Embed Size (px)
DESCRIPTION
Quarterly magazine published by the Children's Hospital of the Greenville Health System
Citation preview

Supportive Care Team
Spartanburg Opens Outpatient Center
Doctors’ Top Apps
New Physicians
Resident News
CME: Nutrition
Quality Counts: Quality Standards
Latest Children’s Hospital Directory
Network Improves GI Care
Clinical Research
Ask the Faculty: Peanut Allergy
Goodnight Greenville Hits Stores

2 Lead Story Supportive Care Team Smooths the Road for Patient Families
6 What’s New? New Outpatient Center in Spartanburg; Four School Clinics Launched; DeLoache Seminar Expands
7 New Technology Doctors Share Their Favorite Medical Apps
8 Medical Staff Spotlight Meet Our New Physicians
11 Academic News Resident and Fellow News
14 Continuing Medical Education Nutrition: The Whole-diet Approach
19 Quality Counts The Alphabet of Quality
20 Celebrations Awards and Philanthropic News
22 Clinical Research Update Pediatric Sleep Studies
24 Feature Story Collaborating to Improve Inflammatory Bowel Disease Care
26 Ask the Faculty The LEAP Study and Changing Peanut Allergy Recommendations
Focus on Pediatrics
This magazine is published quarterly by Children’s Hospital of Greenville Health System.
Medical EditorJoseph L. Maurer, MD
Managing EditorLark Reynolds
GHS PhotographerAV Services
Art DirectorGHS Creative Services
Editorial BoardLinda Baumbach, CAPNichole Bryant, MDSally CadeKristi Coker, MSN, MHA, RNJeanine Halva-NeubauerJennifer Hudson, MDEmily HughesEric NashTerri Negron, MN, RNJanine Sally, MS, CCC-SLPRobert Saul, MD Kerry Sease, MD, MPH
If you would like your name added to or removed from our mailing list or have anycomments, questionsor suggestions, please send the appropriateinformation to:
Marketing ServicesGreenville Health System300 E. McBee Ave. Suite 200Greenville, SC 29601(864) 797-7538
The information contained in theFocus is for educational purposes only—it shouldnot take the placeof medical adviceor diagnoses madeby healthcare professionals.
All facilities and grounds of Greenville Health System are tobacco free.
“Greenville Health System” and GHS symbol design are trademarks of Greenville Health System.
Table of Contents
© 2015 Greenville Health System
15-21447442
On the cover: Cary Stroud, MD, jokes with Sam Esteban and his mother, Leslie Esteban. Dr. Stroud’s Supportive Care Team helps families like the Estebans who are experiencing frequent hospitalizations and/or chronic illness.
Cover and lead photography by Greg Beckner([email protected])
To access this publication online, go to www.ghs.org/publications.

From the Medical DirectorWilliam F. Schmidt III, MD, PhD
An Epic Transition
1
In June, two of our primary care practices commenced converting their electronic medical records (EMRs) from eCW (Electronic Clinical Works) to Epic as part of a pilot launch.
This new EMR software is a major investment for Greenville Health System (GHS), costing more than $100 million. We have spent a full year preparing for this transition, hoping to mitigate as many foreseeable difficulties as possible.
The conversion is going better than expected. Anticipating difficulties, we reduced the number of appointment slots at these two practices by 50% for the first two weeks of the switchover. We then planned to slowly increase availability to 100% over the following two weeks.
At Carolina Pediatrics of Greenville, the physicians adapted to the new EMR system so quickly that they were able to accommodate 106% of their usual visits on the first day, accepting call-ins as fast as arrived.
At Pediatric Associates–Greer, our second test site, full-visit capacity was achieved by the third day. All in all, this success represents a promising and gratifying start, thanks in large part to great can-do attitudes at our test sites and to our physician Epic champions, Drs.
Dominic Gault and Jeff Gerac, along with practice chiefs Drs. Nancy Song and Ed Hausladen.
The transition to Epic for the rest of our pediatric primary care sites and our pediatric specialty outpatient sites occurred July
16. Inpatient practices (PICU, NICU, Nursery, Hematology-Oncology), acute medical surgical practices and Kidnetics® (pediatric therapies) will move to Epic starting February 2016.
By this time next year, our
current 58 different EMRs will be combined into a single, enterprise-wide medical record, bringing us many advantages. Inpatient and outpatient visits will be available in the same EMR, along with imaging and lab results.
Up-to-date patient problem lists and medication reconciliations also will be available for every patient. Clinical information, registration, patient scheduling and billing will all be on the same system. And all clinical information can be shared effectively—and securely—with our entire health community.
By next summer, our Epic journey
will have combined our many different
EMRs into one enterprise-wide medical record.

2
Lead StoryChildren’s Hospital of Greenville Health System (GHS) offers a Supportive Care Team to address quality of life, psychosocial and other issues for some pediatric patients.
A Blanket of Care
Last year, Samuel Esteban spent 116 days as a patient at GHS Children’s Hospital. In 2011, he spent 101 days in the hospital.
Sam has severe spina bifida, and in his 12 short years, he has undergone 43 surgeries and a number of other infections and illnesses. Sam’s family, particularly his mother, Leslie Esteban, have been with him every step of the way. Esteban has spent every night but one with Sam while in the hospital.
“When we go, we go for a while,” she joked. “It’s our home away from home.”
Special Team Assists Pediatric Patients and Families Facing Chronic Illness
It is for patients like Sam, whose conditions cause them frequent and/or lengthy hospitalizations, that Children’s Hospital’s new Supportive Care Team was developed. Cary Stroud, MD, medical director of the Supportive Care Team, says the purpose is to “address the psychosocial needs of children and families with chronic illnesses of uncertain outcome.”
‘Thrown into the Trenches’The team’s purpose covers a wide range of situations and needs. For many families, the beginning is usually a major adjustment to news of a life-altering condition, and that’s something they often need help to process.
Sarah Pierce, CCLS, a child life specialist with the Supportive Care Team, uses a special doll to help Sam Esteban understand how his port works.

3
The Supportive Care Team holds meetings each morning to review pediatric patients and families in the hospital, and determine which patients need what services that day.
Esteban said although there wasn’t a comparable service when Sam was born in Atlanta, they’ve seen the value of that support when other families are suddenly facing an unexpected lifestyle change.
“I’ve seen kids in the pediatric ICU who have been flown in by helicopter because they’ve been in a horrible car accident, and the family is thrown into the trenches,” she said. “Their lives and their child’s life are changed forever. How do you prepare for that?”
The Supportive Care Team addresses these challenges by combining disciplines and backgrounds. Dr. Stroud served as medical director of the hospital’s BI-LO Charities Children’s Cancer Center for several years before he helped develop the Supportive Care Team. A second physician, S. Brooke Johnston, MD, completed a fellowship in pediatric hospice and palliative medicine. Other team members include Abby Rishovd, DNP, who has experience with pediatric hematology/oncology and transplant patients; Kathy Gentry, BSN, RN, who was previously a nurse in the Bryan NICU; chaplain Patrick Jinks, MDiv, BCC; and two child life specialists, Sarah Pierce, CCLS, and Memory Stein, CCLS.
“We try to bring everybody together and have each person, with his or her different experience, look at each patient and family situation and see what we can contribute,” remarked Dr. Johnston.
The Supportive Care Team holds meetings each morning to review pediatric patients and families in the hospital, and determine which patients need what services that day.
With new patients who have just received a life-changing diagnosis, a physician usually will sit down with the family to review all that’s happened up to that point and look at current treatment options as well as long-range plans.
“A large part of that meeting ends up being education and making sure that all of the information that other providers are sharing is getting through to the family in words that make sense to them,” Dr. Stroud noted.
Esteban said that aspect has been a big help to her, even after many years of becoming adjusted to her son’s diagnosis.
“Sam’s got about nine specialists on his team of doctors,” she said. “We’ve had numerous stays where a lot of doctors’ hands were in the pot. We have really good relationships with the doctors and never want to second-guess them, but we do have questions sometimes.”
Esteban continued, “Dr. Stroud has stepped in and been that person for us, to ensure the communication is happening the way it should, which has been really nice.”
When Baby Is IllMany families who receive the services of the Supportive Care Team are those with babies in the NICU.
“We have the largest NICU in South Carolina, so we have the sickest of the sick here, which creates a population needing our support,” Dr. Stroud pointed out.
Gentry and Rishovd spend much of their time with families in that area, reviewing information and offering sources of support. Sometimes, interactions begin before the baby is even born.
“We see families prenatally if they have a diagnosis where we know they’re going to have an extended hospitalization, or if the baby might not survive or will have a chronic illness,” Gentry explained. “So we help those families start coping even before the baby arrives.”
Dr. Stroud said the team helps parents develop a birthing plan if their baby is not expected to live long, outlining their desires for the moments immediately after birth. Pierce, a child life specialist, said she will often do memory-making activities with siblings of these NICU patients, particularly when the baby dies, to help them process what’s happening and remember their baby sibling.
Children’s Hospital has the largest NICU in South Carolina, and many of those patient families benefit from the services of the Supportive Care Team.

4
The good news, though, is that many of these tiny patients do survive, although they often have more medical issues than other children.
“Over the years, we’ve started to save more premature babies, and technology has allowed us to do that,” Gentry said. “However, it hasn’t allowed us to do that without consequences. These children will continue to need support throughout their entire childhood as they are in and out of the hospital frequently.”
Fortunately for those patients, though other circumstances may change—what wing of the hospital they are in and which specialists they are seeing, for example—members of the Supportive Care Team will be there.
“We’re a constant for the family as they’re adding different providers and specialists,” Rishovd said. “We’re the team who has known them from the beginning and can help bring everything together for them.”
Even though many of their patients do live into adulthood, by nature of their specialty, these team members must deal with the deaths of their patients more often than care providers in other specialties. It takes a team mentality to keep the group moving forward in spite of the emotional toll.
“There definitely has to be an intentionality about caring for oneself and caring for each other,” stated Jinks, the chaplain. “It’s never an individual thing.
The Supportive Care Team meets each morning to discuss which patients and families need the team’s services that day. From left: Kathy Gentry, BSN, RN; Brooke Johnston, MD; Cary Stroud, MD; Abby Rishovd, DNP; and Sarah Pierce, CCLS.
“We’re the team who has known them from the beginning and can help bring everything together for them.” —Abby Rishovd, DNP

5
It’s always a group thing in that we’re all kind of watching out for one another.”
Jinks said an extension of that is caring for and supporting the medical staff treating these patients, as each death takes a toll on those care providers. He said they sometimes hold support dinners or debriefing sessions to help co-workers cope with the difficult situations they see.
Goals for GrowthJinks said one goal of the program is to expand bereavement support for families when their child does not survive. Another goal is to add a psychologist and social worker.
Currently, team members cover these functions in addition to their regular duties. For instance, when Sam was being bothered by wounds caused by his wheelchair, Dr. Stroud stepped in to help secure a new chair.
“It’s really a social worker-type of responsibility, but he has been that person to say, ‘Let me get this ball rolling for you,’ and he’s made the phone calls himself,” Esteban observed.
And while the team’s services are available on an inpatient basis only, team members hope to one day offer an outpatient clinic for children who have chronic conditions but are healthy enough to be cared for at home.
“Outpatient care would allow us to offer continued care for things like symptom management, future planning and family support after a patient has left the hospital,” Dr. Johnston explained. “Other subspecialists have wanted to refer these children for our services but have been unable to do so as we need more staff as well as office space to meet with these families.”
To achieve these goals, team members are dependent on philanthropy. Dr. Stroud explained that under the general model for a pediatric palliative care program, a third of the support comes from hospital systems, a third from charges for services and a third from philanthropy.
“The problem is, so many of the things we provide, we can’t charge for,” Dr. Stroud said. “We can’t charge for child life services, we can’t charge for chaplain services, we can’t charge for social work services, and even
psychologist services are very limited in what we can charge fees for.”
He continued, “The things that are needed—that people recognize as important—are things we can’t get compensation for, which is why we have to depend on philanthropy in addition to hospital support and the charges that we can generate.”
One thing that is certain to Sam’s mother is that the services the team provides are invaluable. Esteban said the team members go the extra mile to connect with Sam on a personal level and let him know they are there for him, even bringing him gifts on occasion.
But to her, the most valuable service is the support, because even after a dozen years, she’s sometimes still overwhelmed by Sam’s care.
“It’s hard juggling all of it, and having that resource is great,” Esteban remarked. “I didn’t think I really needed it at first, but I’ve changed my mind. It’s not easy dealing with these conditions. Sometimes, it’s a little overwhelming. It’s nice to know that you have that support—it really is.”
For more information about the Supportive Care Team, visit ghschildrens.org/supportive-care or call (864) 546-8955. For information on giving, visit ghsgiving.org.
Dr. Stroud and the other members of the Supportive Care Team serve as a constant for families like the Estebans, who must visit the hospital often.

