Embed Size (px)
Citation preview

Fluids and Fluids and ElectrolytesElectrolytes

Body FluidsBody Fluids
Water is the major constituent of Water is the major constituent of living cellsliving cells
Extracellular and intracellular fluids Extracellular and intracellular fluids are largely waterare largely water
A loss of 25% of body water can A loss of 25% of body water can lead to deathlead to death

ElectrolytesElectrolytes
Compounds that form ions when Compounds that form ions when dissolved in waterdissolved in water
NaNa++ - primary cation of extracellular - primary cation of extracellular fluidfluid– Retains fluid in the body, generates and Retains fluid in the body, generates and
transmits nerve impulses, maintains acid-transmits nerve impulses, maintains acid-base balance, regulates enzyme activities, base balance, regulates enzyme activities, and regulates osmolarity and and regulates osmolarity and electroneutralityelectroneutrality

ElectrolytesElectrolytes
KK++ - primary cation of intracellular - primary cation of intracellular fluidfluid– Regulates acid-base and water balance, Regulates acid-base and water balance,
important in protein synthesis, important in protein synthesis, carbohydrate metabolism, muscle carbohydrate metabolism, muscle building, and the nervous systembuilding, and the nervous system
CaCa++++ – Important in bone formation, muscle Important in bone formation, muscle
contraction, and blood coagulationcontraction, and blood coagulation

ElectrolytesElectrolytes
MgMg++++ - 2 - 2ndnd most abundant cation most abundant cation in intracellular fluidsin intracellular fluids– Helps maintain normal nerve and Helps maintain normal nerve and
muscular function, transmission of muscular function, transmission of impulses, and steady heart rhythmsimpulses, and steady heart rhythms

Serum electrolyte levelSerum electrolyte level
Na – 135-145 mEq/LNa – 135-145 mEq/L Cl - 95-108 mEq/LCl - 95-108 mEq/L K – 3.5-5 mEq/LK – 3.5-5 mEq/L Ca – 4.5-5.8 mEq/LCa – 4.5-5.8 mEq/L Mg – 1.5-2.5 mEq/LMg – 1.5-2.5 mEq/L

ElectrolytesElectrolytes
ClCl-- – Transports COTransports CO22, forms HCl in the , forms HCl in the
stomach, retains Kstomach, retains K++, maintains , maintains osmolarityosmolarity
HH++
– Determines the acidity and alkalinity Determines the acidity and alkalinity of body fluidsof body fluids

TonicityTonicity
Measures the amount of dissolved Measures the amount of dissolved particles in relation to body fluidsparticles in relation to body fluids
HypotonicHypotonic – lower concentration of – lower concentration of dissolved particlesdissolved particles
HypertonicHypertonic – higher concentration – higher concentration of dissolved particlesof dissolved particles
IsotonicIsotonic – same concentration of – same concentration of dissolved particles (0.9% sodium dissolved particles (0.9% sodium chloride)chloride)

Electrolyte disordersElectrolyte disorders Abnormal electrolytesAbnormal electrolytes
– primary disease stateprimary disease state– secondary consequence of a multitude of secondary consequence of a multitude of
diseasesdiseases– iatrogenic problems are very commoniatrogenic problems are very common
ImportantImportant– maintenance of cellular homeostasismaintenance of cellular homeostasis– cardiovascular physiology - BPcardiovascular physiology - BP– renal physiology renal physiology – electrophyssiology - heart, CNSelectrophyssiology - heart, CNS

Some clinical examplesSome clinical examples Haemorhage - accidents, surgeryHaemorhage - accidents, surgery Poor intake - elderlyPoor intake - elderly Increased losses - pyrexia, heatIncreased losses - pyrexia, heat Diabetes insipidusDiabetes insipidus Diabetes mellitusDiabetes mellitus Diuretic therapyDiuretic therapy Endocrine disorders - ADH, Endocrine disorders - ADH,
aldosteronealdosterone

Important ConceptsImportant Concepts ConcentrationsConcentrations CompartmentsCompartments ContentsContents VolumesVolumes Rates of gain & lossRates of gain & loss

