Embed Size (px)
Citation preview

Hand Clin 19 (2003) 523–538
Focal dystonia: advances in brain imaging andunderstanding of fine motor control in musicians
Eckart AltenmullerUniversity for Music and Drama, Hannover Institute for Music Physiology and Musicians’ Medicine,
Hohenzollernstr. 47, Hannover D-30161, Germany
Music performance at a professional level isone of the most demanding tasks for the human
central nervous system. It involves the preciseexecution of fast and, in many instances, extremelycomplex physical movements under continuousauditory feedback. A further aspect of music per-
formance—although not specifically addressed inthis article—concerns the involvement of emo-tional experiences.
Extensive practice is required to develop newskills and carry out these complex tasks. Motorskills can be automated only by countless re-
petitions; aural skills, in contrast, are developedthrough a broad variety of listening experiences.These skills are not represented in isolated brain
areas, but rather depend on the multiple con-nections and interactions established during train-ing within and between the different regions of thebrain. The general ability of the human central
nervous system to adapt to changing environmen-tal conditions and newly imposed tasks during itsentire lifespan is referred to as plasticity; in music,
learning through experience and training isaccompanied by development and changes thattake place not only in the brain’s neuronal net-
works, for example, as a strengthening of neurons’connections, but also occur in its overall grossstructure.
The aim of the present article is to give a short
review of current knowledge about the basicneurophysiology and the brain mechanisms in-volved in the acquisition and maintenance of
manual skills in professional musicians. To un-derstand neural substrates of music performance
E-mail address: [email protected]
0749-0712/03/$ - see front matter � 2003 Elsevier Inc. All ri
doi:10.1016/S0749-0712(03)00043-X
it is first necessary to understand some basicneuroanatomy.
Neuroanatomic and neurophysiologic background
Brain imaging methods
During the last decade, rapid improvements inbrain imaging methods have enabled researchers
to carry out substantial new investigations intothe biologic foundations of music performance.The term ‘‘functional brain imaging’’ covers the
various methods of objectively monitoring neuro-nal activity during music production, musicalreasoning, and motor learning in general. Thesemethods allow documentation of the dynamics of
developing brain circuitry during the acquisitionof new manual skills. They show our brain ‘‘atwork.’’
There are two principal approaches that can beused to assess brain activity. The first of thesetakes advantage of methods such as electroen-
cephalography (EEG) and magnetoencephalogra-phy (MEG) that make it possible to measuredirectly the electrical activity of neurons in thecerebral cortex. The second enables the assess-
ment of brain metabolism, cerebral blood flow,and oxygen consumption of nerve cells. Sucha method allows for indirect analysis of neuronal
activity based on the close links between oxygenconsumption and the firing activities of nervecells. The need for oxygen is reflected in local
increases of blood flow in the nervous tissue,which in turn can be assessed by measuring thelocal concentration of radioactively labeledmarker
substances in blood, such as oxygen or glucose.Although positron emission tomography (PET)
ghts reserved.

524 E. Altenmuller /Hand Clin 19 (2003) 523–538
uses this kind of data collection, there arecertain disadvantages that arise with the use ofthis method because of the application of low
dosages of radioactivity. Much safer is themethod of functional magnetic resonance imag-ing (fMRI) that uses the magnetic properties ofoxygen in blood cells to calculate oxygen
consumption.The main advantage of EEG and MEG is their
excellent temporal resolution, which enables the
monitoring of rapid processes and changes. Thesemethods also allow communication flows betweendifferent areas of the brain to be analyzed through
the calculation of so-called ‘‘coherence’’ betweenactivated neuronal cell assemblies. In contrast, themain advantage of PET and fMRI is their ex-cellent spatial resolution, which allows particular
tasks to be related to specific brain structures.Nevertheless, the temporal resolutions of PETand fMRI are still poor (ranging from 6 seconds
to 1 minute), meaning that more rapid cognitiveprocesses cannot be tracked. A further factor iscost: MEG, PET, and fMRI rely on extremely
complex and expensive technologies. Only EEG isaffordable enough to be used outside specializedbrain imaging centers [1].
General structure of the brain
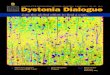
The human brain can be subdivided into threeparts: the hindbrain, the midbrain, and theforebrain (Fig. 1). The hindbrain consists of the
medulla, pons, and the cerebellum. The hindbrainand the midbrain together constitute the brainstem, which is phylogenetically (ie, in evolution)
the oldest part of the brain. The brain stem
regulates all vital functions such as breathing,heartbeat, arousal, body temperature, and equi-librium. Furthermore, the brain stem controls
many sensory and motor functions, such as eyemovements and the coordination of visual andauditory reflexes. The cerebellum lies behind thepons and mainly processes body equilibrium and
the accurate timing of movements. It is involvedin the learning of motor skills and is particularlyrelevant to the learning skills required in musical
performance. The midbrain lies above the ponsand contains two structures. The first ofthese—the thalamus—transmits incoming infor-
mation from all sensory systems to the cerebralcortex, and so acts as a gateway to the cortex. Thelatter—the hypothalamus—regulates autonomicand endocrine functions. Finally, the forebrain
consists of the two outer cerebral hemispheres andthree deep-lying structures: the basal ganglia, thehippocampus, and the amygdaloid nucleus. The
last two structures lie at the inner border ofthe temporal lobe and are not shown in Fig. 1.The basal ganglia participate in regulating motor
performance; the hippocampus is involved withaspects of memory storage; and the amygdaloidnucleus coordinates autonomic and endocrine
responses in conjunction with emotional states.All cognitive functions are governed by the
cerebral cortex—the outer part of the brain—which is the most complex organ in the human
body. According to recent estimates, the cerebralcortex consists of approximately 100 billionneurons that are interconnected by a dense web
of nerve fibers. By way of synapses, each nerve cellcan communicate with approximately 10,000
Fig. 1. Overview of the anatomic structures of the brain. Left hemisphere is shown.