6
What’s New?Greenville Health System (GHS) opens a pediatric outpatient center in Spartanburg, starts clinics in four area middle schools and expands an annual lecture to a two-day pediatric resident education symposium.
Comprehensive Center Comes to Spartanburg
The Children’s Hospital Outpatient Center, a new facility in Spartanburg housing pediatric specialty practices along with Pediatric Associates–Spartanburg and Kidnetics® (pediatric therapies), has opened at 249 N. Grove Medical Park Drive. The 24,000-square-foot facility features nearly 40 exam rooms and is located near the intersection of Business Interstate 85 and Boiling Springs Road.
The combining of these three entities in one physical location makes it more convenient for Spartanburg parents to access the care they need for their children. The phone number for each entity will remain the same:
Pediatric Associates–Spartanburg: (864) 582-8135Pediatric Specialties: (864) 573-8732 Kidnetics: (864) 598-0420
GHS Launches Clinics in Four SchoolsAs part of a United Way of Greenville County program to ensure the success of middle school students, GHS will begin offering school-based clinics at Berea, Tanglewood and Lakeview middle schools and the Greenville Early College.
A registered nurse or nurse practitioner will travel to each school once a week to provide care for acute, non-emergent injuries and illnesses. Telemedicine will be used on the days the providers are not present so that the school nurse will be able to connect with a physician if a diagnosis is needed.
One of the primary goals of the program, called OnTrack Greenville, is to reduce absenteeism, which the clinics can help achieve. They also represent another step in increasing access to care for children in the Greenville area.
The United Way received a $3 million grant from the Social Innovation Fund, a program of the Corporation for National and Community Service, to help fund OnTrack Greenville. Through a competitive grant process, GHS earned a sub-grant that will help cover clinic costs.
DeLoache Seminar to Expand The annual DeLoache Pediatrics Lecture, named in honor of longtime Greenville pediatrician William R. DeLoache, MD, will expand this year into a two-day symposium—the William R. DeLoache, MD, Pediatric Resident Education Symposium—that will bring together current residents and alumni of Children’s Hospital’s Pediatric Residency Program.
The symposium will feature a nationally known speaker and highlight accomplishments of Children’s Hospital’s faculty, residents and fellows. It also will include posters from residents’ quality improvement projects, a joint Grand Rounds with Internal Medicine spotlighting the keynote speaker and platform presentations highlighting the research of Children’s Hospital faculty. An evening gala in Greenville’s West End will include a band, drinks and heavy hors d’oeuvres.
The speaker at this year’s symposium, scheduled for Nov. 5-6, will be Colleen Kraft, MD, of Cincinnati Children’s Hospital, an expert in population-based medicine. For more information about the symposium and how to register, call Dawn Van Lew at (864) 454-2420.

“When I’m on call, but not near a computer, I often get calls asking for help with a rash, and providers will email or text pictures. The diagnosis usually is not clear, and I find the VisualDx app
useful in expanding my differential diagnosis. I’ve also used it in the exam room when a patient’s rash is no longer present. I’ll show the family pictures of rashes from the app that I think are likely based on the description.”
Josh Brownlee, MDPediatric Infectious Disease Division
Free if done through your institution; $29.99/month or $299/year for individual users; for iPhone, iPad and Android devices
For GHS users:Search for “VisualDX” on Plexus, and create an account for your mobile device. Then follow the instructions in the email you receive.
“I recommend my patients download FatSecret to keep track of their exercise and calorie/fat intake. Keeping a diary is one of the most effective manners to change any behavior. A food diary makes
patients aware of the quantity and quality of their intake and helps them see where their excesses or deficits may be. Just the simple act of accountability and tracking everything that goes into your mouth is eye-opening.”
Manisha Patel, MDPediatric Cardiology Division
Free, for iPhone, iPad and Android devices
7
New TechnologyGHS pediatricians share ways they are using mobile apps to improve patient care.
“I use an app for iPhone called Pedi QuikCalc where you can find appropriate medication dosing based on a patient’s weight. Other features include a shot schedule, bilitool, and blood pressure
and growth charts.”
Ashley Godwin, MDPediatric Associates–Easley/Powdersville
$1.99; for iPhone and iPad devices
“LactMed, by the National Library of Medicine, provides information about medications and whether they are safe to use while breastfeeding. As we have achieved Baby-Friendly status at GHS,
questions about meds for mom while breastfeeding have come up frequently.”
Matt Grisham, MDGeneral Pediatrics, Greenville Memorial Hospital
Free; for iPhone, iPad and Android devices
What’s App, Doc?
(l-r) LactMed, VisualDx, Pedi QuikCalc

8
Medical Staff SpotlightChildren’s Hospital of Greenville Health System (GHS) announces a new director of Pediatric Hematology/Oncology and welcomes 11 new physicians.
Developmental-Behavioral Pediatrics
Victoria L. Sheppard-LaBrecque, MD, earned her medical degree from the University of Illinois College of Medicine in Urbana. She completed her pediatric residency at Loyola University Medical Center in Maywood, Ill.
After working as a pediatric hospitalist for three years, Dr. Sheppard-LaBrecque completed a fellowship in developmental-behavioral pediatrics at the University of Massachusetts Medical School in Worcester. She spent the last 14 years working with the Olson Huff Center for Child Development at Mission Children’s Hospital in Asheville, NC. She can be reached at (864) 454-5115.
General & Inpatient Pediatrics
Britni M. Bradshaw, MD, earned her medical degree at the University of South Alabama School of Medicine in Mobile, Ala. She completed her pediatric residency at GHS. Dr. Bradshaw is working as a pediatrician with the
Center for Pediatric Medicine. She can be reached at (864) 220-7270.
Rachael D. Davis, MD, earned her medical degree from Medical College of Georgia at Georgia Regents University in Augusta, Ga. She completed her residency training in pediatrics at GHS. Dr. Davis is working as a pediatrician
with the Center for Pediatric Medicine. She can be reached at (864) 220-7270.
Jennifer B. Harling, MD, earned her medical degree at Mercer University School of Medicine in Macon, Ga. She completed her residency training in pediatrics at GHS. Dr. Harling works as a pediatrician at Kids’ Care, an
urgent care facility at AnMed Women’s and Children’s Hospital. She can be reached at (864) 512-6544.
Anna C. Neal, MD, completed her medical degree at Louisiana State University School of Medicine in Shreveport, La. She completed her residency training in pediatrics at the University of Arkansas for Medical Sciences and Arkansas
Children’s Hospital in Little Rock, Ark. She has spent the last three years working as a pediatrician at Children’s Urgent Care at Blakeney with Carolinas HealthCare System in Charlotte, NC. Dr. Neal will be working as a pediatrician with Kids’ Care, a pediatric urgent care clinic at AnMed Women’s and Children’s Hospital in Anderson. She can be reached at (864) 512-6544.
Elizabeth A. Shirley, MD, attendedmedical school at the University ofSouth Carolina School of Medicinein Columbia, SC. She completedher pediatric residency at GHS. Dr.Shirley is working as a pediatrichospitalist for Children’s Hospital
at AnMed Health in Anderson. She can be reached at(864) 455-3512.
Rebecca P. Wright, MD, a Wofford College graduate, earned her medical degree and completed her pediatric residency at the University of South Carolina School of Medicine in Columbia. Dr. Wright is working as a newborn
hospitalist. She can be reached at (864) 455-3512.
Meet Our New Physicians

9
Neonatology
Nicole A. Cothran, MD, has joined Neonatology at Children’s Hospital as a member of Pediatrix Medical Group. Dr. Cothran earned her medical degree and completed her pediatric residency at the Eastern Virginia Medical School in Norfolk,
Va. She completed a perinatal/neonatal fellowship at the University of Pittsburgh Medical Center. She can be reached at (864) 455-7939.
Pediatric Hematology/Oncology
Cristina Fernandes, MD, earned her medical degree from Federal University of Bahia in Salvador, Brazil. She completed her residency in pediatrics at the Medical University of South Carolina (MUSC) in Charleston and University of South Florida Health in Tampa. Dr. Fernandes completed a fellowship in pediatric hematology/oncology at MUSC. She served for nine years as an assistant professor in Pediatrics at the University of Miami. She can be reached at (864) 455-8898.
Leslie E. Gilbert, MD, MSCI, a Wofford College graduate, attended medical school at the University of South Carolina School of Medicine in Columbia. She completed her pediatric residency at Levine Children’s Hospital at Carolinas
Medical Center in Charlotte, NC. Dr. Gilbert then completed a fellowship in pediatric hematology/oncology at Vanderbilt University/Monroe Carell Jr. Children’s Hospital. She also holds a Master of Science in Clinical Investigation degree. Dr. Gilbert can be reached at (864) 455-8898.
Aniket Saha, MD, MSCI, MS, completed medical school at St. George’s University School of Medicine in Grenada, West Indies. Dr. Saha also holds two MS degrees in clinical investigation and bioengineering. He completed
his residency in Pediatrics at Winthrop-University Hospital in Mineola, NY, and a fellowship in pediatric hematology/oncology at New York University’s Langone Medical Center in NYC. Dr. Saha spent the last two years serving as a physician at PM Pediatrics urgent care center in Syosset, NY, and as an attending in Pediatric Hematology/Oncology at Winthrop-University Hospital. He can be reached at (864) 455-8898.
Addie Hunnicutt, MD, presents Dr. Blouin with a gift from Children’s Hospital at a retirement reception in May.
Dr. Blouin RetiresRandall Blouin, MD, assistant medical director of Pediatric Neurology, retired in May after 18 years of service with GHS.
Dr. Blouin first joined GHS in 1976 as a resident with the Family Practice Program. Following completion of that residency, he began a pediatric residency at GHS. After completing a fellowship in pediatric neurology at Vanderbilt University from 1981-1984, Dr. Blouin returned to Greenville and joined Neurology Associates, seeing both adult and pediatric patients. He was the Upstate’s first fellowship-trained pediatric neurologist.
Dr. Blouin joined the Department of Pediatrics in 1997 and with Augusto Morales, MD, developed the Pediatric Neurology division at GHS. Since then, three other pediatric neurologists have joined the team. In 2010, the division launched the Epilepsy Monitoring Unit, with Dr. Blouin serving as medical director.
“Over the past 38 years, I’ve watched GHS grow from a single hospital on Mallard Street to what it is now,” Dr. Blouin reflected. “It’s been an amazing journey!”
We thank Dr. Blouin for his many years of service to the children of the Upstate!

