Embed Size (px)
Citation preview

Original Article
Fluorescein-Guided Resection of Intramedullary Spinal Cord Tumors: Results from a
Preliminary, Multicentric, Retrospective StudyFrancesco Acerbi1, Claudio Cavallo1, Karl-Michael Schebesch2, Mehmet Osman Akcakaya3, Camilla de Laurentis1,
Mustafa Kemal Hamamcioglu3, Morgan Broggi1, Alexander Brawanski2, Jacopo Falco1, Roberto Cordella1,
Paolo Ferroli1, Talat Kiris3, Julius Hohne2
-BACKGROUND: Intramedullary spinal cord tumors(IMSCTs) are rare, heterogenous lesions that are usuallyenhanced on preoperative magnetic resonance imaging(MRI) because of a damaged blood-brain barrier. Sodiumfluorescein is a dye that accumulates in areas of the centralnervous system with a damaged BBB. Given the pattern ofMRI contrast enhancement of the majority of IMSCTs, theuse of this fluorescent tracer could improve tumor visuali-zation and quality of resection. In this article, we present thefirst experience with the application of fluorescein-guidedtechnique for surgical removal of IMSCTs.
-METHODS: Eleven patients (6 men, 5 women; mean age,50.1 years), harboring 5 ependymomas, 3 hemangio-blastomas, 1 astrocytoma, 1 pilocytic astrocytoma, and 1glioneuronal tumor forming rosettes were included. Sodiumfluorescein (5 mg/kg) was injected immediately after pa-tient intubation. Tumors were removed with microsurgicaltechnique and standard neurophysiological monitoring,under YELLOW 560 filter (Pentero 900) visualization. Sur-gical reports were reviewed regarding usefulness andgrade of fluorescein staining. Postoperative MRI was per-formed within 72 hours after surgery, and postoperativeclinical outcome was registered.
-RESULTS: No adverse events were registered. Fluores-cent staining was reported in 9 of 11 cases (82%), all of
Key words- Intramedullary spinal cord tumor- Resection- Sodium fluorescein- YELLOW 560 filter
Abbreviations and AcronymsBBB: Blood-brain barrierCNS: Central nervous systemGOS: Glasgow outcome scoreGTR: Gross total resectionHGG: High-grade gliomaIMSCT: Intramedullary spinal cord tumorMRI: Magnetic resonance imagingmRS: Modified Rankin scaleSF: Sodium fluorescein
WORLD NEUROSURGERY 108: 603-609, DECEMBER 2017
them enhancing on preoperative MRI (100% of ependymo-mas, 100% of pilocytic astrocytomas, 100% of hemangio-blastomas). No fluorescence was reported in 1 astrocytomaand 1 glioneuronal tumoreforming rosette. Intraoperativefluorescence was considered helpful for tumor resection in9 of 11 cases (82%). Gross total resection was obtained in 8of 11 cases (72.7%).
-CONCLUSIONS: Our results suggest that fluorescein-guided surgery is a safe and effective technique that canbe used during the surgical resection of IMSCTs presentingwith contrast-enhancement on preoperative MRI.
INTRODUCTION
ntramedullary spinal cord tumors (IMSCTs) are relatively rareneoplasms comprising a miscellaneous group of tumors
I affecting the central nervous system (CNS). They represent2%e4% of all CNS neoplastic lesions and are associated with alow incidence of approximately 1.1 cases per 100.000 persons.1,2
Among them, ependymomas are the most common overall, andthey frequently affect the adults, whereas astrocytomas present amuch higher occurrence in the pediatric population.3 IMSCTsinclude heterogeneous lesions, and they consequently present avariable behavior ranging from highly aggressive to relatively
From the 1Neurosurgical Unit 2, Department of Neurosurgery, Foundation IRCCS IstitutoNeurologico Carlo Besta, Milan, Italy; 2Department of Neurosurgery, University MedicalCenter, Regensburg, Germany; and 3Department of Neurosurgery, Liv Hospital Ulus affiliatedto Istinye University Medical Faculty, Istanbul, Turkey
To whom correspondence should be addressed: Francesco Acerbi, M.D., Ph.D.[E-mail: [email protected]]
Supplementary digital content available online.