525E. Altenmuller /Hand Clin 19 (2003) 523–538
other cells. The cerebral cortex is divided into twohemispheres that are interconnected by a largefiber bundle containing approximately 100 millionfibers, known as the corpus callosum.
Four important features characterize the orga-nization of the cortex. First of all, each hemi-sphere is concerned primarily with sensory and
motor processes on the contralateral side of thebody. Second, although seeming to be similar,these hemispheres are neither completely symmet-
ric in structure nor equivalent in function. Third,the cortex is organized hierarchically, with distinctprimary, secondary, and tertiary (or associative)
sensory or motor regions. Primary sensory regions(or areas) are linked directly to the sensory organsby way of the thalamus. Primary motor regionsare linked directly to the spinal chord. Secondary
and tertiary sensory and motor areas are adjacentto the primary areas and process more complexstimulus features. Finally, early intense training
processes starting before the age of approximately10 years may lead to enlargement of the corticalareas involved in the trained faculty.
Each hemisphere is divided into four anatom-ically distinct cortical lobes, called the frontal(front), temporal (side), parietal (upper back), and
occipital (back) lobe (Figs. 1, 2). The frontal lobesare concerned largely with the planning of futureaction and the control of movement. The parietallobes, which are located behind the frontal lobe
and are separated by a deep fissure known as thecentral sulcus, are concerned mainly with the pro-
cessing of somatic sensation and body image. Theoccipital lobes, which are responsible for process-ing vision, lie behind the parietal lobes at the backof the brain. The temporal lobes are separated
from the frontal and the parietal lobes by a furtherdeep fissure, the lateral sulcus. It is these temporallobes that deal not only with hearing, but also
with other aspects, such as cross-modal learning,memory, and emotion.
Neurophysiology of music performance
Music performance on a professional levelrequires extremely refined motor skills that areacquired over many years of extensive training,
and that have to be stored and maintainedthrough further regular practice. Auditory feed-back is needed to improve and perfect perfor-
mance. Music making, therefore, relies primarilyon a highly developed auditory–motor integrationcapacity that can be compared with the oral–aural
loop in speech production. In addition, somato-sensory feedback constitutes another basis ofhigh-level performance. Here, the kinestheticsense, which allows for control and feedback of
muscle and tendon–tension and joint positionsand which enables continuous monitoring offinger-, hand-, or lip-position in the frames of
body and instrument coordinates (eg, the key-board, the mouthpiece), is especially important. Ina more general context, the motor system of music
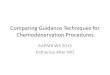
Fig. 2. Brain regions involved in sensory and motor music processing. Left hemisphere is shown in the foreground, right
in the background. a, area.

526 E. Altenmuller /Hand Clin 19 (2003) 523–538
performance can be understood as a subspecialtyof the motor systems for planned and skilledvoluntary limb movements.
Voluntary skilled hand movements involvefour cortical regions in both hemispheres (Fig. 2):the primary motor area (M1) located in theprecentral gyrus directly in front of the central
sulcus; the supplementary motor area (SMA)located anterior to the M1 of the frontal lobe andthe inner (medial) side of the cortex; the cingulate
motor area (CMA) below the SMA and above thecorpus callosum on the inner (medial) side of thehemisphere; and the premotor area (PMA), which
is located adjacent to the lateral aspect of theprimarymotor area. SMA,CMA, and PMAcan bedescribed as secondary motor areas, processingmovement patterns rather than simple movements.
In addition to the cortical regions, themotor systemincludes the subcortical structures of the basalganglia and the cerebellum. The sensory areas are
necessary to maintain the control of movements.Their steady kinesthetic feedback information isrequired for any guided motor action. The sensory
areas are located in the primary somatosensoryarea (S1), behind the central sulcus in the parietallobe. The parietal lobe is involved in many aspects
of movement processing. It is an area in whichinformation from multiple sensory regions con-verges. In the posterior parietal area, the bodycoordinates in space are monitored and calculated
and visual information is transferred into bodycoordinates. As far asmusicians are concerned, thisarea is activated prominently during sight-reading
and the playing of a complex piece of music [2].The primary motor area (M1) represents the
movements of body parts in a separate but
systematic order. The representation of the legis located on the top and the inner side of thehemisphere, the arm in the upper portion, and thehand and mouth in the lower portion of M1. This
representation of distinct body parts in corre-sponding brain regions is called somatotopic orhomuncular order. Just as the motor homunculus
is represented upside down, so too is the sensoryhomunculus on the other side of the centralsulcus. The proportions of the motor and the
sensory homunculus are distorted markedly be-cause they are determined by the density of motorand sensory innervation of the respective body
parts. For example, control of fine movementsof the tongue requires many more nerve fiberstransmitting the information to this muscle ascompared with muscles of the back. The hands
therefore require almost one third of the neurons
in this area. The representation of the body partsmay be modified by use, however. Moreover, theprimary motor area does not simply represent
individual muscles: multiple muscular representa-tions are arranged in a complex way so as to allowthe execution of simple types of movements ratherthan the activation of a specific muscle. This is
a consequence of the fact a two-dimensional arrayof neurons in M1 has to code for three-di-mensional movements in space [3,4]. Quite simply,
our brain does not represent muscles, but rathermovements.
The supplementary motor area (SMA) is
involved mainly in the coordination of the twohands, in the sequencing of complex movements,and in the triggering of movements based oninternal cues. It is engaged particularly when the
execution of a sequential movement depends oninternally stored and memorized information. TheSMA can be subdivided into two distinct func-
tional areas. In the anterior SMA, it would seemthat the planning of complex movement patternsis processed. The posterior SMA seems to be
engaged predominantly in two-handed move-ments and, in particular, in the synchronizationof both hands during complex movement pat-
terns. Electrical stimulation of this area duringopen brain surgery can produce an interruption oftwo-handed piano playing [5].
The functionof the cingulatemotor area (CMA)
is still under debate. Electrical stimulation andbrain imaging studies demonstrate its involvementin movement selection based on reward, with
reference to the close links between the cingulategyrus and the emotion-processing limbic system. Insummary, it would seem that the CMA plays
an important role in mediating cortical cognitivefunctions and limbic–emotional functions.
The premotor area (PMA) is engaged primar-ily when externally stimulated behavior is being
planned and prepared. It is involved in the learn-ing, execution, and recognition of limb move-ments and seems to be particularly concerned with
the visual information necessary for movementplanning.
The basal ganglia, located deep inside the
cerebral hemispheres, are interconnected recipro-cally by way of the thalamus to the motor andsensory cortices, thus constituting a loop of in-
formation flow between the cortex and the basalganglia. They are indispensable for any kind ofvoluntary actions that are not highly automated.Their special role consists in the control of
voluntary action by selecting appropriate motor