Jonathan Markowitz, MD, MSCE, was featured in a cover story and photo in the May issue of the journal Infectious Diseases in Children. The story, on the subject of managing food allergies, included comments from Dr.
Markowitz on treatment options for eosinophilic esophagitis.
10
Markowitz, Raunikar Featured in Publications
The Duncan Chapel office of the Children’s Clinic is open and serving families in the north Greenville area. The office is located at 415 Duncan Chapel Road. Phone number is (864) 522-2600. Fax is (864) 522-2605.
R. Austin Raunikar, MD, was featured in Presbyterian College’s alumni magazine, which was published in May.
Dr. Bryant Assumes New Role
Nichole Bryant, MD, was named medical director of Pediatric Hematology/Oncology in April. Dr. Bryant has been part of this division since 2008. She is board-certified in pediatric hematology/oncology and completed a
fellowship in neuro-oncology at the University of Alabama at Birmingham School of Medicine.
Expanded Care for Complex NeedsIn April, GHS Children’s Hospital took over operations of the former Pediatric TEAM Center at Baptist Easley Hospital. Now called Children’s Hospital Center for Complex Health Conditions, the center offers pediatric therapy, medical care and caregiver education. Services of the center’s staff (including pediatrician Kent Jones, MD) have moved to the Center for Pediatric Medicine at 57 Cross Park Court in Greenville.
Pediatric therapies will be offered through Children’s Hospital’s Kidnetics program. For more information, call the Center for Complex Health Conditions at (864) 220-7270.

11
Congratulations Graduates!
Academic NewsChildren’s Hospital of Greenville Health System (GHS) congratulates all of our residents and fellows who graduated in May 2015, and welcomes 11 new Pediatric residents, five Medicine-Pediatrics residents and a new Developmental-Behavioral fellow.
PediatricBritni Bradshaw, MD, has joined GHS Children’s Hospital as co-chief pediatric resident and junior faculty member.
Jeff Broome, DO, began work in private practice at Parkside Pediatrics in Simpsonville, SC.
Jessica Crowe, MD, began work in private practice at Clinton Pediatrics in Clinton, Tenn.
Rachael Davis, MD, has joined Children’s Hospital as co-chief pediatric resident and junior faculty member.
Sarahbeth Eriksen, MD, began work in private practice at Pediatric Partners of Augusta in Augusta, Ga.
Jennifer Harling, MD, is working as a pediatric hospitalist for Children’s Hospital at Kids’ Care minor care clinic at AnMed Health in Anderson.
Sarah Oliver, MD, is working as a general pediatrician at Rockcastle Pediatrics and Adolescents in Mt. Vernon, Ky.
Holly Payne, MD, began work in private practice at Mercy Pediatrics in Paducah, Ky.
Liz Shirley, MD, is working as a pediatric hospitalist for Children’s Hospital at AnMed Women’s and Children’s Hospital in Anderson, SC.
Jenny Thomas, MD, is taking time off before pursuing a pediatric position.
Andy Wilt, MD, is working as a pediatric hospitalist at Niswonger Children’s Hospital in Johnson City, Tenn.
Medicine-PediatricsSam Holdiness, MD, joined the Med-Peds practice of Kosciusko Medical Clinic in Kosciusko, Miss.
Laura Johnson, MD, has joined the faculty of the Department of Family Medicine at GHS.
Kelly Kays, MD, is working as a Med-Peds hospitalist at Maury Regional Medical Center in Columbia, Tenn.
Broome Crowe Davis
Harling Oliver Payne
Thomas Wilt
Johnson Kays Ravindran
Sen Ravindran, MD, is working as a Med-Peds hospitalist at rotating GHS locations and serving as associate program director for the Med-Peds Residency Program.
Jill Sullivan, MD, has started an adult hematology/oncology fellowship at Duke University School of Medicine.
Bradshaw
Eriksen
Shirley
Sullivan
Holdiness

12
PediatricEric Bankert, DO: Lincoln Memorial University–DeBusk College of Osteopathic Medicine, Harrogate, Tenn.
Meghan Jordan, MD: Medical University of South Carolina College of Medicine, Charleston, SC
Lindsey McAmis Gouge, MD: East Tennessee State University, Quillen College of Medicine, Johnson City, Tenn.
Matt McGee, MD: Mercer University School of Medicine, Macon, Ga.
Ashtin Nix, MD: University of Kentucky College of Medicine, Lexington, Ky.
Colton Ragsdale, MD: Texas Tech University Health Sciences Center Paul L. Foster School of Medicine, El Paso, Texas
Christine Riyad, MD: Medical University of South Carolina College of Medicine, Charleston, SC
Andreea Stoichita, MD: University of South Carolina School of Medicine, Columbia, SC
McGeeJordan
Riyad Stoichita
Nix
WinninghamTwitty
Busch Dean
Bankert RagsdaleGouge
Grenade Kidd Webb
Grace Twitty, MD: University of South Carolina School of Medicine, Columbia, SC
John “Rob” Winningham, MD: East Tennessee State University, Quillen College of Medicine, Johnson City, Tenn.
Victoria “Torie” Winningham, MD: East Tennessee State University, Quillen College of Medicine, Johnson City, Tenn.
Medicine-PediatricsMegan Busch, MD: University of South Carolina School of Medicine, Columbia, SC
Ryan Dean, MD: University of Minnesota Medical School, Minneapolis, Minn.
Tori Grenade, MD: Mercer University School of Medicine, Macon, Ga.
Charles Kidd, MD: East Tennessee State University, Quillen College of Medicine, Johnson City, Tenn.
Lécé Webb, MD: University of Louisville School of Medicine, Louisville, Ky.
Welcome, New Residents!
Winningham

Developmental-Behavioral Pediatrics Fellowship
Fellowship graduate Tara Cancellaro, MD, will join the faculty of Children’s Hospital’s Division of Developmental-
Behavioral Pediatrics in October.
New Developmental-Behavioral Fellow
Steven Ma, MD, has joined Children’s Hospital as a fellow with the Division of Developmental-Behavioral Pediatrics. He earned
his medical degree from the University of Texas Medical Branch School of Medicine in Galveston, Texas. Dr. Ma completed his pediatric residency at Georgia Regents University in Augusta, Ga.
13
Resident and Faculty Awards
The following doctors and caregivers were recognized at Pediatric Residency Program graduation ceremonies:
• Sarahbeth Eriksen, MD: Pediatric Resident Teaching Award (voted on by first- and second-year pediatric residents)
• Britni Bradshaw, MD: Pediatric Resident Teaching Award (voted on by medical students); Miracle Maker Award (given by pediatric faculty for extraordinary care, community service and furtherance of health education); House Staff Research Award (system-wide)
• Matthew Grisham, MD, and Joshua Brownlee, MD: John P. Matthews Jr., MD, Outstanding Faculty Teaching Award (given by residents to a general pediatrician and a subspecialist for superb teaching and enthusiasm for resident education)
• Michael Guyton, MD: Paul V. Catalana Exemplary Character Award (given by the graduating class to a caregiver who exhibits the qualities of honesty, fairness, compassion, altruism and leadership by example)
• Pediatric Intensive Care Unit: 2015 Division of the Year Award (chosen by pediatric residents)
• Jeffrey Broome, DO: Outstanding Grand Rounds Award
• Savonya McAllister, MD: Pediatric Resident Journal Club Award
• Senthuran Ravindran, MD: Medicine-Pediatrics Resident Achievement Award (chosen by pediatric faculty for teaching and research skills and commitment to education); Pediatric Resident Research Award; Gold Humanism and Excellence in Teaching Award (voted on by rising fourth-year students)
• Easter Pennington, MD: Inpatient Care Award (voted on by inpatient pediatric faculty)
• Emily C. Walroth, MD: Primary Care Award (for outstanding care in the outpatient setting as voted on by ambulatory pediatric faculty)
• Jennifer Harling, MD: Gold Humanism and Excellence in Teaching Award (voted on by rising fourth-year students)Pictured from left: Emily Campolong, Whitney Wheeler, Mary Van
Wert, Hannah Shull, Brittany Lamont (kneeling), Stephen Hudson.
In April, students at the University of South Carolina School of Medicine Greenville who are part of the Pediatric Interest Group organized an Easter/Spring Festival for children at Marshall I. Pickens Hospital. The event included an egg hunt, cookie decorating, field games and a water balloon toss.

