and, in al-pacas, the administration of 1 to 2 (4.5 oz/13 mL each) monobasic/dibasic sodiumphosphate enemas in oral fluids by one of the authors (M.J.) has resulted in increasesin serum phosphorus level of 2 to 3 mg/dL.
PARENTERAL NUTRITION
PN is an effective means for providing nutrients to anorectic or hypophagic animalsthat warrant aggressive therapy. PN can be costly, requires careful monitoring, andshould be initiated early in the course of treatment to maximize its efficacy. Indicationsfor PN include anorexia for longer than 3 days, severe systemic disease, and evidenceof protein loss. Total PN (TPN) is designed to meet all of an animal’s nutritional needs,with base components of dextrose, amino acids, and lipids. PPN is limited in either thecomponents it provides or the amount of components relative to the animal’s needs.The cost of TPN precludes its use in many cases, but PPN formulations exist to pro-vide valuable nutrients for maintenance and repair at a reasonable cost. The lipidcomponent is the most costly, and is typically the component omitted when formu-lating PPN.A retrospective study was performed evaluating PN in alpacas suffering from
gastrointestinal disease, liver disease, neoplasia, and other conditions.16 Twenty of22 animals had severe metabolic derangements before therapy, and at least 1 compli-cation from PN occurred in 21 of 22 animals, including hyperglycemia, lipemia, hypo-kalemia, and refeeding syndrome. Overall survival rate to discharge was 45% and wasunrelated to diagnosis, although the study population was small.
� PPN solution for sheep and goats
� 5 L commercial balanced electrolyte solution� 500 mL 50% dextrose� 1 L 8.5% amino acids (commercially available preparation)� 20 mL B-complex vitamins� Potassium chloride (20–40 mEq/L) and calcium gluconate 23% (20–50 mL/L)as indicatedThis solution has been used by one of the authors (C.N.) in adult sheep, goats,and camelids. It is administered at a rate of 5% of body weight per day, andmay be administered without the use of a fluid pump.� PPN for camelids� Clore and colleagues,16 2011
- Amino acid to provide 4 to 6 g/100 kcal protein- 50% dextrose to provide 40% to 60% of nonprotein calories- 20% lipid to provide remaining 40% to 60% of nonprotein calories

Box
Gen
Initi
Thelipid
A la
A sesho
Whhypwei
Dail
Thecom
Vita
Bloo
The
Bod
Asseplas
Asseadd
Cess
If inof P
Wh
Fluid Therapy in Small Ruminants and Camelids 451
- Additional B vitamins with or without trace minerals- OR- Commercial dextrose/amino acid solution to provide 4.25 g/100 kcal protein
plus 100% nonprotein calories from dextrose- Calcium gluconate, trace minerals, magnesium sulfate, and B complex
added as indicated by intake and serum biochemistryThese protocols were compounded and used at 2 academic institutions fora variety of disease conditions in alpacas along with other specific and sup-portive therapies.
� Van Saun and colleagues,1 2000- 880 mL of 50% dextrose- 2000 mL of 8.5% amino acids- 100 mL of 23% calcium gluconate- 5 mL vitamin B complex- 30 mL potassium chloride (4 mEq/mL)- Sufficient quantity to 4 L in a base solution of lactated Ringer’s solution- Administered at a rate of 2.5 mL/kg/h- 30 U NPH insulin (animal weighed 102 kg) was administered subcutaneously
every 12hours initially and thenwhenever bloodglucose exceeded400mg/dLThis protocol was used in an adult female llama with hepatic lipidosis for
1
eral guidelines for administration of parenteral nutrition (PN)
ation
components should be mixed aseptically, with amino acids added first, followed by anycomponent, then dextrose
rge-gauge, long catheter is preferable and must be aseptically placed
parate catheter should be placed if other drugs are to be administered, or the PN catheteruld be flushed well before and after drug administration
en PN is initiated, it should be at 25% to 50% of target rate for a few hours. Iferglycemia does not develop, the rate is increased to the target rate, usually 5% of bodyght daily
y
catheter should be examined 3 to 4 times per day for evidence of phlebitis or otherplications
l parameters should be monitored every 8 hours
d glucose may need to be monitored every 6 to 8 hours
PN solution and all lines should be changed daily
y weight should be monitored daily
ssment of packed cell volume and total plasma protein should be performed daily, and thema evaluated visually for evidence of lipemia
ssment of serum electrolytes, creatinine, and liver enzymes should be performed daily, inition to urinalysis
ation
sulin is administered with PN, insulin therapy should be stopped 24 hours before cessationN
en PN is discontinued, it should be decreased slowly over 24 to 48 hours