527E. Altenmuller /Hand Clin 19 (2003) 523–538
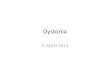
Fig. 3. Structural changes in the brains of musicians. Some of the brain areas that have been found to be enlarged in
musicians in morphometric studies based on structural magnetic resonance imaging. Arrows indicate primary motor
cortex; planum temporale in the temporal lobe and the anterior part of the corpus callosum.
actions and by comparing the goal and course of
those actions with previous experience. In thebasal ganglia, the flow of information between thecortex and the limbic emotion system, in partic-
ular the amygdala, converges. It is assumed,therefore, that the basal ganglia process andcontrol the emotional evaluation of motor behav-
ior in expected reward or punishment. Finally, thecerebellum contributes essentially to the timingand accuracy of fine-tuned movements.
Musicians’ brains are different
The organization of motor systems describedpreviously can be applied to skilled movements ingeneral. In the following section, however, the
author expands this notion to include literaturethat focuses on the unique qualities of themusicians’ brain.
Amunts and colleagues [6] have estimated the
size of the primary hand motor area by deter-mining the intrasulcular length of the posteriorbank of the precentral gyrus in linearly normal-
ized MRI images. Musicians had a greater intra-sulcular length on both sides, but more so on theright, nondominant hemisphere, resulting in re-
duced asymmetry scores for this area in musi-cians. There was a strong negative correlation
between the time at which musical training had
begun and the size of the right and left handmotor areas. This was reflected behaviorally inreduced hand skill asymmetry and a negative
correlation between hand skill asymmetry and ageof commencement of musical training [7] (Fig. 3).
Many musical instruments require precise co-
ordination of bimanual movements. Musicianswho had begun their musical training before theage of 7 years have a larger anterior midsagittalcorpus callosum (CC) than control subjects or
musicians who started training later [8]. Becausethe size of the midsagittal CC is a good indicatorof the number of axons crossing through the
midline, this finding suggests that this subgroup ofmusicians have enhanced interaction between thetwo hemispheres. Because this part of the corpus
callosum contains fibers from the motor andsupplementary motor areas, it seems plausible toassume that the high demands on coordination
between the two hands and the rapid exchange ofinformation may either stimulate the nerve fibergrowth, the myelination of nerve fibers thatdetermines the velocity of nerve conduction, or
prevent the physiologic loss of nerve tissue dur-ing aging. This hypothesis has been corroboratedby a bilateral transcranial magnetic stimulation
study in pianists and guitarists [9] that revealed

528 E. Altenmuller /Hand Clin 19 (2003) 523–538
decreased interhemispheric inhibition. This inturn might facilitate bimanual coordination inmusicians by increasing signal transfer between
the hemispheres.Precise timing of movements also requires the
participation of the cerebellum. Recently, malemusicians have been shown to have a greater
mean relative cerebellar volume than male non-musicians. The difference could not be ascribed toa difference in total brain volume, as this was
similar in both groups [10]. Together the findingssuggest that musicians show anatomic differencesin multiple brain areas that are involved in motor
processing. Changes in such large-scale neuralnetworks can be detected using voxel-basedmorphometry, a statistical method of revealingdifferences in brain anatomy between groups
without the need to focus on target structures.Such an analysis revealed increased gray mattervolume in a motor network that included the left
and right primary sensorimotor regions, the leftbasal ganglia, the bilateral cerebellum, and theleft posterior perisylvian region [11].
It is not only motor areas that are subjectto anatomic adaptation, however. By means ofmagnetoencephalography (MEG), the number of
nerve cells involved in the processing of sensorystimulation in individual fingers can be moni-tored. Using this technique, professional violinistshave been shown to possess enlarged sensory
areas corresponding to the index through to thesmall (second to fifth) fingers of the left hand [48].Their left thumb representation (the left thumb
only supports the violin) is no different from thatof nonmusicians. Again, these effects were mostpronounced in violinists who started their in-
strumental training before the age of 10 years.In summary, available evidence suggests that
the central nervous system adapts to the challeng-ing demands of professional musicianship during
prolonged training. These adaptations are un-derstood as brain plasticity. When training startsat an early age (before approximately 7 years),
this adaptation affects brain anatomy in the en-largement of certain brain structures involved inthe respective skill. When training starts later, it
modifies brain organization by rewiring neuronalwebs and involving adjacent nerve cells to con-tribute to the required tasks. These changes
result in enlarged cortical representations of, forexample, specific fingers within existing brainstructures [13].
To understand these processes more fully, the
following section focuses on the short- and long-
term effects of musical training on neuronalrepresentations and brain networks.
Sensorimotor plasticity and sensorimotor learning
Our knowledge concerning the regions andmechanisms of the brain involved in sensorimotorlearning is still incomplete. According to present
concepts, all structures involved in motor controlparticipate in the acquisition of new sensorimotorskills. Besides the motor areas in the cerebralcortex, the basal ganglia and the cerebellum also
play an important role. It has been assumed sincethe nineteenth century that the cerebellum playsan important role in the acquisition of new motor
skills. Such information was based on studiesin which patients suffering from lesions of thecerebellum were found to be unable to increase
the speed of a sequence of complex finger move-ments after practice. More recent evidence dem-onstrates that the cerebellum is involved in the
selection, the sequence, and the timing of move-ments. It seems not to contribute to the motorlearning itself, however, but is engaged primarilyin the modification of performance subsequent to
a learning process [14].Another functional system that is equally
important for the development and learning
of fine finger movements is the basal ganglia.Patients suffering from Parkinson disease havedeficits in learning new motor tasks and, although
they can improve the speed of complex movementpatterns during practice sessions, they do notlearn as quickly and do not reach the level ofperformance of normal control subjects [15].
It has been known for a long time that withincreasing complexity of finger movement sequen-ces, the activity in the SMA and in the premotor
area are enhanced [16]. Using fMRI, Karni andcoworkers [17] investigated the learning of com-plex finger sequences similar to those necessary
for piano playing. After 30 minutes of practice,the representation of the fingers in the primarymotor cortex was increased. Without further
training, however, this effect diminished after 1week with the hand representation returning to itsprevious size. In contrast, continuous practiceresulted in a stable enlargement of the hand area
in primary motor cortex. This effect was specificfor the daily trained sequence of complex fingermovements and did not occur when the subjects
improvised complex finger movements that werenot repeated subsequently. Parallel to the enlarge-ment of the hand area in the primary motor

