Embed Size (px)
Citation preview

FNE Mission
• To improve health outcomes of our citizens by enhancing the practice of nursing through….– leadership development– research– demonstration projects
FNE Vision
To become a significant conduit through which innovative ideas related to health and healthcare can be evaluated and disseminated to the principal arenas of professional nursing and healthcare practice in North Carolina
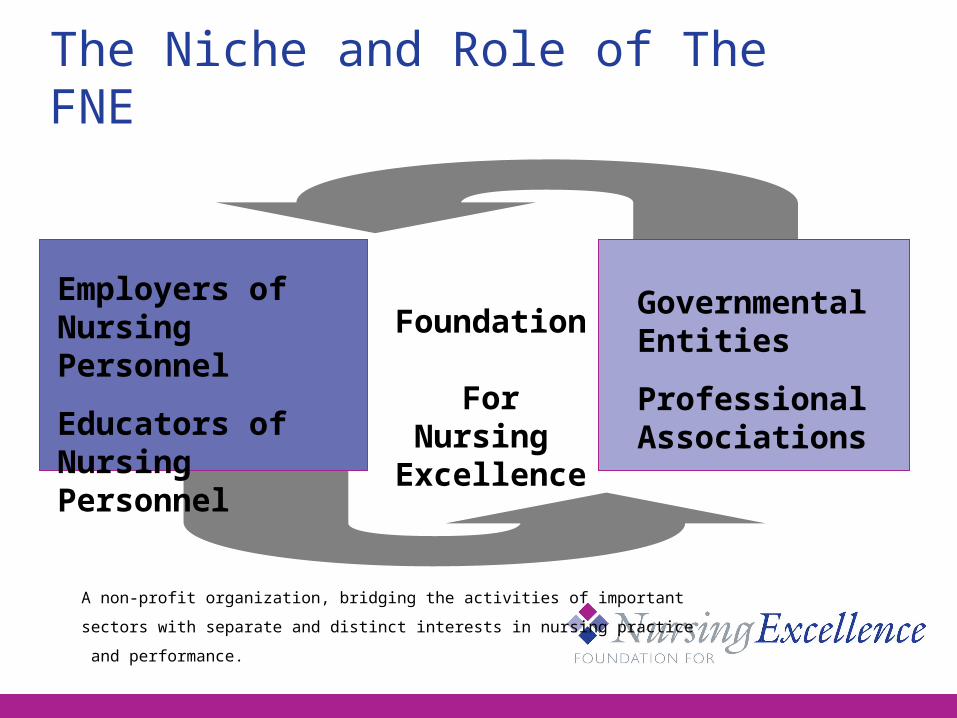
The Niche and Role of The FNE
A non-profit organization, bridging the activities of important
sectors with separate and distinct interests in nursing practice
and performance.
Employers ofNursing Personnel
Educators ofNursing Personnel
Foundation For Nursing Excellence
GovernmentalEntities
Professional Associations
Board of Directors• Beverly Foster, RN, PhD – Chair• Janice McRorie, RN, MSN – Vice Chair• Gordon DeFriese, PhD – Sec/Treas• Lynda McDaniel, MPA• Gary Bowers, JD• Tremonteo Crawford, RN, MSN• Mary Ellen Bonczek, RN, MPA• Charles Willson, MD• Chair, NC Board of Nursing Ex-officio
• Polly Johnson, RN, MSN, FAAN, President & CEO
Foundation History & Initiatives
• Created in 2002 by NC Board of Nursing
• Convened first Patient Safety Symposium in NC – 2005; Just Culture
• Enhancing new nurse competence and confidence development; retention
• Increasing # of BSN-prepared nurses in NC
Financial Support
• Grants to support specific projects from BCBSNCF, TDE, KBR, UNC-GA, RWJF/NWHF/Jonas Center
• Major support from leading healthcare systems in NC and the NCBON
• Individual donations