Jones & Navarre452
1 week, and PNwas gradually discontinued over 3 days once the clinical con-dition had stabilized and the animal was eating.
The metabolism of carbohydrates and lipids by camelids is complex and compli-cated.11,17 Therefore, PNsolutions for camelids are sometimes formulatedwith ahigherratio of aminoacids to nonprotein sourcesof energy in comparisonwithPNsolutions forother species. Closemonitoring for hyperlipemia and the need for insulin administrationis critical. General guidelines for administration of PN are shown in Box 1.Refeeding syndrome, an important potential complication in the initial days of recov-
ery from starvation or treatment with PN,16,18 is characterized by hypophosphatemia,hypokalemia, hypomagnesemia, and other electrolyte and metabolic abnormalities,with severe effects on most body systems. Patients at risk for refeeding syndromeshould undergo gradual refeeding or PN administration, be monitored closely for itsdevelopment, and be supplemented with target electrolytes and minerals.
REFERENCES
1. Van Saun RJ, Callihan BR, Tornquist SJ. Nutritional support for treatment of hepat-ic lipidosis in a llama. J Am Vet Med Assoc 2000;217(10):1531–5.
2. Nutrient requirements of small ruminants: sheep, goats, cervids, and New Worldcamelids. Washington, DC: The National Academies Press; 2007.
3. Gottardo F, Mattiello S, Cozzi G, et al. The provision of drinking water to vealcalves for welfare purposes. J Anim Sci 2002;80(9):2362–72.
4. Smith J, Kramer GC, Perron P, et al. A comparison of several hypertonic solutionsfor resuscitation in bled sheep. J Surg Res 1985;39:517–28.
5. Lorenz I, Vogt S. Investigations on the association of D-lactate blood concentra-tions with the outcome of therapy of acidosis, and with posture and demeanour inyoung calves with diarrhoea. J Vet Med A Physiol Pathol Clin Med 2006;53(9):490–4.
6. Angell JW, Jones G, Grove-White DH, et al. A prospective on farm cohort studyinvestigating the epidemiology and pathophysiology of drunken lamb syndrome.Vet Rec 2013;172:154–7.
7. Bleul U, Schwantag S, Stocker H, et al. Floppy kid syndrome caused by D-lacticacidosis in goat kids. J Vet Intern Med 2006;20:1003–8.
8. Angell JW, Jones GL, Voight K, et al. Successful correction of D-lactic acid neuro-toxicity (drunken lamb syndrome) by bolus administration of oral sodium bicar-bonate. Vet Rec 2013;173:193–5.
9. Van Saun RJ. Pregnancy toxemia in a flock of sheep. J Am Vet Med Assoc 2000;217(10):1536–9.
10. Grunberg W, Morin DE, Drackley JK, et al. Effect of continuous intravenousadministration of a 50% dextrose solution on phosphorus homeostasis in dairycows. J Am Vet Med Assoc 2006;229:413–20.
11. Firshman AM, Cebra CK, Schanbacher BJ, et al. Evaluation of insulin secretionand action in New World camelids. Am J Vet Res 2013;74:96–101.
12. Cebra CK. Hyperglycemia, hypernatremia and hyperosmolarity in 6 neonatalllamas and alpacas. J Am Vet Med Assoc 2000;217(11):1701–4.
13. Buchheit TM, Sommardahl CS, Frank N, et al. Use of a constant rate infusion ofinsulin for the treatment of hyperglycemic, hypernatremic, hyperosmolar syn-drome in an alpaca cria. J Am Vet Med Assoc 2010;236:562–6.
14. Carney KR, McKenzie EC, Mosley CA, et al. Evaluation of the effect of hetastarchand lactated Ringer’s solution on plasma colloid osmotic pressure in healthyllamas. J Am Vet Med Assoc 2011;238:768–72.

Fluid Therapy in Small Ruminants and Camelids 453
15. Cheng YH, Goff JP, Horst RL. Restoring normal blood phosphorus concentrationsin hypophosphatemic cattle with sodium phosphate. Vet Med 1998;93:240–3.
16. Clore ER, Freeman LM, Bedenice D, et al. Retrospective evaluation of parenteralnutrition in alpacas: 22 cases (2002-2008). J Vet Intern Med 2011;25:598–604.
17. Waitt LH, Cebra CK. Characterization of hypertriglyceridemia and response totreatment with insulin in llamas and alpacas: 31 cases (1995-2005). J Am VetMed Assoc 2008;232:1362–7.
18. Marinella MA. The refeeding syndrome and hypophosphatemia. Nutr Rev 2003;61(9):320–3.