529E. Altenmuller /Hand Clin 19 (2003) 523–538
cortex, the size of the cerebellar hand representa-tion diminished, suggesting that the cerebellumplays no major role in long-term motor learning.It has been proposed on the basis of these
neuroimaging studies that motor learning occursin several phases: a fast initial phase of perfor-mance gains is followed by a period of consolida-
tion that lasts for several hours. This is succeededby a slow learning phase that occurs duringcontinued practice and leads to gradual increases
in performance [18]. When highly skilled pianistsand nonmusicians were exposed to a novel tap-ping task during a single scanning session,
musicians showed a rapid increase of primarymotor cortex activation, whereas nonmusiciansdid not. This effect of recruitment in the primarymotor area thus resembled the slow learning
described previously in nonmusicians, eventhough it occurred within minutes rather thanmonths. It was interpreted therefore as an effect
of pre-practice experience [19]. With regard tosecondary motor areas, in contrast, musiciansshowed a much smaller area of activation in the
SMA, pre-SMA, and CMA in several studies.This finding is compatible with the idea thatthe anterior SMA is essential for setting up and
executing complex motor programs before auto-matic performance. The pianists were able tolearn rapidly and thoroughly the complex fingersequence, reaching a high degree of automaticity
during the first minutes of motor learning.Most interestingly, the motor cortex of the
untrained hand was, at the same time, contribut-
ing to motor learning. This resulted in improvedperformance of the motor task in the untrainedleft hand in pianists and nonmusicians. One of the
most fascinating features of the human sensori-motor system relates to this phenomenon. Despiteclear somatotopic organization of the motorcortex, a movement can be learned with one ex-
tremity and performed with the other. Rijntjesand colleagues [20] investigated subjects writingtheir signature with their right index finger and
with their right big toe. The results of their fMRIstudy show that the movement parameters forthese highly trained movements are stored in
premotor and supplementary motor cortex adja-cent to the right hand area in the primary motorcortex, but are also accessible for the foot area.
Thus, somatotopy in secondary motor areas(SMA, PM) seems to be defined functionally, asabstract movement information independent fromthe executing limb (movement ideas or Bewe-
gungs-Ideen), and not on the basis of anatomic
representations. Although these studies refer toexplicit motor learning by trial and error andsensory feedback, implicit motor learning seemsto be processed in a different way. When subjects
were unaware of a motor learning task—becausetheir attention was drawn to a different prob-lem—activity of the basal ganglia correlated with
motor learning.All of the studies mentioned do not take into
account the special quality of musicianship, and in
particular, the strong coupling of sensorimotorand auditory processing. Practicing an instrumentmeans assembling, storing, and constantly im-
proving complex sensorimotor programs throughprolonged and repeated execution of motor pat-terns under control of the auditory system.
Many professional pianists report that their
fingers move more or less automatically when theyare listening to piano music played by a colleague.In a cross-sectional experiment, the author
demonstrated that, as a result of many yearsof practice, a strong linkage between auditoryand sensorimotor cortical regions develops [21]
(Fig. 4).Furthermore, in a longitudinal study, it was
possible to follow up the formation of such
neuronal multisensory connections together withpiano training in beginner piano players. Non-musicians who had never played an instrumentbefore were trained on a computer piano twice
a week over a period of 5 weeks. They listenedto short piano melodies of a 3-second durationplayed in a five-tone range. After a brief pause
they were required to replay the melodies with theright hand as accurately as possible. After 10minutes of training, listening to piano tunes
produced additional activity in the central andleft sensorimotor regions. In turn, playing ona keyboard produced additional activity in theauditory regions of both temporal lobes. These
early signs of cortical plasticity during the firsttraining session were not stable, but stabilizedwithin the subsequent 5 weeks of training. In the
movement task, the most remarkable effect after 5weeks was the development of additional activa-tion of the right anterior temporal and frontal
lobe. Because it has been demonstrated that thisarea is involved in the perception of pitchsequences, such activation might reflect the
auditory imagery of sounds while moving thefingers on a soundless keyboard. In this context, itshould be mentioned that the results of theexperiment support the idea of the direct effec-
tiveness of mental training on subtle sensorimotor

530 E. Altenmuller /Hand Clin 19 (2003) 523–538
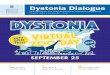
Fig. 4. Auditory–sensory-motor corepresentation in a professional pianist investigated with fMRI. Listening to piano
tunes activates sensory-motor areas in addition to auditory brain regions; playing on a mute keyboard also activates
mainly left auditory areas. (Courtesy of Dr. Marc Bangert and Dr. Thomas Peschel.)
activation patterns represented in the centralnervous system.
Many questions concerning the brain mecha-nisms of sensorimotor learning and processing
during music performance remain to be clarified. Itis still unclear, for example, how and where therapid adjustment of the sensorimotor system to
different spatial coordinates is processed whenmusicians switch between instruments of differentsizes (eg, from alto flute to piccolo). This phenom-
enon is referred to as response size or movementschema. Besides the limb-independent storage ofmovement information in the secondary motor
areas mentioned previously, the cerebellum mightcalculate a magnification or diminution factor.Another unsolved problem is the neuronal basis ofthe transition from guided slow movements, which
are performedunder steady sensory control, to fast,ballistic movements, which have to be performedwithout online sensory feedback. It is assumed that
different brain regions produce these two types ofmovements and that the transition fromone type tothe other may be incomplete. This might explain
why practicing guidedmovements while slowly andsystematically increasing the tempo may finallyhamper the execution of this movement at a very
fast tempo.
Musicians’ dystonia: loss of manual coordination
in highly trained musicians
There is a dark side to the increasing special-ization and prolonged training of modern musi-
cians, namely loss of control and degradation ofskilled hand movements, a disorder referred to asmusicians’ cramp or focal dystonia. The firsthistorical record from 1830 appears in the diaries
of the famous pianist and composer RobertSchumann [22]. As was probably the case forSchumann, prolonged practice and pain syn-
dromes caused by overuse can precipitate dysto-nia, which is developed by approximately 1% ofprofessional musicians and usually ends their
career [23–25].Focal dystonia is characterized by insidious
or sudden deterioration of voluntary control of
extensively trained, complex sensorimotor skills.Subtle loss of control in fast passages, fingercurling (Fig. 5), lack of precision in forked finger-ings in woodwind players, irregularity of trills,
sticking fingers on the keys, involuntary flexion ofthe bowing thumb in strings, and impairment ofcontrol of the embouchure in woodwind and brass
players in certain registers are the various symp-toms that can mark the beginning of the disorder.At this stage, most musicians believe that the
reduced precision of their movements is causedby a technical problem. As a consequence, theyintensify their efforts, but this often only exacer-
bates the problem [26,27].Males (83%), classical musicians of a younger
age (89%), and instrumentalists such as guitarists,pianists, and woodwinds (together 70%) are
among the most commonly affected by focaldystonia [25,28]. Most patients have solo