ConceptsConcepts
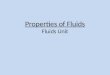
ICF28L
ECF14L Plasma + Interstitial
Intake Excetion
Normally the system is maintained in equilibriumChanging any factor causes a new steady state to be reached

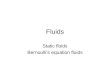
Decreasing the volume Decreasing the volume -4L-4L
ICF26L
ECF10L Plasma + Interstitial
Intake Excetion
This will raise the concentration of any solute

Increasing the Increasing the excretion of a soluteexcretion of a solute
ICF28L
ECF14L Plasma + Interstitial
Intake Excretion
This will decrease the solute concentration

Body Fluid DistributionBody Fluid DistributionWaterWater [Na] [Na] [K][K]
(L)(L) (mmol/L) (mmol/L) (mmol/L) (mmol/L)
ECFECF
VascularVascular 33 140140 55
InterstitialInterstitial 1616 140140 55
ICFICF
IntracellularIntracellular 2323 1010 150150
TOTALTOTAL 4242

Loss of Isotonic Loss of Isotonic SolutionsSolutions
Haemorrhage

Compensatory Compensatory mechanismsmechanisms PhysiologicalPhysiological
– ThirstThirst– ADHADH– Renin / Angiotensin systemRenin / Angiotensin system
TherapeuticTherapeutic– Intravenous therapyIntravenous therapy– DiureticsDiuretics– DialysisDialysis

Replacement of loss of Replacement of loss of 2L of isotonic fluid2L of isotonic fluid
ICF28L
ECF12L
ICF29L
ECF13L
ICF28L
ECF14L
With isotonic fluid
No change in [Na]No fluid redistribution
With hypotonic fluid
Fall in [Na]Fluid redistribution

Replacement of loss of Replacement of loss of 3L of hypotonic fluid3L of hypotonic fluid
With isotonic fluid
[Na] slightly increasedNo fluid redistribution
With hypotonic fluid
[Na] restoredFluid redistribution
ICF26L
ECF13L
ICF28L
ECF14L
ICF26L
ECF16L
ICF26L
ECF16L
ICF26L
ECF16L

Clinical ProblemsClinical Problems HyponatraemiaHyponatraemia
– Too little Na in ECFToo little Na in ECF– Excess water in ECFExcess water in ECF
HypernatraemiaHypernatraemia– Too little water in ECFToo little water in ECF– Too much Na in ECFToo much Na in ECF
DehydrationDehydration– Water deficiencyWater deficiency– Fluid (Na and water) depletionFluid (Na and water) depletion

Disorders of PotassiumDisorders of Potassium Potassium reference range - 3.6 to 5.0 Potassium reference range - 3.6 to 5.0
mmol/Lmmol/L Values < 3.0 or > 6.0 are potentially Values < 3.0 or > 6.0 are potentially
dangerousdangerous– Cardiac conduction defectsCardiac conduction defects– Abnormal neuromuscular excitabilityAbnormal neuromuscular excitability
Clinical Problems are commonClinical Problems are common Many are iatrogenic and avoidableMany are iatrogenic and avoidable

Potassium DistributionPotassium Distribution
TotalTotal
NaNa K K mmolmmol
PlasmaPlasma 140140 5 5 2%2% 7070
Interstitial fluidInterstitial fluid 140140 55
Intracellular fluidIntracellular fluid 1010 150150 98% 98% 34003400
Intake 60 - 200 mmols/dIntake 60 - 200 mmols/d

Relationship of Potassium Relationship of Potassium to Hydrogen Ionsto Hydrogen Ions
K+ and H+ exchange across cell membraneK+ and H+ exchange across cell membrane Both bind to negatively charged proteins (eg Hb)Both bind to negatively charged proteins (eg Hb) Changes in pH cause shifts in the equilibriumChanges in pH cause shifts in the equilibrium
– acidosis - potassium moves out of cells -> acidosis - potassium moves out of cells -> hyperkalaemiahyperkalaemia
– alkalosis - potassium moves into cells -> alkalosis - potassium moves into cells -> hypokalaemiahypokalaemia
Conversely Potassium depletion and excess can Conversely Potassium depletion and excess can affect acid-base statusaffect acid-base status