14
In South Carolina, obesity rates have doubled since 1990, with more than one-third of middle school students considered overweight and nearly one-third of high school students (31%) considered overweight or obese. Approximately one-half of all African American children in rural areas of South Carolina are overweight or obese.
Another aspect of the obesity crisis is that children’s diets have become inadequate or deficient in several crucial nutrients, based on key recommendations of the Dietary Guidelines for Americans (DGA) 2010. Consistently, 30% to 40% of daily energy consumed by children and adolescents comes from calorie-dense, nutrient-poor foods and drinks.
Continuing Medical EducationArticle author Kristan Stewart, MPH, MS, RD, LD, is the dietitian for New Impact, a comprehensive weight-management program for children up to age 21 at Children’s Hospital of Greenville Health System (GHS). Her article is written under faculty direction of Kerry Sease, MD, medical director of New Impact.
Childhood Nutrition: Challenges and Tools AAP Recommends Whole-diet Approach to Children’s Nutrition
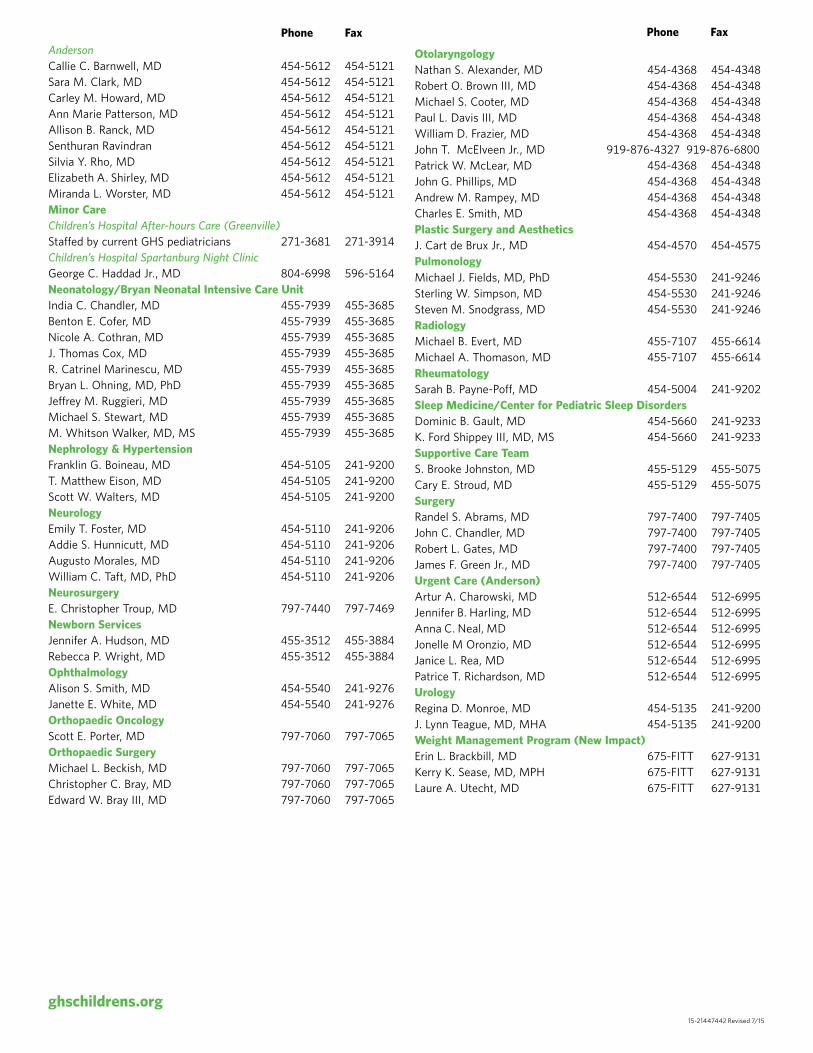
The Pediatric Obesity Crisis The rising rate of obesity in the United States has resulted in increased attention to nutrition and long-term health. In 2009-2010, 16.9% of US children and adolescents were obese, defined as having a body mass index (BMI) greater than or equal to the age- and sex-specific 95th percentiles of the 2000 CDC growth charts. Prevalence rates were higher among teens and school-age children than preschool-age children and among boys than girls (Figure 1).
Recent studies indicate that obesity levels in the United States have begun to level off—there was no change in the prevalence of obesity among children from 2007-2008 to 2009-2010. Even so, several public health concerns remain.
15
Energy balance—the balance of calories consumed through eating and drinking with calories burned through physical activity—is one of many reasons to promote healthful eating habits in children. Age-appropriate energy and nutrient intake are essential to support normal growth and development and to prevent acute nutrition problems such as iron-deficiency and dental caries.
In addition, healthy eating and physical activity can reduce the risk of early development of diet-related chronic diseases such as cardiovascular disease, type 2 diabetes, cancer, obesity, and osteoporosis. Furthermore, these healthy habits promote learning and academic success.
Parents and other caregivers need education about nutrition and mealtime behaviors that promote the adoption of healthy eating habits in their children’s lives.
Family Dinners: Convenience Over HealthThe home environment is important to children’s nutritional intake. The once-traditional pattern of the family having dinner together at the table has changed. Time and convenience are major influences in food choices, and the desire to limit the amount of time spent in food preparation and nutrition monitoring has taken priority over researching and preparing healthier meals.
When parents and food providers have demanding schedules such as long hours away from home or evening shifts or activities, they often cope with time challenges by using more takeout meals and precooked entrees. These foods tend to be higher in energy and fat compared to food prepared and eaten at home.
For children, fast food now is the largest contributor to foods prepared away from home—having surpassed foods eaten at school. Fast food meals contribute fewer servings of fruits, vegetables, whole grains, and dairy products and higher intakes of energy, fat, and sugar. Regular consumption of such food leads to poorer diet quality.
Conversely, having family meals provides psychological benefits such as a positive impact on
children’s beliefs and attitudes in addition to an inverse association with the onset and persistence of being overweight.
Importance of Healthy HabitsData from the National Health and Nutrition Examination Survey (NHANES) indicate that approximately 20% of children skip breakfast. These children tend to consume less energy and nutrients and have lower school performance than children who eat breakfast.
In addition, the survey showed that snacking has drastically increased among children. More than 27% of children’s daily caloric intake came from snacks, with the largest increases in salty snacks and candy. Desserts and sweetened beverages represent the snack categories that contain the most calories.
Recent surveys show consumption of fruit juice has increased by 50%. Consumption of soft drinks and other sugar-sweetened beverages is associated with greater caloric intake and decreased fruit and vegetable intake among children who drink medium and large amounts.
Greater emphasis needs to be placed on encouraging better meal patterns, including eating breakfast, more balanced meals and appropriate, healthy snacks.
If current trends continue, one out of three children born in South Carolina in the year 2000 will be a high risk for type 2 diabetes, primarily because of poor diet and lack of physical activity.
Figure 1: Prevalence of Obesity Among Children and Adolescents Ages 2-19, United States (2009-10)
CDC/NCHS, National Health and Nutrition Examination Survey, 2009-2010http://www.cdc.gov/nchs/data/databriefs/db82.pdf
0
5
10
15
20
25
All Boys Girls
Age 2-19 Age 2-5 Age 6-11 Age 12-19

16
Portion DistortionPortion sizes consumed both at home and away from home have increased significantly since 1977. Several studies have shown that providing children with larger food portions leads to significant increases in food and energy intake. Package size, serving size, and dishware size all influence how much people eat, and all have increased significantly in recent decades:
• At the supermarket, package size increased 10-fold between 1970 and 2000.
• At restaurants, jumbo-sized portions are consistently 250% larger than the regular portion.
• At home, bowls and glasses have steadily increased in size, and the surface area of the average dinner plate has increased 36%.
These increases have led to an increase in the amount people assume they should eat or drink to be full. The larger sizes set an expectation for people to serve and eat more food than smaller plates or smaller packages would suggest. This norm can inhibit people, especially children, from identifying and listening to hunger and satiety cues.
Furthermore, large portion sizes lead to underestimation of calories. The ability to monitor or estimate how many calories one is eating becomes increasingly less accurate as portion sizes increase. With any large portion of food, a lot of calories can be eaten before there is any noticeable difference that the supply has decreased.
Encouraging a change in the home and outside environment, such as choosing smaller packages, servings, and dinnerware, can help with portion control. We also must remind parents that children do not need the same serving size as an adult.
Schools on the Right TrackChildren consume 47% of their calories each day from meals and snacks consumed at school. Much progress has been made in schools in the last decade to improve the health and nutrition of our nation’s children.
Since 1995, steady improvements have been made that include serving meals with more lean meats, lower fat milks, and more fruit, vegetables, and whole grains.
National standards now limit the types of food and drinks sold in schools. The Healthy, Hunger Free Act of 2010 requires national nutrition standards to be set for all foods sold on school campuses throughout the day.
The act also requires schools to plan food-based menus versus nutrient-based menus (e.g., one cup of fruit as opposed to a certain amount of vitamin A). The breakfast and lunch changes that are being implemented in phases include:
• Minimum requirements of fruits and vegetables• A student must have a fruit or vegetable on his or her
tray• Minimum and maximum calorie levels• Strict sodium requirements• Low-fat or fat-free milk and 100% whole grain
products must be offered• Lower fat and no trans-fat content in foods
However, these improvements to school meals are largely lost on the population of students who bring lunches from home. A study published in the Journal of Nutrition Education and Behavior compared school lunches to lunches students brought from home at three Virginia schools over a five-day period. The study reports the following:
• Sixty-one percent of school lunches contained a vegetable other than juice, compared to 17% of packed lunches.
• Five percent of school lunches included chips or crackers compared to 57% of packed lunches.
• School lunches did not include dessert, compared to 61% of packed lunches, with 17% including more than one dessert.
• School lunches contained less saturated fat and sugar, more protein, fiber, vitamin A and calcium than packed lunches.
Parents must be encouraged to take a close look at the foods they are providing in their children’s lunches to help their offspring achieve better health.
The Whole-diet ApproachIn a new policy statement issued by the American Academy of Pediatrics (AAP), the organization recommends considering a child’s overall diet pattern rather than the amounts of sugar, fat or specific nutrients in individual foods. Parents and caregivers need to offer more balanced and proportioned, nutrient-dense meals and snacks at home as well as in packed lunches. In addition, parents and caregivers play a crucial role in a child’s development of life-long healthy eating habits.
The whole-diet recommendations are consistent with the fundamental principles of the 2010 Dietary

17
Parents must be encouraged to take a close look at the foods they are providing in their children’s lunches to help their offspring achieve better health.
Guidelines for Americans (DGA). The DGA defines total diet as the combination of food and beverages that provide energy and nutrients and constitute an individual’s complete dietary intake, on average, over time. As previously mentioned, schools are using and/or phasing in this approach through the Healthy, Hungry Kids Act of 2010.
The AAP recommends a five-step approach for parents when selecting foods at home and for school:
• Select a mix of foods from the five food groups—vegetables, fruits, grains, low-fat dairy, and quality protein sources such as lean meats, fish, nuts, seeds, and eggs
• Offer a variety of food experiences• Avoid highly processed foods• Use small amounts of sugar, salt, fat, and oils with
highly nutritious foods to enhance enjoyment and consumption
• Offer appropriate portions
Key Messages and ToolsMany children do not meet the minimum recommendations for the fruit, vegetable, grain or dairy groups, and they exceed the recommendations for total and saturated fats. Other concerns include energy balance and high intakes of sugar and sodium. There are several key messages/tools being utilized to meet the DGA.
One tool for helping children meet the DGA is the USDA’s MyPlate (Figure 2), which provides a visual of how a plate should look with emphasis on portion sizes and nutrient-dense foods for each food group. The simplicity of this visual aid along with clear, defined messages can help practitioners provide recommendations as well as assist parents and caregivers to accomplish healthy eating habits.
Other key messages include the 5-2-1-0 graphic, which brings awareness to daily recommendations for diet and physical activity, and the Go, Slow, Whoa chart, which helps guide families in making healthy food choices (Figure 2). Many of these messages already are displayed in schools.
Figure 2
or more fruits & vegetables hours or less recreational screen time*
hour or more of physical activity sugary drinks, more water & low fat milk
*Keep TV/Computer out of the bedroom. No screen time under the age of 2.
FRUITS Fuel Up With Fruits at Meals or Snacks Oranges, pears, berries, watermelon, peaches, raisins, and applesauce (without extra sugar) are just a few of the great choices. Make sure your juice is 100% fruit juice.
VEGETABLES Color Your Plate With Great-Tasting VeggiesTry to eat more dark-green, red, and orange vegetables, and beans and peas.
GRAINS Make at Least Half Your Grains Whole GrainsChoose whole-grain foods, such as whole-wheat bread, oatmeal, whole-wheat tortillas, brown rice, and light popcorn, more often.
PROTEIN Vary Your Protein FoodsTry fish, shellfish, beans, and peas more often. Some tasty ways include a bean burrito, hummus, veggie chili, fish taco, shrimp or tofu stir-fry, or grilled salmon.
DAIRY Get Your Calcium-Rich FoodsChoose fat-free or low-fat milk, yogurt, and cheese at meals or snacks. Dairy foods contain calcium for strong bones and healthy teeth.
Know Your “Sometimes” Foods Look out for foods with added sugars or solid fats. They fill you up so that you don’t have room for the foods that help you eat smart and play hard.
Serving Up MyPlate http://teamnutrition.usda.govU.S. Department of Agriculture • Food and Nutrition Service • September 2012 • FNS-451 • USDA is an equal opportunity provider and employer.
Eat Smart To Play HardUse MyPlate to help you fuel up with foods from each food group.
Keep on Moving!You need at least 60 minutes of
physical activity each day. Whether that’s skateboarding, tossing a ball,
or playing tag, every little bit counts!
“G ” “ w” “ oa”
U R What U Eat Food supplies the nutrients needed to fuel your body so you can perform your best. Go, Slow, Whoa is a simple way to recognize foods that are the smartest choices. • Foods: Eat almost anytime (Most often) — they are lowest in fat, added sugar, and calories • Foods: Eat sometimes (Less often) — they are higher in fat, added sugar, and/or calories • Foods: Eat once in a while (Least often) — they are very high in fat and/or added sugar, and are much higher in calories
Food Groups GO SLOW WHOA Fruits Whole fruits (fresh, frozen, canned, dried) are smart choices. You need 2 cups of fruit a day. 1 cup is about the size of a baseball.
Vegetables Adding fat (butter, oils, and sauces) to vegetables turns them from Go foods to Slow or Whoa foods.You need 2 ½ cups of vegetables a day. Dark green and orange vegetables are smart choices.
Grains Try to make at least half of your servings whole grain choices and low in sugar. An ounce of a grain product is 1 slice of bread, 1 cup of dry cereal, or ½ cup of cooked rice or pasta.You need about 6 ounces a day.
Milk Milk products are high in vitamins and minerals. Fat-free and low-fat milk and milk products are smart choices. About 3 cups are needed each day; 1 cup of milk,1 cup of yogurt or 1 ½ ounces of natural cheese count as 1 cup.
Meats & Beans Eating 5 ½ oz. a day will give you the protein, vitamins and minerals you need. Limit meats with added fat. Smart choices include beans (¼ cup cooked), nuts (½ oz.) and lean meats (1 oz.) baked or broiled.
The amounts of foods recommended per food group are based on a 2,000-calorie diet, the approximate number of calories for most active boys and girls ages 9-13. U.S. Department of Agriculture, Center for Nutrition Policy and Promotion.
We Can! and the We Can! logo are trademarks of the U.S. Department of Health & Human Services (DHHS). U.S. Department of Health & Human Services.