531E. Altenmuller /Hand Clin 19 (2003) 523–538
Fig. 5. Typical example of musician’s cramp in a pianist, a flutist, and a violinist.
positions and often have a perfectionist, control-type personality. Some statistics concerning pos-sible risk factors are shown in Table 1.
In summary, the development of hand dystoniain musicians is related to the intense and prolongedpractice of fast and highly precise externally
predefined actions. Movement patterns, which areworked on extensively and which require force andskills in one hand at the same time, seem to be
affected predominantly. Chronic pain syndromesand sensory dysesthesia may precede overt dys-tonic symptoms or even may induce the develop-ment of focal dystonia in musicians susceptible to
this movement disorder. Freedom of interpreta-tion in mainly improvising musicians and freedomfrom external professional pressures in amateurs
seems to be a protective factor.
Some remarkable symptoms in focal
hand dystonia
At first glance, some characteristics of focalhand dystonia seem to be incompatible with theview of an organic disorder of the central
sensorimotor system. One of these strange phe-nomena is the task specificity of the motor prob-lem. In most cases, focal dystonia only presents
in the context of instrumental playing. It mightoccur when playing the clarinet, but not whenplaying the saxophone in the same person.
Another interesting feature is the ‘‘sensory-trickphenomenon’’: usually, the coordination problem
largely depends on the afferent somatosensoryinput, for example, from the skin of the fingertips.The author has seen two pianists who had focal
dystonia almost exclusively when playing on ivorybut not on plastic keys. Playing with a latex gloveusually improves the condition. Frequently this
effect is not stable, however, and fades away aftersome minutes of playing.
Focal dystonia often occurs together with focal
tremor as an associated symptom.When observingthe dystonic movement, increased tremor ampli-tude (when compared with the unaffected move-ment of the other hand) can be recognized in more
than 50% of cases. In a few cases, dystonic tremorcan be observed as an isolated but equally disablingsymptom. According to Kaji et al [29], isolated
focal tremor can be interpreted as a ‘‘minus’’variant of focal cramping, characterized as a lackof activation of appropriate muscles in contrast to
the overshooting activation in focal dystonia.Usually neurologic examination does not
reveal any further abnormalities. Additional neu-
rophysiologic and neuroradiologic routine inves-tigations are normal and therefore not helpful inclassifying the focal dystonia with respect to theunderlying pathology.
Focal limb dystonia in musicians may originate
from maladaptive plasticity
Although the neurobiologic origins of this
disorder are not clarified completely, the link

532 E. Altenmuller /Hand Clin 19 (2003) 523–538
Table 1
Which musician is at risk to develop focal dystonia?
Males 83%
Classical musicians 89%
Younger age
Onset of disorder before age 40 years (average: 32 years, range 15–67 years) 80%
Certain instruments vs. normal distribution
Guitarists 20% 5%
Pianists 29% 15%
Woodwinds (hand dystonia) 21% 16%
Strings 15% 44%
Brass (embouchure d.) 11% 14%
Woodwinds (embouchure d.) 3% 16%
Miscellaneous 2%
n.b. only one double-bass player
Outstanding professional position
Soloists 49%
Solo performing teachers 17%
Tuttists 13%
Students 14%
Amateurs 7%
Personality
Music loving, ambitious, perfectionist, control type
Genetics
(Family history of dystonia) 10%
n ¼ 189 patients, 10/1994–12/1999.
between chronic pain and overuse suggests that
focal dystonia as a cortical sensorimotor mis-learning syndrome may be caused by abnormalplasticity [30]. A study with trained monkeys [31]
demonstrated that chronic overuse and repetitivestrain injury in highly stereotyped movements candegrade actively the cortical representation of the
somatosensory information that guides the finemotor hand movements in primates. A similardegradation of sensory feedback information and
concurrent fusion of the digital representations inthe somatosensory cortex was confirmed in anMEG study conducted in musicians with focaldystonia, although these musicians had no history
of chronic pain (Fig. 6) [12]. These findings arecorroborated by psychophysical measurementsand fMRI investigations in a related disorder,
writer’s cramp, which showed decreased temporaland spatial discrimination at the fingertips [32,33].In a further study, symptoms were provoked in
five dystonic guitarists when they played a modi-fied guitar inside an fMRI scanner [34]. Relativeto nondystonic guitarists, they showed moreactivation of the contralateral sensorimotor cor-
tex but less activation of premotor areas, suggest-ing abnormal recruitment of cortical areasinvolved in the control of complex movements.
Because most musicians play their whole lives
without any coordination problems, however,additional factors, such as a genetic predispositionand a certain susceptibility, seem to play an
important role in the development of focaldystonia.
The most important and, up to now, unsolved
question concerning the therapy of musicians’dystonia is why this condition cannot be over-come easily by retraining and establishing
new and appropriately functioning sensorimotormovement patterns. The author suggests that thisis because of the strong linkage of musicians’movements to emotions and to the limbic system.
From animal experiments it is known that thelimbic system strongly influences memory pro-cesses. Whenever an experience is perceived as a
threatening event, the limbic evaluation systemreinforces memory storage for this experience.When considering musicianship in this context, it
is clear that musicians have to perform complexmovement patterns requiring high-speed motorcontrol under an unyielding auditory feedback. Amusician wants to express and to communicate
his feelings on one side and might be afraid tomake mistakes on the other side. This ‘‘doublelinkage’’ to emotions is reflected in the strong

533E. Altenmuller /Hand Clin 19 (2003) 523–538
Fig. 6. Fusion of the somatosensory representation of single digits of the hand in a musician suffering from focal
dystonia. The best-fitting dipoles to explain the evoked magnetic fields after sensory stimulation of single digits (D1–D5)
are shown projected on the individual’s MRI scan. Although for the nonaffected hand the typical homuncular
organization (inset) reveals a distance of �2.5 cm between the sources for the thumb and the little finger (bright circle
and square on the right of the brain), the somatosensory representations of the fingers on the dystonic side are blurred,
resulting from a fusion of the neural networks that process incoming sensory stimuli from different fingers (dark circles).
(Modified from Elbert T, Candia V, Altenmuller E, Rau H, Sterr A, Rockstroh B, et al. Alterations of digital
representations in somatosensory cortex in focal hand dystonia. Neuroreport 1998;9:3571–5, Lippincott, Williams and
Wilkins; with permission).
reward–punishment system acting in professional
musicianship. One could speculate that the fear offalse notes and false movements may enhanceparadoxically the memory for such unsuccess-
ful movements. Support for this theory is theobservation that especially ambitious and enthu-siastic musicians are affected with the disorder
and that a high percentage of dystonic musiciansare suffering from other forms of phobias andpanic attacks [35]. The basal ganglia constitute thecrossover points between the limbic system and
the sensorimotor circuits, and therefore could play
a crucial role concerning the pathophysiologic
mechanisms in dystonia.In a smaller group of musicians there is a close
relationship between musician’s cramp and other
dystonias. In the authors’ group, writer’s crampand musician’s cramp is associated in 37 patients.Writer’s cramp can appear before, synchronously
with, or even years after focal dystonia duringinstrumental playing had become apparent. Inrare cases, focal dystonia manifests as the initialsymptom of a segmental dystonia or a generalized
dystonia. These disorders progress slowly and