WNC RIBN Project
RIBN Background• Partners Investing in Nursing (PIN) grant from
RWJF/NWHF/Jonas Center for Nursing Excellence of NYC
• Multi-regional project (NC & NYC)• Adapt Oregon (OCNE) model to increase
supply & distribution of BSN-prepared RNs
• WNC Project Partners: WCU, AB Tech, FNE• NC IOM Nursing Workforce Priority
Expected Outcomes
• Increase # of BSNs poised for higher degrees
• Increase RN preparation for complex, hi tech, fast-paced work environment
• Increase RN preparation in public health, gerontology, leadership
• Increase diversity of nursing workforce
Increasing Nurse Faculty Pipeline
• Current & increasing faculty shortage
• 65% of new nurses have ADN degrees
• 80% of current MSN/doctoral faculty began @ BSN level
• Only 15% of ADN graduates complete BSN degrees; 3% complete MSN or higher degree
New Educational Tract
• Partnership between community college and baccalaureate nursing programs
• Dual Acceptance/Dual Enrollment • Four Year program:
– Year 1: Meet prerequisites for both nursing programs @ community college
– Years 2 -3: Complete ADN Program plus university courses; take NCLEX
– Year 4: Complete BSN degree while eligible for employment as licensed RN
RIBN Project Status
• Finalize all CC and University entrance and curriculum requirements – Fall 2009
• Hired RIBN Nursing Advisor 9/2009
• 1st cohort of students begin Fall 2010; first BSN graduates in 2014
• To serve as model for implementation across NC
Transition to Practice Project• NC IOM Nursing Workforce Priority
• AHRQ-funded Research Conference 2005
• Funders: BCBSNCF, TDE, KBR
• Phase I – 2006-08– Survey existing transition programs in NC– Identify key elements that contribute to
competence and confidence development
Phase I Study Population
• Newly Licensed RNs within 1st 6 months of employment and their preceptors
• 3 comparison groups in 29 hospitals: – a nationally standardized assessment and
competence development system– employer-developed formal transition
programs– “traditional” new employee orientation
programs
Phase I Research Questions• What is the relationship of the type of
transition to practice experience and:– progression of competency development – practice errors– risk for practice breakdown?
• What is the relationship of the preceptor characteristics to competency development among newly licensed RNs?
The Data Reveals…
• The better the quality rating of new nurse/preceptor relationship, the higher the new RN perceived competence (statistically significant across all 3 rounds of data collection)
• The higher the competency score, the fewer reported errors (statistically significant Rounds 2 and 3)
Competence DevelopmentAreas of Concern
– Recognizing care demands exceeding ability
– Effective time management/workload organization
– Recognizing implications of clinical presentation
– Appropriate use of research findings– Fully understanding
assignments/physician’s orders (Statistically significant differences between comparison
groups in Round 3)
Errors & Risk for Practice Breakdown
• 30-55% reported errors in 1st 6 months• >70% new nurses in all three rounds reported
risk for practice breakdown occurring at least once
• New nurse identified a significantly higher risk for practice breakdown than that identified by the preceptor
• The longer the orientation period the fewer errors or risk for breakdown reported
Summary of Findings• Quality of partnership with preceptor has a direct
relationship with how competent new RNs feel about their nursing practice; competence links to fewer errors
• No one transition approach emerged as significantly superior to others in all perspectives
• 8 weeks = average length of orientation• New RNs reported lower competence scores in
clinical reasoning and judgment across all Rounds • Full Report of Data Analysis @ www.ffne.org
Phase II - Transition to Practice Project
• Identify Best/Promising Practices:– Preceptor role development/preparation– Preceptor interface with new nurse– Use of simulation in competence assessment
and development
• Develop Interventions based on best/promising
practices

Preceptor Role Development Best Practices
• Need organizational “buy in” for effective preceptor preparation and function.
• Preceptor selection criteria, competencies, position description, and performance evaluation, plus recognition are needed.
• Ongoing preceptor education and support are needed.
• A “tool box” for preceptors to use with new nurses helpful
Best Practices in Simulation
• Facilitator development & debriefing essential to successful use of tool
• Collaboration among organizations to decrease cost & maintain quality
• Build statewide “scenario” bank• Relationship between SONs & healthcare
delivery systems builds stronger baseline for new grad performance
Preceptor Role Development Training Package
• QSEN Competencies as framework
• Basic preceptor training principles in online learning modules
• On-site interactive learning modules using simulation scenarios
• Incorporates TeamSTEPPS and other patient safety training modules/concepts
Transition to Practice Project Timeline
• Phase II– Identification of Best Practices 2009– Development of Interventions 2009 (in progress)
• Phase III– Pilot/evaluate/Revise Interventions 2010-11– Training package available for use 2012
• Phase IV – Consider Preceptor Certification Program– Augment new nurse training scenarios– Finalize model for statewide implementation by 2015
Building a Just Culture Healthcare Community
• To enhance patient safety by supporting:– Cultural shift from “blame and shame” to learning
and quality improvement– Analyze behaviors/causes of adverse events– Assign accountability
• Support current efforts of NC Hospital Center for Quality & Patient Safety and the NC BON
• Extend this framework into all delivery and regulatory systems
Questions?
Please visit our website at www.ffne.org





