18
Messages are more likely to result in healthy dietary and lifestyle changes when they have a consistent emphasis on a total dietary pattern that is balanced and moderate. To reduce confusion from the high volume and occasional inconsistency of nutrition advice, the Academy of Nutrition and Dietetics (AND) has several recommendations summarized in Table 1.
ConclusionThe evidence is clear that children are not meeting the minimum requirements established by the DGA principles. Focusing on the total diet and overall eating patterns instead of specific foods and nutrients appears to be the best approach to meeting these requirements. Key messages from the DGA—maintaining an appropriate calorie balance and focusing on nutrient-dense foods and beverages—can help improve overall healthy eating patterns. There is an ongoing need for nutrition education with children, their parents and caregivers that should be provided by all healthcare practitioners.
References• Wansin B, Van Inttersum K. Portion Size Me: Downsizing
Our Consumption Norms. Journal of the American Dietetic Association. 2007;107:925-945.
• Position of the Academy of Nutrition and Dietetics: Nutrition Guidance for Healthy Children Ages 2 to 11 Years. Journal of the Academy of Nutrition and Dietetics. 2014;114:1257-1276
• Position of the Academy of Nutrition and Dietetics: Total Diet Approach to Healthy Eating. Journal of the Academy of Nutrition and Dietetics. 2013;113:307-317.
• AAP Committee on Snacks, Sweetened Beverages, Added Sugars and Schools. Pediatrics. 2015;135(3):575-583.
• Healthier School Meals: A Summary of the New USDA Standards for School Breakfast and Lunch. http://frac.org/federal-foodnutrition-programs/school-meal-nutrition-standards/.
Table 1AND Recommendations 1. Support and promote use of the USDA’s MyPlate as a guide for meeting
dietary recommendations with use of the Eat Smart to Play Hard.2. Promote a variety of foods, i.e., an eating pattern that includes foods from
all MyPlate food groups and subgroups. 3. Promote proportionality—consuming more nutrient-dense foods and
beverages (fruit, vegetables, whole grains, fat-free or low-fat milk products), and fewer calorie-dense foods.
4. Promote moderation of foods by limiting overall portion size and intake of saturated and trans fat, added sugars, cholesterol, and salt.
5. Emphasize gradual improvement—take small steps to improve diet and lifestyle each day.
6. Emphasize food patterns, rather than individual nutrients or individual foods.
7. Highlight the importance of obtaining nutrients from foods rather than unnecessary reliance on supplements.
8. Stress that physical activity complements the total diet approach, as it permits individuals to help manage weight and lowers the risk of premature diseases.
CME Questions Available OnlineAs a convenience for our audience and to conserve resources, Focus on Pediatrics has transitioned to an online format for the Q&A portion of CME articles. Here is a link and a QR code you can use to access the CME questions online.
http://www.ghs.org/PediatricsElectronic
CME Credit InformationTo receive possible continuing medical education (CME) credit for this article, please complete the online Q&A that can be accessed below. Both physicians and nurses are eligible to test for the credit.
It is the policy of the GHS Continuing Medical Education Committee to ensure balance, independence, objectivity and scientific rigor in all its individually sponsored or jointly sponsored education activities. Article author Kristan Stewart, MPH, MS, RD, LD, has disclosed that she has no significant financial interest or relationship with any company that may be considered an actual or potential conflict of interest with this educational activity.
Resources• Eat Smart, Move More South Carolina, a 501(c)(3) nonprofit organization,
is dedicated to positively impacting the health of all South Carolinians by promoting healthy eating and active living where we live, learn, work, pray and play. The organization also assists in the implementation of South Carolina’s Obesity Prevention Plan. (eatsmartmovemoresc.org)
• LiveWell Greenville, formed in 2011 by the Piedmont Health Care Foundation, is a partnership of more than 100 public and private organizations committed to making Greenville County a healthier place to live, work and play. It brings community partners and individuals together to shepherd positive initiatives such as creating safe places to bike and walk, and providing healthier foods in schools and workplaces, nutritious snacks in child care centers and better access to parks. (livewellgreenville.org)
• New Impact is a part of GHS Children’s Hospital, and provides a comprehensive weight management program for children up to age 21. The mission is to treat overweight and obese children in upstate South Carolina and empower them to develop active and healthy lifestyles through targeting the exercise and eating behavior of the entire family system. The program, which consists of a multidisciplinary team, provides individual nutrition counseling, partners with participating upstate YMCAs to provide the exercise component of the program, and offers monthly cooking classes as well as other resources.
• YMCA Greenville is part of the nation’s leading nonprofit committed to strengthening communities through youth development, healthy living and social responsibility. The YMCA encourages good health and fosters connections through fitness, sports, fun, and shared interests. Families receive support, guidance and resources needed to achieve greater health and well-being. (ymcagreenville.org)
• Kids Eat Right (Academy of Nutrition and Dietetics and its Foundation) provides comprehensive, science-based resources for families on eating right, cooking healthy, and shopping smart, with tips, recipes, videos, and in-depth information. (eatright.org/kids)
• USDA’s MyPlate provides science-based resources for parents and educators, including tip sheets on nutrition as well as games, activity sheets, videos, songs, and recipes for kids. (choosemyplate.gov)