534 E. Altenmuller /Hand Clin 19 (2003) 523–538
include step-by-step larger groups of muscles. Theunderlying pathology is located in the basalganglia [36].
Finally, there is a small subgroup of patientssuffering from focal dystonia caused by a psycho-genic origin. These patients develop incoordina-tion in the context of a neurosis. It is difficult to
distinguish a psychogenic incoordination froma nonpsychogenic one. The author has the im-pression that the pattern of psychogenic incoor-
dination has a more demonstrative character withsometimes strange and ‘‘expressive’’ motions.There are no data available on the long-term
outcome in these patients. The author supposesthat the spontaneous remission of focal dystoniaseen occasionally might occur predominantly inthese patients.
Treatment of musicians’ dystonia
The different origins of focal dystonia requiredifferent therapeutic approaches. In Fig. 7, a
simplified diagram of the author’s understandingof the pathologic mechanisms in focal dys-tonia is shown. As a hypothesis, the author sug-
gests that inappropriate sensorimotor programshave been established because of misguided plas-ticity of cortical or subcortical sensorimotor re-presentations of the affected limbs. Because large
neural circuits connect premotor, motor andsensory areas, the basal ganglia, and the limbicsystem, the origin of the fatal maladaptive process
may be in one of these structures, but it influencesthe whole circuit (Fig. 7).
The aim of treatment must be establishing
a new sensorimotor program. This can be ac-hieved using different methods. One possibility iscircumventing the disabled movements by mod-
ifications of the instrument (eg, alteration of theposition of keys in woodwinds and use of otherergonomic devices). Neuromuscular reeducation(eg, Feldenkrais and Alexander techniques) may
be helpful, although in the author’s experience,functional recovery to a high technical standard isan exception. Retraining by experienced teachers
as offered in Europe by Phillip Chamagne [37] andLaurent Boullet [38] seems to be more effective;however, these methods usually require several
years of specific instruction.A novel treatment approach is based on the
principle of the constraint-induced movementtherapy (CIMT) in stroke patients. CIMT in
stroke patients means that patients are encour-
aged and even forced to use the paretic limbs andthat movements of the unaffected healthy limbsare actively constrained (eg, by fixing them in
a cast). Stroke patients treated in such a way hadbetter outcome with respect to their motorabilities. In brain imaging studies in these patients,it emerged that the cortical representation of the
affected limbs was reorganized better than inuntreated controls. For dystonic musicians, thisbehavioral treatment has been adapted by a group
in Konstanz in close cooperation with theauthor’s institution [39,40]. In musicians sufferingfrom hand dystonia, the disturbed movement
patterns usually include one focal dystonic fingercramping in flexion and compensating fingerstrying to help the flexed finger out of its position.During the behavioral therapy, the compensating
finger is immobilized with a splint. Under theseconditions the dystonic finger has to carry outrepetitive exercises in coordination with one or
more of the nonsplinted fingers according toa certain schedule. As a result, six pianists andtwo guitarists showed marked improvement of the
dystonia, whereas woodwinds did not benefitfrom this therapy. At present, follow-up studiesconcerning long-term improvement under this
therapy are conducted. Furthermore, the authorplans to apply this therapy in a considerablylarger group of dystonic musicians. Related to thetreatment mentioned previously and similarly
based on the assumption of cortical dysplasticityin focal dystonia, a prospective treatment trial ona mixed group of patients with focal dystonia was
conducted [41]. The investigators used variousmethods of sensory retraining and visual mirrorfeedback in addition to physiotherapy for
strengthening the hand muscles. The patientsimproved significantly in obtaining motor control,accuracy, sensory discrimination, and physicalperformance. Prolonged splinting and careful
retraining yielded equal improvements in a groupof Italian musicians [42].
Another therapeutic option is a symptomatic
treatment with local intramuscular injections ofbotulinum toxin (Botox). Botulinum toxins areproduced by Clostridium botulinum bacteria; seven
serotypes or forms of botulinum toxin have beenisolated (A–G). Each has different properties andactions and no two are exactly alike. Of these
subtypes, botulinum toxin type A and B arecurrently the most studied and most widely used.Intramuscularly injected, Botox reduces the re-lease of the neurotransmitter acetylcholine at the
neuromuscular junction, resulting in a weakening

535E. Altenmuller /Hand Clin 19 (2003) 523–538
Fig. 7. Simplified scheme of the different methods of treatment in focal dystonia related to the underlying
pathophysiologic mechanisms. For further explanations see text.
of the muscle [43]. The effect of Botox lasts forapproximately 2–3 months and is reversible.
Botox has been used with some success inmusicians with focal dystonia. Its therapeuticwindow is narrow, however, rendering its man-
agement difficult. There is a fine line betweenadministering not enough Botox and too much ofit, which may weaken the muscles and impair their
control [24,44–46]. Injections into the intrinsichand muscles hold several advantages overinjections into the long flexor and extensormuscles of the forearm. There is a lower risk for
impairing movement in adjacent fingers, eitherbecause of diffusion of the botulinum toxinsolution or the intermingling of muscular fascicles
of different fingers. The required dosage is small,which lowers the risk for antibody development.In the case of overdosage, serious paresis impair-
ing the function of dystonic fingers is less frequentand is compensated for more easily by thefunctionally intact long flexors and extensors.
Injections should be performed, however, onlyinto those intrinsics that are not required toperform rapid lateral movements of the fingerson the instrument. In woodwinds, most of the
instruments equipped with the Boehm-system(eg, flute, saxophone, clarinet) almost exclusively
demand such lateral movements in the right andleft little fingers. According to the author’s
experience, injections into the involved interosseusand lumbrical muscles therefore should be ad-ministered in all cases of flexion or extension
dystonia in index, middle, or ring finger ofwoodwind instrumentalists.
Anticholinergic drugs that influence predomi-
nantly neurotransmission in the basal ganglia arehelpful in some cases of focal dystonia. Accord-ing to the author’s experience, trihexyphenidyl(Artane�) is the most effective substance. It must
be mentioned, however, that long-term improve-ment is not so common, because many patients donot tolerate the drug over a long period of time.
Even at a low dosage of 4–6 mg daily, side effectssuch as fatigue, dry mouth, or slight memoryimpairment are reported frequently. Also used is
Madopar, which acts on the dopaminergic trans-mission; however, it does not seem to be aseffective as Artane [47].
Finally, it is crucial to consider the psychologicfactors when treating patients with focal dystonia.The frustrating dystonia paradox mentioned pre-viously should be an occasion to reflect on one’s
attitudes concerning the playing of an instrumentand the life of a musician. It is important to keep