Causes of HyperkalaemiaCauses of Hyperkalaemia ArtefactualArtefactual
– Delay in sample analysisDelay in sample analysis– HaemolysisHaemolysis– Drug therapy - Excess intakeDrug therapy - Excess intake
RenalRenal– Acute Renal FailureAcute Renal Failure– Chronic Renal FailureChronic Renal Failure
Acidosis (intracellular exchange)Acidosis (intracellular exchange) Mineralocorticoid Dysfunction Mineralocorticoid Dysfunction
– Adrenocortical failureAdrenocortical failure– Mineralocorticoid resistance - eg spironolactoneMineralocorticoid resistance - eg spironolactone
Cell DeathCell Death– Cytoxic therapyCytoxic therapy

Treatment of Treatment of HyperkalaemiaHyperkalaemia Correct acidosis if this is causeCorrect acidosis if this is cause Stop unnecessary supplements / intakeStop unnecessary supplements / intake Give Glucose & insulinGive Glucose & insulin
– Drives potassium into cellsDrives potassium into cells Ion exchange resinsIon exchange resins
– GIT potassium bindingGIT potassium binding DialysisDialysis
– short and long-termshort and long-term

Causes of Potassium Causes of Potassium DepletionDepletion
Low intakeLow intake Increased urine lossIncreased urine loss
– diuretics / osmotic diuresisdiuretics / osmotic diuresis– tubular dysfunctiontubular dysfunction– mineralocorticoid excessmineralocorticoid excess
GIT lossesGIT losses– vomitingvomiting– diarrhoea / laxativesdiarrhoea / laxatives– fistulaefistulae
Hypokalaemia without depletionHypokalaemia without depletion– alkalosisalkalosis– insulin / glucose therapy.insulin / glucose therapy.

Effects of Potassium Effects of Potassium depeletiondepeletion(< 2.5 mmol/l)(< 2.5 mmol/l) Acute changes in ICF/ECF ratiosAcute changes in ICF/ECF ratios
– Neuromuscular: Neuromuscular: lethargy, muscle weakness, heart arrhythmiaslethargy, muscle weakness, heart arrhythmias
Chronic losses from the ICFChronic losses from the ICF– Neuromuscular: Neuromuscular:
lethargy, muscle weakness, heart arrhythmiaslethargy, muscle weakness, heart arrhythmias– Kidney:Kidney:
polyuriapolyuria alkalosis - increase renal HCO3 productionalkalosis - increase renal HCO3 production
– Vascular:Vascular:
– Gut:Gut:

Detection of Potassium Detection of Potassium DepletionDepletion History: History:
– diarhoea, vomiting, drugs (diuretics, diarhoea, vomiting, drugs (diuretics, digoxin)digoxin)
– symptoms of lethargy / weaknesssymptoms of lethargy / weakness– cardiac arythmiascardiac arythmias
Electrolytes investigation:Electrolytes investigation:– hypokalaemiahypokalaemia– alkalosis - raised HCOalkalosis - raised HCO33

Treatment of Potassium Treatment of Potassium DepletionDepletion
PreventionPrevention– Adequate supplementation Adequate supplementation
Replacement of deficitReplacement of deficit– oraloral -- 48 mmol/day + diet48 mmol/day + diet– IVIV -- < 20 mmol/L< 20 mmol/L
Monitor plasma potassium regularly especially:Monitor plasma potassium regularly especially:– Diuretic therapyDiuretic therapy– Digoxin useDigoxin use– Compromised renal functionCompromised renal function– In support of IV resuscitation (eg DM In support of IV resuscitation (eg DM
Ketacidosis)Ketacidosis)

IV TherapyIV Therapy
Goal: provide sufficient water and Goal: provide sufficient water and electrolytes to maintain fluids and electrolytes to maintain fluids and excrete waste productsexcrete waste products
Solvent in IV solutions is waterSolvent in IV solutions is water

IV TherapyIV Therapy
Goal: provide sufficient water and Goal: provide sufficient water and electrolytes to maintain fluids and electrolytes to maintain fluids and excrete waste productsexcrete waste products
Solvent in IV solutions is waterSolvent in IV solutions is water
D5W = 5 g of Dextrose in 100 ml of D5W = 5 g of Dextrose in 100 ml of waterwater
NS = 0.9 g of NaCl in 100 ml of waterNS = 0.9 g of NaCl in 100 ml of water