Citation: World Neurosurg. (2017) 108:603-609.https://doi.org/10.1016/j.wneu.2017.09.061
Journal homepage: www.WORLDNEUROSURGERY.org
Available online: www.sciencedirect.com
1878-8750/$ - see front matter ª 2017 Elsevier Inc. All rights reserved.
www.WORLDNEUROSURGERY.org 603

ORIGINAL ARTICLE
FRANCESCO ACERBI ET AL. FLUORESCEIN-GUIDED RESECTION OF INTRAMEDULLARY SPINAL CORD TUMORS
indolent clinical course. Despite this finding, most IMSCTs appearwith characteristic contrast enhancement on preoperativemagnetic resonance imaging (MRI) because of a damagedblood-brain barrier (BBB).4,5 Because surgical removal withpossible gross total resection (GTR) represents the standard ofcare in the management of these tumors,6 the use of technicaltools that can increase tumor visualization during surgicalprocedures could give a major contribution for patient prognosis.For example, sodium fluorescein (SF) is a dye with the peculiar
characteristic of accumulating in areas of the CNS showingdamage to the BBB.7 Recently, dedicated filters with a specificwavelength for SF have been integrated into the surgicalmicroscope.8 In this way, SF has been proposed as a fluorescenttracer for different kinds of tumors of the CNS, including high-grade gliomas, metastasis, lymphomas, and hemangio-blastomas.9-12 Given the pattern of contrast enhancement uptakeon MRI of the majority of IMSCTs, the use of this fluorescenttracer could allow a better intraoperative discrimination of thedifferent tumor subtypes compared with the surrounding normalspinal cord parenchyma. To our knowledge, we present the firstexperience with the application of a fluorescein-guided techniquefor surgical removal of IMSCTs.
METHODS
Patients, Preoperative, and Postoperative Clinical andNeuroradiologic EvaluationIn this study, we retrospectively reviewed surgical databases,approved by a local ethical committee in 3 neurosurgical de-partments (Fondazione IRCCS Istituto Neurologico Besta, Milano,Italy; Department of Neurosurgery, Regensburg University Hos-pital, Regensburg, Germany; Department of Neurosurgery LivHospital Ulus affiliated with Istinye University Medical Faculty,Istanbul, Turkey), to identify the cohort of patients with IMSCTswho underwent surgical removal using the fluorescein-guidedtechnique from January 2014 to December 2016. We identified 11patients (6 men, 5 women; mean age, 50.1 years) with 5 ependy-momas, 3 hemangioblastomas, 1 astrocytoma (World Health Or-ganization [WHO] grade II), 1 pilocytic astrocytoma (WHO grade I),and 1 glioneuronal tumor forming rosettes (WHO grade I).All patients underwent preoperative and immediately post-
operative (within 72 hours after surgery) contrast-enhanced MRI.Preoperative neuroimaging studies were reviewed to determine theexact location of the tumor and the presence of contrastenhancement. The extent of resection was estimated by analyzingthe results of comparison between preoperative and postoperative
Video available atWORLDNEUROSURGERY.org
neuroimaging. The preoperative tumor diameterswere calculated using OsiriX for Macintosh (http://www.osirix-viewer.com).Clinical and neurologic conditions were available
for hospital admission, discharge, and follow-up. Inparticular, clinical presentation; the use of preopera-tive corticosteroid treatment, radiotherapy, orchemotherapy; intraoperative complications,
including possible adverse effects of SF injection; and post-operative Glasgow outcome score (GOS), modified Rankin Scale(mRS) score, and Barthel index were collected in the surgicaldatabase.604 www.SCIENCEDIRECT.com WORLD NE