536 E. Altenmuller /Hand Clin 19 (2003) 523–538
in mind that musicians play music and do not
‘‘work an instrument.’’ Helping the patient tobreak out of their prison of coordination prob-lems, helping them to widen and free their mind,
and enabling them to develop perspectives for thefuture is important.
What can doctors do for patients with focal
limb-dystonia?
The treatment of focal dystonia remains
a difficult task for the performing artist’s doctor.Improvement in symptoms can be attained inmany cases, but it is understandable that for manypatients this is not enough. They want all or
nothing! Once having played Tchaikovsky’s B flatminor concerto as a soloist with the BerlinPhilharmonic it is not easy to accept limitations
in repertoire or to perform at a lower technicallevel in a small town. How to deal with thisproblem must be part of the psychologic support
and must be considered when developing futureperspectives with the individual patient. As ageneral rule, complete recovery cannot be ac-
hieved. Even under optimal conditions, somerestrictions in repertoire or tempo and power ofcertain movements remain. The results of treat-ment in the author’s group are summarized in
Table 2.The author’s experience indicates the six most
important steps in treating musicians suffering
from focal limb dystonia are:
1. Make the right diagnosis. Approximately40% of the author’s patients came with
Table 2
Outcome of treatment in focal dystonia
No treatment wanted or possible n = 35 (19%)
Botox injections n = 54 (29%)
Long-term improvement n = 20 (11%)
Anticholinergic drugs n = 75 (40%)
Long-term improvement n = 10 (5%)
Constrained movement therapy n = 11 (6%)
Long-term improvement n = ?
Ergonomic changes eg, keys n = 4 (2%)
Long-term improvement n = 4 (2%)
No benefit at all from any therapy n = 42 (22%)
Change of profession at present n = 26 (14%)
Positive development
without treatment
n = 14 (7%)
No information about follow-up n = 20 (11%)
Multiple naming possible
n = 189 patients, 10/1994–12/1999.
a wrong diagnosis (eg, tendinitis, snapping-finger syndrome, depression).
2. Relieve your patient of guilt feelings. De-
veloping focal dystonia is not from a faultytechnique or a faulty posture. It is fate and itprobably can happen to any passionatemusician.
3. Protect your patient from useless cures.4. Discuss the therapeutic possibilities realisti-
cally. Do not awaken false hopes.
5. Pragmatic therapy should include Botox,anticholinergic drugs, and, depending oninstrument and individual situation, reeduca-
tion with an experienced instructor.6. Your patient needs steady psychologic sup-
port. Help them to not look back all the time,deploring their misfortune, but to develop
new perspectives.
Acknowledgments
This work was supported by a grant from theDFG (SPP 1001, Al 269/1-3). Many thanks toMarc Bangert, Thomas Elbert, Hans-Christian
Jabusch, Thomas Munte, and Thomas Peschel,who all contributed to the investigations andshared their enthusiasm for the neurophysiology
of the musician’s hand with me.
References
[1] Altenmuller E, Gerloff Ch. Psychophysiology and
the EEG. In: Niedermeyer E, Lopes da Silva F,
editors. Electroencephalography. 4th edition. Balti-
more: Williams and Wilkins; 1998. p. 637–55.
[2] Sergent J. Mapping the musician brain. Hum Brain
Map 1993;1:20–38.
[3] Graziano MS, Taylor CS, Moore T, Cooke DF.
The cortical control of movement revisited. Neuron
2002;36:49–62.
[4] Rouiller EM. Multiple hand representations in the
motor cortical areas. In: Wing AM, Haggard P,
Flanagan JR, editors. Hand and brain. San Diego:
Academic Press; 1997. p. 99–124.
[5] Marsden CD, Deecke L, Freund H-J. The functions
of the supplementary motor area. Summary of
a workshop. In: Luders H, editor. Advances in
neurology. Vol. 70 Supplementary sensorimotor
area, Philadelphia: Lippincott-Raven Publishers;
1996. p. 477–87.
[6] Amunts K, Schlaug G, Jancke L, Steinmetz H,
Schleicher A, Dabringhaus A, Zilles K. Motor
cortex and hand motor skills: structural compliance
in the human brain. Hum Brain Map 1996;5:
206–15.