Crysrtaloids Crysrtaloids
Normal Saline (NS) (0.9% NaCl)Normal Saline (NS) (0.9% NaCl) Hypertonic saline (3% NaCl)Hypertonic saline (3% NaCl) Lactated Ringer’s (na, Cl, K, Ca, Lactated Ringer’s (na, Cl, K, Ca,
Lactate)Lactate) D5W (5% dextrose)D5W (5% dextrose)

Colloids Colloids
DextranDextran HetastarchHetastarch 5 and 25 % Albumin5 and 25 % Albumin

Crysrtaloids and Crysrtaloids and collloids: indication collloids: indication Acute liver failureAcute liver failure Acute nephrosisAcute nephrosis Adult respiratory disterss syndromeAdult respiratory disterss syndrome BurnsBurns Cardiopulmonary bypassCardiopulmonary bypass HypoproteinemiaHypoproteinemia Reduction of the risk of DVTReduction of the risk of DVT Renal dialysisRenal dialysis ShockShock

Acid-Base Acid-Base HomeostasisHomeostasis
Kidneys
OutputOutput
Lungs
Maintenance of
Normal [H+]BuffersBuffers
Metabolism
InputInput

Acid productionAcid production
total COtotal CO22 25 mol/day25 mol/day
unmetabolised acidsunmetabolised acids 50 mmol/day50 mmol/day
plasma [Hplasma [H++]] 40 nmol/L40 nmol/L

Buffering SystemsBuffering Systems
• HaemoglobinHaemoglobin• BicarbonateBicarbonate• PhosphatePhosphate• ProteinsProteins• AmmoniaAmmonia• Misc organic Misc organic
acidsacids

Integrated approach to Integrated approach to acid-baseacid-base

AcidosisMetabolic
Alkalosis
AcidosisRespiratory
Alkalosis
Acid-Base Acid-Base PathologyPathology

Acidosis treatment - 4 % Sodium 4 % Sodium hydrocarbon hydrocarbon
Alkalosis treatment – Citric acidAlkalosis treatment – Citric acid

Coagulation Coagulation Modifiers Agents. Modifiers Agents.

Blood ClottingBlood Clotting
Anticoagulants Anticoagulants – Prevent clot formation by inhibiting Prevent clot formation by inhibiting
clotting factorsclotting factors

Blood ClottingBlood Clotting
Anticoagulants Anticoagulants – Prevent clot formation by inhibiting Prevent clot formation by inhibiting
clotting factorsclotting factors AntiplateletsAntiplatelets
– Reduce risk of clot formation by Reduce risk of clot formation by inhibiting platelet aggregationinhibiting platelet aggregation

Blood ClottingBlood Clotting
Anticoagulants Anticoagulants – Prevent clot formation by inhibiting Prevent clot formation by inhibiting
clotting factorsclotting factors AntiplateletsAntiplatelets
– Reduce risk of clot formation by Reduce risk of clot formation by inhibiting platelet aggregationinhibiting platelet aggregation
FibrinolyticsFibrinolytics– Dissolve clots already formedDissolve clots already formed

Clotting CascadeClotting Cascade

Clotting CascadeClotting Cascade
If any factor in the cascade is If any factor in the cascade is missing, blood will not clot missing, blood will not clot (hemophilia)(hemophilia)

Clinical ThrombosisClinical Thrombosis
>2.5 million cases of deep venous >2.5 million cases of deep venous thrombosis (DVT) per yearthrombosis (DVT) per year
>600,000 cases of pulmonary >600,000 cases of pulmonary embolism (PE) per yearembolism (PE) per year
>50,000 deaths per year from PE>50,000 deaths per year from PE PE contributes to another 150,000 PE contributes to another 150,000
deaths per yeardeaths per year > 11,000 postsurgical PE deaths per > 11,000 postsurgical PE deaths per
yearyear

Venous ThrombiVenous Thrombi
Usually form in areas of slow Usually form in areas of slow blood flow, surgical or vein blood flow, surgical or vein injuries, large venous sinuses, or injuries, large venous sinuses, or pockets formed by valves in deep pockets formed by valves in deep veinsveins
If the clot breaks off, it can travel If the clot breaks off, it can travel to the lung causing pulmonary to the lung causing pulmonary embolism (PE)embolism (PE)