Surgical Protocol of Fluorescein-Guided TechniqueThe surgical protocol for the fluorescein-guided technique was thesame as described previously for the removal of other tumors of theCNS.8,12,13 To summarize, 5 mg/kg of fluorescein (Monico SpA,Venice, Italy; Alcon Pharma, Freiburg im Breisgau, Germany; AlconLaboratuvarları, Istanbul, Turkey) were injected intravenously at thetime of induction of general anesthesia. Surgical resection wassubsequently performed with a microsurgical technique with the aidof a dedicated filter designed for the intraoperative visualization offluorescein excitation and emission wavelength, specifically theYELLOW560 filter equipped on the Pentero microscope (Carl ZeissMeditec, Oberkochen, Germany). Neurophysiologic monitoring(SSEP, MEP, D-wave) was used in the standard fashion.14
The surgical protocol was screened for any detailed informationregarding the usefulness and grade of fluorescence staining ofIMSCTs, as reported in our institutions for all lesions submitted tofluorescein-guided resection.SF was used off-label, and written informed consent was ob-
tained from all patients. One patient who underwent an operationat the Fondazione IRCCS Istituto Neurologico Besta (patient 11) ispart of the FLUOCERTUM study, a prospective observational studyof the use of fluorescein for removal of CNS tumors, performedafter approval of reimbursement for SF as a fluorescent tracer inneuro-oncology by the Italian Drug Agency (AIFA) obtained in July2015 (determination 905/2015, Gazette n. 168., 22 July, 2015; http://www.gazzettaufficiale.it/atto/serie_generale/caricaDettaglioAtto/originario;jsessionid¼izVcTOmnjOzfNRjjw56kAA__.ntc-as2-guri2b?atto.dataPubblicazioneGazzetta¼2015-07-22&atto.codiceRedazionale¼15A05620&elenco30giorni¼false).
RESULTS
No patient received radiotherapy or chemotherapy before surgeryor preoperative glucocorticoids.Patients were in good preoperative neurologic and clinical
condition, with an mRS score of 0 in 1 patient, 1 in 8 patients, and3 in 2 patients.Tumors were at the following locations in the spinal cord: 8 cer-
vical, 1 cervicothoracic, 1 thoracic, 1 conus. Nine of 11 (82%) patientshad contrast enhancement on preoperative MRI. In particular, 100%(5/5) of ependymomas, 100% (3/3) of hemangioblastomas, and 100%(1/1) of pilocytic astrocytomas were enhanced on preoperative MRI.Enhancement was not visible in 1 grade II astrocytoma and in 1glioneuronal tumoreforming rosette (WHO grade I). Maximum tu-mor diameter ranged from 8 to 208 mm (median, 20 mm).Fluorescent staining was reported in 9 of 11 cases (82%). In
UROSURG
particular, bright and homogenous fluorescence wasreported in 100% of ependymomas (5/5 patients;Figures 1 and 2; Video 1) and 100% of pilocyticastrocytomas (1/1); slight fluorescence was reportedin 100% of hemangioblastomas (3/3). Nofluorescence was reported in 1 astrocytoma (WHOgrade II) and 1 glioneuronal tumor forming rosette(WHO grade I). Considering the finding of
fluorescence staining, intraoperative fluorescence was consideredhelpful for tumor resection in 9 of 11 cases (82%).GTR was obtained in 8 of 11 cases (72.7%) and specifically in 5
of 5 (100%) cases of ependymoma, 2 of 3 (66.6%) cases of
ERY, https://doi.org/10.1016/j.wneu.2017.09.061

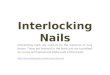
Figure 1. (A, B) Preoperative and (C, D) postoperativesagittal T2 (A, C) precontrast and (B, D) T1 postcontrastimaging of a 59-year-old female patient with a history ofcervical and upper limb pain (patient 10). Magneticresonance imaging (MRI) showed the presence of aC2-C6 intramedullary spinal cord tumor with cysticcomponent as for previous bleeding, T2 hyperteintense
tissue marginal to the cyst (A) and contrastenhancement (white arrow in B). The lesion wascompletely removed by microscopic fluorescein-guidedtechnique with neurophysiologic monitoring. Histologicdiagnosis was ependymoma. (C, D) Postoperative MRIconfirmed complete removal.