Continued on back
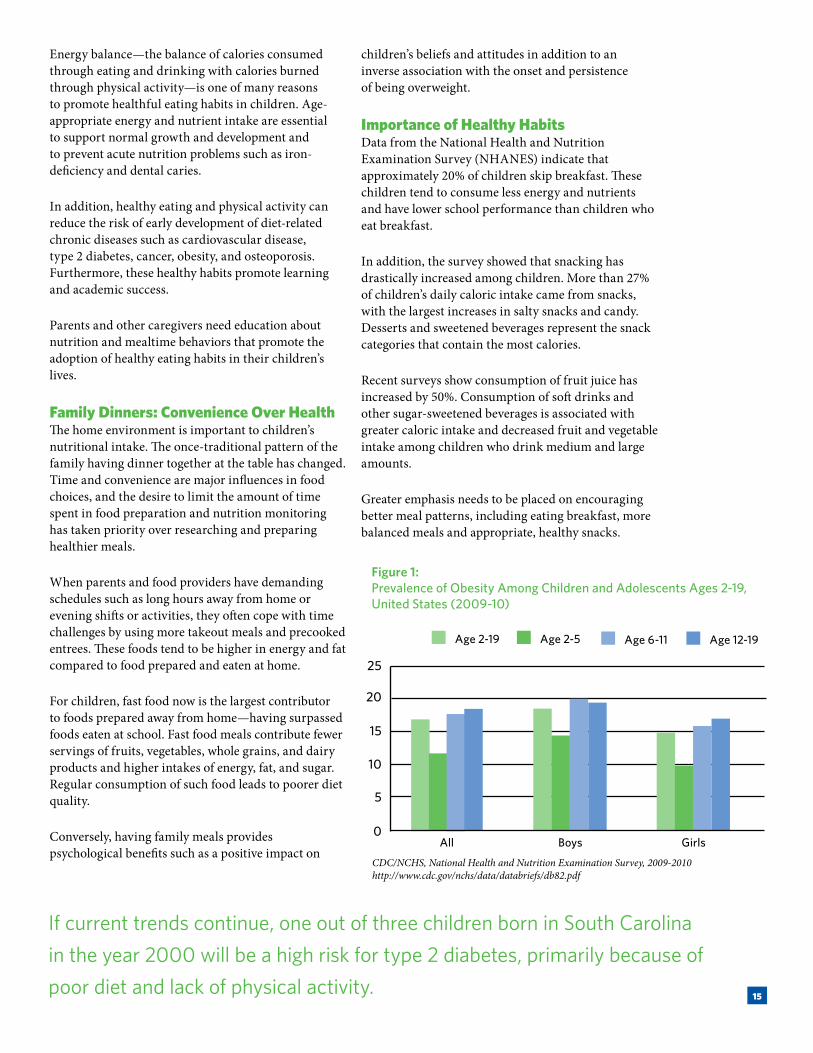
GHS Children’s Hospital Physician Directory
Phone Fax Phone FaxWilliam F. Schmidt III, MD, PhD 455-8401 455-3884 Medical Director; Chairman, Department of Pediatrics
Adolescent Bariatric Surgery Eric S. Bour, MD 676-1072 676-0729Adolescent Medicine Michael F. Guyton Jr., MD 220-7270 241-9211 Allergy, Immunology and Asthma Charles W. Greene Jr., MD 675-5000 675-5005James L. Kuhlen Jr., MD 675-5000 675-5005John M. Pulcini, MD 675-5000 675-5005 Ambulatory Pediatrics/Center for Pediatric Medicine (Medicaid)J. Blakely Amati, MD 220-7270 241-9211Jessica P. Boyd, MD 220-7270 241-9211 Britni M. Bradshaw, MD 455-9261 455-9264Elizabeth W. Burton, MD 220-7270 241-9211Rachael D. Davis, MD 220-7270 241-9211Janelle E. Godlewski, MD 220-7270 241-9211 Jill D. Golden, MD 220-7270 241-9211 Lochrane Grant, MD 220-7270 241-9211 Michael F. Guyton Jr, MD 220-7270 241-9211 Robert A. Saul, MD 220-7270 241-9211Kerry K. Sease, MD, MPH 220-7270 241-9211Cady F. Williams, MD 220-7270 241-9211Center for Complex Health ConditionsW. Kent Jones, MD 220-7270 241-9211Pediatric Rapid Access (Medicaid)Doreen P. Patterson, MD 220-7270 241-9211 Angela M. Young, MD 220-7270 241-9211Anesthesiology Carlos L. Bracale, MD 242-4602 242-0129Michael G. Danekas, MD 242-4602 242-0129Lauren H. Doar, MD 242-4602 242-0129John P. Kim, MD 242-4602 242-0129Richard F. Knox, MD 242-4602 242-0129 Steven W. Samoya, MD 242-4602 242-0129 Matthew R. Vana, MD 242-4602 242-0129 Randall D. Wilhoit III, MD 242-4602 242-0129Cardiology Benjamin S. Horne III, MD 454-5120 241-9202Jon F. Lucas, MD 454-5120 241-9202 David G. Malpass, MD 454-5120 241-9202Manisha S. Patel, MD 454-5120 241-9202R. Austin Raunikar, MD 454-5120 241-9202Child Abuse/Neglect / Forensic PediatricsMary-Fran R. Crosswell, MD 335-5288 331-0565Nancy A. Henderson, MD 335-5288 331-0565Critical Care Michael G. Avant, MD 455-7146 455-5380 Eric L. Berning, MD 455-7146 455-5380Darryl R. Gwyn, MD 455-7146 455-5380 Robert S. Seigler, MD 455-7146 455-5380
Developmental-Behavioral Peds/Gardner Center for Developing Minds James H. Beard Jr., MD 454-5115 241-9205Gerald J. Ferlauto, MD 454-5115 241-9205R. Lynne Hornsby, MD 454-5115 241-9205 Desmond P. Kelly, MD 454-5115 241-9205Nancy R. Powers, MD 454-5115 241-9205Victoria L. Sheppard-LaBrecque, MD 454-5115 241-9205John E. Williams, MD 454-5115 241-9205Emergency Medicine Elizabeth L. Foxworth, MD 455-6016 455-6199Jacqueline J. Granger, MD 455-6016 455-6199Alison M. Jones, MD 455-6016 455-6199Matthew B. Neal, MD 455-6016 455-6199Kevin A. Polley, MD 455-6016 455-6199John D. Wilson Jr., MD 455-6016 455-6199Endocrinology James A. Amrhein, MD 454-5100 241-9238Elaine A. Apperson, MD 454-5100 241-9238Bryce A. Nelson, MD, PhD 454-5100 241-9238 GastroenterologyLiz D. Dancel, MD 454-5125 241-9201 Michael J. Dougherty, DO 454-5125 241-9201 Emily N. Kevan, MD 454-5125 241-9201Jonathan E. Markowitz, MD, MSCE 454-5125 241-9201 Colston F. McEvoy, MD 454-5125 241-9201Genetics David B. Everman, MD 250-7944 250-9582R. Curtis Rogers, MD 250-7944 250-9582Gynecology Benjie B. Mills, MD 455-1600 455-2805Hematology/Oncology / BI-LO Charities Children’s Cancer CenterNichole L. Bryant, MD 455-8898 241-9237Rebecca P. Cook, MD 455-8898 241-9237Cristina E. Fernandes, MD 455-8898 241-9237Leslie E. Gilbert, MD, MSCI 455-8898 241-9237Aniket Saha, MD, MSCI, MS 455-8898 241-9237William F. Schmidt III, MD, PhD 455-8898 241-9237Infectious Disease Joshua W. Brownlee, MD 454-5130 241-9202Sue J. Jue, MD 454-5130 241-9202 Robin N. LaCroix, MD 454-5130 241-9202 Inpatient PediatricsGreenville April O. Buchanan, MD 455-8401 455-3884Karen Eastburn, DO, MS 455-8401 455-3884Jeffrey A. Gerac, MD 455-4411 455-4480Matthew P. Grisham, MD 455-8401 455-3884Amanda G. Hartke, MD, PhD 455-8401 455-3884Russ C. Kolarik, MD 455-7844 455-3884Elizabeth S. Tyson, MD 455-8401 455-3884GreerMatthew N. Hindman, MD 455-4411 455-4480
For admission to Children’s Hospital: (864) 455-0000
Phone Fax Phone FaxAndersonCallie C. Barnwell, MD 454-5612 454-5121Sara M. Clark, MD 454-5612 454-5121Carley M. Howard, MD 454-5612 454-5121Ann Marie Patterson, MD 454-5612 454-5121Allison B. Ranck, MD 454-5612 454-5121Senthuran Ravindran 454-5612 454-5121Silvia Y. Rho, MD 454-5612 454-5121Elizabeth A. Shirley, MD 454-5612 454-5121Miranda L. Worster, MD 454-5612 454-5121Minor CareChildren’s Hospital After-hours Care (Greenville)Staffed by current GHS pediatricians 271-3681 271-3914Children’s Hospital Spartanburg Night Clinic George C. Haddad Jr., MD 804-6998 596-5164Neonatology/Bryan Neonatal Intensive Care UnitIndia C. Chandler, MD 455-7939 455-3685Benton E. Cofer, MD 455-7939 455-3685 Nicole A. Cothran, MD 455-7939 455-3685J. Thomas Cox, MD 455-7939 455-3685R. Catrinel Marinescu, MD 455-7939 455-3685 Bryan L. Ohning, MD, PhD 455-7939 455-3685 Jeffrey M. Ruggieri, MD 455-7939 455-3685 Michael S. Stewart, MD 455-7939 455-3685 M. Whitson Walker, MD, MS 455-7939 455-3685 Nephrology & Hypertension Franklin G. Boineau, MD 454-5105 241-9200T. Matthew Eison, MD 454-5105 241-9200Scott W. Walters, MD 454-5105 241-9200Neurology Emily T. Foster, MD 454-5110 241-9206Addie S. Hunnicutt, MD 454-5110 241-9206 Augusto Morales, MD 454-5110 241-9206 William C. Taft, MD, PhD 454-5110 241-9206 Neurosurgery E. Christopher Troup, MD 797-7440 797-7469Newborn Services Jennifer A. Hudson, MD 455-3512 455-3884Rebecca P. Wright, MD 455-3512 455-3884Ophthalmology Alison S. Smith, MD 454-5540 241-9276 Janette E. White, MD 454-5540 241-9276 Orthopaedic Oncology Scott E. Porter, MD 797-7060 797-7065Orthopaedic Surgery Michael L. Beckish, MD 797-7060 797-7065Christopher C. Bray, MD 797-7060 797-7065Edward W. Bray III, MD 797-7060 797-7065
Otolaryngology Nathan S. Alexander, MD 454-4368 454-4348Robert O. Brown III, MD 454-4368 454-4348Michael S. Cooter, MD 454-4368 454-4348Paul L. Davis III, MD 454-4368 454-4348William D. Frazier, MD 454-4368 454-4348 John T. McElveen Jr., MD 919-876-4327 919-876-6800Patrick W. McLear, MD 454-4368 454-4348 John G. Phillips, MD 454-4368 454-4348 Andrew M. Rampey, MD 454-4368 454-4348 Charles E. Smith, MD 454-4368 454-4348Plastic Surgery and Aesthetics J. Cart de Brux Jr., MD 454-4570 454-4575Pulmonology Michael J. Fields, MD, PhD 454-5530 241-9246 Sterling W. Simpson, MD 454-5530 241-9246Steven M. Snodgrass, MD 454-5530 241-9246Radiology Michael B. Evert, MD 455-7107 455-6614 Michael A. Thomason, MD 455-7107 455-6614RheumatologySarah B. Payne-Poff, MD 454-5004 241-9202Sleep Medicine/Center for Pediatric Sleep DisordersDominic B. Gault, MD 454-5660 241-9233K. Ford Shippey III, MD, MS 454-5660 241-9233Supportive Care Team S. Brooke Johnston, MD 455-5129 455-5075Cary E. Stroud, MD 455-5129 455-5075 Surgery Randel S. Abrams, MD 797-7400 797-7405 John C. Chandler, MD 797-7400 797-7405 Robert L. Gates, MD 797-7400 797-7405 James F. Green Jr., MD 797-7400 797-7405 Urgent Care (Anderson)Artur A. Charowski, MD 512-6544 512-6995 Jennifer B. Harling, MD 512-6544 512-6995Anna C. Neal, MD 512-6544 512-6995 Jonelle M Oronzio, MD 512-6544 512-6995Janice L. Rea, MD 512-6544 512-6995 Patrice T. Richardson, MD 512-6544 512-6995UrologyRegina D. Monroe, MD 454-5135 241-9200J. Lynn Teague, MD, MHA 454-5135 241-9200Weight Management Program (New Impact)Erin L. Brackbill, MD 675-FITT 627-9131Kerry K. Sease, MD, MPH 675-FITT 627-9131Laure A. Utecht, MD 675-FITT 627-9131
15-21447442 Revised 7/15
ghschildrens.org

19
Quality CountsArticle author Robin LaCroix, MD, is vice chair of Medical Staff Affairs for Children’s Hospital at Greenville Health System (GHS) and a Pediatric Infectious Disease physician at GHS. Dr. LaCroix can be reached at (864) 454-5130.
The Alphabet of Quality
Many practitioners navigating the insurance and exchange maze now face a multitude of acronyms representing quality.
The National Center for Quality Assurance (NCQA) is the group that accredits and certifies practices and health plans as having met nationally established quality measure criteria. These criteria are designed to standardize practices.
NCQA has a foundation of evidence-based quality measures. The most well-known accreditation overseen by NCQA is the Patient-Centered Medical Home (PCMH), a designation that the Center for Pediatric Medicine (CPM) at GHS Children’s Hospital achieved in 2013. In fact, CPM was the first pediatric practice in the state to attain Level 3 (highest level) recognition.
Twelve of 14 GHS primary care pediatric practices have since received Level 3 PCMH status (see Page 20). The other two are new GHS offices.
The NCQA also establishes Healthcare Effectiveness Data and Information Set (HEDIS) measures. These tools—used by over 90 percent of the nation’s health
plans to measure quality performance—allow for a standard comparison of care delivery by providers.The care we as physicians provide now is benchmarked against other doctors’ care to provide standard expectations for insurance providers and patients.
Becoming familiar with the current quality measures being used and ensuring the necessary documentation are key initial steps. The goal of these measures is to be recognized as a practice that excels at delivering evidence-based care.
HEDIS measures that directly apply to pediatrics include …
• Weight assessment and nutrition counseling for children and adolescents
• Childhood and adolescent immunizations• Appropriate testing for children with pharyngitis• Appropriate treatment for children with upper
respiratory infection (URI)• Well child visits the first 15 months of life• Well child visits ages 3-6 years of life• Adolescent well care visits• Follow-up care for children with URI• Metabolic monitoring for children and adolescents
on antipsychotics• Use of first-line psychosocial care for children and
adolescents on antipsychotics• Evaluation of use of multiple concurrent
antipsychotics in children and adolescents
Included in the benchmarking activities are Consumer Assessment of Healthcare Providers and Systems (CAHPS) surveys. CAHPS surveys allow patients to give feedback on services they have received from your practice or consultants to whom you referred them.
Knowledge of these standards helps practices understand the platform that payers and consumers use to determine the network and providers they want involved in the care of their families.