DVTDVT
Deep vein thrombosis above the Deep vein thrombosis above the knee is the most serious and may knee is the most serious and may be fatalbe fatal



Risk Factors for DVTRisk Factors for DVT
Age over 40Age over 40 Bed rest over 4 Bed rest over 4
daysdays Estrogen Estrogen
combined with combined with nicotinenicotine
High dose High dose estrogen therapyestrogen therapy
Major illnessMajor illness
ObesityObesity ParturitionParturition PregnancyPregnancy Previous DVTPrevious DVT SurgerySurgery TraumaTrauma Varicose veinsVaricose veins

Laboratory TestingLaboratory Testing
Certain lab tests must be done on Certain lab tests must be done on patients who are on anticoagulant patients who are on anticoagulant therapytherapy

Laboratory TestingLaboratory Testing
Partial thromboplastin time (PTT) – Partial thromboplastin time (PTT) – affected by heparinaffected by heparin
APTT – Activated Partial APTT – Activated Partial thromboplastin time thromboplastin time
Prothrombin Time (PT) – affected by Prothrombin Time (PT) – affected by warfarinwarfarin
International Normalized Ration (INR)International Normalized Ration (INR) HematocritHematocrit

Anticoagulant Anticoagulant AgentsAgents
argatroban argatroban bivalirudin (Angiomax)bivalirudin (Angiomax) fondaparinux (Arixtra)fondaparinux (Arixtra) heparin heparin lepirudin (Refludan)lepirudin (Refludan) warfarin (Coumadin)warfarin (Coumadin)
Drug List

THE IDEAL THE IDEAL ANTICOAGULANTANTICOAGULANT
1)1) Would be effective for prophylaxis of clots, Would be effective for prophylaxis of clots, prevention of clot extension, and clot lysisprevention of clot extension, and clot lysis
2)2) Would be able to be given orally and Would be able to be given orally and parenterallyparenterally
3)3) Would be inexpensiveWould be inexpensive4)4) Would be devoid of side effectsWould be devoid of side effects5)5) Would have a long half-lifeWould have a long half-life6)6) Would be easy to monitor or not require Would be easy to monitor or not require
monitoringmonitoring7)7) Would not interact with food or other Would not interact with food or other
medicationsmedications8)8) Would be rapidly and easily reversibleWould be rapidly and easily reversible

heparinheparin
Inhibits thrombin formation Inhibits thrombin formation preventing clots from formingpreventing clots from forming
Only anticoagulant that does not Only anticoagulant that does not cross the placentacross the placenta
Given for prophylaxis of DVT in Given for prophylaxis of DVT in postoperative, bedridden, obese postoperative, bedridden, obese patients, and otherspatients, and others

HEPARIN HEPARIN DescriptionDescription
1)1) Discovered in 1916 by McLean; isolated from Discovered in 1916 by McLean; isolated from liver, thus liver, thus the name heparinthe name heparin
2)2) Anionic glycosaminoglycan available as calcium Anionic glycosaminoglycan available as calcium or or sodium saltsodium salt
3)3) Molecular weight 15,000 D (avg.)Molecular weight 15,000 D (avg.)
4)4) Prepared from porcine intestinal mucosa and Prepared from porcine intestinal mucosa and bovine lungbovine lung
5)5) Does not cross placentaDoes not cross placenta
6)6) Little interaction with other medicationsLittle interaction with other medications
7)7) IV or SC administration onlyIV or SC administration only
8)8) Reversible with protamine (1 mg/200 U heparin) Reversible with protamine (1 mg/200 U heparin)

HEPARIN HEPARIN ActionAction
1)1) Binds to and potentiates antithrombin IIIBinds to and potentiates antithrombin III
2)2) Heparin-antithrombin III complex Heparin-antithrombin III complex inactivates inactivates thrombin (factor IIa) and thrombin (factor IIa) and factor Xafactor Xa
3)3) Secondary effect against platelet functionSecondary effect against platelet function

