Embed Size (px)
Citation preview

7/28/2019 Fluoroscopy-Guided Periradicular Injections in Spine
http://slidepdf.com/reader/full/fluoroscopy-guided-periradicular-injections-in-spine 1/8
Fluoroscopy-guided Periradicular Injections in Spine
Naresh Kumar, MBBS, MS (Orth), DNB, FRCS Ed, FRCS (Orth), DM (Orth)*
and Barry W. L. Tan, MBBS w
Summary: Periradicular injection is a modality that is extensively
used for diagnosing and treating nerve root pain both in the cervical
and lumbar spinal regions. It offers a viable alternative to surgical
management of radicular pain because of disorders of the intervertebral
disks or degenerative spinal conditions. These injections usually
comprise steroids and local anaesthetics. There is evidence suggesting
that periradicular injections of local anaesthetic without steroids may
be equally effective treatment for a select group of patients with
chronic function-limiting axial or extremity pain secondary to spinal
stenosis. These injections can be administered by transforaminal,
interlaminar, or caudal routes with the aid of fluoroscopy or computed tomography guidance. Despite good clinical outcomes, the underlying
mechanism of action of periradicular steroid and local anesthetic
injections is still not fully understood. We hereby describe the tech-
nique of transforaminal periradicular injections at the lumbar, lumbo-
sacral, cervical, and thoracic levels. The article gives an overview of
essential requirements for the procedure, concepts, technical tips, and
potential complications.
Key Words: selective nerve root block—transforaminal block—
epidural steroids—radicular pain—periradicular injection.
(Tech Orthop 2013;28: 55–62)
S pinal pain is a highly prevalent condition causing chronic pain and disability.1,2 Spinal pain can be present as axial
pain, radicular pain, or a combination of both.3 There areseveral possible underlying pathologies behind radicular pain,with common conditions being degenerative disk disease and disk herniation.4,5 The management of spinal radicular paininvolves a spectrum of treatment modalities—which could beconservative or interventional. The selection of a modalitydepends on the underlying pathology, severity of the condition,and the degree of symptoms.
Periradicular spinal injection is an integral part of thearmamentarium in the treatment of spinal radicular pain and isregarded as a less invasive procedure as compared to thevariety of surgical interventions available. It is reported to be
one of the most commonly performed interventions in theUnited States,6 and we surmise that it would be a similarly performed procedure worldwide. Despite its popularity, theunderlying mechanism of action, exact clinical benefit, and optimum technical aspects of the procedure have yet to befully understood and determined.7–9 It is believed that
corticosteroids are an important component of these injectionswhich work by membrane stabilization, inhibition of synthesisor action of neural peptides, phospholipase A2 activity blockade, suppression of sensitization of dorsal horn neurons,and prolonged suppression of ongoing neuronal discharge.8,9
The underlying biochemical effects of local anesthetic agentsare mediated by neural blockade altering or disrupting noci-ceptive input, reflex mechanisms of afferent fibres, self-sus-taining activity of the neurons, and the pattern of centralneuronal activities.10 There are, however, numerous studiesthat have suggested that the steroid component of the injectionmay not be essential in resulting in clinical improvement innerve root blocks, with local anesthetic-only injections show-ing similar clinical efficacy.11
There are 3 main routes of approaching the epidural spacein current practice that have been described in the literature:caudal epidural, interlaminar, and transforaminal.12 It is gen-erally regarded that the transforaminal route offers the bestclinical outcome of the 3. Transforaminal injections are per-formed with fluoroscopic or computed tomography (CT)guidance.13 Majority of the surgeons and anaesthetists prac-tising nerve root injections utilize fluoroscopic guidance.14
Guidelines for the safe conduct of periradicular injectionshave been developed by the International Spinal InterventionSociety, emphasizing specifically vigilance in avoiding unin-tended, intra-arterial injections. The risks of the procedure arelow and considering the lower costs of the procedure compared with surgical interventions, periradicular injections with or without steroids appears to be cost effective. Overall, there is a paucity of quality literature evaluating the effectiveness of periradicular injections.
PROCEDURE
We hereby describe the prerequisites for the perineuralnerve root block.
Indications15
Indications for periradicular spinal injections include, but
are not limited to the following.(1) Patients with known cause for pain who benefit by
temporary pain relief for example, disk prolapse, foraminalstenosis, degenerative disk disease with nerve rootirritation.
(2) Patients with multilevel imaging abnomalities, to moreaccurately defining the levels for possible surgery (ie, for surgical planning).
(3) Patients with equivocal neurological examination.(4) Patients with symptoms but minimal or no definitive
imaging findings.(5) Postoperative patients with unexplainable or complex
recurrent pain.
Contraindications15
Contraindications for periradicular spinal injectionsinclude, but are not limited to the following.
From the *University Orthopaedics, Hand & Reconstructive Micro-surgery Cluster; and wOrthopedic Surgery, University Spine Centre,
National University Hospital, Singapore.The authors declare that they have nothing to disclose.Address correspondence and reprint requests to Naresh Kumar, MBBS,
MS (Orth), DNB, FRCS Ed, FRCS (Orth), DM (Orth), University Orth-opaedics, Hand & Reconstructive Microsurgery Cluster, University SpineCentre, National University Hospital, 1E Kent Ridge Road, NUHS Tower Block, Level 11, Singapore 119228. E-mail: [email protected] r 2013 by Lippincott Williams & WilkinsISSN: 0148-703/13/2801-0055
I NVITED R EVIEW ARTICLE
Techniques in Orthopaedics $ Volume 28, Number 1, 2013 www.techortho.com | 55
7/28/2019 Fluoroscopy-Guided Periradicular Injections in Spine
http://slidepdf.com/reader/full/fluoroscopy-guided-periradicular-injections-in-spine 2/8
(1) Coagulopathy (International Normalized Ratio of >1.5 or platelets <50,000 /mm3).
(2) Pregnancy (because of teratogenic effects of radiation).(3) Systemic infection or skin infection over the puncture site.(4) Severe allergy to any component of the injection mixture
(injectate) or other medication.(5) Patient has received the maximum amount of steroids
allowed for a given time period unless the injection is performed without steroids.