Pediatric Practices Earn Medical Home RecognitionIn May, 12 of GHS Children’s Hospital’s 14 pediatric primary care practices were awarded recognition at Level 3 (highest status) by the National Committee for Quality Assurance (NCQA) Patient-Centered Medical Home Program. The Center for Pediatric Medicine was the first to attain this status in 2013 (see also Page 19). The other practices to attain Level 3 include all three Christie Group offices, all Pediatric Associates locations, Carolina Pediatrics of Greenville, and The Children’s Clinic’s Greenville, Greer and Simpsonville offices.
Heritage Pediatrics & Internal Medicine–Wren (in collaboration with Baptist Easley) also earned Level 3 recognition. Heritage Pediatrics & Internal Medicine–Simpsonville earned Level 2 designation.
The NCQA Patient-Centered Medical Home standards emphasize the use of systematic, patient-centered, coordinated care that supports access, communication and patient involvement. The recognition programs are built on evidence-based, national clinical standards of care. Learn more at ghs.org/pcmh.
GMH Receives Grant for Baby-Friendly StatusGreenville Memorial Hospital was awarded $25,000 from the SC Department of Health and Human Services’ Birth Outcomes Initiative (BOI) for achieving Baby-Friendly designation. This international designation recognizes hospitals and birthing centers that offer an optimal level of care for infant feeding and mother/baby bonding. Learn more at ghswomens.org.
(l-r) Sarah Taylor, MD, then-chair of the SC BOI’s Baby-Friendly Workgroup; BZ Geise, director of SC BOI; and Jennifer Hudson, MD, medical director of Newborn Services at Children’s Hospital, at the check presentation ceremony in March.
Dr. Hayes Elected to National BoardJames Hayes, MD, has been elected to the National Alliance on Mental Illness’ national board of directors. Dr. Hayes served for many years in the Division of Pediatric Hematology/Oncology at Children’s Hospital before he retired.
CelebrationsChildren’s Hospital of Greenville Health System (GHS) has many reasons to celebrate.
20 Tune in to the Children’s Hospital Radiothon on August 27-28!

21
Safe Kids™ Highlighted in International VideosSafe Kids Upstate, led by GHS Children’s Hospital, was featured in two videos to be used by Safe Kids Worldwide. The videos contain various aspects of a routine car seat inspection, along with short interviews.
One video will be used to help recruit General Motors dealerships to partner with local Safe Kids coalitions. The other will focus on child passenger safety and the importance of getting car seats inspected, plus highlight how partnerships with community groups make inspections accessible.
Safe Kids Upstate was chosen for the videos because of their strong partnerships with Bradshaw Automotive Group and local fire departments.
Safe Kids staff and their VP George Maynard with Greenville Drive mascot Reedy Rip-It and members of the baseball team.
Col. Doug Horton of the GHS Police Department fits a helmet during Safe Kids Night at the Drive.
Driving Home the Safe Kids Message Safe Kids held its annual Night at the Drive on April 12 at Fluor Field. The event featured bicycle helmet fittings and four activity stations focused on sports, home, child passenger and fire safety for children and adults. Safe Kids staff fitted more than 450 helmets at the event.
Safe Kids Museum ExhibitThe Children’s Museum of the Upstate will host a safety-themed exhibit as part of the 20-year anniversary of Safe Kids Upstate. The exhibit will run September 26 through January 3.

22
Pediatric Home Sleep Testing StudyHome sleep testing is a well-accepted technology for diagnosing obstructive sleep apnea (OSA) in adults who have a high pretest probability for moderate to severe OSA who do not have any other suspected comorbid sleep disorders. It is significantly easier for patients and is dramatically less expensive than attended overnight polysomnography.
The effectiveness of home sleep studies has not been well described in children, and currently there is no FDA indication for use in pediatric patients. If we are able to demonstrate efficacy of home sleep testing in children, it could potentially broaden access to care for children across the nation, as well as lead to a significant healthcare savings for families and managed care organizations.
Up to 50 patients will be selected by chart review and offered the chance to take part. Participants will attend overnight polysomnography as ordered by their sleep physician and complete a sleep questionnaire. Participants also will wear an overnight home sleep testing device within seven days of their in-lab polysomnography.
Patient Selection/Exclusion Criteria1. Age 12 to 18
2. No past medical history of significant psychiatric illness, congestive heart failure, neuromuscular disease, significant developmental delay, moderate to severe pulmonary disease or active pregnancy.
3. Investigators will give preference to patients who have no concern for comorbid sleep disorders such as moderate-to-severe insomnia, severe periodic limb movement disorder (PLMD), frequent parasomnias, nocturnal seizures or REM sleep behavior disorder; however, they may allow participants with narcolepsy or circadian rhythm disorders at the PI’s discretion for purposes of this study.
Contact Ford Shippey, MD, for more information about this study at [email protected] or (864) 454-5660.
Xyrem Pediatric Narcolepsy StudyThe Xyrem Pediatric Narcolepsy Study is a 52-week, Phase 3 randomized, double-blind, open-label, multicenter clinical trial that will evaluate the safety, efficacy and pharmacokinetics of Xyrem in narcolepsy patients ages 7 to 17. Ford Shippey, MD, is the principal investigator for GHS in this multi site study. The trial will enroll up to 100 pediatric patients globally at sites in the US and several countries in Europe.
Xyrem is the only US Food and Drug Administration (FDA) approved treatment for narcolepsy with cataplexy in adults. The FDA approval was based on clinical data in primarily adult patients.
Contact Ford Shippey, MD, for more information about this study at [email protected] or (864) 454-5660.
Clinical Research UpdateResearch studies at Children’s Hospital of Greenville Health System (GHS) are approved by GHS’ Institutional Review Board.

23
Baby-Friendly Initiative Reduces HyperbilirubinemiaJennifer Hudson, MD, medical director of Newborn Services at GHS Children’s Hospital; Britni Bradshaw, MD; and Mark Krom, DO, have completed a retrospective study on the impact of Baby-Friendly practices on hyperbilirubinemia rates. The results of the study show a significant increase in exclusive breastfeeding and a corresponding dramatic reduction in rates of neonatal hyperbilirubinemia.
The trio studied two groups of approximately 1,200 healthy newborns, one pre-implementation of the Baby-Friendly Hospital Initiative (BFHI) in 2011 and one post-implementation in 2013. After BFHI implementation, overall exclusive breastfeeding rates increased from 30% to 71%. Hyperbilirubinemia rates decreased overall from 17.5% to 6.8%, and among newborns exclusively breastfed, the rate fell from 31% to 5.3% (Figure 1).
This study is the first to demonstrate that implementation of the BFHI is associated with significant increases in overall exclusive breastfeeding and with significant decreases in neonatal hyperbilirubinemia, without an increase in readmission rates.
Exclusive breastfeeding has historically been considered a risk factor for neonatal hyperbilirubinemia. The authors hypothesized that implementing BFHI, with its emphasis on early and effective exclusive breastfeeding, significantly reduced exclusive breastfeeding as a risk factor for hyperbilirubinemia in the newborn population.
The basis of the BFHI are the Ten Steps to Successful Breastfeeding (Table 1), through which hospital staff and physicians provide intensive support to breastfeeding mothers, helping them establish effective breastfeeding. Effective breastfeeding provides adequate nutrition to the newborn, reducing the risk of hyperbilirubinemia.
For more information about the study, contact Dr. Hudson at [email protected].
0
5
10
15
20
25
30
35
All Newborns Late Preterm Exclusively Breastfed
Perc
ent o
f Inf
ants
2011 (n=1098)
2013 (n=1303)
17.5
6.8
16.5
7.5
31
5.3
Figure 1: Rates of Neonatal Hyperbilirubinemia Before and After BFHI Implementation
Table 1Ten Steps to Successful Breastfeeding
Every facility providing maternity services and care for newborn infants should …1) Have a written breastfeeding
policy that is routinely communicated to all healthcare staff.
2) Train all healthcare staff in the skills necessary to implement this policy.
3) Inform all pregnant women about the benefits and management of breastfeeding.
4) Help mothers initiate breastfeeding within one hour of birth.
5) Show mothers how to breastfeed and how to maintain lactation even if they are separated from their infants.
6) Give infants no food or drink other than breastmilk, unless medically indicated.
7) Practice rooming-in—allow mothers and infants to remain together 24 hours a day.
8) Encourage breastfeeding on demand.
9) Give no pacifiers or artificial nipples to breastfeeding infants.
10) Foster the establishment of breastfeeding support groups and refer mothers to them on discharge from the hospital or birth center.
Source: Baby-Friendly Hospital Initiative (babyfriendlyusa.org)

24
Feature StoryArticle author Liz Dancel, MD, is a pediatric gastroenterologist at Children’s Hospital of Greenville Health System (GHS).
Improving IBD Care Through Collaboration
The number of children in the US diagnosed with inflammatory bowel disease (IBD) continues to grow. Currently, over 100,000 children under age 18 may have IBD. In the Division of Pediatric Gastroenterology at GHS Children’s Hospital, we follow more than 200 children and adolescents with Crohn’s disease or ulcerative colitis.
Since March 2013, Children’s Hospital has been an active member of ImproveCareNow, a national collaborative of pediatric GI providers whose aim is to improve care for children with IBD by building a sustainable chronic care network that enables patients, their families, clinicians and researchers to work together.
Children’s Hospital’s Division of Pediatric Gastroenterology Is Part of National Network
GHS was the first program in the state to enroll patients in the ImproveCareNow Network, and we continue to ensure all of our patients with IBD are enrolled in the registry. In addition, we have been actively involved in identifying parents and/or adolescent patients to act as partners with the healthcare team to improve access, communication and overall care of our children with IBD.
One of our first goals is to work with our parent partners to develop an IBD “handbook” to use as a resource for our families. We have implemented monthly “Population Management” meetings with providers to keep them updated on our progress in enrollment, discuss data quality and review our clinical
Members of Children’s Hospital’s Division of Pediatric Gastroenterology: (back row, l-r) Colston McEvoy, MD; Janet Williams, RD; Amy Hayes, RN; Jonathan Markowitz, MD, MSCE; Michael Dougherty, DO; Carrie Frost, RN; Emily Kevan, MD; (front row, l-r) Donna Wade, PNP; Liz Dancel, MD. Not pictured: Mary Frances Stribling, RN.