WORLD NEUROSURGERY 108: 603-609, DECEMBER 2017 www.WORLDNEUROSURGERY.org 605
ORIGINAL ARTICLE
FRANCESCO ACERBI ET AL. FLUORESCEIN-GUIDED RESECTION OF INTRAMEDULLARY SPINAL CORD TUMORS

606 www.SCIENCEDIRECT.com WORLD NE
ORIGINAL ARTICLE
FRANCESCO ACERBI ET AL. FLUORESCEIN-GUIDED RESECTION OF INTRAMEDULLARY SPINAL CORD TUMORS
hemangioblastoma, and 1/1 (100%) case of pilocytic astrocytoma.Subtotal resection (>75%) was obtained in the remaining 3 cases.Two of the tumors (1 grade II astrocytoma and 1 grade I glio-neuronal tumor forming rosette) did not enhance on preoperativeMRI, in which no fluorescence was evident during surgical pro-cedure. The last case of subtotal resection was a hemangio-blastoma in which a small fluorescent residual was left because ofits adherence to the spinal cord and change in MEPs and D-waveduring its manipulation.No adverse reactions to SF injection were reported. Two pa-
tients exhibited a slight clinical deterioration (mRS scores of 1and 2) that recovered at late follow-up. After a median follow-up of15 months, all patients are alive. Characteristics of the patients andmain results are described in Table 1.
DISCUSSION
To our knowledge, our retrospective analysis showed for the firsttime that the use of SF could add significant advantages in terms oftumor visualization and resection for the vast majority of IMSCTs.In particular, bright fluorescence was present in all cases of epen-dymomas and pilocytic astrocytomas, whereas it was less evidentfor hemangioblastomas and absent in the grade II astrocytoma andbenign glioneuronal tumor. These findings are clearly correlated tothe characteristics enhancement of tumors at preoperative MRI. Infact, 100% of the cases (9/9) enhanced on preoperative MRI showedbright (6/9) or slight (3/9) fluorescence during intraoperative visu-alization; in all these cases SF was considered helpful by theoperating surgeon to complete tumor removal.IMSCTs are a miscellaneous group that constitutes 20%e30% of
all primary spinal tumors.15 Among the different histopathologicentities comprised within the IMSCTs, ependymomas are themost common overall, and they more frequently affect the adults,whereas astrocytomas come next and represent up to 90% ofIMSCTs in the pediatric population.15 Hemangioblastomas are thethird most frequent subtype, accounting for 2%e15%16 of allIMSCTs. Even with these heterogeneous clinical andhistopathologic features, it was reported that most casesexhibited some degree of contrast enhancement on preoperativeMRI. For example, only 11 of 130 cases (8.5%) retrospectively
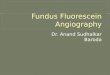
Figure 2. Intraoperative pictures taken from the same patient (patient 10).Immediately after dural opening, the cervical spinal cord appeared enlargedwithout signs of superficial disease, with (A) white light or (B) fluoresceinvisualization with a YELLOW 560 filter. After median mielotomy, the cysticcomponent of the previous bleeding was opened, and a greyish tissue wasvisible on the superior margin of the cyst (white arrow in C) and brightlyfluorescent when the YELLOW 560 filter was activated (white arrow in D).Bright fluorescent tissue was clearly distinguished from the wall of thehematoma only under YELLOW 560 filter visualization. Mielotomy wasextended superiorly, and the lesion was progressively separated from thenormal spinal cord parenchyma, identifying a clear plane of dissection byusing the fluorescent visualization with Yellow 560 filter (white line in E).The tumor was completely removed. At the end of resection, the cavity didnot show any sign of residual tumor (F), as confirmed by fluorescentvisualization with Yellow 560 filter (G).