(6) A solid bone fusion that does not allow access to the nerveroot foramen.
(7) Significant compression of the spinal cord (thoracic and cervical region) at the level to be injected.
We hereby describe the procedure of fluoroscopic-guided periradicular injections for the lumbar, cervical, and thoracicspine in Table 1.
Medication9
Diagnostic injectate - Bupivacaine Hydrochloride (0.25%)0.5 to 1 mL.
Therapeutic injectate - combination of Bupivacaine Hydro-chloride (0.25%) 0.5 to 1 mL and Triamcinolone Acetonide1 mL (40 mg/mL) (Table 2).
AnesthesiaThe procedure is carried out under adequate local
anaesthesia and minimal sedation when required. Adequatelocal anaesthesia is necessary so that the patient is cooperativeduring the procedure, whereas minimal sedation ensures thathe is conscious and coherent to answer questions about pain.
The back/neck region is painted with povidone iodine and draped. Lignocaine (2%) is infiltrated into the skin, the sub-cutaneous tissue, and the underlying musculature.
When periradicular injection is contemplated in a suitablecandidate, the following protocol is suggested.
Reconfirmation of Patient SymptomsPatient’s symptoms must be carefully assessed, especially
in terms of the following.(1) The amount of back/neck pain versus leg/arm pain.
(2) Nature of pain.(3) Location of pain.(4) Intensity of pain—Visual Analogue Score.(5) Aggravating and relieving factors.
The levels at which periradicular injection is performed is based on the history provided by the patient with regard to thedistribution and location of pain, clinical examination, and imaging findings.
Preprocedural AssessmentAllergy to contrast agent must be evaluated by the
clinician. In cases of severe iodine contrast allergy, gadoliniumand saline have been suggested as options.16 Renal impairmentalso has to be taken into consideration before the admin-
istration of contrast agents. It is still possible to perform the procedure without intravenous contrast medium enhancement, but it is more difficult. Analgesic and anti-inflammatorymedications must be stopped on the day of the procedure toavoid any likely interference to the perception of pain duringthe procedure. Informed consent must be obtained.
LUMBAR PERIRADICULAR INJECTION
Patient PositionWe prefer the prone position as it allows better visual-
ization of the lumbosacral junction and there is no need for any
TABLE 1. Equipment and Supplies Used in SNRBs
Equipment/Supplies Details and Specifications
Spinal needle (Steriseal;Unomedical, UK)
22 G, 125 mm (lumbar)22 G, 100 mm (thoracic and cervical)
Spinal needle (Steriseal) 25G, 150 mm (lumbar)
22 G, 125 mm (thoracic and cervical)Syringe 5.0mL Containing injectate (local anaesthetic and steroid)Syringe 2.5 mL Containing noniodinated myelographic contrast medium (Omnipaque 350; GE Healthcare, Cork, Ireland)Syringe 10mL With 23G, 40-mm needle containing 10mL of 1% lignocaine for local anaesthesia for skin infiltrationMiscellanous Sterile gauze, povidone-iodine scrub, alcohol scrub, sterile towel and drapes, lead apron, C-arm (Phillips BV
Libra or Siemens Arcadis Orbic)
TABLE 2. Steroid Preparations Used in SNRBs
Corticosteroids Brand Name DescriptionCommon
Dose
Methylprednisoloneacetate
Depo-Medrol Particles densely packed; smaller than red blood cells; not prone to aggregation;contains benzyl alcohol (potentially neurotoxic); may not completely dissolve
20-80 mg
Triamcinolone diacetate Aristocort Particles vary greatly in size; form aggregations 40-120 mgTriamcinolone acetonide Kenalog Particles vary greatly in size; form aggregations 40-80 mg
(ESI)20-40 mg
(other sites)
Triamcinolonehexacetonide
Aristospan Similar to triamcinolone acetonide, with less intense but more sustained action 20-40 mg
Betamethasone acetate/ phosphate mixture
CelestoneSoluspan Particles vary greatly in size; form aggregations but is soluble 12-18mg(ESI)
Dexamethasone Decadron Particles 5-10 times smaller than red blood cells; can aggregate Variable
Kumar and Tan Techniques in Orthopaedics $ Volume 28, Number 1, 2013
56 | www.techortho.com c 2013 Lippincott Williams & Wilkins

7/28/2019 Fluoroscopy-Guided Periradicular Injections in Spine
http://slidepdf.com/reader/full/fluoroscopy-guided-periradicular-injections-in-spine 3/8
side supports or restraints to support the patient during the procedure. The fluoroscopic C-arm must be positioned with acephalad tilt to allow end-on visualization of the end plates and pedicles at the level where the injection is to be carried out. Atthe lumbosacral junction, the fluoroscopic C-arm may need to be tilted up to 45 degrees for adequate visualisation of the disk
space. The patient’s lower back is prepared and draped in asterile manner.