25
outcome measures. Some outcomes ImproveCareNow is particularly interested in are clinical remission, adequate nutrition and growth, and model treatment (such as percent of patients seen within the last 200 days or percent on the recommended dose of their specific medication).
ImproveCareNow is the largest and fastest-growing pediatric IBD registry, with 610 participating pediatric gastroenterologists representing 74 care centers. Based on data from April 2015, 78% of patients enrolled in the network were in remission, 95% were not taking steroids, 93% had satisfactory growth and 90% showed satisfactory nutrition.
Since the network’s inception in 2007, the remission rate has increased from 50% to 78% without the introduction of any new medications. Currently, over 20,000 patients are enrolled in the network, and every one of them is helping us expand our knowledge on how best to care for children and adolescents with IBD.
At GHS, not only are we actively involved in quality improvement, but we also are participating in several clinical research initiatives being conducted in conjunction with the ImproveCareNow Network. Children’s Hospital is a clinical site for a patient-reported outcome measure initiative involving our IBD patients already enrolled in the network. We also will be a site for an upcoming clinical trial looking at methotrexate and TNF inhibitors, two classes of medications commonly used to treat patients with IBD.
As a pediatric gastroenterologist, I have had a longstanding interest in IBD. As the physician leader for our site, I recently attended the biannual Community Conference in Chicago, where I learned more about the importance of working together as a community of physicians, nurses, dietitians, psychologists, coordinators, parents and patients to raise the standard of care for pediatric IBD.
“Share seamlessly and steal shamelessly” is a running theme of the network, based on the idea that working together and sharing resources can result not only in changes and improvements at a single institution, but also in system-wide improvements across all participating care centers.
Through our involvement with the ImproveCareNow Network, we are able to take part in quality improvement, learn more precisely how our patients are doing, and establish systems for measuring and tracking our performance. We also learn from and collaborate with other centers of excellence that
20,600
93%
95%
49% 90%
74
34
610
35 50
7 10
75%
April 2015
78%
share similar goals. We are excited to be part of this endeavor, and it is our hope that collaborating with this network will lead to the best care possible for our patients with IBD.
For more information about Children’s Hospital’s involvement in the ImproveCareNow Network, contact Dr. Dancel at [email protected] or (864) 454-5125.
We are excited to be part of this endeavor, and it is our hope that collaborating with this network will lead to the best care possible.
26
Q: I’ve heard about a study that indicates early introduction of peanuts may help prevent peanut allergy in children. Can you tell me more about the study?
A: Peanut allergy is this country’s leading cause of food anaphylaxis and death resulting from a food allergy. It carries a significant economic and psychological impact on patients and their families.
Guidelines from the American Academy of Pediatrics (AAP) in 2000 recommended exclusion of allergenic foods from the diets of infants at high risk for food allergy as well as their mothers during pregnancy and lactation. In addition, the AAP recommended parents refrain from feeding peanuts to children at risk for allergic disease until age 3.
However, those guidelines came into question in the late 2000s, after the prevalence of peanut allergies in
For many parents and healthcare providers, this study has been a dramatic change in their understanding of peanut allergy.
Ask the FacultyArticle author John Pulcini, MD, is an allergist/immunologist at Acadia Allergy & Immunology, which is affiliated with Greenville Health System (GHS).
Peanut Allergy Western nations more than doubled in a span of 10 years. In 2008, the AAP retracted its recommendation that mothers exclude peanuts from their diets during pregnancy or lactation to prevent the development of food allergy. But the clinical question remained whether early exposure to or avoidance of peanuts is the better strategy to prevent peanut allergy.
The LEAP Study (Learning Early About Peanut), a five-year study that was performed in the United Kingdom and published in March 2015, evaluated infants in two groups—one with early peanut consumption and another with peanut avoidance.
In this study, 640 infants age 4-11 months with severe eczema, egg allergy or both were skin tested to investigate for peanut sensitivity. Next, study participants were split into two groups—those who were mildly peanut skin-test sensitive (skin test of 1-4 mm) and those who were entirely negative. Infants

Pediatric Specialty Services
William F. Schmidt III, MD, PhD _____________________(864) 455-8401 Medical Director; Chairman, Department of PediatricsKerry K. Sease, MD, MPH _______________________________ 455-7895 Pediatric Residency Program DirectorRuss C. Kolarik, MD ____________________________________ 455-7844 Medicine-Pediatrics Residency Program Director Desmond P. Kelly, MD __________________________________ 454-5115 Developmental-Behavioral Fellowship Program Director
Adolescent Pediatrics ___________________________________ 220-7270Allergy and Immunology_________________________________ 675-5000Ambulatory Pediatrics __________________________________ 220-7270Cardiology ____________________________________________ 454-5120Child Abuse and Neglect/Forensic Pediatrics ______________ 335-5288 Critical Care ___________________________________________ 455-7146Developmental-Behavioral Pediatrics ______________________ 454-5115 Emergency Pediatrics ___________________________________ 455-6016Endocrinology __________________________________________ 454-5100Gastroenterology _______________________________________ 454-5125Genetics _______________________________________________ 250-7944Hematology/Oncology __________________________________ 455-8898Infectious Disease ______________________________________ 454-5130Minor Care (Spartanburg Night Clinic) ____________________ 804-6998 Children’s Hospital After-Hours Care ___________________ 271-3681Neonatology ___________________________________________ 455-7939Nephrology and Hypertension ____________________________ 454-5105Neurology _____________________________________________ 454-5110Neurosurgery __________________________________________ 797-7440Newborn Services ______________________________________ 455-3512 Ophthalmology _________________________________________ 454-5540Orthopaedic Oncology __________________________________ 797-7060Orthopaedic Surgery ____________________________________ 797-7060Plastic Surgery _________________________________________ 454-4570Pulmonology ___________________________________________ 454-5530Radiology ______________________________________________ 455-7107Rheumatology __________________________________________ 454-5004 Sleep Medicine _________________________________________ 454-5660Supportive Care Team (formerly Palliative Care) ____________ 455-5129Surgery ________________________________________________ 797-7400Urgent Care (Anderson) _________________________________ 512-6544Urology________________________________________________ 454-5135
Children’s Hospital Programs
BI-LO Charities Children’s Cancer Center __________________ 455-8898Bryan Neonatal Intensive Care Unit _______________________ 455-7939Center for Complex Health Conditions ____________________ 220-7270Child Life ______________________________________________ 455-7846Children’s Advocacy Program ____________________________ 454-1100Cystic Fibrosis Clinic ____________________________________ 454-5530Family Connection ______________________________________ 331-1340Gardner Center for Developing Minds _____________________ 454-5115Infant Apnea Program ___________________________________ 455-3913International Adoptee Program ___________________________ 454-5130Kidnetics® (pediatric therapies) __________________________ 331-1350Neonatal Developmental Follow-up Services _______________ 331-1333New Impact (weight management) _________________ 675-FITT (3488)Office of Philanthropy & Partnership/CMN ________________ 797-7735Pastoral Care ___________________________________________ 455-7942Pediatric HIV Clinic _____________________________________ 454-5130 Safe Kids™ Upstate _____________________________________ 454-1100Wonder Center _________________________________________ 331-1380 Day treatment for medically fragile children
For admission to Children’s Hospital: (864) 455-0000This number connects you to GHS’ Patient Referral and Transfer Center, which can handle all arrangements for admission. You also may call 455-7000 and ask the operator to page the admitting resident.
Neonatal Transport _________________________________ (864) 455-7165
To reach a Children’s Hospital doctor or program, call 1-800-4RBUDDY.
Pediatric Outpatient Service LocationsCall the appropriate Greenville number above for an appointment.
AndersonCardiologyEndocrinologyHematology/OncologyNephrology and HypertensionNeurosurgery
GreenwoodCardiologySurgery
Spartanburg(864) 573-8732CardiologyDevelopmental-BehavioralEndocrinologyGastroenterology/NutritionHematology/OncologyKidneticsNephrology and HypertensionNeurologyNeurosurgeryPulmonologySleep MedicineUrology
27
whose skin test was greater than 4 mm were considered strongly positive and excluded.
These two groups were further divided into a peanut consumption group (consuming 6 grams of peanut protein per week) or a peanut avoidance group (not consuming peanut at all). Participants followed these guidelines until age 5 and then the authors determined the percentage of peanut sensitivity in each group.
The results showed that in the group initially negative to peanuts (n=530), the prevalence of peanut allergy at age 5 was actually higher in the group that avoided peanuts (13.7%) as compared to the infants advised to consume peanuts at a regular interval (1.9%). Of those who had mild positive peanut skin prick testing at the onset of the study (n=98), which may indicate mild peanut allergy, the prevalence of peanut allergy at age 5 was again higher in the avoidance subgroup (35.3%) as compared to 10.6% in the consumption group.
As a result of these findings, the authors concluded that early introduction of peanuts significantly decreased, by 70-80%, the frequency of peanut allergy among children at high risk for peanut allergy—even in those who already showed an early low-level sensitization.
For many parents and healthcare providers, this study has been a dramatic change in their understanding of peanut allergy. Unfortunately, many questions remain unanswered: Will different doses and frequencies of peanut have the same effect? If regular peanut consumption is discontinued for a period, will tolerance persist or is it transient? How do these results impact patients with severe peanut anaphylaxis? Can these results be applied to patients with other food allergies?
Questions aside, the study results are compelling enough that leading US experts in food allergy research already are recommending a new approach: Infants 4-8 months of age believed to be at risk for peanut allergy should undergo peanut skin-prick testing. If the test is negative, patients should start 2 grams of peanut protein three times a week for three years. If the test is mildly positive (greater than 4 mm), they should undergo a physician-observed oral food challenge before consuming peanuts in their diet.
For more information, call Dr. Pulcini at (864) 675-5000.
References1. Du Toit, G, Robert, G, Sayre, P et al. Randomized Trial of Peanut
Consumption in Infants at Risk for Peanut Allergy. N Engl J. Med 2015; 272; 9:803-813.
2. Gruchalla, R and Sampson, H. Preventing Peanut Allergy through Early Consumption—Ready for Prime Time? N Engl J. Med 2015; 272; 9:875-877.

Non-Profit Org.U.S. Postage
P A I DGreenville SC
Permit No. 842
701 Grove RoadGreenville, SC 29605-5601
Change Service Requested
Picture Book Benefits GHS Children’s Hospital
For information about Children’s Hospital giving opportunities, call GHS’ Office of Philanthropy & Partnership at (864) 797-7732 or visit ghsgiving.org.
Joe Maurer, MD, a pediatrician at The Children’s Clinic, has written a children’s book titled Goodnight Greenville. The book, derived from the classic children’s picture book Goodnight Moon, features whimsical illustrations of some of Greenville’s most beloved attractions—including Falls Park, GHS Swamp Rabbit Trail and Fluor Field—drawn by local artist Joseph Bradley.
Children’s Hospital also is featured in the story, and benefits from book sales go to the Child Life Program at Children’s Hospital. Child life specialists work one-on-one with children and families to ease the stress of medical procedures and hospitalizations.
“The Greenville community is rightfully proud of the extraordinary landmarks that have made it so iconic and resonated with families throughout the years,” noted Dr. Maurer. “I believe the book is a perfect fit for our community. My hope is that this book taps into children’s enjoyment of our many landmarks to engage them in reading.”
Greenville Mayor Knox White already is a fan. “Goodnight Greenville is a wonderful book that takes kids on an adventure through many of the landmarks that make our city great,” he said. “It is a book that we can be proud of and that all Greenville families should have on their nightstands.”
The book is available at several upstate venues, such as The Children’s Museum of the Upstate, Greenville Zoo and GHS gift shops. The cost is $17.99 plus tax.
For more information and to find out how to purchase the book online, visit goodnightgreenville.com.
GHS VisionTransform health care for the benefit
of the people and communities we serve.
GHS MissionHeal compassionately. Teach Innovatively.
Improve constantly.
GHS ValuesTogether we serve with integrity, respect,
trust and openness.
Visit our website: ghschildrens.orgCheck out our Family Advisory Council at
facebook.com/ChildrensHospitalFACConnect at
twitter.com/ghs_childrens
Written by Joe Maurer Illustrated by Joseph Bradley
Proceeds from this book go directly to Child Life, a part
of Children’s Hospital of Greenville Health System.
Through Child Life, certified educational and
developmental specialists work one-on-one with
children and families to ease the stress and even
trauma of medical procedures and hospitalizations.
Interventions range from bubble-fueled distraction
therapy to medical play, age-appropriate explanations
of procedures and extended support for families
facing difficult situations. Many hospitals do not offer this service, and many
Child Life activities and services depend solely on the
generosity of donors. Thank you for your support of
this valuable program! To learn more about Child Life,
visit ghschildrens.org/child-life.
ISBN 978-0-692-41058-5$17.99Printed in Greenville, SC
9 780692 410585
51799>
ISBN 978-0-692-41058-5
$17.99
GOO
DNIGHT GREENVILLE
MA
URER/BRA
DLEY