UROSURGERY, https://doi.org/10.1016/j.wneu.2017.09.061

Table 1. Patient Population
PatientNumber
Age(years) Sex
ClinicalPresentation
TumorLocation
PreoperativeTumor
Diameter(mm)
TumorEnhancement
FluoresceinDose
IntraoperativeFluorescence* EOR
Surgeon’sOpinion Histology
PreoperativemRS Score
EarlyPostoperativemRS Score
LatePostoperativemRS Score
EarlyPostoperative
Outcome(GOS)
LatePostoperativeOutcome (GOS)
PostoperativeBarthel Index
PostopSurvival Status(Follow-up)
1 66 Female Pain betweenblades,paresthesiadig II-IV left
C6 3 � 8 � 6 Yes 5 mg/kg þ GTR Helpful Hemangioblastoma 1 1 1 5 5 80 Alive (16 mo)
2 60 Male Paresthesiaboth soles ofthe feetfor >10 years
Conus 15 � 16 � 12 Yes 5 mg/kg þþ GTR Helpful Pilocytic astrocytoma 1 1 1 5 5 90 Alive (21 mo)
3 27 Female Paresthesia leftarm, positiveLhermitte sign
C5 12 � 8 � 5 Yes 5 mg/kg þ GTR Helpful Hemangioblastoma 1 3 2 5 5 70 Alive (15 mo)
4 54 Male Neck pain,paresthesiaright hand
C1 12 � 4 � 7 Yes 5 mg/kg þ STR Helpful Hemangioblastoma 1 2 1 5 5 85 Alive (3 mo)
5 51 Female Cephalalgia,paresthesialeft arm
C2 12 � 8 � 5 Yes 5 mg/kg þþ GTR Helpful Ependymoma 1 1 1 5 5 80 Alive (6 mo)
6 43 Male Spastictetraparesis
Bulbus-T5
208 � 15 � 9 No 5 mg/kg e STR Not helpful Astrocytoma(WHO II)
3 2 2 4 5 70 Alive (22 mo)
7 38 Male Incidentallydiagnosed aftera fall fromheight(2 years’ follow-up, operatedbecauseof tumorgrowth)
T1-T2 24 � 8 � 6 Yes 5 mg/Kg þþ GTR Helpful Ependymoma 0 0 0 5 5 100 Alive (16 mo)
8 45 Female Cephalgia,paresthesia leftarm,
C1-C4 55 � 9 � 7 Yes 5 mg/Kg þþ GTR Helpful Ependymoma 3 3 1 4 5 90 Alive (15 mo)
9 58 Male Spastictetraparesis
C5-C7 35 � 8 � 7 Yes 5 mg/Kg þþ GTR Helpful Ependymoma 1 1 1 5 5 65 Alive (14 mo)
10 59 Female Pain in cervicalregion andsuperior limbs
C2-C6 8 � 20 � 11 Yes 5 mg/kg þþ GTR Helpful Ependymoma 1 1 1 5 5 90 Alive (12 mo)
11 37 Male Pain in superiorlimbs
C2-C5 65 � 10 � 10 Slight 5 mg/kg e STR Not helpful Glioneuronaltumor formingrosettes (WHO I)
1 1 1 5 5 90 Alive (4 mo)
EOR, extent of resection; mRS, modified Rankin Scale; GOS, Glasgow Outcome Scale; WHO, World Health Organization; C, cervical; T, thoracic; GTR, gross total resection; STR, subtotal resection.*Intraoperative fluorescence were graded as follows: þþ, bright fluorescence; þ, slight fluorescence; e, no fluorescence.
WORLD
NEUROSURGERY
108:603-6
09,D
ECEMBER2017
www.W
ORLDNEUROSURGERY.o
rg
607
ORIG
INALARTICLE
FRANCESCO
ACERBIETAL.