Approach for L1-L4 Selective Nerve RootBlocks (SNRBs)
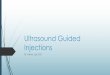
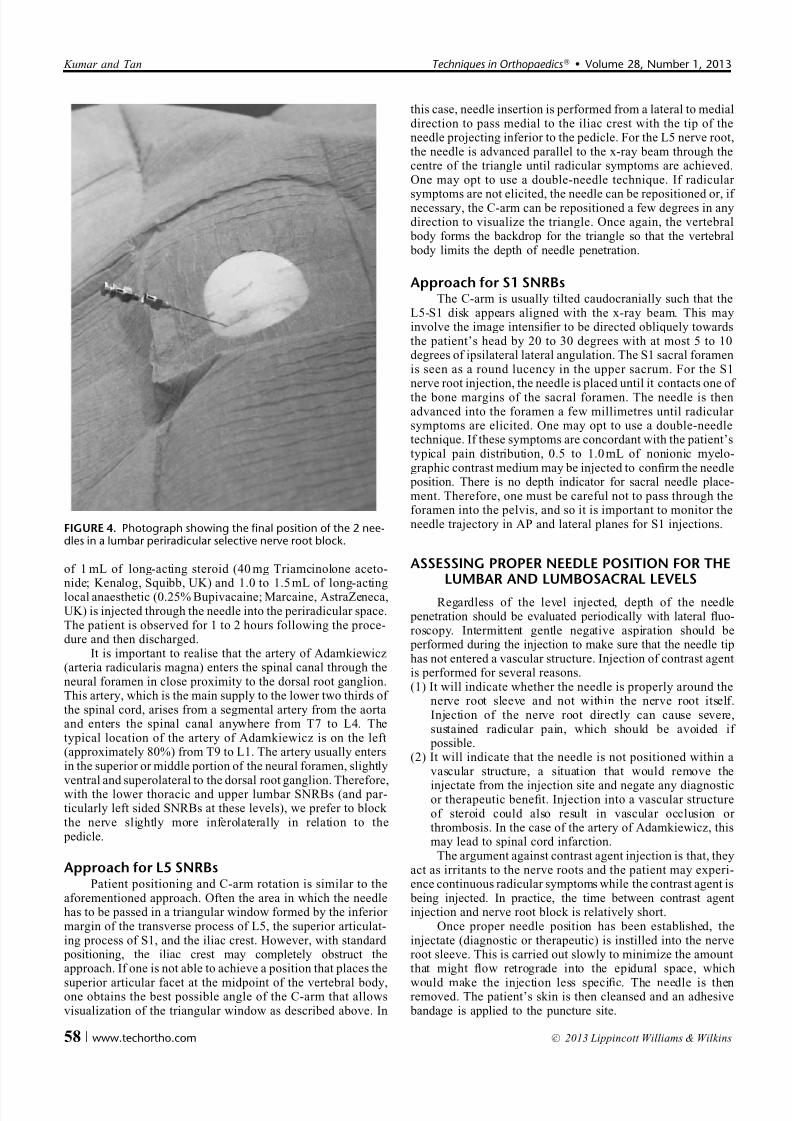
For lumbar spine, the entry point is located by measuringapproximately 4 finger-breadths distance from either side of the midline at the desired disk level using fluoroscopic C-armguidance taking images in the anteroposterior (AP) and lateral plane (Fig. 1). A coaxial 2-needle (Fig. 2, Steriseal; Uno-medical, UK), oblique extradural approach is used. First, a0.9Â125 mm needle is introduced at about 45 degrees to thehorizon. It is targeted to reach dorsal to the nerve root or in theaxilla of the nerve root depending on the requirement. For periradicular injections of lumbar nerve roots L3 and L4, theneedle is advanced to a point just inferolateral to the pedicleuntil radicular symptoms are elicited. For L1 and L2 (and T9 toT12), the needle is positioned more inferior and lateral inrelation to the pedicle (in the inferior neural foramen) todecrease the risk of injury to the artery of Adamkiewicz. Often,the needle must be passed until it makes contact with thevertebral body. If radicular symptoms are not elicited, theneedle is repositioned a few millimitres away until radicular symptoms are reported. Once the tip of this needle is just
proximal to the site of the desired position, a smaller diameter longer needle of 0.45Â150 mm is railroaded through the firstneedle such that it emerges in a suitably close position to thenerve root (Figs. 3, 4). A thicker (0.9 mm), outer needle is wellsuited to negotiate the skin, deep fascia, and muscle layerswithout bending. Thereafter, a thinner (0.45 mm) and longer second needle is railroaded through the outer needle in the
periradicular space. A thinner needle causes less damage and isassociated with a lower risk of nerve root injury. The above-mentioned technique is the author’s preference and is called the “2-needle technique.” A fair number of practitioners would be happy to use the outer thicker needle as the only conduit for delivery of the injectate.
Aspiration is attempted with a 5 mL syringe to ensure thatthe needle tip is not in any blood vessel. 0.2 to 0.5 mL of radio-opaque dye (Omnipaque 350; GE Healthcare, Cork, Ireland) isinjected through the inner needle to obtain an epidurogram,showing spread of the contrast medium along the nerve root. Ahard copy of the epidurogram is printed for record. A mixture
FIGURE 1. Photograph depicting localization of the periradicular space utilizing radiopaque ruler and anatomical landmarks usingC-arm fluoroscopy.
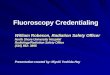
FIGURE 2. The 2 needles used in our technique. The top 2 pic-tures show the needles with stylets in situ. The bottom pictureshows the long 0.45 mm diameter needle being passed throughthe lumen of shorter 0.9-mm needle.
FIGURE 3. Photograph showing the second inner needle beingreadied for insertion through the first needle in a “railroad”technique.
Techniques in Orthopaedics $ Volume 28, Number 1, 2013 Fluoroscopy-guided Periradicular Injections
c 2013 Lippincott Williams & Wilkins www.techortho.com | 57
7/28/2019 Fluoroscopy-Guided Periradicular Injections in Spine
http://slidepdf.com/reader/full/fluoroscopy-guided-periradicular-injections-in-spine 4/8
of 1 mL of long-acting steroid (40 mg Triamcinolone aceto-nide; Kenalog, Squibb, UK) and 1.0 to 1.5 mL of long-actinglocal anaesthetic (0.25% Bupivacaine; Marcaine, AstraZeneca,UK) is injected through the needle into the periradicular space.The patient is observed for 1 to 2 hours following the proce-dure and then discharged.
It is important to realise that the artery of Adamkiewicz(arteria radicularis magna) enters the spinal canal through theneural foramen in close proximity to the dorsal root ganglion.This artery, which is the main supply to the lower two thirds of the spinal cord, arises from a segmental artery from the aortaand enters the spinal canal anywhere from T7 to L4. Thetypical location of the artery of Adamkiewicz is on the left(approximately 80%) from T9 to L1. The artery usually entersin the superior or middle portion of the neural foramen, slightlyventral and superolateral to the dorsal root ganglion. Therefore,with the lower thoracic and upper lumbar SNRBs (and par-ticularly left sided SNRBs at these levels), we prefer to block the nerve slightly more inferolaterally in relation to the pedicle.