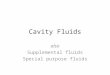
Plasminogen
PlasminogenActivator
PAI*
Plasmin
2 Anti-plasmin
XII
XI
IX
X
V
II
I
Fibrin
VIII VII
InhibitoryActivating * Plasminogen Activator Inhibitor
Antithrombin III

HEPARIN HEPARIN IndicationsIndications
Full Dose: 5000 U or 80 U/kg IV bolus, followed by 1200-Full Dose: 5000 U or 80 U/kg IV bolus, followed by 1200-1600 U/hr 1600 U/hr adjusted to therapeutic adjusted to therapeutic rangerange 1)1) Acute deep venous thrombosisAcute deep venous thrombosis 2)2) Pulmonary emboliPulmonary emboli 3)3) Unstable angina and myocardial infarctionUnstable angina and myocardial infarctionLow Dose:Low Dose: 5000 U sq q12 h5000 U sq q12 h 1)1) Postoperative prophylaxis of any major abdominal, Postoperative prophylaxis of any major abdominal, thoracic, thoracic, gynecologic, or orthopedic proceduregynecologic, or orthopedic procedure 2)2) Immobilized medical patients >40 yrs. with CHF, Immobilized medical patients >40 yrs. with CHF, CVA, CVA, malignant diseasemalignant disease 3)3) Prophylaxis for underlying hypercoagulable stateProphylaxis for underlying hypercoagulable stateOther Dose:Other Dose: 1)1) Extracorporeal bypassExtracorporeal bypass 2)2) HemodialysisHemodialysis 3)3) After thrombolytic therapyAfter thrombolytic therapy

HEPARIN HEPARIN ContraindicationContraindicationss
1)1) ThrombocytopeniaThrombocytopenia2)2) Aspirin or alcohol useAspirin or alcohol use3)3) Hepatic or renal diseaseHepatic or renal disease4)4) Other platelet Other platelet dysfunctiondysfunction5)5) GI bleedingGI bleeding6)6) Tumors, esp. CNSTumors, esp. CNS

HEPARIN (6) HEPARIN (6) Side EffectsSide Effects
1)1) Major side effect is Major side effect is bleedingbleeding2)2) Osteoporosis with Osteoporosis with prolonged useprolonged use3)3) ThrombocytopeniaThrombocytopenia

LEPIRUDINLEPIRUDIN1)1) Recombinant form of hirudinRecombinant form of hirudin
2)2) Highly specific direct thrombin inhibitorHighly specific direct thrombin inhibitor
3)3) Not associated with HITNot associated with HIT
4)4) Short half-life 1-2 hoursShort half-life 1-2 hours
5)5) Monitored by APTT or ecarin clotting Monitored by APTT or ecarin clotting timetime
6)6) Crosses placenta in rats, would not use Crosses placenta in rats, would not use in pregnancy at present in pregnancy at present
7)7) No antidoteNo antidote

PENTASACCHARIDPENTASACCHARIDEE fondaparinux fondaparinux (Arixtra)(Arixtra)
1)1) New type of anticoagulantNew type of anticoagulant
2)2) Indicated for DVT Indicated for DVT prophylaxis in orthopedic prophylaxis in orthopedic surgerysurgery
3)3) Dose is 2.5 mg SC qdDose is 2.5 mg SC qd
4)4) ? benefit in HIT? benefit in HIT

ARGATROBANARGATROBAN1)1) Synthetic moleculeSynthetic molecule2)2) Direct thrombin inhibitorDirect thrombin inhibitor3)3) Not associated with HITNot associated with HIT4)4) Monitored by APTT, also prolongs PTMonitored by APTT, also prolongs PT5)5) Must be dose reduced in hepatic failureMust be dose reduced in hepatic failure6)6) Half-life 40-50 min.Half-life 40-50 min.7)7) No antidoteNo antidote8)8) Dose: Dose: 2 microgm/kg/min IV adjusted to 2 microgm/kg/min IV adjusted to 1.5-3.0 x baseline APTT1.5-3.0 x baseline APTT

Low-Molecular-Weight Heparins:Low-Molecular-Weight Heparins: dalteparin (Fragmin)dalteparin (Fragmin) enoxaparin (Lovenox)enoxaparin (Lovenox) tinzaparin (Innohep)tinzaparin (Innohep)
Drug List