FLUORESCEIN
-GUID
ED
RESECTIO
NOFIN
TRAMEDULLARYSPIN
ALCORD
TUMORS

ORIGINAL ARTICLE
FRANCESCO ACERBI ET AL. FLUORESCEIN-GUIDED RESECTION OF INTRAMEDULLARY SPINAL CORD TUMORS
reviewed in a series of patients with surgically resected IMSCTswere nonenhancing on preoperative MRI.4 In another series of101 patients with surgically resected IMSCTs, all patients hadsome degree of contrast enhancement on preoperative MRI, evenfor infiltrating grade II astrocytomas.17
The standard of care for most IMSCTs is surgical resection,whereas adjuvant therapies (including radiotherapy and chemo-therapy) are usually considered second-line treatments reservedfor tumor recurrence and for cases in which surgery is contra-indicated or unsuccessful.6 The primary goal of resection is toachieve GTR while preserving the patient’s neurologic functionand obtaining a histopathologic diagnosis. Unfortunately, GTRis not always possible. In fact, it has been reported to rangefrom 69% to 97% in ependymomas18-20 and from 11% to 31% ininfiltrating astrocytomas,20-22 based on tumor size and identifi-cation of a plane of dissection, which is usually more common forependymomas.17
Innovative technical tools that can improve tumor visualizationand margin of differentiation to the normal peritumoral paren-chyma could have a positive influence on GTR. SF, the sodium saltof fluorescein, is a synthetic organic compound that accumulatesin CNS areas with an altered vessel permeability caused by adamaged BBB.7 Its use as a fluorescent tracer in neuro-oncologyhas been shown to provide significant advantages in terms ofextent of resection for high-grade gliomas.23-25
Recently, the introduction of dedicated filters specific for theexcitation and emission wavelengths of fluorescein integrated onthe surgical microscope (Pentero with YELLOW 560 Module; KarlZeiss, Oberkochen, Germany) have further improved the intra-operative visualization of the fluorescent staining. This adjunctsignificantly affected the development of fluorescein-guided sur-gery having increased the discrimination of tumoral tissue fromthe surrounding viable CNS parenchyma and allowed forexpanding indications to other type of CNS tumors, includingbrain metastasis, lymphomas, and hemangioblastomas.8-11,13,26-30
We hypothesized that IMSCTs presenting a gadolinium uptakein T1 MRI sequences could be shown intraoperatively as a fluo-rescent mass, using SF with a dedicated filter in the surgicalmicroscope. Our results clearly confirmed this hypothesis for thefirst time, to our knowledge, and suggested that fluorescein-guided technique could be used in a standardized fashion formost IMSCTs. As for other types of tumors, no adverse reactionswere reported. A bright tumor visualization was evident for mostcases (67%) that presented with clear contrast enhancement of thetumor mass on preoperative MRI, and SF was considered helpful
608 www.SCIENCEDIRECT.com WORLD NE
to achieve GTR in all these cases (Table 1). In particular, astratified analysis of our results revealed that the contribution offluorescein has been considered more significant forependymomas and pilocytic astrocytomas, which alwaysappeared with contrast enhancement on preoperative MRI,100% of bright fluorescence visualization, and 100% of GTR(Table 1). Despite the subjective intraoperative evaluation offluorescein possibly representing a major bias in our study, theclear and intense fluorescence delineating the tumor margin forthese histologic entities, along with the GTR performed inall cases, apparently supports the great benefit offluorescein utilization, particularly for these tumor subtypes(Figures 1 and 2). On the contrary, the use of fluoresceinremains questionable for tumors showing a minimal or aheterogeneous pattern of contrast medium uptake, such as forgrade I or some infiltrating grade II cases.Despite the use of fluorescein being helpful in improving both
the visualization and the resection in our 3 cases of hemangio-blastoma, these lesions presented only a slight fluorescent nodulewhen visualized with a YELLOW 560 filter. A more appropriateapplication of fluorescein was proposed by Rey-Dios et al.11 forthese tumor subtypes. They reported the intravenousadministration of fluorescein in bolus immediately beforemicrodissection to better visualize the vascular network of thetumor, including tumor arterial feeders, draining veins, and thenodule, as it has been already reported by our group withindocyanine green videoangiography.31
An important limitation of this retrospective study is the rela-tively small cohort and the heterogeneous histology of IMSCTsincluded. In addition, the lack of a significant long-term follow-upprevents the elucidation of a possible correlation between the useof SF, extent of resection, and survival. Future prospective studiescould better address these limitations by stratifying the cohortsaccording to the major predicting factors of IMSCT resectability,including tumor histology and the identification of a plane ofdissection.
CONCLUSION
Our results suggest that fluorescein-guided surgery is a safe andeffective technique that can be used during the surgical resectionof IMSCTs with contrast enhancement on preoperative MRI.Prospective studies with long-term follow-up could provide majorinsights into the effects of fluorescein application on progression-free survival and overall survival of patients with IMSCTs.