Approach for L5 SNRBsPatient positioning and C-arm rotation is similar to the
aforementioned approach. Often the area in which the needlehas to be passed in a triangular window formed by the inferior margin of the transverse process of L5, the superior articulat-ing process of S1, and the iliac crest. However, with standard positioning, the iliac crest may completely obstruct theapproach. If one is not able to achieve a position that places the
superior articular facet at the midpoint of the vertebral body,one obtains the best possible angle of the C-arm that allowsvisualization of the triangular window as described above. In
this case, needle insertion is performed from a lateral to medialdirection to pass medial to the iliac crest with the tip of theneedle projecting inferior to the pedicle. For the L5 nerve root,the needle is advanced parallel to the x-ray beam through thecentre of the triangle until radicular symptoms are achieved.One may opt to use a double-needle technique. If radicular
symptoms are not elicited, the needle can be repositioned or, if necessary, the C-arm can be repositioned a few degrees in anydirection to visualize the triangle. Once again, the vertebral body forms the backdrop for the triangle so that the vertebral body limits the depth of needle penetration.
Approach for S1 SNRBsThe C-arm is usually tilted caudocranially such that the
L5-S1 disk appears aligned with the x-ray beam. This mayinvolve the image intensifier to be directed obliquely towardsthe patient’s head by 20 to 30 degrees with at most 5 to 10degrees of ipsilateral lateral angulation. The S1 sacral foramenis seen as a round lucency in the upper sacrum. For the S1nerve root injection, the needle is placed until it contacts one of
the bone margins of the sacral foramen. The needle is thenadvanced into the foramen a few millimetres until radicular symptoms are elicited. One may opt to use a double-needletechnique. If these symptoms are concordant with the patient’stypical pain distribution, 0.5 to 1.0 mL of nonionic myelo-graphic contrast medium may be injected to confirm the needle position. There is no depth indicator for sacral needle place-ment. Therefore, one must be careful not to pass through theforamen into the pelvis, and so it is important to monitor theneedle trajectory in AP and lateral planes for S1 injections.
ASSESSING PROPER NEEDLE POSITION FOR THELUMBAR AND LUMBOSACRAL LEVELS
Regardless of the level injected, depth of the needle penetration should be evaluated periodically with lateral fluo-roscopy. Intermittent gentle negative aspiration should be performed during the injection to make sure that the needle tiphas not entered a vascular structure. Injection of contrast agentis performed for several reasons.(1) It will indicate whether the needle is properly around the
nerve root sleeve and not within the nerve root itself.Injection of the nerve root directly can cause severe,sustained radicular pain, which should be avoided if possible.
(2) It will indicate that the needle is not positioned within avascular structure, a situation that would remove the
injectate from the injection site and negate any diagnosticor therapeutic benefit. Injection into a vascular structureof steroid could also result in vascular occlusion or thrombosis. In the case of the artery of Adamkiewicz, thismay lead to spinal cord infarction.
The argument against contrast agent injection is that, theyact as irritants to the nerve roots and the patient may experi-ence continuous radicular symptoms while the contrast agent is being injected. In practice, the time between contrast agentinjection and nerve root block is relatively short.
Once proper needle position has been established, theinjectate (diagnostic or therapeutic) is instilled into the nerveroot sleeve. This is carried out slowly to minimize the amountthat might flow retrograde into the epidural space, which
would make the injection less specific. The needle is thenremoved. The patient’s skin is then cleansed and an adhesive bandage is applied to the puncture site.
FIGURE 4. Photograph showing the final position of the 2 nee-dles in a lumbar periradicular selective nerve root block.
Kumar and Tan Techniques in Orthopaedics $ Volume 28, Number 1, 2013
58 | www.techortho.com c 2013 Lippincott Williams & Wilkins

7/28/2019 Fluoroscopy-Guided Periradicular Injections in Spine
http://slidepdf.com/reader/full/fluoroscopy-guided-periradicular-injections-in-spine 5/8
CERVICAL PERIRADICULAR INJECTION
Author’s Preferred Technique17
Patient PositioningThe patient is placed in the lateral position on the oper-
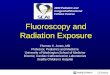
ating table with the symptomatic side facing up ( Fig. 5). Oneor 2 pillows are placed under the head to prevent lateral flexionof the cervical spine. The neck is slightly extended and the patient is requested to depress both the shoulders. This positionhelps to visualize the entire cervical spine in a majority of patients.
Approach for C3-C8 SNRBsThe fluoroscopic C-arm is centred on the relevant level and
tilted by 20 to 30 degrees to obtain oblique projections of thecervical spine (Fig. 5). This would show the neural foramen end-on. A metallic ruler is placed transversely on the patient’s neck,so that it projects at the upper border of the nerve root foramen of the level to be injected and parallel to the disk space. A hori-
zontal line is drawn on the skin at this level. A vertical line isdrawn joining the posterior borders of the lateral masses of theadjacent vertebrae. Intersection of these lines gives us the entry point for the needle, which overlies the bulk of the trapeziusmuscle and falls in the posterior triangle of the neck.