LOW MOLECULAR WEIGHT HEPARIN
General1) 1) Molecular weight 3,000- 7,000 DMolecular weight 3,000- 7,000 D2)2) Inhibits factor Xa rather than thrombinInhibits factor Xa rather than thrombin3)3) Factor Xa assay used for monitoring Factor Xa assay used for monitoring 4)4) Administered subcutaneouslyAdministered subcutaneously5)5) Probably less antigenic than standard Probably less antigenic than standard heparinheparin6)6) Recommended for prophylaxis and Recommended for prophylaxis and treatmenttreatment7)7) Enoxaparine, dalteparin, and tinzaparin Enoxaparine, dalteparin, and tinzaparin available available in U.S.in U.S.

LOW MOLECULAR WEIGHT HEPARINMonitoring
1) PT, APTT not usually prolonged
2) May be monitored with anti-factor Xa assay

warfarin (Coumadin)warfarin (Coumadin)
Prevents production of vitamin Prevents production of vitamin K-dependent clotting K-dependent clotting factorsfactors
Prevents future clots with no Prevents future clots with no effect on existing clotseffect on existing clots
Should not be taken with ASA or Should not be taken with ASA or NSAIDsNSAIDs

Vitamin K-antagonists of the coumarin Vitamin K-antagonists of the coumarin type and vitamin Ktype and vitamin K

COUMADIN COUMADIN DescriptionDescription
1)1) Isolated by Link in 1939 after previous Isolated by Link in 1939 after previous observation that cattle developed bleeding observation that cattle developed bleeding disorder after ingestion of spoiled cloverdisorder after ingestion of spoiled clover
2)2) Is 4-hydroxycoumarin compound, similar Is 4-hydroxycoumarin compound, similar in in structure to vitamin Kstructure to vitamin K
3)3) Administered p.o., rapid GI absorptionAdministered p.o., rapid GI absorption
4)4) Crosses placenta easilyCrosses placenta easily
5)5) Interacts with a variety of drugsInteracts with a variety of drugs
6)6) Hereditary resistance has been describedHereditary resistance has been described

COUMADIN COUMADIN ActionsActions
1)1) Blocks the carboxylation of the Blocks the carboxylation of the vitamin K vitamin K dependent clotting dependent clotting proteins, factors II proteins, factors II VII, IX, and VII, IX, and X, maintaining them in their X, maintaining them in their inactive formsinactive forms
2)2) Also blocks the anticoagulant Also blocks the anticoagulant proteins proteins C and S C and S

COUMADIN COUMADIN LaboratoryLaboratory
1)1) Prolongs the PT and APTTProlongs the PT and APTT
2)2) PT and International PT and International Normalized Ratio Normalized Ratio (INR) (INR) used for monitoringused for monitoring

INTERNATIONAL NORMALIZED RATIO (INR)
Ideal INR depends on clinical situation
ISI = Sensitivity Index for thromboplastin
INR = PATIENT PT CONTROL PT
ISI

COUMADINContraindications
1) Pre-existing hemostatic defects
2) GI bleeding
3) CNS hemorrhage
4) Pregnancy, esp. 1st trimester

COUMADINSide Effects
1) Hemorrhage
2) Unmasking of underlying anatomic lesion
3) Surreptitious use
4) Fetal abnormalities
5) Skin necrosis with deficiencies of proteins C or S usually on 3rd to 8th day of therapy

COUMADIN-COUMADIN-INDUCED SKIN INDUCED SKIN NECROSISNECROSIS
1)1) Usually occurs on days 3-8 after Usually occurs on days 3-8 after initiation of initiation of Coumadin Coumadin
2) 2) More common in females (75%)More common in females (75%)
3)3) Most common on the breast, Most common on the breast, buttocks, or buttocks, or extremities, occ. on extremities, occ. on penis in malespenis in males
4)4) Not predictable by history or Not predictable by history or protein C levelprotein C level