REFERENCES
1. Fischer G, Brotchi J. Intramedullary Spinal Cord Tu-mors. Stuttgart, Germany: Thieme; 1996.
2. McCormick PC, Stein BM. Spinal cord tumors inadults. In: Winn H, Winn H, eds. YoumansNeurological Surgery. Philadelphia: WB Saunders;1996:3102-3122.
3. DeSousa AL, Kalsbeck JE, Mealey J Jr,Campbell RL, Hockey A. Intraspinal tumors inchildren. A review of 81 cases. J Neurosurg. 1979;51:437-445.
4. White JB, Miller GM, Layton KF, Krauss WE.Nonenhancing tumors of the spinal cord.J Neurosurg Spine. 2007;7:403-407.
5. Sun B, Wang C, Wang J, Liu A. MRI features ofintramedullary spinal cord ependymomas.J Neuroimaging. 2003;13:346-351.
6. Tobin MK, Geraghty JR, Engelhard HH,Linninger AA, Mehta AI. Intramedullary spinalcord tumors: a review of current and futuretreatment strategies. Neurosurg Focus. 2015;39:E14.
7. Diaz RJ, Dios RR, Hattab EM, Burrell K,Rakopoulos P, Sabha N, et al. Study of the
UROSURGERY, http
biodistribution of fluorescein in glioma-infiltrated mouse brain and histopathologicalcorrelation of intraoperative findings in high-grade gliomas resected under fluorescein fluo-rescence guidance. J Neurosurg. 2015;122:1360-1369.
8. Acerbi F, Broggi M, Eoli M, Anghileri E,Cuppini L, Pollo B, et al. Fluorescein-guidedsurgery for grade IV gliomas with a dedicatedfilter on the surgical microscope: preliminary re-sults in 12 cases. Acta Neurochir (Wien). 2013;155:1277-1286.
s://doi.org/10.1016/j.wneu.2017.09.061

ORIGINAL ARTICLE
FRANCESCO ACERBI ET AL. FLUORESCEIN-GUIDED RESECTION OF INTRAMEDULLARY SPINAL CORD TUMORS
9. Höhne J, Hohenberger C, Proescholdt M,Riemenschneider MJ, Wendl C, Brawanski A,et al. Fluorescein sodium-guided resection of ce-rebral metastases-an update. Acta Neurochir (Wien).2017;159:363-367.
10. Schebesch KM, Hoehne J, Hohenberger C,Acerbi F, Broggi M, Proescholdt M, et al. Fluo-rescein sodium-guided surgery in cerebral lym-phoma. Clin Neurol Neurosurg. 2015;139:125-128.
11. Rey-Dios R, Cohen-Gadol AA. Intraoperativefluorescence for resection of hemangioblastomas.Acta Neurochir (Wien). 2013;155:1287-1292.
12. Acerbi F, Broggi M, Eoli M, Anghileri E, Cavallo C,Boffano C, et al. Is fluorescein-guided techniqueable to help in resection of high-grade gliomas?Neurosurg Focus. 2014;36:E5.
13. Schebesch KM, Proescholdt M, Höhne J,Hohenberger C, Hansen E, Riemenschneider MJ,et al. Sodium fluorescein-guided resection underthe YELLOW 560 nm surgical microscope filter inmalignant brain tumor surgeryea feasibility study.Acta Neurochir (Wien). 2013;155:693-699.
14. Sala F, Bricolo A, Faccioli F, Lanteri P, Gerosa M.Surgery for intramedullary spinal cord tumors: therole of intraoperative (neurophysiological) moni-toring. Eur Spine J. 2007;16(suppl 2):S130-S139.
15. Samartzis D, Gillis CC, Shih P, O’Toole JE,Fessler RG. Intramedullary spinal cord tumors:part i-epidemiology, pathophysiology, and diag-nosis. Glob Spine J. 2015;5:425-435.
16. Mandigo CE, Ogden AT, Angevine PD,McCormick PC. Operative management of spinalhemangioblastoma. Neurosurgery. 2009;65:1166-1177.