The injection site is aseptically prepared and localanaesthetic is infiltrated into skin and subcutaneous tissues. For the “2-needle technique” we use a 0.9Â100 mm needle as the“outer needle” and 0.45Â125 mm needle as the “inner nee-dle.” The 0.9-mm needle with stylet is introduced through theentry point on the skin and directed using image guidance
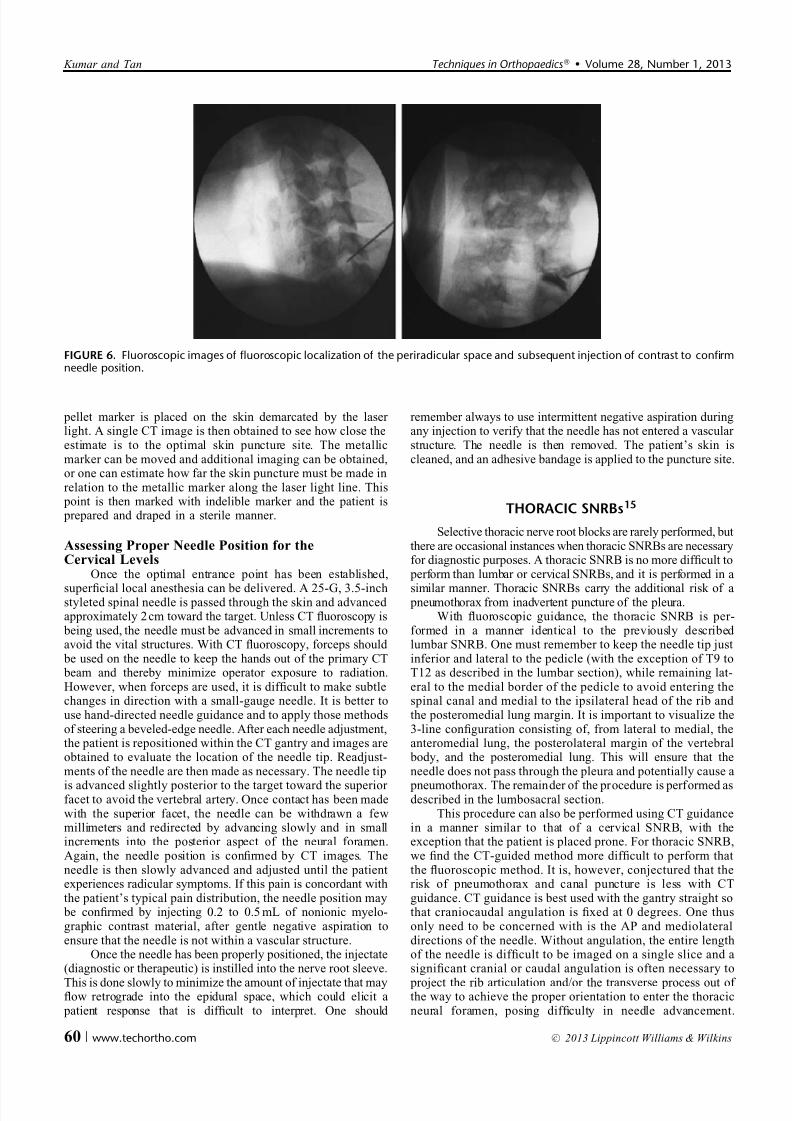
through the bulk of the trapezius muscle, keeping it posterior tothe neurovascular bundle of the neck. The needle is advanced under image guidance until the tip of the needle is just ante-rolateral to the posterior border of neural foramen, withoutactually entering it (Fig. 6). An AP view is also obtained at thisstage. The stylet is removed and the inner needle is inserted through the lumen of the outer needle. The inner needle isadvanced with caution, to enter the nerve root canal under image guidance, observing the patient’s response. In a majorityof patients, radicular pain is reproduced at this point,which usually matches their clinical symptoms. Aspiration isattempted with a 5-mL syringe to ensure that the needle tip isnot in any blood vessel. A 0.2 to 0.5 mL of radio-opaque dye isinjected through the inner needle to obtain an epidurogram,
showing spread of the contrast medium along the nerve root(Fig. 6). A hard copy of the epidurogram is printed for record.A mixture of 1 mL of long-acting steroid and 0.5 to 1 mL of long-acting local anaesthetic is injected through the needle intothe periradicular space. The patient is observed for 1 to 2 hoursfollowing the procedure and then discharged.
Alternative Approach for C3-C8 SNRBs UsingCT-guidance15
The cervical nerve roots must be approached from theanterolateral aspect of the neck because of the lateral massobstructing a posterolateral or lateral approach. The antero-lateral approach has greater risk because the ipsilateral carotid sheath, adjacent nerves, and vertebral artery are along the
needle pathway. Therefore, it is believed that the safestapproach for cervical SNRB is with CT guidance. This willdemonstrate the location of the carotid sheath structures and vertebral artery.
The patient is placed on the CT table in the lateraldecubitus position with the side to be injected up. A cushion is placed under the head and/or neck to make the patient morecomfortable and also to keep the patient’s neck in neutral position without any significant lateral flexion. Most impor-tantly, the neck should not be flexed toward the side to beinjected, because this narrows the ipsilateral neural foramen.Slight lateral flexion contralateral to the side of puncture mayfurther facilitate needle placement into the target foramen.Many patients have their neck flexed anteriorly when placed in
the lateral decubitus position. The patient’s neck is optimally positioned in neutral position by slight “hyperextension” rel-ative to the beginning position. Another obstacle may be vis-ualizing the upper cervical nerve roots in a patient who hasmetallic dental work. This may cause significant streak artifactand suboptimal visualization of the nerve root. If it is antici- pated that streak artifact will significantly alter the CT imagequality, we position the patient’s head in mild hyperextensionto raise the jaw out of the scanning plane. If this does not work,asking the patient to open his or her mouth during the proce-dure may reduce the streak artifact.
There is only a very narrow window in which to safelyaccess the cervical nerve root, hence it is extremely importantthat the site of skin puncture be as close as possible to the
preplanned trajectory. This method uses a small metallic BB pellet marker to localize the puncture site instead of the grid. Aseries of localizer CT scans are first obtained. Next, the BB
FIGURE 5. Photograph showing positioning of patient andC-arm fluoroscopy during cervical SNRB.
Techniques in Orthopaedics $ Volume 28, Number 1, 2013 Fluoroscopy-guided Periradicular Injections
c 2013 Lippincott Williams & Wilkins www.techortho.com | 59
7/28/2019 Fluoroscopy-Guided Periradicular Injections in Spine
http://slidepdf.com/reader/full/fluoroscopy-guided-periradicular-injections-in-spine 6/8
pellet marker is placed on the skin demarcated by the laser light. A single CT image is then obtained to see how close theestimate is to the optimal skin puncture site. The metallicmarker can be moved and additional imaging can be obtained,or one can estimate how far the skin puncture must be made inrelation to the metallic marker along the laser light line. This point is then marked with indelible marker and the patient is prepared and draped in a sterile manner.