COUMADIN COUMADIN DosingDosing
1)1) Usual recommendation is 5 mg Usual recommendation is 5 mg initial daily doseinitial daily dose
2)2) Larger loading dose not beneficialLarger loading dose not beneficial3)3) Should be continued for at least 3-6 Should be continued for at least 3-6
months after initial DVT, 1 yr. for months after initial DVT, 1 yr. for recurrent thrombi, and indefinitely for recurrent thrombi, and indefinitely for atrial fibrillation and prosthetic valvesatrial fibrillation and prosthetic valves
4)4) Must be aware of changes in Must be aware of changes in concomitant concomitant drugs and dietdrugs and diet

COUMADIN COUMADIN InteractionsInteractions
POTENTIATORS:POTENTIATORS:SulfasSulfasPhenylbutazonePhenylbutazoneCimetidineCimetidineOmeprazoleOmeprazoleAmiodaroneAmiodaroneAnabolic steroidsAnabolic steroids
ANTAGONISTS:ANTAGONISTS:BarbituratesBarbituratesRifampinRifampinPenicillinsPenicillinsAntacidsAntacids

Antiplatelet Antiplatelet AgentsAgents
aspirinaspirin clopidogrel (Plavix)clopidogrel (Plavix) ticlopidine (Ticlid)ticlopidine (Ticlid)
Drug List

ANTIPLATELET ANTIPLATELET THERAPYTHERAPYAspirin IndicationsAspirin Indications
1)1) Stroke, TIAStroke, TIA
2)2) MI, recurrent MIMI, recurrent MI
3)3) Unstable anginaUnstable angina

Inhibitors of platelet Inhibitors of platelet aggregationaggregation

Presystemic inactivation of platelet Presystemic inactivation of platelet cyclooxygenase by acetylsalicylic acidcyclooxygenase by acetylsalicylic acid

TICLOPIDINETICLOPIDINE
1)1) Interferes with platelet-fibrinogen bindingInterferes with platelet-fibrinogen binding
2)2) Exerts its action for the life of the plateletExerts its action for the life of the platelet
3)3) May prolong bleeding timeMay prolong bleeding time
4)4) Useful for coronary artery stents and CVAUseful for coronary artery stents and CVA
5)5) Methylprednisolone may reverse its effectMethylprednisolone may reverse its effect
6)6) Associated with TTP, neutropenia, and Associated with TTP, neutropenia, and diarrheadiarrhea

clopidogrel (Plavix)clopidogrel (Plavix)
Blocks ADP receptors and Blocks ADP receptors and prevents platelet adhesion and prevents platelet adhesion and aggregationaggregation
Used to prevent MI and strokeUsed to prevent MI and stroke Major side effect is bleedingMajor side effect is bleeding

CLOPIDOGREL
1) Interferes with GP IIb/IIIa binding site
2) Exerts its action for the life of the platelet
3) May prolong bleeding time
4) Indicated for prevention of MI, CVA, and vascular death in pts with ASCD
5) Fewer side effects than ticlopidine
6) Dose: 75 mg qd

Antiplatelet Antiplatelet AgentsAgents
Glycoprotein Antagonists:Glycoprotein Antagonists: abciximab (ReoPro)abciximab (ReoPro) eptifibatide (Integrilin)eptifibatide (Integrilin) tirofiban (Aggrastat)tirofiban (Aggrastat)
Drug List

Abciximab (ReoPro)
1) Human-mouse monoclonal Ab
2) Binds to GP IIb/IIIa receptor on platelets
3) Half-life 10 min.
4) May block receptor for 10 days
5) Indicated for prevention of closure of coronary vessels after angioplasty
6) May cause thrombocytopenia
7) Used with heparin and ASA

Fibrinolytic Fibrinolytic AgentsAgents
alteplase (Activase)alteplase (Activase) reteplase (Retavase)reteplase (Retavase) streptokinase (Streptase)streptokinase (Streptase) tenecteplase (TNKase)tenecteplase (TNKase) urokinase (Abbokinase)urokinase (Abbokinase)
Drug List

Fibrinolytic AgentsFibrinolytic Agents
Dissolve existing emboli or Dissolve existing emboli or thrombithrombi
Indications:Indications:– DVTDVT– Acute peripheral occlusionAcute peripheral occlusion– Acute MI with embolizationAcute MI with embolization– PEPE– Coronary embolusCoronary embolus