17. Garcés-Ambrossi GL, McGirt MJ, Mehta VA,Sciubba DM, Witham TF, Bydon A, et al. Factorsassociated with progression-free survival andlong-term neurological outcome after resection ofintramedullary spinal cord tumors: analysis of 101
WORLD NEUROSURGERY 108: 603-609,
consecutive cases. J Neurosurg Spine. 2009;11:591-599.
18. Ferrante L, Mastronardi L, Celli P, Lunardi P,Acqui M, Fortuna A. Intramedullary spinal cordependymomas—a study of 45 cases with long-term follow-up. Acta Neurochir (Wien). 1992;119:74-79.
19. Chang UK, Choe WJ, Chung SK, Chung CK,Kim HJ. Surgical outcome and prognostic factorsof spinal intramedullary ependymomas in adults.J Neurooncol. 2002;57:133-139.
20. Raco A, Esposito V, Lenzi J, Piccirilli M, Delfini R,Cantore G. Long-term follow-up of intramedullaryspinal cord tumors: a series of 202 cases. Neuro-surgery. 2005;56:972-981.
21. Klekamp J, Samii M. Intramedullary tumors. In:Klekamp J, Samii M, eds. Surgery of Spinal Tumors.Berlin: Springer Verlag; 2007:120-131.
22. Kim MS, Chung CK, Choe G, Kim IH, Kim HJ.Intramedullary spinal cord astrocytoma in adults:postoperative outcome. J Neurooncol. 2001;52:85-94.
23. Shinoda J, Yano H, Yoshimura S, Okumura A,Kaku Y, Iwama T, et al. Fluorescence-guidedresection of glioblastoma multiforme by usinghigh-dose fluorescein sodium. Technical note.J Neurosurg. 2003;99:597-603.
24. Koc K, Anik I, Cabuk B, Ceylan S. Fluoresceinsodium-guided surgery in glioblastoma multi-forme: a prospective evaluation. Br J Neurosurg.2008;22:99-103.
25. Chen B, Wang H, Ge P, Zhao J, Li W, Gu H, et al.Gross total resection of glioma with the intra-operative fluorescence-guidance of fluoresceinsodium. Int J Med Sci. 2012;9:708-714.
26. Kabuto M, Kubota T, Kobayashi H, Nakagawa T,Ishii H, Takeuchi H, et al. Experimental andclinical study of detection of glioma at surgeryusing fluorescent imaging by a surgical
DECEMBER 2017 ww
microscope after fluorescein administration. Neu-rol Res. 1997;19:9-16.
27. Kuroiwa T, Kajimoto Y, Ohta T. Development of afluorescein operative microscope for use duringmalignant glioma surgery: a technical note andpreliminary report. Surg Neurol. 1998;50:41-48.
28. Kuroiwa T, Kajimoto Y, Ohta T. Comparison be-tween operative findings on malignant glioma bya fluorescein surgical microscopy and histologicalfindings. Neurol Res. 1999;21:130-134.
29. Kuroiwa T, Kajimoto Y, Ohta T. Surgical man-agement for supratentorial astrocytic tumors.Minim Invasive Neurosurg. 1999;42:182-186.
30. Okuda T, Yoshioka H, Kato A. Fluorescence-guided surgery for glioblastoma multiformeusing high-dose fluorescein sodium with exci-tation and barrier filters. J Clin Neurosci. 2012;19:1719-1722.
31. Ferroli P, Acerbi F, Albanese E, Tringali G,Broggi M, Franzini A, et al. Application of intra-operative indocyanine green angiography for CNStumors: results on the first 100 cases. Acta NeurochirSuppl. 2011;109:251-257.
Conflict of interest statement: F. Acerbi, A. Brawanski, T.Kiris, and K-M. Schebesh received honoraria from the ZeissMeditec Company for lectures at international congresses.This work was partially supported by a donation fromMonico SpA (Venice, Italy).
Received 5 August 2017; accepted 9 September 2017
Citation: World Neurosurg. (2017) 108:603-609.https://doi.org/10.1016/j.wneu.2017.09.061
Journal homepage: www.WORLDNEUROSURGERY.org
Available online: www.sciencedirect.com
1878-8750/$ - see front matter ª 2017 Elsevier Inc. Allrights reserved.
w.WORLDNEUROSURGERY.org 609