Assessing Proper Needle Position for theCervical Levels
Once the optimal entrance point has been established,
superficial local anesthesia can be delivered. A 25-G, 3.5-inchstyleted spinal needle is passed through the skin and advanced approximately 2 cm toward the target. Unless CT fluoroscopy is being used, the needle must be advanced in small increments toavoid the vital structures. With CT fluoroscopy, forceps should be used on the needle to keep the hands out of the primary CT beam and thereby minimize operator exposure to radiation.However, when forceps are used, it is difficult to make subtlechanges in direction with a small-gauge needle. It is better touse hand-directed needle guidance and to apply those methodsof steering a beveled-edge needle. After each needle adjustment,the patient is repositioned within the CT gantry and images areobtained to evaluate the location of the needle tip. Readjust-ments of the needle are then made as necessary. The needle tip
is advanced slightly posterior to the target toward the superior facet to avoid the vertebral artery. Once contact has been madewith the superior facet, the needle can be withdrawn a fewmillimeters and redirected by advancing slowly and in smallincrements into the posterior aspect of the neural foramen.Again, the needle position is confirmed by CT images. Theneedle is then slowly advanced and adjusted until the patientexperiences radicular symptoms. If this pain is concordant withthe patient’s typical pain distribution, the needle position may be confirmed by injecting 0.2 to 0.5 mL of nonionic myelo-graphic contrast material, after gentle negative aspiration toensure that the needle is not within a vascular structure.
Once the needle has been properly positioned, the injectate(diagnostic or therapeutic) is instilled into the nerve root sleeve.
This is done slowly to minimize the amount of injectate that mayflow retrograde into the epidural space, which could elicit a patient response that is difficult to interpret. One should
remember always to use intermittent negative aspiration duringany injection to verify that the needle has not entered a vascular structure. The needle is then removed. The patient’s skin iscleaned, and an adhesive bandage is applied to the puncture site.
THORACIC SNRBs15
Selective thoracic nerve root blocks are rarely performed, butthere are occasional instances when thoracic SNRBs are necessaryfor diagnostic purposes. A thoracic SNRB is no more difficult to perform than lumbar or cervical SNRBs, and it is performed in a
similar manner. Thoracic SNRBs carry the additional risk of a pneumothorax from inadvertent puncture of the pleura.
With fluoroscopic guidance, the thoracic SNRB is per-formed in a manner identical to the previously described lumbar SNRB. One must remember to keep the needle tip justinferior and lateral to the pedicle (with the exception of T9 toT12 as described in the lumbar section), while remaining lat-eral to the medial border of the pedicle to avoid entering thespinal canal and medial to the ipsilateral head of the rib and the posteromedial lung margin. It is important to visualize the3-line configuration consisting of, from lateral to medial, theanteromedial lung, the posterolateral margin of the vertebral body, and the posteromedial lung. This will ensure that theneedle does not pass through the pleura and potentially cause a
pneumothorax. The remainder of the procedure is performed asdescribed in the lumbosacral section.
This procedure can also be performed using CT guidancein a manner similar to that of a cervical SNRB, with theexception that the patient is placed prone. For thoracic SNRB,we find the CT-guided method more difficult to perform thatthe fluoroscopic method. It is, however, conjectured that therisk of pneumothorax and canal puncture is less with CTguidance. CT guidance is best used with the gantry straight sothat craniocaudal angulation is fixed at 0 degrees. One thusonly need to be concerned with is the AP and mediolateraldirections of the needle. Without angulation, the entire lengthof the needle is difficult to be imaged on a single slice and asignificant cranial or caudal angulation is often necessary to
project the rib articulation and/or the transverse process out of the way to achieve the proper orientation to enter the thoracicneural foramen, posing difficulty in needle advancement.
FIGURE 6. Fluoroscopic images of fluoroscopic localization of the periradicular space and subsequent injection of contrast to confirmneedle position.
Kumar and Tan Techniques in Orthopaedics $ Volume 28, Number 1, 2013
60 | www.techortho.com c 2013 Lippincott Williams & Wilkins
7/28/2019 Fluoroscopy-Guided Periradicular Injections in Spine
http://slidepdf.com/reader/full/fluoroscopy-guided-periradicular-injections-in-spine 7/8
Therefore, we believe that fluoroscopic guidance is best suited for a thoracic SNRB.
Pain Response Assessment in Nerve Root BlocksWhen radicular pain is elicited, it is essential to question
the patient about the pain distribution. Often, the patient
describes the procedurally induced pain as much more severeand often in a larger distribution than expected. This responsemay still be considered concordant if the patient’s typicalradicular pain is a subset of this larger distribution. If the procedural pain is entirely discordant with the patient’s typical pain, the SNRB for this nerve root should be abandoned and either another nerve root level should be selected or the pro-cedure should be aborted. If the patient is uncertain whether the procedural pain is concordant or discordant, that level can be injected and the patient can be reassessed before discharge.If, at the time, the patient’s symptoms have resolved, there isnothing further to do. If the patient remains symptomatic, the patient can be brought back in a few days after any availableimaging has been reassessed.
It is common for a patient to experience numbness in thedistribution of the nerve injected. This typically lasts < 3 hours,although it can persist for up to 24 hours. Mild, persistent painmay linger, but severe pain after injection is unusual. For alumbar injection, it is important to observe the patient’s sta- bility on standing immediately after the procedure becausemotor nerve fibers can also be affected. The response should becompared with the preprocedure evaluation. Weakness is moreoften seen when 0.5%, as opposed to 0.25%, bupivacaine isused. Patients are often not aware that they are weak until theytry to walk, and so it is important to assist them when theystand and walk initially as they get up from the table. Weak-ness may last 1 to 3 hours, and the patient’s postprocedure stayshould be extended if weakness is observed after SNRB. For a
cervical injection, the patient’s upper extremity strength should be tested and compared with the preprocedure evaluation.