537E. Altenmuller /Hand Clin 19 (2003) 523–538
[7] Jancke L, Schlaug G, Steinmetz H. Hand skill
asymmetry in professional musicians. Brain Cog
1997;34:424–32.
[8] Schlaug G, Jancke L, Huang Y, Steinmetz H.
Increased corpus callosum size in musicians. Neuro-
psychologia 1995;33:1047–55.
[9] Ridding MC, Brouwer B, NordstromMA. Reduced
interhemispheric inhibition in musicians. Exp Brain
Res 2000;133:249–53.
[10] Schlaug G. The brain of musicians. A model for
functional and structural adaptation. Ann NY
Acad Sci 2001;930:281–99.
[11] Sluming V, Barrick T, Howard M, Cezayirli E,
Mayes A, Roberts N. Voxel-based morphometry
reveals increased gray matter density in Broca’s area
in male symphony. Neuroimage 2002;17:1613–22.
[12] Elbert T, Candia V, Altenmuller E, Rau H, Sterr A,
Rockstroh B, et al. Alterations of digital represen-
tations in somatosensory cortex in focal hand
dystonia. Neuroreport 1998;9:3571–5.
[13] Munte TF, Altenmuller E, Jancke L. The musician’s
brain as a model of neuroplasticity. Nat Rev
Neurosci 2002;3:473–8.
[14] Seidler RD, Purushotham A, Kim SG, Ugurbil K,
Willingham D, Ashe J. Cerebellum activation as-
sociated with performance change but not motor
learning. Science 2002;296:2043–6.
[15] Salmon DP, Butters N. Neurobiology of skill and
habit learning. Curr Opin Neurobiol 1995;5:184–90.
[16] Roland P, Larsen B, Lassen NA, Skinhoi E.
Supplementary motor area and other cortical areas
in organization of voluntary movements in man.
J Neurophysiol 1980;43:118–36.
[17] Karni A, Meyer G, Jezzard P, Adams MM, Turner
R, Ungerleider LG. Functional MRI evidence for
adult motor cortex plasticity during motor skill
learning. Nature 1995;377:155–8.
[18] Karni A, Meyer G, Rey-Hipolito C, Jezzard P,
Adams M, Turner R, Ungerleider LG. The ac-
quisition of skilled motor performance: fast and
slow experience-driven changes in primary motor
cortex. Proc Natl Acad Sci USA 1998;95:861–8.
[19] Hundt-Georgiadis M, Cramon DY. Motor-learning
related changes in piano players and non-musicians
revealed by functional magnetic resonance signals.
Exp Brain Res 1999;125:417–25.
[20] Rijntjes M, Dettmers C, Buchel C, Kiebel S,
Frackowiak RS, Weiller C. A blueprint for move-
ment. Functional and anatomical representations
in the human motor system. J Neurosci 1999;19:
8043–8.
[21] Bangert M, Haeusler U, Altenmuller E. On
practice: how the brain connects piano keys and
piano sounds. Ann NY Acad Sci 2001;930:425–8.
[22] Schumann R. Diaries. Quotation according to
Eismann G, Hrsg. Tagebucher. Basel/Frankfurt:
Stroemfeld/Roter Stern; 1971. Band I.
[23] Altenmuller E. Fokale Dystonien bei Musikern:
Eine Herausforderung fur die Musiker-Medizin.
Musikphysiologie und Musikermedizin 1996;3:
29–40.
[24] Altenmuller E. Causes et traitements de la dystonie
de fonction chez les musicians. Une etude sur 5 ans.
Medecine des Arts 2001;36:19–26.
[25] LimVK,Altenmueller E, Bradshaw JL. Focal dysto-
nia: current theories.HumMovSci 2001;20:875–914.
[26] Fry HJ, Hallett M, Mastroianni T, Dang N,
Dambrosia J. Incoordination in pianists with over-
use syndrome. Neurology 1998;51:512–9.
[27] Lederman RJ. Focal dystonia in instrumentalists:
clinical features. Med Prob Perf Art 1991;6:132–6.
[28] Lim VK, Altenmuller E. Musicians’ cramp: in-
strumental and gender differences. Med Prob Perf
Art 2003;18:21–6.
[29] Kaji R, Shibasaki H, Kimura J. Writer’s cramp. A
disorder of a motor subroutine? Ann Neurol
1995;38:835–6.
[30] Hallett M. The neurophysiology of dystonia. Arch
Neurol 1998;55:601–3.
[31] Byl NN, Merzenich MM, Jenkins WM. A primate
genesis model of focal dystonia and repetitive strain
injury. Neurology 1996;47:508–20.
[32] Sanger TD, Tarsy D, Pascual-Leone A. Abnormal-
ities of spatial and temporal sensory discrimination
in writer’s cramp. Mov Disord 2001;16:94–9.
[33] Sanger TD, Pascual-Leone A, Tarsy D, Schlaug G.
Nonlinear sensory cortex response to simultaneous
tactile stimuli in writer’s cramp. Mov Disord
2002;17:105–11.
[34] Pujol J, Roset-Llobet J, Rosines-Cubells D, Deus J,
Narberhaus B, Valls-Sole J, et al. Brain cortical
activation during guitar-induced hand dystonia
studied by functional MRI. Neuroimage 2000;12:
257–67.
[35] Jabusch HC, Muller S, Altenmuller E. Psychologi-
sche Pradispositionen bei Musikern mit Bewegungs-
storungen. Musikphysiologie und Musiker-Medizin
2000;7:126–7.
[36] Sheehy MP, Marsden CD. Writers’ cramp—a focal
dystonia. Brain 1982;105:461–80.
[37] Chamagne P. Traitement des dystonies de fonctions
des musiciens par une reeducation pronlongee.
Revue Medecine des Arts 2001;36:31–3.
[38] Boullet L. Is there a cure for focal dystonia?
[abstract]. Freiburg, Germany: Presented at the Pro-
ceedings of the Deutsche Gesellschaft fur Musik-
physiologie und Musiker-Medizin, April 4, 2003.
[39] Candia V, Elbert T, Altenmuller E, Rau H, Schafer
T, Taub E. A constraint induced movement therapy
for focal hand dystonia in musicians. Lancet
1999;353:42.
[40] Candia V, Schafer T, Taub E, Rau H, Altenmuller
E, Rockstroh B, et al. Sensory motor retuning:
a behavioral treatment for focal hand dystonia of
pianists and guitarists. Arch Phys Med Rehabil
2002;83:1342–8.
[41] Byl NN, McKenzie A. Treatment effectiveness for
patients with a history of repetitive hand use and

538 E. Altenmuller /Hand Clin 19 (2003) 523–538
focal hand dystonia: a planned, prospective follow-
up study. J Hand Ther 2000;13:289–301.
[42] Priori A, Pesenti A, Cappellari A, Scarlato G,
Barbieri S. Limb immobilization for the treatment
of focal occupational dystonia. Neurology 2001;
57:405–9.
[43] Coffield JA, Considine RV, Simpson LL. The site
and mechanism of action of botulinum neurotoxin.
In: Jankovic J, Hallett M, editors. Therapy with
botulinum toxin 3–13. New York: Marcel Dekker;
1994.
[44] Charness ME, Ross MH, Shefner JM. Ulnar
neuropathy and dystonic flexion of the fourth and
fifth digits: clinical correlation in musicians. Musc
Nerve 1996;19:431–7.
[45] Cole R, Hallett M, Cohen LG. Double-blind trial of
botulinum toxin for treatment of focal hand
dystonia. Mov Disord 1995;10:466–71.
[46] Ross MH, Charness ME, Sudarsky L, Logigian EL.
Treatment of occupational cramp with botulinum
toxin: diffusion of toxin to adjacent noninjected
muscles. Musc Nerve 1997;20:593–8.
[47] Muller F, Dichgans J, Jankovic J. Dyskinesias. In:
Brandt T, Caplan LR, Dichgans J, Diener HC, Ken-
nard C, editors. Neurological disorders: course and
treatment. SanDiego:AcademicPress; 1996. p. 779–95.
[48] Elbert T, Pantev Ch., Wienbruch Chr., Rockstroh
B, Taub E. Increased cortical representation of the
fingers of the left hand in string players. Science
1995;270:305–7.