For any SNRB, the patient should refrain from perform-ing tasks that require the strength and dexterity of the affected muscles, at least for the remainder of the day and until pre- procedure strength and dexterity have returned. Rarely, bilat-eral epidural spread may occur after SNRB that may affectsensation or cause weakness bilaterally. SNRB may rarely beassociated with vasovagal reactions.
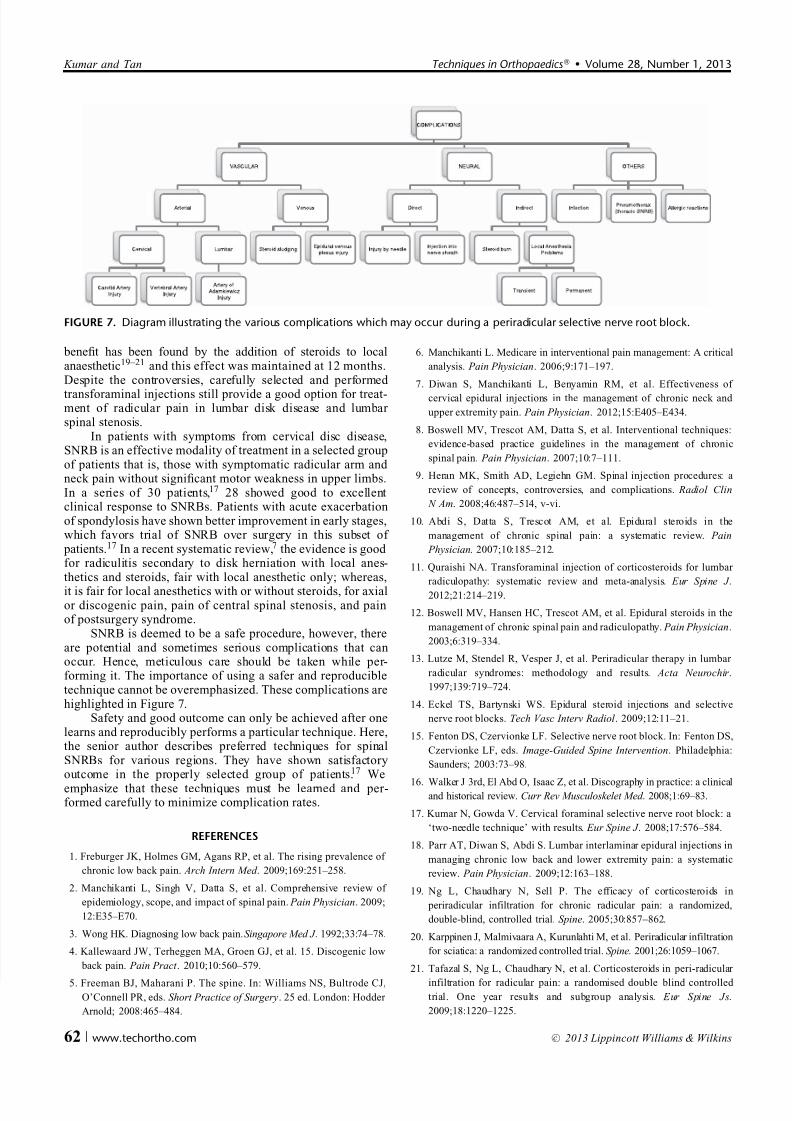
POTENTIAL COMPLICATIONS
(1) Bleeding(2) Infection
(3) Thecal sac puncture and headache(4) Allergic reactions pertaining to the medications(5) Risk of pneumothorax for thoracic nerve block (6) Vasovagal reactions and ataxia, especially for cervical
nerve block (7) Paraplegia caused by damage to the artery of Adamkiewicz
POSTPROCEDURE CARE/FOLLOW-UP
If the patient has no appreciable loss of motor strength or coordination, he or she can be observed for 1 to 2 hours,reevaluated, and then discharged. If there is some loss of motor strength or coordination, the patient is placed in a bed or lounge chair and is reevaluated every 30 minutes until he or
she returns to normal levels of strength. Until that time, the patient is allowed to ambulate only with assistance. All patients having SNRB are discharged into the care of a
responsible person. The patient is asked not to drive or performany heavy tasks that would require the use of the affected musculature until at least the next morning, at which timestrength should be reevaluated.
Immediate
(1) The patient should be observed for at least 1 to 2 hoursafter SNRB or longer if there is a motor deficit.(2) The patient may sit in a reclining lounge chair, however, if
there is significant postprocedure pain, or if the patientreceived intravenous sedation, he or she should be placed at bed rest.
(3) Blood pressure, pulse, heart rate, and respiration areevaluated every 30 minutes.
Discharge(1) The patient is discharged into the care of a responsible
person especially if sedation was administered.(2) The patient is instructed not to drive or perform any other
tasks that require quick reaction time for the remainder of
the day, especially if sedation is administered.(3) A 2- to 3-day nonrenewable prescription for a narcotic painreliever and/or a muscle relaxant is given to the patient.
(4) Multiple adhesive bandages may be on the patient’s back or neck. These should remain dry for at least 24 hours, atwhich point they can be removed.
(5) Patients are instructed to continue to take their prescriptionmedication, although pain medication may be tapered asindicated.
(6) A discharge summary should be given to the patientoutlining the following.
(a) Which procedure was performed and at what levels.(b) Procedurally related symptoms that typically resolve in
7 to 10 days.
i Pain at the needle puncture site(s).ii Mild increased back or neck stiffness.
iii Deep back or neck pain.
(7) Treatment for mild postprocedure symptoms.
i Rest the affected area for 3 to 4 days.ii Avoid movements that aggravate the pain.
iii Use cold compresses to the painful area.
(8) Signs and symptoms of infection.
i Fever.ii Chills.
iii Swelling or drainage from the puncture sites.
iv New back or neck pain that is different from theusual pain.
(9) Signs and symptoms of possibly more serious problems.
i Stiff neck.ii Increasing pain.
iii Motor dysfunction such as difficulty walking or lifting.
iv Bowel or bladder dysfunction.
DISCUSSION
Transforaminal epidural injections show a significantreduction of pain scores in patients with lumbar radiculopathy
when compared with doing nothing, conservative managementwithout injection therapy, and probably lumbar interlaminar epidural injections.18 In a meta-analysis,11 no additional
Techniques in Orthopaedics $ Volume 28, Number 1, 2013 Fluoroscopy-guided Periradicular Injections
c 2013 Lippincott Williams & Wilkins www.techortho.com | 61
7/28/2019 Fluoroscopy-Guided Periradicular Injections in Spine
http://slidepdf.com/reader/full/fluoroscopy-guided-periradicular-injections-in-spine 8/8
benefit has been found by the addition of steroids to localanaesthetic19–21 and this effect was maintained at 12 months.Despite the controversies, carefully selected and performed
transforaminal injections still provide a good option for treat-ment of radicular pain in lumbar disk disease and lumbar spinal stenosis.
In patients with symptoms from cervical disc disease,SNRB is an effective modality of treatment in a selected groupof patients that is, those with symptomatic radicular arm and neck pain without significant motor weakness in upper limbs.In a series of 30 patients,17 28 showed good to excellentclinical response to SNRBs. Patients with acute exacerbationof spondylosis have shown better improvement in early stages,which favors trial of SNRB over surgery in this subset of patients.17 In a recent systematic review,7 the evidence is good for radiculitis secondary to disk herniation with local anes-thetics and steroids, fair with local anesthetic only; whereas,
it is fair for local anesthetics with or without steroids, for axialor discogenic pain, pain of central spinal stenosis, and painof postsurgery syndrome.
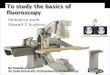
SNRB is deemed to be a safe procedure, however, thereare potential and sometimes serious complications that canoccur. Hence, meticulous care should be taken while per-forming it. The importance of using a safer and reproducibletechnique cannot be overemphasized. These complications arehighlighted in Figure 7.
Safety and good outcome can only be achieved after onelearns and reproducibly performs a particular technique. Here,the senior author describes preferred techniques for spinalSNRBs for various regions. They have shown satisfactoryoutcome in the properly selected group of patients.17 We
emphasize that these techniques must be learned and per-formed carefully to minimize complication rates.
REFERENCES
1. Freburger JK, Holmes GM, Agans RP, et al. The rising prevalence of
chronic low back pain. Arch Intern Med . 2009;169:251–258.
2. Manchikanti L, Singh V, Datta S, et al. Comprehensive review of
epidemiology, scope, and impact of spinal pain. Pain Physician. 2009;
12:E35–E70.
3. Wong HK. Diagnosing low back pain. Singapore Med J . 1992;33:74–78.
4. Kallewaard JW, Terheggen MA, Groen GJ, et al. 15. Discogenic low
back pain. Pain Pract . 2010;10:560–579.
5. Freeman BJ, Maharani P. The spine. In: Williams NS, Bultrode CJ,O’Connell PR, eds. Short Practice of Surgery. 25 ed. London: Hodder
Arnold; 2008:465–484.
6. Manchikanti L. Medicare in interventional pain management: A critical
analysis. Pain Physician. 2006;9:171–197.
7. Diwan S, Manchikanti L, Benyamin RM, et al. Effectiveness of
cervical epidural injections in the management of chronic neck and
upper extremity pain. Pain Physician. 2012;15:E405–E434.
8. Boswell MV, Trescot AM, Datta S, et al. Interventional techniques:
evidence-based practice guidelines in the management of chronic
spinal pain. Pain Physician. 2007;10:7–111.
9. Heran MK, Smith AD, Legiehn GM. Spinal injection procedures: a
review of concepts, controversies, and complications. Radiol Clin
N Am. 2008;46:487–514, v-vi.
10. Abdi S, Datta S, Trescot AM, et al. Epidural steroids in the
management of chronic spinal pain: a systematic review. Pain
Physician. 2007;10:185–212.
11. Quraishi NA. Transforaminal injection of corticosteroids for lumbar
radiculopathy: systematic review and meta-analysis. Eur Spine J .
2012;21:214–219.
12. Boswell MV, Hansen HC, Trescot AM, et al. Epidural steroids in the
management of chronic spinal pain and radiculopathy. Pain Physician.
2003;6:319–334.
13. Lutze M, Stendel R, Vesper J, et al. Periradicular therapy in lumbar
radicular syndromes: methodology and results. Acta Neurochir .
1997;139:719–724.
14. Eckel TS, Bartynski WS. Epidural steroid injections and selective
nerve root blocks. Tech Vasc Interv Radiol . 2009;12:11–21.
15. Fenton DS, Czervionke LF. Selective nerve root block. In: Fenton DS,
Czervionke LF, eds. Image-Guided Spine Intervention. Philadelphia:
Saunders; 2003:73–98.
16. Walker J 3rd, El Abd O, Isaac Z, et al. Discography in practice: a clinical
and historical review. Curr Rev Musculoskelet Med . 2008;1:69–83.
17. Kumar N, Gowda V. Cervical foraminal selective nerve root block: a
‘two-needle technique’ with results. Eur Spine J . 2008;17:576–584.
18. Parr AT, Diwan S, Abdi S. Lumbar interlaminar epidural injections in
managing chronic low back and lower extremity pain: a systematic
review. Pain Physician. 2009;12:163–188.
19. Ng L, Chaudhary N, Sell P. The efficacy of corticosteroids in
periradicular infiltration for chronic radicular pain: a randomized,
double-blind, controlled trial. Spine. 2005;30:857–862.
20. Karppinen J, Malmivaara A, Kurunlahti M, et al. Periradicular infiltration
for sciatica: a randomized controlled trial. Spine. 2001;26:1059–1067.
21. Tafazal S, Ng L, Chaudhary N, et al. Corticosteroids in peri-radicular
infiltration for radicular pain: a randomised double blind controlled trial. One year results and subgroup analysis. Eur Spine Js.
2009;18:1220–1225.
FIGURE 7. Diagram illustrating the various complications which may occur during a periradicular selective nerve root block.
Kumar and Tan Techniques in Orthopaedics $ Volume 28, Number 1, 2013
62 | www.techortho.com c 2013 Lippincott Williams & Wilkins